 Divya Kanchibhotla
Divya Kanchibhotla Saumya Subramanian†
Saumya Subramanian† Deeksha Singh
Deeksha Singh
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pain Res. , 30 March 2023
Sec. Musculoskeletal Pain
Volume 4 - 2023 | https://doi.org/10.3389/fpain.2023.1107669
This article is part of the Research Topic Yoga for Pain Relief View all 5 articles
Menstrual pain also known as dysmenorrhea is one of the most common and underrated gynecological disorders affecting menstruating women. Although the symptoms and impact might vary greatly, it is defined by cramps in the lower abdomen and pain that radiates to lower back and thighs. In some cases it is also accompanied by nausea, loose stool, dizziness etc. A primary narrative review was conducted on the impact of yoga on dysmenorrhea experienced by women. The English-language literature published until 2022 was searched across databases such as PubMed, Google Scholar and Scopus. “Yoga” and “menstrual pain” OR “dysmenorrhea” were used as keywords for the search across several databases. A total of 816 title searches were obtained across all the database searches. This review article included 10 studies based on the selection criteria. The studies examined the impact of a varied set of 39 asanas, 5 pranayamas and Yoga nidra on dysmenorrhea. The studies demonstrated a significant relief in dysmenorrhea among those who practiced Yoga (asanas/pranayama/yoga nidra) with improved pain tolerance and reduced stress levels. Regulating the stress pathways through yoga was found to be a key in regulating hormonal balance and reduction in dysmenorrhea.
Dysmenorrhea is a common issue in menstruating women where the most typical symptoms are cramps and lower abdominal pain. Several experts agree that an aberrant increase in the endometrium's synthesis and vasoactive prostaglandins may cause myometrial hyperactivity, uterine tissue ischemia and discomfort, causing the monthly pain (1). Dysmenorrhea is also accompanied by a number of other premenstrual disorders. Primary dysmenorrhea is a common disorder affecting the Quality of Life (QOL) of many women due to intense pain and related social and psychological implications (2). Appropriate therapy and management are required due to the decreased quality of life, ineffective working hours, and mood swings caused by dysmenorrhea.
In order to improve women's health, several complementary and alternative strategies have been employed to reduce dysmenorrhea, which includes the use of medicinal herbs with analgesic properties (3). Typically, non-steroid anti-inflammatory medications or oral contraceptives are used to treat dysmenorrhea (4). Transcutaneous electrical nerve stimulation, acupuncture, acupressure, topical heat, behavioral interventions, relaxation, herbal and dietary therapy are just a few of the alternatives for dysmenorrhea that are receiving more attention in recent years (5). Among the several complementary therapies accepted, practice of yoga has been added to the list. Yoga is a type of mind-body exercise that combines physical body with a conscious mental emphasis. Yoga is regarded as one of the best holistic stress management approaches since it causes a series of physiological changes in the body that lessen the stress and pain response (6). In case of dysmenorrhea, yoga suppresses the pain by lowering the level of prostaglandin production and myometrial ischemia (1, 2).
Over the years, a number of hypotheses have been put forth to evaluate the cause of primary dysmenorrhea. Experimental and clinical research has revealed the release of uterine prostaglandins which play a significant role in the progression of primary dysmenorrhea (7). NSAIDs nonsteroidal anti-inflammatory drugs have shown to be effective in reducing the prostaglandin levels so produced during the bleeding (8). As a result of endometrial shedding during menstruation, prostaglandins are released along with the blood. This is accompanied by other enzyme release that breaks down the cell membranes (9). This release of prostaglandin stimulates myometrial contraction and constricts small endometrial blood vessels, resulting in tissue ischemia, endometrial disintegration, bleeding and pain (10) (Figure 1). Another study also suggested an upregulated cyclooxygenase (COX) enzyme activity as a major contributor to the pain experienced by women with primary dysmenorrhea. This is because COX aids in the production of prostaglandins (11).
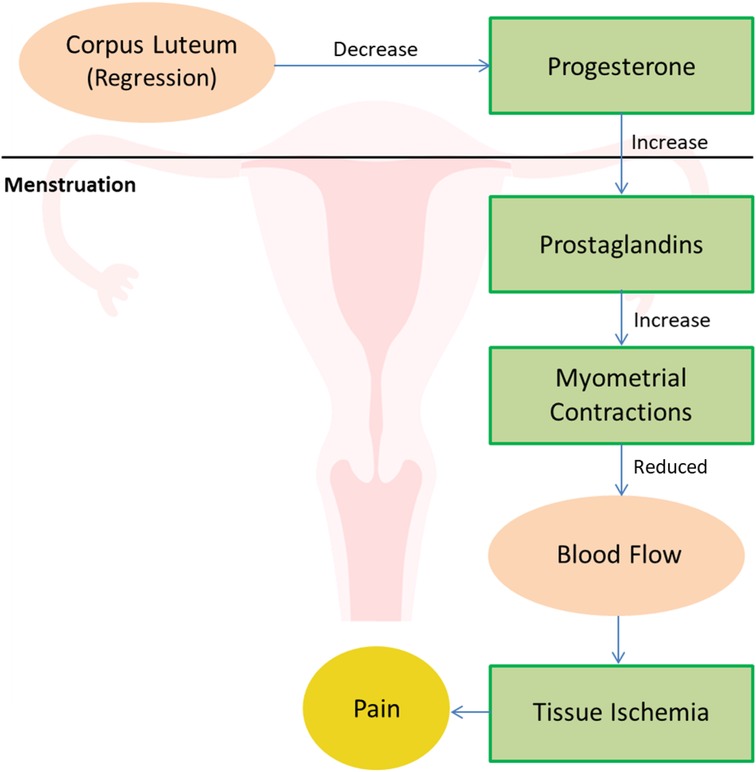
Figure 1. Physiology of dysmenorrhea.
The clinical feature of dysmenorrhea due to intense vasoconstriction includes cramping that typically begins a few hours before the onset of bleeding and can last for several hours or days after the onset of bleeding (12). The pain originates in the lower abdomen and may spread to the lower back and thighs (13). The pain is occasionally attributed to stretching of the peritoneum surrounding the ovary which also involves contraction-induced nerve impulses (14). Changes in bowel habits, nausea, exhaustion, dizziness, and headaches may be concomitant effects of dysmenorrhea (15).
In addition, vasopressin also contributes to vasoconstriction. Increased intrauterine pressure, vascular constriction, and reduced uterine blood flow, all contribute to tissue ischemia, leading to dysmenorrhea (16). The small afferent fibers originating from pelvic organs accompanied by sympathetic nerves are the carriers of pain information (17). However, any therapeutic strategy to suppress pain perception from these areas is challenging since the exact pathways of dysmenorrhea is unknown (18).
Several randomized, placebo-controlled studies have demonstrated that patients with presumed primary dysmenorrhea typically start their treatment with nonsteroidal anti- inflammatory medications (NSAIDs), which function as COX (cyclooxygenase) inhibitors (13). This in turn reduces the levels of prostaglandins and ceases tissue ischemia in the pelvic region (19). Transvaginal rings and patches reduce dysmenorrhea hence act as effective treatments for primary dysmenorrhea (20). Depot medroxyprogesterone acetate (an injectable progestin-only contraceptive) and oral contraceptives have also shown to be efficient for the treatment (21). The effectiveness of lifestyle-modification therapies in the management of dysmenorrhea has not been extensively studied. One crossover study comparing a low-fat vegetarian diet vs. placebo pill revealed that women in the intervention group experienced dysmenorrhea for shorter periods of time and with less intensity (22). Another double blind RCT studied thiamine, an amino acid elevating Vitamin B1, as a treatment among 500 women with moderate to severe symptoms of dysmenorrhea. The study showed significant relief of pain among the women in the intervention group compared to women in the placebo group (23). Another study successfully demonstrated the benefits of vasopressin-receptor as an antagonist for the treatment of dysmenorrhea (24). Psychotherapy, hypnotherapy, heat patches, and transcutaneous electrical stimulation are a few non-pharmacologic pain management techniques that are seen to be helpful (25). Surgical alternatives for pain relief include uterosacral ligament section and presacral neurectomy, however do not show a long-term pain alleviation (26). Further, surgical interventions can give rise to problems such as severe bleeding and constipation. These might be connected to the regrowth of nerves or the transmission of pain signals via other pathways (27). Therefore, surgical therapies for dysmenorrhea are typically not prescribed.
Hormonal contraception, topical heat, thiamine, vitamin E, or fish oil supplements; a low- fat vegetarian diet and acupressure are few viable alternatives that have been explored in several combinations (28).
Refer to Table 1 for further details
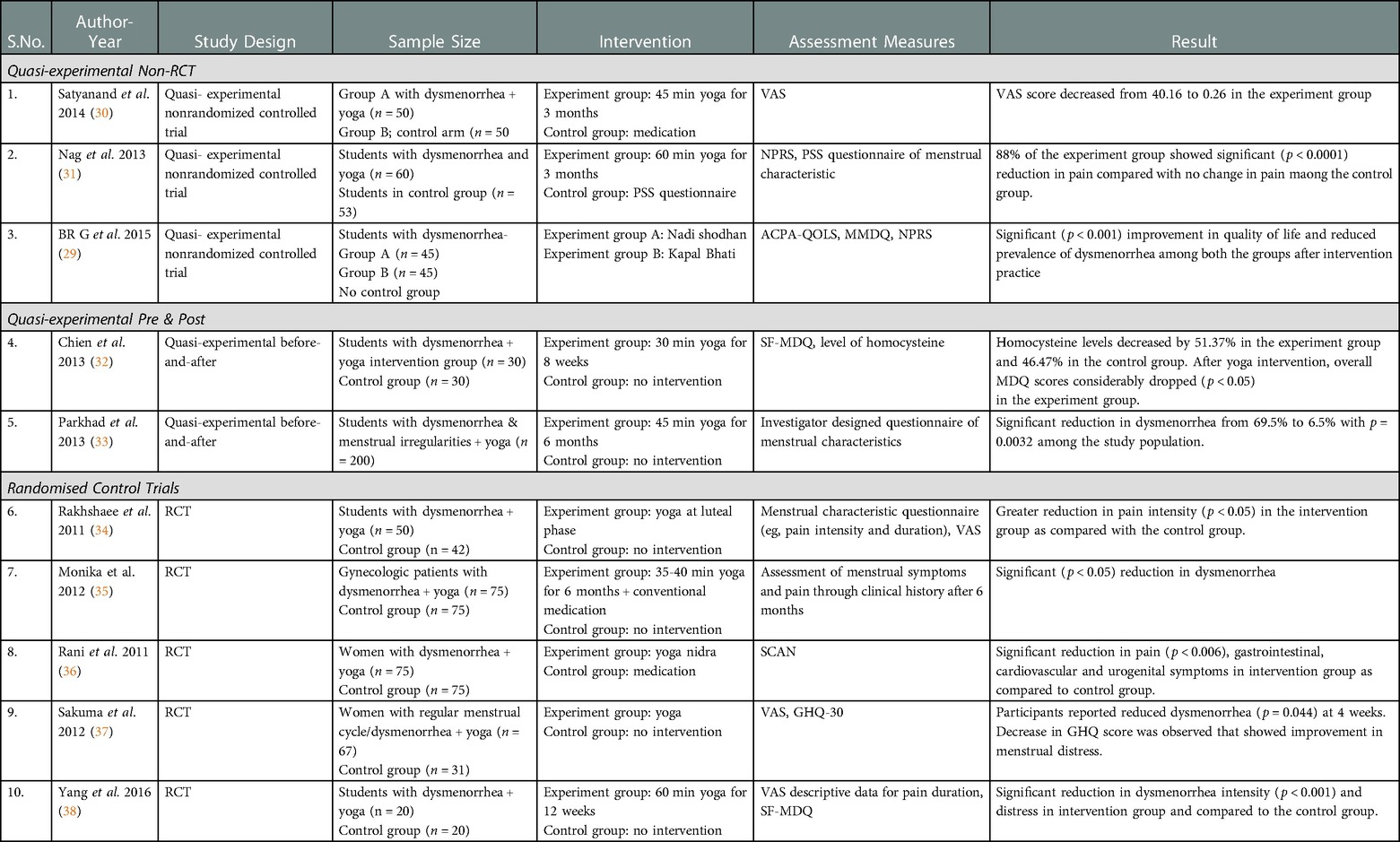
Table 1. Review of literature on benefits of Yoga on Dysmenorrhea.
Yoga is being explored as a non-pharmacological, cost effective and feasible alternative that can benefit women with dysmenorrhea. It concentrates on aligning the body through gentle, focused movements along with improved breathing practices (39).
A search was conducted to identify all studies that were undertaken from July 1990 to September 2022, to assess the effects of yogic practice on dysmenorrhea. These trials were published in various databases such as PubMed, Google Scholar and Scopus. These trials were published in various databases such as PubMed, Google Scholar and Scopus. The keywords selected were “yoga,” “menstrual pain,” or “dysmenorrhea.” The title search yielded a total of 861 studies. The review selection criteria were studies that included “yoga” as the intervention and “dysmenorrhea” as the issue. Studies on any other menstrual disorders apart from dysmenorrhea or if Yoga was not the intervention provided were excluded. Of the 861 studies only 10 studies met the selection criteria that involved participants with primary dysmenorrhea during the menstrual cycles in the past three months. The studies which included yogic intervention have been added in this review. The review search included all the study design to ensure a comprehensive literature on benefits of Yoga on dysmenorrhea (Figure 2).
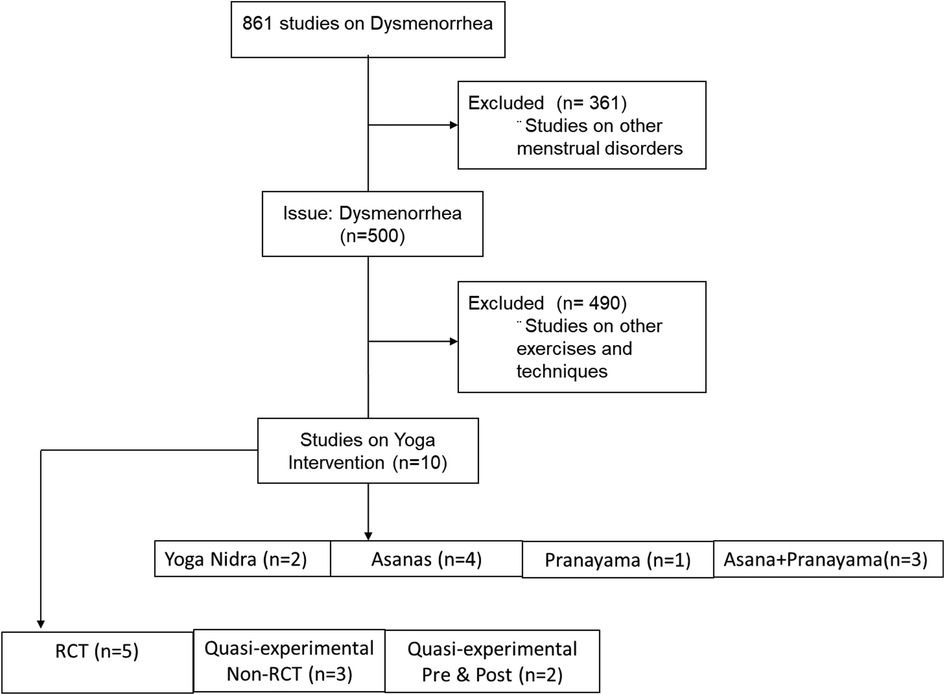
Figure 2. Flow diagram of research studies on dysmenorrhea.
The review included 1 study on pranayama, 4 studies on asanas, 3 studies on asanas and pranayama together; and 2 studies on Yoga Nidra.
Refer to Table 1 for further details
Sakuma et al. conducted a trial comprising 83 females in the yoga intervention group and 40 females in the control group. The reported change in pain at 2 weeks and at 4 weeks (after the intervention) served as the primary outcome while the 30-item General Health Questionnaire (GHQ30) score served as the secondary outcome measure. The results showed significant improvement in dysmenorrhea (p = 0.044) at 4 weeks along with reduced lower back pain during the intervention (p = 0.006). Decrease in GHQ score was observed that showed improvement in menstrual distress (37). A study by Rakhshaee et al. included 50 adolescent girls with primary dysmenorrhea who were randomized into a yogic intervention and 42 girls in a control module to study the effect of yoga on pain intensity, physical fitness and quality of life. The intervention included three yoga poses (Cobra, Cat and Fish). Visual Analog Scale (VAS) and Mann-Whitney test was used to assess the intensity for pain. The results of the study showed a significantly lower intensity of pain (p < 0.05) and pain duration in the experimental group from first to second month of intervention as compared to the control group. They also showed improved physical fitness and general health (34). Yang et al. conducted a clinical investigation on undergraduate girls with dysmenorrhea and studied the effect of yogic asanas on dysmenorrhea. 40 undergrad students selected at random were engaged in 12 h of practice, one hour every week. The intervention included Surya namaskar, Bhujangasana, Marjariasana and Matsyasana combined with relaxation and meditation. The results showed significant reduction in dysmenorrhea intensity (p < 0.001) and distress in the intervention group compared to the control group (38).
Another study was explored by Chien et al. to assess the effect of yoga intervention on a group of 35 women with primary dysmenorrhea compared to a group of 35 women as control. The women in the yoga group were provided with yoga intervention twice a week for 30 min, consecutively for 8 weeks. The cohort was administered a set of specific yoga asanas like Ardha Kurmasana, Ardha Purvottanasana, Setu Bandha, Sarvangasana and Baddha Konasana. The outcomes of the study were monitored by the level of homocysteine, an oxidative stress marker known to induce dysmenorrhea, and Menstrual Distress Questionnaires (MDQs). The results showed decrease in homocysteine level by 51.37% in experiment group and 46.47% in control group. After yoga intervention, overall MDQ score considerably dropped (p < 0.05) in the experiment group. The results suggested the therapeutic effect of yoga for dysmenorrhea (32).
Parkhad et al. conducted a study on 200 adolescent girls who experienced dysmenorrhea. They were given a yoga protocol of 45 min every day for 6 months which included Swastikasana, Virasana, Padmasana, Gomukhasana, Paschimottanasana, Baddha konasana, Janu sirsasana, Trikonasana, Ardha chandrasana, Setu bandhasana, Supta Vajrasana and Savasana. At the time of assessment after 6 months of practice, it was observed that there was significant reduction in dysmenorrhea from 69.5% to 6.5% with p = 0.0032 among the study population (33).
In a randomized controlled trial conducted by Satyanand et al., 100 female subjects with primary dysmenorrhea were studied. The study included 50 participants in the intervention group while 50 others in the control group. Females in the intervention group practiced Sukshma vyayama, Padmasana, Paschimottanasana, Vajrasana, Ushtrasana, Shashankasana, Matsyasana, Uttanpadasana, Sarvangasana, Surya namaskara followed by Shavasana. Both groups were evaluated for pain intensity using Visual Analog Scale (VAS) after three months. The result showed a decrease in VAS score from 4.16 to 0.26 in the experiment group indicating pain reduction post yoga intervention. The authors also suggested that yoga promotes physical relaxation by activating parasympathetic activity (30). Nag et al. studied the benefits of yoga on 113 girls who complained of primary dysmenorrhea and stress. The intervention cohort of 60 practiced Navasana, Matsyasana, Dhanurasana, Vajrasana, Paschimottanasana, Ustrasana, Ardha matsyendrasana, Salabhasana, Bhujangasana, Sarvangasana, Uttanapadasana, Padmasana, and Surya namaskar every day for 3 months under the supervision of a yoga trainer. 3 months later 88% of the experiment group showed significant (p < 0.0001) reduction in pain compared with no change in pain among the control group who did not receive any intervention (31).
The reviewed studies suggest that yoga can help reduce dysmenorrhea and related symptoms like anxiety and stress (Figure 3). Several yoga asanas and treatments, such as physical postures, breathing exercises, and relaxation methods, were regularly practiced over the course of many weeks or months that proved as effective complementary therapy for managing dysmenorrhea. The outcomes demonstrated the value of yoga intervention as a conventional therapy.
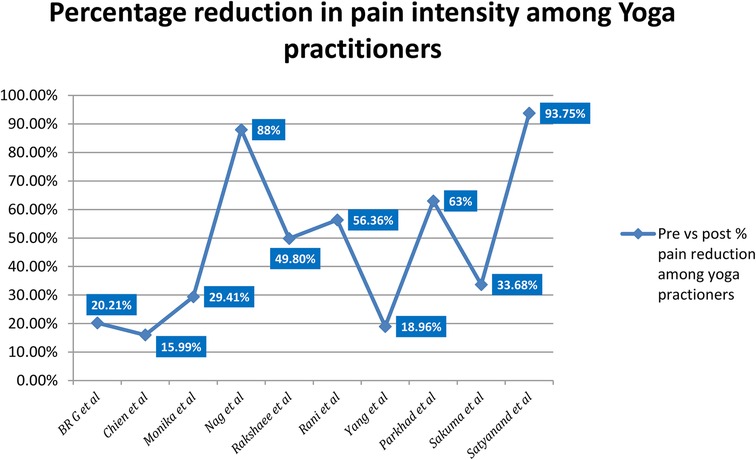
Figure 3. Graphical representation of percentage reduction in pain intensity among the yoga group.
Refer to Table 1 for further details
While asanas include one limb of Yoga, pranayama or breathing exercise are the other limbs of Yoga. Studies show deep breathing exercises (DBE) like Kapalbhati, Bhastrika and Nadi Shodhan pranayama are a set of breathing modules that can also act as an alternative form of treatment for primary dysmenorrhea (40). In a randomized control trial conducted by BR et al., 90 young women with primary dysmenorrhea between the ages of 18 and 25 were chosen at random to participate. The study group underwent yogic intervention consisting of Nadi shodhan in Group A and Kapalbhati in Group B for 30 days. The subjects were assessed at baseline and after 30 days for pain and distress using the Menstrual Distress Questionnaire (MMDQ), the American Chronic Pain Association's Quality of Life Scale and the numerical pain rating scale for pain. The results demonstrated the primary prevalence of dysmenorrhea among 65% of the population before the start of yogic intervention while the prevalence of dysmenorrhea significantly reduced post intervention (p value = <.001) with improvement in quality of life and reduced pain among the intervention group compared to the control group. The result suggested a decrease in the pain intensity with a parasympathetic activity following pranayama practice (29).
Pranayama, or breathing exercises are crucial component of yoga which can be used as a complementary therapy for various menstrual conditions. Studies show that certain breathing exercises can reduce pain and distress, and improve quality of life. Regular practice of pranayama can activate the parasympathetic nervous system, leading to reduced pain intensity and better overall well-being.
Refer to Table 1 for further details
Rani et al. studied the effect of yoga nidra on 150 female subjects with menstrual irregularities and pain. The subjects were provided with 25 min of yoga nidra intervention for 6 months and assessment for pain was done using the Schedule for Clinical Assessment in Neuropsychiatry (SCAN) rating scale. The results showed a significant reduction in pain (p < 0.006), gastrointestinal, cardiovascular, and urogenital symptoms in the intervention group compared to the control group. The authors suggested the stimulation of the pituitary gland following the practice of yoga nidra produces compounds with analgesic properties, could be a probable mechanism of action for pain relief (36).
Monika et al. conducted a randomized control trial among 150 women with dysmenorrhea. The study measured hormone levels, as a marker of pain, in the subjects before and after 6 months of Yoga Nidra practice. Reduction in dysmenorrhea (p < 0.05) was observed in the intervention group (35).
In summary, practicing Yoga Nidra may reduce dysmenorrhea and related symptoms in women, possibly by stimulating the pituitary gland. These findings suggest that Yoga Nidra could be a useful complementary therapy for managing menstrual irregularities and pain in women. Further research is needed to investigate its long-term effects.
As mentioned above, increase of vasoactive prostanoids leads to myometrial hyperactivity, reduced uterine blood flow and tissue ischemia all causing pain or dysmenorrhea during the cycle. Yoga and pelvic asanas are known to improve blood flow in the pelvic region thereby managing pain in the body (41). Further yoga also stimulates the release of beta- endorphins which are analgesics in nature (42). Studies have also shown the release of hormones like cortisol, glucose, plasma's renin, epinephrine and norepinephrine in the bloodstream as an effect of yoga that helps in regulating healthy body functions (43). Voluntary breathing control technique has been employed in many yogic interventions to decrease autonomic reactivity (44). Yoga also decreases sympathetic activity via the hypothalamic-pituitary-adrenal axis which plays an important role in contributing to pain reduction. Deep breathing and long exhalation relaxes the skeletal muscles in the body, especially the pelvic area and also contribute to pain reduction (45). A study suggests regulation of alpha brain waves, responsible for relaxation, pain relief and release of serotonin, favorably during yoga practice (46). One longitudinal study indicated that being overweight was a significant risk factor for both the likelihood of feeling dysmenorrhea and the increased duration of suffering (47). In two cross-sectional investigations, heavy or irregular periods were linked to a higher prevalence of dysmenorrhea (48). Four studies that investigated the association between smoking cigarettes and dysmenorrhea found that smokers had a higher risk of developing dysmenorrhea (49). According to Akerlund et al., cigarette smoking is known to cause vasoconstriction. He demonstrated reduced endometrial blood flow in women with dysmenorrhea using a thermistor probe technique (50). Many studies have also found a correlation between perceived stress linked to work or general life events and the prevalence of dysmenorrhea among the psychological factors investigated.
Improved body circulation with good physical and mental health has been highlighted as key factors in reducing dysmenorrhea and experiencing a healthy menstrual cycle.
Menstruation is an integral part of every woman's life cycle influencing the physical, mental, emotional health and quality of life. Unfortunately, women's health is not much attended in society. Many menstrual disorders including dysmenorrhea go unrecognized and untreated. With women's health gaining increased attention, several cost-effective, alternate salubrious interventions are being investigated to treat the women's health disorder. A significant amount of literature supports the benefits of Yoga (asanas/pranayama/Yoga Nidra) in reducing the dysmenorrhea. While few studies have demonstrated the positive effects of Yoga in treating dysmenorrhea and several more on other menstrual disorders, more studies with good scientific rigor can promote yoga as evidence based solution in treating menstrual health problems.
All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sabar UJ. The effect of prostaglandins in myometrial tissue; a functional and lipidomic study. The influence of the hormonal milieu on the functional response to prostaglandins and ex vivo lipid biosynthesis in myometrial tissues (Doctoral dissertation, University of Bradford).
3. Bergsjø P. Socioeconomic implications of dysmenorrhea. Acta Obstet Gynecol Scand. (1979) 58(sup87):67–8. doi: 10.3109/00016347909157793
4. Maia H Jr, Casoy J. Non-contraceptive health benefits of oral contraceptives. Eur J Contracept Reprod Health Care. (2008) 13(1):17–24. doi: 10.1080/13625180701712745
5. Lewers D, Clelland JA, Jackson JR, Varner RE, Bergman J. Transcutaneous electrical nerve stimulation in the relief of primary dysmenorrhea. Phys Ther. (1989) 69(1):3–9. doi: 10.1093/ptj/69.1.3
6. Woodyard C. Exploring the therapeutic effects of yoga and its ability to increase quality of life. Int J Yoga. (2011) 4(2):49–54. doi: 10.4103/0973-6131.85485
7. Li X, Guo S, Chen Z, Ren K, Zhang H, Yu S, et al. Regulation of mild moxibustion on uterine vascular and prostaglandin contents in primary dysmenorrhea rat model. Evidence-Based Complementary Altern Med. (2021) 2021:9949642. doi: 10.1155/2021/
8. Hawkey CJ. Nonsteroidal anti-inflammatory drug gastropathy. Gastroenterology. (2000) 119(2):521–35. doi: 10.1053/gast.2000.9561
9. Ferenczy A. Pathophysiology of endometrial bleeding. Maturitas. (2003) 45(1):1–4. doi: 10.1016/S0378-5122(03)00068-9
10. Rosenwaks Z, Seegar-Jones G. Menstrual pain: its origin and pathogenesis. J Reprod Med. (1980) 25(4 Suppl):207–12. PMID: 7001019.7001019
11. Morrison BW, Daniels SE, Kotey P, Cantu N, Seidenberg B. Rofecoxib, a specific cyclooxygenase-2 inhibitor, in primary dysmenorrhea: a randomized controlled trial. Obstet Gynecol. (1999) 94(4):504–8.10511349
12. Vincenzo De Sanctis M, Soliman A, Bernasconi S, Bianchin L, Bona G, Bozzola M, et al. Primary dysmenorrhea in adolescents: prevalence, impact and recent knowledge. Pediatric Endocrinology Reviews (PER. (2015) 13(2):465–73. PMID: 26841639.26540763
13. Durain D. Primary dysmenorrhea: assessment and management update. J Midwifery & women's health. (2004) 49(6):520–8. doi: 10.1016/j.jmwh.2004.08.013
14. Hayes SG. Neural control of the cardiovascular and ventilatory systems during exercise. Davis: University of California (2001).
15. Abreu-Sánchez A, Parra-Fernández ML, Onieva-Zafra MD, Ramos-Pichardo JD, Fernández-Martínez E. Type of dysmenorrhea, menstrual characteristics and symptoms in nursing students in southern Spain. InHealthcare. (2020) 8(3):302. MDPI. doi: 10.3390/healthcare8030302
16. Åkerlund M. Pathophysiology of dysmenorrhea. Acta Obstet Gynecol Scand. (1979) 58(sup87):27–32. doi: 10.3109/00016347909157786
18. Jabbour HN, Kelly RW, Fraser HM, Critchley HO. Endocrine regulation of menstruation. Endocr Rev. (2006) 27(1):17–46. doi: 10.1210/er.2004-0021
19. Denney DR, Gerrard M. Behavioral treatments of primary dysmenorrhea: a review. Behav Res Ther. (1981) 19(4):303–12. doi: 10.1016/0005-7967(81)90051-6
20. Harel Z. Dysmenorrhea in adolescents and young adults: an update on pharmacological treatments and management strategies. Expert Opin Pharmacother. (2012) 13(15):2157–70. doi: 10.1517/14656566.2012.725045
21. Bettendorf B, Shay S, Tu F. Dysmenorrhea: contemporary perspectives. Obstet Gynecol Surv. (2008) 63(9):597–603. doi: 10.1097/OGX.0b013e31817f15ff
23. Hosseinlou A, Alinejad V, Alinejad M, Aghakhani N. Effects of fish oil capsules and vitamin B1 tablets on duration and severity of dysmenorrhea in students of high school in Urmia-Iran. Glob J Health Sci. (2014) 6(7):124. doi: 10.5539/gjhs.v6n7p124
24. Aboualsoltani F, Bastani P, Khodaie L, Fazljou SM. Non-pharmacological treatments of primary dysmenorrhea: a systematic review. Arch Pharma Pract. (2020) 11(S1):136–42.
25. El Geziry A, Toble Y, Al Kadhi F, Pervaiz M, Al Nobani M. Non-pharmacological pain management. Pain Management in Special Circumstances. (2018):1–4.
26. Proctor M, Latthe P, Farquhar C, Khan K, Johnson N. Surgical interruption of pelvic nerve pathways for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. (2005) 4:1–27. doi: 10.1002/14651858.CD001896.pub2
27. Vercellini P, Fedele L, Bianchi S, Candiani GB. Pelvic denervation for chronic pain associated with endometriosis: fact or fancy? Am J Obstet Gynecol. (1991) 165(3):745–9. doi: 10.1016/0002-9378(91)90322-I
28. Fugh-Berman A, Kronenberg F. Complementary and alternative medicine (CAM) in reproductive-age women: a review of randomized controlled trials. Reprod Toxicol. (2003) 17(2):137–52. doi: 10.1016/S0890-6238(02)00128-4
29. Ganesh BR, Donde MP, Hegde AR. Comparative study on effect of slow and fast phased pranayama on quality of life and pain in physiotherapy girls with primary dysmenorrhoea: randomized clinical trial. Int J Physiother Res. (2015) 3(2):960–5. doi: 10.16965/ijpr.2015.115
30. Satyanand V, Hymavathi K, Panneerselvam E, Mahaboobvali S, Basha SA, Shoba C. Effects of yogasanas in the management of pain during menstruation. J Med Sci Clin Res. (2014) 2(11):2969–74.
31. Nag U, Dip P, Kodali M. Effect of yoga on primary dysmenorrhea and stress in medical students. IOSR J Dent Med Sci. (2013) 4(1):69–73. doi: 10.9790/0853-0416973
32. Chien LW, Chang HC, Liu CF. Effect of yoga on serum homocysteine and nitric oxide levels in adolescent women with and without dysmenorrhea. J Altern Complement Med. (2013) 19(1):20–3. doi: 10.1089/acm.2011.0113
33. Parkhad SB, Palve SB, Latti RG, Kulkarni NB. Effect of yoga on premenstrual and menstrual cycle disorders in adolescent girls. Biomedicine. (2013) 33(2):170–5.
34. Rakhshaee Z. Effect of three yoga poses (cobra, cat and fish poses) in women with primary dysmenorrhea: a randomized clinical trial. J Pediatr Adolesc Gynecol. (2011) 24(4):192–6. doi: 10.1016/j.jpag.2011.01.059
35. Monika SU, Ghildiyal A, Kala S, Srivastava N. Effect of yoga nidra on physiological variables in patients of menstrual disturbances of reproductive age group. Indian J Physiol Pharmacol. (2012) 56(2):161–7.23387245
36. Rani K, Tiwari SC, Singh U, Agrawal GG, Srivastava N. Six-month trial of yoga nidra in menstrual disorder patients: effects on somatoform symptoms. Ind Psychiatry J. (2011) 20(2):97–102. doi: 10.4103/0972-6748.102489
37. Sakuma Y, Sasaki-Otomaru A, Ishida S, Kanoya Y, Arakawa C, Mochizuki Y, et al. Effect of a home-based simple yoga program in child-care workers: a randomized controlled trial. J Altern Complement Med. (2012) 18(8):769–76. doi: 10.1089/acm.2011.0080
38. Yang NY, Kim SD. Effects of a yoga program on menstrual cramps and menstrual distress in undergraduate students with primary dysmenorrhea: a single-blind, randomized controlled trial. J Alternative and Complementary Med. (2016) 22(9):732–8. doi: 10.1089/acm.2016.0058
39. Archana SD. Effect of Surya Namaskar in primary dysmenorroea (Doctoral dissertation, Government Yoga and Naturopathy Medical College, Chennai).
40. Purnamasari KD, Rohita T, Zen DN, Ningrum WM. The effect of deep breathing exercise on menstrual pain perception in adolescents with primary dysmenorrhea. Pertanika Journal. (2020) 2(28):649–57.
41. Dauneria S, Keswani J. A study on the effect of yoga and naturopathy on dysmenorrhea. Int J Yoga Allied Sci. (2014) 3(1):38–42.
42. Suri M, Sharma R, Saini N. Neuro-physiological correlation between yoga, pain and endorphins. Int J Adapted Phys Educ and Yoga. (2017) 2(9):18–32.
43. Kamalifard M, Yavari A, Asghari-Jafarabadi M, Ghaffarilaleh G, Kasb-Khah A. The effect of yoga on women's Premenstrual syndrome: a randomized controlled clinical trial. Int J Women's Health and Reprod Sci. (2017) 5(3):205–11. doi: 10.15296/ijwhr.2017.37
44. Nayak NN, Shankar K. Yoga: a therapeutic approach. Phys Med and Rehab Clin. (2004) 15(4):783–98. doi: 10.1016/j.pmr.2004.04.004
45. Vallath N. Perspectives on yoga inputs in the management of chronic pain. Indian J Palliat Care. (2010) 16(1):1. doi: 10.4103/0973-1075.63127
46. Desai R, Tailor A, Bhatt T. Effects of yoga on brain waves and structural activation: a review. Complement Ther Clin Pract. (2015) 21(2):112–8. doi: 10.1016/j.ctcp.2015.02.002
47. Harlow SD, Park M. A longitudinal study of risk factors for the occurrence, duration and severity of menstrual cramps in a cohort of college women. Bjog: An Int J Obstetr & Gynaecol. (1996) 103(11):1134–42. doi: 10.1111/j.1471-0528.1996.tb09597.x
48. Patel V, Tanksale V, Sahasrabhojanee M, Gupte S, Nevrekar P. The burden and determinants of dysmenorrhoea: a population-based survey of 2262 women in goa, India. BJOG: An Int J Obstetr & Gynaecol. (2006) 113(4):453–63. doi: 10.1111/j.1471-0528.2006.00874.x
49. Burnett MA, Antao V, Black A, Feldman K, Grenville A, Lea R, et al. Prevalence of primary dysmenorrhea in Canada. J Obstet Gynaecol Can. (2005) 27(8):765–70. doi: 10.1016/S1701-2163(16)30728-9
Keywords: asanas, dysmenorrhea, meditation, menstrual pain, pranayama, yoga, yoga nidra
Citation: Kanchibhotla D, Subramanian S and Singh D (2023) Management of dysmenorrhea through yoga: A narrative review. Front. Pain Res. 4:1107669. doi: 10.3389/fpain.2023.1107669
Received: 4 January 2023; Accepted: 28 February 2023;
Published: 30 March 2023.
Edited by:
Apar Avinash Saoji, Swami Vivekananda Yoga Anusandhana Samsthana, IndiaReviewed by:
P. S. Swathi, Swami Vivekananda Yoga Anusandhana Samsthana, India© 2023 Kanchibhotla, Subramanian and Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Divya Kanchibhotla ZGlyZWN0b3Iuc3NpYXJAYXJ0b2ZsaXZpbmcub3Jn
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Musculoskeletal Pain, a section of the journal Frontiers in Pain Research
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.