 Golnaz Barjandi1,†
Golnaz Barjandi1,† Johanna Svedenlöf1*†
Johanna Svedenlöf1*† Hajer Jasim1,2
Hajer Jasim1,2 Malin Collin1
Malin Collin1 Britt Hedenberg-Magnusson1,2
Britt Hedenberg-Magnusson1,2 Nikolaos Christidis1
Nikolaos Christidis1 Malin Ernberg1
Malin Ernberg1
- 1Department of Dental Medicine, Karolinska Institutet, and the Scandinavian Center for Orofacial Neuroscience (SCON), Huddinge, Sweden
- 2Department of Orofacial Pain and Jaw Function, Eastman Institute, Stockholm, Sweden
Mastication myalgia is the most common cause of non-odontogenic pain in the orofacial region and is often associated with a reduced quality of life. The purpose of this review is to provide an overview of the clinical aspects of myalgia based on available research. The review includes epidemiological, diagnostic, and etiological aspects. In addition, the potential risk factors related to the transition from acute to chronic myalgia are explored and treatment strategies are presented for its management. As a result, this review may increase clinical knowledge about mastication myalgia and clarify strategies regarding prevention, diagnostics, and management to improve prognosis and reduce patient suffering.
1 Introduction
Pain is a complex and multi-faceted phenomenon shaped by biological and psychosocial factors (1). While acute pain (short term pain) serves as a protective mechanism crucial for our survival, chronic pain (pain lasting more than 3 months) lacks a clear biological purpose (2).
Chronic pain is considered a significant public health problem globally and approximately one in five people in USA and Europe are estimated to have chronic pain (3, 4). It is more common in women compared to men, implying potential gender-related nuances in its development and persistence (3, 4).
Temporomandibular disorders (TMDs) are the most common type of chronic pains in the orofacial region and include pathological conditions affecting the masticatory muscles, temporomandibular joints (TMJs) and their associated structures. Among these, pain in masticatory muscles i.e., mastication myalgia (M-TMD) is more frequently encountered compared to TMJ disorders. M-TMD is characterized by local or regional pain in the masticatory muscles, increased tenderness, chewing difficulties, and restricted mouth opening (5). It is a debilitating condition often accompanied by a reduced quality of life for the patients. Similar to other pain conditions, M-TMD is more common in women compared to men and often co-occurs with other chronic painful and non-painful conditions of neurological, psychological, and gastrointestinal origin (6–8).
Although some patients, often those with localized M-TMD, have complete remission, the persistence of pain in the masticatory muscles is common (9–11). These cases frequently present a clinical challenge due to their complexity and the limited understanding of their origins and development pathways. Managing these patients proves complex due to the restricted range of treatment options, further aggravated by the occurrence of other comorbid health conditions, for example other pain conditions, depression, anxiety, stress, and sleep disruptions. Consequently, persistent pain and M-TMD is a frequent cause of sick leave, imposing substantial financial strains on the society, in the form of healthcare usage as well as reduced work and productivity (12).
This review aims to provide an up-to-date clinical overview of M-TMD including its epidemiology, etiology, and diagnosis as well as treatment approaches aimed at mitigating its incidence. Increasing our knowledge of M-TMD may facilitate early detection, effective management, and could potentially lead to reduced chronicity.
2 Prevalence and incidence
The prevalence of M-TMD is difficult to estimate accurately, as it varies widely depending on differences in study cohorts, diagnostic criteria, and examination methods (13, 14). However, research suggests that it is a relatively common condition worldwide and the lifetime prevalence is between 3% and 15% in the general population. Nevertheless, the prevalence of M-TMD can be higher in specific subgroups with conditions, such as fibromyalgia, chronic fatigue, or whiplash syndrome (13, 15, 16).
Several studies have investigated the prevalence and incidence of orofacial pain in individuals between 10 and 80 years old (17–20). The prevalence varies considerably depending on how the question was posed. Studies that ask for TMD symptoms generally show higher prevalence, while studies asking for more frequent orofacial pain in general show lower prevalence. For example, a large study in Sweden including 137,000 individuals reported an overall prevalence of frequent orofacial pain (at least once per week) of almost 5% (18). Fewer studies have specifically investigated the prevalence of M-TMD. A meta-analysis of 21 studies including a total of 3,463 patients with TMD found an overall prevalence of M-TMD of 45.3%, but a prevalence of 9.7% in studies conducted in the general population (2,491 subjects) (17). A study from Brazil where 1,643 subjects were randomly selected and examined according to the RDC/TMD criteria revealed that 29.5% fulfilled the criteria for M-TMD (19). The prevalence of signs and symptoms of M-TMD in children and adolescents is even more variable due to the absence of a validated diagnostic criteria for this specific population.
Numerous studies consistently demonstrate a higher prevalence of M-TMD in females compared to males (13, 17, 18) with women being two to three times more likely to suffer from M-TMD than men. However, the gender differences are greater in samples drawn from tertiary clinics than from the population and one reason to this may be differences in health care seeking (21). There are also signs of increasing prevalence of orofacial pain over time and more so in women, indicating an increasing gender difference for orofacial pain including M-TMD (22).
M-TMD can occur at any age but is often reported to occur more frequently in young to middle-aged adults. The Orofacial Pain: Prospective Evaluation and Risk Assessment (OPPERA) study, a comprehensive cohort study conducted in the United States, provided estimates regarding the development of painful TMD in adults aged 18–44 years (23). The study revealed that approximately 4% of healthy pain-free adults within this age range develop clinically confirmed first-onset painful TMD each year. Furthermore, the annual incidence of painful TMD was observed to increase with age, with rates of 2.5% for those aged 18–25 years, 3.7% for those aged 25–34 years, and 4.5% for those aged 35–44 years (23). While M-TMD can also affect elderly individuals, its frequency appears to decrease in this population (20). In such cases, myalgia is particularly associated with age-related changes in the musculoskeletal system or may be secondary to osteoarthritis.
3 Etiology
There is not one specific cause of TMD, and studies have shown TMD to have a biopsychosocial and multifactorial background with several risk factors that increase the susceptibility of developing TMD (16, 24–26). These factors can be biological, behavioral, psychosocial, but also previous chronic pain conditions and trauma are important risk factors. It has been suggested that one of the most important factors to develop TMD is other somatic symptoms (27). For instance, patients with fibromyalgia have a higher prevalence of TMD symptoms (28). Furthermore, having another chronic pain condition increases the risk of developing a new chronic pain disorder (21).
In addition to somatic symptoms, increased levels of anxiety, sleep difficulties and depression are often found in TMD patients making biopsychosocial aspects strong predictor for developingpainful TMDs (29). It has been hypothesized that pain amplification may be important in the etiology since it seems to occur more often in patients TMD-M. The pain amplification may be caused by enhanced pain facilitation and deficient pain inhibition. This is supported by increased mechanical sensitivity (lower pain thresholds), greater temporal summation, and impaired conditioned pain modulation in TMD compared to pain-free controls (21, 30). Biological sex is among identified risk factors for TMD-M, which is not surprising given the higher prevalence of orofacial pain in women than men in the general population (18, 22). However, other studies have reported only marginally increased risk for TMD in women (15, 31) and suggested that this may be due to prevalence-incidence bias (15). However, other factors such as sex hormones, psychosocial factors and gender role expectations may also explain these differences. Also, prior trauma, both macro- and microtrauma, such as prolonged mouth opening, intubation, and parafunctional activities have been suggested as a denominator of TMD etiology (24, 26). The OPPERA study found that parafunctional activity, reported by the patient, was a predictor for TMD (15, 32).
4 The transition from acute to chronic TMD pain
In TMD, the transition to chronic pain and the risk factors associated with the transition are important to understand for determination of a personalized treatment strategy.
A few studies have investigated differences between patients with acute and chronic TMD pain. Sabsoob and coworkers in a critical review including seven studies found no significant difference regarding age, race, gender and socioeconomical status between the groups (33). However, one of the included studies reported that chronic TMD pain was more prevalent in females than in males (34). Psychological factors such as depression, stress and somatization were more prevalent in chronic TMD pain patients, whereas anxiety showed conflicting results (33). The study by Cao et al. (34) also reported that patients with chronic TMD pain more often reported impaired sleep quality than patients with acute TMD pain. This indicates that poor sleep may be important for the transition from acute to chronic TMD pain. Further, chronic TMD pain patients more often had a diagnosis of TMD-M than acute TMD patients, while arthralgia was more common in acute TMD patients (33). Meloto et al. (2019) found that the vertical mobility of the mandible in combination with experience of a pain-sensation that was altered by mandibular movements was correlated with persistent TMD, indicating that hyperalgesia could be a predictor (35). The OPPERA study in a cluster analysis found three clusters in their cohort, an adaptive, a pain-sensitive with increased sensitivity to experimental pain, and a global symptoms cluster with increased sensitivity and greater psychological distress. The chronic TMD cases were more likely to belong to the pain-sensitive and global symptoms cluster and they showed greater pain intensity, jaw functional limitation, and more comorbid pain conditions than the cases in the adaptive cluster (36).
A diagnosis of TMD-M was found important for the transition from acute to chronic TMD pain. This risk appeared to be greater in women and was not confounded by pain intensity, pain disability, or non-specific symptoms (33). Another risk factor identified in the critical review (33) was pain intensity at baseline, which also has been reported previously in other pain conditions (37, 38). Also, patients with high grade of disability at baseline had an increased risk of developing chronic TMD, even if this risk did not reach significance (33). Finally, another study found that chronic neck pain was more prevalent in patients with chronic TMD pain and disability than acute TMD pain, suggesting that chronic disability might be involved in the transition from acute to chronic TMD pain (39). However, the factors involved in the transition from acute to chronic pain are almost unknown and much more research is needed to understand this in order to be able to prevent the transition.
5 Classification
Ideally diagnostics should be based on objective measures with high sensitivity and specificity for the disease in question. Objective measures require that the underlying mechanisms of the disease are known, for example through specific biomarkers. Biomarkers have been defined as “…characteristics that are objectively measured and evaluated as indicators of normal biological processes, pathogenic processes, or responses to an intervention” (40). This means that the measurement of blood pressure for diagnostics of hypertension or blood glucose level for diabetes can be classified as biomarkers.
For chronic pain, such as M-TMD, there is no single biomarker that can be used for diagnosis. Instead, we must rely on symptoms and signs specific for the disorder. Pain is the most prominent symptom and can be classified in many ways. For example, according to its anatomical location, such as headache or orofacial pain. As mentioned above, pain can also be classified as acute or chronic. In contrast to acute pain, which is regarded a symptom of a disease, chronic pain is defined as a disease in itself (41). Another way of classifying pain is by the supposed mechanism, for example nociceptive, neuropathic, and nociplastic pain. The term nociplastic pain was introduced in 2016 and describes a “pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain” (42). In the suggested clinical criteria for nociplastic pain the presence of comorbidities (e.g., sleep disturbance and fatigue) and sensory disturbances in the region of pain (e.g., mechanical, or cold allodynia) are important for clinical diagnostics (43). These are common features of TMD patients. Therefore, at least a subgroup of patients with TMD could probably be classified as having nociplastic pain, while others may have nociceptive pain. It is also possible to have a combination of nociceptive and nociplastic pain and ongoing nociceptive pain has been suggested to be a risk factor for developing nociplastic pain (43, 44).
To diagnose TMD several classifications exist (Table 1). Many of these include a set of criteria that are not validated, e.g., the 2008 classification of orofacial pain by the American Academy of Orofacial Pain (AAOP) (45) that was intended to be used “as a road map” for clinical purposes. The Research Diagnostic Criteria for TMD (RDC/TMD) (46) introduced a paradigm shift as it considered the biopsychosocial model, and, in addition to the clinical diagnoses (axis I), included psychosocial assessment (axis II). The axis I includes validated examination methods. Thus, it was the first classification that was at least partly validated. Later validation, however, found that the sensitivity and specificity for the diagnoses were low (47, 48); only for myofascial pain and myofascial pain with limited opening combined, the validity reached the pre-set criteria. To try to overcome this, and to make the classification clinically more useful, the algorithms were revised and updated diagnoses were later presented in the Diagnostic Criteria for TMD (DC/TMD) (5). This classification includes validated criteria for the most common TMD diagnoses. The DC/TMD reached excellent sensitivity and specificity for M-TMD and the other pain diagnoses, but for the intracapsular TMJ disorders the preset limits for sensitivity and specificity were still not met. Nevertheless, it was suggested to be used in both research and clinical settings and is now the most used classification at specialist clinics world-wide with translations into many languages.
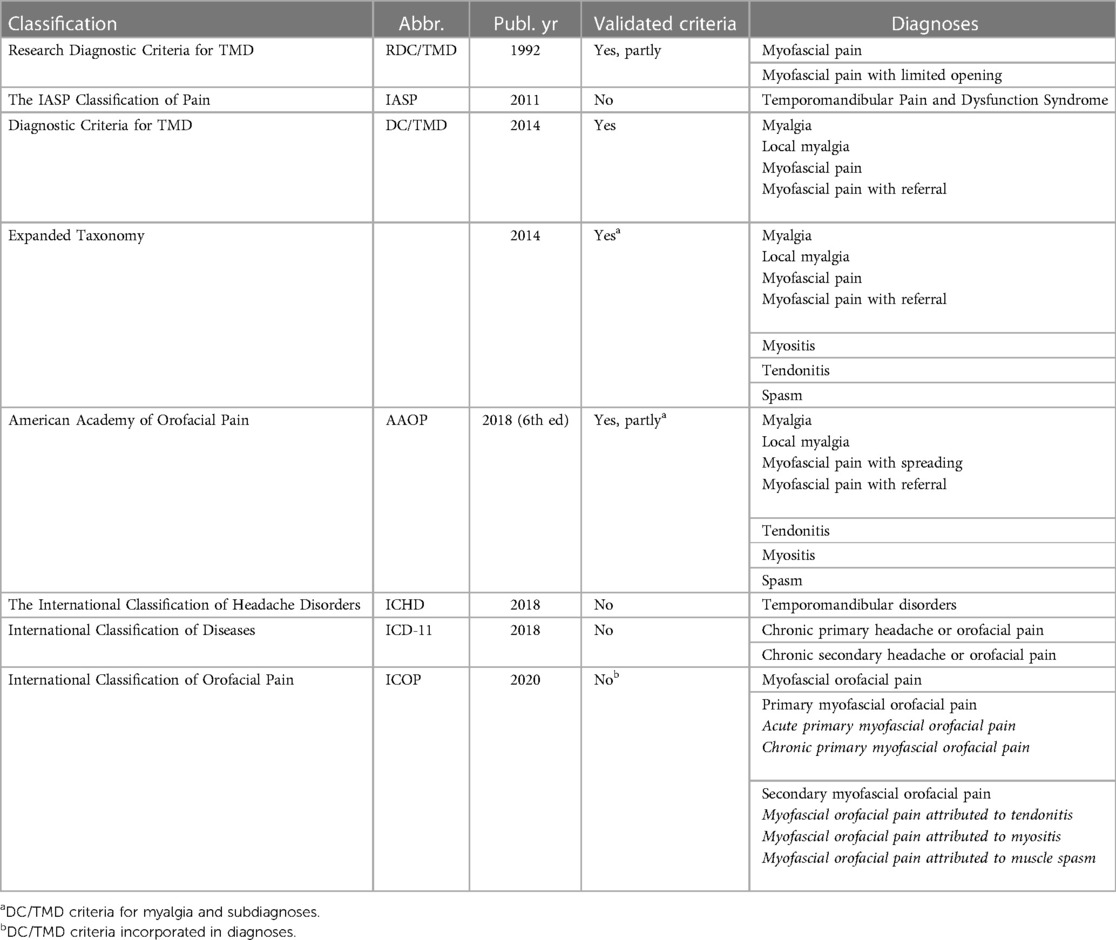
Table 1. Classifications that include M-TMD diagnoses.
At the same time as the development of the DC/TMD an Expanded Taxonomy of the DC/TMD was developed and published (49). This is a broader classification of orofacial pain based on the AAOP classification for orofacial pain with expert-based criteria also for more rare conditions that awaits further research for validation. However, for M-TMD (and other DC/TMD diagnoses), the DC/TMD diagnoses and criteria were adopted (5). Also, the AAOP has adopted the DC/TMD in the 2018 edition (50) (Table 1).
Shortly after the work with DC/TMD, the International Association for the Study of Pain (IASP) began work to include pain diagnoses in the new version of the International Classification of Diseases (ICD-11) (51). In this, orofacial pain is included under the code MG30.03 (Chronic primary headache or orofacial pain) and MG30.6 (Chronic secondary headache or orofacial pain), but no specific TMD diagnoses are included.
Another classification is the International Classification of Headache Disorders (ICHD-3) which includes criteria for Headache attributed to TMD (52). However, it is stated that since diagnosis of TMD can be difficult, “the diagnostic criteria evolved by the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group is recommended”, i.e., the DC/TMD classification (5).
The most recent classification for orofacial pain is the International Classification of Orofacial Pain (53). This includes myofascial orofacial pain. The classification follows the structure of the ICHD criteria for tension-type headache where the pain is classified according to its frequency (infrequent, frequent, and highly frequent) but have included the validated DC/TMD criteria for diagnosis.
The DC/TMD has now been used for almost ten years and recently the DC/TMD for children and adolescents was published (54). This is the first classification of TMDs in children. It was developed after a Delphi process and includes the DC/TMD axis I. However, it needs to be validated in this patient group. The diagnostics according to DC/TMD require the use of specified commands and examination procedures, why it has shown difficult to implement it in general dentistry. A simplified version for general dentistry, which includes only the examinations of importance for pain diagnoses is under development (personal communication). This lacks the verbal commands as a study showed that excluding the commands did not impair the diagnostic reliability (55). The hope is that these new criteria will be used by general dentists. In Sweden, these criteria are now taught at all dental schools.
To screen for TMDs there are also a few instruments available. The TMD pain screener is a validated instrument that includes three (short version) or six (long version) questions about the presence of orofacial pain in general, pain or stiffness at awakening, and activities that may influence pain during the last 30 days (56). A score of 2 out of 4 for the short version and 3 out 7 for the long version are cut-off values. Another validated screener is the 3Q/TMD (57). This also includes three questions, two concerning the presence of orofacial pain in general and at jaw opening once per week or more often, and one question about jaw catching/locking, once per week or more often. A positive answer to any of these questions imply the need for further interview and examination of the jaw system. The use of a short screening questionnaire together with a shorter DC/TMD examination is expected to facilitate diagnostics for practicing general dentists.
6 DC/TMD myalgia diagnostics
For M-TMD, the DC/TMD lists four diagnoses, of which two are validated. The sensitivity and specificity for myalgia are 0.90 and 0.99, respectively, and for myofascial pain with referral, 0.86 and 0.98, respectively (5). With the publication, two additional diagnoses were included without being validated, local myalgia and myofascial pain. The structure of the DC/TMD is built on both subjective and clinical criteria. For the pain diagnoses these are very similar for all diagnoses, which facilitates learning.
What was new in the DC/TMD compared to the RDC/TMD (46) is that the diagnostic algorithm for myalgia is based on pain in the temporalis or masseter muscle only, no other jaw muscles are included. The clinical DC/TMD examination includes confirmation of pain and headache location; mandibular movement capacity and pain on movements, palpation for TMJ sounds, and palpatory pain of the TMJ, masseter, and temporalis muscle (5). With the diagnostic criteria structured and clearly specified examination procedures are included, for example verbal commands and specification of palpatory time and pressure.
The four DC/TMD myalgia diagnoses are based on subjective reports of pain in the jaw, temple, ear, or in front of the ear during the last 30 days, which is modified with jaw movement, function, or parafunction. During the clinical examination the examiner confirms that the pain area is located within the masseter or temporalis muscle, and the patient report if familiar pain in the masseter and temporalis muscle during jaw opening or palpation of these muscles is present. Depending on if muscle palpation elicits pain that only is experienced in the point that is being palpated, or spreads within or beyond the muscle (for example to the teeth) the sub-diagnoses local myalgia, myofascial pain, and myofascial pain with pain referral can be determined (5).
In DC/TMD, as well as in its predecessor the RDC/TMD psychosocial factors are assessed with the axis II (5, 46). This includes instruments for assessment of pain intensity and pain interference (Graded Chronic Pain Scale), oral parafunctions (Oral Behavior Checklist), Jaw function (Jaw Function Limitation Scale), distress (Patient Health Questionnaire-4 or -9), anxiety (General Anxiety Disorder-7), and physical symptoms (patient History Questionnaire-15).
7 Treatment approaches
It is important to remember that every individual experience pain uniquely and, therefore, treatment regimens need to be individually tailored for each patient (58). Although several treatment approaches have been shown to be successful in management of M-TMD (59), to our knowledge, no single treatment approach has been found superior to all other approaches. Thus, a comprehensive biopsychosocial treatment approach is recommended (60, 61).
According to a recent network meta-analysis (62), the most effective treatment approaches in M-TMD seem to be counseling, occlusal appliances, and jaw exercises, manual therapy or physiotherapy (Table 2). An important point of note is that all these treatments are minimally invasive and for the most part reversible. Other suggested treatment approaches for M-TMD include e.g., acupuncture and needling therapy (63), oral pharmacological treatments (64), behavioural therapies (65), and physical therapies such as for instance transcutaneous electrical nerve stimulation (TENS) (66)and thermal therapy (67).
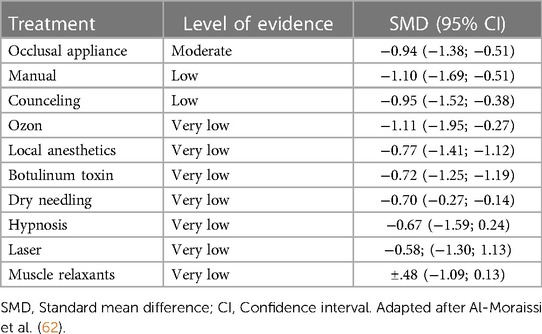
Table 2. Ranking of TMD treatments according to best evidence.
Considering the wide range of available therapies, the everyday clinical decision-making can be a hassle and difficult. Therefore, clinical treatment guidelines can be helpful. In Sweden, for instance, the Swedish Academy of Temporomandibular Disorders, has developed a national treatment protocol for general dentists regarding TMD including M-TMD (68). The national treatment protocol for TMD is based on the Swedish National Guidelines in Dentistry, by The Swedish National Board of Health and Welfare (69), that in turn are based on current best evidence (science and proven experience).
A short overview of the most common treatment approaches will follow.
7.1 Information and counseling
When planning a treatment, it is of great importance to set realistic treatment goals and choose the most suitable treatment strategy for the individual patient. The purpose of the treatment should be to eliminate or reduce the effect of the underlying causes and not just alleviate the symptoms or consequences of these. Since M-TMD is multifactorial with both functional, structural, and psychological causal factors great emphasis should be placed on information and counseling (70).
According to science and proven experience, patients with M-TMD should be offered information and advice as a first step in their treatment (68, 69). Treatment should always begin by giving the patient a simple and clear explanation of the condition, the causal relationships that exist, and that M-TMDs are common, benign conditions, with a good prognosis. Information and counseling can be calming, which in turn can lead to a reduction in anxiety, helping the patient to better tolerate their pain. Information and advice that includes instructions on self-care should be provided together and in a sequence. After information about the condition and causal relationship, counseling should be offered regarding M-TMD followed by individualized advice on self-care (71). One has not to forget that stress management and sleep hygiene also can be included in counseling. This, since it is well known that disturbed sleep increases pain sensitivity (72, 73), and that incorporating physical activity such as forest walks has proven to relive stress and improve overall physical wellbeing (74).
Finally, it is common that patients are unaware of possible parafunctions, or when such parafunctions occur. Therefore, it is important to make the patients aware of their parafunctions and to justify why they need to reduce their parafunctions to motivate them (71). For example, reduction of chewing or clenching, nail-biting, cheek- or lip-biting can in many cases be enough to relieve patients' M-TMD pain.
7.2 Behavioral therapy
Orofacial behaviors encompass mastication, communication (verbally and by facial expressions), and nonfunctional behaviors, such as excessive overuse and parafunctions. The importance of addressing orofacial behaviors in the management of M-TMD has been recognized since the 1950s (75), with increasing evidence since then (75, 76). The management include techniques to create awareness regarding the patients' own body's functions and parafunctions. One commonly used technique is biofeedback. Usually, different kinds of devices are used to register muscle activity and when activity occurs this is signaled to the patients, thus encouraging them to observe or change their behavior. Although time consuming, biofeedback is shown to be effective in reducing masticatory muscle activity (77). However, there is no consensus regarding biofeedback and pain alleviation in M-TMD.
Visual feedback, on the other hand, is a simple and cost-effective method to change a parafunctional behavior. By first identifying situations and/or places where muscle tension or parafunction are induced, a visual reminder, i.e., a colorful sticker is placed there so the patients constantly become reminded and prompted to change their behavior. These situations or places can for instance be working on the computer, driving a car, or using a phone or a tablet. Recently digital applications that automatically send reminder to the patient have been developed.
7.3 Occlusal therapy
Occlusal appliances are commonly used in the treatment of painful TMDs, with the stabilization appliance being the one most used (78). A recent meta-analysis showed that there is moderate evidence that the stabilization appliance reduces M-TMD pain (79), and it has recently been shown as being among the most effective treatments of M-TMD (62). Further, its treatment effect is better than placebo, which is not the case with other types of occlusal appliances (80).
As the mechanisms of action still are unclear, some possible mechanisms that could explain the beneficial effects of stabilization appliances have been proposed. There could be a change in the reflective pattern of the chewing muscles, an increase in awareness of parafunctional activity in the patients, a decrease of the load of the chewing muscles, and last but never to be forgotten, the placebo effect (81–83).
Though occlusal adjustment is an irreversible treatment and there is no evidence that it is effective in treating M-TMD (84), it is still used by dentists, especially in general practice. Since the treatment is doing more harm than good it should not be used to treat M-TMD (85).
7.4 Physiotherapy and self-exercise
Individualized self-exercises for the jaw has been shown to relieve pain both in localized/regional M-TMD and M-TMD associated with generalized pain (86, 87). Further, combining jaw exercises with counselling and relaxation is even more effective (87–89). Self-exercise modalities can be categorized as mobilization exercise, muscle strengthening exercise (resistance training), coordination exercise, and postural exercise. Mobilization and coordination exercises aim to improve muscle flexibility and normalize imbalanced muscle activity by changing patterns of movement and thus relieve muscle pain. Isometric resistant training on the other hand, may relieve muscle pain through an inhibitory effect on muscle activity via Golgi tendons (90). As with most treatments, the outcome of self-exercises regimes heavily relies on the degree of compliance and should therefore be structured, supervised, and evaluated to be effective (86).
7.5 Pharmacological therapy
7.5.1 Per oral
Analgesics are considered a good complement to other treatment modalities for M-TMD. Non-opioid analgesic drugs, which are relevant in this context, is a heterogeneous group mainly consisting of paracetamol and anti-inflammatory drugs. These are recommended for patients with mild to moderate M-TMD pain (91–93).
The analgesic mechanism of action for paracetamol is not fully known. What is known is that paracetamol inhibits the prostaglandin synthesis in the central nervous system, and that it acts via the cannabinoid system (94). Since paracetamol does not act on the cyclooxygenase enzyme (COX) it has no anti-inflammatory effect. Nonsteroidal anti-inflammatory drugs (NSAIDs), on the other hand, inhibit both the enzymes COX-1 and COX-2. The different NSAIDs have varying selectivity for the COX enzymes. By inhibiting the COX enzymes, prostaglandin synthesis is inhibited which in turn reduces inflammation and pain signalling (95). Even though naproxen and ibuprofen (COX-1) are considered the safest NSAIDs to use when it comes to the cardiovascular system, they have been shown to have adverse effect on the gastrointestinal tract causing ulcers and gastric bleeding (92, 96). On the other hand, the COX-2 inhibitor celecoxib has shown to have a small risk for gastrointestinal bleeding, but a high risk for cardiovascular disease (92). So, if the patient is at risk for cardiovascular disease the first-line NSAID choice is naproxen or ibuprofen. If the patient, on the other hand, is at risk for gastrointestinal bleeding and at no risk for cardiovascular disease the first-line NSAID choice is celecoxib.
Another proposed approach is the use of muscle relaxants. Even though they have been used for years to treat M-TMD pain there is very little evidence of an effect, and it seems to be minimal (62, 97). Their usefulness is also limited due to the reported side effect in the form of, for example, drowsiness, dizziness, weakness, and ataxia (98, 99). The mechanism of action of muscle relaxants is that they reduce muscle tension. Therefore, they can sometimes be indicated for reduction of muscle spasms, muscle pain, and headaches. However, a recent network meta-analysis reported that the muscle-relaxant substance cyclobenzaprine could have a short-term pain reducing effect in M-TMD (97). Muscle relaxants must be used with caution since they may induce a significant degree of sedation. Further, these kind of medications are contraindicated for patients with hyperthyroidism and/or congestive heart failure, or patients using monoamine oxidase inhibitors and tramadol (92).
For chronic pain, antidepressants, such as amitriptyline are often recommended and proved to be effective (100). However, a recent network meta-analysis showed that duloxetine was superior to other antidepressants for chronic pain treatment having moderate to high certainty evidence (101). The antidepressants exert their analgesic effect by blocking the re-uptake of serotonin, and/or noradrenalin in doses lower than their antidepressant effect (100). Studies investigating antidepressants in the treatment of M-TMD are scarce. However, a systematic review concluded that there is weak evidence that they are effective but that more studies with sound methodology are needed to demonstrate their effectiveness (102). There are also side-effects to consider with these kinds of drugs. For instance, tricyclic antidepressants are associated with dizziness, blurred vision, constipation, sedation, and dry mouth (103). As for muscle relaxants, tricyclic antidepressants should be avoided for patients using or patients using monoamine oxidase inhibitors since this combination of medications has, in worst case scenario, been shown to lead to lethal serotonin syndrome, which is a condition consisting of confusion, fever, ataxia, as well as severe hypertension (92, 104). Finally, tricyclic antidepressants should be used with caution among elderly and for patients with cardiac disease (92). Even the selective serotonin re-uptake inhibitors should be used with caution since they have been shown to cause dry mouth, nausea and vomiting, headaches, sexual dysfunction, and sweating (105).
7.5.2 Local
Although an increasing number of patients with M-TMD are treated with botulinum toxin, the evidence for its pain reducing effect is still sparse and equivocal (106). Results from the most recent meta-analysis and two netwok meta-analyses indicate that botulinum toxin might have a pain reducing effect, at least in a long-term perspective (62, 107, 108). Though the evidence is very low, more recent RCTs with good methodology seem to show more favourable effects on M-TMD (109, 110). Botulinum toxin is considered safe with few serious side-effects (106). Nevertheless, headache is a known short-term side effect, that is induced as the toxin initially causes muscle spasm and then complete paralysis (111). Further, multiple (112–114), and even a single dose (109) of botulinum toxin causes muscle atrophy and decreased bone volume at the mandibular condyle and body. Because of the low evidence for an effect and high cost, botulinum toxin should be used restrictively.
Similar to botulinum toxin the evidence for a pain-reducing effect by local anaesthetics M-TMD is, very low both in a short- and a long-term perspective (62). Other agents, such as granisetron (a serotonin receptor type 3 antagonist) and platelet rich plasma are reported effective in M-TMD, but also here the evidence is very low due to the few studies done so far (62). The included studies in this review did not report any side-effects for local anaesthetics, granisetron or platelet rich plasma (62). Taken together, future studies on the effect of local pharmacological treatments in M-TMD are needed.
7.6 Needling therapy
Needling techniques include acupuncture and deep dry needling (115, 116). Though acupoints often coincide with myofascial trigger points, acupuncture and dry needling are different therapies (117). In acupuncture thin filiform and dry needles are inserted into defined acupoints in meridians and non-trigger points (115, 118), to induce a better flow of the energy (qi) (119). In deep dry needling, on the other hand, a thin monofilament needle is directly inserted in myofascial trigger points to inactivate them (116).
Even though several studies have shown that acupuncture and deep dry needling are effective, minimally invasive, cheap, and easy to learn treatment modalities for musculoskeletal pain conditions (120), these studies have been carried out in larger muscle-groups as well as in areas outside the orofacial region (121). When the pain reducing effect of acupuncture and deep dry needling was investigated and compared to active or inactive placebo for TMD treatment in a recent network meta-analysis no beneficial effects were found neither regarding pain reducing effect, nor mechanical sensitization (122). However, on an individual basis both acupuncture and deep dry needling can have a pain reducing effect in M-TMD.
7.7 Transcutaneous electrical nerve stimulation
TENS is an effective non-invasive method that promote analgesia and a decrease in EMG activity of masticatory muscles at rest (123). The mechanisms by which TENS exert its effects is believed to be by activation of “gate control” (high-frequency TENS, 50–120 HZ) or by inducing release of endogenous opioids (low-frequency TENS, 2 Hz). A recent systematic review including eight studies with painful TMDs found a significant and considerable pain reduction and improvement of mouth opening immediately after TENS treatment and that the pain intensity was still 40% lower than at baseline one month after completion of treatment (124). In M-TMD, and for treatment of the masseter and temporalis muscles high frequency TENS therapy is recommended (123). However, there are no consensus on an optimal TENS protocol for M-TMD; clinicians are advised to follow manufactures recommendations and regular follow-ups are essential with TENS therapy.
8 Future directions
Ongoing research is actively exploring various dimensions of M-TMD, offering prospects to improve diagnostic, management, and prognostic approaches.
In this regard, the field of genetics and proteomics emerges as a promising avenue. An evolving taxonomy would benefit from embracing a mechanistic classification that not only segregates pain disorders by M-TMD signs and symptoms, but also factors in the underlying mechanisms. This enhanced diagnostic framework has the potential to elucidate the diversity in prognosis and treatment response observed within existing diagnostic categories. For instance, identifying local and systemic biomarkers specific to M-TMD could enhance diagnostic precision and treatment strategies.
Moreover, future research in the heritability of M-TMD may also lead to personalized treatment modalities, grounded in individual genetic profiles. The complex mechanisms connecting genes, epigenetic factors, and masticatory muscle pain certainly need further research (125). Although there are conflicting results regarding the roles of genetic markers for M-TMD, studies indicate that certain gene polymorphisms may be associated with M-TMD. Therefore, “omics” research, i.e., studying genomic, transcriptomic, metablomic, and proteomic markers hold significant potential for future investigation into acute and chronic TMD development, which could facilitate early identification of individuals predisposed to M-TMD (126).
Advancements in brain imaging could also improve management of those with M-TMD. For instance, functional imaging techniques have previously been found distinctive patterns of functional and structural changes within the “pain matrix” (i.e., thalamus, the insular cortex, the primary and secondary somatosensory cortices, the anterior cingulate cortex, and the prefrontal cortex) in patients with chronic M-TMD (127). This emphasizes the potential of brain imaging to increase our knowledge of M-TMD.
Lastly, strategies targeting the transition from acute to chronic pain, lifestyle modifications, and early interventions could potentially mitigate the severity and occurrence of M-TMD. Building on the studies examining M-TMD, future research should delve deeper into stressful life factors, biopsychosocial aspects as well as genetics and pathophysiological changes of the diagnoses to get insights into the etiological factors driving the transition from acute to chronic M-TMD.
9 Conclusion
M-TMD is a complex condition that usually represents a clinical challenge, both in terms of diagnosis and treatment, but also due to lack of deeper knowledge about the etiology. Precise diagnosis is important and, the absence of an accurate diagnosis, may lead to treatment failure and perhaps even exacerbation of the condition. It is therefore important that healthcare professionals know how to recognize risk factors and provide accurate early diagnosis as well as appropriate management to prevent the acute M-TMD to become a chronic condition.
Moreover, this paper shed light on the various factors that contribute to the conditions, including muscular and psychological factors. The diagnostic process for M-TMD can be challenging and requires a thorough evaluation of the patient symptoms and medical history. Treatment options for M-TMD range from conservative measures to more invasive interventions. Therefore, it is important that healthcare providers understand and are familiar with the classifications of M-TMD and its treatments as well as the multifactorial etiology of each patient, to offer comprehensive, multifaceted treatment strategy for best prognosis of these patients.
Author contributions
GB: Conceptualization, Writing – original draft, Writing – review & editing. JS: Conceptualization, Writing – original draft, Writing – review & editing. HJ: Conceptualization, Writing – original draft, Writing – review & editing. MC: Conceptualization, Writing – original draft, Writing – review & editing. BH-M: Conceptualization, Writing – review & editing. NC: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. ME: Conceptualization, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was funded by Karolinska Institutet, Huddinge, Sweden.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain (Amsterdam). (2020) 161(9):1976–82. doi: 10.1097/j.pain.0000000000001939
2. Merskey H, Bogduk N. Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. 2nd ed. Seattle: IASP Press (1994).
3. Rikard SM, Strahan AE, Schmit KM, Guy GP Jr. Chronic pain among adults—United States, 2019–2021. MMWR Morb Mortal Wkly Rep. (2023) 72(15):379–85. doi: 10.15585/mmwr.mm7215a1
4. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. (2006) 10(4):287–333. doi: 10.1016/j.ejpain.2005.06.009
5. Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network* and orofacial pain special interest group. J Oral Facial Pain Headache. (2014) 28(1):6–27. doi: 10.11607/jop.1151
6. Moreno-Fernández AM, Jiménez-Castellanos E, Iglesias-Linares A, Bueso-Madrid D, Fernández-Rodríguez A, De Miguel M. Fibromyalgia syndrome and temporomandibular disorders with muscular pain. A review. Mod Rheumatol. (2017) 27:210–6. doi: 10.1080/14397595.2016.1221788
7. Costa YM, Conti PCR, de Faria FAC, Bonjardim LR. Temporomandibular disorders and painful comorbidities: clinical association and underlying mechanisms. Oral Surg Oral Med Oral Pathol Oral Radiol. (2017) 123(3):288–97. doi: 10.1016/j.oooo.2016.12.005
8. Hoffmann GR, Kotchen MJ, Kotchen AT, Cowley WT, Dasgupta WM, Cowley WA. Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. (2011) 27(3):268–74. doi: 10.1097/AJP.0b013e31820215f5
9. Ohrbach R, Dworkin SF. Five-year outcomes in TMD: relationship of changes in pain to changes in physical and psychological variables. Pain. (1998) 74(2-3):315–26. doi: 10.1016/S0304-3959(97)00194-2
10. Rammelsberg P, LeResche L, Dworkin S, Mancl L. Longitudinal outcome of temporomandibular disorders: a 5-year epidemiologic study of muscle disorders defined by research diagnostic criteria for temporomandibular disorders. J Orofac Pain. (2003) 17(1):9–20.12756926
11. Ohrbach R, Slade GD, Bair E, Rathnayaka N, Diatchenko L, Greenspan JD, et al. Premorbid and concurrent predictors of TMD onset and persistence. Eur J Pain. (2020) 24(1):145–58. doi: 10.1002/ejp.1472
12. Lundberg D, Axelsson S. Treatment of chronic pain—a systematic literature review. SBU’s summary and conclusions. Behandling av Långvarig Smärta—en Systematisk Litteraturöversikt SBUs Sammanfattning och Slutsatser. (2006) 103(17):1297–303.
13. Fernandez-de-las-Penas C, Svensson P. Myofascial temporomandibular disorder. Curr Rheumatol Rev. (2016) 12(1):40–54. doi: 10.2174/1573397112666151231110947
14. Valesan LF, Da-Cas CD, Réus JC, Denardin ACS, Garanhani RR, Bonotto D, et al. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig. (2021) 25(2):441–53. doi: 10.1007/s00784-020-03710-w
15. Slade GD, Ohrbach R, Greenspan JD, Fillingim RB, Bair E, Sanders AE, et al. Painful temporomandibular disorder: decade of discovery from OPPERA studies. J Dent Res. (2016) 95(10):1084–92. doi: 10.1177/0022034516653743
16. Kapos FP, Exposto FG, Oyarzo JF, Durham J. Temporomandibular disorders: a review of current concepts in aetiology, diagnosis and management. Oral Surg. (2020) 13(4):321–34. doi: 10.1111/ors.12473
17. Manfredini D, Guarda-Nardini L, Winocur E, Piccotti F, Ahlberg J, Lobbezoo F. Research diagnostic criteria for temporomandibular disorders: a systematic review of axis I epidemiologic findings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2011) 112(4):453–62. doi: 10.1016/j.tripleo.2011.04.021
18. Lovgren A, Haggman-Henrikson B, Visscher CM, Lobbezoo F, Marklund S, Wanman A. Temporomandibular pain and jaw dysfunction at different ages covering the lifespan—a population based study. Eur J Pain. (2016) 20(4):532–40. doi: 10.1002/ejp.755
19. Progiante PS, Pattussi MP, Lawrence HP, Goya S, Grossi PK, Grossi ML. Prevalence of temporomandibular disorders in an adult Brazilian community population using the research diagnostic criteria (axes I and II) for temporomandibular disorders (the maringá study). Int J Prosthodont. (2015) 28(6):600–9. doi: 10.11607/ijp.4026
20. Carlsson GE, Ekbäck G, Johansson A, Ordell S, Unell L. Is there a trend of decreasing prevalence of TMD-related symptoms with ageing among the elderly? Acta Odontol Scand. (2014) 72(8):714–20. doi: 10.3109/00016357.2014.898787
21. Maixner W, Diatchenko L, Dubner R, Fillingim RB, Greenspan JD, Knott C, et al. Orofacial pain prospective evaluation and risk assessment study—the OPPERA study. J Pain. (2011) 12(11):T4–T11.e2. doi: 10.1016/j.jpain.2011.08.002
22. Häggman-Henrikson B, Liv P, Ilgunas A, Visscher CM, Lobbezoo F, Durham J, et al. Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain. (2020) 161(8):1768–75. doi: 10.1097/j.pain.0000000000001872
23. Slade GD, Fillingim RB, Sanders AE, Bair E, Greenspan JD, Ohrbach R, et al. Summary of findings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder: implications and future directions. J Pain. (2013) 14(12 Suppl):T116–24. doi: 10.1016/j.jpain.2013.09.010
24. Suvinen TI, Reade PC, Kemppainen P, Könönen M, Dworkin SF. Review of aetiological concepts of temporomandibular pain disorders: towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur J Pain. (2005) 9(6):613–33. doi: 10.1016/j.ejpain.2005.01.012
25. Macfarlane TV, Glenny AM, Worthington HV. Systematic review of population-based epidemiological studies of oro-facial pain. J Dent. (2001) 29(7):451–67. doi: 10.1016/S0300-5712(01)00041-0
26. List T, Jensen RH. Temporomandibular disorders: old ideas and new concepts. Cephalalgia. (2017) 37(7):692–704. doi: 10.1177/0333102416686302
27. Viñals Narváez AC, Sánchez-Sánchez T, García-González M, Ardizone García I, Cid-Verdejo R, Sánchez Romero EA, et al. Psychological and behavioral factors involved in temporomandibular myalgia and migraine: common but differentiated profiles. Int J Environ Res Public Health. (2023) 20(2):1545. doi: 10.3390/ijerph20021545
28. Ananthan S, Benoliel R. Chronic orofacial pain. J Neural Transm. (2020) 127(4):575–88. doi: 10.1007/s00702-020-02157-3
29. Carlson CR, Reid KI, Curran SL, Studts J, Okeson JP, Falace D, et al. Psychological and physiological parameters of masticatory muscle pain. Pain. (1998) 76(3):297–307. doi: 10.1016/S0304-3959(98)00063-3
30. Sarlani E, Greenspan JD. Evidence for generalized hyperalgesia in temporomandibular disorders patients. Pain. (2003) 102(3):221–6. doi: 10.1016/S0304-3959(03)00095-2
31. Von Korff M, Resche LL, Dworkin SF. First onset of common pain symptoms: a prospective study of depression as a risk factor. Pain. (1993) 55(2):251–8. doi: 10.1016/0304-3959(93)90154-H
32. Ohrbach R, Bair E, Fillingim RB, Gonzalez Y, Gordon SM, Lim PF, et al. Clinical orofacial characteristics associated with risk of first-onset TMD: the OPPERA prospective cohort study. J Pain. (2013) 14(12 Suppl):T33–50. doi: 10.1016/j.jpain.2013.07.018
33. Sabsoob O, Elsaraj SM, Gornitsky M, Laszlo E, Fricton JR, Schiffman EL, et al. Acute and chronic temporomandibular disorder pain: a critical review of differentiating factors and predictors of acute to chronic pain transition. J Oral Rehabil. (2022) 49(3):362–72. doi: 10.1111/joor.13283
34. Cao Y, Yap AU, Lei J, Zhang MJ, Fu KY. Subtypes of acute and chronic temporomandibular disorders: their relation to psychological and sleep impairments. Oral Dis. (2021) 27(6):1498–506. doi: 10.1111/odi.13692
35. Meloto CB, Slade GD, Lichtenwalter RN, Bair E, Rathnayaka N, Diatchenko L, et al. Clinical predictors of persistent temporomandibular disorder in people with first-onset temporomandibular disorder: a prospective case-control study. J Am Dent Assoc. (2019) 150(7):572–81 e10. doi: 10.1016/j.adaj.2019.03.023
36. Bair E, Gaynor S, Slade GD, Ohrbach R, Fillingim RB, Greenspan JD, et al. Identification of clusters of individuals relevant to temporomandibular disorders and other chronic pain conditions: the OPPERA study. Pain. (2016) 157(6):1266–78. doi: 10.1097/j.pain.0000000000000518
37. Itz CJ, Geurts JW, van Kleef M, Nelemans P. Clinical course of non-specific low back pain: a systematic review of prospective cohort studies set in primary care. Eur J Pain. (2013) 17(1):5–15. doi: 10.1002/j.1532-2149.2012.00170.x
38. Juwara L, Arora N, Gornitsky M, Saha-Chaudhuri P, Velly AM. Identifying predictive factors for neuropathic pain after breast cancer surgery using machine learning. Int J Med Inform. (2020) 141:104170. doi: 10.1016/j.ijmedinf.2020.104170
39. Botros J, Gornitsky M, Samim F, der Khatchadourian Z, Velly AM. Back and neck pain: a comparison between acute and chronic pain-related temporomandibular disorders. Can J Pain. (2022) 6(1):112–20. doi: 10.1080/24740527.2022.2067032
40. Biomarkers Definitions Working G. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. (2001) 69(3):89–95. doi: 10.1067/mcp.2001.113989
41. Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. (2019) 160(1):19–27. doi: 10.1097/j.pain.0000000000001384
42. Kosek E, Cohen M, Baron R, Gebhart GF, Mico JA, Rice ASC, et al. Do we need a third mechanistic descriptor for chronic pain states? Pain. (2016) 157(7):1382–6. doi: 10.1097/j.pain.0000000000000507
43. Kosek E, Clauw D, Nijs J, Baron R, Gilron I, Harris RE, et al. Chronic nociplastic pain affecting the musculoskeletal system: clinical criteria and grading system. Pain. (2021) 162(11):2629–34. doi: 10.1097/j.pain.0000000000002324
44. Pollard LC, Ibrahim F, Choy EH, Scott DL. Pain thresholds in rheumatoid arthritis: the effect of tender point counts and disease duration. J Rheumatol. (2012) 39(1):28–31. doi: 10.3899/jrheum.110668
45. Okeson JP. The classification of orofacial pains. Oral Maxillofac Surg Clin North Am. (2008) 20(2):133–44. doi: 10.1016/j.coms.2007.12.009
46. Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. (1992) 6(4):301–55.1298767
47. Look JO, Schiffman EL, Truelove EL, Ahmad M. Reliability and validity of axis I of the research diagnostic criteria for temporomandibular disorders (RDC/TMD) with proposed revisions. J Oral Rehabil. (2010) 37(10):744–59. doi: 10.1111/j.1365-2842.2010.02121.x
48. Truelove E, Pan W, Look JO, Mancl LA, Ohrbach RK, Velly AM, et al. The research diagnostic criteria for temporomandibular disorders. III: validity of axis I diagnoses. J Orofac Pain. (2010) 24(1):35–47.20213030
49. Peck CC, Goulet JP, Lobbezoo F, Schiffman EL, Alstergren P, Anderson GC, et al. Expanding the taxonomy of the diagnostic criteria for temporomandibular disorders. J Oral Rehabil. (2014) 41(1):2–23. doi: 10.1111/joor.12132
50. de Leeuw R, Klasser G. Orofacial pain: Guidelines for assessment, diagnosis, and management, 6th ed. Chicago (IL), USA: Quintessence Publiching Co., Inc (2018).
51. International Classification of Diseases, Eleventh Revision (ICD-11), World Health Organization (2019/2021). Available online at: Available at: https://icd.who.int/browse11
52. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. (2018) 38(1):1–211. doi: 10.1177/0333102417738202
53. International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia. (2020) 40(2):129–221. doi: 10.1177/0333102419893823
54. Rongo R, Ekberg E, Nilsson IM, Al-Khotani A, Alstergren P, Conti PCR, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for children and adolescents: an international Delphi study-part 1-development of axis I. J Oral Rehabil. (2021) 48(7):836–45. doi: 10.1111/joor.13175
55. Osterlund C, Berglund H, Akerman M, Nilsson E, Petersson H, Lam J, et al. Diagnostic criteria for temporomandibular disorders: diagnostic accuracy for general dentistry procedure without mandatory commands regarding myalgia, arthralgia and headache attributed to temporomandibular disorder. J Oral Rehabil. (2018) 45(7):497–503. doi: 10.1111/joor.12643
56. Gonzalez YM, Schiffman E, Gordon SM, Seago B, Truelove EL, Slade G, et al. Development of a brief and effective temporomandibular disorder pain screening questionnaire: reliability and validity. J Am Dent Assoc. (2011) 142(10):1183–91. doi: 10.14219/jada.archive.2011.0088
57. Lovgren A, Visscher CM, Haggman-Henrikson B, Lobbezoo F, Marklund S, Wanman A. Validity of three screening questions (3Q/TMD) in relation to the DC/TMD. J Oral Rehabil. (2016) 43(10):729–36. doi: 10.1111/joor.12428
58. Villemure C, Bushnell CM. Cognitive modulation of pain: how do attention and emotion influence pain processing? Pain. (2002) 95(3):195–9. doi: 10.1016/S0304-3959(02)00007-6
59. Kuttila M, Niemi PM, Kuttila S, Alanen P, Le Bell Y. TMD Treatment need in relation to age, gender, stress, and diagnostic subgroup. J Orofac Pain. (1998) 12(1):67–74.9656901
60. Gil-Martínez A, Paris-Alemany A, López-de-Uralde-Villanueva I, La Touche R. Management of pain in patients with temporomandibular disorder (TMD): challenges and solutions. J Pain Res. (2018) 11(null):571–87. doi: 10.2147/JPR.S127950
61. Clark MV, Donnell CC, Durham J, Balasubramaniam R. Pharmacological management of orofacial pain—a clinician’s guide. Oral Surg. (2020) 13(4):422–49. doi: 10.1111/ors.12542
62. Al-Moraissi EA, Conti PCR, Alyahya A, Alkebsi K, Elsharkawy A, Christidis N. The hierarchy of different treatments for myogenous temporomandibular disorders: a systematic review and network meta-analysis of randomized clinical trials. Oral Maxillofac Surg. (2021) 21:21. doi: 10.1007/s10006-021-01009-y
63. Al-Moraissi EA, Alradom J, Aladashi O, Goddard G, Christidis N. Needling therapies in the management of myofascial pain of the masticatory muscles: a network meta-analysis of randomised clinical trials. J Oral Rehabil. (2020) 47(7):910–22. doi: 10.1111/joor.12960
64. Romero-Reyes M, Arman S, Teruel A, Kumar S, Hawkins J, Akerman S. Pharmacological management of orofacial pain. Drugs. (2023) 83(14):1269–92. doi: 10.1007/s40265-023-01927-z
65. Penlington C, Bowes C, Taylor G, Otemade AA, Waterhouse P, Durham J, et al. Psychological therapies for temporomandibular disorders (TMDs). Cochrane Database Syst Rev. (2022) 8(8):CD013515. doi: 10.1002/14651858.CD013515.pub2
66. Long DM, Hagfors N. Electrical stimulation in the nervous system: the current status of electrical stimulation of the nervous system for relief of pain. Pain. (1975) 1(2):109–23. doi: 10.1016/0304-3959(75)90096-2
67. Wig AD, Aaron LA, Turner JA, Huggins KH, Truelove E. Short-term clinical outcomes and patient compliance with temporomandibular disorder treatment recommendations. J Orofac Pain. (2004) 18(3):203–13.15508999
68. Swedish-Academy-of-Temporomandibular-Disorders. Treatment Protocol for General Dentists for Patients with Orofacial Pain and Jaw Dysfunction (2021). (Available online at: Available at: https://mau.se/om-oss/fakulteter-och-institutioner/odontologiska-fakulteten/odontologiska-fakulteten/dctmd/#accordion-93126
69. The-Swedish-National-Board-of-Health-and-Welfare. The Swedish National Guidelines in Dentistry (2022). (Available online at: Available at: https://www.socialstyrelsen.se/en/clinical-practise-guidelines-and-regulations/regulations-and-guidelines/national-guidelines/
70. de Freitas RF, Ferreira MA, Barbosa GA, Calderon PS. Counselling and self-management therapies for temporomandibular disorders: a systematic review. J Oral Rehabil. (2013) 40(11):864–74. doi: 10.1111/joor.12098
71. Dworkin SF, Huggins KH, Wilson L, Mancl L, Turner J, Massoth D, et al. A randomized clinical trial using research diagnostic criteria for temporomandibular disorders-axis II to target clinic cases for a tailored self-care TMD treatment program. J Orofac Pain. (2002) 16(1):48–63.11889659
72. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. (2020) 45(1):205–16. doi: 10.1038/s41386-019-0439-z
73. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. (2013) 14(12):1539–52. doi: 10.1016/j.jpain.2013.08.007
74. Kavanaugh J, Hardison ME, Rogers HH, White C, Gross J. Assessing the impact of a shinrin-yoku (forest bathing) intervention on physician/healthcare professional burnout: a randomized, controlled trial. Int J Environ Res Public Health. (2022) 19(21):14505. doi: 10.3390/ijerph192114505
75. Ohrbach R, Sharma S. Behavioral therapy for temporomandibular disorders. Front Oral Maxillofacial Med. (2021) 3:37. doi: 10.21037/fomm-20-65
76. Ohrbach R, Fillingim RB, Mulkey F, Gonzalez Y, Gordon S, Gremillion H, et al. Clinical findings and pain symptoms as potential risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J Pain. (2011) 12(11 Suppl):T27–45. doi: 10.1016/j.jpain.2011.09.001
77. Florjanski W, Malysa A, Orzeszek S, Smardz J, Olchowy A, Paradowska-Stolarz A, et al. Evaluation of biofeedback usefulness in masticatory muscle activity management-A systematic review. J Clin Med. (2019) 8(6):766. doi: 10.3390/jcm8060766
79. Al-Moraissi EA, Farea R, Qasem KA, Al-Wadeai MS, Al-Sabahi ME, Al-Iryani GM. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: network meta-analysis of randomized controlled trials. Int J Oral Maxillofac Surg. (2020) 49(8):1042–56. doi: 10.1016/j.ijom.2020.01.004
80. Alkhutari AS, Alyahya A, Conti PCR, Christidis N, Al-Moraissi EA. Is the therapeutic effect of occlusal stabilization appliances more than just placebo effect in the management of painful temporomandibular disorders? A network meta-analysis of randomized clinical trials. J Prosthet Dent. (2021) 126(1):24–32. doi: 10.1016/j.prosdent.2020.08.015
81. Forssell H, Kalso E, Koskela P, Vehmanen R, Puukka P, Alanen P. Occlusal treatments in temporomandibular disorders: a qualitative systematic review of randomized controlled trials. Pain. (1999) 83(3):549–60. doi: 10.1016/S0304-3959(99)00160-8
82. Ekberg EC, Vallon D, Nilner M. Occlusal appliance therapy in patients with temporomandibular disorders. A double-blind controlled study in a short-term perspective. Acta Odontol Scand. (1998) 56(2):122–8. doi: 10.1080/00016359850136102
83. Kreiner M, Betancor E, Clark GT. Occlusal stabilization appliances. Evidence of their efficacy. J Am Dent Assoc. (2001) 132(6):770–7. doi: 10.14219/jada.archive.2001.0274
84. Fricton J. Current evidence providing clarity in management of temporomandibular disorders: summary of a systematic review of randomized clinical trials for intra-oral appliances and occlusal therapies. J Evid Based Dent Pract. (2006) 6(1):48–52. doi: 10.1016/j.jebdp.2005.12.020
85. Manfredini D. Occlusal equilibration for the management of temporomandibular disorders. Oral Maxillofac Surg Clin North Am. (2018) 30(3):257–64. doi: 10.1016/j.coms.2018.04.002
86. Häggman-Henrikson B, Wiesinger B, Wänman A. The effect of supervised exercise on localized TMD pain and TMD pain associated with generalized pain. Acta Odontol Scand. (2018) 76(1):6–12. doi: 10.1080/00016357.2017.1373304
87. Shimada A, Ishigaki S, Matsuka Y, Komiyama O, Torisu T, Oono Y, et al. Effects of exercise therapy on painful temporomandibular disorders. J Oral Rehabil. (2019) 46(5):475–81. doi: 10.1111/joor.12770
88. Truelove E, Huggins KH, Mancl L, Dworkin SF. The efficacy of traditional, low-cost and nonsplint therapies for temporomandibular disorder: a randomized controlled trial. J Am Dent Assoc. (2006) 137(8):1099–107. doi: 10.14219/jada.archive.2006.0348
89. Makino I, Arai YC, Aono S, Hayashi K, Morimoto A, Nishihara M, et al. The effects of exercise therapy for the improvement of jaw movement and psychological intervention to reduce parafunctional activities on chronic pain in the craniocervical region. Pain Pract. (2014) 14(5):413–8. doi: 10.1111/papr.12075
90. Contento VS, Dalton BH, Power GA. The inhibitory tendon-evoked reflex is increased in the torque-enhanced state following active lengthening compared to a purely isometric contraction. Brain Sci. (2019) 10(1):13. doi: 10.3390/brainsci10010013
91. Abbadie C, Besson JM. Chronic treatments with aspirin or acetaminophen reduce both the development of polyarthritis and Fos-like immunoreactivity in rat lumbar spinal cord. Pain. (1994) 57(1):45–54. doi: 10.1016/0304-3959(94)90106-6
92. Ouanounou A, Goldberg M, Haas DA. Pharmacotherapy in temporomandibular disorders: a review. J Can Dent Assoc. (2017) 83(7):1–8.
93. Andre A, Kang J, Dym H. Pharmacologic treatment for temporomandibular and temporomandibular joint disorders. Oral Maxillofac Surg Clin North Am. (2022) 34(1):49–59. doi: 10.1016/j.coms.2021.08.001
94. Smith HS. Potential analgesic mechanisms of acetaminophen. Pain Physician. (2009) 12(1):269–80. doi: 10.36076/ppj.2009/12/269
95. Zeilhofer HU, Brune K. Analgesic strategies beyond the inhibition of cyclooxygenases. Trends Pharmacol Sci. (2006) 27(9):467–74. doi: 10.1016/j.tips.2006.07.007
96. Ouanounou A, Haas DA. Pharmacotherapy for the elderly dental patient. J Can Dent Assoc. (2015) 80:f18.26679331
97. Häggman-Henrikson B, Alstergren P, Davidson T, Högestätt ED, Östlund P, Tranaeus S, et al. Pharmacological treatment of oro-facial pain—health technology assessment including a systematic review with network meta-analysis. J Oral Rehabil. (2017) 44(10):800–26. doi: 10.1111/joor.12539
98. Nance PW, Sheremata WA, Lynch SG, Vollmer T, Hudson S, Francis GS, et al. Relationship of the antispasticity effect of tizanidine to plasma concentration in patients with multiple sclerosis. Arch Neurol. (1997) 54(6):731–6. doi: 10.1001/archneur.1997.00550180049011
99. Newman PM, Nogues M, Newman PK, Weightman D, Hudgson P. Tizanidine in the treatment of spasticity. Eur J Clin Pharmacol. (1982) 23(1):31–5. doi: 10.1007/BF01061374
100. Onghena P, Van Houdenhove B. Antidepressant-induced analgesia in chronic non-malignant pain: a meta-analysis of 39 placebo-controlled studies. Pain. (1992) 49(2):205–19. doi: 10.1016/0304-3959(92)90144-Z
101. Birkinshaw H, Friedrich CM, Cole P, Eccleston C, Serfaty M, Stewart G, et al. Antidepressants for pain management in adults with chronic pain: a network meta-analysis. Cochrane Database Syst Rev. (2023) 5(5):CD014682. doi: 10.1002/14651858.CD014682.pub2
102. Cascos-Romero J, Vazquez-Delgado E, Vazquez-Rodriguez E, Gay-Escoda C. The use of tricyclic antidepressants in the treatment of temporomandibular joint disorders: systematic review of the literature of the last 20 years. Med Oral Patol Oral Cir Bucal. (2009) 14(1):E3–7.19114953
103. Haas DA. Pharmacologic considerations in the management of temporomandibular disorders. J Can Dent Assoc. (1995) 61(2):105–9.7600411
104. Hersh EV, Balasubramaniam R, Pinto A. Pharmacologic management of temporomandibular disorders. Oral Maxillofac Surg Clin North Am. (2008) 20(2):197–210. doi: 10.1016/j.coms.2007.12.005
105. Kreisberg MK. Tricyclic antidepressants: analgesic effect and indications in orofacial pain. J Craniomandib Disord. (1988) 2(4):171–7.3076592
106. Delcanho R, Val M, Guarda Nardini L, Manfredini D. Botulinum toxin for treating temporomandibular disorders: what is the evidence? J Oral Facial Pain Headache. (2022) 36(1):6–20. doi: 10.11607/ofph.3023
107. Machado D, Martimbianco ALC, Bussadori SK, Pacheco RL, Riera R, Santos EM. Botulinum toxin type a for painful temporomandibular disorders: systematic review and meta-analysis. J Pain. (2020) 21(3-4):281–93. doi: 10.1016/j.jpain.2019.08.011
108. Feng J, Luo M, Ma J, Tian Y, Han X, Bai D. The treatment modalities of masticatory muscle pain a network meta-analysis. Medicine (Baltimore). (2019) 98(46):e17934. doi: 10.1097/MD.0000000000017934
109. De la Torre Canales G, Alvarez-Pinzon N, Muñoz-Lora VRM, Vieira Peroni L, Farias Gomes A, Sánchez-Ayala A, et al. Efficacy and safety of botulinum toxin type A on persistent myofascial pain: a randomized clinical trial. Toxins (Basel). (2020) 12(6):395. doi: 10.3390/toxins12060395
110. Montes-Carmona JF, Gonzalez-Perez LM, Infante-Cossio P. Treatment of localized and referred masticatory myofascial pain with botulinum toxin injection. Toxins (Basel). (2020) 13(1):6. doi: 10.3390/toxins13010006
111. Vartanian AJ, Dayan SH. Complications of botulinum toxin A use in facial rejuvenation. Facial Plast Surg Clin North Am. (2005) 13(1):1–10. doi: 10.1016/j.fsc.2004.04.008
112. Balanta-Melo J, Toro-Ibacache V, Kupczik K, Buvinic S. Mandibular bone loss after masticatory muscles intervention with botulinum toxin: an approach from basic research to clinical findings. Toxins (Basel). (2019) 11(2):84. doi: 10.3390/toxins11020084
113. Raphael KG, Janal MN, Tadinada A, Santiago V, Sirois DA, Lurie AG. Effect of multiple injections of botulinum toxin into painful masticatory muscles on bone density in the temporomandibular complex. J Oral Rehabil. (2020) 47(11):1319–29. doi: 10.1111/joor.13087
114. Hong SW, Kang J-H. Decreased mandibular cortical bone quality after botulinum toxin injections in masticatory muscles in female adults. Sci Rep. (2020) 10(1):3623. doi: 10.1038/s41598-020-60554-w
115. Dunning J, Butts R, Mourad F, Young I, Flannagan S, Perreault T. Dry needling: a literature review with implications for clinical practice guidelines. Phys Ther Rev. (2014) 19(4):252–65. doi: 10.1179/108331913X13844245102034
116. Lewit K. The needle effect in the relief of myofascial pain. Pain. (1979) 6(1):83–90. doi: 10.1016/0304-3959(79)90142-8
117. Zhou W, Benharash P. Effects and mechanisms of acupuncture based on the principle of meridians. J Acupunct Meridian Stud. (2014) 7(4):190–3. doi: 10.1016/j.jams.2014.02.007
118. Lee H, Lee JY, Kim YJ, Kim S, Yin C, Khil JH, et al. Acupuncture for symptom management of rheumatoid arthritis: a pilot study. Clin Rheumatol. (2008) 27(5):641–5. doi: 10.1007/s10067-007-0819-3
119. Yang Y, Wang LP, Zhang L, Wang LC, Wei J, Li JJ, et al. Factors contributing to de qi in acupuncture randomized clinical trials. Evid Based Complement Alternat Med. (2013) 2013:329392. doi: 10.1155/2013/329392
120. Kalichman L, Vulfsons S. Dry needling in the management of musculoskeletal pain. J Am Board Family Med. (2010) 23(5):640–6. doi: 10.3122/jabfm.2010.05.090296
121. Berger AA, Liu Y, Mosel L, Champagne KA, Ruoff MT, Cornett EM, et al. Efficacy of dry needling and acupuncture in the treatment of neck pain. Anesth Pain Med. (2021) 11(2):e113627. doi: 10.5812/aapm.113627
122. Al-Moraissi EA, Goddard G, Christidis N. Are acupuncture and dry needling effective in the management of masticatory muscle pain: a network meta-analysis of randomised clinical trials. J Oral Rehabil. (2022) 50(1):87–97. doi: 10.1111/joor.13382
123. Rodrigues D, Siriani AO, Bérzin F. Effect of conventional TENS on pain and electromyographic activity of masticatory muscles in TMD patients. Braz Oral Res. (2004) 18(4):290–5. doi: 10.1590/S1806-83242004000400003
124. Fertout A, Manière-Ezvan A, Lupi L, Ehrmann E. Management of temporomandibular disorders with transcutaneous electrical nerve stimulation: a systematic review. Cranio. (2022) 40(3):217–28. doi: 10.1080/08869634.2019.1687986
125. Smith SB, Maixner DW, Greenspan JD, Dubner R, Fillingim RB, Ohrbach R, et al. Potential genetic risk factors for chronic TMD: genetic associations from the OPPERA case control study. J Pain. (2011) 12(11 Suppl):T92–101. doi: 10.1016/j.jpain.2011.08.005
126. Smith SB, Mir E, Bair E, Slade GD, Dubner R, Fillingim RB, et al. Genetic variants associated with development of TMD and its intermediate phenotypes: the genetic architecture of TMD in the OPPERA prospective cohort study. J Pain. (2013) 14(12 Suppl):T91–101.e1-3. doi: 10.1016/j.jpain.2013.09.004
Keywords: diagnosis, epidemiology, etiology, masticatory muscle, myalgia, treatment
Citation: Barjandi G, Svedenlöf J, Jasim H, Collin M, Hedenberg-Magnusson B, Christidis N and Ernberg M (2024) Clinical aspects of mastication myalgia—an overview. Front. Pain Res. 4:1306475. doi: 10.3389/fpain.2023.1306475
Received: 3 October 2023; Accepted: 26 December 2023;
Published: 9 January 2024.
Edited by:
Frederick Freitag, Medical College of Wisconsin, United StatesReviewed by:
Jie Lei, Peking University Hospital of Stomatology, ChinaInna E. Tchivileva, University of North Carolina at Chapel Hill, United States
© 2024 Barjandi, Svedenlöf, Jasim, Collin, Hedenberg-Magnusson, Christidis and Ernberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johanna Svedenlöf am9oYW5uYS5zdmVkZW5sb2ZAa2kuc2U=
†These authors share first authorship