 Michael Silvey
Michael Silvey Leonardo R. Brandão
Leonardo R. Brandão- 1Department of Pediatrics, Children’s Mercy Hospital, Kansas City, MO, United States
- 2Department of Paediatrics, University of Toronto, Toronto, ON, Canada
Congenital heart disease (CHD) is a common condition in the pediatric population, affecting up to 1% of all live births (i.e., around 40,000 newborns/year in the United States). Although CHD does have a wide range of severity, by the age of 5 years approximately 80% of patients will require at least one surgical intervention to achieve a complete/palliative cardiac repair. Today, in light of their much-improved surgical survival, the care of these patients focuses on morbidity prevention and/or treatment. One such morbidity has been the increased frequency of thrombotic occlusions [e.g., cardioembolic arterial ischemic strokes; arterial, cardiac, and/or newly created shunt thrombosis; venous thromboembolism (VTE)]. Patients with CHD are at high risk of developing thrombosis due to the disruption of blood flow, CHD-related coagulopathy, inflammation, and/or platelet activation secondary to extracorporeal circulation support required during open-heart surgery or as a bridge to recovery, which can increase thrombus formation. In this article, we will discuss how the coagulation system is altered in patients with CHD in regard to the patient’s anatomy, procedures they undergo to correct their congenital heart defect, and other risk factors that may increase their thrombotic risk, focusing on VTE. We will also discuss the most recently published reports pertaining to guidelines on prophylaxis and treatment of VTE in this population. Finally, we will briefly address the long-term VTE outcomes for patients with CHD.
Introduction
Congenital heart disease (CHD) is a common condition that affects approximately 40,000 births/year in the United States. Most cardiac birth defects classified as CHD occur in healthy children and are relatively minor (1). By contrast, until recently, complex CHD was accompanied by a significant mortality rate. Although survival has significantly improved, CHD patients are still at risk of significant morbidities particularly after their cardiac surgeries (2). Therefore, a better understanding of venous thromboembolism (VTE), one of the most common types of thrombotic occlusions occurring in this specific group, has become imperative, due to the increasing VTE incidence in hospitalized pediatric patients, including CHD patients (3–5). Moreover, it is well known that CHD is one of the main underlying conditions contributing to VTE in pediatric patients (6, 7).
Congenital heart disease patients are at high risk of developing thrombosis for various reasons: the type of cardiac defect, CHD-related complications, and stage of their care. For example, many of the structural cardiac abnormalities lead to changes in blood rheology or to natural anticoagulant deficiencies due to hepatic hypoperfusion secondary to impaired heart function, further contributing to a hypercoagulable state. In addition, many patients undergoing open-heart surgery necessitate cardiopulmonary bypass, where the required blood product exposure can lead to hemodilution and coagulation derangements. Finally, the increasing use of central venous catheterization in the care of such patients has also contributed to the VTE incidence escalation in this patient population.
This review will discuss several factors that increase the risk of developing thrombosis in CHD patients, including coagulation system changes due to their CHD and the procedures that they undergo to correct their heart defects. VTE prophylaxis and treatment will also be discussed. As these patients now have a normal or near normal lifespan, long-term VTE outcomes will also be discussed briefly.
Differences in the Coagulation System of CHD Patients
The coagulation system in neonates and infants is physiologically distinct from adulthood. Neonates and infants have lower concentrations of both pro-coagulant and natural anticoagulant proteins compared to adult values, as a reflection of the physiologic developmental hemostasis process that occurs in all children. Circulating levels can take up to 12 months, and in some instances only reach adult levels in adolescence (8, 9). Furthermore, neonatal and infant CHD patients have lower concentrations of pro-coagulant and natural anticoagulant proteins than normal age-appropriate controls (10–13). The cause for lower concentrations of coagulation proteins is believed to be multifactorial (i.e., increased consumption, decreased production, and increased fibrinolysis).
As CHD patients have their surgical corrective procedures, the coagulation profile showing decreased pro-coagulant and anticoagulation proteins is enforced. Odegard et al. examined coagulation profiles of 37 patients with hypoplastic left heart syndrome before their stage I palliation, bidirectional Glenn, and before and after the Fontan procedure. The investigators found that all coagulation proteins were at significantly lower concentrations except for factor VIII, which only increased after the Fontan procedure (12). The authors posited that the increased factor VIII production was due to increased production from liver sinusoidal epithelium secondary to chronically elevated central and hepatic venous pressures associated with Fontan physiology.
Congenital heart disease patients may also present with thrombocytopenia (10), which is multifactorial. For instance, thrombocytopenia can be secondary to hypoxic inhibition of platelet production, increased platelet destruction with shunt placement in single-ventricle physiology, or increased RBC production. Lill et al. hypothesized that right-to-left shunts in CHD patients decreased megakaryocyte delivery to the lungs, impairing platelet production in the pulmonary bed (14). In addition, CHD patients have been shown to have abnormal platelet function. Maurer et al. reported decreased aggregation when platelets were exposed to platelet agonists (15). Furthermore, Bailly et al. found patients with systolic flow abnormalities to have abnormal platelet function (16), which could be explained by the fact that CHD patients may develop acquired von Willebrand disease, known to affect platelet aggregation testing (17). Finally, CHD associated with other genetic disorders may also present with platelet dysfunction. CHD patients with Noonan’s syndrome, velocardiofacial syndrome, and Jacobson’s syndrome can have quantitative or qualitative platelet defects, which can increase risk of bleeding.
The Coagulation System and Cardiopulmonary Bypass (CPB)
Patients who undergo CPB are temporarily exposed to a non-physiologic circulatory system, which disrupts their coagulation system. Once CPB is initiated, the contact factors are activated, and tissue factor is exposed, which lead to increased thrombin generation. Upon thrombin generation, production of fibrin as well as protein C activation (18) ensues. Therefore, as a result of the increased thrombin generation and subsequent fibrin deposition within the CPB circuit, anticoagulation is required during CPB to prevent excessive thrombus formation. In addition to consumption of several coagulation factors within the circuit, platelets are significantly affected during CPB. When CHD patients are placed on CPB, platelet activation occurs immediately (19, 20) followed by platelet consumption, leading to an acquired quantitative or qualitative platelet defect (21). Patients younger than 1 year of age are more likely to have this complication. Second, hemodilution due to priming of the CPB circuit can also lead to thrombocytopenia. Third, CPB confers a pro-inflammatory state as it activates both humoral and cellular aspects of the immune system (18). With the activation of the inflammatory response, endothelial cells will express tissue factor, further promoting thrombin generation (22). Consequently, in light of the CPB-induced coagulopathy that may develop, CHD patients have an increased risk of bleeding in the immediate post-operative period and can be treated with blood-derived products, anti-fibrinolytics, and hemostatic agents such as recombinant activated factor VII (23), as needed.
Cyanotic CHD and Thrombosis Risk Factors
Patients with cyanotic CHD (e.g., Tetralogy of Fallot, tricuspid atresia, and single-ventricle physiology) can be at high risk of developing VTE due to the surgical procedures required to correct their originally abnormal cardiac anatomy. The Blalock–Taussig (BT) shunt is a common surgical procedure in neonates with single-ventricle physiology, where a shunt is created between the subclavian artery and the ipsilateral pulmonary artery to increase pulmonary blood flow (24, 25). This shunt creates a low blood flow area that increases the risk of thrombosis, and surgically removed shunts have been found to be obstructed. Of note, complete BT shunt obstruction creates a significant decrease in pulmonary blood flow, almost invariably requiring an immediate mechanical thrombectomy. The frequency of BT shunt thrombosis reported in the literature ranges from 1 to 17% (24). Wells et al. reported BT shunt histopathology for the detection of shunt obstruction from 155 patients and found a median shunt lumen narrowing of 34%. Moreover, 21% of cases showed a shunt stenosis greater than 50%. The identified risk factors for obstruction were smaller shunt size, age less than 14 days, and shunt placement while on bypass (26).
A second palliative surgical procedure to increase oxygenation in patients with single-ventricle physiology is the bidirectional Glenn procedure. This procedure connects the superior vena cava to the right pulmonary artery (27). The largest concern regarding thrombosis is the development of pulmonary embolism, with a subsequent increase in pulmonary vascular resistance, making patients unsuitable for further palliative surgeries (25). Though Glenn Shunt thrombosis is rare, a study by Manlhiot et al. comprising 203 cardiac operations performed in single-ventricle patients showed that the second highest occurrence of VTE (12%) corresponded to cavopulmonary shunt operations (28).
The final palliative surgical stage for single-ventricle physiology patients is the Fontan procedure. This procedure involves rerouting the systemic venous return directly to the pulmonary arteries (29). The Fontan procedure has undergone many modifications, though the mechanism of the anastomosis of the inferior vena cava to the pulmonary arteries has remained unchanged (25). Patients undergoing the Fontan procedure are also at an increased risk of developing thromboembolism, and the reported incidence of thromboembolism ranges from 3 to 20% (30). Identified post-Fontan thrombosis risk factors include passive blood flow, chronic venous hypertension, and atrial arrhythmias. Patients undergoing Fontan procedures were found to have elevated factor VIII levels, which may further increase VTE risk (12). Patients may or may not have a fenestration placed within the atria; the latter procedure could lead to the development of paradoxical emboli if a thrombotic source is present within the right cardiac chambers. As many modifications have been made to the Fontan, Coon et al. examined whether thrombosis rates and risk factors varied among patients undergoing different types of procedures. No difference was found in thrombosis incidence in either the pulmonary or venous system in any of the modifications (31). These findings suggest that the physiology of the Fontan circulation leads to thrombus formation.
Additional cyanotic CHD conditions do not pose higher thrombotic risk. The higher risk of these patients developing thrombosis is more strongly associated with CPB and the coagulation abnormalities described earlier.
Acyanotic CHD
Patients with acyanotic congenital heart lesions do not usually have a significant rate of thrombotic complications. Depending on the type of atrial/ventricular septal defect, the patient may or may not undergo CPB surgery to close the defect (32). Ventricular septal defects are more likely to require surgical closure than atrial septal defects. Recent advances in interventional closure devices, specifically for perimembranous ventricular septal defects, have decreased the need for CPB (33, 34).
Cardiac Catheterization
Congenital heart disease patients commonly undergo a cardiac catheterization procedure for both diagnostic and treatment purposes. When undergoing cardiac catheterization, the femoral artery or femoral vein is accessed for catheter insertion immediately prior to a bolus of unfractionated heparin (UFH). Thrombosis and pulse loss after catheterization are known complications of this procedure. Venous thrombosis has a prevalence ranging from 0 to 27% and the reported prevalence for femoral artery occlusion is between 0.6 and 9.6% (35–38). Post-cath thrombosis risk factors in both the femoral artery and vein include younger age, patient size, use of larger catheters, longer procedural time, and need for repeat procedures.
VTE Prophylaxis for CHD Patients
Due to the high risk of developing thrombosis with CHD and cardiac surgery, studies have examined the role of thromboprophylaxis to decrease thrombosis development. Low molecular weight heparin (LMWH), oral vitamin K antagonists (OVKA; i.e., warfarin), and aspirin have been successfully used as primary thromboprophylaxis options for CHD patients undergoing cardiac procedures; this strategy has also decreased patient mortality (39, 40). To help clinicians decide which prophylaxis is more appropriate, evidence-based guidelines for the management of CHD patients after cardiac surgery have been published (41–43).
Antiplatelet Therapy
Aspirin is widely used; commonly, it is typically started on patients after systemic to pulmonary shunt placement as long-term prophylaxis. Additionally, aspirin may also be considered for primary prophylaxis in children undergoing the Fontan procedure (44). The usual aspirin dosing for prophylaxis is 3–5 mg/kg daily, and treatment duration can vary. Aspirin prophylaxis may be used in patients undergoing cardiac catheterization if a device is placed during the procedure. Clopidogrel, another antiplatelet agent, is increasingly being used in children (45). Despite its widespread use, a recent trial showed clopidogrel was not more effective than placebo in reducing mortality or shunt-related morbidity in high risk CHD patients (46).
Anticoagulation Therapy
Unfractionated heparin and warfarin are the most commonly used anticoagulants for patients undergoing cardiac surgery. UFH is used mostly as an immediate post-operative medication for thromboprophylaxis, particularly in patients undergoing a systemic to pulmonary shunt placement. For patients with clinically significant post-operative bleeding, low-dose standard heparin may be preferred prior to starting antiplatelet therapy. Systemic heparinization may also be continued with additional antiplatelet therapy if there is sustained high risk of developing thrombosis. In such cases, further evaluation regarding the thrombosis risk will determine whether the UFH infusion needs to be switched to LMWH in addition to aspirin.
Warfarin prophylaxis may be started on patients after the Fontan procedure for, at least, 3–12 months. Warfarin may be continued for much longer periods when in the presence of certain thrombosis risk factors. Patients are usually dosed to maintain an international normalized ratio (INR) between 2.0 and 3.0 to minimize bleeding risk. Point-of-care monitoring is likely an option for outpatient INR laboratory monitoring in children receiving long-term oral anticoagulation with an OVKA (47). Direct oral anticoagulants (DOACs) are not approved for use in the pediatric population and are only recommended for pediatric patients if they are participating in a clinical trial. At present, there is only one clinical trial open for the use of a DOAC in CHD patients (Apixaban in Children with Cardiac Conditions; NCT02981472).
Patients undergoing a cardiac catheterization usually receive a heparin bolus prior to and possibly during the catheterization, if the procedure extends beyond 2 h. Patients are usually given 100 U/kg prior to the procedure, but smaller doses have also been employed (48). Activated clotting time allows monitoring monitor anticoagulation, and heparin bolus dosing should be determined following the American Heart Association Guidelines (43).
Risk Factors of VTE in CHD Patients
Besides cardiac procedures, additional thrombosis risk factors have been identified in CHD patients (Table 1). Likely, the most pervasive VTE risk factor in children is central line (CVC) use. Central venous access is vital to manage children post-operatively, and many children with CHD will have multiple CVCs placed at once in both the lower and upper extremities. Moore et al. prospectively evaluated CVC-related VTE in CHD patients via lineograms at CVC removal and reported a VTE prevalence of 20%. All lines were placed in the jugular veins; 60% of thromboses were located in the jugular veins while the remaining 40% were located in the right atrium (49). Additionally, Hanson et al. found 41% of CHD patients developing a VTE to have a CVC-related event. The time length of CVC placement was directly associated with thrombosis (50).
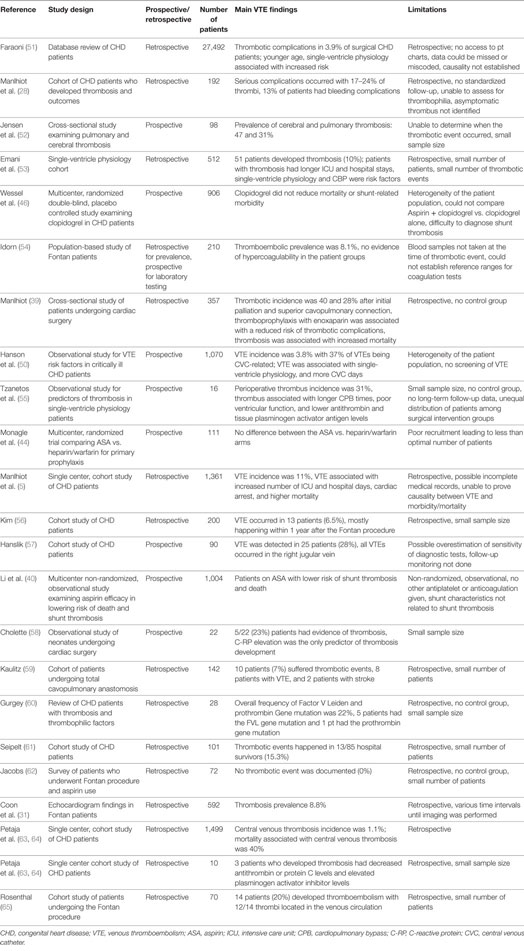
Table 1. Published literature regarding thrombosis risk factors and outcomes in CHD patients.
Other studies have examined additional potential VTE risk predictors, including clinical and laboratory markers. Tzanetos et al. examined 19 patients who underwent palliative surgery for single-ventricle physiology and found that those who developed thrombus had worse pre-operative ventricular function, longer CPB time, decreased circulating antithrombin levels, and increased tissue plasminogen activator antigen concentrations (55). Similarly, Petaja et al. examined 10 neonates who underwent CPB. Three patients developed thrombosis and were found to have decreased circulating antithrombin or protein C levels and elevated plasminogen activator inhibitor levels (63).
Aspirin prophylaxis response has also been explored as a predictor of VTE development. Emani et al. described decreased aspirin response as a predictor for VTE development; 95 patients were followed 30 days after initiation of aspirin therapy. Patients not responding to aspirin, particularly patients weighing less than 5 kg had a higher thrombosis rate compared to those showing adequate aspirin response (53). Mir et al. examined the incidence of aspirin responsiveness in 20 infants with single-ventricle physiology after palliative heart surgery by measuring urine thromboxane (UTX) levels and thromboelastography (TEG). The authors found aspirin resistance in around 80% of infants using TEG; no patients had adequate UTX levels and clinical variables such as age, weight, hemoglobin level, and platelet count were not associated with aspirin resistant status (66).
Congenital heart disease patients who undergo cardiac surgery are also at risk for developing ischemic stroke. Domi et al. examined 5,526 patients who underwent cardiac surgery and found that the incidence of arterial ischemic stroke/cerebral sinus venous thrombosis was 5.4 strokes per 1,000 children. Risk factors associated with stroke included older age, longer duration of CPB, reoperation, and number of days hospitalized after the operation (67).
VTE Treatment for CHD Patients
Patients with an acute, symptomatic VTE and no relevant contraindication are treated with anticoagulation, namely, systemic UFH or LMWH (41–43). The anticoagulation modality of choice depends on the circumstances of the patient (surgical needs, liver/kidney dysfunction). Patients started on systemic anticoagulation for VTE are usually treated for 3–6 months (41–43). Moreover, patients receiving systemic anticoagulation should be monitored throughout treatment for bleeding complications, and frequent laboratory testing is recommended to ensure their anticoagulation dosing is therapeutic. For patients undergoing UFH therapy, a target PTT of 70–100 s, which correlates to an anti-factor Xa level of 0.3–0.7, is considered therapeutic. For patients undergoing LMWH therapy, an anti-factor Xa level of 0.5–1.0 is considered therapeutic. Patients may be transitioned to warfarin therapy depending on their clinical circumstances, and the target INR for these patients is 2.0–3.0. If the patient does have a life or limb-threatening thrombus, thrombolysis should be strongly considered (41–43).
Outcomes for CHD Patients with VTE
Patients who undergo CPB surgery can be at significant risk of developing comorbidities if they develop VTE (Table 1). Manlhiot et al. retrospectively reviewed 1,361 CHD patients after cardiac surgery and described morbidities associated with VTE. VTE was associated with increased number of ICU days and increased length of stay. VTE was also associated with increased risk of cardiac arrest, and thrombosis-related mortality was 5%. However, in light of the retrospective study design, VTE causality could not be inferred (5). Pejata et al. also conducted a single center retrospective review to evaluate mortality in 20 CHD patients after developing thrombosis. VTE was associated with increased mortality rate, as VTE patients had a 40% mortality rate compared to patients who did not develop VTE (8.3%). Again, due to the study limitations, causality between VTE and mortality could not be established (64).
Long-Term Outcomes for CHD Patients
Post-thrombotic syndrome (PTS; chronic venous insufficiency secondary to vessel damage) is recognized as an important long-term complication in CHD patients. Brandao et al. examined 70 CHD patients aged 0.5–5 years after their surgical repair and found that 30% of patients had clinical evidence of PTS (68). Most patients had lower limb PTS, and all patients had mild PTS.
Post-thrombotic syndrome after cardiac catheterization is a newly recognized long-term complication for patients. Luceri et al. studied 62 patients who underwent cardiac catheterization and found that 40 children had PTS (prevalence 64%, 95% CI 51.3–76.3%). Most cases were mild, though seven children had clinically significant PTS (69).
Importantly, CHD patients seem to carry their increased thrombotic risk into adulthood. Jensen et al. reported a prevalence of cerebral and pulmonary thrombosis of 47 and 31%, respectively, in adult survivors (52).
Conclusion
The risk of thrombosis development in CHD patients is multifactorial. Thrombotic events lead to short- and long-term complications for these patients. Although guidelines for thromboprophylaxis and treatment are currently available, more research is needed to increase the knowledge of how thrombosis develops in these patients and how to prevent this common complication.
Author Contributions
MS performed the literature search and wrote the manuscript. LB also performed the literature search and edited the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hoffman JIE, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol (2002) 39(12):1890–900. doi:10.1016/S0735-1097(02)01886-7
2. Khairy P, Ionescu-Ittu R, Mackie AS, Abrahamowicz M, Pilote L, Marelli AJ. Changing mortality in congenital heart disease. J Am Coll Cardiol (2010) 56(14):1149–57. doi:10.1016/j.jacc.2010.03.085
3. Monagle P. Thrombosis in pediatric cardiac patients. Semin Thromb Hemost (2003) 29(6):547–55. doi:10.1055/s-2004-815637
4. Raffini L, Huang Y, Witmer C, Feudtner C. Dramatic increase in venous thromboembolism in children’s hospitals in the United States from 2001 to 2007. Pediatrics (2009) 124(4):1001–7. doi:10.1542/peds.2009-0768
5. Manlhiot C, Menjak I, Brandao L, Gruenwald C, Schwartz S, Sivarajan B, et al. Risk, clinical features, and outcomes of thrombosis associated with pediatric cardiac surgery. Circulation (2011) 124:1511–9. doi:10.1161/CIRCULATIONAHA.110.006304
6. Monagle P, Adams M, Mahoney M, Ali K, Barnard D, Berstein M, et al. Outcome of pediatric thromboembolic disease: a report from the Canadian thrombophilia registry. Pediatr Res (2000) 47(6):763–6. doi:10.1203/00006450-200006000-00013
7. Andrew M, David M, Adams M, Ali K, Anderson R, Barnard D, et al. Venous thromboembolism (VTE) in children: first analyses of the Canadian registry of VTE. Blood (1994) 83(5):1251–7.
8. Kuhle S, Male C, Mitchell L. Developmental hemostasis: pro- and anticoagulation systems during childhood. Semin Thromb Hemost (2003) 29(4):329–37. doi:10.1055/s-2003-42584
9. Nardi M, Karpatkin M. Prothrombin and protein C in early childhood: normal adult levels are not achieved until the fourth year of life. J Pediatr (1986) 109(5):843–5. doi:10.1016/S0022-3476(86)80708-9
10. Henriksson P, Varendh G, Lundstrom N. Haemostatic defects in cyanotic congenital heart disease. Br Heart J (1979) 41:23–7. doi:10.1136/hrt.41.1.23
11. Odegard K, Zurakowski D, Hornykewycz S, DiNardo J, Castro R, Neufeld E, et al. Evaluation of the coagulation system in children with two-ventricle congenital heart disease. Ann Thorac Surg (2007) 83:1797–804. doi:10.1016/j.athoracsur.2006.12.030
12. Odegard K, Zurakowski D, DiNardo J, Castro R, McGowan F, Neufeld E, et al. Prospective longitudinal study of coagulation profiles in children with hypoplastic left heart syndrome from stage I through Fontan completion. J Thorac Cardiovasc Surg (2009) 137:934–41. doi:10.1016/j.jtcvs.2008.09.031
13. Tempe D, Virmani S. Coagulation abnormalities in patients with cyanotic congenital heart disease. J Cardiothorac Vasc Anesth (2002) 16(6):752–65. doi:10.1053/jcan.2002.128436
14. Lill M, Perloff J, Child J. Pathogenesis of thrombocytopenia in cyanotic congenital heart disease. Am J Cardiol (2006) 98:254–8. doi:10.1016/j.amjcard.2006.01.083
15. Maurer H, McCue C, Caul J, Still W. Impairment in platelet aggregation in congenital heart disease. Blood (1972) 40(2):207–16.
16. Bailly D, Boskkov L, Zubair M, Rogers V, Lantz G, Armsby L, et al. Congenital cardiac lesions involving systolic flow abnormalities are associated with platelet dysfunction in children. Ann Thorac Surg (2014) 98:1419–24. doi:10.1016/j.athoracsur.2014.05.035
17. Loeffelbein F, Funk D, Nakamura L, Zieger B, Grohmann J, Siepe M, et al. Shear-stress induced acquired von Willebrand syndrome in children with congenital heart disease. Interact Cardiovasc Thorac Surg (2014) 19:926–32. doi:10.1093/icvts/ivu305
18. Eaton M, Iannoli E. Coagulation considerations for infants and children undergoing cardiopulmonary bypass. Pediatr Anaesth (2011) 21:31–42. doi:10.1111/j.1460-9592.2010.03467.x
19. Romlin B, Soderlund F, Wahlander H, Nilsson B, Baghaei F, Jeppsson A. Platelet count and function in paediatric cardiac surgery: a prospective observational study. Br J Anaesth (2014) 113(5):847–54. doi:10.1093/bja/aeu194
20. Ignjatovic C, Than J, Summerhayes R, Newall F, Horton S, Cochrane A, et al. The quantitative and qualitative responses in platelets in pediatric patients undergoing cardiopulmonary bypass surgery. Pediatr Cardiol (2012) 33:55–9. doi:10.1007/s00246-011-0079-5
21. Guay J, Ruest P, Lortie L. Cardiopulmonary bypass induces significant platelet activation in children undergoing open-heart surgery. Eur J Anaesthesiol (2004) 21:953–6. doi:10.1097/00003643-200412000-00005
22. Jaggers J, Lawson J. Coagulopathy and inflammation in neonatal heart surgery: mechanisms and strategies. Ann Thorac Surg (2006) 81:S2360–6. doi:10.1016/j.athoracsur.2006.02.072
23. Giglia T, DiNardo J, Ganayem N, Ichor R, Niebler R, Odegard K, et al. Bleeding and thrombotic emergencies in pediatric cardiac intensive care: unchecked balances. World J Pediatr Congenit Heart Surg (2012) 3(4):470–91. doi:10.1177/2150135112460866
24. Blalock A. Physiopathology and surgical treatment of congenital cardiovascular defects. Harvey Lect (1945-1946) 41:90–116.
25. Monagle P. Thrombosis in children with BT shunts, glenns, and fontans. Prog Pediatr Cardiol (2005) 21:17–21. doi:10.1016/j.ppedcard.2005.09.003
26. Wells W, Yu J, Batra A, Monforte H, Sintek C, Starnes V. Obstruction in modified Blalock shunts: a quantitative analysis with clinical correlation. Ann Thorac Surg (2005) 79:2072–6. doi:10.1016/j.athoracsur.2004.12.050
27. Glenn W. Circulatory bypass of the right side of the heart. N Engl J Med (1958) 259(3):117–20. doi:10.1056/NEJM195807172590304
28. Manlhiot C, Brandão LR, Schwartz SM, Sivarajan VB, Williams S, Collins TH, et al. Management and outcomes of patients with occlusive thrombosis after pediatric cardiac surgery. J Pediatr (2016) 169:146–53. doi:10.1016/j.jpeds.2015.10.046
29. Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax (1972) 26(3):240–8. doi:10.1136/thx.26.3.240
30. Firdouse M, Agarwal A, Chan A, Mondal T. Thrombosis and thromboembolic complications in Fontan patients: a literature review. Clin Appl Thromb Hemost (2014) 20(5):484–92. doi:10.1177/1076029613520464
31. Coon P, Rychik J, Novello R, Ro P, Gaynor J, Spray T. Thrombus formation after the Fontan operation. Ann Thorac Surg (2001) 71:1990–4. doi:10.1016/S0003-4975(01)02472-9
32. Backer C, Eltayeb P, Monge M, Mazwi M, Costello J. Shunt lesions part I: patent ductus arteriosus, atrial septal defect, ventricular septal defect, and atrioventricular septal defect. Pediatr Crit Care Med (2016) 17:S302–9. doi:10.1097/PCC.0000000000000786
33. Kerts G, Moysich A, Ho S, Apitz C, Latus H, Schranz D. Transcatheter closure of perimembranous ventricular septal defects with left ventricular to right atrial shunt. Pediatr Cardiol (2015) 36:1386–92. doi:10.1007/s00246-015-1170-0
34. Yang J, Yang L, Yu S, Liu J, Zou J, Chen W, et al. Transcatheter versus surgical closure of perimembranous ventricular septal defects in children: a randomized control trial. Am J Cardiol (2014) 63:1159–68. doi:10.1016/j.jacc.2014.01.008
35. Glatz A, Keashen R, Chang J, Balsama L, Dori Y, Gillespie M, et al. Outcomes using a clinical practice pathway for the management of pulse loss following pediatric cardiac catherization. Catheter Cardiovasc Interv (2015) 85(1):111–7. doi:10.1002/ccd.25686
36. Laurin S, Lundstrom N. Venous thrombosis after cardiac catheterization in infant. Acta Radiol (1987) 28:241–6. doi:10.3109/02841858709177342
37. Ruud E, Natvig S, Holmstrom H, Wesenber F. Low prevalence of femoral venous thrombus after cardiac catheterization in children: a prospective study. Cardiol Young (2002) 12:513–8. doi:10.1017/S1047951102000938
38. Hanslik A, Kitzmuller E, Thom K, Haumer M, Mlekusch W, Salzer-Muhar U, et al. Incidence of thrombotic and bleeding complications during cardiac catheterization in children: comparison of high-dose vs. low-dose heparin protocols. J Thomb Haemost (2011) 9:2353–60. doi:10.1111/j.1538-7836.2011.04539.x
39. Manhliot C, Brandao L, Kwok J, Kegel S, Menjak I, Carew C, et al. Thrombotic complications and thromboprophylaxis across all three stages of single ventricle heart palliation. J Pediatr (2012) 161:513–9. doi:10.1016/j.jpeds.2012.03.004
40. Li J, Yow E, Berezny K, Rhodes J, Bokesch P, Charpie J, et al. Clinical outcomes of palliative surgery including a systemic-pulmonary artery shunt in infants with cyanotic congenital heart disease: does aspirin make a difference? Circulation (2007) 116:293–7. doi:10.1161/CIRCULATIONAHA.106.652172
41. Massicotte M, Chair P. Evidence based recommendation for anticoagulation in children with congenital heart disease (primary prophylaxis: cardiac catheterization, mechanical heart valves, cardiac shunts, central lines and secondary prophylaxis: systemic thrombosis and stroke). Prog Pediatr Cardiol (2005) 21:123–7. doi:10.1016/j.ppedcard.2005.09.001
42. Monagle P, Chan A, Goldenberg N, Ichord R, Journeycake J, Nowak-Gottl U, et al. Antithrombic therapy in neonates and children. Chest (2012) 141(2 Suppl):e737S–e801S. doi:10.1378/chest.11-2308
43. Giglia T, Massicotte M, Tweddell J, Barst R, Bauman M, Erickson C, et al. Prevention and treatment of thrombosis in pediatric and congenital heart disease. Circulation (2013) 128:2622–703. doi:10.1161/01.cir.0000436140.77832.7a
44. Monagle P, Cochrane A, Roberts R, Manlhiot C, Weintraub R, Szechtman B, et al. A multicenter, randomized trial comparing heparin/warfarin and acetylsalicylic acid as primary thromboprophylaxis for 2 years after the Fontan procedure in children. J Am Coll Cardiol (2011) 58(6):645–51. doi:10.1016/j.jacc.2011.01.061
45. Gentilomo C, Huang Y, Raffini L. Significant increase in clopidogrel use across U.S. childrens hospitals. Pediatr Cardiol (2011) 32:167–75. doi:10.1007/s00246-010-9836-0
46. Wessel D, Berger F, Li J, Dahnert I, Rakhit A, Fontecave S, et al. Clopidogrel in infants with systemic-to-pulmonary-artery shunts. N Engl J Med (2013) 368:2377–84. doi:10.1056/NEJMoa1114588
47. Bauman ME, Massicotte MP, Kuhle S, Siddon S, Bruce AA. EMPoWARed: Edmonton pediatric warfarin self-management study. Thromb Res (2015) 136(5):887–93. doi:10.1016/j.thromres.2015.08.026
48. Hanslik A, Kitzmüller E, Tran US, Thom K, Karapetian H, Prutsch N, et al. Monitoring unfractionated heparin in children: a parallel-cohort randomized controlled trial comparing 2 dose protocols. Blood (2015) 126(18):2091–7. doi:10.1182/blood-2015-06-651661
49. Moore R, McNicholas K, Naidech H, Flicker S, Gallagher J. Clinically silent venous thrombosis following internal and external jugular central venous cannulation in pediatric cardiac patients. Anesthesiology (1985) 62(5):640–3. doi:10.1097/00000542-198505000-00018
50. Hanson S, Punzalan R, Christensen M, Ghanayem R, Kuhn E, Havens PL. Incidence and risk factors for venous thromboembolism in critically ill children with cardiac disease. Pediatr Cardiol (2012) 33:103–8. doi:10.1007/s00246-011-0098-2
51. Faraoni D, Gardella K, Odegard K, Emani S, DiNardo J. Incidence and Predictors for Postoperative Thrombotic Complications in Children With Surgical and Nonsurgical Heart Disease. Ann Thorac Surg (2016) 102: 1360–7. doi:10.1016/j.athoracsur.2016.03.083
52. Jensen AS, Idorn L, Thomsen C, von der Recke P, Mortensen J, Sorensen K, et al. Prevalence of cerebral and pulmonary thrombosis in patients with cyanotic congenital heart disease. Heart (2015) 101:1540–6. doi:10.1136/heartjnl-2015-307657
53. Emani S, Trainor B, Zurakowski D, Baird C, Fynn-Thompson F, Pigula F, et al. Aspirin unresponsiveness predicts thrombosis in high-risk pediatric patients after cardiac surgery. J Thorac Cardiovasc Surg (2014) 148:810–6. doi:10.1016/j.jtcvs.2014.06.016
54. Idorn L, Jensen AS, Juul K, Reimers JI, Johansson P, Sorensen KE, et al. Thromboembolic complications in Fontan patients: population-based prevalence and exploration of the etiology. Pediatr Cardiol (2013) 34:262–72. doi:10.1007/s00246-012-0431-4
55. Tzanetos D, Yu C, Hernanz-Schulman M, Barr F, Brown N. Prospective study of the incidence and predictors of thrombus in children undergoing palliative surgery for single ventricle physiology. Intensive Care Med (2012) 38:105–12. doi:10.1007/s00134-011-2378-y
56. Kim SJ, Kim WH, Lim HG, Lee JY. Outcome of 200 patients after an extracardiac Fontan procedure. J Thorac Cardiovasc Surg (2008) 136:108–16. doi:10.1016/j.jtcvs.2007.12.032
57. Hanslik A, Thom K, Haumer M, Kitzmuller E, Albinni S, Wolfsberger M, et al. Incidence and diagnosis of thrombosis in children with short-term central venous lines of the upper venous system. Pediatrics (2008) 122:1284–91. doi:10.1542/peds.2007-3852
58. Cholette J, Rubenstein J, Alfieris G, McDermott M, Harmon W, Vermilion R, et al. Elevated risk of thrombosis in neonates undergoing initial palliative cardiac surgery. Ann Thorac Surg (2007) 84:1320–5. doi:10.1016/j.athoracsur.2007.05.026
59. Kaulitz R, Ziemer G, Rauch R, Girisch M, Bertram J, Wessel A, et al. Prophylaxis of thromboembolic complications after the Fontan operation (total cavopulmonary anastomosis). J Thorac Cardiovasc Surg (2005) 129:569–75. doi:10.1016/j.jtcvs.2004.08.045
60. Gurgey A, Ozyurek E, Gumruk F, Celiker A, Ozkutlu S, Ozer S, et al. Thrombosis in children with cardiac pathology: frequency of factor V Leiden and prothrombin G20210A mutations. Pediatr Cardiol (2003) 24:244–8. doi:10.1007/s00246-002-0170-z
61. Seipelt RG, Franke A, Vazquez-Jimenez JF, Hanrath P, von Bernuth G, Messmer BJ, et al. Thromboembolic complications after Fontan procedures: comparison of different therapeutic approaches. Ann Thorac Surg (2002) 74:556–62. doi:10.1016/S0003-4975(02)03677-9
62. Jacobs MI, Pourmoghadam KK, Geary EM, Reyes At, Madan N, McGrath LB, et al. Fontan’s operation: is aspirin enough? Is Coumadin too much? Ann Thorac Surg (2002) 73:64–8. doi:10.1016/S0003-4975(01)03068-5
63. Petaja J, Peltola K, Sairanen H, Leijala M, Kekomaki R, Vahtera E, et al. Fibrinolysis, antithrombin III, and protein C in neonates during cardiac operations. J Thorac Cardiovasc Surg (1996) 112:665–71. doi:10.1016/S0022-5223(96)70050-8
64. Petaja J, Lundstrom U, Sairanen H, Marttinen E, Griffin J. Central venous thrombosis after cardiac operations in children. J Thorac Cardiovasc Surg (1996) 12:883–9. doi:10.1016/S0022-5223(96)70087-9
65. Rosenthal DN, Friedman AH, Kleinman CS, Kopf GS, Rosenfeld LE, Hellenbrand WE. Thromboembolic complications after Fontan operations. Circulation (1995) 92(9 Suppl):287–93. doi:10.1161/01.CIR.92.9.287
66. Mir A, Frank S, Journeycake J, Joshua Wolovits J, Guleserian K, Heistein L, et al. Aspirin resistance in single-ventricle physiology: aspirin prophylaxis is not adequate to inhibit platelets in the immediate postoperative period. Ann Thorac Surg (2015) 99:2158–65. doi:10.1016/j.athoracsur.2015.02.026
67. Domi T, Edgell D, McCrindle B, Williams W, Chan A, MacGregor D, et al. Frequency, predictors, and neurological outcomes of vaso-occlusive strokes associated with cardiac surgery in children. Pediatrics (2008) 122:1292–8. doi:10.1542/peds.2007-1459
68. Brandao LR, Manlhiot C, Williams S, McCrindle BC. Characterization of post-thrombotic syndrome in children with congenital heart disease: a comparison of instruments. Poster Presentation, International Society of Hemostasis and Thrombosis. Kyoto, Japan (2011).
Keywords: congenital heart disease, venous thromboembolism, venous thromboembolism prophylaxis, venous thromboembolism treatment, congenital heart disease and thrombosis, venous thromboembolism risk factors
Citation: Silvey M and Brandão LR (2017) Risk Factors, Prophylaxis, and Treatment of Venous Thromboembolism in Congenital Heart Disease Patients. Front. Pediatr. 5:146. doi: 10.3389/fped.2017.00146
Received: 28 October 2016; Accepted: 09 June 2017;
Published: 19 June 2017
Edited by:
John Joseph Strouse, Duke University, United StatesReviewed by:
Benjamin Barnes, Johns Hopkins University, United StatesLasya Gaur, Johns Hopkins Medicine, United States
Copyright: © 2017 Silvey and Brandão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Silvey, bXNpbHZleUBjbWguZWR1