
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pain Res. , 15 March 2024
Sec. Pharmacological Treatment of Pain
Volume 5 - 2024 | https://doi.org/10.3389/fpain.2024.1306479
This article is part of the Research Topic Behavioural Approaches to Management of Pain in Later Life View all 4 articles
 Meriem Zerriouh1
Meriem Zerriouh1 Gwenaelle De Clifford-Faugère1
Gwenaelle De Clifford-Faugère1 Hermine Lore Nguena Nguefack1
Hermine Lore Nguena Nguefack1 M. Gabrielle Pagé2,3Line Guénette4,5Lucie Blais6
M. Gabrielle Pagé2,3Line Guénette4,5Lucie Blais6 Anaïs Lacasse1*
Anaïs Lacasse1*
Objectives: Randomized clinical trials are used to evaluate the efficacy of various pain treatments individually, while a limited number of observational studies have portrayed the overall relief experienced by persons living with chronic pain. This study aimed to describe pain relief in real-world clinical settings and to identify associated factors.
Methods: This exploratory web-based cross-sectional study used data from 1,419 persons recruited in the community. Overall pain relief brought by treatments used by participants was assessed using a 0%–100% scale (10-unit increments).
Results: A total of 18.2% of participants reported minimal pain relief (0%–20%), 60.0% moderate to substantial pain relief (30%–60%), and 21.8% extensive pain relief (70%–100%). Multivariable multinomial regression analysis revealed factors significantly associated with greater pain relief, including reporting a stressful event as circumstances surrounding the onset of pain, living with pain for ≥10 years, milder pain intensity, less catastrophic thinking, use of prescribed pain medications, use of nonpharmacological pain treatments, access to a trusted healthcare professional, higher general health scores, and polypharmacy. Factors associated with lower pain relief included surgery as circumstances surrounding pain onset, use of over-the-counter pain medications, and severe psychological distress.
Discussion: In this community sample of persons living with chronic pain, 8 out of 10 persons reported experiencing at least moderate relief with their treatment. The analysis has enabled us to explore potential modifiable factors as opportunities for improving the well-being of persons living with chronic pain.
Chronic pain (CP), defined as pain persisting or recurring for more than three months (1), is a serious condition which affects 19% of adults in Canada (2, 3) and has been shown to be a major economic burden (4). It is one of the most common reasons of healthcare utilization (5), a major cause of disability (6), and results in high societal costs (7–9). In Canada, the direct healthcare costs and lost productivity costs of CP are estimated at $40.4 billion per year (10). CP is a complex disease resulting from the interaction of multiple biological (e.g., tissue health, physiology and neurochemistry), psychological (e.g., catastrophic thinking, depression, anxiety), and social (e.g., scepticism, socioeconomic status) factors (11). A multimodal approach is thus recommended to better alleviate CP. Such an approach provides a balance of pharmacologic, physical, and psychological treatments, while building on patient self-management skills (12, 13). Pharmacological treatment may include prescribed and over-the-counter medications such as nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, antidepressants, anticonvulsants, and acetaminophen (14, 15). Physical treatments can be based on a set of stretches and light aerobic exercises performed on a daily basis (e.g., physiotherapy, yoga) or massage therapy (16) and psychological treatments may include cognitive–behavioural therapy, acceptance and commitment therapy, relaxation strategies, and hypnosis (16). Herbal medicine is also used by some patients for pain relief (e.g., St John's Wort, ginger, turmeric) (17).
In real-world clinical settings, the implementation of the multimodal approach is fraught with several challenges, such as difficult access to multidisciplinary pain clinics (18), lack of access to support groups, and poor access to certain nonpharmacological pain treatments for those without insurance and with a limited budget (19). Also, for people living with CP, playing an active role in managing one's disease daily and applying different self-management methods prove challenging. Medications are in fact, used by a majority of persons living with CP (62%–84%) (20–22). Unfortunately, their expectations regarding medication efficacy are often unrealistically high (e.g., expecting complete pain relief), and these expectations are seldom discussed with healthcare professionals to jointly establish realistic and achievable therapeutic goals (23). Moreover, a substantial proportion perceive their treatment as inadequate (37%–64%) (24, 25). The heterogeneity of people living with CP who present with different comorbidities and symptoms of pain may complexify the multimodal approaches proposed by healthcare professionals (26).
Understanding the efficacy of the multimodal approach in real-world clinical settings and unveiling modifiable factors associated with greater pain relief could help provide manageable solutions to alleviate CP and to improve its management, especially for persons without access to facilities offering multidisciplinary care. However, the evidence regarding the efficacy of pain treatments comes mainly from the results of experimental or quasi-experimental clinical trials (14, 15, 24, 25, 27). To our knowledge, a few observational studies representing the real-world have examined self-reported pain relief experienced by people living with CP in the community with their diverse array of treatments (24, 25). Those studies measured the relief provided by treatments independently of pain intensity, but have used simple dichotomous measurements—e.g., perceived treatment adequacy (adequate/inadequate) (25) or pain control from medication (adequate/inadequate) (24)—to evaluate pain relief. A more discriminative portrait is thus warranted. In addition, data is scarce about factors associated with pain relief using multivariable analysis in order to account for and understand the simultaneous effects of multiple variables. Furthermore, these studies were conducted in Asian or European countries (24, 25), potentially not reflecting the reality of pain treatment in Canada. The present study thus aimed to provide a detailed depiction of the pain relief experienced by persons living with CP in real-world clinical settings. Sociodemographic and clinical factors associated with moderate to substantial (30%–60%) or extensive pain relief (70%–100%), as opposed to minimal pain relief (0%–20%), were also explored.
This cross-sectional observational study was conducted using the ChrOnic Pain trEatment (COPE) Cohort (28) data. It consists of a database containing information about 1,935 persons living with CP, collected through a web-based cross-sectional survey conducted between June and October 2019. The COPE Cohort was established to better understand the real-life use of pharmacological and nonpharmacological treatments among people living with CP in the province of Quebec (Canada) (28). Participant selection criteria were as follows: (1) reporting living with persistent or recurrent pain for more than three months [as per ICD-11 definition (1)]; (2) aged 18 years or older; (3) residing in Quebec; and (4) ability to complete an online questionnaire in French. The Cohort methods are described in detail elsewhere (28). The COPE Cohort profile was found to be comparable to random samples of Canadians living with CP in terms of age, employment, education and pain characteristics. However, women are overrepresented [84% vs. 55%–65% in Canadian CP samples (28)], justifying gender-stratified or gender-standardized statistics and multivariable analyses. The study protocol was approved by the Research Ethics Committee of the University of Quebec in Abitibi-Témiscamingue (#2018-05-Lacasse, A.) and all participants gave their informed electronic consent. No monetary or material incentive was given for participation. The present study used self-reported data from participants who answered the questionnaire section about pain relief (n = 1,419).
The web-based questionnaire consisted of items used in prior studies and validated composite scales (variables and the integral questionnaire are presented in Supplementary Appendix S1). The questionnaire items were derived from recommended outcome domains and core measures: the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) (29, 30), the Canadian minimum dataset for chronic low back pain research (31), as well as measures included in the Quebec Pain Registry (32). In addition to the variables prioritized by the research team (the balance between validity and parsimony was thoroughly assessed), all indicators identified as a minimum dataset by the Canadian Registry Working Group of the Strategy for Patient-Oriented Research Chronic Pain Network (SPOR CPN) (33) were included in the questionnaire: pain location, circumstances surrounding onset, duration, frequency, intensity, neuropathic component, interference, physical function, anxiety and depressive symptoms, age, gender, and occupational status.
Participants were invited to rate their pain relief using a 0 to 100 scale, expressed as percentages with 10-unit increments, where 0 represented no relief, and 100 represented complete relief. For this purpose, the following question was asked immediately after thoroughly inquiring about participants' pharmacological and nonpharmacological pain treatments: “Overall, how much relief do you get from the treatments or medications currently used in your treatment?”. The format of the response choices was inspired by the pain relief question from the Brief Pain Inventory (BPI) (34), which typically measures the relief provided by treatments over the last 24 h. We then chose to analyze this measure in the form of clinically meaningful categories rather than on a continuous scale to enhance the interpretability of the results. According to the literature, pain relief can be considered moderate and clinically meaningful when ≥30%, substantial when ≥50% and extensive when ≥70% (35, 36). According to the distribution of our data, three groups were thus created to classify the dependent variable: (1) minimal pain relief (0%–20%), (2) moderate to substantial pain relief (30%–60%) and (3) extensive pain relief (70%–100%).
The inclusion of a wide range of variables within the COPE Cohort facilitated a comprehensive selection of potential sociodemographic and clinical factors. The identification of relevant variables was guided by two models for reference. The first was the Andersen model (37), which is widely used in healthcare studies (38, 39). It focuses on factors influencing healthcare utilization, such as predisposing factors (e.g., gender, age, education level, lifestyle), facilitating/inhibiting factors (e.g., region of residence, having a family physician), and need factors (e.g., self-reported symptoms, perceived general health). The second was the biopsychosocial model of CP (40) according to which biological, psychological, and social factors interact with the nervous system and impact the onset and experience of pain. Consequently, the present study incorporated a diverse set of sociodemographic, psychosocial, and clinical variables. Sociodemographic characteristics, included age, gender identity, stereotypically feminine and masculine personality traits according to the Bem Sex-Role Inventory (BSRI) (41, 42), professional status, education level, country of birth, living in a remote area, and receiving disability benefits. CP characteristics included circumstances surrounding its onset (semi-closed question e.g., accident, disease, stressful event), multisite pain (≥2 pain sites assessed using a semi-closed question listing 21 bodily locations), pain frequency (continuous/recurrent), pain duration, pain intensity in the past seven days and at its worst (0–10 numerical rating scale), neuropathic pain screening using the DN4 (Douleur Neuropathique en 4 Questions) (43), pain interference according to the Brief Pain Inventory (44), and agreeing with the statement “I feel that my pain is terrible and it's never going to get any better” (this single item from the Pain Catastrophizing Scale (45) is referred to as “catastrophizing” in the National Institute of Health [NIH] minimal dataset for chronic low back pain (46) and in the STarT Back Screening Tool (47)). Pain management assessment included dichotomized measures (yes/no) of the use of prescription or over-the-counter medications, nonpharmacological treatments, and access to a trusted health professional for pain management. Were also measured psychological distress (Patient Health Questionnaire-4 [PHQ-4] (48)), perceived general health (12-Item Short Form Survey version 2 [SF-12v2] subscale (49)), physical functioning [SF-12v2 subscale (49)], the number of medications currently used (all health conditions considered; polypharmacy was defined as the use of ≥5 medications), feeling the need to reduce alcohol or drug consumption, cigarette smoking, and cannabis use for pain management.
The characteristics of participants were depicted using descriptive statistics (numbers and proportions for categorical variables; means, standard deviations, medians and interquartile ranges for continuous variables). To complete the first objective (depiction of the pain relief), the percentage of participants reporting each 10-unit increment on the 0%–100% pain relief scale were reported for the entire sample and according to pain intensity and gender identity as per good practices in terms of sex- and gender-based analysis. Stratification was also achieved according to nonpharmacological treatments used by participants. To achieve the study's second objective (identify sociodemographic and clinical factors associated with greater pain relief), a multivariable multinomial regression model was used (50). In the model, minimal pain relief (0%–20%) was used as the reference group, to which the moderate to substantial pain relief group (30%–60%) and the extensive pain relief group (70%–100%) were compared. All the sociodemographic and clinical factors were included in the model. The a priori selection of those variables was based on the latest recommendations (51). Due to our substantial sample size, this method was favoured over criticized selection techniques such as relying on bivariate regression analysis p-values (51) or stepwise selection (50). Variance inflation factors (VIFs) below 5 were used to detect potential multicollinearity issues (52). The adjusted odd ratios (aOR) estimating the associations between independent variables and the likelihood of getting moderate-substantial or extensive pain relief (vs. minimal pain relief), along with their 95% confidence intervals (95% CIs) and p-values were computed. A sensitivity analysis was carried out to assess the impact of a multiple imputation technique for missing data (50) on our conclusions. Multiple imputation by fully conditional specification (FCS) method was applied with 5 repetitions. The Hosmer-Lemeshow test (53) confirmed goodness of fit of the models (Chi-square:12.2–18.7; p = 0.3–0.7). All analyses were achieved using SPSS Statistics for Windows version 27 (IBM Corp., Armonk, NY, USA) and SAS version 9.4 (SAS Institute, Cary, NC, USA).
Among the 1,935 participants of the COPE Cohort, 1,419 persons (73.3%) answered the question about the percentage of pain relief brought by the treatments or medications currently used. No clinically important differences were observed between those included and excluded (n = 516) in terms of the proportion of individuals born in Canada (95.9% vs. 92.9%), having a post-secondary education (79.2% vs. 76.9%), or residing in remote regions (23.9% vs. 18.8%). However, a higher proportion of women (84.0% vs. 63.2%) were included, justifying the use of gender-stratified or gender-standardized statistics and multivariable analyses. The mean age was slightly lower among included participants (50 vs. 57 years old).
Participant characteristics are reported in Table 1. Regarding pain characteristics, average pain intensity in the past 7 days (0–10 numerical rating scale) was 5.4 ± 1.9, and more than half of the participants (51.8%) reported living with pain for ≥10 years. Prescribed pain medications were used by 79.9% of participants, over-the-counter pain medication by 67.0% and nonpharmacological approaches (physical or psychological treatments) by 85.9%. The perceived general health SF-12v2 score in our sample was 36.4 ± 12.7 [scores <47 indicate impaired wellbeing when compared to general population norms (49)].
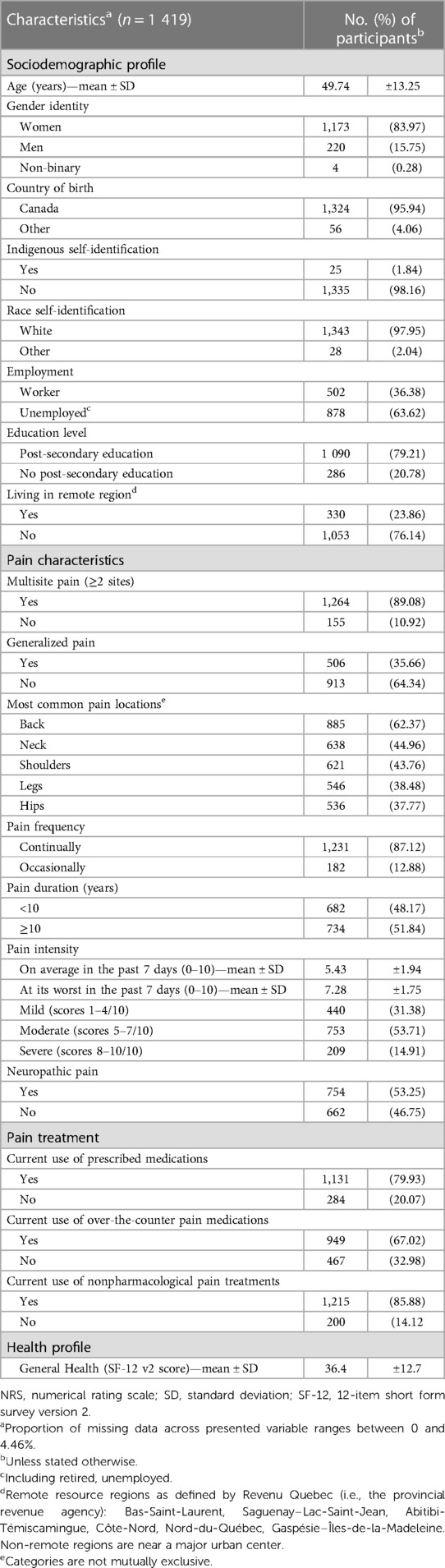
Table 1. Sample characteristics.
The percentages of participants reaching each 10-unit increment on the 0%–100% pain relief scale are presented in Figure 1. Minimal pain relief (10%–20%) was reported by 18.2% of participants, moderate to substantial pain relief (30%–60%) by 60.0% of participants, and extensive pain relief (70%–100%) by 21.8% of participants. In other words, 81.8% reached the 30% clinically meaningful pain relief cut-off suggested in the literature (35). The proportions of participants reaching such a pain relief cut-off among persons reporting mild, moderate and severe pain intensity were respectively 89.5%, 81.3%, and 68.4%. Figure 2 shows the percentage of participants reaching a particular percentage of pain relief in participants who self-identified as women and men respectively, the portrait being very similar. In the non-binary group (n = 4), three persons experienced moderate to substantial (30%–60%) pain relief, and one reported extensive (70%–100%) pain relief. Percentages of participants reaching various cut-offs of pain relief among users of various nonpharmacological treatments (physical and psychological) are presented in Figure 3.
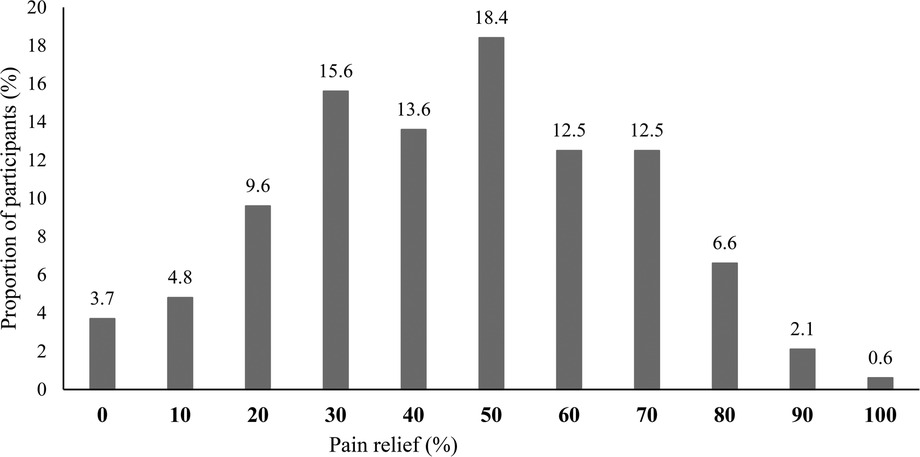
Figure 1. Percentages of participants reaching each 10-unit increment on the 0%–100% pain relief scale (n = 1,419). Mutually exclusive categories (total equals 100%).
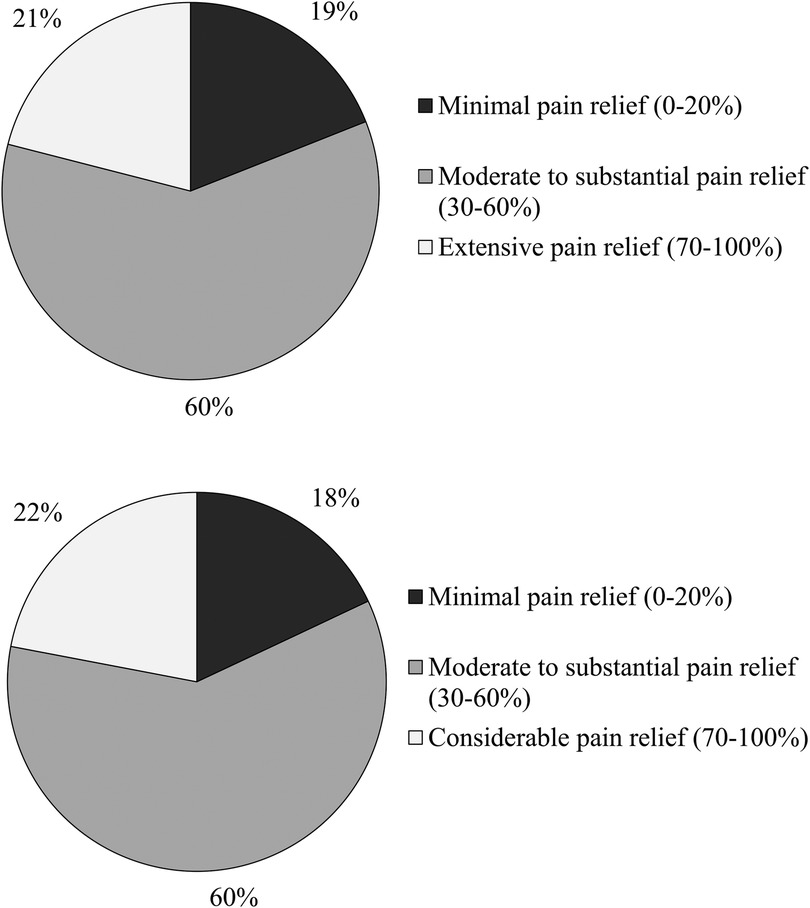
Figure 2. Percentages of participants reaching various cut-offs of pain relief (n = 1,419). The upper panel shows results among the woman subsample and lower panel among the men subsample.
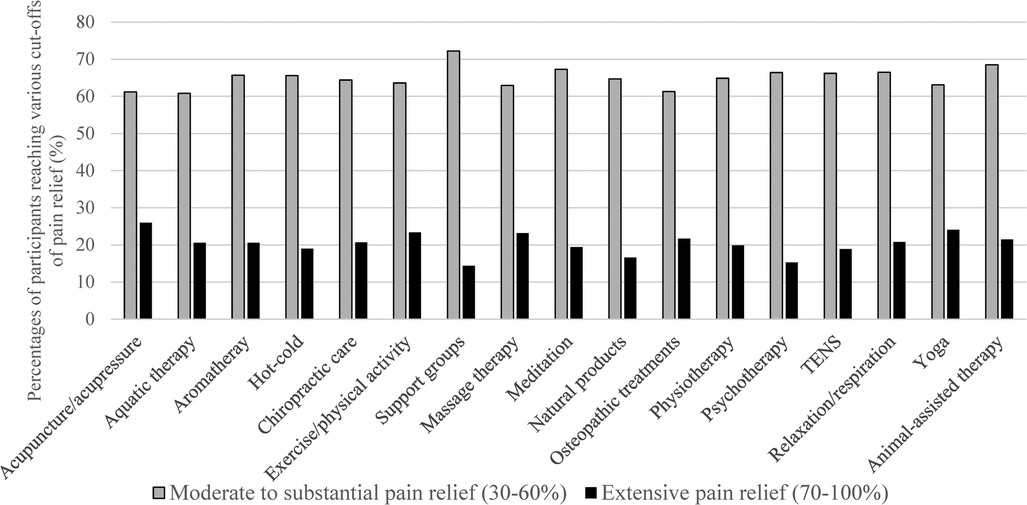
Figure 3. Percentages of participants reaching various cut-offs of pain relief (n = 1,419) among users of various physical and psychological treatments. Non-mutually exclusive categories of treatment users. TENS = Transcutaneous electrical nerve stimulation; For statistically sound numbers, achievement of pain relief cut-offs are presented for treatments used by at least 100 participants. For statistically sound numbers, achievement of pain relief cut-offs is presented for treatments used by at least 100 participants. Less than 100 participants used biofeedback, ergotherapy, hypnosis, neurostimulator implantation, group intervention, music therapy, homeopathic product, virtual/augmented reality, reflexology, reiki, tai chi or taping/elastic-bands.
Table 2 shows the estimates of the multivariable multimodal regression model used to investigate the relationship between the different factors and moderate to substantial (30%–60%) or extensive pain relief (70%–100%). Factors associated with an increased likelihood of being in the moderate to substantial pain relief group (30%–60%), as compared to the minimal pain relief group (0%–20%), were: (1) the use of prescribed pain medications (aOR = 2.2, 95% CI: 1.4–3.5), (2) the use of nonpharmacological pain treatments (aOR = 2.2, 95% CI: 1.3–3.5), (3) self-reported access to a trusted healthcare professional for pain management (aOR = 1.5, 95% CI: 1.0–2.2), and (4) use of five or more drugs (polypharmacy) (aOR = 1.8, 95% CI: 1.2–2.8). In contrast, factors associated with a decreased likelihood of reporting moderate to substantial pain relief were: (1) greater pain intensity (moderate vs. mild pain intensity; aOR = 0.3, 95% CI: 0.2–0.6), and (2) feeling that pain is terrible and will never improve (aOR = 0.6, 95% CI: 0.4–0.9).

Table 2. Factors associated (p < .05) with greater pain relief in the multivariable multinomial regression model.
Factors associated with an increased likelihood of being in the extensive pain relief group (70%–100%), as compared to the minimal pain relief group (0%–20%), were: (1) reporting a stressful event as circumstances surrounding pain onset (vs. no such circumstances; aOR = 2.1, 95% CI: 1.2–3.9), (2) living with CP for ≥10 years (aOR = 1.7, 95% CI: 1.0–3.0), (3) using prescribed pain medications (aOR = 2.3, 95% CI: 1.3–4.1), (4) reporting having access to a trusted healthcare professional for pain management (aOR = 2.6, 95% CI: 1.5–4.5), and (5) having high general health scores (OR = 1.0, 95% CI: 1.0–1.1, i.e., a clinically meaningful 10-point increase in this continuous variable leads to a 10.3 fold increase in the odds). On the other hand, they had fewer chances of: (1) reporting surgery as circumstances surrounding pain onset (vs. no such circumstances; aOR = 0.5, 95% CI: 0.2–1.0), (2) reporting moderate (OR = 0.2, 95% CI: 0.1–0.4) or severe (aOR = 0.4, 95% CI: 0.2–0.7) pain intensity, (3) feeling that pain is terrible and will never going to get any better (aOR = 0.4, 95% CI: 0.2–0.7), (4) using over-the-counter pain medications (aOR = 0.6, 95% CI: 0.4–0.9), and (5) reporting severe psychological distress (vs. mild psychological distress; aOR = 0.3, 95% CI: 0.1–0.7). Multiple imputations of missing values did not change these conclusions.
This study aimed to describe the pain relief brought by treatments used in real-world clinical settings and, in an exploratory fashion, to identify clinical, psychosocial, and sociodemographic factors associated with greater pain relief. Among our participants, 81.8% reported experiencing at least moderate pain relief. Various factors were found to be significantly associated with greater pain relief, including reporting a stressful event as a circumstance surrounding the onset of pain, living with pain for ≥10 years, milder pain intensity, less catastrophic thinking, use of prescribed pain medications, use of nonpharmacological pain treatments, access to a trusted healthcare professional, higher general health scores and polypharmacy. Factors associated with lower pain relief included surgery as circumstances surrounding pain onset, use of over-the-counter pain medications, and severe psychological distress.
Some cross-sectional observational studies have measured pain relief experienced by persons living with CP (24, 25). However, such studies have used poorly discriminating dichotomous measures despite the recommendation by IMMPACT to measure pain relief percentages, independently from pain intensity, along with the improvement of physical and emotional functioning (29, 30, 35). In the present study, only 18.2% of participants reported minimal pain relief (0%–20%), as opposed to two large studies conducted in over 25 countries and regions across Europe and Asia who showed that 37%–64% of the participants reported treatment inadequacy/inadequate pain control from medications (yes/no) (24, 25). A significant proportion of our participants reported at least moderate relief (≥30%), specifically 81.8%. This finding is surprising given the above-mentioned studies and literature highlighting poor physical and psychological health among persons living with CP (24, 25). This could be attributed to our web-based community sample, as opposed to several CP studies conducted within pain clinic settings with more severe populations. Indeed, in comparison to a population of individuals living with CP followed in tertiary care in the province of Quebec (32), our study population had a lower average pain intensity in the past seven days (5.4 ± 2 vs. 6.7 ± 2), a lower proportion of individuals with evidence of neuropathic pain (53% vs. 76%), and a lower proportion of individuals reporting pain interference with general activity (BPI item ≥7/10: 51.4% vs. 59.17%). Our sample also had a higher proportion of individuals living with pain for ≥10 years (51.8% vs. 26.2%), and possibly more time to find better ways to manage their pain. It is a positive observation to have as many participants reporting at least moderate relief. Such a result suggests the importance of future research targeting samples that are more representative of the general population of persons living with CP, including individuals experiencing better pain relief. Those persons can certainly provide valuable insights into their pain management strategies.
As previously mentioned, few observational studies identified factors associated with greater pain relief using multivariable analysis, which restricts our ability to compare our results with those of other studies. In the present study, participants who lived with chronic post-surgical pain were less likely to experience pain relief (independently from evidence of neuropathic pain). It is important to highlight that chronic post-surgical pain represents a significant and often overlooked clinical problem (54) affecting a important proportion of patients who undergo surgery (10% to 60%) (55, 56). This condition has been associated with impaired physical function and reduced quality of life (57, 58), as well as poor mental health, general health status, sleep outcomes (59), and functional impairment (58). A literature review (n = 16) led to the conclusion that there is a limited body of research specifically addressing the management of chronic post-surgical pain (60). Limited by our inability to compare our results with those of other similar studies, we could hypothesize that chronic post-surgical pain is more challenging to control than other types of chronic pain or that pain relief is lower because of underlying medical conditions not resolved by the surgery. Psychological factors (e.g., surgical-induced trauma) could also be a research avenue.
Our results highlight that participants who achieved greater pain relief had an increased likelihood of reporting stressful events as circumstances surrounding the onset of pain (e.g., a trauma, a car accident, or financial difficulties perceived by the participant as stressful). It is possible that these individuals were healthy before the accident or trauma, so they may have had fewer underlying health issues than others, which could explain why they recover better. However, this result still requires further exploration in future studies.
The duration of CP experienced by patients varies and is directly proportional to the extent of the suffering and poorer outcomes of treatment (61, 62). Pagé et al. (63) reported that longer pain duration was significantly associated with a higher likelihood of reporting worsened pain. However, our results demonstrated that, independently from pain intensity, living with pain for more than ten years was associated with higher chances of achieving extensive pain relief. This result is non-intuitive as in clinical treatment settings, patients living with pain for a long time are often treatment resistant (64, 65). Unfortunately, our data do not allow for a deeper exploration of the mechanics of this association, but our hypothesis to explain this result revolves around psychosocial factors influencing the experience of chronic pain (e.g., acceptance, self-efficacy). In fact, the literature points out that longer pain duration can be associated with better self-efficacy (66), an important predictor of less functional impairment, affective distress, and severe pain (67). Self-efficacy–impairment associations are even moderated by pain duration, with larger effect sizes observed in studies involving patients living with pain for a longer time (67). The association between pain duration and pain relief found in our analysis must, however, be thoroughly investigated in future studies before drawing premature conclusions.
Pain intensity is also a crucial component of CP assessment according to IMMPACT guidelines (29, 30, 35) and potential intersecting factor. Numerous studies have established the relationship between severe pain intensity and worse CP outcomes, such as anxiety symptoms (68), high healthcare utilization and pain catastrophizing (69), and poor quality of life (70). In the present study, it was not surprising that mild pain intensity was associated with reports of greater pain relief. This result aligns with previous research that has also demonstrated a significant overall correlation between pain intensity and pain relief measurements (71–73). It is noteworthy that these findings do not imply that pain intensity should be the primary focus to achieve greater pain relief. In fact, prioritizing the improvement of other co-occurring issues, such as sleep, mood, and function, may lead to higher levels of pain relief (74). Although treatment adequacy is sometimes defined based on pain intensity scores (27, 75), we suggest measuring these two elements separately because our study demonstrates that pain intensity is associated with, but does not fully explain, the extent of pain relief. Further studies should explore the intersections of various pain qualities in relation to pain relief.
In this study, participants experiencing catastrophic thinking (i.e., feeling that the pain is terrible and will never improve) were less likely to achieved moderate to substantial or extensive pain relief. While the standard measurement of catastrophizing is the 13-item Pain Catastrophizing Scale (45), it should be noted that we used a single-item question referred to as “catastrophizing” in the NIH Minimal Dataset for Chronic Low Back Pain (46) and STarT Back Screening Tool (47). Pain catastrophizing is an important factor to consider when dealing with the psychological components of pain (69). It is among the most important predictors of poor outcomes in CP samples (76). Although our study does not allow us to establish the direction of this association (whether catastrophizing hinders pain relief or not being relieved worsens catastrophic thinking), catastrophizing is a modifiable factor that could potentially be prioritized for better pain management.
The use of prescribed pain medications was found to be significantly associated with greater pain relief. While more than 60% of persons living with CP turn to medications for pain relief (20, 21), this treatment option is considered to provide limited efficacy (14, 15). In our study, we adjusted for the use of physical or psychological treatments. This finding may indicate that, regardless of other factors, prescribed medications have an important place in the toolkit of a multimodal approach to pain management for some individuals. It is important to note that our study was conducted among a cohort of prevalent prescribed pain medication users, who probably continue to use their medication because they appreciate the balance between benefits and risks (reducing their susceptibility to adverse effects). Therefore, participants in our study who use prescribed medications likely derive benefits from their use. Our study is, however, a first exploratory step. Further studies should conduct an analysis that includes and differentiates the specific types of pharmacological, interventional (e.g., injections), physical, and psychological treatments in the analysis.
On the other hand, the use of over-the-counter pain medications was found to be associated with a decreased likelihood of reporting extensive pain relief. A possible explanation is that patients who are not relieved are seeking solutions, which is why they use over-the-counter medications. These unmet needs could be a reflection of a lack of access to care or suboptimal care. In fact, persons living with CP often resort to self-medication using over-the-counter analgesics to alleviate their symptoms (77). While over-the-counter analgesics are generally deemed safe for most adults when used according to package instructions, the literature suggests that persons with lower levels of education, more severe pain, or recurrent or persistent pain are more prone to exceed the recommended daily dosage (78). Over-the-counter pain medications, without personalized follow-up by a healthcare professional may potentially do more harm than good. Further studies could delve into the extent to which persons living with CP are well supported in their use of over-the-counter medications.
Unsurprisingly, the use of nonpharmacological pain treatments (physical or psychological) was found to be associated with an increased likelihood of reporting moderate to substantial pain relief. Many are publicly or privately accessible in the Canadian context, or can be used freely as self-management strategies (79). Such treatments are known to provide pain relief and are well tolerated (80–85).
In our study, it was observed that participants who reported having access to a trusted healthcare professional for pain management reported greater pain relief. Previous research has emphasized the significance of the relationship between healthcare professionals and their patients, recognizing it as a crucial factor in therapeutic outcomes (86, 87). This relationship encompasses various aspects, including trust, which can impact continuity of care, treatment adherence, and the willingness to seek healthcare (86). Additionally, agreement on diagnosis and treatment plans are known as variables associated with better patient satisfaction, mental health, social function and vitality (88).
In this study, greater self-perceived general health was associated with an increased likelihood of reporting extensive pain relief. Also, we found that higher levels of psychological distress were associated with a lower likelihood of achieving greater pain relief. These results are consistent with numerous studies suggesting that improving overall well-being may contribute to alleviating CP (89–92). Additionally, it is well established that psychological factors such as depression and anxiety are predictors of poorer pain-related health outcomes (93–96).
Polypharmacy (concomitant use of ≥5 medications) is a common clinical consequence of multimorbidity (97–99). For pain management, multimodal analgesia is common. It consists in the administration of multiple medications, each with a unique mechanism of action, which, when taken concurrently, can provide adequate pain relief (100). In the present study, participants with polypharmacy were more likely to achieve moderate to substantial pain relief than those without polypharmacy. Polypharmacy can lead to potential problems, such as an increased risk of drug-related adverse events, drug interactions (101, 102) and drug cascades. Still, it can be “rational” (103) and lead to positive clinical outcomes by approaching diseases through multiple mechanisms of action (104). For example, given the highly contentious nature of opioid prescribing and the frequent instances of forced withdrawal and insufficient pain relief experienced by patients (22, 105), rational polypharmacy presents an alternative approach (combining medications to address the multifaceted aspects of CP while minimizing their risks). That said, further studies should explore the specific medications used by participants in the COPE Cohort to support this hypothesis.
Although the literature is abundant with evidence demonstrating gender differences in pain “experience and treatment” (106), no association was found between gender identity or gender-stereotyped personality traits and the level of pain relief in our study (univariable or multivariable analyses).
While the web-based self-reported questionnaire provides no control over the real underlying condition compared to in-person assessments, the web survey approach enabled the recruitment of a large sample without geographical limitations (remote and non-remote regions). COPE Cohort participant characteristics have been shown to be similar to randomly selected samples of Canadians living with CP in terms of age, employment status, educational level, and pain characteristics (28). Furthermore, the study employed a multivariable approach to examine the relationships between numerous factors that had not been previously explored. However, at this level, our study should be considered exploratory due to its cross-sectional nature, which does not allow for establishing causal relationships. Also, despite the diversity and inclusiveness of the variables considered in the study survey, not all relevant factors were included in the questionnaire, particularly regarding information on social support, clinically meaningful relief, satisfaction with treatment or the types of medication used, dosage, and purpose (for pain or other conditions). Other aspects (e.g., economic considerations, pain meanings, beliefs, fear, avoidance) could also be relevant and even deepened using qualitative interviews. More advanced statistical approaches (e.g., interaction testing, mediation analysis, machine learning) could also be relevant to deepen our understanding of the underlying modulators of CP and pain relief. Finally, there was a higher representation of women in our sample [in random samples of Canadians with CP, women typically represent 55%–65% of the sample (28)]. This could be explained by the web-based recruitment method, as women are known to use social media more frequently and work in front of a computer more often (107). Additionally, women generally consume more medication than men (108). However, this was circumvented by the use of stratification and multivariable analysis.
Based on our results, it is possible, depending on various health factors, to achieve pain relief with treatment. Individuals in this situation can provide valuable insights into their pain management strategies. The identification of factors associated with greater pain relief enabled us to explore potential opportunities for improving the well-being of individuals living with CP. For example, our results reiterate the importance of implementing a comprehensive and personalized approach to pain treatment, which integrates pharmacological, physical, and psychological interventions, along with the involvement of a trusted healthcare provider. Additionally, individuals with CP need better support if they feel the need to use over-the-counter pain medications. Improving overall well-being by addressing psychological distress and general health should also be a focal point for healthcare professionals who assist individuals living with CP. Other factors listed in the above paragraphs should also be considered in further studies, and analytical approaches should allow for exploring their intersections.
The datasets presented in this article are not readily available because COPE Cohort participants did not initially provide consent to open data. The data that support the findings of this study are available from the corresponding author upon reasonable request and conditionally to a proper ethical approval for a secondary data analysis. Programming codes can be obtained directly from the corresponding author. Requests to access the datasets should be directed tobGFjYXNzZWFAdXFhdC5jYQ==.
The studies involving humans were approved by Ethics Committee for Research Involving Human Beings at Université du Québec in Abitibi-Témiscamingue (CÉR-UQAT) (#2018-05-Lacasse, A.). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MZ: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal Analysis, Methodology. GD: Writing – review & editing, Methodology. HN: Writing – review & editing, Formal Analysis, Methodology. GP: Writing – review & editing, Funding acquisition, Methodology. LG: Writing – review & editing, Funding acquisition, Methodology. LB: Writing – review & editing, Funding acquisition, Methodology. AL: Conceptualization, Data curation, Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
The implementation of the COPE Cohort was supported by the Quebec Network on Drug Research and the exploitation of its data was co-funded by the Quebec Pain Research Network, two thematic networks of the Fonds de recherche du Québec—Santé (FRQS). During her Masters' degree training, MZ (first author) received scholarships from: Hecla Québec in partnership with the Fondation de l'Université du Québec en Abitibi-Témiscamingue (FUQAT), the Quebec Pain Research Network (QPRN), and the Intersectoral Health Research Network of University of Quebec (RISUQ). GDF and HLNN hold FRQS and Canadian Institutes of Health Research (CIHR) scholarships. MG Pagé is a Junior 2 research scholar from the FRQS.
We would like to thank the study participants for their contribution to the research, and Ms. Véronique Gagnon, who was involved in the implementation, data cleaning and data management of the COPE Cohort. We also thank Emily-Jayn Rubec, who provided linguistic revision services for this paper.
The Chronic Pain Epidemiology Laboratory led by AL is funded by the FUQAT, in partnership with local businesses: the Pharmacie Jean-Coutu de Rouyn-Noranda and Glencore Fonderie Horne (copper smelter). LB received research grants from AstraZeneca, TEVA and Genentech, as well as consultation fees from AstraZeneca, TEVA and Genentech for projects unrelated to this study. MGP received honoraria from Canopy Growth and research funds from Pfizer Canada for projects unrelated to this study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2024.1306479/full#supplementary-material
1. Treede R-D, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. (2019) 160(1):19–27. doi: 10.1097/j.pain.0000000000001384
2. Schopflocher D, Taenzer P, Jovey R. The prevalence of chronic pain in Canada. Pain Res Manag. (2011) 16(6):445–50. doi: 10.1155/2011/876306
3. Andrew R, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic pain. Pain Pract. (2014) 14(1):79–94. doi: 10.1111/papr.12050
4. Rice ASC, Smith BH, Blyth FM. Pain and the global burden of disease. Pain. (2016) 157(4):791–6. doi: 10.1097/j.pain.0000000000000454
5. Mäntyselkä P, Kumpusalo E, Ahonen R, Kumpusalo A, Kauhanen J, Viinamäki H, et al. Pain as a reason to visit the doctor: a study in Finnish primary health care. Pain. (2001) 89(2–3):175–80. doi: 10.1016/S0304-3959(00)00361-4
6. Atun R. Transitioning health systems for multimorbidity. Lancet. (2015) 386(9995):721–2. doi: 10.1016/S0140-6736(14)62254-6
7. Azevedo LF, Costa-Pereira A, Mendonça L, Dias CC, Castro-Lopes JM. The economic impact of chronic pain: a nationwide population-based cost-of-illness study in Portugal. Eur J Health Econ. (2016) 17(1):87–98. doi: 10.1007/s10198-014-0659-4
8. Mayer S, Spickschen J, Stein KV, Crevenna R, Dorner TE, Simon J, et al. The societal costs of chronic pain and its determinants: the case of Austria. PLoS One. (2019) 14(3):e0213889. doi: 10.1371/journal.pone.0213889
9. Mutubuki EN, Luitjens MA, Maas ET, Huygen FJ, Ostelo RW, van Tulder MW, et al. Predictive factors of high societal costs among chronic low back pain patients. Eur J Pain. (2020) 24(2):325–37. doi: 10.1002/ejp.1488
10. Santé Canada. Report No.: 9780660363967 0660363968. Ce que nous avons entendu: travailler ensemble pour mieux comprendre, prévenir et gérer la douleur chronique. Ottawa (Ontario): Health Canada=Santé Canada (2020).
11. Adams LM, Turk DC. Central sensitization and the biopsychosocial approach to understanding pain. J Appl Biobehav Res. (2018) 23(2):1–18. doi: 10.1111/jabr.12125
12. Kress HG, Aldington D, Alon E, Coaccioli S, Collett B, Coluzzi F, et al. A holistic approach to chronic pain management that involves all stakeholders: change is needed. Curr Med Res Opin. (2015) 31(9):1743–54. doi: 10.1185/03007995.2015.1072088
13. Santé Canada. Report No.: 9780660317489 0660317486. La douleur chronique au Canada: jeter les bases d'un programme d'action: rapport du Groupe de travail canadien sur la douleur. Ottawa (Ontario): Santé Canada (2019).
14. Chou R, Hartung D, Turner J, Blazina I, Chan B, Levander X, et al. Opioid Treatments for Chronic Pain. Rockville, MD: Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services (2020). http://www.ncbi.nlm.nih.gov/books/NBK556253/
15. McDonagh M, Selph S, Buckley D, Holmes R, Mauer K, Ramirez S, et al. Nonopioid Pharmacologic Treatments for Chronic Pain. Rockville (MD): Agency for Healthcare Research and Quality (US) (2020). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK556277/
16. Hylands-White N, Duarte RV, Raphael JH. An overview of treatment approaches for chronic pain management. Rheumatol Int. (2017) 37(1):29–42. doi: 10.1007/s00296-016-3481-8
17. Behdad J, Iulia P, Kenneth DC, Nebojsa Nick K. Herbal medicine for pain management: efficacy and drug interactions. Pharmaceutics. (2021) 13(2):251. doi: 10.3390/pharmaceutics13020251
18. Lalonde L, Choinière M, Martin E, Lévesque L, Hudon E, Bélanger D, et al. Priority interventions to improve the management of chronic non-cancer pain in primary care: a participatory research of the ACCORD program. J Pain Res. (2015) 8:203–15. doi: 10.2147/JPR.S78177
19. Becker WC, Dorflinger L, Edmond SN, Islam L, Heapy AA, Fraenkel L. Barriers and facilitators to use of non-pharmacological treatments in chronic pain. BMC Fam Pract. (2017) 18(1):1–8. doi: 10.1186/s12875-017-0608-2
20. Andersson HI, Ejlertsson G, Leden I, Schersten B. Impact of chronic pain on health care seeking, self care, and medication. Results from a population-based Swedish study. J Epidemiol Community Health. (1999) 53(8):503–9. doi: 10.1136/jech.53.8.503
21. Choiniere M, Dion D, Peng P, Banner R, Barton PM, Boulanger A, et al. The Canadian STOP-PAIN project—part 1: who are the patients on the waitlists of multidisciplinary pain treatment facilities? Can J Anaesth. (2010) 57(6):539–48. doi: 10.1007/s12630-010-9305-5
22. Toblin RL, Mack KA, Perveen G, Paulozzi LJ. A population-based survey of chronic pain and its treatment with prescription drugs. Pain. (2011) 152(6):1249–55. doi: 10.1016/j.pain.2010.12.036
23. Wiering B, de Boer D, Krol M, Wieberneit-Tolman H, Delnoij D. Entertaining accurate treatment expectations while suffering from chronic pain: an exploration of treatment expectations and the relationship with patient- provider communication. BMC Health Serv Res. (2018) 18(1):1–9. doi: 10.1186/s12913-018-3497-8
24. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. (2006) 10(4):287–333. doi: 10.1016/j.ejpain.2005.06.009
25. Cheung CW, Choo CY, Kim Y-C, Lin FS, Moon S-H, Osio-Salido E, et al. Inadequate management of chronic non-cancer pain and treatment-related adverse events in Asia: perspectives from patients from 10 countries/regions. SN Compr Clin Med. (2019) 1(6):442–50. doi: 10.1007/s42399-019-00060-x
26. Price TJ, Gold MS. From mechanism to cure: renewing the goal to eliminate the disease of pain. Pain Med. (2018) 19(8):1525–49. doi: 10.1093/pm/pnx108
27. Costa D, Cruz EB, Lopes DG, da Silva CN, Henriques AR, Luis D, et al. Prevalence of and factors associated with unmanageable pain levels in people with knee or hip osteoarthritis: a cross-sectional population-based study. BMC Musculoskelet Disord. (2023) 24(1):1–13. doi: 10.1186/s12891-022-06110-1
28. Lacasse A, Gagnon V, Nguena Nguefack HL, Gosselin M, Pagé MG, Blais L, et al. Chronic pain patients’ willingness to share personal identifiers on the web for the linkage of medico-administrative claims and patient-reported data: the chronic pain treatment cohort. Pharmacoepidemiol Drug Saf. (2021) 30(8):1012–26. doi: 10.1002/pds.5255
29. Turk DC, Dworkin RH, Allen RR, Bellamy N, Brandenburg N, Carr DB, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. (2003) 106(3):337–45. doi: 10.1016/j.pain.2003.08.001
30. Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. (2005) 113(1):9–19. doi: 10.1016/j.pain.2004.09.012
31. Lacasse A, Roy JS, Parent AJ, Noushi N, Odenigbo C, Page G, et al. The Canadian minimum dataset for chronic low back pain research: a cross-cultural adaptation of the national institutes of health task force research standards. CMAJ Open. (2017) 5(1):E237–E48. doi: 10.9778/cmajo.20160117
32. Choinière M, Ware MA, Pagé MG, Lacasse A, Lanctôt H, Beaudet N, et al. Development and implementation of a registry of patients attending multidisciplinary pain treatment clinics: the Quebec pain registry. Pain Res Manag. (2017) 2017:8123812. doi: 10.1155/2017/8123812
34. Cleeland CS. The Brief Pain Inventory User Guide. Houston, TX: The University of Texas MD Anderson Cancer Center (2009).
35. Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. (2008) 9(2):105–21. doi: 10.1016/j.jpain.2007.09.005
36. Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta-analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Ann Rheum Dis. (2010) 69(2):374–9. doi: 10.1136/ard.2009.107805
37. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. (1995) 36(1):1–10. doi: 10.2307/2137284
38. Babitsch B, Gohl D, von Lengerke T. Re-revisiting Andersen’s behavioral model of health services use: a systematic review of studies from 1998 to 2011. Psychosoc Med. (2012) 9:11. doi: 10.3205/psm000089
39. Gamboa CM, Colantonio LD, Brown TM, Carson AP, Safford MM. Race-sex differences in statin use and low-density lipoprotein cholesterol control among people with diabetes mellitus in the reasons for geographic and racial differences in stroke study. J Am Heart Assoc. (2017) 6(5):e004264. doi: 10.1161/JAHA.116.004264
40. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. (2007) 133(4):581–624. doi: 10.1037/0033-2909.133.4.581
41. Bem SL. The measurement of psychological androgyny. J Consult Clin Psychol. (1974) 42(2):155–62. doi: 10.1037/h0036215
42. Fontayne P, Sarrazin P, Famose J-P. The bem sex-role inventory: validation of a short version for French teenagers. Eur Rev Appl Psychol. (2000) 50(4):405–16.
43. Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. (2005) 114(1–2):29–36. doi: 10.1016/j.pain.2004.12.010
44. Cleeland CS. The Brief Pain Inventory user Guide. Houston (TX): The University of Texas MD Anderson Cancer Cente (2009). Available online at: https://www.mdanderson.org/content/dam/mdanderson/documents/Departments-and-Divisions/Symptom-Research/BPI_UserGuide.pdf
45. Sullivan MJL. The pain catastrophizing scale: development and validation. Psychol Assess. (1995) 7(4):524–32. doi: 10.1037/1040-3590.7.4.524
46. Deyo RA, Dworkin SF, Amtmann D, Andersson G, Borenstein D, Carragee E, et al. Report of the NIH task force on research standards for chronic low back pain. J Pain. (2014) 15(6):569–85. doi: 10.1016/j.jpain.2014.03.005
47. Bruyère O, Demoulin M, Brereton C, Humblet F, Flynn D, Hill JC, et al. Translation validation of a new back pain screening questionnaire (the STarT back screening tool) in French. Arch Public Health. (2012) 70(1):12. doi: 10.1186/0778-7367-70-12
48. Kroenke K, Spitzer RL, Williams JBW, Löwe B. An ultra-brief screening scale for anxiety and depression: the PHQ–4. Psychosomatics. (2009) 50(6):613–21. doi: 10.1016/S0033-3182(09)70864-3
49. Maruish ME. User’s Manual for the SF-12v2 Health Survey. Lincoln: QualityMetric Incorporated (2012).
50. Katz MH. Multivariable Analysis: A Practical Guide for Clinicians and Public Health Researchers. New York: Cambridge University Press (2011).
51. Sourial N, Vedel I, Le Berre M, Schuster T. Testing group differences for confounder selection in nonrandomized studies: flawed practice. CMAJ. (2019) 191(43):E1189–E93. doi: 10.1503/cmaj.190085
52. Vatcheva KP, Lee M, McCormick JB, Rahbar MH. Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiology. (2016) 6(2):227. doi: 10.4172/2161-1165.1000227
53. Gauss C, Bursac Z, Hosmer D, Williams D. Purposeful selection of variables in logistic regression. Source Code Biol Med. (2008) 3(1):1–8. doi: 10.1186/1751-0473-3-1
54. Hanley C, Ladha KS, Clarke HA, Cuthbertson BC, Wijeysundera DN, Investigators MS. Association of postoperative complications with persistent post-surgical pain: a multicentre prospective cohort study. Br J Anaesth. (2022) 128(2):311–20. doi: 10.1016/j.bja.2021.10.027
55. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. (2017) 10:2287–98. doi: 10.2147/JPR.S144066
56. Willingham MD, Vila MR, Ben Abdallah A, Avidan MS, Haroutounian S. Factors contributing to lingering pain after surgery: the role of patient expectations. Anesthesiology. (2021) 134(6):915–24. doi: 10.1097/ALN.0000000000003754
57. Minami K, Kazawa M, Kakuta T, Fukushima S, Fujita T, Ohnishi Y. U-shaped association between elapsed time after surgery and the intensity of chronic postsurgical pain following cardiac surgery via thoracotomy: an observational cohort study. Gen Thorac Cardiovasc Surg. (2022) 70(11):931–8. doi: 10.1007/s11748-022-01825-3
58. Fletcher D, Lavand'-homme P, Stamer UM, Pogatzki-Zahn E, Zaslansky R, Tanase NV, et al. Chronic postsurgical pain in Europe: an observational study. Eur J Anaesthesiol. (2015) 32(10):725–34. doi: 10.1097/EJA.0000000000000319
59. Parsons B, Schaefer C, Mann R, Sadosky A, Daniel S, Nalamachu S, et al. Economic and humanistic burden of post-trauma and post-surgical neuropathic pain among adults in the United States. J Pain Res. (2013) 6:459–69. doi: 10.2147/JPR.S44939
60. Thapa P, Euasobhon P. Chronic postsurgical pain: current evidence for prevention and management. Korean J Pain. (2018) 31(3):155–73. doi: 10.3344/kjp.2018.31.3.155
61. Majedi H, Amini MH, Yousefshahi F, Khazaeipour Z, Majedi M, Rahimi M, et al. Predicting factors of pain duration in patients with chronic pain: a large population-based study. Anesth Pain Med. (2020) 10(1):e95776. doi: 10.5812/aapm.95776
62. Gerdle B, Rivano Fischer M, Cervin M, Ringqvist Å. Spreading of pain in patients with chronic pain is related to pain duration and clinical presentation and weakly associated with outcomes of interdisciplinary pain rehabilitation: a cohort study from the Swedish quality registry for pain rehabilitation (SQRP). J Pain Res. (2021) 14:173–87. doi: 10.2147/JPR.S288638
63. Pagé MG, Lacasse A, Dassieu L, Hudspith M, Moor G, Sutton K, et al. Une étude transversale sur l’évolution de la douleur et la détresse psychologique chez les personnes atteintes de douleur chronique: l’étude pancanadienne « Douleur chronique et COVID-19. Health Promot Chronic Dis Prev Can. (2021) 41(5):141–52. doi: 10.24095/hpcdp.41.5.01
64. Borsook D, Youssef AM, Simons L, Elman I, Eccleston C. When pain gets stuck: the evolution of pain chronification and treatment resistance. Pain. (2018) 159(12):2421–36. doi: 10.1097/j.pain.0000000000001401
65. Pagé MG, Romero Escobar EM, Ware MA, Choinière M. Predicting treatment outcomes of pain patients attending tertiary multidisciplinary pain treatment centers: a pain trajectory approach. Can J Pain. (2017) 1(1):61–74. doi: 10.1080/24740527.2017.1325715
66. Bonafé FSS, Marôco J, Campos JADB. Pain self-efficacy questionnaire and its use in samples with different pain duration time. Br J Pain. (2018) 1(1):33–9. doi: 10.5935/2595-0118.20180008
67. Jackson T, Wang Y, Wang Y, Fan H. Self-efficacy and chronic pain outcomes: a meta-analytic review. J Pain. (2014) 15(8):800–14. doi: 10.1016/j.jpain.2014.05.002
68. Hu Y, Yang Z, Li Y, Xu Y, Zhou X, Guo N. Anxiety symptoms and associated factors among chronic low back pain patients in China: a cross-sectional study. Front Public Health. (2022) 10:878865. doi: 10.3389/fpubh.2022.878865
69. Jöud A, Björk J, Gerdle B, Grimby-Ekman A, Larsson B. The association between pain characteristics, pain catastrophizing and health care use—baseline results from the SWEPAIN cohort. Scand J Pain. (2017) 16:122–8. doi: 10.1016/j.sjpain.2017.04.071
70. Yazdi-Ravandi S, Taslimi Z, Jamshidian N, Saberi H, Shams J, Haghparast A. Prediction of quality of life by self-efficacy, pain intensity and pain duration in patient with pain disorders. Basic Clin Neurosci. (2013) 4(2):117–24.25337337
71. Angst Martin S, Brose William G, Dyck John B. The relationship between the visual analog pain intensity and pain relief scale changes during analgesic drug studies in chronic pain patients. Anesthesiology. (1999) 91(1):34–41. doi: 10.1097/00000542-199907000-00009
72. Littman GS, Walker BR, Schneider BE. Reassessment of verbal and visual analog ratings in analgesic studies. Clin Pharmacol Ther. (1985) 38(1):16–23. doi: 10.1038/clpt.1985.127
73. Farrar JT, Young JP Jr., LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. (2001) 94(2):149–58. doi: 10.1016/S0304-3959(01)00349-9
74. Sturgeon JA, Langford D, Tauben D, Sullivan M. Pain intensity as a lagging indicator of patient improvement: longitudinal relationships with sleep, psychiatric distress, and function in multidisciplinary care. J Pain. (2021) 22(3):313–21. doi: 10.1016/j.jpain.2020.10.001
75. Conaghan PG, Peloso PM, Everett SV, Rajagopalan S, Black CM, Mavros P, et al. Inadequate pain relief and large functional loss among patients with knee osteoarthritis: evidence from a prospective multinational longitudinal study of osteoarthritis real-world therapies. Rheumatology. (2015) 54(2):270–7. doi: 10.1093/rheumatology/keu332
76. Feinstein AB, Sturgeon JA, Darnall BD, Dunn AL, Rico T, Kao MC, et al. The effect of pain catastrophizing on outcomes: a developmental perspective across children, adolescents, and young adults with chronic pain. J Pain. (2017) 18(2):144–54. doi: 10.1016/j.jpain.2016.10.009
77. Eaves ER. “Just Advil”: harm reduction and identity construction in the consumption of over-the-counter medication for chronic pain. Soc Sci Med. (2015) 146:147–54. doi: 10.1016/j.socscimed.2015.10.033
78. Kim J, Kinney K, Nyquist M, Capellari E, Vordenberg SE. Factors that influence how adults select oral over-the-counter analgesics: a systematic review. J Am Pharm Assoc (2003). (2022) 62(4):1113–23. doi: 10.1016/j.japh.2022.03.007
79. Ndegwa S, Dolcine B, Frey N, Quay T. Report No.: 81. Access to and availability of non-pharmacological treatments for chronic non-cancer pain in Canada: an environmental scan. Ottawa: Canadian Agency for Drugs and Technologies in Health (CADTH) (2018).
80. Park J, Hughes AK. Nonpharmacological approaches to the management of chronic pain in community-dwelling older adults: a review of empirical evidence. J Am Geriatr Soc. (2012) 60(3):555–68. doi: 10.1111/j.1532-5415.2011.03846.x
81. Allen S. Seeking pain relief with fewer side effects. IEEE Pulse. (2022) 13(2):11–5. doi: 10.1109/MPULS.2022.3159065
82. Yoon J, Choi J, Shin M. Self-natural posture exercise and chronic pain reduction. Soc Behav Pers. (2019) 47(11):1–11. doi: 10.2224/sbp.8273
83. Houzé B, El-Khatib H, Arbour C. Reprint of: efficacy, tolerability, and safety of non-pharmacological therapies for chronic pain: an umbrella review on various CAM approaches. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 87(Part B):307–21. doi: 10.1016/j.pnpbp.2018.08.002
84. Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: recommendation from the American college of sports medicine and the American heart association. Circulation. (2007) 116(9):1094–105. doi: 10.1161/CIRCULATIONAHA.107.185650
85. Ng MML, Leung MCP, Poon DMY. The effects of electro-acupuncture and transcutaneous electrical nerve stimulation on patients with painful osteoarthritic knees: a randomized controlled trial with follow-up evaluation. J Altern Complement Med. (2003) 9(5):641–9. doi: 10.1089/107555303322524490
86. Dugan E, Trachtenberg F, Hall MA. Development of abbreviated measures to assess patient trust in a physician, a health insurer, and the medical profession. BMC Health Serv Res. (2005) 5:64. doi: 10.1186/1472-6963-5-64
87. Henry SG, Bell RA, Fenton JJ, Kravitz RL. Goals of chronic pain management: do patients and primary care physicians agree and does it matter? Clin J Pain. (2017) 33(11):955–61. doi: 10.1097/AJP.0000000000000488
88. Staiger TO, Jarvik JG, Deyo RA, Martin B, Braddock CH. BRIEF REPORT: patient-physician agreement as a predictor of outcomes in patients with back pain. J Gen Intern Med. (2005) 20(10):935–7. doi: 10.1111/j.1525-1497.2005.0175.x
89. Ng SK, Cicuttini FM, Davis SR, Bell R, Botlero R, Fitzgibbon BM, et al. Poor general health and lower levels of vitality are associated with persistent, high-intensity low back pain and disability in community-based women: a prospective cohort study. Maturitas. (2018) 113:7–12. doi: 10.1016/j.maturitas.2018.04.007
90. Safakish R, Ko G, Salimpour V, Hendin B, Sohanpal I, Loheswaran G, et al. Medical cannabis for the management of pain and quality of life in chronic pain patients: a prospective observational study. Pain Med. (2020) 21(11):3073–86. doi: 10.1093/pm/pnaa163
91. Ferrari R, Zanolin ME, Duse G, Visentin M. Effectiveness of opioid analgesics in chronic noncancer pain. Pain Pract. (2015) 15(3):272–8. doi: 10.1111/papr.12176
92. Chapman KB, Groenen PS, Patel KV, Vissers KC, Helmond N. T12 dorsal root ganglion stimulation to treat chronic low back pain: a case series. Neuromodulation. (2020) 23(2):203–12. doi: 10.1111/ner.13047
93. Hemington KS, Cheng JC, Bosma RL, Rogachov A, Kim JA, Davis KD. Beyond negative pain-related psychological factors: resilience is related to lower pain affect in healthy adults. J Pain. (2017) 18(9):1117–28. doi: 10.1016/j.jpain.2017.04.009
94. Sheffler JL, Schmiege SJ, Sussman J, Bekelman DB. A longitudinal analysis of the relationships between depression, fatigue, and pain in patients with heart failure. Aging Ment Health. (2021) 25(12):2272–8. doi: 10.1080/13607863.2020.1855626
95. Danielle SC, Nicole EC, Rodrigo BM, Yena L, Hyun Jung P, Nelson BR, et al. Pain and major depressive disorder: associations with cognitive impairment as measured by the THINC-integrated tool (THINC-it). Scand J Pain. (2017) 15(1):62–7. doi: 10.1016/j.sjpain.2016.12.004
96. Bai J, Cheng C. Anxiety, depression, chronic pain, and quality of life among older adults in rural China: an observational, cross-sectional, multi-center study. J Community Health Nurs. (2022) 39(3):202–12. doi: 10.1080/07370016.2022.2077072
97. Blyth FM, Rochat S, Cumming RG, Creasey H, Handelsman DJ, Couteur DGL, et al. Pain, frailty and comorbidity on older men: the CHAMP study. Pain. (2008) 140(1):224–30. doi: 10.1016/j.pain.2008.08.011
98. Leong IY, Farrell MJ, Helme RD, Gibson SJ. The relationship between medical comorbidity and self-rated pain, mood disturbance, and function in older people with chronic pain. J Gerontol A Biol Sci Med Sci. (2007) 62(5):550–5. doi: 10.1093/gerona/62.5.550
99. Schneider J, Algharably EAE, Budnick A, Wenzel A, Dräger D, Kreutz R. High prevalence of multimorbidity and polypharmacy in elderly patients with chronic pain receiving home care are associated with multiple medication-related problems. Front Pharmacol. (2021) 12:686990. doi: 10.3389/fphar.2021.686990
100. D’Souza RS, Langford B, Wilson RE, Her YF, Schappell J, Eller JS, et al. The state-of-the-art pharmacotherapeutic options for the treatment of chronic non-cancer pain. Expert Opin Pharmacother. (2022) 23(7):775–89. doi: 10.1080/14656566.2022.2060741
101. Chang TI, Park H, Kim DW, Jeon EK, Rhee CM, Kalantar-Zadeh K, et al. Polypharmacy, hospitalization, and mortality risk: a nationwide cohort study. Sci Rep. (2020) 10(1):1–9. doi: 10.1038/s41598-019-56847-4
102. Shi S, Mörike K, Klotz U. The clinical implications of ageing for rational drug therapy. Eur J Clin Pharmacol. (2008) 64(2):183–99. doi: 10.1007/s00228-007-0422-1
103. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. (2017) 17(1):230. doi: 10.1186/s12877-017-0621-2
104. Ferrari A, Baraldi C, Licata M, Rustichelli C. Polypharmacy among headache patients: a cross-sectional study. CNS Drugs. (2018) 32(6):567–78. doi: 10.1007/s40263-018-0522-8
105. Comerci G, Katzman J, Duhigg D. Controlling the swing of the opioid Pendulum. N Engl J Med. (2018) 378(8):691–3. doi: 10.1056/NEJMp1713159
106. Godbout-Parent M, Julien N, Nguena Nguefack HL, Pagé MG, Guénette L, Blais L, et al. Changing society, changing research: integrating gender to better understand physical and psychological treatments use in chronic pain management. Pain. (2023) 165(3):674–84. doi: 10.1097/j.pain.0000000000003072
107. Marshall K. Utilisation de l'ordinateur au travail. L'emploi et le revenu en perspective. L'édition en Ligne. (2001).
Keywords: chronic pain, pain, management, relief, treatment, clinical relevance, clinically meaningful, associated factors
Citation: Zerriouh M, De Clifford-Faugère G, Nguena Nguefack HL, Pagé MG, Guénette L, Blais L and Lacasse A (2024) Pain relief and associated factors: a cross-sectional observational web-based study in a Quebec cohort of persons living with chronic pain. Front. Pain Res. 5:1306479. doi: 10.3389/fpain.2024.1306479
Received: 3 October 2023; Accepted: 4 March 2024;
Published: 15 March 2024.
Edited by:
Stephen E. Nadeau, University of Florida, United StatesReviewed by:
Robert L. Barkin, Rush University Medical Center, United States© 2024 Zerriouh, De Clifford-Faugère, Nguena Nguefack, Pagé, Guénette, Blais and Lacasse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anaïs Lacasse bGFjYXNzZWFAdXFhdC5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.