 Matthieu Vincenot1,2
Matthieu Vincenot1,2 Alexia Coulombe-Lévêque1,2
Alexia Coulombe-Lévêque1,2 Monica Sean1,3
Monica Sean1,3 Félix Camirand Lemyre4,5
Félix Camirand Lemyre4,5 Louis Gendron3,4
Louis Gendron3,4 Serge Marchand2†
Serge Marchand2† Guillaume Léonard1,6*†
Guillaume Léonard1,6*†- 1Research Center on Aging, Université de Sherbrooke, Sherbrooke, QC, Canada
- 2Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada
- 3Department of Pharmacology-Physiology, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada
- 4Centre de Recherche du Centre Hospitaliser Universitaire de Sherbrooke, Sherbrooke, QC, Canada
- 5Département de Mathématiques, Faculté des Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada
- 6Faculty of Medicine and Health Sciences, School of Rehabilitation, Université de Sherbrooke, Sherbrooke, QC, Canada
Introduction: Quantitative sensory testing is frequently used in research to assess endogenous pain modulation mechanisms, such as Temporal Summation (TS) and Conditioned Pain Modulation (CPM), reflecting excitatory and inhibitory mechanisms, respectively. Numerous studies found that a dysregulation of these mechanisms is associated with chronic pain conditions. In turn, such a patient's “profile” (increased TS and/or weakened CPM) could be used to recommend different pharmacological treatments. However, the procedure to evaluate these mechanisms is time-consuming and requires expensive equipment that is not available in the clinical setting. In this study, we aim to identify psychological, physiological and socio-demographic markers that could serve as proxies to allow healthcare professionals to identify these pain phenotypes in clinic, and consequently optimize pharmacological treatments.
Method: We aim to recruit a healthy participant cohort (n = 360) and a chronic pain patient cohort (n = 108). Independent variables will include psychological questionnaires, pain measurements, physiological measures and sociodemographic characteristics. Dependent variables will include TS and CPM, which will be measured using quantitative sensory testing in a single session. We will evaluate one prediction model and two validation models (for healthy and chronic pain participants) using multiple regression analysis between TS/CPM and our independent variables. The significance thresholds will be set at p = 0.05, respectively.
Perspectives: This study will allow us to develop a predictive model to compute the pain modulation profile of individual patients based on their biopsychosocial characteristics. The development of the predictive model is the first step toward the overarching goal of providing clinicians with a set of quick and cheap tests, easily applicable in clinical practice to orient pharmacological treatments.
Introduction
Chronic pain, which affects one in five people worldwide (1), has been defined as pain that persists beyond the usual healing time (2). However, merely relying on this temporal aspect is not enough to account for the complexity of chronic pain vs. acute pain. As such, the notion of inadequate response to treatment and significant, lasting alterations of functional and psychosocial status have increasingly been recognized as an integral part of this condition (3). Several factors have been associated with chronic pain, including physical limitations (4, 5), cognitive impairments (6), and psychological conditions, such as anxiety and depression (7).
Dysregulations of endogenous pain modulating systems are also thought to be involved in the development of chronic pain. These dysregulations include increases in pain facilitation [which amplify our body's alertness (8)], and decreases in pain inhibition [which triggers diffuse hypoalgesia (9)]. These endogenous pain modulation mechanisms can be measured using quantitative sensory testing based on Temporal Summation (TS) and Conditioned Pain Modulation (CPM), respectively. Both of these testing paradigms have high test-retest reliability (10–12).
TS is the psychophysical correlate of central sensitization, which is defined as an increased responsiveness of second order neurons (located in the spinal cord) to afferent C-fibers (13) resulting in a heightened pain perception (14). Increased TS is thought to be involved in various chronic pain conditions, such as fibromyalgia (14, 15), chronic low back pain (16), and painful knee osteoarthritis (17). CPM, on the other hand, refers to the phenomenon wherein a noxious stimulation results in widespread hypoalgesia (18), akin to the diffuse noxious inhibitory control involving a spino-bulbo-spinal loop studied in animal models (9, 19). Weakened CPM is found in chronic pain conditions, such as chronic tension headaches (20), provoked vestibulodynia (21), atypical trigeminal neuralgia (22), temporomandibular disorders (23), fibromyalgia (24), and irritable bowel syndrome (23).
TS and CPM measures can be used to identify individuals at risk of developing chronic pain (25). For example, the amplitude of pre-operative TS is correlated with the intensity of post-operative pain (26), while a placebo-controlled study has found that weaker CPM is associated with a better response to duloxetine (a serotonin-noradrenalin reuptake inhibitor) in patients suffering from neuropathic pain (27). This line of research has led authors to suggest that it is the presence of specific deficits in endogenous pain modulation mechanisms, rather than the type of chronic pain, that best predicts response to treatment (28, 29). Indeed, according to Yarnitsky and colleagues, each individual can be placed along a spectrum ranging from an antinociceptive (normal TS/effective CPM) to a pronociceptive (increased TS/weak CPM) profile, and as such should be more receptive to an individually tailored treatment that specifically counteracts their deficits (25).
The evaluation of these endogenous mechanisms could therefore prove useful in the clinic, by providing healthcare professionals with valuable information regarding the pain modulation profile of patients to help them choose the most appropriate pharmacological approach. Unfortunately, to the best of our knowledge, no study has attempted to estimate the amplitude of TS and CPM using readily accessible measures. Protocols currently used to evaluate endogenous pain modulation mechanisms are time consuming and require expensive, complex equipment that would not be practical for daily clinical practice. As such, an alternative approach, which would allow clinicians to easily estimate their patient's CPM and TS using readily available tests, would be highly relevant to clinical practice.
Despite the lack of predictive models using TS and CPM as outcome, numerous association studies suggest that certain factors influence endogenous mechanisms. TS and CPM have long been known to be affected by age and sex (30–38), but more recently they have also been linked to a number of other psychophysiological variables. For instance, TS is consistently associated with pain catastrophizing (39–42), whereas CPM is modulated by both catastrophizing (43, 44) and expectations (45); additionally, a wide array of other psychological factors have been related to pain mechanisms, albeit in a method-dependent manner [for a review, see (46)]. Certain physiological factors, such as blood pressure, also seem to correlate with TS/CPM (47, 48) response, whereas others, such as activation of endocannabinoid and opioid systems, are known to directly contribute to pain inhibition (49–51). Moreover, a lower plasma concentration of dopamine (52) and catecholamines (norepinephrine and serotonin) (53) is associated with deficient CPM in chronic pain patients and, interestingly, it seems that this low plasma concentration is attributable to genetic polymorphisms, which suggests that CPM deficiency could in fact have a genetic correlate (54).
Different approaches have been developed (based on similar theoretical frameworks) to assess endogenous mechanisms. For TS, constant (47, 53–55) and pulsed (15, 31, 56, 57) nociceptive stimulations are commonly used, with a large variety of stimuli (58). For CPM, protocols include parallel (27, 34, 59, 60) or sequential (35, 38, 61–63) paradigms. In this context, the heterogeneity of the aforementioned studies and approaches makes it difficult to draw any meaningful generalization (64). Moreover, these factors have yet to be systematically evaluated within a single study.
The first objective of this study is to develop and validate a predictive model to estimate the amplitude of TS and CPM. Our second objective is to estimate reference values of these endogenous excitatory and inhibitory modulation mechanisms of pain in a healthy population.
Methods
Participants
Our participants will take part in a single experimental session, taking place at the Centre de Recherche du CHUS (Sherbrooke, Quebec, Canada). Eligibility criteria (56) are listed in Table 1. We will ask that participants refrain from consuming tobacco (65, 66), alcohol (67, 68), and stimulants (69) (caffeine, theine, etc.) in the 24 h preceding the experimental visit, and that they skip their last dose of pain medication (acetaminophen, non-steroidal anti-inflammatory drugs, and narcotics), such that they are not under the influence of an analgesic agent during the session. Recreational substances are also prohibited up to 7 days before the testing. Participants who fail to adhere to these instructions will be asked to reschedule their session. Participants will be recruited using volunteer registers; Facebook advertisement, posters, and leaflets; those interested will be invited to contact the team and to complete screening questionnaires to confirm their eligibility.
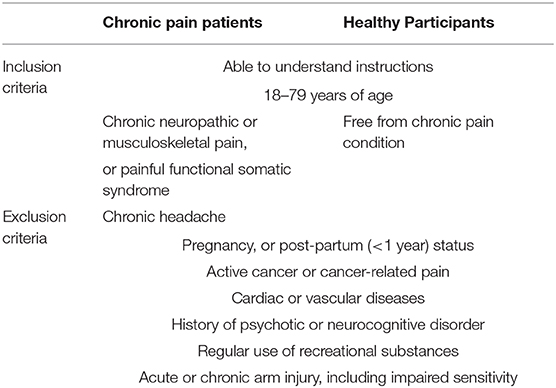
Table 1. Eligibility criteria.
Independent Variables
Psychological Distress
A number of psychological conditions are comorbidities of chronic pain (7). For this reason, different psychological variables will be evaluated.
Anxiety and Depression
The Hospital Anxiety and Depression Scale is an instrument used to screen for anxiety and depressive disorders. It comprises 14 items (seven each for anxiety and depression) rated from 0 to 3, for a maximum score of 21. Subjects are classified as presenting no symptoms (≤7), mild symptoms (8–10), or moderate to severe symptoms (≥11) for both disorders. The psychometric properties of this questionnaire are qualified as excellent (70).
Catastrophizing
The Pain Catastrophizing Scale (71) is a 13-item questionnaire representing the three components of pain catastrophizing: rumination, magnification, and helplessness. A score above 30/52 indicates a clinically significant level of catastrophizing. This questionnaire has good psychometric properties (72).
Pain Measurements
Pain Intensity
The Brief Pain Inventory (BPI) (73) will be used to measure pain intensity and interference with daily life. The BPI is a generic, self-administered pain questionnaire for chronic pain conditions. The psychometric qualities of this test are excellent (74–76).
Pain Type
The Douleur Neuropathique 4 (77) is a diagnostic tool used to identify neuropathic pain. It assesses pain symptoms (type of pain and presence of dysesthesia, out of seven) and signs (physical examination, out of three). A score ≥ 4/10 suggests a neuropathic component. This tool is regularly used in research, and has excellent psychometric properties (77).
General Clinical Pain
A pain diary will be used to measure daily clinical pain. Participants with chronic pain will be asked to indicate the highest, average and lowest level of pain they feel on seven occasions (3 days prior to the visit, the day of the visit and the 3 days following the visit).
Somatization
The Somatization subscale of the Symptoms Checklist 90 (78, 79) will be used to assess somatization in our participants. The subscale comprises 12 items, each rated on a 5-point scale. Psychometric properties of this subscale are excellent (79).
Mechanical Pain Threshold
A digital algometer will be used to assess the mechanical pain threshold (i.e., the point at which a mechanical pressure starts to elicit pain). The algometer will be placed on the upper trapezius muscle, and the pressure will be gradually increased until the participant verbally reports pain. Four trials will be conducted—two on each side—and the average pressure required to reach the mechanical pain threshold will be recorded. This test has good to excellent reliability and validity (80–82).
Pain Persistence
A digital algometer will be used to assess pain persistence. Following the mechanical pain trials described above, the algometer will be applied on the right upper trapezius muscle, and pressure will be increased until participants verbally report a pain intensity of 5/10 (numerical rating scale). This pressure will be maintained for 20 s (Tonic Mechanical Pain test). Immediately after the algometer is removed, participants will be asked to rate the intensity of their lingering pain sensation (if any), again using the numerical rating scale. Pain scores will subsequently be collected every 2 min, until participants report two consecutive scores of 0/10.
Physiological Measurements
Blood Pressure
The cardiovascular system and the descending inhibitory pathways of pain appear to be closely related (48, 75). Blood pressure will be measured three times (at rest, before, and after the conditioning stimulus—see below) using a digital sphygmomanometer.
Blood Concentration
Catecholamines (53) (adrenaline, noradrenaline, dopamine, serotonin, and their metabolites), Endocannabinoids (anandamide, N-olcoylethanilamine, palmitoylethanolamine), and Peptides (83, 84) (Leu-Enképhaline, B-Endorphin, Dynorphine A, Substance P). Blood samples will be collected in K2-EDTA tubes and will be placed directly on ice. After centrifugation (4°C, 1,500 g, 15 min), samples will be directly stored at −80°C before analysis. The different analytes will be separated and analyzed by liquid chromatography coupled to a tandem mass spectrometer. The analysis will be carried out at the bioanalysis platform of the Sherbrooke Pharmacology Institute.
Dependent Variables
CPM and TS Amplitude
The amplitude of CPM and TS will be assessed within a single experimental procedure, developed by Tousignant-Laflamme (85) and in accordance with Yarnitsky (18, 86). This procedure consists of a Test Stimulus applied before and after a Conditioning Stimulus (CS); the amplitude of TS is measured as the changes in pain levels observed throughout the first administration of the Test Stimulus, and the amplitude of CPM is measured as the difference in pain levels elicited by the Test Stimulus before and after the CS. This method is commonly used to measure these mechanisms (35, 55, 87, 88).
Pain Perception
Pain perception will be assessed using a Computerized Visual Analog Scale (CoVAS). This tool, highly validated and commonly used in research (89–91), consists of a slider placed along a visual analog scale (left end: 0, or no pain; right end: 100, or worst pain imaginable), linked to a computer. Participants move the slider along the scale according to their pain levels, such that their perceived pain intensity is continuously recorded by the computer.
Procedure
At the beginning of the session, we will reassess participants' eligibility, and we will collect their informed consent. We will also collect data relating to our independent variables, using a series of questionnaires, physiological measures, and a blood sample. All questionnaires will be provided in each participant's preferred language (English or French). We will then assess the amplitude of their CPM and TS using quantitative sensory testing (Figure 1):
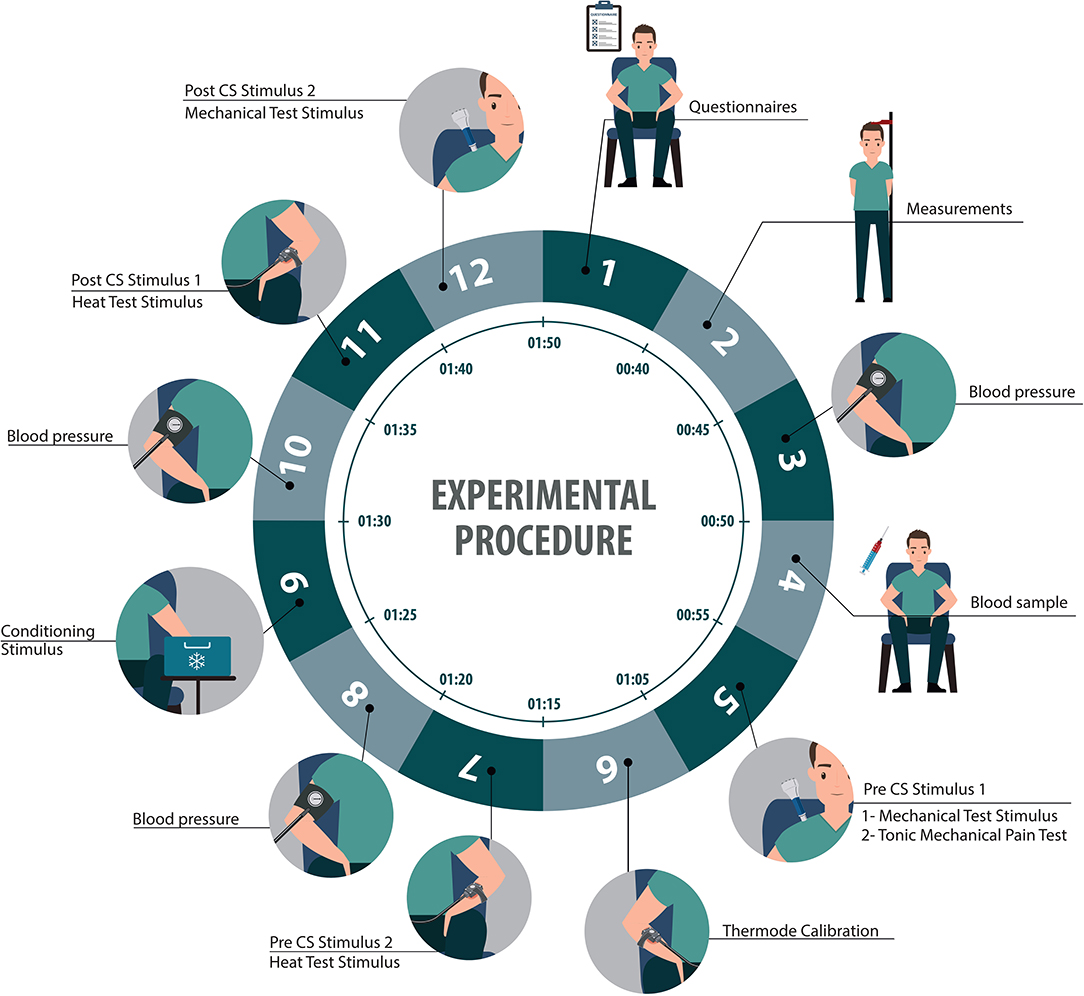
Figure 1. Illustration representing the sequence of the experimental procedure.
Thermode Calibration
Pre-tests will be conducted using an experimental thermode (9 cm2, TSA II), at a temperature increasing from 32° to 51°C at a rate of 0.3°C/s. Participants will be asked to identify the point at which heat becomes painful (heat pain threshold) and the point at which it becomes intolerably painful (heat pain tolerance).
One pre-tests will be conducted on the left hand of each participant, so they become familiar with the thermode and CoVAS. Three more pre-tests will be conducted on the anterior side of the left forearm, to identify the average temperature eliciting a pain intensity of 50/100. This temperature will be used as the Heat Test Stimulus (see below).
Pre-CS Test Stimuli
Two Pre-CS Test Stimuli will be used in our study: a painful mechanical pressure and a painful heat stimulus. The Mechanical Test Stimulus will be administrated using the digital algometer, applied on the upper trapezius muscle at the mechanical pain threshold (see Independent Variables—Mechanical pain). The average pressure required to reach the mechanical pain threshold before and after the CS will be compared to assess CPM.
The second Test Stimulus will consist of a 2 min heat pain stimulation, delivered by the thermode applied on the left forearm of participants, at an individually tailored temperature selected to evoke pain levels of 50/100 (based on the pre-tests). Although the thermode temperature will be kept constant during the stimulation (following a gradual increase from 32°C to the target temperature, at a rate of 0.3°C/s), participants will be told that the temperature will randomly vary (increase, remain stable, or decrease). Participants will be asked to rate their pain during the stimulation using the CoVAS. This Heat Test Stimulus will serve two purposes: first, like the Mechanical Test Stimulus, it will be used as a pre- and post-CS comparator to assess CPM; second, it will be used to evaluate TS, which will be measured as the change in pain levels throughout the heat test stimulation.
Conditioning Stimulus (CS)
The conditioning stimulus, which serves to trigger CPM, will consist of the Cold Pressor Test, wherein participants immerse their right arm (up above the elbow) in a painfully cold water bath [10°C; (44)] for 2 min. This technique has been shown to consistently elicit CPM (92).
Post-CS Test Stimuli
The Heat Test Stimulus will be administered again immediately after the CS, using the same parameters as for the pre-CS stimulation. Following this, the Mechanical Test Stimulus will also be re-administered; again, four trials will be conducted and the average pressure corresponding to the pain threshold will be recorded. Comparisons between pre-CS and post-CS scores will be used to assess CPM.
Ethical Aspects
This study will be conducted in accordance with the Helsinki Declaration and the International Council for Harmonization of Good Clinical Practices. Participants will be informed of the purpose and process of this study. We will collect their written informed consent, reminding them that participation in this study is purely voluntary and that they can withdraw at any time without negative repercussions, and we will preserve the confidentiality of their data. Participants will be asked to skip only the dose of their analgesic medication immediately preceding the experimental session, to minimize undue pain. The trial is registered at clinicaltrial.gov (NCT03376867).
Statistical Considerations
Sample Size
It is customary in predictive analysis to use a rule of thumb to calculate the sample size, wherein the number of subjects required for a multiple regression analysis is n = 10–15 subjects per variable (93). However, this rule often yields fitted models with limited predictive capabilities (94–98); as such, it is recommended that two cohorts be used: a discovery cohort, and a validation cohort—which, as their names suggest, are used to build the predictive model and to validate it, respectively (99).
We calculated a sample size of 360 participants for the discovery cohort, based on the smallest expected R2 (0.4) and the highest expected number of predictors (24) required to obtain a shrinkage coefficient (100) of at least 0.9 (101). The discovery cohort will be representative of the overall population, such that it will be comprised of 85% (n = 306) of healthy participants and 15% (n = 54) of patients suffering from chronic pain (102). The external validation cohort will be comprised of 54 (new) participants, corresponding to 15% of the size of the discovery cohort (103). We will use two such validation cohorts (n = 54 for both) in order to validate our model using both healthy participants and patients suffering from chronic pain. As such, a total of 468 participants will be recruited (360 healthy participants, and 108 patients suffering from chronic pain).
TS and CPM Amplitude
The amplitude of TS (ATS) will be measured as the difference in pain intensity elicited by the thermode during the heat test stimulation (first instance the Heat Test Stimulus). We will subtract the pain level at 0 s (time the thermode reaches the target temperature) from the pain level at 120 s, so that a positive score represents an increase in pain level. The amplitude of CPM (ACPM) will be measured as the difference in pain level elicited by the thermode (calculated as the average of all pain scores taken throughout the 2 min test stimulation) before and after the cold water bath, and as the difference in pressure required to reach mechanical pain threshold before and after the cold water bath.
Statistical Analyses
The sample will be characterized using descriptive statistics. The underlying assumptions of the regression model will be verified by analyzing the residuals distribution.
The main objective (identifying predictors of excitatory (TS) and inhibitory (CPM) endogenous pain mechanisms) will be achieved through the development of two predictive models (one for each mechanism). Development of a predictive model requires two steps: (1) Building and (2) Validation, which each use their own participant cohorts (see Sample Size section). Building involves a data-driven selection of the variables to be included as predictors in the model; for each variable, the beta coefficient is calculated and fitted to the model. Validation involves testing the model with data from new participants, in order to quantify the predictive capacity of the model. Validation will be conducted twice for each model: once with a healthy cohort, and once with a chronic pain cohort.
We will use a lasso regression on the discovery cohort to determine which variables will be included in the model for each mechanism. Lasso regression fits a linear model between an outcome and a set of predictors by adding a penalty term that shrinks coefficients associated to poor predictive capacity variables to 0 (i.e., Lasso automatically excludes poor predictors). This approach thus encourages simple and sparse models, and is widely used to perform variable selection in prediction contexts (103). The penalty term involves a coefficient (often denoted by lambda) that determines the amount of shrinkage to perform. This coefficient is often set so as to maximize a cross-validation estimate of the predictive capability of a model (103). Accordingly, we will select the shrinkage coefficient that minimizes the leave-one-out cross-validation estimate of the mean square prediction error. The resulting “optimal” shrinkage coefficient will be used within the lasso regression model, and the predictors and non-zero fitted parameters will be retained to constitute our predictive model.
In order to complete the validation (validation cohort), we will calculate the mean square prediction error of the predictive model for the healthy and chronic pain cohorts. If the mean square prediction error is smaller than 10%, the model will be considered to have a good predictive value. We will compare this predictive error between the two populations, to assess whether predictors are the same between healthy and patient populations.
The second objective (i.e., estimating reference TS and CPM values in healthy subjects) will use data from the 360 healthy participants (306 from the discovery cohort and the 54 from the healthy validation cohort). Participants will be separated into subgroups based on biological sex (male, female) and age (18–39, 40–59, and 60–79 years old), for a total of six subgroups. For each subgroup, a kernel estimation method will be used to obtain density curves, from which percentile reference charts will be generated (104). These analyses will be run separately for TS and CPM data.
Discussion
To our knowledge, this is the first protocol that single handedly studies psychological, physiological and socio-demographic markers of endogenous pain modulation mechanisms.
The protocol we adopted to assess TS and CPM is frequently used in our laboratory; its reliability has been validated (10–12), and our expertise with the procedure and our familiarity with the equipment considerably reduces the risk of bias and confounding factors.
Chronic pain is a highly prevalent condition, for which there is currently no satisfying treatment approach. The success rates of surgery are subpar (105, 106); therapeutic exercises (107) only have limited success; and the current pharmacological approach, which relies mostly on drawn-out trial and error, is disheartening for both the patients, who struggle to see a finality to their pain, and the clinicians, who are confronted with their powerlessness in the face of their patients' everlasting ailment (108).
It is becoming more and more apparent that chronic pain treatment should focus not on the symptomatology—or type of condition—of chronic pain patients, but rather on the underlying imbalance in their pain modulation mechanisms. The amplitude of CPM and TS has been shown to correlate with the development of chronic pain conditions (109, 110), which imparts them with a predictive quality that could be extremely useful in clinical practice. Moreover, specific assessments of CPM and TS can effectively predict treatment success rates in patients suffering from chronic pain (27). As such, an individualized pharmacological treatment informed by the pain modulation profile of each patient could significantly improve treatment outcome. Unfortunately, current CPM and TS testing procedures remain too expensive and time-consuming to be used on a regular basis in hospitals or family medicine clinics.
This study will further our understanding of modulatory mechanisms and their relationship with a complex system of physiological, psychological and socio-demographic correlates, which will allow us to develop a predictive model to compute the pain modulation profile of individual patients based on their biopsychosocial characteristics. This model will consist in a simple equation in which clinicians can input the value of selected variables (obtained via simple clinical tests), in order to yield the predictive amplitude of their patients' CPM and/or TS response. The overarching goal of this study is to provide clinicians with a set of quick and cheap tests, easily applicable in day-to-day practice, in order to identify markers of pain modulation profiles and in turn orient pharmacological treatment, which will ultimately provide patients with a more hopeful outlook on their future and will lead to a more optimal use of ever limited health care resources. This protocol is the first step toward the development of a validated clinical tool.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material; further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the Comité d'éthique de la recherche du Centre intégré universitaire de santé et de services sociaux de l'Estrie - Centre hospitalier universitaire 3001, 12e Avenue Nord, Local HF-2929 Sherbrooke, QC J1H 5N4. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MV wrote the manuscript with support from AC-L and MS. FCL helped the design statistical analysis. SM, GL, and LG conceived the study and helped draft the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was funded, in part, by the Chronic Pain Network, through the Canadian Institutes of Health Research (CIHR) funded Strategy for Patient Oriented Research (SPOR), as well as by the Centre de Recherche du CHUS and the Faculty of Medicine and Health Sciences of the Université de Sherbrooke for scholarship to MV. GL and LG receive salary support by the Fonds de Recherche du Québec—Santé (FRQS).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors gratefully thank SophieGraphisme for illustrations. The authors wish to highlight the contribution of Amélie Tétu, Virginie Bolduc, Catherine Raynauld, and Marie-Claude Battista form the Unité de Recherche Clinique et Épidémiologique of the CRCHUS in providing logistical and technical support in data collection and study coordination. Also, the authors underline the contribution of Mrs. Nathalie Ouellet, patient partner for her involvement in the creation of the research protocol.
References
1. Goldberg DS, and McGee SJ. Pain as a global public health priority. BMC Public Health. (2011) 11:770. doi: 10.1186/1471-2458-11-770
2. Available online at: https://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698#Pain (2019).
3. Sanders SH, Harden RN, and Vicente PJ. Evidence-based clinical practice guidelines for interdisciplinary rehabilitation of chronic nonmalignant pain syndrome patients. Pain Pract. (2005) 5:303–15. doi: 10.1111/j.1533-2500.2005.00033.x
4. Doury-Panchout F, Metivier JC, Borie-Malavieille MJ, and Fouquet B. VO2max in patients with chronic pain: comparative analysis with objective and subjective tests of disability. Ann Phys Rehabil Med. (2012) 55:294–311. doi: 10.1016/j.rehab.2012.04.001
5. Sakai Y, Matsui H, Ito S, Hida T, Ito K, Koshimizu H, et al. Sarcopenia in elderly patients with chronic low back pain. Osteoporos Sarcopenia. (2017) 3:195–200. doi: 10.1016/j.afos.2017.09.001
6. Moriarty O, Ruane N, O'Gorman D, Maharaj CH, Mitchell C, Sarma KM, et al. Cognitive impairment in patients with chronic neuropathic or radicular pain: an interaction of pain and age. Front Behav Neurosci. (2017) 11:100. doi: 10.3389/fnbeh.2017.00100
7. O'Reilly A. La dépression et l'anxiété dans la douleur chronique : une revue de travaux. J Thérapie Comport Cogn. (2011) 21:126–31. doi: 10.1016/j.jtcc.2011.08.003
8. Reinert A, Treede RD, and Bromm B. The pain inhibiting pain effect: an electrophysiological study in humans. Brain Res. (2000) 862:103–10. doi: 10.1016/S0006-8993(00)02077-1
9. LeBars D. Diffuse noxious inhibitory controls (DNIC). II. Lack of effect on non-convergent neurones, supraspinal involvement and theoretical implications. Pain. (1979) 6:305–27. doi: 10.1016/0304-3959(79)90050-2
10. Cathcart S, Winefield AH, Rolan P, and Lushington K. Reliability of temporal summation and diffuse noxious inhibitory control. Pain Res Manag. (2009) 14:433–8. doi: 10.1155/2009/523098
11. Kong J-T, Johnson KA, Balise RR, and Mackey S. Test-retest reliability of thermal temporal summation using an individualized protocol. J Pain. (2013) 14:79–88. doi: 10.1016/j.jpain.2012.10.010
12. Kennedy DL, Kemp HI, Ridout D, Yarnitsky D, and Rice ASC. Reliability of conditioned pain modulation: a systematic review. Pain. (2016) 157:2410–9. doi: 10.1097/j.pain.0000000000000689
13. Mendell LM, and Wall PD. Response of single dorsal cord cells to peripheral cutaneous unmyelinated fibers. Nature. (1965) 206:97–9. doi: 10.1038/206097a0
14. Staud R, Vierck CJ, Cannon RL, Mauderli AP, and Price DD. Abnormal sensitization and temporal summation of second pain (wind-up) in patients with ®bromyalgia syndrome. Pain. (2001) 91:165–75. doi: 10.1016/S0304-3959(00)00432-2
15. Staud R, Cannon RC, Mauderli AP, Robinson ME, Price DD, and Vierck CJ. Temporal summation of pain from mechanical stimulation of muscle tissue in normal controls and subjects with fibromyalgia syndrome. Pain. (2003) 102:87–95. doi: 10.1016/s0304-3959(02)00344-5
16. Giesecke T, Gracely RH, Grant MAB, Nachemson A, Petzke F, Williams DA, et al. Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum. (2004) 50:613–23. doi: 10.1002/art.20063
17. Arendt-Nielsen L, Nie H, Laursen MB, Laursen BS, Madeleine P, Simonsen OH, et al. Sensitization in patients with painful knee osteoarthritis. Pain. (2010) 149:573–81. doi: 10.1016/j.pain.2010.04.003
18. Yarnitsky D, Arendt-Nielsen L, Bouhassira D, Edwards RR, Fillingim RB, Granot M, et al. Recommendations on terminology and practice of psychophysical DNIC testing. Eur J Pain. (2010) 14:339. doi: 10.1016/j.ejpain.2010.02.004
19. LeBars D, Dikenson AH, and Besson J-M. Diffuse noxious inhibitory controle (DNIC). I. Effects on dorsal horn convergent neurones in the rat. Pain. (1979) 6:283–304. doi: 10.1016/0304-3959(79)90049-6
20. Pielsticker A, Haag G, Zaudig M, and Lautenbacher S. Impairment of pain inhibition in chronic tension-type headache. Pain. (2005) 118:215–23. doi: 10.1016/j.pain.2005.08.019
21. Johannesson U, de Boussard CN, Jansen GB, and Bohm-Starke N. Evidence of diffuse noxious inhibitory controls (DNIC) elicited by cold noxious stimulation in patients with provoked vestibulodynia. Pain. (2007) 130:31–9. doi: 10.1016/j.pain.2006.10.022
22. Leonard G, Goffaux P, Mathieu D, Blanchard J, Kenny B, and Marchand S. Evidence of descending inhibition deficits in atypical but not classical trigeminal neuralgia. Pain. (2009) 147:217–23. doi: 10.1016/j.pain.2009.09.009
23. King CD, Wong F, Currie T, Mauderli AP, Fillingim RB, and Riley JL. Deficiency in endogenous modulation of prolonged heat pain in patients with irritable bowel syndrome and temporomandibular disorder. Pain. (2009) 143:172–8. doi: 10.1016/j.pain.2008.12.027
24. O'Brien AT, Deitos A, Triñanes Pego Y, Fregni F, and Carrillo-de-la-Peña MT. Defective endogenous pain modulation in fibromyalgia: a meta-analysis of temporal summation and conditioned pain modulation paradigms. J Pain. (2018) 19:819–36. doi: 10.1016/j.jpain.2018.01.010
25. Yarnitsky D. Role of endogenous pain modulation in chronic pain mechanisms and treatment. Pain. (2015) 156:S24–31. doi: 10.1097/01.j.pain.0000460343.46847.58
26. Weissman-Fogel I, Granovsky Y, Crispel Y, Ben-Nun A, Best LA, Yarnitsky D, et al. Enhanced presurgical pain temporal summation response predicts post-thoracotomy pain intensity during the acute postoperative phase. J Pain. (2009) 10:628–36. doi: 10.1016/j.jpain.2008.12.009
27. Yarnitsky D, Granot M, Nahman-Averbuch H, Khamaisi M, and Granovsky Y. Conditioned pain modulation predicts duloxetine efficacy in painful diabetic neuropathy. Pain. (2012) 153:1193–8. doi: 10.1016/j.pain.2012.02.021
28. Olesen SS, Graversen C, Bouwense SAW, van Goor H, Wilder-Smith OHG, and Drewes AM. Quantitative sensory testing predicts pregabalin efficacy in painful chronic pancreatitis. PLoS ONE. (2013) 8:e57963. doi: 10.1371/journal.pone.0057963
29. Kisler LB, Weissman-Fogel I, Coghill RC, Sprecher E, Yarnitsky D, and Granovsky Y. Individualization of migraine prevention: a randomized controlled trial of psychophysical-based prediction of duloxetine efficacy. Clin J Pain. (2019) 35:753–65. doi: 10.1097/AJP.0000000000000739
30. Lautenbacher S, Kunz M, Strate P, Nielsen J, and Arendt-Nielsen L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain. (2005) 115:410–8. doi: 10.1016/j.pain.2005.03.025
31. Edwards RR, and Fillingim RB. Effects of age on temporal summation and habituation of thermal pain: clinical relevance in healthy older and younger adults. J Pain. (2001) 2:307–17. doi: 10.1054/jpai.2001.25525
32. Khan J, Korczeniewska O, Benoliel R, Kalladka M, Eliav E, and Nasri-Heir C. Age and gender differences in mechanically induced intraoral temporal summation and conditioned pain modulation in healthy subjects. Oral Surg Oral Med Oral Pathol Oral Radiol. (2018) 126:134–41. doi: 10.1016/j.oooo.2018.03.021
33. Washington LL, Gibson SJ, and Helme RD. Age-related differences in the endogenous analgesic response to repeated cold water immersion in human volunteers. Pain. (2000) 89:89–96. doi: 10.1016/S0304-3959(00)00352-3
34. Tsao JCI, Seidman LC, Evans S, Lung KC, Zeltzer LK, and Naliboff BD. Conditioned pain modulation in children and adolescents: effects of sex and age. J Pain. (2013) 14:558–67. doi: 10.1016/j.jpain.2013.01.010
35. Tousignant-Laflamme Y, and Marchand S. Excitatory and inhibitory pain mechanisms during the menstrual cycle in healthy women. Pain. (2009) 146:47–55. doi: 10.1016/j.pain.2009.06.018
36. Bulls H, Freeman E, Anderson A, Ness T, and Goodin B. Sex differences in experimental measures of pain sensitivity and endogenous pain inhibition. J Pain Res. (2015) 8:311–20. doi: 10.2147/JPR.S84607
37. Larivière M, Goffaux P, Marchand S, and Julien N. Changes in pain perception and descending inhibitory controls start at middle age in healthy adults. Clin J Pain. (2007) 23:506–10. doi: 10.1097/AJP.0b013e31806a23e8
38. Grashorn W, Sprenger C, Forkmann K, Wrobel N, and Bingel U. Age-dependent decline of endogenous pain control: exploring the effect of expectation and depression. PLoS ONE. (2013) 8:e75629. doi: 10.1371/journal.pone.0075629
39. Edwards RR, Smith MT, Stonerock G, and Haythornthwaite JA. Pain-related catastrophizing in healthy women is associated with greater temporal summation of and reduced habituation to thermal pain. Clin J Pain. (2006) 22:730–7. doi: 10.1097/01.ajp.0000210914.72794.bc
40. Rhudy JL, Martin SL, Terry EL, France CR, Bartley EJ, DelVentura JL, et al. Pain catastrophizing is related to temporal summation of pain but not temporal summation of the nociceptive flexion reflex. Pain. (2011) 152:794–801. doi: 10.1016/j.pain.2010.12.041
41. Awali A, Alsouhibani AM, and Hoeger Bement M. Lean mass mediates the relation between temporal summation of pain and sex in young healthy adults. Biol Sex Differ. (2018) 9:42. doi: 10.1186/s13293-018-0200-z
42. Awali A, Nevsimal R, Hrdina E, Alsouhibani A, and Bement MH. Physical activity and pain catastrophizing predict temporal summation of mechanical pain. J Pain. (2018) 19:S51. doi: 10.1016/j.jpain.2017.12.118
43. Weissman-Fogel I, Sprecher E, and Pud D. Effects of catastrophizing on pain perception and pain modulation. Exp Brain Res. (2008) 186:79–85. doi: 10.1007/s00221-007-1206-7
44. Granot M, Weissman-Fogel I, Crispel Y, Pud D, Granovsky Y, Sprecher E, et al. Determinants of endogenous analgesia magnitude in a diffuse noxious inhibitory control (DNIC) paradigm: do conditioning stimulus painfulness, gender and personality variables matter? Pain. (2008) 136:142–9. doi: 10.1016/j.pain.2007.06.029
45. Goffaux P, Redmond WJ, Rainville P, and Marchand S. Descending analgesia–when the spine echoes what the brain expects. Pain. (2007) 130:137–43. doi: 10.1016/j.pain.2006.11.011
46. Nahman-Averbuch H, Nir R-R, Sprecher E, and Yarnitsky D. Psychological factors and conditioned pain modulation: a meta-analysis. Clin J Pain. (2016) 32:541–54. doi: 10.1097/AJP.0000000000000296
47. Chalaye P, Devoize L, Lafrenaye S, Dallel R, and Marchand S. Cardiovascular influences on conditioned pain modulation. Pain. (2013) 154:1377–82. doi: 10.1016/j.pain.2013.04.027
48. de la Coba P, Bruehl S, Duschek S, and Reyes del Paso GA. Blood pressure-related pain modulation in fibromyalgia: differentiating between static vs. dynamic pain indicators. Int J Psychophysiol. (2018) 134:79–85. doi: 10.1016/j.ijpsycho.2018.10.006
49. Zogopoulos P, Vasileiou I, Patsouris E, and Theocharis SE. The role of endocannabinoids in pain modulation. Fundam Clin Pharmacol. (2013) 27:64–80. doi: 10.1111/fcp.12008
50. Hohmann AG, and Suplita RL. Endocannabinoid mechanisms of pain modulation. AAPS J. (2006) 16:E693–708. doi: 10.1208/aapsj080479
51. Cichewicz DL. Synergistic interactions between cannabinoid and opioid analgesics. Life Sci. (2004) 74:1317–24. doi: 10.1016/j.lfs.2003.09.038
52. Treister R, Pud D, Ebstein RP, Laiba E, Raz Y, Gershon E, et al. Association between polymorphisms in serotonin and dopamine-related genes and endogenous pain modulation. J Pain. (2011) 12:875–83. doi: 10.1016/j.jpain.2011.02.348
53. Parent AJ, Beaudet N, Daigle K, Sabbagh R, Sansoucy Y, Marchand S, et al. Relationship between blood- and cerebrospinal fluid–bound neurotransmitter concentrations and conditioned pain modulation in pain-free and chronic pain subjects. J Pain. (2015) 16:436–44. doi: 10.1016/j.jpain.2015.01.007
54. Potvin S, Larouche A, Normand E, de Souza JB, Gaumond I, Grignon S, et al. DRD3 Ser9Gly polymorphism is related to thermal pain perception and modulation in chronic widespread pain patients and healthy controls. J Pain. (2009) 10:969–75. doi: 10.1016/j.jpain.2009.03.013
55. Potvin S, and Marchand S. Pain facilitation and pain inhibition during conditioned pain modulation in fibromyalgia and in healthy controls. Pain. (2016) 157:1704–10. doi: 10.1097/j.pain.0000000000000573
56. Martel MO, Petersen K, Cornelius M, Arendt-Nielsen L, and Edwards R. Endogenous pain modulation profiles among individuals with chronic pain: relation to opioid use. J Pain. (2019) 20:462–71. doi: 10.1016/j.jpain.2018.10.004
57. Bosma RL, Cheng JC, Rogachov A, Kim JA, Hemington KS, Osborne NR, et al. Brain dynamics and temporal summation of pain predicts neuropathic pain relief from ketamine infusion. Anesthesiology. (2018) 129:1015–24. doi: 10.1097/ALN.0000000000002417
58. Eckert NR, Vierck CJ, Simon CB, Calderon S, Cruz-Almeida Y, Staud R, et al. Methodological considerations for the temporal summation of second pain. J Pain. (2017) 18:1488–95. doi: 10.1016/j.jpain.2017.07.009
59. Harte S, Schoen C, Ablin J, Ichesco E, Bhavsar R, Kochlefl L, et al. A novel paradigm to evaluate conditioned pain modulation in fibromyalgia. J Pain Res. (2016) 9:711–9. doi: 10.2147/JPR.S115193
60. Granovsky Y, Sprecher E, and Sinai A. Motor corticospinal excitability: a novel facet of pain modulation? Pain Rep. (2019) 4:e725. doi: 10.1097/PR9.0000000000000725
61. Mlekusch S, Schliessbach J, Cámara RJA, Arendt-Nielsen L, Jüni P, and Curatolo M. Do central hypersensitivity and altered pain modulation predict the course of chronic low back and neck pain? Clin J Pain. (2013) 29:673–80. doi: 10.1097/AJP.0b013e318275773c
62. Grosen K, Vase L, Pilegaard HK, Pfeiffer-Jensen M, and Drewes AM. Conditioned pain modulation and situational pain catastrophizing as preoperative predictors of pain following chest wall surgery: a prospective observational cohort study. PLoS ONE. (2014) 9:e90185. doi: 10.1371/journal.pone.0090185
63. Teles AR, Ocay DD, Bin Shebreen A, Tice A, Saran N, Ouellet JA, et al. Evidence of impaired pain modulation in adolescents with idiopathic scoliosis and chronic back pain. Spine J. (2019) 19:677–86. doi: 10.1016/j.spinee.2018.10.009
64. Matre D. Conditioned pain modulation (CPM) is not one single phenomenon–large intra-individual differences depend on test stimulus (TS) and several other independent factors. Scand J Pain. (2013) 4:8–9. doi: 10.1016/j.sjpain.2012.11.003
65. Shi Y, Weingarten TN, Mantilla CB, Hooten WM, and Warner DO. Smoking and pain pathophysiology and clinical implications. Anesthesiol J Am Soc Anesthesiol. (2010) 113:977–92. doi: 10.1097/ALN.0b013e3181ebdaf9
66. Ditre JW, Zale EL, Heckman BW, and Hendricks PS. A measure of perceived pain and tobacco smoking interrelations: pilot validation of the pain and smoking inventory. Cogn Behav Ther. (2017) 46:339–51. doi: 10.1080/16506073.2016.1256347
67. Horn-Hofmann C, Büscher P, Lautenbacher S, and Wolstein J. The effect of nonrecurring alcohol administration on pain perception in humans: a systematic review. J Pain Res. (2015) 8:175–87. doi: 10.2147/JPR.S79618
68. Horn-Hofmann C, Capito ES, Wolstein J, and Lautenbacher S. Acute alcohol effects on conditioned pain modulation, but not temporal summation of pain. Pain. (2019) 160:2063–71. doi: 10.1097/j.pain.0000000000001597
69. Baratloo A, Rouhipour A, Forouzanfar MM, Safari S, Amiri M, and Negida A. The role of caffeine in pain management: a brief literature review. Anesthesiol Pain Med. (2016) 6:e33193. doi: 10.5812/aapm.33193
70. Roberge P, Doré I, Menear M, Chartrand É, Ciampi A, Duhoux A, et al. A psychometric evaluation of the French Canadian version of the hospital anxiety and depression scale in a large primary care population. J Affect Disord. (2013) 147:171–9. doi: 10.1016/j.jad.2012.10.029
71. Sullivan MJL, Bishop SR, and Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 7:524–32. doi: 10.1037/1040-3590.7.4.524
72. French DJ, Noël M, Vigneau F, French JA, Cyr CP, and Evans RT. L'Échelle de dramatisation face à la douleur PCS-CF: Adaptation canadienne en langue française de l'échelle ≪Pain Catastrophizing Scale≫. Can J Behav Sci Rev Can Sci Comport. (2005) 37:181–92. doi: 10.1037/h0087255
73. Daut RL, Cleeland CS, and Flanery RC. Development of the Wisconsin Brief Pain Questionnaire to assess pain in cancer and other diseases. Pain. (1983) 17:197–210. doi: 10.1016/0304-3959(83)90143-4
74. Keller S, Bann CM, Dodd SL, Schein J, Mendoza TR, and Cleeland CS. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin J Pain. (2004) 20:309–18. doi: 10.1097/00002508-200409000-00005
75. Tan G, Jensen MP, Thornby JI, and Shanti BF. Validation of the brief pain inventory for chronic nonmalignant pain. J Pain. (2004) 5:133–7. doi: 10.1016/j.jpain.2003.12.005
76. Poundja J, Fikretoglu D, Guay S, and Brunet A. Validation of the French Version of the Brief Pain Inventory in Canadian veterans suffering from traumatic stress. J Pain Symptom Manage. (2007) 33:720–6. doi: 10.1016/j.jpainsymman.2006.09.031
77. Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. (2005) 114:29–36. doi: 10.1016/j.pain.2004.12.010
78. Derogadis LR, and Savitz KL. The SCL-90-R, Brief Symptom Inventory, and Matching Clinical Rating Scales. In: Maruish ME, editor. The Use of Psychological Testing for Treatment Planning and Outcomes Assessment. Mahwah, NJ: Lawrence Erlbaum Associates Publishers (1999). p. 679–724.
79. Fortin MF, and Coutu-Wakulczyk G. Validation et Normalisation d'une Mesure de Santé Mentale: le SCL-90-R. Rapport présenté au Conseil québécois de la recherche sociale (CQRS). Faculté des sciences infirmières, Université de Montréal (1985).
80. Potter L, McCarthy C, and Oldham J. Algometer reliability in measuring pain pressure threshold over normal spinal muscles to allow quantification of anti-nociceptive treatment effects. Int J Osteopath Med. (2006) 9:113–9. doi: 10.1016/j.ijosm.2006.11.002
81. Park G, Kim CW, Park SB, Kim MJ, and Jang SH. Reliability and usefulness of the pressure pain threshold measurement in patients with myofascial pain. Ann Rehabil Med. (2011) 35:412. doi: 10.5535/arm.2011.35.3.412
82. Koo TK, Guo J, and Brown CM. Test-retest reliability, repeatability, and sensitivity of an automated deformation-controlled indentation on pressure pain threshold measurement. J Manipulative Physiol Ther. (2013) 36:84–90. doi: 10.1016/j.jmpt.2013.01.001
83. Bruehl S, and Chung OY. Interactions between the cardiovascular and pain regulatory systems: an updated review of mechanisms and possible alterations in chronic pain. Neurosci Biobehav Rev. (2004) 28:395–414. doi: 10.1016/j.neubiorev.2004.06.004
84. Benarroch EE. Descending monoaminergic pain modulation: bidirectional control and clinical relevance. Neurology. (2008) 71:217–21. doi: 10.1212/01.wnl.0000318225.51122.63
85. Tousignant-Laflamme Y, Pagé S, Goffaux P, and Marchand S. An experimental model to measure excitatory and inhibitory pain mechanisms in humans. Brain Res. (2008) 1230:73–9. doi: 10.1016/j.brainres.2008.06.120
86. Yarnitsky D, Bouhassira D, Drewes AM, Fillingim RB, Granot M, Hansson P, et al. Recommendations on practice of conditioned pain modulation (CPM) testing: CPM consensus meeting recommendations 2014. Eur J Pain. (2015) 19:805–6. doi: 10.1002/ejp.605
88. Damien J, Colloca L, Bellei-Rodriguez C-É, and Marchand S. Pain modulation: from conditioned pain modulation to placebo and nocebo effects in experimental and clinical pain. Int Rev Neurobiol. (2018) 139:255–96. doi: 10.1016/bs.irn.2018.07.024
89. Price DD, McGrath PA, Rafii A, and Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. (1983) 17:45–56. doi: 10.1016/0304-3959(83)90126-4
90. Bahreini M, Jalili M, and Moradi-Lakeh M. A comparison of three self-report pain scales in adults with acute pain. J Emerg Med. (2015) 48:10–8. doi: 10.1016/j.jemermed.2014.07.039
91. Karcioglu O, Topacoglu H, Dikme O, and Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. (2018) 36:707–14. doi: 10.1016/j.ajem.2018.01.008
92. Ruscheweyh R, Stumpenhorst F, Knecht S, and Marziniak M. Comparison of the cold pressor test and contact thermode-delivered cold stimuli for the assessment of cold pain sensitivity. J Pain. (2010) 11:728–36. doi: 10.1016/j.jpain.2009.10.016
93. Peduzzi P, Concato J, Kemper E, Holford TR, and Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. (1996) 49:1373–9. doi: 10.1016/S0895-4356(96)00236-3
94. van Smeden M, de Groot JAH, Moons KGM, Collins GS, Altman DG, Eijkemans MJC, et al. No rationale for 1 variable per 10 events criterion for binary logistic regression analysis. BMC Med Res Methodol. (2016) 16:163. doi: 10.1186/s12874-016-0267-3
95. Ogundimu EO, Altman DG, and Collins GS. Adequate sample size for developing prediction models is not simply related to events per variable. J Clin Epidemiol. (2016) 76:175–82. doi: 10.1016/j.jclinepi.2016.02.031
96. Austin PC, Allignol A, and Fine JP. The number of primary events per variable affects estimation of the subdistribution hazard competing risks model. J Clin Epidemiol. (2017) 83:75–84. doi: 10.1016/j.jclinepi.2016.11.017
97. Austin PC, and Steyerberg EW. Events per variable (EPV) and the relative performance of different strategies for estimating the out-of-sample validity of logistic regression models. Stat Methods Med Res. (2017) 26:796–808. doi: 10.1177/0962280214558972
98. van Smeden M, Moons KG, de Groot JA, Collins GS, Altman DG, Eijkemans MJ, et al. Sample size for binary logistic prediction models: beyond events per variable criteria. Stat Methods Med Res. (2019) 28:2455–74. doi: 10.1177/0962280218784726
99. Steyerberg EW, and Harrell FE. Prediction models need appropriate internal, internal–external, and external validation. J Clin Epidemiol. (2016) 69:245–7. doi: 10.1016/j.jclinepi.2015.04.005
100. Copas JB. Regression, prediction and shrinkage. J R Stat Soc B Methodol. (1983) 45:311–35. doi: 10.1111/j.2517-6161.1983.tb01258.x
101. Riley RD, Ensor J, Snell KIE, Harrell FE, Martin GP, Reitsma JB, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. (2020) 368:m441. doi: 10.1136/bmj.m441
102. Schopflocher D, Taenzer P, and Jovey R. The prevalence of chronic pain in Canada. Pain Res Manag. (2011) 16:445–50. doi: 10.1155/2011/876306
103. Hastie T, Tibshirani R, and Friedman J. The Elements of Statistical Learning Data Mining, Inference, and Prediction. Springer Series in Statistics, Vol. 2. New York, NY: Springer (2001).
104. Fan J, and Gijbels I. Local Polynomial Modelling and Its Applications, Monographs on Statistics and Applied Probability. London: CRC Press (1996).
105. Fontaine D, Blond S, Mertens P, and Lanteri-Minet M. Traitement neurochirurgical de la douleur chronique. Neurochirurgie. (2015) 61:22–9. doi: 10.1016/j.neuchi.2014.11.008
106. Lyons R, and Koneti KK. Surgical management for chronic pain. Surg Oxf. (2019) 37:472–7. doi: 10.1016/j.mpsur.2019.05.006
107. Oliveira CB, Franco MR, Maher CG, Ferreira PH, Morelhão PK, Damato TM, et al. Physical activity–based interventions using electronic feedback may be ineffective in reducing pain and disability in patients with chronic musculoskeletal pain: a systematic review with meta-analysis. Arch Phys Med Rehabil. (2018) 99:1900–12. doi: 10.1016/j.apmr.2017.10.013
108. Bouckenaere D. La douleur chronique et la relation médecin-malade. Cah Psychol Clin. (2007) 28:167. doi: 10.3917/cpc.028.0167
109. Yarnitsky D, Crispel Y, Eisenberg E, Granovsky Y, Ben-Nun A, Sprecher E, et al. Prediction of chronic post-operative pain: pre-operative DNIC testing identifies patients at risk. Pain. (2008) 138:22–8. doi: 10.1016/j.pain.2007.10.033
Keywords: chronic pain, temporal summation, conditional pain modulation, pain modulation profile, catecholamines, clinical feasibility
Citation: Vincenot M, Coulombe-Lévêque A, Sean M, Camirand Lemyre F, Gendron L, Marchand S and Léonard G (2021) Development and Validation of a Predictive Model of Pain Modulation Profile to Guide Chronic Pain Treatment: A Study Protocol. Front. Pain Res. 2:606422. doi: 10.3389/fpain.2021.606422
Received: 14 September 2020; Accepted: 13 January 2021;
Published: 15 February 2021.
Edited by:
Vivianne L. Tawfik, Stanford University, United StatesReviewed by:
Marc Landry, Université de Bordeaux, FranceKristin Schreiber, Brigham and Women's Hospital and Harvard Medical School, United States
Copyright © 2021 Vincenot, Coulombe-Lévêque, Sean, Camirand Lemyre, Gendron, Marchand and Léonard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillaume Léonard, Z3VpbGxhdW1lLmxlb25hcmQyQHVzaGVyYnJvb2tlLmNh
†These authors have contributed equally to this work