 Björn Gerdle
Björn Gerdle Elena Dragioti
Elena Dragioti Marcelo Rivano Fischer2,3
Marcelo Rivano Fischer2,3 Huan-Ji Dong
Huan-Ji Dong- 1Pain and Rehabilitation Centre, Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
- 2Department of Neurosurgery and Pain Rehabilitation, Skåne University Hospital, Lund, Sweden
- 3Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden
Background: Sleep problems (insomnia) and chronic pain are associated. Chronic pain and insomnia/insufficient sleep quality share similar symptoms and features. Although they have a bidirectional relationship, more research is needed to understand how they interact via mediators and how moderators influence this relationship.
Aims: In this large clinical registry-based cohort study (N = 6,497), we investigate important mediators between insomnia and pain intensity in a cross-sectional sample of chronic pain patients using advanced path analysis. In addition, we investigate whether some background variables were moderators of the identified important paths or not and the correlation patterns between insomnia and pain intensity in relation to the mediators.
Methods: This study includes a cohort of adult patients with chronic non-cancer pain from the Swedish Quality Registry for Pain Rehabilitation (SQRP) with data on patient-reported outcome measures (PROMs) (2008–2016). The PROMs cover the background, pain aspects, psychological distress, pain-related cognitions, activity/participation, and health-related quality of life variables of the patients. Partial least squares structural equation modeling was used to explore the direct and indirect (via mediators) relationships between insomnia and pain intensity at baseline.
Results: In this cohort study, insomnia was prevalent at 62.3%, and both direct and indirect mediating paths were present for the insomnia–pain intensity relationship. All of the mediating effects combined were weaker than the direct effect between insomnia and pain intensity. The mediating effects via catastrophizing and acceptance showed the strongest and equal mediating paths, and mediating effects via fear avoidance were the second strongest. Insomnia showed stronger direct significant correlations with psychological distress, catastrophizing, and acceptance compared with those of pain intensity. Sex, age, education level, spatial extent of pain, or body mass index did not moderate the mediating paths.
Discussion and conclusion: This study confirms the existence of significant direct and mediating paths between reported insomnia and pain intensity. Future studies should focus on illuminating how sleep interventions influence pain intensity and other important key factors that contribute to the distress of chronic pain patients.
1. Introduction
Approximately 20% of the European adult population suffers from chronic pain of at least moderate intensity (1). Chronic pain patients frequently report comorbidities, increased sick leave, and low quality of health (2). These common comorbidities include obesity, insomnia, cardiovascular conditions, and anxiety and depressive symptoms (2, 3). Insomnia, the most prevalent sleep disorder, is estimated to have a prevalence rate of 10%–15% in adults (4, 5). Insomnia/poor quality of sleep is associated with an increase in light sleep and a decrease in the deepest sleep stages (i.e., slow-wave sleep) (6, 7). Prevalence rates in cohorts of chronic pain patients differ considerably depending on the measures used. However, a recent systematic review (SR) of studies using the Insomnia Severity Index (ISI) reported a prevalence of 72.9% in chronic pain patients (8), indicating that the prevalence of insomnia is considerably higher in chronic pain conditions.
Several studies, including polysomnography studies, have reported cross-sectional and longitudinal associations between sleep problems/insomnia and chronic pain (6, 7, 9–15). Thus, poor sleep increases pain and pain affects sleep. Longitudinal studies reported that poor sleep is the factor with the strongest empirical support for its effect on chronic pain (14, 16, 17). Moreover, a large prospective study conducted over 11 years found that obesity, poor sleep, and chronic disease all predicted persistent chronic widespread pain (CWP), except for depression (15). In addition, the number of sleep-related complaints was found to be positively and substantially correlated with an increased risk of developing CWP, musculoskeletal pain, and pain-related disability (18). Thus, insomnia seems closely connected to the development of chronic pain.
Chronic pain and insomnia/insufficient sleep quality share similar symptoms and features, including age (1, 19), obesity (20, 21), female sex (1, 22), catastrophizing (23, 24, 25), low physical activity (PA) (26, 27), socioeconomic factors such as education (3, 22), and anxiety and depressive symptoms (28–32). In addition, the literature suggests a possible role of acceptance both for chronic pain and insomnia (33, 34). Hence, a link between sleep and pain is well established, but the mechanisms for their associations—for instance, the relative importance of direct associations and mediating factors—are less well understood, although polymodal influences of sleep on pain have been proposed. Impaired sleep is believed to have a negative influence on top-down pain control and sensitization and lower the capacity to adequately attend to or disengage from pain—i.e., a reduced allocation of attentional resources (35, 36). Other possible shared mechanisms for pain and insomnia and possibly mediating factors that are discussed include affect and mood, catastrophizing, endogenous pain modulation including activated hyperalgesic systems, mesolimbic dopaminergic pathways and serotonergic pathways, low-grade inflammatory substances and other endogenous substances [e.g., growth hormone (GH) and prolactin], alterations in autonomic balance, and a cyclic alternating pattern (6, 7, 37–39).
More research is needed to determine whether mediators are present between insomnia and chronic pain or not (40–42). A mediator, located between the independent and the dependent variable, can either increase or decrease the effect of the independent variable. A SR identified nine cross-sectional mediation studies focusing on the sleep–pain relationship (43). Although there was some evidence for the mediating roles of the psychological and physiological aspects of emotional and attentional processes, methodological limitations remained apparent (43). Furthermore, the studies included were generally small; only one study included more than 300 chronic pain patients. Hence, large cohort studies are required to investigate the mediators for the insomnia–pain intensity relationships in chronic pain patients. Although longitudinal studies of mediators are needed (43), cross-sectional studies are also important for understanding the clinical presentations of patients during assessment. Considering the available data from the Swedish Quality Registry for Pain Rehabilitation (SQRP) and the referred results from the literature, we found that it is possible to investigate the importance of the following five mediators, namely, catastrophizing, fear avoidance, physical activity, acceptance, and psychological distress, for insomnia–pain intensity relationship.
In addition, important moderators of direct and mediation paths between insomnia and pain aspects in chronic pain patients must also be identified. A moderator effect is present when a causal relationship between two variables changes due to a change in a third variable, which indicates cohort heterogeneity. Common examples of moderators are sex, age, and education level.
Cross-sectional studies are important for understanding the clinical presentations of patients. This cross-sectional study of chronic pain patients employs advanced path analysis to investigate mediators between insomnia and pain intensity using data from a large clinical registry-based cohort. In line with this, we investigate whether the five variables—sex, age, obesity, education level, and spatial extent of pain—are moderators of the identified paths or not and the correlation patterns between insomnia and pain intensity in relation to the mediators.
2. Subjects and methods
2.1. Subjects and the Swedish Quality Registry for Pain Rehabilitation
Chronic pain patients from most specialist departments in Sweden report patient-reported outcome measures (PROMs) to the SQRP (44). A cohort of adult patients (i.e., ≥18 years) who had chronic non-malignant pain and were registered in the SQRP between 2008 and 2016 was included. The pain conditions are generally complex, i.e., comorbidities are prevalent, prolonged sick leave, inadequate coping, and/or unimodal treatment failures. This clinical registry does not have strict inclusion and exclusion criteria. Patients with severe psychiatric morbidity, a history of drug and alcohol abuse, and conditions that do not allow physical exercise are excluded. Swedish guidelines, which have been approved by several authorities and professional organizations, recommend that interdisciplinary pain rehabilitation programs (IPRPs) is offered to chronic pain patients with complex clinical presentations, including insufficient coping strategies, and when monodisciplinary interventions have failed (45). Most primary care physicians refer patients to specialist care, and no exact figures are available regarding the number of patients managed within primary care with monodisciplinary pain interventions.
2.2. Ethics
This study was conducted in accordance with the Helsinki Declaration. The Ethical Review Board in Linköping (Dnr: 2015/108-31) approved the study. All included patients gave their written consent after written information about the study. We did not exactly know how many patients declined to participate in the SQRP. Overall estimations made by the steering group of the SQRP indicated that more than 90% of the patients referred to the specialist departments in Sweden choose to participate in the SQRP.
2.3. PROMs
The PROMs cover sociodemographic characteristics, pain, psychological variables, cognitions, participation factors, and quality of life facets. The patients completed the PROMs up to three times. This study used baseline data, and we only provided a brief description of the variables because they have been described in detail in previous studies (2, 46–48).
2.4. Background variables
The following aspects were used:
• Age (years).
• Sex.
• Education level (university education versus no university education).
• Country of birth (in versus outside of Europe).
• Number of days with pain.
• Number of painful areas (range: 1–36) [pain region index (PRI)] (2, 49).
• Body mass index (BMI, kg/m2) was determined. The World Health Organization (WHO) criteria were used for classification: <18.5 kg/m2 = underweight; 18.5–24.9 kg/m2 = normal; 25.0–29.9 kg/m2 = overweight; ≥30.0 kg/m2 = obese.
2.4.1. Path model analysis
Consistent with the recent SR, we investigated the mediation paths for the insomnia–pain intensity relationship (43). Throughout the text below, we capitalize the initial letter of latent variables (constructs)—e.g., Insomnia and Pain intensity. Five mediation paths were investigated, i.e., 1) Catastrophizing, 2) Fear avoidance, 3) Physical activity level, 4) Acceptance and 5) Psychological distress (Figure 1). The arrows in the figures and text (–>) express a hypothesized relationship in agreement with the referred SR (43).
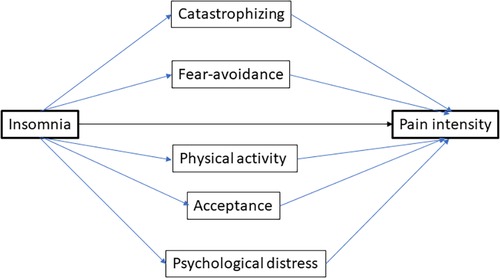
Figure 1. The theoretical model of the Insomnia–Pain intensity relationship together with five mediating paths. Latent variables (constructs) are shown together with the paths and directions. Note that a mediating path consists of two parts—i.e., from insomnia to the moderator (part 1) and from the mediator to pain intensity (part 2). The standardized coefficient β for the mediating path is obtained by multiplying the standard coefficients for the two parts of the mediating path.
2.5. Variables included in the path analyses
2.5.1. Pain intensity aspects
Three variables were used as indicators of Pain intensity, namely, (1) NRS-7d, average pain intensity over the past week using a numerical rating scale (0 = no pain and 10 = worst possible pain); (2) MPI-pain severity, pain severity scale (range: 0–6) of the multidimensional pain inventory (MPI) that indicates current and average pain intensity over the previous week; and (3) RAND36-bodily pain, the bodily pain subscale (range: 0–100) of the Short Form Health Survey (SF36), where a low value denotes a high intensity. Two identical versions of the SF36 exist; the license-free RAND36 was used.
2.5.2. Psychological distress aspects
Four variables were included as indicators: (1) HADS-tot, the two scales of the hospital anxiety and depression scale (HADS), which obtain symptoms of depression and anxiety (50, 51), were summed (range: 0–42) (52); (2) MPI-distress, this subscale of MPI captures the perceived feelings of patients concerning anxiety, depression, and irritation in the previous week (range: 0–6); (3) RAND36-mental health, based on items concerning mood, mental wellbeing, and behavioral/emotional control, with a range of 0–100, where a high value denotes good mental health; and (4) RAND36-role emotional, a subscale based on three items covering the role limitations related to emotional facets, with a range of 0–100, where a high value denotes a positive situation.
2.5.3. Fear avoidance aspects
The Tampa scale for kinesiophobia (TSK) (range: 17–68) was used because it is a validated scale used to indicate fear avoidance—i.e., fear of injury or (re)injury—in cohorts of chronic pain patients (53–57).
2.5.4. Acceptance aspects
To indicate acceptance, we used the validated Swedish version of the chronic pain acceptance questionnaire eight-item version (CPAQ8) (58). This questionnaire consists of two subscales: the activity engagement scale (CPAQ8-AE) (range: 0–24) and the pain willingness scale (CPAQ8-PW) (range: 0–24) (59). In the literature, the total sum of CPAQ8 is used as a general indicator of acceptance (CPAQ8-tot) (range: 0–48).
2.5.5. Catastrophizing aspects
The pain catastrophizing scale (PCS) was used to map catastrophizing aspects. It measures three dimensions of pain catastrophizing: rumination (PCS-rum) (range: 0–16); helplessness (PCS-help) (range: 0–24); and magnification (PCS-Magn) (range: 0–12) (60–62). These three scales represent different cognitive processes. Rumination is a tendency to have repetitive thoughts and dwell on pain and its impact. Helplessness indicates a reduced confidence in the ability to cope with the pain. Magnification is the tendency to overemphasize the seriousness or threat of pain.
2.5.6. Physical activity-level aspect
Physical activity level was assessed using a question about physical activity developed by the Swedish National Board of Health and Welfare. This ordinal item has the following wording: “How much time do you spend in a typical week doing physical exercise that leaves you out of breath, such as running, calisthenics or ball sports?” (63). The respondents chose one of the following: 0, <30, 30–60, 60–90, 90–120, or >120 min.
2.5.7. Insomnia aspects
The ISI captures the degree of insomnia symptoms (64). The scores of seven items (range: 0–4) are summed to produce the total ISI score (range: 0–28), which is divided into four categories; 0–7 = no insomnia; 8–14 = sub-threshold insomnia; 15–21 = moderate insomnia; and 22–28 = severe insomnia. A score of ≥15 was deemed as clinical insomnia.
2.5.8. Moderators
Sex/gender, education level, age, PRI, and BMI were investigated as possible moderators. All moderators were coded as binary/categorical variables. For education, the levels of university versus no university were applied. For age and PRI, the median values were used as cutoffs. For BMI, ≥30 kg/m2 (i.e., obesity) was used as a cutoff.
2.6. Statistics
The statistical packages IBM SPSS Statistics (version 28.0; IBM Corporation, Route 100 Somers, NY, USA) and SmartPLS version 4 (SmartPLS 4, Boenningstedt, SmartPLS. Retrieved from https://www.smartpls.com) were used. The mean values (±1 standard deviation; SD) of continuous variables and percentages (%) for categorical variables are presented. For the coefficients of the path analyses, mean ± SD, t-values, p-values, and 95% CI are reported. The retrieved data set included missing data (Table 1). Due to the low percentages of missing data, these were replaced with the mean values in the path analyses.
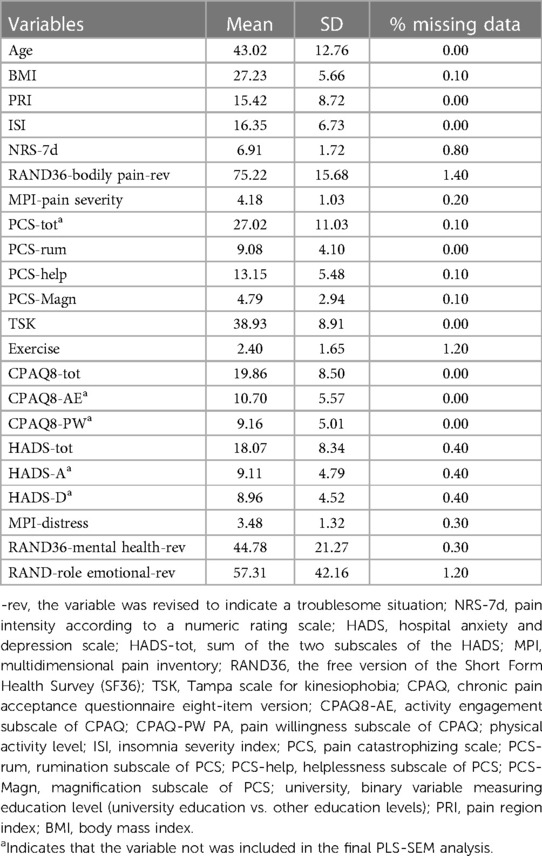
Table 1. Descriptive data for the included cohort of chronic pain patients: mean, 1 standard deviation (SD), and % missing data.
SmartPLS version 4 was used for the partial least squares structural equation modeling (PLS-SEM). This is a non-parametric method that models and estimates complex relationships among variables [see (65) for details including performance recommendations]. Generally, several indicators were used to define a latent variable (construct), and these needed to have the same direction (i.e., positively intercorrelated). Therefore, some indicators were reversed. RAND36-bodily pain can illustrate this. The scale has a possible range of 0–100, where a high value means low pain intensity and a low value means high pain intensity. To be consistent with other scales that capture the intensity of pain, i.e., NRS-7 days and MPI-pain severity where high values mean high pain intensity, the following calculation was made: 100—RAND36-bodily pain = RAND36-bodily pain-reversed. Using loadings, the outer model describes the relationships between the latent variable and their indicator variables. A reflective relationship was assumed for all latent variable–indicator relationships (not relevant for single-indicator latent variables). The inner model displayed the associations (paths) between the defined latent variables.
2.6.1. Evaluation of the outer model
A close association (indicator reliability) between the indicators and the latent variables was necessary. For each indicator, the loadings were used to determine if such an association is present or not. For indicator reliability, the absolute outer loadings of >0.708 (possible range: −1 to +1) were required (65). Indicators were excluded when absolute loadings ≤0.40. For indicators with loadings 0.40–0.708, the exclusion was made if internal consistency and convergent validity increased. The composite reliability coefficient (rhoc) (range: 0–1, with >0.50 required) was used to measure the internal consistency reliability. The average variance extracted (AVE) (range: 0–1, with >0.50 required) was used to measure the convergent validity. The discriminant validity was indicated using the heterotrait–monotrait ratio (HTMT) (values <0.90 required, preferably <0.85).
2.6.2. Evaluation of the inner model
To check the collinearity, we used the variance inflation factor (VIF); values <5 were required (65). To determine path coefficients (standardized; β) including specific indirect (mediating paths) effects, we applied the bootstrapping technique. The following specifications were used for the bootstrapping: complete bootstrapping, percentile bootstrap, 10,000 samples, and two-tailed (p = 0.05). The determination coefficient (R2) (range: 0–1) indicating explanatory power and the effect size (f2) were also determined. The latter was used to indicate clinical relevance: <0.02 = no measurable effect; 0.02–0.14 = small effect; 0.15–0.34 = medium effect; and ≥0.35 large effect (65, 66). The mean ± SD, t-values, p-values, and 95% CI of these coefficients were obtained from the bootstrapping.
For mediating effect sizes (i.e., clinical importance), we applied the following guidelines (66, 67): β, 0.01–0.08 = small effect; 0.09–0.24 = medium effect; and ≥0.25 = large effect.
When analyzing the possible effects of the five moderators, we focused on the direct effect of insomnia on pain intensity and the most important mediator paths. All moderators were transformed into binary variables (see above), and multigroup analysis (MGA) was conducted to analyze moderator effects (65).
While predictive power was not the focus of this study, we determined Q2predictive values (>0 indicated predictive relevance). The greater the Q2, the greater the predictability (68).
3. Results
3.1. The investigated cohort
The investigated cohort consisted of 6,497 patients, of whom 74.6% were women. One-third (31.2%) had the highest education level (i.e., university education). Descriptive data for the continuous variables are shown in Table 1. Moderate or severe insomnia was reported by 62.3% of the patients. The mean pain intensity according to NRS-7d was moderate to high (mean = 6.9, SD = 1.7). The proportion of obese patients was 27.4%. The proportions of definite cases of anxiety and depression (cutoff ≥ 11 for both subscales) according to HADS were 38.7% and 37.4%, respectively; in addition, 48.2% reported no signs of definite anxiety or depression.
3.2. PLS-SEM
3.2.1. Evaluation of the outer model
The included indicators in the subsequent PLS-SEM analyses and their latent variables are listed in Table 2. In the initial analysis indicator, reliability (i.e., outer loadings) was above the threshold (i.e., above 0.708) for all indicators except for one of the subscales of CPAQ8. Internal consistency reliability (rhoc) and convergent validity (AVE) increased and were both above the >0.50 level when the sum of the two CPAQ8 subscales (i.e., CPAQ8-tot) was used instead. Hence, Acceptance only had one indicator. The final model is shown in Figure 2, loadings in Table 3, and internal consistency reliability (rhoc: 0.906–0.925) and convergent validity (AVE: 0.755–0.772) in Supplementary Table S1. The discriminant validity was satisfactory (well below 0.85) for all relevant latent variable combinations according to HTMT (Supplementary Table S2). In conclusion, the final outer model was associated with good indicator reliability, internal consistency reliability, convergent validity, and discriminant validity.

Table 2. List of the latent variables (constructs) and their potential indicators together with the moderators included in the PLS-SEM analyses.
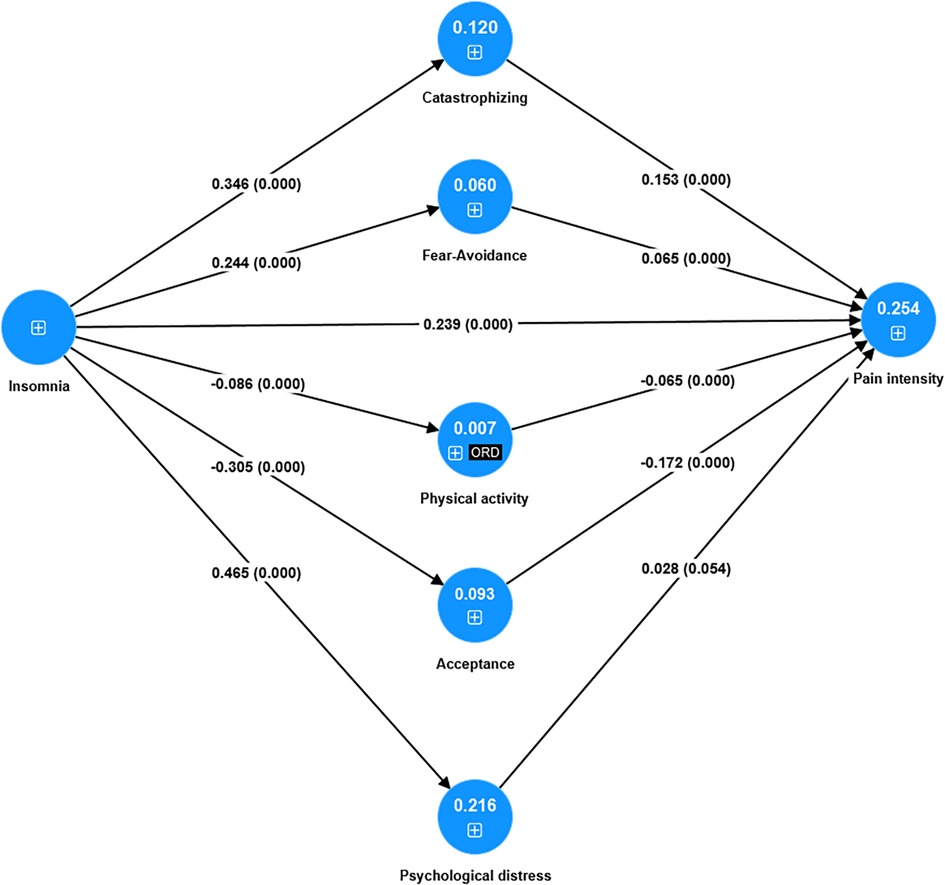
Figure 2. The final model analyzed using PLS-SEM (N = 6,497), that is, if insomnia affects pain intensity together with the five mediating paths. The blue circles show the latent variables (constructs). Loadings are not shown (see Table 3). For each path, the path coefficient β and the p-value are in parentheses (0.000 denotes p < 0.001). The explained variance (R2) is reported within the relevant latent variables. ORD = ordinal indicator for this latent variable.+sign indicates the existence of indicator/s for the latent variable.
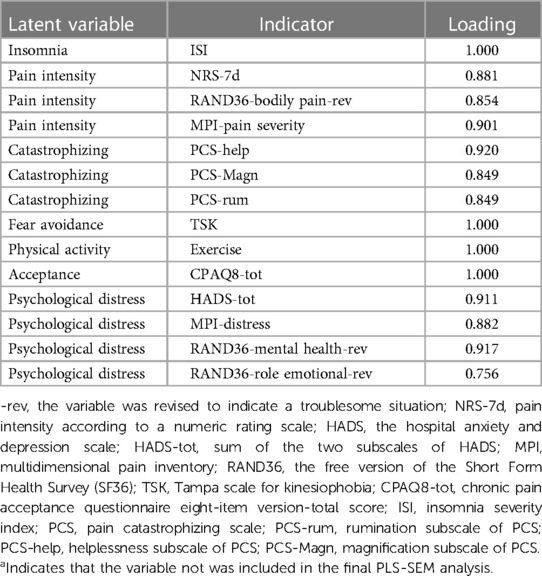
Table 3. Loadings of the indicators in the final model (cf. Figure 2). Note that when a latent variable has one indicator, the loading is 1.0.
3.2.2. Evaluation of the inner model
The VIF values were below 3.70 (1.00–3.66)—i.e., model collinearity was not an issue. For details, see Supplementary Table S3.
The path coefficients (β) are presented in Figure 2 and Table 4. All path coefficients (direct effects), except between Psychological distress and Pain intensity (p = 0.054), were highly significant (all other p-values <0.001).
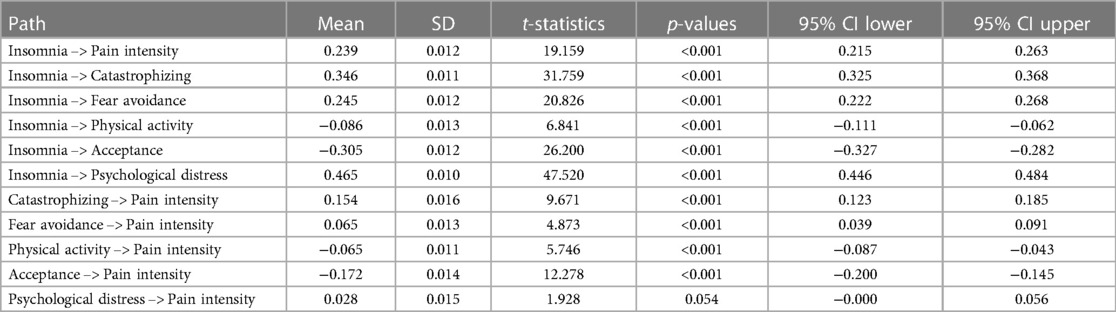
Table 4. Path coefficients (β) for the PLS-SEM model as shown in Figure 2. The mean ± SD, t-values, p-values, and 95% CI are shown.
The model in Figure 2 explained 25% of the variation in Pain intensity—i.e., R2 = 0.254 ± 0.010, p < 0.001. Insomnia showed the strongest absolute direct effects with Psychological distress (β = 0.465 ± 0.010, p < 0.001; medium effect size according to f2), Catastrophizing (β = 0.346 ± 0.011, p < 0.001; small effect size according to f2), Acceptance (β = −0.305 ± 0.012, p < 0.001, small effect size according to f2), and Fear avoidance (β = −0.245 ± 0.012, p < 0.001, small effect size according to f2). Hence, the relationships between Insomnia and Pain intensity (β = 0.239 ± 0.012, p < 0.001; small effect size according to f2) and between Insomnia and Physical activity (β = -0.086 ± 0.013, p < 0.001; non-significant effect size) were weaker according to the path coefficients. The coefficients of determination (R2) showed similar patterns as the path coefficients—i.e., Psychological distress (R2 = 0.216 ± 0.009), Catastrophizing (R2 = 0.120 ± 0.008), and Acceptance (R2 = 0.093 ± 0.007). For details, see Table 5. The effect sizes according to f2 are shown in Table 6. In conclusion, Insomnia showed significant direct associations with Pain intensity and the five mediators.

Table 5. The coefficients of determination (R2) for the relevant latent variables in the PLS-SEM model as depicted in Figure 2. The mean ± SD, t-values, p-values, and 95% CI are shown.

Table 6. Effects sizes according to f2 for the paths in the PLS-SEM model in Figure 2. The mean ± SD, t-values, p-values, and 95% CI are shown together with the clinical importance (see Methods for details concerning the categorization).

Table 7. Specific indirect effects (i.e., mediating effects β). The mean ± SD, t-values, p-values, and 95% CI are shown together with the clinical importance (see Methods for details concerning the categorization).
Generally, weaker but still significant direct associations (paths) were observed for the direct relationships between each mediator and Pain intensity (Table 4). However, the clinical importance was limited because the effect sizes were non-significant for four of the paths and small for the Acceptance–Pain intensity relationship.
3.2.3. Mediating effects (special indirect effects)
The total indirect effects (all mediating effects taken together) (β = 0.140 ± 0.007, p < 0.001; small effect size) were weaker than the direct path coefficient between Insomnia and Pain intensity (β = 0.239 ± 0.012, p < 0.001; medium effect size).
All of the mediating effects investigated except for Psychological distress (i.e., insomnia –> psychological distress –> pain intensity; p = 0.054) were significant (p-values < 0.001) (Table 6). The strongest and equal mediating effects were noted for Catastrophizing (β = 0.053 ± 0.006, p < 0.001; small effect size) and Acceptance (β = 0.053 ± 0.005, p < 0.001; small effect size), which were followed by Fear avoidance (0.016 ± 0.003, p < 0.001; small effect size) (Table 6). Also, the other significant mediating paths had small effect sizes except those involving Physical activity, which was associated with a non-significant effect size.
3.2.4. Predictive power
The model had predictive relevance according to the Q2predictive values (i.e., all > 0.00) (Supplementary Table S4).
3.2.5. Moderating effects
None of the mediating paths was significantly influenced by any of the five moderators, but other effects were found for four of the moderators.
3.2.5.1. Sex
No significant path coefficient differences were found between men and women.
3.2.5.2. Age
Age was associated with four significant group differences:
(1) Insomnia –> Pain intensity (group difference: p > 0.001; younger: 0.273 ± 0.017 p < 0.001 vs. older: 0.185 ± 0.018 p < 0.001);
(2) Insomnia –> Catastrophizing (group difference: p = 0.033; younger: 0.331 ± 0.016 p < 0.001 vs. older: 0.377 ± 0.015 p < 0.001);
(3) Insomnia –> Fear avoidance (group difference: p = 0.045; younger: 0.225 ± 0.017 p < 0.001 vs. older: 0.272 ± 0.016 p < 0.001); and
(4) Insomnia –> Psychological distress (group difference: p = 0.013; younger: 0.451 ± 0.014 p < 0.001 vs. older: 0.499 ± 0.013 p < 0.001).
3.2.5.3. Education level
One of the paths differed between those without and with university education (Group difference: p = 0.007)—i.e., Acceptance –> Pain intensity without university education (−0.149 ± 0.017 95% CI: −0.182 to −0.117) vs. Acceptance –> Pain intensity with university education (−0.230 ± 0.025, 95% CI: −0.279 to −0.181).
3.2.5.4. BMI
For BMI, the Insomnia –> Physical activity path was associated with a significant group difference (p = 0.004) (non-obese: −0.100 ± 0.015; p < 0.001; obese: −0.015 ± 0.025, p = 0.563). Thus, the path in the obese patients was not significant compared to the path in the non-obese patients.
3.2.5.5. Spatial extent of pain (PRI)
When comparing those with lower and higher PRI, we noted three significant group differences. Thus, more widespread pain in the body was associated with stronger effects for these three paths:
(1) Insomnia –> Pain intensity (group difference: p = 0.030; lower PRI: 0.199 ± 0.017 p < 0.001 vs. higher PRI: 0.253 ± 0.018 p < 0.001);
(2) Insomnia –> Catastrophizing (group difference: p = 0.003; lower PRI: 0.317 ± 0.016 p < 0.001 vs. higher PRI: 0.381 ± 0.015 p < 0.001); and
(3) Insomnia –> Fear avoidance (group difference: p = 0.013; lower PRI: 0.223 ± 0.017 p < 0.001 vs. higher PRI: 0.271 ± 0.017 p < 0.001).
4. Discussion
This large cohort study (N > 6,400) of patients with an insomnia prevalence of more than 60% (62.3%) produced several important results when the paths from insomnia to pain intensity were explored. Both direct and indirect (mediating) paths existed for the insomnia–pain intensity relationship. The mediating effects taken together were weaker than the direct effect between insomnia and pain intensity. Three of the five mediating paths were significant and associated with small effect sizes; the mediating effects via Catastrophizing and Acceptance showed the strongest and equal mediating paths, which were followed by those via Fear avoidance. Insomnia showed direct significant correlations with Psychological distress, Catastrophizing, Acceptance, and Fear avoidance stronger than those with Pain intensity. The five moderators did not significantly affect the mediating paths.
4.1. A high prevalence of insomnia
A high prevalence of insomnia (62.3%) was observed in this cohort of chronic pain patients, which was very similar to the figures reported from smaller SQRP cohorts—i.e., 65%–66% (9, 69). A recent SR reported an insomnia prevalence of 72.9% in chronic pain patients using ISI (8); however, a similar prevalence (75.3%) was noted for studies using the Pittsburgh Sleep Quality Index (PSQI). Hence, these figures are somewhat higher than the present prevalence, but this cohort is markedly larger than the studies included in the SR (ISI, total N = 2,578; PSQI, total N = 3,597) (8). Although the prevalence rates differ somewhat, most studies have indicated that insomnia probably affects most patients with chronic pain. In addition to pain, insomnia, poor sleep, and sleep deprivation are associated with conditions, such as cancer, type 2 diabetes, hypertension, heart disease, reduced cognitive functioning, somatic complaints, psychological distress, fatigue, and impaired quality of life (70–75). As such, sleep appears to be very important in the regulation of biological processes pivotal for health (71). The present cross-sectional study indeed confirmed a significant direct path between reported Insomnia and Pain intensity. Hence, it seems highly reasonable to include screening for sleep problems in the assessment of chronic pain patients (5).
4.2. Mediating effects
Insomnia was significantly related to Pain intensity (and vice versa) both directly and indirectly via mediating paths. The direct effect was stronger than the five mediating effects taken together. Together, the direct and indirect effects explained approximately 25% of the variation in the latent variable Pain intensity (R2 = 0.254) (Figure 2). Three of the five investigated mediating paths were significant and had small effect sizes. The strongest mediating effects were noted for Catastrophizing and Acceptance, which had equal mediating effects (both β = 0.053). Thus, some of the effects of Insomnia on Pain intensity were indirect and thus mediated by Catastrophizing and Acceptance. Fear avoidance was also a mediator, although its role (β = 0.016) was somewhat weaker than that of Catastrophizing and Acceptance. The mediating path via Psychological distress was not significant, and the mediating path via Physical activity was associated with a non-significant effect size.
Catastrophizing is the tendency to amplify negative cognitive and emotional processes related to pain. It is mainly due to environmental factors although heritability factors also exist (36%–37%) (76, 77). Catastrophizing negatively influences pain sensation and intensity (78, 79), depression and anxiety (79), and disability and quality of life (79) and may be a risk factor for chronic pain development (79, 80). Catastrophizing may be a transdiagnostic process that ties pain and depression/emotion together (81–83). It is associated with worse treatment outcomes, but it is modifiable and therefore a possible prevention and treatment target (84, 85). Several explanations exist for the role that catastrophizing might have in chronic pain as briefly summarized by Racine et al. (85). These explanations posit that catastrophizing not only reflects pain but also has a causal influence on pain and its consequences (85). Consistent with the above literature, we noted that both parts of the mediating path via Catastrophizing had positive β values—i.e., the path from Insomnia to Pain intensity increased pain intensity. Our results are in line with a small study of fibromyalgia patients who identified pain helplessness (cf. PCS-help) as a significant mediating path between insomnia and pain intensity (86).
Fear avoidance is a coping strategy that involves avoidance of physical and social activities of daily living due to fear of increased pain and/or fear of injury or reinjury (53). This is associated with risk of pain chronification, increased chronic pain intensity, and disability (87–89). Catastrophizing could be a key driver in the fear avoidance model of pain (79). Similarly, the mediating path via Fear avoidance was also positive (i.e., insomnia increased pain intensity via this path); however, the mediating path was weaker than the mediating paths via catastrophizing and acceptance. Even when these two mediating paths (i.e., via Fear avoidance and Catastrophizing) are combined, the effect size remains small. Several instruments are available for measuring fear avoidance (87), and TSK is one of those. Although these instruments have been extensively used, there are still some psychometric critiques (87). For example, TSK contains items concerning fear but only in the context of injury or reinjury (87), which may help explain the lower but still significant coefficient for this mediating path. A broader and more general measure of fear avoidance is desirable in future studies and may be associated with a more valid picture of its role in the insomnia–pain intensity relationship.
The mediating effect of Acceptance on the Insomnia–Pain intensity relationship was associated with lower pain intensity in contrast to the mediating result via catastrophizing (i.e., both parts of this mediating path had negative β values). Acceptance, a component of psychological flexibility, is the willingness to remain in contact with and to actively engage in unpleasant experiences despite chronic pain (90–92). Low acceptance has been perceived as an unproductive inner struggle with the pain experience, including attempts to avoid pain. Low acceptance is associated with chronic pain management problems and with suffering, depressive symptoms, avoidance, healthcare utilization, and poorer functioning (59, 93–97). Thus, patients reporting higher levels of acceptance may struggle less while trying to control and fall asleep and have fewer fears of being tired or exhausted during the day. Increasing evidence has emerged with regard to the effect of acceptance and commitment therapy (ACT) on primary and comorbid insomnia (98) and chronic pain conditions (99). Chronic pain conditions are associated with abnormal hyper-connectivity of brain networks associated with self-reflection (default mode, DMN), emotion (salience, SN), and cognitive control (frontal-parietal, FPN) (100). Mainly consistent with a few other studies, reductions within and between these networks were noted after ACT treatment (100).
Longitudinal studies indicated that depressive and/or anxiety symptoms mediated the effect between insomnia and pain symptoms (17). The mediating path via Psychological distress was not significant in this cross-sectional study. Other cross-sectional studies indicated that anxiety and/or depressive symptoms were positive mediators as summarized in the referred SR (43). In this context, more complex models have been called for (43). Our study is a parallel mediating study—i.e., the mediating latent variables competed against each other. Except for Physical activity, all mediating latent variables were intercorrelated according to a principal component analysis in this sample (data not shown). Although psychological distress aspects may be significant in a single mediation analysis, other psychological factors (e.g., catastrophizing, fear avoidance, and acceptance) may be more important in a parallel mediation analysis.
A reduced prevalence of insomnia was found in physically active individuals with chronic pain (37). However, although the mediating path via Physical activity level was significant, the importance from a clinical perspective was negligible. Our results with regard to physical activity were consistent with those of a longitudinal study of young adults in a population study (101).
4.3. Moderation aspects
Sex was not a moderator of the paths explored even though women report, for example, higher prevalence of chronic pain and widespread pain (102–104), greater pain severity (not consistent) (46, 48, 105–107), and higher prevalence of sleep problems/insomnia (108–110).
None of the moderators significantly affected the mediating paths considered in this study. However, for moderators other than sex, some of the direct effects of insomnia showed group differences, which may have clinical implications.
Age was a significant moderator of the direct effects between Insomnia and several of the latent variables. In older patients, three of the associations with Insomnia were stronger (Catastrophizing, Fear avoidance, and Psychological distress) and one weaker (Pain intensity). Thus, in older ages, insomnia will be more strongly tied to psychological distress and two negative coping aspects.
Education level not only reflects school background but also serves as a proxy for socioeconomic status, including work situation. The prevalence of chronic pain, severity of pain, and disability are inversely related to socioeconomic status (111–114). The only difference was found for the Acceptance–Pain intensity relationship: a stronger negative coefficient was noted for those with a university education. This moderating effect must be confirmed in other studies before making any conclusions as to whether the design of treatments needs to vary by education level.
Some studies reported that both pain and insomnia are related to obesity (20, 21), but the relationships between obesity/BMI and insomnia symptoms/disorders have been challenged in recent meta-analyses (37, 75, 115). The clinical importance of the fact that BMI significantly moderated the path from Insomnia to Physical activity remains unclear.
Positive associations exist between insomnia and the spatial extent of pain in the body both in cross-sectional and longitudinal perspectives (11, 15, 116). Both Norwegian and Swedish longitudinal studies reported that insomnia is a risk factor for increased spreading of pain (15, 116). This study shows that more widespread pain (an increased spatial extent) was associated with stronger effects for three of the direct paths from Insomnia—i.e., to Pain intensity, Catastrophizing, and Fear avoidance. Consistent with our results, a recent network study (insomnia was not included) reported that the pain extent was a moderator of the relationships between several of the variables included in the present PLS-SEM (117).
4.4. Insomnia correlations (i.e., the direct paths from Insomnia)
The importance of assessing sleep problems, especially insomnia, is further strengthened by the present observations that insomnia showed significant associations (i.e., significant direct path coefficients) with all clinical aspects of the clinical presentation included in this study (Figure 2 and Table 4). Thus, Insomnia was most strongly associated with Psychological distress (positively), Catastrophizing (positively), and Acceptance (negatively). The paths with Pain intensity and Fear avoidance were positive and significant but weaker than for the other latent variables. On a general level, several other studies have reported associations between insomnia and these clinical variables (9, 37, 118–120). However, our results are partly in contrast to a network study that demonstrated that insomnia had a stronger correlation with pain intensity aspects than with depression and anxiety symptoms (121). On the other hand, our results agree with another smaller SQRP real-world study from one department, which found that ISI had the strongest correlations with anxiety and depressive symptoms (9). Obviously, more studies are required to understand these intercorrelations, including both their causal cross-sectional and longitudinal associations.
4.5. Latent variables correlating with pain intensity (i.e., the direct paths to pain intensity)
One important observation is that the correlations (direct paths) between Insomnia and the five mediators are stronger than the correlations between the five mediators and pain intensity. Nevertheless, our results concerning the direct paths from the five mediators to pain intensity indicate that it is clinically important that the assessment process focuses on more than just psychological distress levels. In fact, it can be even more important to focus on insomnia and coping aspects such as catastrophizing and acceptance. Hence, Pain intensity had the strongest absolute correlation (positive β) with Insomnia followed by Acceptance (negative β) and Catastrophizing (positive β). Interestingly, the Psychological distress–Pain intensity direct path did not reach significance (p = 0.054), and other studies have reported weak intercorrelations between pain intensity and psychological distress aspects (117, 121). Such results concerning the levels of these two latent variables do not invalidate that psychological distress is a common comorbidity in chronic pain (122, 123).
4.6. Clinical significance
The present study confirmed a significant direct path not only between Insomnia and Pain intensity (and vice versa) but also via other mediating latent variables—i.e., Catastrophizing, Acceptance, and Fear avoidance. In addition, Insomnia showed even stronger direct associations with Psychological distress, Catastrophizing, and Acceptance. As all these clinical facets contribute to considerable suffering for the individual and are interconnected both at the psychological and physiological level, it is relevant to address them in a clinical setting. Poor acceptance, for example, is characterized by an inability to come to terms with the chronic pain condition where considerable effort is made to solve an unsolvable problem, leaving patients in constant limbo, further contributing to their stress. The fear and helplessness of catastrophizing will naturally also contribute to negative behavioral feedback loops, which produce considerable stress and heightened pain. Poor sleep, psychological distress, catastrophizing, and low acceptance all constitute considerable stressors that can affect the balance that individuals maintain between biological, psychological, and sociocontextual aspects or factors, leading to a vicious unhealthy cycle. For example, Haack et al. (124) found that sleep deficiency can affect various neurobiological systems that influence nociceptive processing. Hence, it is easy to perceive how such a situation impacts, for example, autonomous control, leading to a restless state and poorer sleep. As such, vicious psychological and physiological circles are intertwined, which is both problematic and hopeful in the sense that identifying and influencing one factor might lead to beneficial effects for the whole circle. Clinical assessments including both pain and insomnia are reasonable since both direct and mediating factors are present between insomnia and pain intensity. Although Swedish IPRPs generally address acceptance and behaviors such as avoidance, they do not for the most part adequately address insomnia (125). This oversight neglects a huge potential to attend to an important physiological key factor that can have many beneficial effects. Future research should focus on illuminating how sleep interventions influence pain intensity and other important key factors contributing to distress for chronic pain patients.
4.7. Strength and limitations
A strength of this study is its large cohort of chronic pain patients with nationwide representation. Our results are relevant for patients referred to specialist care, which represent the most complex patients with chronic pain on a general level. Most of the mediating studies included in the SR of mediating paths were single mediation studies (43). Hence, they represent a too simplistic view of the clinical presentation of patients with chronic pain. Parallel mediation more adequately mirrors the clinical situation. Several of the latent variables had several indicators, which is an advantage from a measurement error point of view compared to path analyses, which only use single items representing a certain latent variable. The present cohort is representative—with respect to sex and education level—for the chronic pain patients referred to specialist departments in Sweden. The moderator analyses showed no major differences in path patterns. Hence, we therefore have no reason to believe that a more even distribution regarding, e.g., sex or education level would change our results.
Another strength of this study is the consistency of the overall findings supports the conclusions. Similarly, the overall point—to quantify the relative contributions of these latent variables on the insomnia/ chronic pain cycle—does not depend entirely on many individual statistical tests that are vulnerable to false positives.
The obvious limitation is that our study is based on cross-sectional data. Thus, future studies using PLS-SEM may include within-day and day-to-day variability studies. On the other hand, from the perspective of the clinical assessment, it is also important that cross-sectional studies deepen the understanding of how insomnia and pain intensity interact. Our PLS-SEM analysis is based on a specific overarching hypothesis concerning the insomnia–pain intensity relationship, which in essence was investigated in the SR of Whibley et al. (43). Future studies—which may be based on other hypotheses—are needed to validate our results. Moreover, cohort heterogeneity concerning the latent variables (Insomnia–Pain intensity relationship including mediators) may be present for other aspects than the moderators investigated in this study. Moreover, questionnaires such as ISI serve as a proxy for capturing insomnia problems; polysomnography is considered the golden standard, and actigraphy is considered the second best way to capture insomnia problems (126, 127). Measuring insomnia and other sleep problems with more objective methods may further strengthen results from PLS-SEM analyses. The inclusion of objective methods has the disadvantage that the studies must be considerably smaller both for practical and financial reasons.
4.8. Conclusions
This large cohort study of chronic pain patients with an insomnia prevalence of more than 60% (62.3%) revealed that both direct and mediating paths exist for the Insomnia–Pain intensity relationship. Together, these mediating effects were weaker than the direct effect between Insomnia and Pain intensity. The mediating effects via Catastrophizing and Acceptance showed the strongest and equal mediating paths, which were followed by those via Fear avoidance. Insomnia showed direct significant correlations with Psychological distress, Catastrophizing, Acceptance, and Fear avoidance stronger than those with Pain intensity. The five moderators did not significantly affect the mediating paths. Future research should focus on illuminating how sleep interventions influence pain intensity and other important key factors that contribute to the distress of chronic pain patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethical Review Board in Linköping (Dnr: 2015/108-31), Sweden. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization: All authors. Data curation: BG and ÅR. Formal analysis: BG. Methodology: All authors. Writing – original draft: BG and ÅR. Writing – review and editing: All authors. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2023.1244606/full#supplementary-material
References
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. (2006) 10(4):287–333. doi: 10.1016/j.ejpain.2005.06.009
2. Ringqvist Å, Dragioti E, Björk M, Larsson B, Gerdle B. Moderate and stable pain reductions as a result of interdisciplinary pain rehabilitation—a cohort study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). J Clin Med. (2019) 8:905. doi: 10.3390/jcm8060905
3. Grimby-Ekman A, Gerdle B, Bjork J, Larsson B. Comorbidities, intensity, frequency and duration of pain, daily functioning and health care seeking in local, regional, and widespread pain—a descriptive population-based survey (SwePain). BMC Musculoskelet Disord. (2015) 16:165. doi: 10.1186/s12891-015-0631-1
4. Morin CM, Drake CL, Harvey AG, Krystal AD, Manber R, Riemann D, et al. Insomnia disorder. Nat Rev Dis Primers. (2015) 1:15026. doi: 10.1038/nrdp.2015.26
5. Husak AJ, Bair MJ. Chronic pain and sleep disturbances: a pragmatic review of their relationships, comorbidities, and treatments. Pain Med. (2020) 21(6):1142–52. doi: 10.1093/pm/pnz343
6. Bjurstrom M, Irwin M. Polysomnographic characteristics in nonmalignant chronic pain populations: a review of controlled studies. Sleep Med Rev. (2016) 26:74–86. doi: 10.1016/j.smrv.2015.03.004
7. Mathias J, Cant M, Burke A. Sleep disturbances and sleep disorders in adults living with chronic pain: a meta-analysis. Sleep Med Rev. (2018) 52:198–210. doi: 10.1016/j.sleep.2018.05.023
8. Sun Y, Laksono I, Selvanathan J, Saripella A, Nagappa M, Pham C, et al. Prevalence of sleep disturbances in patients with chronic non-cancer pain: a systematic review and meta-analysis. Sleep Med Rev. (2021) 57:101467. doi: 10.1016/j.smrv.2021.101467
9. Alfoldi P, Wiklund T, Gerdle B. Comorbid insomnia in patients with chronic pain: a study based on the Swedish Quality Registry for Pain Rehabilitation (SQRP). Disabil Rehabil. (2014) 36(20):1661–9. doi: 10.3109/09638288.2013.864712
10. Ohayon M. Relationship between chronic painful physical condition and insomnia. J Psychiatr Res. (2005) 39(2):151–9. doi: 10.1016/j.jpsychires.2004.07.001
11. Alfoldi P, Dragioti E, Wiklund T, Gerdle B. Spreading of pain and insomnia in patients with chronic pain: results from a national quality registry (SQRP). J Rehabil Med. (2017) 49(1):63–70. doi: 10.2340/16501977-2162
12. Smith M, Haythornthwaite J. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive-behavioral clinical trials literature. Sleep Med Rev. (2004) 8(2):119–32. doi: 10.1016/S1087-0792(03)00044-3
13. Aili K, Nyman T, Svartengren M, Hillert L. Sleep as a predictive factor for the onset and resolution of multi-site pain: a 5-year prospective study. Eur J Pain. (2015) 19:341–9. doi: 10.1002/ejp.552
14. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. (2013) 14(12):1539–52. doi: 10.1016/j.jpain.2013.08.007
15. Mundal I, Grawe RW, Bjorngaard JH, Linaker OM, Fors EA. Prevalence and long-term predictors of persistent chronic widespread pain in the general population in an 11-year prospective study: the HUNT study. BMC Musculoskelet Disord. (2014) 15:213. doi: 10.1186/1471-2474-15-213
16. Andersen ML, Araujo P, Frange C, Tufik S. Sleep disturbance and pain: a tale of two common problems. Chest. (2018) 154(5):1249–59. doi: 10.1016/j.chest.2018.07.019
17. Arnison T, Schrooten MGS, Hesser H, Jansson-Frojmark M, Persson J. Longitudinal, bidirectional relationships of insomnia symptoms and musculoskeletal pain across adolescence: the mediating role of mood. Pain. (2022) 163(2):287–98. doi: 10.1097/j.pain.0000000000002334
18. Skarpsno E, Mork P, Hagen K, Nilsen T, Marcuzzi A. Number of chronic nighttime insomnia symptoms and risk of chronic widespread pain and pain-related disability: the HUNT study. Nat Sci Sleep. (2020) 12:1227–36. doi: 10.2147/NSS.S284498
19. Sivertsen B, Krokstad S, Overland S, Mykletun A. The epidemiology of insomnia: associations with physical and mental health. The HUNT-2 study. J Psychosom Res. (2009) 67(2):109–16. doi: 10.1016/j.jpsychores.2009.05.001
20. Wu Y, Gong Q, Zou Z, Li H, Zhang X. Short sleep duration and obesity among children: a systematic review and meta-analysis of prospective studies. Obes Res Clin Pract. (2017) 11(2):140–50. doi: 10.1016/j.orcp.2016.05.005
21. Okifuji A, Hare BD. The association between chronic pain and obesity. J Pain Res. (2015) 8:399–408. doi: 10.2147/JPR.S55598
22. Bevenius-Carrick J. Summary and conclusions of the SBU report: treatment of insomnia in adults: a systematic review. Stockholm: Swedish Council on Health Technology Assessment (SBU) (2010).
23. Linton SJ, Nicholas MK, Macdonald S, Boersma K, Bergbom S, Maher C, et al. The role of depression and catastrophizing in musculoskeletal pain. Eur J Pain. (2011) 15(4):416–22. doi: 10.1016/j.ejpain.2010.08.009
24. Jansson-Frojmark M, Harvey A, Flink I. Psychometric properties of the insomnia catastrophizing scale (ICS) in a large community sample. Cogn Behav Ther. (2020) 49(2):120–36. doi: 10.1080/16506073.2019.1588362
25. Gerhart JI, Burns JW, Post KM, Smith DA, Porter LS, Burgess HJ, et al. Relationships between sleep quality and pain-related factors for people with chronic low back pain: tests of reciprocal and time of day effects. Ann Behav Med. (2017) 51(3):365–75. doi: 10.1007/s12160-016-9860-2
26. Mahdavi SB, Riahi R, Vahdatpour B, Kelishadi R. Association between sedentary behavior and low back pain; a systematic review and meta-analysis. Health Promot Perspect. (2021) 11(4):393–410. doi: 10.34172/hpp.2021.50
27. Sporndly-Nees S, Asenlof P, Lindberg E. High or increasing levels of physical activity protect women from future insomnia. Sleep Med. (2017) 32:22–7. doi: 10.1016/j.sleep.2016.03.017
28. Espie C. Insomnia: conceptual issues in the development, persistence, and treatment of sleep disorder in adults. Annu Rev Psychol. (2002) 53:215–43. doi: 10.1146/annurev.psych.53.100901.135243
29. Linton S. A review of psychological risk factors in back and neck pain. Spine (Phila Pa 1976). (2000) 25(9):1148–56. doi: 10.1097/00007632-200005010-00017
30. Mundal I, Grawe R, Bjorngaard J, Linaker O, Fors EA. Psychosocial factors and risk of chronic widespread pain: an 11-year follow-up study–the HUNT study. Pain. (2014) 155(8):1555–61. doi: 10.1016/j.pain.2014.04.033
31. Tang NK, Wright KJ, Salkovskis PM. Prevalence and correlates of clinical insomnia co-occurring with chronic back pain. J Sleep Res. (2007) 16(1):85–95. doi: 10.1111/j.1365-2869.2007.00571.x
32. O'Brien EM, Waxenberg LB, Atchison JW, Gremillion HA, Staud RM, McCrae CS, et al. Negative mood mediates the effect of poor sleep on pain among chronic pain patients. Clin J Pain. (2010) 26(4):310–9. doi: 10.1097/AJP.0b013e3181c328e9
33. McCracken LM, Williams JL, Tang NK. Psychological flexibility may reduce insomnia in persons with chronic pain: a preliminary retrospective study. Pain Med. (2011) 12(6):904–12. doi: 10.1111/j.1526-4637.2011.01115.x
34. Ong JC, Ulmer CS, Manber R. Improving sleep with mindfulness and acceptance: a metacognitive model of insomnia. Behav Res Ther. (2012) 50(11):651–60. doi: 10.1016/j.brat.2012.08.001
35. Tiede W, Magerl W, Baumgärtner U, Durrer B, Ehlert U, Treede R. Sleep restriction attenuates amplitudes and attentional modulation of pain-related evoked potentials, but augments pain ratings in healthy volunteers. Pain. (2010) 148(1):36–42. doi: 10.1016/j.pain.2009.08.029
36. Simpson NS, Scott-Sutherland J, Gautam S, Sethna N, Haack M. Chronic exposure to insufficient sleep alters processes of pain habituation and sensitization. Pain. (2018) 159(1):33–40. doi: 10.1097/j.pain.0000000000001053
37. Bilterys T, Siffain C, De Maeyer I, Van Looveren E, Mairesse O, Nijs J, et al. Associates of insomnia in people with chronic spinal pain: a systematic review and meta-analysis. J Clin Med. (2021) 10(14):3175. doi: 10.3390/jcm10143175
38. Babiloni AH, De Koninck BP, Beetz G, De Beaumont L, Martel MO, Lavigne GJ. Sleep and pain: recent insights, mechanisms, and future directions in the investigation of this relationship. J Neural Transm (Vienna). (2020) 127(4):647–60. doi: 10.1007/s00702-019-02067-z
39. Dijk D. Slow-wave sleep, diabetes, and the sympathetic nervous system. Proc Natl Acad Sci U S A. (2008) 105:1107–8. doi: 10.1073/pnas.0711635105
40. Landis CA. Sleep, pain, fibromyalgia, and chronic fatigue syndrome. Handb Clin Neurol. (2011) 98:613–37. doi: 10.1016/B978-0-444-52006-7.00039-3
41. Tang NK, Goodchild CE, Sanborn AN, Howard J, Salkovskis PM. Deciphering the temporal link between pain and sleep in a heterogeneous chronic pain patient sample: a multilevel daily process study. Sleep. (2012) 35(5):675–87A. doi: 10.5665/sleep.1830
42. Okifuji A, Hare BD. Do sleep disorders contribute to pain sensitivity? Curr Rheumatol Rep. (2011) 13(6):528–34. doi: 10.1007/s11926-011-0204-8
43. Whibley D, AlKandari N, Kristensen K, Barnish M, Rzewuska M, Druce KL, et al. Sleep and pain: a systematic review of studies of mediation. Clin J Pain. (2019) 35(6):544–58. doi: 10.1097/AJP.0000000000000697
44. Bromley Milton M, Borsbo B, Rovner G, Lundgren-Nilsson A, Stibrant-Sunnerhagen K, Gerdle B. Is pain intensity really that important to assess in chronic pain patients? A study based on the Swedish quality registry for pain rehabilitation (SQRP). PLoS One. (2013) 8(6):e65483. doi: 10.1371/journal.pone.0065483
45. Gerdle B, Rivano Fischer M, Ringqvist Å. Interdisciplinary pain rehabilitation programs: evidence and clinical real-world results. In: Aslanidis T, Nouris C, editors. Pain management—from pain mechanisms to patient care. London: IntechOpen (2022). p. 1–36.
46. Gerdle B, Boersma K, Asenlof P, Stalnacke BM, Larsson B, Ringqvist A. Influences of sex, education, and country of birth on clinical presentations and overall outcomes of interdisciplinary pain rehabilitation in chronic pain patients: a cohort study from the Swedish quality registry for pain rehabilitation (SQRP). J Clin Med. (2020) 9(8):2374. doi: 10.3390/jcm9082374
47. Gerdle B, Cervin M, Rivano Fischer M, Ringqvist A. Outcomes of interdisciplinary pain rehabilitation across subgroups of the multidimensional pain inventory—a study from the Swedish quality registry for pain rehabilitation. Pain Pract. (2021) 21(6):662–79. doi: 10.1111/papr.13007
48. Gerdle B, Rivano Fischer M, Cervin M, Ringqvist Å. Spreading of pain in patients with chronic pain is related to pain duration and clinical presentation and weakly associated with outcomes of interdisciplinary pain rehabilitation: a cohort study from the Swedish quality registry for pain rehabilitation (SQRP). J Pain Res. (2021) 14:173–87. doi: 10.2147/JPR.S288638
49. Gerdle B, Åkerblom S, Brodda Jansen G, Enthoven P, Ernberg M, Dong HJ, et al. Who benefits from multimodal rehabilitation—an exploration of pain, psychological distress, and life impacts in over 35,000 chronic pain patients identified in the Swedish quality registry for pain rehabilitation. J Pain Res. (2019) 12:891–908. doi: 10.2147/JPR.S190003
50. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67(6):361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
51. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. (2002) 52(2):69–77. doi: 10.1016/S0022-3999(01)00296-3
52. LoMartire R, Ang BO, Gerdle B, Vixner L. Psychometric properties of short form-36 health survey, EuroQol 5-dimensions, and hospital anxiety and depression scale in patients with chronic pain. Pain. (2020) 161(1):83–95. doi: 10.1097/j.pain.0000000000001700
53. Vlaeyen J, Kole-Snijders A, Boeren R, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain. (1995) 62:363–72. doi: 10.1016/0304-3959(94)00279-N
54. Roelofs J, Sluiter J, Frings-Dresen M, Goossens M, Thibault P, Boersma K, et al. Fear of movement and (re)injury in chronic musculoskeletal pain: evidence for an invariant two-factor model of the Tampa scale for kinesiophobia across pain diagnoses and Dutch, Swedish, and Canadian samples. Pain. (2007) 131:181–90. doi: 10.1016/j.pain.2007.01.008
55. Leeuw M, Goossens ME, van Breukelen GJ, de Jong JR, Heuts PH, Smeets RJ, et al. Exposure in vivo vs. operant graded activity in chronic low back pain patients: results of a randomized controlled trial. Pain. (2008) 138(1):192–207. doi: 10.1016/j.pain.2007.12.009
56. Lundberg M, Larsson M, Ostlund H, Styf J. Kinesiophobia among patients with musculoskeletal pain in primary healthcare. J Rehabil Med. (2006) 38(1):37–43. doi: 10.1080/16501970510041253
57. Crombez G, Vlaeyen J, Heuts P, Lysens R. Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain. (1999) 80:329–39. doi: 10.1016/S0304-3959(98)00229-2
58. Rovner GS, Arestedt K, Gerdle B, Borsbo B, McCracken LM. Psychometric properties of the 8-item chronic pain acceptance questionnaire (CPAQ-8) in a Swedish chronic pain cohort. J Rehabil Med. (2014) 46(1):73–80. doi: 10.2340/16501977-1227
59. Kranz D, Bollinger A, Nilges P. Chronic pain acceptance and affective well-being: a coping perspective. Eur J Pain. (2010) 14(10):1021–5. doi: 10.1016/j.ejpain.2010.03.010
60. Miro J, Nieto R, Huguet A. The Catalan version of the pain catastrophizing scale: a useful instrument to assess catastrophic thinking in whiplash patients. J Pain. (2008) 9(5):397–406. doi: 10.1016/j.jpain.2007.12.004
61. Sullivan M, Bishop S, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. (1995) 7:524–32. doi: 10.1037/1040-3590.7.4.524
62. Kemani MK, Grimby-Ekman A, Lundgren J, Sullivan M, Lundberg M. Factor structure and internal consistency of a Swedish version of the pain catastrophizing scale. Acta Anaesthesiol Scand. (2019) 63(2):259–66. doi: 10.1111/aas.13246
63. Olsson S. Studies of physical activity in the Swedish population. Stockholm: The Swedish School of Sport and Health Sciences (2016).
64. Bastien C, Vallieres A, Morin C. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. (2001) 2(4):297–307. doi: 10.1016/S1389-9457(00)00065-4
65. Hair J Jr., Hult G, Ringle C, Sarstedt M. A primer on partial least squares structural equation modelling (PLS-SEM). 3rd ed. Los Angeles: Sage (2022).
66. Chua Y. A step-by-step guide: PLS-SEM data analysis using SmartPLS 4. Kuala Lumpur: Researchtree Education (2023).
67. Kenny D. Mediation 2021. Available at: https://davidakenny.net/cm/mediate.htm (Accessed May 4, 2021).
68. Sheko A, Braimllari A. Information technology inhibitors and information quality in supply chain management: a PLS-SEM analysis. Acad J Interdiscipl Stud. (2018) 7(3):125–38. doi: 10.2478/ajis-2018-0064
69. Lind J, Andrell P, Grimby-Ekman A. Insomnia symptoms and chronic pain among patients participating in a pain rehabilitation program—a registry study. J Clin Med. (2021) 10(18):4040. doi: 10.3390/jcm10184040
70. Alimoradi Z, Jafari E, Brostrom A, Ohayon MM, Lin CY, Griffiths MD, et al. Effects of cognitive behavioral therapy for insomnia (CBT-I) on quality of life: a systematic review and meta-analysis. Sleep Med Rev. (2022) 64:101646. doi: 10.1016/j.smrv.2022.101646
71. Carpi M, Cianfarani C, Vestri A. Sleep quality and its associations with physical and mental health-related quality of life among university students: a cross-sectional study. Int J Environ Res Public Health. (2022) 19(5):2874. doi: 10.3390/ijerph19052874
72. Kyle SD, Morgan K, Espie CA. Insomnia and health-related quality of life. Sleep Med Rev. (2010) 14(1):69–82. doi: 10.1016/j.smrv.2009.07.004
73. Dragioti E, Bernfort L, Larsson B, Gerdle B, Levin LA. Association of insomnia severity with well-being, quality of life and health care costs: a cross-sectional study in older adults with chronic pain (PainS65+). Eur J Pain. (2018) 22(2):414–25. doi: 10.1002/ejp.1130
74. Whale K, Gooberman-Hill R. The importance of sleep for people with chronic pain: current insights and evidence. JBMR Plus. (2022) 6(7):e10658. doi: 10.1002/jbm4.10658
75. Johnson KA, Gordon CJ, Chapman JL, Hoyos CM, Marshall NS, Miller CB, et al. The association of insomnia disorder characterised by objective short sleep duration with hypertension, diabetes and body mass index: a systematic review and meta-analysis. Sleep Med Rev. (2021) 59:101456. doi: 10.1016/j.smrv.2021.101456
76. Trost Z, Strachan E, Sullivan M, Vervoort T, Avery AR, Afari N. Heritability of pain catastrophizing and associations with experimental pain outcomes: a twin study. Pain. (2015) 156(3):514–20. doi: 10.1097/01.j.pain.0000460326.02891.fc
77. Burri A, Ogata S, Rice D, Williams F. Pain catastrophizing, neuroticism, fear of pain, and anxiety: defining the genetic and environmental factors in a sample of female twins. PLoS One. (2018) 13(3):e0194562. doi: 10.1371/journal.pone.0194562
78. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. (2016) 17(9 Suppl):T70–92. doi: 10.1016/j.jpain.2016.01.001
79. Martinez-Calderon J, Jensen MP, Morales-Asencio JM, Luque-Suarez A. Pain catastrophizing and function in individuals with chronic musculoskeletal pain: a systematic review and meta-analysis. Clin J Pain. (2019) 35(3):279–93. doi: 10.1097/AJP.0000000000000676
80. Leung L. Pain catastrophizing: an updated review. Indian J Psychol Med. (2012) 34:204–17. doi: 10.4103/0253-7176.106012
81. Linton SJ. A transdiagnostic approach to pain and emotion. J Appl Biobehav Res. (2013) 18(2):82–103. doi: 10.1111/jabr.12007
82. Linton S, Bergbom S. Understanding the link between depression and pain. Scand J Pain. (2011) 2:47–54. doi: 10.1016/j.sjpain.2011.01.005
83. Svanberg M, Stalnacke BM, Enthoven P, Brodda-Jansen G, Gerdle B, Boersma K. Impact of emotional distress and pain-related fear on patients with chronic pain: subgroup analysis of patients referred to multimodal rehabilitation. J Rehabil Med. (2017) 49(4):354–61. doi: 10.2340/16501977-2212
84. Schutze R, Rees C, Smith A, Slater H, Campbell JM, O’Sullivan P. How can we best reduce pain catastrophizing in adults with chronic noncancer pain? A systematic review and meta-analysis. J Pain. (2018) 19(3):233–56. doi: 10.1016/j.jpain.2017.09.010
85. Racine M, Moulin DE, Nielson WR, Morley-Forster PK, Lynch M, Clark AJ, et al. The reciprocal associations between catastrophizing and pain outcomes in patients being treated for neuropathic pain: a cross-lagged panel analysis study. Pain. (2016) 157(9):1946–53. doi: 10.1097/j.pain.0000000000000594
86. Hamilton NA, Pressman M, Lillis T, Atchley R, Karlson C, Stevens N. Evaluating evidence for the role of sleep in fibromyalgia: a test of the sleep and pain diathesis model. Cognit Ther Res. (2012) 36(6):806–14. doi: 10.1007/s10608-011-9421-8
87. Neblett R, Mayer TG, Williams MJ, Asih S, Cuesta-Vargas AI, Hartzell MM, et al. The fear-avoidance components scale (FACS): responsiveness to functional restoration treatment in a chronic musculoskeletal pain disorder (CMPD) population. Clin J Pain. (2017) 33(12):1088–99. doi: 10.1097/AJP.0000000000000501
88. Zale EL, Ditre JW. Pain-related fear, disability, and the fear-avoidance model of chronic pain. Curr Opin Psychol. (2015) 5:24–30. doi: 10.1016/j.copsyc.2015.03.014
89. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. (2007) 133(4):581. doi: 10.1037/0033-2909.133.4.581
90. Hayes S, Jacobson N, Follette V, Dougher M. Acceptance and change: content and context in psychotherapy. Reno: Context Press (1994).
91. McCracken L. Commentary: toward understanding acceptance and psychological flexibility in chronic pain. Pain. (2010) 149:420–1. doi: 10.1016/j.pain.2010.02.036
92. Scott W, McCracken L. Psychological flexibility, acceptance and commitment therapy, and chronic pain. Curr Opin Psychol. (2015) 2:91–6. doi: 10.1016/j.copsyc.2014.12.013
93. McCracken LM, Eccleston C. A prospective study of acceptance of pain and patient functioning with chronic pain. Pain. (2005) 118(1–2):164–9. doi: 10.1016/j.pain.2005.08.015
94. Viane I, Crombez G, Eccleston C, Devulder J, De Corte W. Acceptance of the unpleasant reality of chronic pain: effects upon attention to pain and engagement with daily activities. Pain. (2004) 112(3):282–8. doi: 10.1016/j.pain.2004.09.008
95. McCracken LM, Spertus IL, Janeck AS, Sinclair D, Wetzel FT. Behavioral dimensions of adjustment in persons with chronic pain: pain-related anxiety and acceptance. Pain. (1999) 80(1–2):283–9. doi: 10.1016/S0304-3959(98)00219-X
96. McCracken LM. Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain. (1998) 74(1):21–7. doi: 10.1016/S0304-3959(97)00146-2
97. Viane I, Crombez G, Eccleston C, Poppe C, Devulder J, Van Houdenhove B, et al. Acceptance of pain is an independent predictor of mental well-being in patients with chronic pain: empirical evidence and reappraisal. Pain. (2003) 106(1–2):65–72. doi: 10.1016/S0304-3959(03)00291-4
98. Salari N, Khazaie H, Hosseinian-Far A, Khaledi-Paveh B, Ghasemi H, Mohammadi M, et al. The effect of acceptance and commitment therapy on insomnia and sleep quality: a systematic review. BMC Neurol. (2020) 20(1):300. doi: 10.1186/s12883-020-01883-1
99. Ma TW, Yuen AS, Yang Z. The efficacy of acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. Clin J Pain. (2023) 39(3):147–57. doi: 10.1097/AJP.0000000000001096
100. Aytur SA, Ray KL, Meier SK, Campbell J, Gendron B, Waller N, et al. Neural mechanisms of acceptance and commitment therapy for chronic pain: a network-based fMRI approach. Front Hum Neurosci. (2021) 15:587018. doi: 10.3389/fnhum.2021.587018
101. Bonvanie IJ, Oldehinkel AJ, Rosmalen JGM, Janssens KAM. Sleep problems and pain: a longitudinal cohort study in emerging adults. Pain. (2016) 157(4):957–63. doi: 10.1097/j.pain.0000000000000466
102. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL 3rd. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. (2009) 10(5):447–85. doi: 10.1016/j.jpain.2008.12.001
103. Greenspan JD, Craft RM, LeResche L, Arendt-Nielsen L, Berkley KJ, Fillingim RB, et al. Studying sex and gender differences in pain and analgesia: a consensus report. Pain. (2007) 132(Suppl 1):S26–45. doi: 10.1016/j.pain.2007.10.014
104. Gerdle B, Bjork J, Henriksson C, Bengtsson A. Prevalence of current and chronic pain and their influences upon work and healthcare-seeking: a population study. J Rheumatol. (2004) 31(7):1399–406. 15229963.15229963
105. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. (2013) 111(1):52–8. doi: 10.1093/bja/aet127
106. Unruh AM. Gender variations in clinical pain experience. Pain. (1996) 65(2–3):123–67. doi: 10.1016/0304-3959(95)00214-6
107. Pieh C, Altmeppen J, Neumeier S, Loew T, Angerer M, Lahmann C. Gender differences in outcomes of a multimodal pain management program. Pain. (2012) 153(1):197–202. doi: 10.1016/j.pain.2011.10.016
108. Groeger JA, Zijlstra FR, Dijk DJ. Sleep quantity, sleep difficulties and their perceived consequences in a representative sample of some 2000 British adults. J Sleep Res. (2004) 13(4):359–71. doi: 10.1111/j.1365-2869.2004.00418.x
109. Kocevska D, Lysen TS, Dotinga A, Koopman-Verhoeff ME, Luijk M, Antypa N, et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: a systematic review and meta-analysis. Nat Hum Behav. (2021) 5(1):113–22. doi: 10.1038/s41562-020-00965-x
110. Morssinkhof MWL, van Wylick DW, Priester-Vink S, van der Werf YD, den Heijer M, van den Heuvel OA, et al. Associations between sex hormones, sleep problems and depression: a systematic review. Neurosci Biobehav Rev. (2020) 118:669–80. doi: 10.1016/j.neubiorev.2020.08.006
111. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. (2019) 123(2):e273–83. doi: 10.1016/j.bja.2019.03.023
112. Carr JL, Moffett JA. The impact of social deprivation on chronic back pain outcomes. Chronic Illn. (2005) 1(2):121–9. doi: 10.1177/17423953050010020901
113. Hammarstrom A, Haukenes I, Fjellman Wiklund A, Lehti A, Wiklund M, Evengard B, et al. Low-educated women with chronic pain were less often selected to multidisciplinary rehabilitation programs. PLoS One. (2014) 9(5):e97134. doi: 10.1371/journal.pone.0097134
114. Jordan KP, Thomas E, Peat G, Wilkie R, Croft P. Social risks for disabling pain in older people: a prospective study of individual and area characteristics. Pain. (2008) 137(3):652–61. doi: 10.1016/j.pain.2008.02.030
115. Chan WS, Levsen MP, McCrae CS. A meta-analysis of associations between obesity and insomnia diagnosis and symptoms. Sleep Med Rev. (2018) 40:170–82. doi: 10.1016/j.smrv.2017.12.004
116. Wiklund T, Gerdle B, Linton SJ, Dragioti E, Larsson B. Insomnia is a risk factor for spreading of chronic pain: a Swedish longitudinal population study (SwePain). Eur J Pain. (2020) 24(7):1348–56. doi: 10.1002/ejp.1582
117. Zhao X, Boersma K, Gerdle B, Molander P, Hesser H. Fear network and pain extent: interplays among psychological constructs related to the fear-avoidance model. J Psychosom Res. (2023) 167:111176. doi: 10.1016/j.jpsychores.2023.111176
118. Catala P, Gutierrez L, Ecija C, Penacoba C. Pathological cycle between pain, insomnia, and anxiety in women with fibromyalgia and its association with disease impact. Biomedicines. (2023) 11(1):148. doi: 10.3390/biomedicines11010148
119. Taylor JL, Regier NG, Li Q, Liu M, Szanton SL, Skolasky RL. The impact of low back pain and vigorous activity on mental and physical health outcomes in older adults with arthritis. Front Pain Res (Lausanne). (2022) 3:886985. doi: 10.3389/fpain.2022.886985
120. Dong HJ, Gerdle B, Bernfort L, Levin LA, Dragioti E. Pain catastrophizing in older adults with chronic pain: the mediator effect of mood using a path analysis approach. J Clin Med. (2020) 9(7):2073. doi: 10.3390/jcm9072073
121. Akerblom S, Cervin M, Perrin S, Rivano Fischer M, Gerdle B, McCracken LM. A network analysis of clinical variables in chronic pain: a study from the Swedish quality registry for pain rehabilitation (SQRP). Pain Med. (2021) 22(7):1591–602. doi: 10.1093/pm/pnaa473
122. Hooten W. Chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. (2016) 91:955–70. doi: 10.1016/j.mayocp.2016.04.029
123. Armbrecht E, Shah A, Schepman P, Shah R, Pappadopulos E, Chambers R, et al. Economic and humanistic burden associated with noncommunicable diseases among adults with depression and anxiety in the United States. J Med Econ. (2020) 23(9):1032–42. doi: 10.1080/13696998.2020.1776297
124. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. (2020) 45(1):205–16. doi: 10.1038/s41386-019-0439-z
125. Rivano Fischer M, Schults M, Stålnacke B, Ekholm J, Persson E, Löfgren M. Variability in patient characteristics and service provision of interdisciplinary pain rehabilitation: a study using the Swedish national quality registry for pain rehabilitation. J Rehabil Med. (2020) 52(11):jrm00128. doi: 10.2340/16501977-2765
126. Lauderdale D, Knutson K, Yan L, Liu K, Rathouz P. Self-reported and measured sleep duration: how similar are they? Epidemiology. (2008) 19:838–45. doi: 10.1097/EDE.0b013e318187a7b0
Keywords: acceptance, anxiety, catastrophizing, depression, fear avoidance, insomnia, pain, physical activity
Citation: Gerdle B, Dragioti E, Rivano Fischer M, Dong H-J and Ringqvist Å (2023) Catastrophizing and acceptance are mediators between insomnia and pain intensity—an SQRP study of more than 6,400 patients with non-malignant chronic pain conditions. Front. Pain Res. 4:1244606. doi: 10.3389/fpain.2023.1244606
Received: 23 June 2023; Accepted: 5 September 2023;
Published: 27 September 2023.
Edited by:
Karin N. Westlund, University of New Mexico Health Sciences Center, United StatesReviewed by:
Timothy Petersen, University of New Mexico, United StatesEleni G. Hapidou, McMaster University, Canada
© 2023 Gerdle, Dragioti, Rivano Fischer, Dong and Ringqvist. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Björn Gerdle Ympvcm4uZ2VyZGxlQGxpdS5zZQ==