 Junning Zhang
Junning Zhang Weizhen Wu
Weizhen Wu Yuehan Ren
Yuehan Ren Yi Yuan
Yi Yuan Liqun Jia
Liqun Jia- 1Graduate School, Beijing University of Chinese Medicine, Beijing, China
- 2Department of Oncology of Integrative Chinese and Western Medicine, China-Japan Friendship Hospital, Beijing, China
Objective: This paper aims to review the current evidence on electroacupuncture as an effective and safe therapy for cancer pain management.
Methods: Five databases were searched from their inception through November 11, 2022. Only the randomized controlled trials that meet the eligibility criteria were finally included in the study. Literature screening and data extraction were performed independently by two reviewers, and RevMan 5.3 used for meta-analysis.
Results: A total of 17 RCTs met our inclusion criteria. We used 8 indicators to estimate the meta-analysis results, most of which proved statistically significant, including VAS scores, NRS scores, and KPS scores. To be specific, VAS scores (MD = −1.41, 95% CI: −2.42 to −0.41, P = 0.006) and NRS scores (MD = −1.19, 95% CI: −1.72 to −0.66, P < 0.0001) were significantly lower in the treatment group compared to the control group. The treatment group's KPS scores (MD = 5.48, 95% CI: 3.27 to 7.69, P < 0.00001) were higher than those of the control group. Also, in the treatment group, the number of burst pain (MD = −2.66, 95% CI: −3.32 to −1.99, P < 0.00001) and side effect rates (RR = 0.51, 95% CI: 0.39 to 0.67, P < 0.00001) greatly reduced, while the response rate (RR = 1.17, 95% CI: 1.09 to 1.26, P < 0.0001) significantly increased compared to the control group.
Conclusion: This study demonstrates the advantages of electroacupuncture in the treatment of cancer pain. Meanwhile, rigorous RCTs should be designed and conducted in the future to further demonstrate the exact efficacy of electroacupuncture.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42022376148.
1. Introduction
Cancer is a large group of diseases that can start in almost any organ or tissue of the body when abnormal cells grow uncontrollably and spread to other organs (1). It is a leading cause of death worldwide, accounting for nearly 10 million deaths in 2020, or nearly one in six deaths (2). One of the major challenges in cancer treatment is pain management. Cancer pain can be caused by a tumor compressing or infiltrating nearby body parts, treatments and diagnostic procedures, skin, nerve and other changes caused by a hormone imbalance or immune response (3). Up to 2022, the overall prevalence of cancer pain was 44.5% (4). Cancer pain relief is an important aspect of cancer care, which can be achieved by using a combination of pharmacological and non-pharmacological interventions, such as opioids, adjuvant drugs, nerve blocks, acupuncture, massage and psychotherapy (5), although the most widely-used management is analgesic agents alone (6).
The World Health Organization (WHO) proposed a three-step analgesic ladder for cancer pain relief in 1986, which recommends using different types of drugs according to the intensity of pain. The first step involves using non-opioid analgesics (such as paracetamol or ibuprofen) for mild pain; the second step involves using weak opioids (such as codeine or tramadol) for moderate pain; and the third step involves using strong opioids (such as morphine or fentany l) for severe pain (7).
However, this approach has some limitations and drawbacks. First, many patients do not receive adequate pain relief due to under prescription or undertreatment of opioids (8). Second, opioids have significant side effects such as constipation, nausea, sedation, respiratory depression and addiction (9). Third, opioids are often inaccessible or unaffordable in low- and middle-income countries due to regulatory barriers and supply issues (10). Therefore, alternative therapies such as acupuncture have been increasingly used to complement or replace conventional pharmacological interventions (11).
Over the past few decades, acupuncture has gained increasing popularity in the Western world as a complementary therapy for a range of conditions, including pain management (12). One promising therapy that has been increasingly used for cancer pain is electroacupuncture (13). Electroacupuncture is a form of acupuncture that involves applying electrical currents to needles inserted at specific points on the body (14). A growing body of research has demonstrated the effectiveness of electroacupuncture in managing cancer pain. For example, a systematic review of acupuncture in cancer care found that acupuncture was effective in reducing pain in patients with cancer pain, and that electroacupuncture may have additional benefits in reducing pain intensity and duration (15). Electroacupuncture has several advantages over conventional acupuncture. For instance, it can stimulate deeper tissues and produce stronger analgesic effects by activating different types of nerve fibers (16). It can also reduce the number and duration of needles required and allow more precise control over stimulation intensity and frequency (17). Furthermore, electroacupuncture has a low cost and few side effects compared to pharmacological treatments (18).
In summary, this paper aims to review the current evidence on electroacupuncture as an effective and safe therapy for cancer pain management. We will discuss its mechanisms of action, clinical applications, and future directions. We hope that this paper will provide useful information for clinicians and researchers who are interested in electroacupuncture as an alternative or complementary option for cancer pain treatment.
2. Methods
PROSPERO registration has been completed in November 2022 with the registration number CRD42022376148. More details available at https://www.crd.york.ac.uk/PROSPERO/. Before the start of our study, considering that the pre-defined outcome indicators could not cover the main outcomes currently observed for cancer pain, we adjusted the implementation protocol by adding NRS (Numerical Rating Scale), times of burst pain and treatment response rate as our observed indicators. The modified protocol was reviewed and approved by two reviewers (LQJ and JNZ). Reporting standard followed PRISMA statement (see Supplementary Material).
2.1. Data sources
Three English-language databases and two Chinese-language databases were searched from their inception through November 11th, 2022: China National Knowledge Infrastructure (CNKI), Wanfang Database for Chinese Technical Periodicals, PubMed, Web of Science, and Cochrane Central Registry of Controlled Trials (CENTRAL). We use the MeSH term, title, and abstract to search the three English databases were: (electroacupuncture or electro-acupuncture) AND (“cancer” OR “tumour” OR “neoplasm”) AND (“pain OR ache OR cancer pain”) AND (“randomized controlled trial”). The keywords were then translated into Chinese and searched in the two remaining Chinese databases. After reading the full text, we collected them together in the ZOTERO database, in which the repetitive literature was removed.
2.2. Study selection
RCTs were included if electroacupuncture was used as the only intervention or as an adjunct to another standard treatment for cancer pain and the control group received the same concomitant treatment as the electroacupuncture group. We ignored whether the included studies used the correct randomization method, allocation concealment, and blinding. There were no language restrictions. Trials that used comparative treatments/groups that were expected to have similar effects to electroacupuncture (moxibustion, transcutaneous electrical acupoint stimulation, acupoint injection, laser irradiation, cupping, Tuina, etc.) or that used Chinese herbal medicine were excluded. Trials that studied cancer pain mixed with other types of pain and trials that were performed on patients during or a few days after surgery for malignancy were also excluded. Trials were also excluded if their results were not related to cancer pain.
The studies we included involved at least one of the following outcomes.
Primary Outcome Indicators.
• VAS (Visual Analogue Scale);
• NRS (Numerical Rating Scale);
• NPS (Neuropathic Pain Scale);
• BPI (Brief Pain Inventory);
• KPS (Karnofsky Performance Status).
Secondary Outcome Indicators.
• Times of burst pain;
• Treatment response rate;
• Side effect rates.
In addition, considering the differences in the definitions of treatment response rate among studies, we defined the efficiency rate. The treatment response rate was determined by the degree of pain relief, and the efficacy index = (pre-treatment NRS score—post-treatment NRS score)/pre-treatment NRS score × 100%. Complete remission (CR): efficacy index was 91%–100%; apparent remission (AR): efficacy index was 61%–90%; partial remission (PR): efficacy index was 31%–60%. No remission (NR): efficacy index <31%. Effective cases were CR + AR + PR. We included the results of related studies for analysis if their outcome measures approximated our definition.
2.3. Methodology quality assessment and data extraction
The risk of bias was assessed using the following criteria from the Cochrane classification: random sequence generation, allocation concealment, blinding of participants and staff, blinding of outcome assessment, incomplete outcome data, selective reporting and other types of bias. The authors classified studies as “low risk” (L), “unclear risk (U)” and “high risk” (H) (19).
All articles were read by two independent reviewers (JNZ and WZW) who independently assessed the study selection, methodology quality assessment, and data extraction process, then we cross-checked the data. Any disagreements were resolved by discussion or consultation with a third independent reviewer (YHR).
2.4. Data analysis
If the study contained insufficient information, we tried to communicate with the lead author to obtain accurate data. RevMan 5.3 software provided by the Cochrane Collaboration Network was used for the meta-analysis. In this study we choose random effects model for our analysis. The risk ratio (RR) was used for the dichotomous variables, the mean difference (MD) was used for the continuous variables, and the 95% confidence interval (CI) was used for each effect quantity.
The Chi2 test was used for heterogeneity among the results of the included studies. In this study we used the following I² thresholds:
• I²:0%–40%: probably insignificant;
• I²:30%–60%: may represent moderate heterogeneity;
• I²:50%–90%: may represent significant heterogeneity;
• I²:75%–100%: considerable heterogeneity.
The statistical value of I² depends on the size of its influence, and the strength for the evidence of heterogeneity (e.g., the p-value of the Chi2 test). We performed sensitivity analysis on the comparison results with very high heterogeneity. The impact of clinical and statistical heterogeneity on the results will be considered when discussing the results of the analysis.
3. Results
3.1. Search results and study description
The literature search initially identified 643 articles. Of these, 55 duplicate articles and 571 articles that were not relevant to the selection criteria were excluded. Finally, 17 studies were included in our meta-analysis (Figure 1), and the characteristics of all included RCTs are shown in Table 1 (20%–36%). A total of 1,275 cases of cancer pain were included, with study sample sizes ranging from 7 to 360. 11 trials were published in Chinese and another 6 in English. 4 trials used analgesics (three-step analgesic ladder) as comparators (26, 28, 31, 34), 3 trials applied sham controls including minimal or superficial needling at non-acupuncture points (21, 22, 25), and the remaining few trials used other conventional Western medications or usual care.
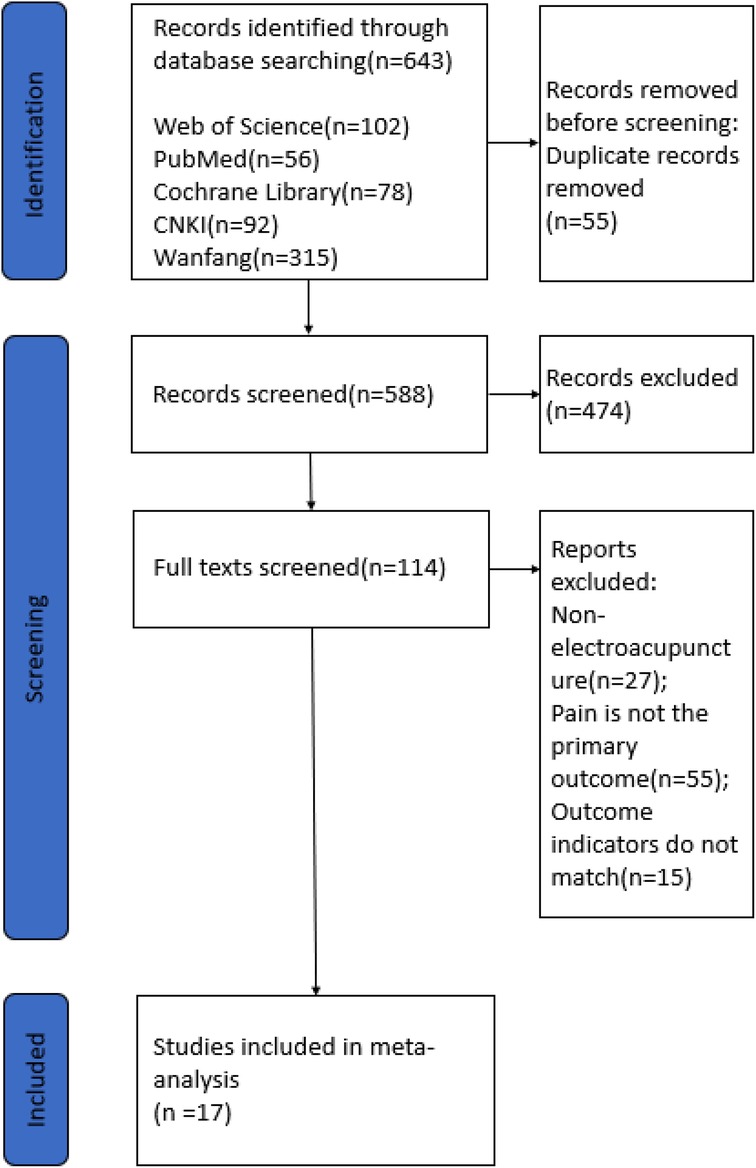
Figure 1. Flowchart of the literature review and selection process.
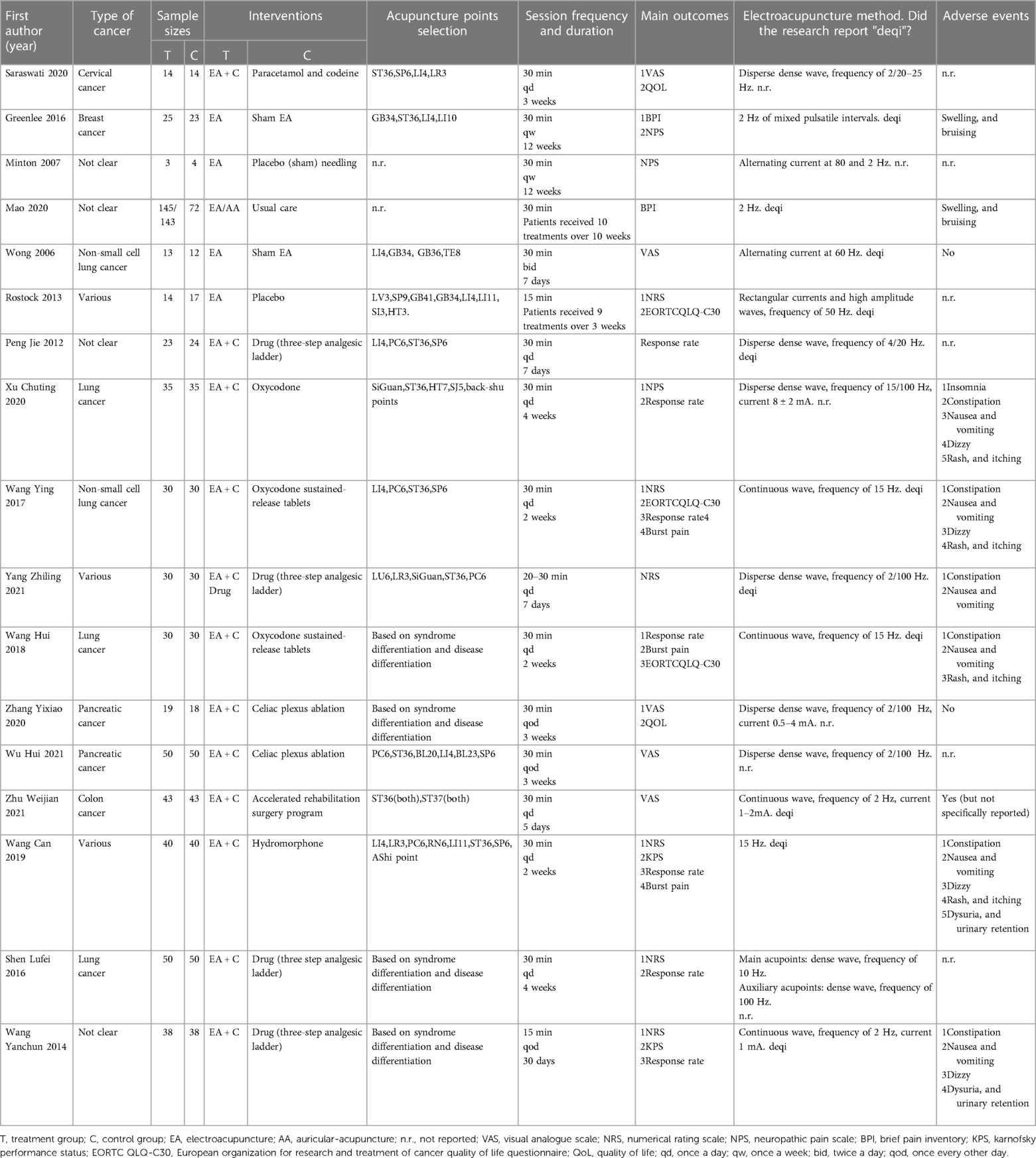
Table 1. Basic information of the included literature.
Zusanli (ST36), Hegu (LI4), Sanyinjiao (SP6), and the extraordinary point Siguan were the most frequently used acupoints. Eleven studies reported “deqi” (21, 23–26, 29–32, 34, 36), a sensation of needling perceived as soreness, numbness, or distension, which is usually achieved by manipulating acupuncture needles to obtain the desired therapeutic effect, and seven other studies did not mention this effect (20, 22, 27, 28, 33, 35). In most studies, patients were treated for 30 min per session. The duration of time patients received electroacupuncture treatment ranged from 1 to 12 weeks. In terms of electroacupuncture waveforms, six studies used disperse dense wave (20, 26, 27, 33–35), four studies used continuous waves (30–32, 36), and one study used only dense waves (28), with the remaining trials not specified; in terms of electroacupuncture frequency, it ranged from 2 hz to 100 hz, in terms of applying electroacupuncture current intensity, only a few studies specifically reported the intensity of the current used (27, 31, 35, 36), most of the other trials stated the maximum intensity within the patients’ tolerance.
3.2. Risk of bias
Risk of bias graph could be founded in Figure 2. Risk of bias summary could be located in Figure 3.
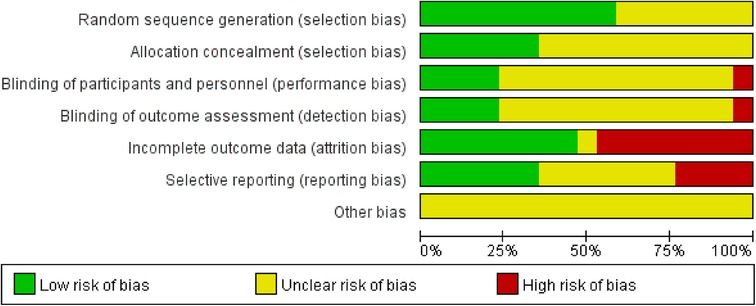
Figure 2. Assessment of cochrane risk of bias presented as percentages across all included studies.
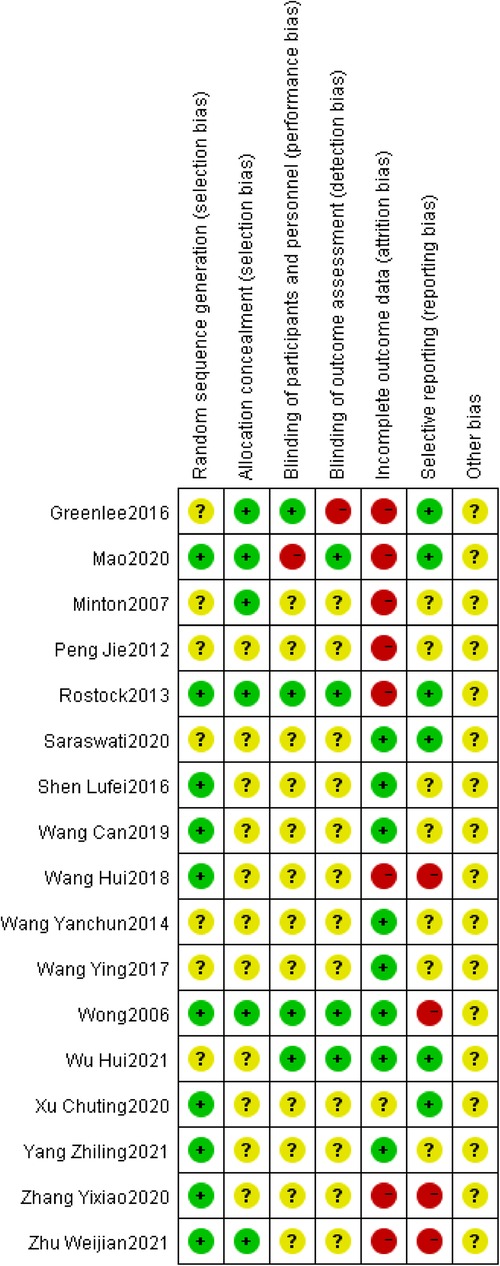
Figure 3. Cochrane risk of bias summary for each included study.
3.2.1. Selection bias
Of the 17 RCTs included, 7 RCTs did not describe problems associated with the randomization process (20–22, 26, 31–33). 7 RCTs used a table of random numbers (27–30, 34–36), Mao et al. performed randomization by a secure system with full allocation hiding (23), and Wong et al. used a computer-generated random sequence (25). Rostock et al. performed randomization by nonstratified block with randomly varying lengths (24). 6 studies used allocation hiding and reported the details (21–25, 36). The remaining trials did not report specific methods of allocation concealment implementation.
3.2.2. Performance bias
Because the RCTs included in this study involved treatment and control groups that differed significantly in the form and manipulation of the intervention, it was more difficult to apply blinding to participants or personnel, and only four RCTs used correct blinding for participants and personnel (21, 24, 25, 33).
3.2.3. Detection bias
Only 4 of the 17 RCTs included implemented correct blinding of assessors for outcome indicators (23–25, 33), 1 study did not use blinding of outcome assessment (21), and the remaining trials did not report the specific method of blinding implementation.
3.2.4. Attrition bias
Eight RCTs reported exit or withdrawal information appropriately (21–24, 26, 30, 35, 36), however, missing data were not addressed, so they were rated as high risk of bias in the attrition bias evaluation. Eight trials did not have missing data (20, 25, 28, 29, 31–34). One trial did not report the presence or absence of missing data and was judged to be at uncertain risk (27).
3.2.5. Reporting bias
Of the 17 RCTs included, 6 RCTs reported that their study teams pre-defined the study protocol and were therefore evaluated as low risk in reporting bias (20, 21, 23, 24, 27, 33). 4 RCTs did not report the full study protocol and were therefore judged to be at high risk (25, 30, 35, 36). The remaining 7 trials did not report relevant information and were therefore evaluated as unclear in the risk of bias judgment.
3.2.6. Other bias
This study evaluated publication bias, study design, and confounding bias in the included randomized controlled trials, and the risk of other bias was not clear for all trials because the content of the relevant information was not sufficient.
3.3. Primary outcome indicators
3.3.1. VAS score
Five studies reported post-treatment VAS scores (20, 25, 33, 35, 36), with 139 cases in the treatment group and 137 cases in the control group overall. Heterogeneity tests for meta-analysis showed a statistically significant difference between studies with I² = 97%. VAS scores were lower in the treatment group than in the control group, with a statistically significant difference (276 participants, MD = −1.41, 95% CI: −2.42 to −0.41, P = 0.006; see Figure 4).
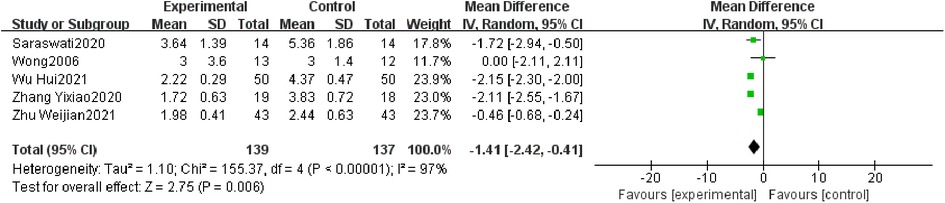
Figure 4. Forest plot of VAS score.
3.3.2. NRS score
Seven studies reported post-treatment NRS scores (24, 27–29, 31, 32, 34), with 237 cases in the treatment group and 240 cases in the control group overall. Heterogeneity tests for meta-analysis showed that I² = 90%. NRS scores were lower in the treatment group than in the control group, with a statistically significant difference (477 participants, MD = −1.19, 95% CI: −1.72 to −0.66, P < 0.0001; see Figure 5).
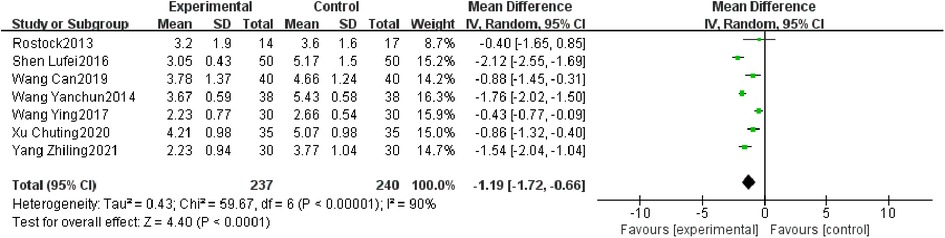
Figure 5. Forest plot of NRS score.
3.3.3. Other pain scores
The Neuropathic Pain Scale (NPS) (21, 22), Brief Pain Inventory (BPI) (21, 23) and Karnofsky performance status (KPS) (29, 31) were reported in two studies each, so they were combined in a single icon and analyzed using a random-effects model in this study. Heterogeneity tests for meta-analysis of the NPS scores showed that I² = 73%, the NPS scores in the treatment group were not lower than those in the control group, the difference was not statistically significant and did not indicate that the treatment group improved the NPS scores better than the control group (55 participants, MD = 4.27, 95% CI: −14.50 to 23.04, P = 0.66;). Heterogeneity tests for meta-analysis of BPI scores showed that I² = 76%, and the BPI scores were statistically lower in the treatment group than in the control group (245 participants, MD = −1.39, 95% CI: −3.31 to 0.54, P = 0.16). KPS scores were higher in the treatment group than in the control group, indicating a better improvement in KPS scores in the treatment group than in the control group (156 participants, MD = 5.48, 95% CI: 3.27 to 7.69, P < 0.00001; see Figure 6).
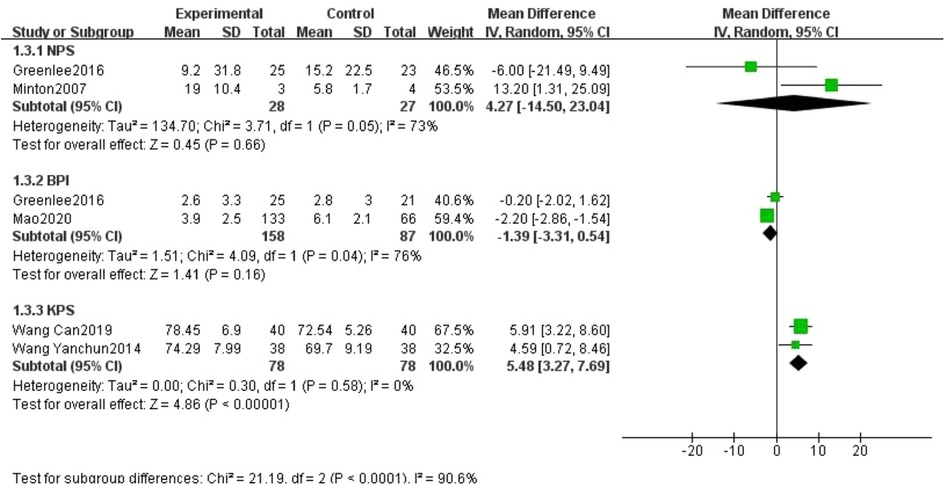
Figure 6. Forest plot of other pain score.
3.4. Secondary outcome indicators
3.4.1. Burst pain
Three studies reported the times of burst pain (29, 30, 32). The combined statistical results showed that the incidence of burst pain was lower in the treatment group than in the control group, with a statistically significant difference (200 participants, MD = −2.66, 95% CI: −3.32 to −1.99, P < 0.00001; see Figure 7).

Figure 7. Forest plot of times of burst pain.
3.4.2. Response rates
Seven studies reported response rates for pain relief after treatment (26–32). Of 246 cases in the treatment group, 224 had a valid response; of 247 cases in the control group, 187 had a valid response. The overall response rate of the treatment group was better than the control group, with a statistically significant difference, (493 participants, RR = 1.17, 95% CI: 1.09 to 1.26, P < 0.0001; see Figure 8).
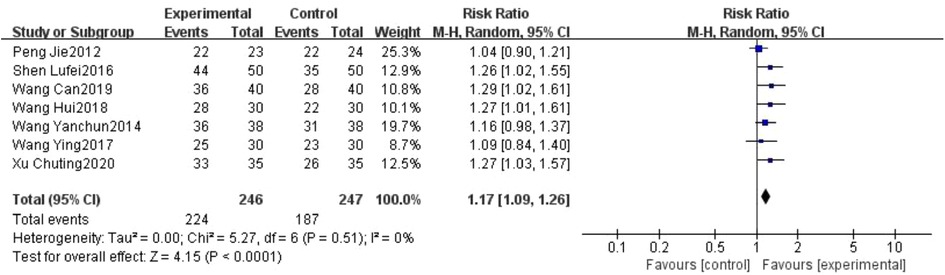
Figure 8. Forest plot of the response rates.
3.4.3. Side effect rates
Side effects mainly included swelling, bruising, constipation, nausea, vomiting, dysuria, urinary retention, dizziness, rash, itching and insomnia. 2 studies reported the number of cases of swelling and bruising (21, 23), 6 studies reported the number of cases of constipation (27, 29–32, 34), 6 studies reported the number of cases of nausea and vomiting (27, 29–32, 34), 2 studies reported the number of cases of difficulty urinating and urinary retention (29, 31), 4 studies reported the number of cases of dizzy (27, 29, 31, 32), 4 studies reported the number of cases of rash and itching (27, 29, 30, 32) and 1 study reported the number of cases of insomnia (27). The combined statistical results showed that the incidence of constipation (406 participants, RR = 0.42, 95% CI: 0.18 to 0.96, P = 0.04) and nausea and vomiting (406 participants, RR = 0.51, 95% CI: 0.39 to 0.68, P < 0.00001) were significantly lower in the treatment group compared with the control group, but the incidence of swelling, and bruising (265 participants, RR = 7.25, 95% CI: 0.89 to 58.84, P = 0.06) was higher; several other adverse reactions were not statistically significant, perhaps due to the small sample size. But overall, adverse reactions occurred in 109 out of 967 cases in the treatment group and in 192 out of 892 cases in the control group. The number of adverse reactions that occurred in the treatment group was lower than in the control group, and the difference was statistically significant, (1,859 participants, RR = 0.51, 95% CI: 0.39 to 0.67, P < 0.00001; see Figure 9).
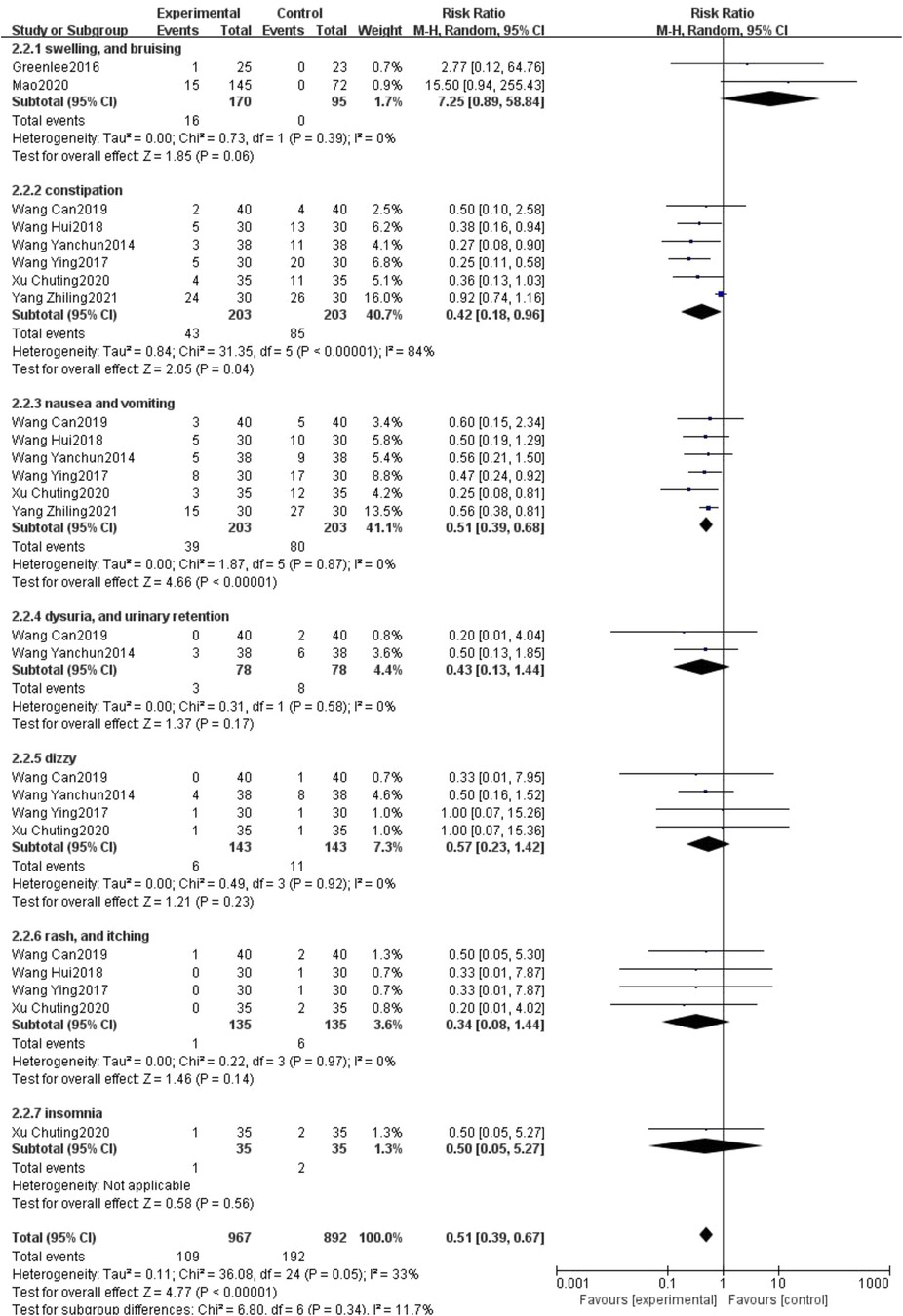
Figure 9. Forest plot of side effect rates.
3.5. Sensitivity analysis
The results of the quantitative synthesis of our involved outcome indicators showed high heterogeneity for only two outcome indicators, VAS score and NRS score, for which we performed sensitivity analysis. While the quantitative synthesis results of the other outcome indicators had low heterogeneity or involved only 2 trials, so sensitivity analysis could not be performed.
Sensitivity analyses showed that we excluded each of the five trials involved in the VAS score and found a significant decrease in inter-study heterogeneity after Zhu Weijian2021 (36) was excluded, and the combined results of the four trials showed I² = 32%, MD = −2.07, 95% CI: −2.38 to −1.76, P < 0.00001.
The results of our sensitivity analysis of the NRS scores showed that combining four of the trials (24, 27, 29, 32) showed I² = 6%, MD = −0.63, 95% CI: −0.89 to −0.38, P < 0.00001 and combining the other three (28, 31, 34) showed I² = 38%, MD = −1.81, 95% CI: −2.09 to −1.53, P < 0.00001. Heterogeneity was also greatly reduced after splitting the analysis into these two parts.
4 . Discussion
The purpose of this systematic review was to critically assess the effectiveness of electroacupuncture for cancer pain by updating and refining new evidence. The current meta-analysis based on 17 studies showed that electroacupuncture was effective in relieving cancer pain in cancer patients, and that compared with controls, electroacupuncture for cancer pain resulted in lower several major pain scores such as VAS scores and NRS scores, lower rates of adverse effects such as constipation, nausea, and vomiting, and fewer times of burst pain.
The mechanism of electroacupuncture for cancer pain is not fully understood, but it may involve multiple pathways that modulate pain signaling and inflammatory responses at different levels of the nervous, immune, and endocrine systems (16). Han et al. revealed the neural mechanism of broad-spectrum analgesia by electroacupuncture: electroacupuncture stimulates specific acupuncture points on the body with electrical impulses, activating surrounding nerve fibers that transmit signals to the spinal cord and brain, which in turn activates the endogenous opioid system, releasing natural analgesics such as endorphins, enkephalins, and dynorphins in the brain and spinal cord (37). In addition to activating the neurological secretion of opioid substances, electroacupuncture acts synergistically with endogenous opioids to inhibit astrocyte activation by suppressing spinal glial fibrillary acidic protein (GFAP) expression, thereby reducing bone cancer pain in rats (38). It's also reported to relieve morphine tolerance of rats with breast cancer by promoting the internalization of µ-opioid receptor (MOR) and Rab5, a protein involved in endocytosis, locating in the locus coeruleus region (39). As for immunology pathways, in a study of a rat model of prostate cancer bone metastases, electroacupuncture was found to inhibit pro-inflammatory cytokines, such as IL-1β, which attenuate nociceptive receptor sensitivity and inhibit pain transmission (40). Electroacupuncture can also directly downregulate the expression of nociceptive receptors in a rat model of cancer pain, such as P2X3 receptors in the dorsal root ganglion of rats (41). Electroacupuncture can modulate immune cells, such as macrophages (42), mast cells (43) and T cells (44), to reduce pain-causing substances produced by inflammation and tissue injury. These mechanisms can work in concert to reduce the intensity of cancer pain and improve the quality of life of cancer survivors.
We found some aspects that need improving in the clinical research of our topic. Most of the included trials lacked a description of the electroacupuncture treatment protocol, such as the sensation of “deqi”, the depth of needling, and the corresponding parameters of electroacupuncture; in addition, the optimal dose of electroacupuncture is not known. This not only limits the quality of the studies, but also raises the question of whether electroacupuncture adequately elicited a functional response and exerted sufficient therapeutic effects to control cancer pain in the included trials. Therefore, we strongly recommend that researchers should clearly validate and report the sensation of gaining breath and the depth of needling in future studies and unify electroacupuncture parameters as much as possible. In addition, future RCTs should focus on exploring the effective dose of electroacupuncture for cancer pain. To achieve this goal, future studies should include sufficiently large samples, extend the duration of treatment and follow-up, and standardize the efficacy evaluation system. Several RCTs had no adverse effects (25, 35), which seems to conflict with research ethics and guidelines for reporting clinical trials. Acupuncture is not completely free of adverse reactions (45). Failure to report adverse effects in clinical trials would create inaccuracies regarding the safety of this treatment. Subjective symptom alleviation of patients' initial cancer pain status was reported in all included RCTs. Due to the absence of objective assessment methods, studies on pain frequently rely on patient testimonies. A methodical, scientific approach is consequently required for the evaluation of cancer pain. Such a strategy must incorporate a thorough study of the available literature, expert judgment and consensus, a strict translation procedure, and thorough validation (46). The application of such a strategy could raise the bar for evaluating cancer pain.
However, this meta-analysis has several limitations. First, the treatment protocols and selected parameters for electroacupuncture were not consistent among the included studies. Second, some of the adverse effects and the differences in NPS scores between groups were not statistically significant due to the small sample size involved, which may be related to the small number of relevant studies available. Third, methodological limitations, although we made considerable efforts to retrieve all RCTs on this issue, there were selection, performance, and detection biases in the included trials that affected the strength of the evidence and limited the internal validity of this review. Therefore, we searched 5 databases to minimize bias in this regard. Nonetheless, this review has several strengths. We are the first meta-analysis on electroacupuncture for cancer pain and include only RCTs.
In conclusion, this study demonstrates the particular advantages of electroacupuncture in the treatment of cancer pain. Rigorous RCTs should be designed and conducted in the future, and these studies need to incorporate accepted trial design and reporting standards. Specifically, they should be based on appropriate sample size calculations, use validated outcome measures, control for nonspecific effects, and adhere to modern human research ethics to further demonstrate the exact efficacy of electroacupuncture.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
Thesis guidance: LQJ. Essay writing: JNZ and WZW. Data analysis and collation: JNZ, WZW and YHR. Illustration of the paper: YY. Table design: JNZ and WZW. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor LM declared a past co-authorship with the author JNZ.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2023.1186506/full#supplementary-material.
References
1. World Health Organization. What Is Cancer? (2023). Available at: https://www.who.int/health-topics/cancer (Accessed March 12, 2023).
2. World Health Organization. Cancer. (2023). Available at: https://www.who.int/news-room/fact-sheets/detail/cancer (Accessed March 12, 2023).
3. Schmidt BL, Hamamoto DT, Simone DA, Wilcox GL. Mechanism of cancer pain. Mol Interv. (2010) 10(3):164–78. doi: 10.1124/mi.10.3.7
4. Snijders RAH, Brom L, Theunissen M, van den Beuken-van Everdingen MHJ. Update on prevalence of pain in patients with cancer 2022: a systematic literature review and meta-analysis. Cancers. (2023) 15(3):591. doi: 10.3390/cancers15030591
5. Deng G. Integrative medicine therapies for pain management in cancer patients. Cancer J. (2019) 25(5):343–8. doi: 10.1097/PPO.0000000000000399
6. Thapa D, Rastogi V, Ahuja V. Cancer pain management-current status. J Anaesthesiol Clin Pharmacol. (2011) 27(2):162–8. doi: 10.4103/0970-9185.81820
7. World Health Organization. Cancer pain relief: With a guide to opioid availability. 2nd edn. Geneva, Switzerland: World Health Organization (1996). 12–3. Available at: http://apps.who.int/iris/bitstream/10665/37896/1/9241544821.pdf
8. Janah A, Bouhnik AD, Touzani R, Bendiane MK, Peretti-Watel P. Underprescription of step III opioids in French cancer survivors with chronic pain: a call for integrated early palliative care in oncology. J Pain Symptom Manage. (2020) 59(4):836–47. doi: 10.1016/j.jpainsymman.2019.10.027
9. Benyamin R, Trescot AM, Datta S, Buenaventura R, Adlaka R, Sehgal N, et al. Opioid complications and side effects. Pain Physician. (2008) 11(2 Suppl):S105–120. doi: 10.36076/ppj.2008/11/S105
10. Vitry A, Forte G, White J. Access to controlled medicines in low-income countries: listening to stakeholders in the field. Int J Health Serv. (2021) 51(3):404–11. doi: 10.1177/0020731420906748
11. Li J, Kou Y, Zhang S, Wang K. Effect of acupotomy combined with electroacupuncture therapy on finger mobility and pain relief in patients with carpal tunnel syndrome. Comput Math Methods Med. (2022) 2022:2550875. doi: 10.1155/2022/2550875
12. Yang J, Wahner-Roedler DL, Zhou X, Johnson LA, Do A, Pachman DR, et al. Acupuncture for palliative cancer pain management: systematic review. BMJ Support Palliat Care. (2021) 11(3):264–70. doi: 10.1136/bmjspcare-2020-002638
13. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. (2014) 120(2):482–503. doi: 10.1097/ALN.0000000000000101
14. Amorim D, Amado J, Brito I, Fiuza SM, Amorim N, Costeira C, et al. Acupuncture and electroacupuncture for anxiety disorders: a systematic review of the clinical research. Complement Ther Clin Pract. (2018) 31:31–7. doi: 10.1016/j.ctcp.2018.01.008
15. Garcia MK, McQuade J, Haddad R, Patel S, Lee R, Yang P, et al. Systematic review of acupuncture in cancer care: a synthesis of the evidence. J Clin Oncol. (2013) 31(7):952–60. doi: 10.1200/JCO.2012.43.5818
16. Li Y, Yang M, Wu F, Cheng K, Chen H, Shen X, et al. Mechanism of electroacupuncture on inflammatory pain: neural-immune-endocrine interactions. J Tradit Chin Med. (2019) 39(5):740–9. doi: 10.19852/j.cnki.jtcm.2019.05.017
17. Zhu D, Bai J, Zhang X, Xu X, Zhang J. Research progress on quantification of electroacupuncture parameters.Chin Acupunct Moxibustion. (2015) 35(05):525–8. doi: 10.13703/j.0255-2930.2015.05.032
18. Park S, Lyu YR, Park SJ, Oh MS, Jung IC, Lee EJ. Electroacupuncture for post-thoracotomy pain: a systematic review and meta-analysis. PLoS One. (2021) 16(7):e0254093. doi: 10.1371/journal.pone.0254093
19. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane Collaboration's tool for assessing risk of bias in randomised trials. Br Med J. (2011) 343:d5928. doi: 10.1136/bmj.d5928
20. Saraswati W, Wardani R, Suhatno S, Hartono P, Imandiri A. The effect of electroacupuncture therapy on pain, plasma β-endorphin, and quality of life of stage III cervical cancer patients: a randomized control trial. J Acupunct Meridian Stud. (2020) 14(1):4–12. doi: 10.51507/j.jams.2021.14.1.4
21. Greenlee H, Crew KD, Capodice J, Awad D, Buono D, Shi Z, et al. Randomized sham-controlled pilot trial of weekly electro-acupuncture for the prevention of taxane-induced peripheral neuropathy in women with early stage breast cancer. Breast Cancer Res Treat. (2016) 156(3):453–64. doi: 10.1007/s10549-016-3759-2
22. Minton O, Higginson IJ. Electroacupuncture as an adjunctive treatment to control neuropathic pain in patients with cancer. J Pain Symptom Manage. (2007) 33(2):115–7. doi: 10.1016/j.jpainsymman.2006.09.011
23. Mao JJ, Liou K, Panageas K, Baser RE, Romero SAD, Li QS, et al. Effects of electroacupuncture and auricular acupuncture for chronic pain in cancer survivors: the PEACE randomized controlled trial. J Clin Oncol. (2020) 38 (15):720–7. doi: 10.1001/jamaoncol.2021.0310
24. Rostock M, Jaroslawski K, Guethlin C, Ludtke R, Schroeder S, Bartsch HH. Chemotherapy-induced peripheral neuropathy in cancer patients: a four-arm randomized trial on the effectiveness of electroacupuncture. Evid Based Complement Altern Med. (2013) 2013:349653. doi: 10.1155/2013/349653
25. Wong RHL, Lee TW, Sihoe ADL, Wan IYP, Ng CSH, Chan SKC, et al. Analgesic effect of electroacupuncture in postthoracotomy pain: a prospective randomized trial. Ann Thorac Surg. (2006) 81(6):2031–6. doi: 10.1016/j.athoracsur.2005.12.064
26. Peng J, Wang W, Zhou R, Shen W, Li J. Clinical study on integrated acupuncture and medication in treating moderate and severe cancer pain. Shanghai J Acupunc Moxibustion. (2012) 31(4):236–8. doi: 10.3969/j.issn.1005-0957.2012.04.236
27. Xu C, Li X, Tan Y. Observation on the effect of dilatational wave electroacupuncture combined with western medicine in the treatment of pain in patients with lung cancer in 35 cases. Zhejiang J Traditional Chin Med. (2020) 55(4):295–6. doi: 10.13633/j.cnki.zjtcm.2020.04.035
28. Shen L, Chen W, Lv X, Liu J, Yang X, Yao M, et al. Study on the effect of electro acupuncture in improving sleep quality of patients with lung cancer-related pain. J Med Res. (2016) 45(6):87–90. doi: 10.11969/j.issn.1673-548X.2016.06.022
29. Wang C. Clinical study on electroacupuncture combined with hydromorphone for moderate and severe cancer pain of stagnation of static blood type. J New Chin Med. (2019) 51(10):242–4. doi: 10.13457/j.cnki.jncm.2019.10.069
30. Wang H, Wang Y, Fang H. Thirty cases of patients with lung cancer pain treated with electro-acupuncture based on syndrome differentiation. Henan Tradit Chin Med. (2018) 38(3):454–7. doi: 10.16367/j.issn.1003-5028.2018.03.0120
31. Wang Y, Chen X, Wei Z, Wang X. Low frequency electroacupuncture combined with three-step analgesic drugs in the treatment of 38 cases of cancer pain. Tradit Chin Med Res. (2014) 27(5):55–7. doi: 10.3969/j.issn.1001-6910.2014.05.30
32. Wang Y, Wang X, Wang H, Zhang Y, Fang H. Electroacupuncture combined with oxycodone sustained-release tablets in the treatment of advanced non-small cell lung cancer pain in 30 cases. Zhejiang J Tradit Chin Med. (2017) 52(9):684–5. doi: 10.3969/j.issn.0411-8421.2017.09.039
33. Wu H, Hu B. Study on analgesic efficacy of celiac plexus lesion combined with electroacupuncture in patients with refractory pancreatic cancer pain. Family Med Med Sel. (2021) (3):392.
34. Yang Z, Gong Y. Clinical observation of electroacupuncture combined with opioids in the treatment of cancerous pain. J Oncol Chin Med. (2021) 3(3):30–5. doi: 10.1007/s12032-021-01474-1
35. Zhang Y, Wan H, Wang Z, Huang L, Qu P, Liu C, et al. Observation on the efficacy of celiac plexus ablation combined with electroacupuncture in the treatment of pain induced by refractory pancreatic cancer. China Modern Doctor. (2020) 58(15):144–7.
36. Zhu W, Wang Y, Gao C, Zhou J, Lu J, Chen X, et al. Influence of electroacupuncture treatment on recovery after colon cancer surgery. Shanghai J Acupunc Moxibustion. (2021) 40(4):416–20. doi: 10.13460/j.issn.1005-0957.2021.04.0416
37. Han JS. Acupuncture and endorphins. Neurosci Lett. (2004) 361(1–3):258–61. doi: 10.1016/j.neulet.2003.12.019
38. Kuai L, Chen H, Zhang TT, Yang HY. Study on dose-effect relationship of electroacupuncture with different current intensities alleviating tibial cancer pain and inhibition of expression of spinal GFAP in rats. Zhongguo Zhen Jiu. (2012) 32(4):331–7. doi: 10.13703/j.0255-2930.2012.04.017
39. Shi RY, Fu TF, Cai YQ, Du JY, Fang JF, Fang JQ, et al. Electroacupuncture intervention relieves pain possibly by promoting MOR endocytosis in locus coeruleus in bone cancer pain rats with morphine tolerance. Zhen Ci Yan Jiu. (2019) 44(3):161–9. doi: 10.13702/j.1000-0607.180635
40. Zhang RX, Li A, Liu B, Wang L, Ren K, Qiao JT, et al. Electroacupuncture attenuates bone cancer pain and inhibits spinal interleukin-1 beta expression in a rat model. Anesth Analg. (2007) 105(5):1482–8. table of contents. doi: 10.1213/01.ane.0000284705.34629.c5
41. Tian SX, Xu T, Shi RY, Cai YQ, Wu MH, Zhen SJ, et al. Analgesic effect of electroacupuncture on bone cancer pain in rat model: the role of peripheral P2X3 receptor. Purinergic Signal. (2023) 19(1):13–27. doi: 10.1007/s11302-022-09861-7
42. Wang Y, Gehringer R, Mousa SA, Hackel D, Brack A, Rittner HL. CXCL10 Controls inflammatory pain via opioid peptide-containing macrophages in electroacupuncture. PLoS One. (2014) 9(4):e94696. doi: 10.1371/journal.pone.0094696
43. Ulloa L, Quiroz-Gonzalez S, Torres-Rosas R. Nerve stimulation: immunomodulation and control of inflammation. Trends Mol Med. (2017) 23(12):1103–20. doi: 10.1016/j.molmed.2017.10.006
44. Xu Z, Zhu Y, Shen J, Su L, Hou Y, Liu M, et al. Pain relief dependent on IL-17-CD4+ T cell-β-endorphin axis in rat model of brachial plexus root avulsion after electroacupuncture therapy. Front Neurosci. (2020) 14:596780. doi: 10.3389/fnins.2020.596780
45. Cho E, Kim W. Effect of acupuncture on diabetic neuropathy: a narrative review. Int J Mol Sci. (2021) 22(16):8575. doi: 10.3390/ijms22168575
Keywords: electroacupuncture, cancer pain, systematic review, complementary and alternative medicine, meta-analysis, rct
Citation: Zhang J, Wu W, Ren Y, Yuan Y and Jia L (2023) Electroacupuncture for the treatment of cancer pain: a systematic review and meta-analysis of randomized clinical trials. Front. Pain Res. 4:1186506. doi: 10.3389/fpain.2023.1186506
Received: 14 March 2023; Accepted: 17 April 2023;
Published: 15 May 2023.
Edited by:
Linqing Miao, Beijing Institute of Technology, ChinaReviewed by:
Cheng-Hao Tu, China Medical University, TaiwanHaowa Li, Capital Medical University, China
Li Tie, Changchun University of Chinese Medicine, China
© 2023 Zhang, Wu, Ren, Yuan and Jia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liqun Jia TGlxdW4tamlhQEhvdG1haWwuY29t
†These authors share first authorship