 Chunqiang Wang
Chunqiang Wang Tianye Huang2
Tianye Huang2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 10 February 2025
Sec. Surgical Oncology
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1545547
This article is part of the Research Topic Optimizing Rectal Cancer Treatment: Evaluating Minimally Invasive Surgical Techniques and Patient Selection View all articles
Background: The gold standard for the treatment of rectal cancer is radical surgery with total mesorectal excision (TME). As one of the alternatives to radical surgery, local resection has been proposed for the treatment of early rectal cancer. The purpose of this article was to evaluate the safety and efficacy of transanal endoscopic microsurgery (TEM) in the treatment of early rectal cancer.
Methods: By searching the PubMed, Cochrane Library, Web of Science, and China National Knowledge Infrastructure databases, we selected all articles on TEM for early rectal cancer. Two researchers independently completed the entire process from screening, inclusion to data extraction and performed statistical analysis using RevMan 5.3. The primary outcomes included basic patient characteristics, overall survival rate, disease-free survival rate, disease-specific survival rate, recurrence rate, and complication rate and type.
Results: A total of 33 articles were included in this meta-analysis. The results showed that the overall survival rate was 100% for T0 stage, 98.1% for Tis (carcinoma in situ) stage, and 80.2% for early stage rectal cancer patients (83.9% for T1 and 72.4% for T2). The weighted overall survival rate was 94% (RD = 0.94, 95% CI = 0.93–0.95, I2 = 80%, P < 0.00001) for all stage patients, the weighted disease-free survival rate was 91% (RD = 0.91, 95% CI = 0.90–0.93, I2 = 83%, P < 0.00001), and the disease-specific survival rate was 97% (RD = 0.97, 95% CI = 0.96–0.98, I2 = 63%, P < 0.00001). The recurrence rate was 0.5% for T0 stage, 1.9% for Tis stage, and 11.9% for early stage rectal cancer patients (8.1% for T1 and 19.7% for T2). The weighted recurrence rate was 7% (RD = 0.07, 95% CI = 0.06–0.08, I2 = 69%, P < 0.00001) for all stage patients. The weighted complications rate was 11% (RD = 0.11, 95% CI = 0.10–0.12, I2 = 66%, P < 0.00001) for all stage patients, with Clavien-Dindo grade I accounting for 77.7%, Clavien-Dindo grade II accounting for 8%, and Clavien-Dindo grade III accounting for 14.3%.
Conclusion: The results showed that TEM has a high postoperative survival rate, low recurrence rate, and low complication rate in the T0 stage, Tis stage, and T1 stage, indicating its good safety and efficacy. For the treatment of T2 stage, TEM has a lower overall survival rate and a higher recurrence rate. Our meta-analysis results suggest that TEM alone is not recommended as a curative treatment for T2 stage; on the contrary, TME is more frequently recommended.
As one of the common malignancies, the incidence and mortality of colorectal cancer in all cancer diseases have long been at the forefront globally. According to the latest data statistics, there were 1.92 million new cases of colorectal cancer worldwide in 2022, ranking third among all tumors, and 904,000 deaths, ranking second among all tumors. In China, there were about 517,000 new cases of colorectal cancer in 2022, accounting for 26.9% of the world’s new cases of colorectal cancer, and about 240,000 deaths from colorectal cancer, accounting for 26.5% of the world’s colorectal deaths (1–3). A reported cancer-specific survival rate is over 95% at 5 years after radical resection as the gold standard surgical modality for the treatment of early rectal cancer (4, 5). However, although radical surgery is valid in removing the cancer, patient death and local recurrence cannot be completely avoided. Moreover, the occurrence of postoperative complications, such as about 26% of genitourinary dysfunction, 5%–10% of anastomotic fistula, and about 30% of temporary or permanent stomas, severely reduces the quality of life of patients (6–11). Therefore, local resection was proposed as one of the alternatives for the treatment of early rectal cancer. At present, the common clinical local resections include endoscopic submucosal dissection, transanal minimally invasive surgery, standard transanal excision, and so forth (12–14). However, these local resection methods have not been widely accepted due to positive tumor resection margins and increased reports of tumor fragments (15).
With the development of the concept of minimally invasive surgery, Buess et al. proposed a local resection procedure for early rectal cancer in 1983 and named it transanal endoscopic microsurgery (TEM) (16). Some clinical studies have shown that TEM has a lower recurrence rate and complication rate compared with traditional transanal local resection, and postoperative patients have a higher quality of life (17, 18). The emergence and development of TEM provide new surgical options for the treatment of early rectal cancer. Due to its less invasive nature, the local amplification function increases the possibility of resection of complete specimens with lateral and vertical margins without tumor, which is considered the most effective method for complete resection of local tumors (19). Therefore, TEM is considered the preferred local resection method for the treatment of early rectal cancer and is currently used in more than 400 centers worldwide for therapeutic use in patients with T1 or T2 rectal cancer without lymph node metastasis and distant metastases (20, 21). Because there is still about an 8.6% risk of lymph node metastasis in early rectal cancer, and TEM cannot remove lymph nodes, the postoperative recurrence rate and survival rate still need a lot of clinical data research to observe (22). Therefore, there is no unified conclusion on the safety and efficacy of TEM in early rectal cancer.
As far as we know, no one has ever analyzed the safety and efficacy of TEM in early rectal cancer alone. This meta-analysis aims to collect relevant literature and analyze the efficacy and safety of TEM in the treatment of patients with early rectal cancer.
According to the PRISMA, we searched the PubMed, Cochrane Library, Web of Science, and China National Knowledge Infrastructure databases (inception-June 2024). We used the following keywords and subheadings: “transanal endoscopic microsurgery,” “rectal cancer,” “rectal tumor,” “local excision,” and “TEM.” In addition, we also manually searched the reference data in the retrieved literature.
Inclusion criteria: Rectal cancer; the pathological stage was either T1 or T2, and the preoperative examination showed no lymph node metastasis and distant metastasis; the surgical procedure was TEM; clinical research.
Exclusion criteria: The patient data was incomplete to extract the required study data; republished literature; randomized controlled trial or meta-analysis; the full text could not be accessed.
Two reviewers individually screened the retrieved literature according to the search criteria, and the controversial article was finally decided by the corresponding author. The extracted information included details of the included studies, tumor stage, postoperative recurrence rate, survival rate, and postoperative complication rate and type.
The methodological index for non-randomized studies (MINORS) was adopted to assess risk bias and the quality of the included studies. This tool consists of eight domains (1): aim (2), inclusion criteria (3), exclusion criteria (4), intervention description (5), outcome measures (6), follow-up duration (7), follow-up rate (8), method of statistical analysis. A score of 0 indicates no report at all, 1 indicates reported but incomplete information, and 2 indicates reported and sufficient information. Higher scores indicate less risk bias. It was defined as good (score 11–16), average (score 5–10), or poor (score 0–4).
The rectoscope was inserted into the rectum to the tumor site, and the electric knife made a circular margin marking line along the normal rectal mucosa 1 cm outside the base edge of the tumor. The tumor tissue was completely removed along the marking line. The wound was continuously closed with sutures.
We used Revman 5.3 from the Cochrane Collaboration for the statistical analysis. Risk differences (RD) and 95% confidence intervals (CI) are used to represent the dichotomous variables. Based on the heterogeneity of the I2 tests, the results were evaluated using a random effect model (I2 > 75%) or a fixed effect model (I2 < 75%). P < 0.05 was considered statistically significant. Potential biases are shown as forest plots.
By searching the literature in the database, a total of 1,040 related articles on TEM for early rectal cancer were found. After initial screening that followed the inclusion and exclusion criteria, we obtained 45 relevant articles by reading the titles and abstracts. Then, by reading the full text of the initially screened articles, we again excluded articles for which the required study data were not available. Finally, a total of 33 articles (23–55) were obtained and included in this study. The specific PRISMA flowchart is shown in Figure 1.
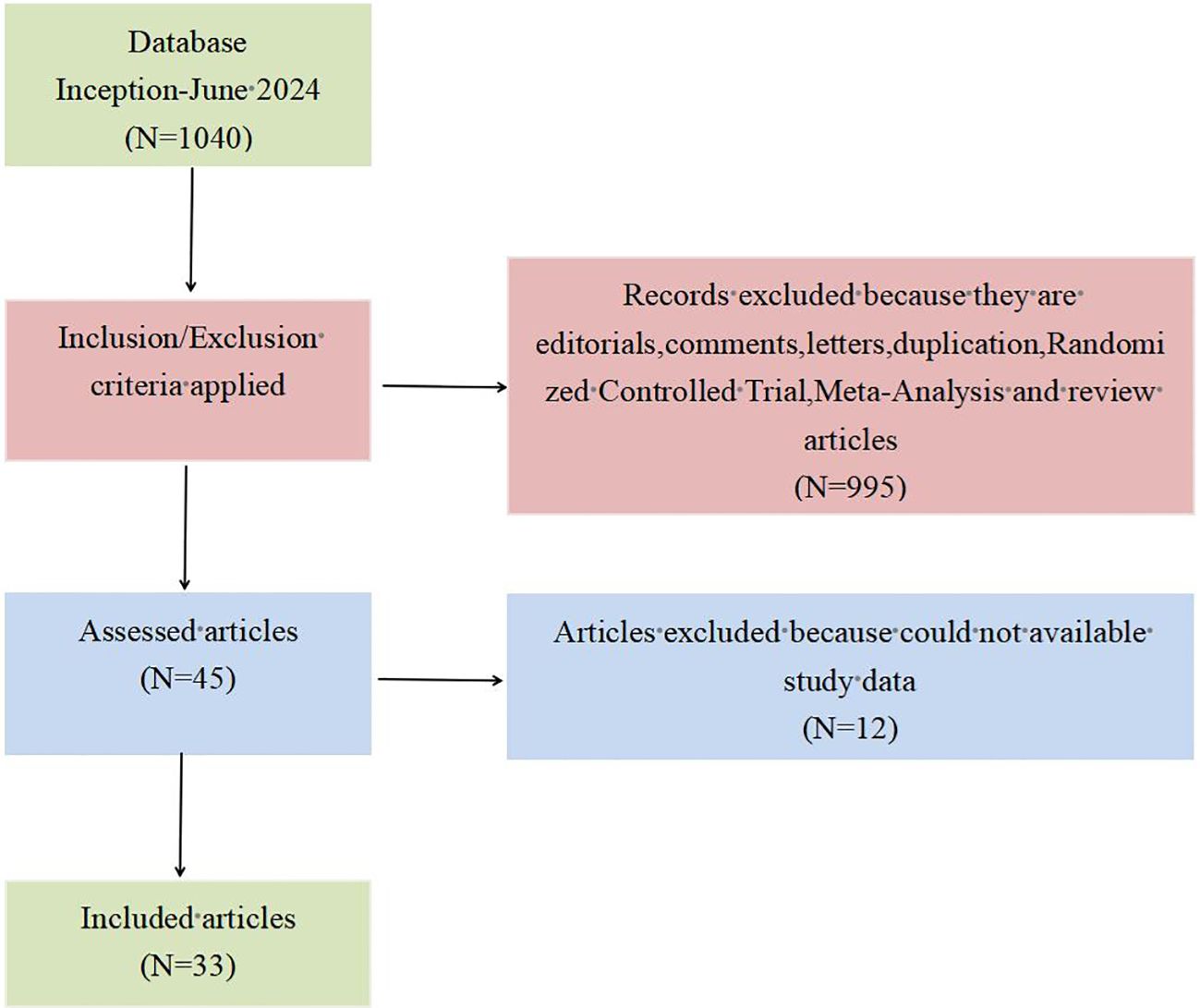
Figure 1. PRISMA flow diagram for the literature search.
A total of 33 articles published between 1996 and 2024 were included in this meta-analysis. These articles contained a total of 2,160 patients treated with TEM, including 105 Tis stage, 263 T0 stage, 1,208 T1 stage, and 584 T2 stage. In terms of quality evaluation, the MINORS scores ranged from 13 to 15, indicating less risk of bias assessment for the articles in the included studies. The details of the included studies are provided in Table 1.
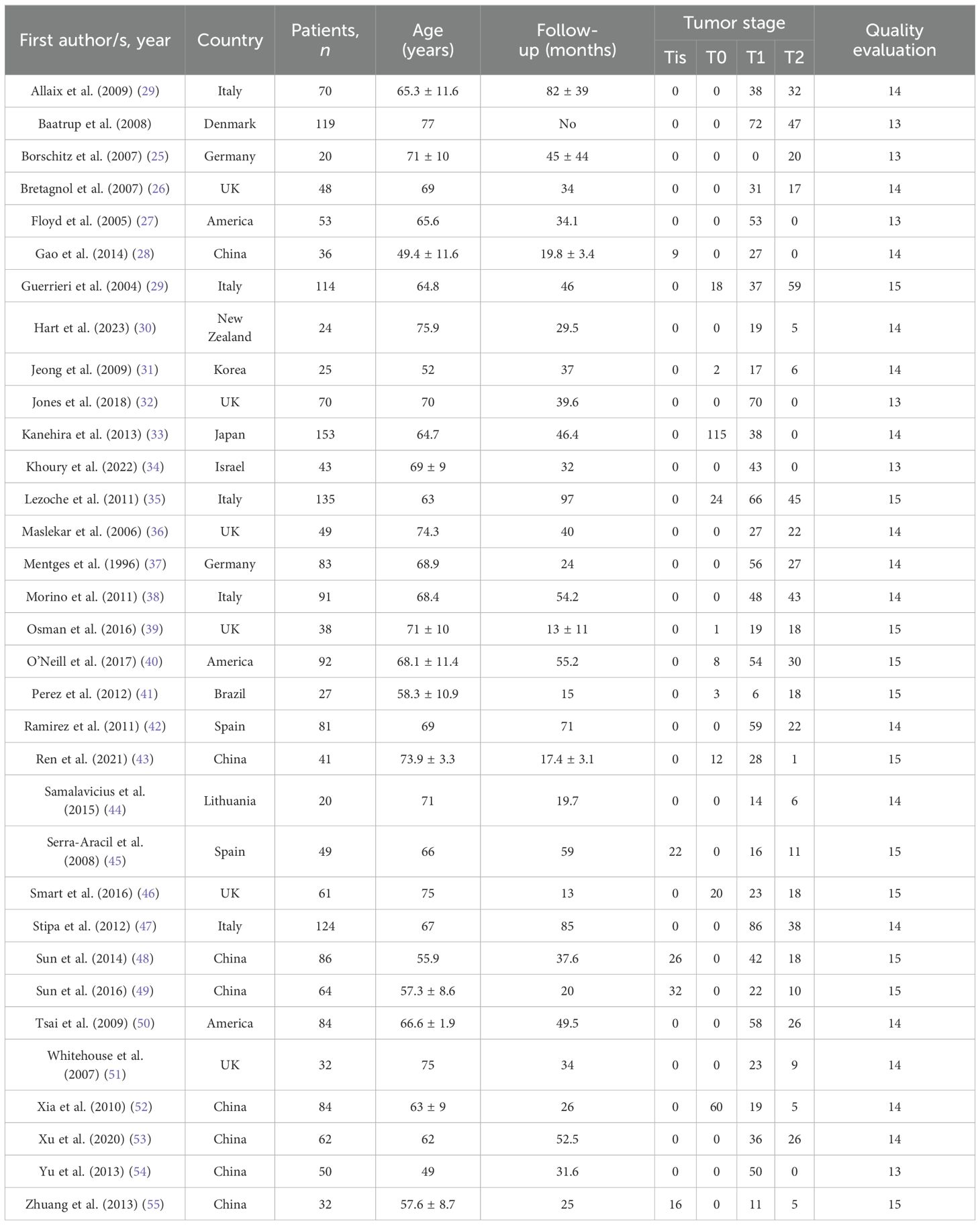
Table 1. Details of the included studies.
The overall survival rate was 100% for T0 stage, 98.1% for Tis stage, and 80.2% for early stage rectal cancer patients (83.9% for T1 and 72.4% for T2). The weighted average overall survival rate was 94% (RD = 0.94; 95% CI = 0.93–0.95; I2 = 80%; P < 0.00001) for all stage patients (Figure 2); the weighted average disease-free survival was 91% (RD = 0.91; 95% CI = 0.90–0.93; I2 = 83%; P < 0.00001) (Figure 3); and disease-specific survival was 97% (RD = 0.97; 95% CI = 0.96–0.98; I2 = 63%; P < 0.00001) (Figure 4).
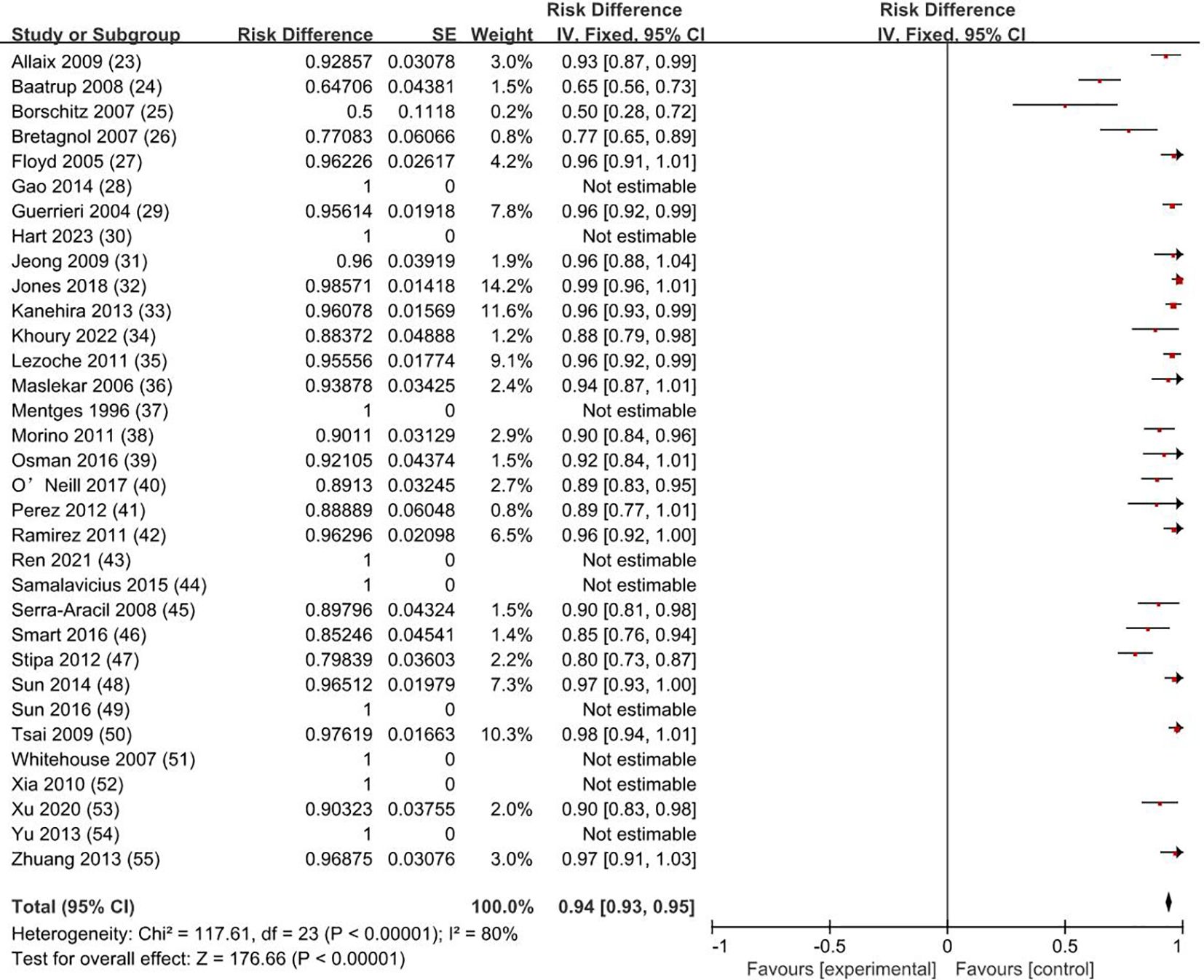
Figure 2. Overall survival rate. SE, standard error; CI, confidence interval.
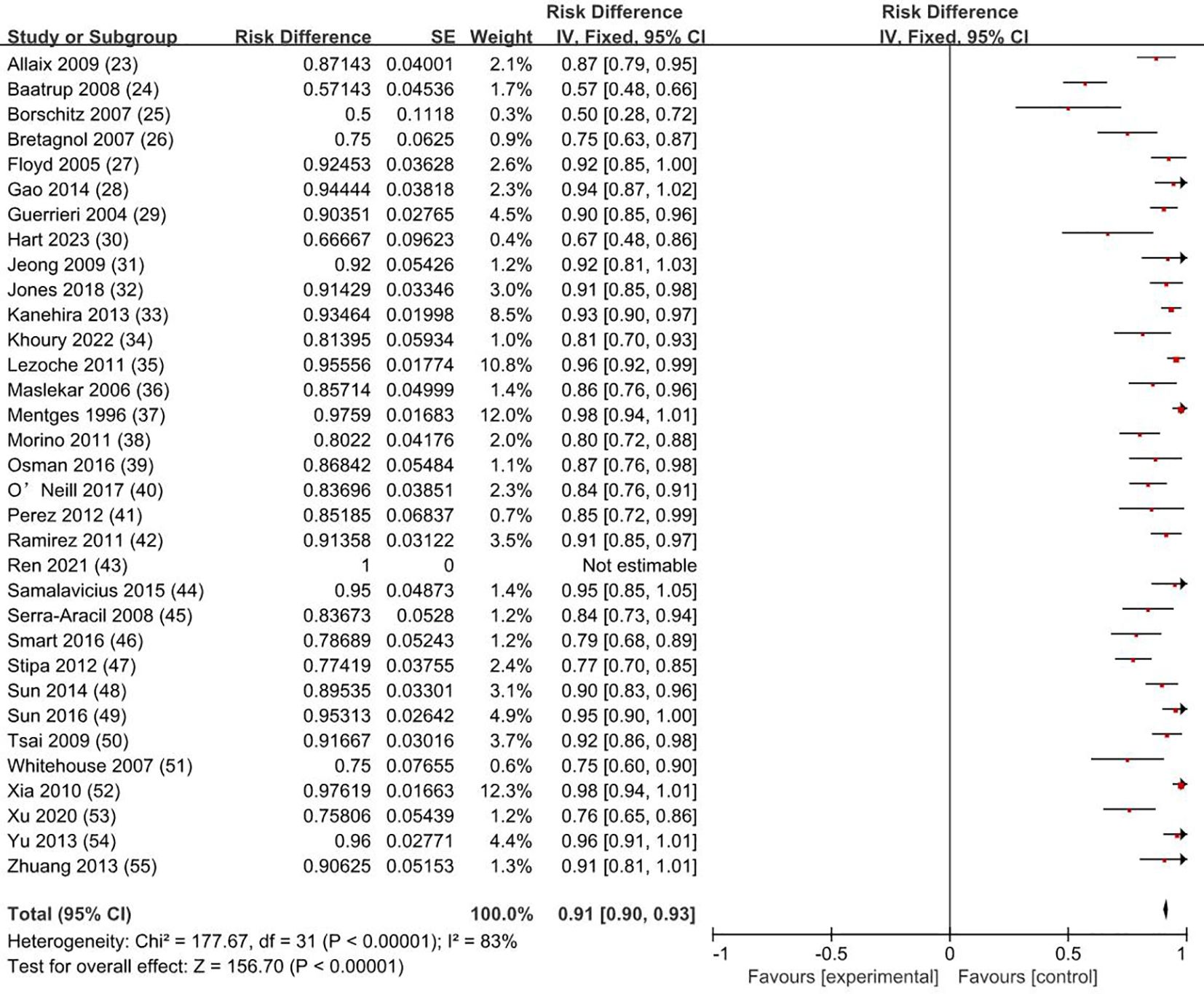
Figure 3. Disease-free survival rate. SE, standard error; CI, confidence interval.
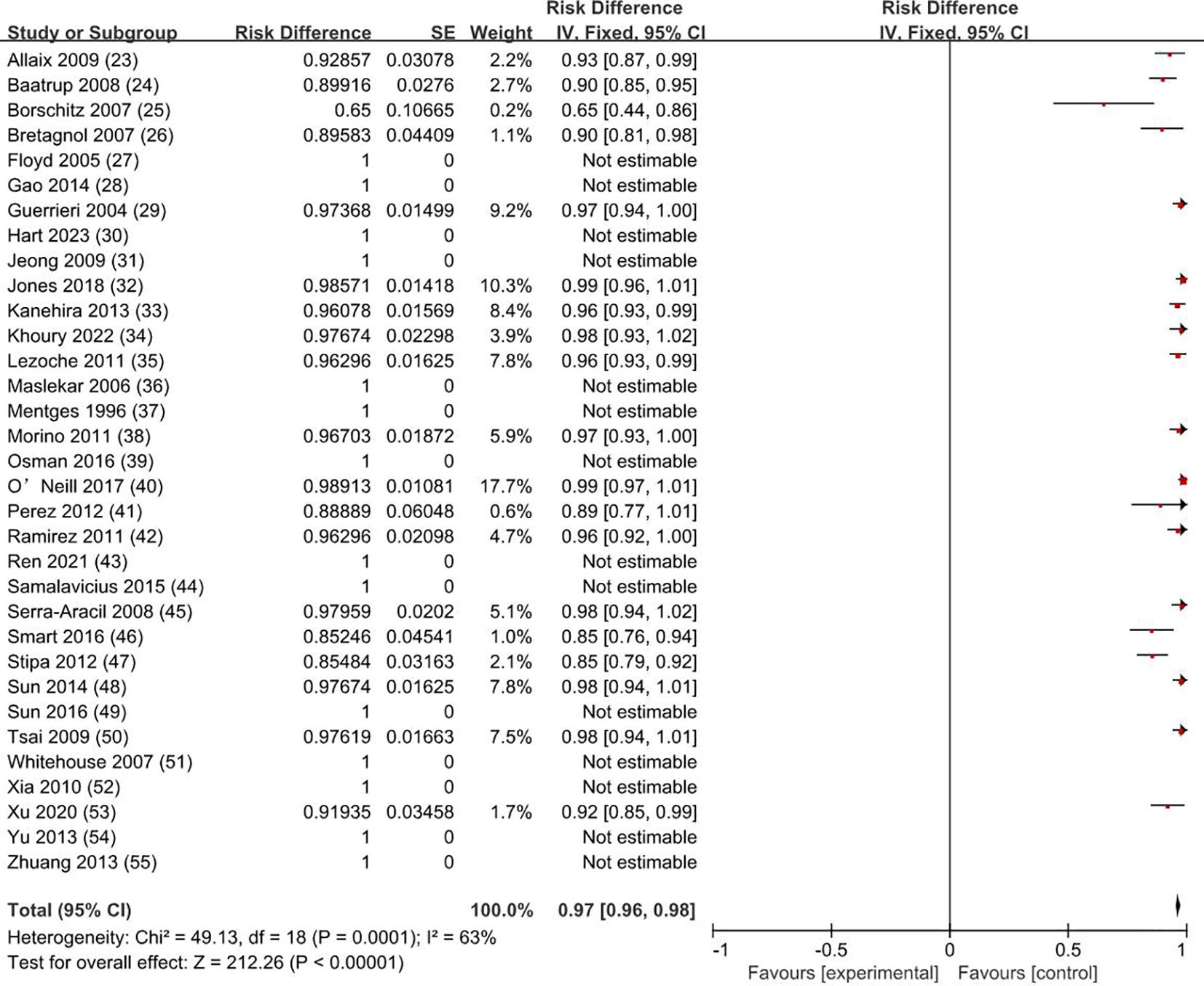
Figure 4. Disease-specific survival rate. SE, standard error; CI, confidence interval.
Our meta-analysis showed that the recurrence rate was 0.5% for T0 stage, 1.9% for Tis stage, and 11.9% for early stage rectal cancer patients (8.1% for T1 and 19.7% for T2). The weighted average recurrence was 7% (RD = 0.07; 95% CI = 0.06–0.08; I2 = 69%; P < 0.00001) for all stage patients (Figure 5).
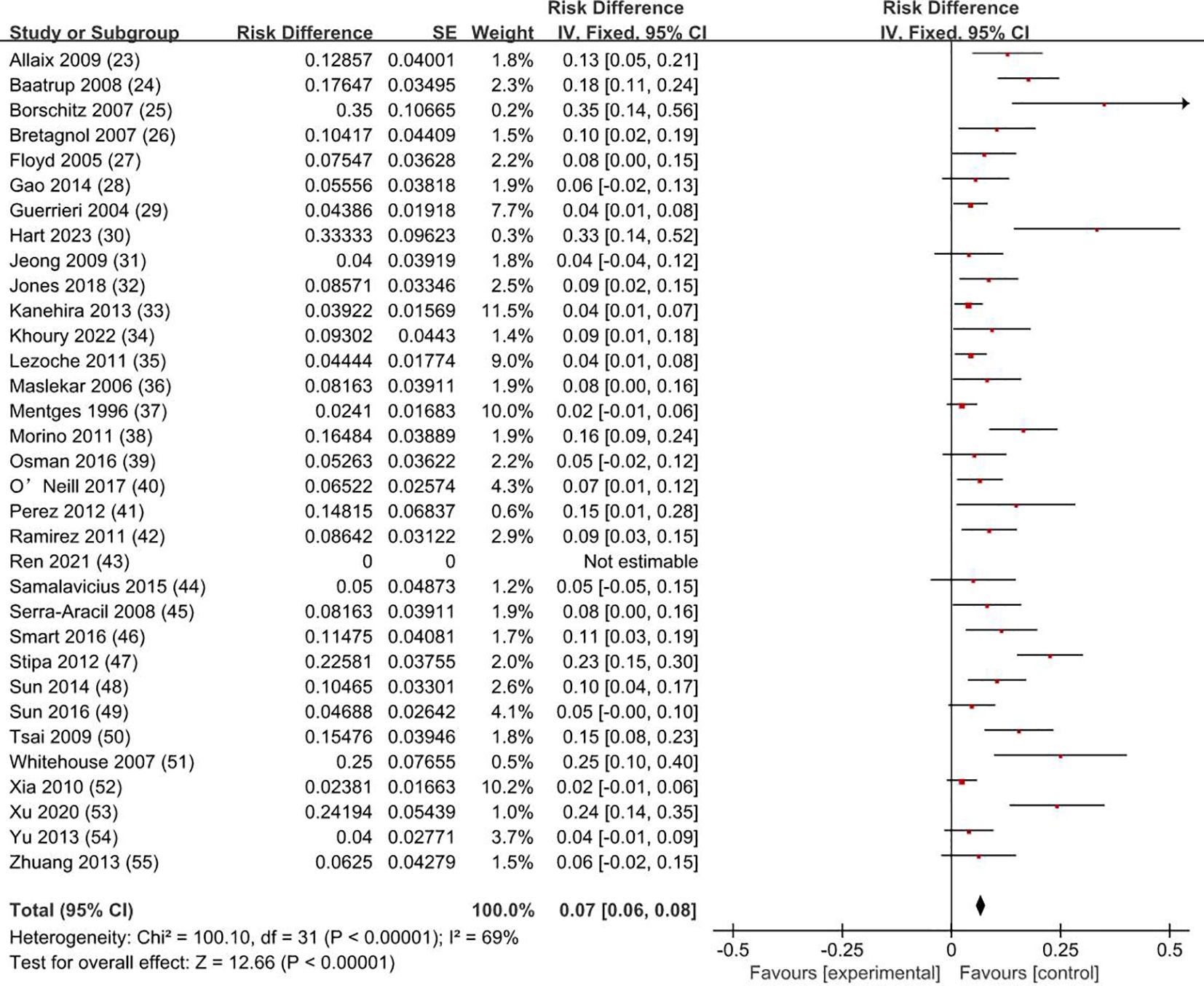
Figure 5. Recurrence rate. SE, standard error; CI, confidence interval.
The weighted average complication rate was 11% (RD = 0.11; 95% CI = 0.10–0.12; I2 = 66%; P < 0.00001) (Figure 6) for all stage patients, with Clavien-Dindo grade I accounting for 77.7%, Clavien-Dindo grade II accounting for 8%, and Clavien-Dindo grade III accounting for 14.3%. The most common postoperative complication was temporary anal incontinence in 64 patients (30%), followed by bleeding in 44 patients (21%) and dehiscence of sutures in 30 patients (14%). Specific types of complications are shown in Figure 7.
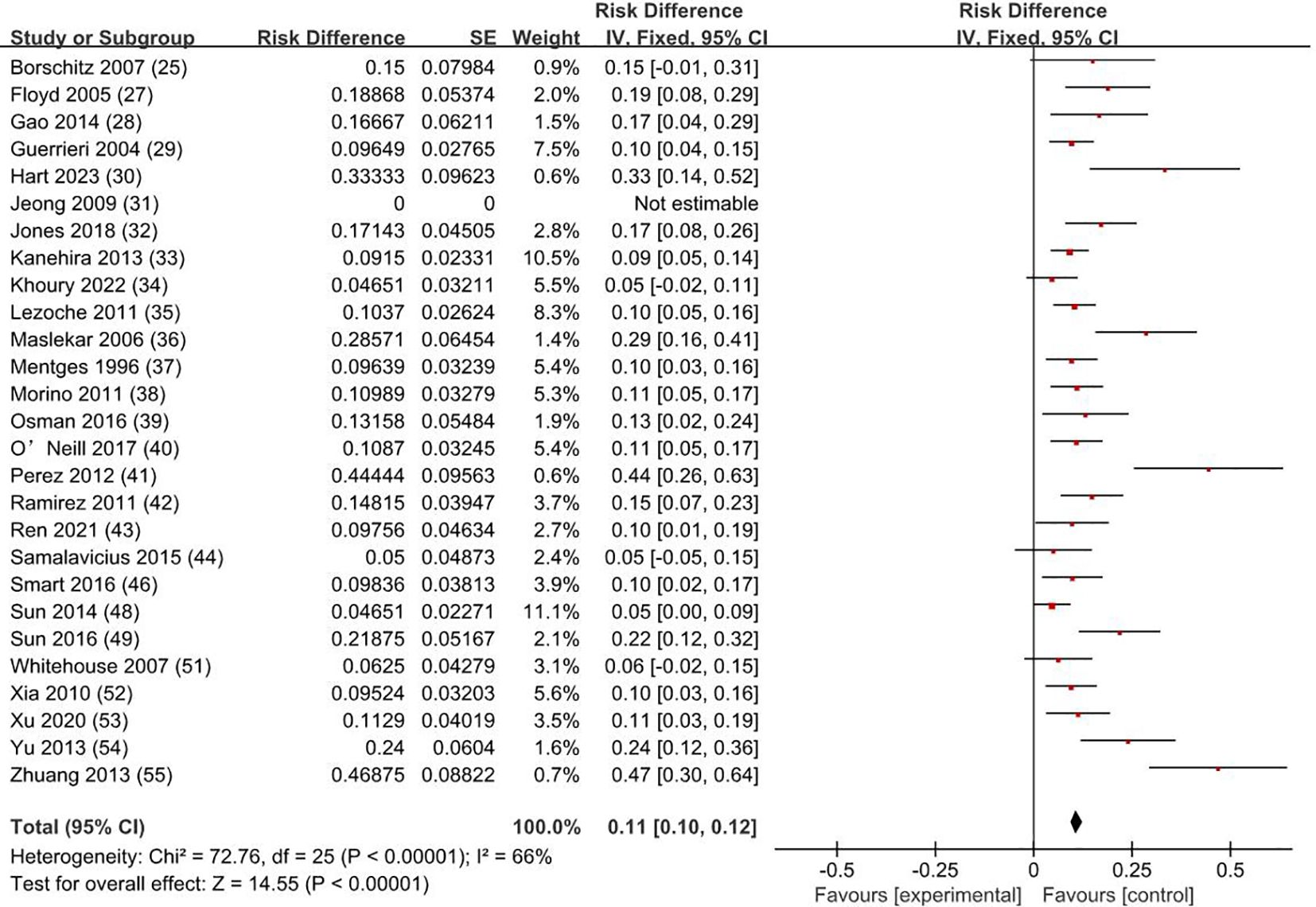
Figure 6. Complication rate. SE, standard error; CI, confidence interval.
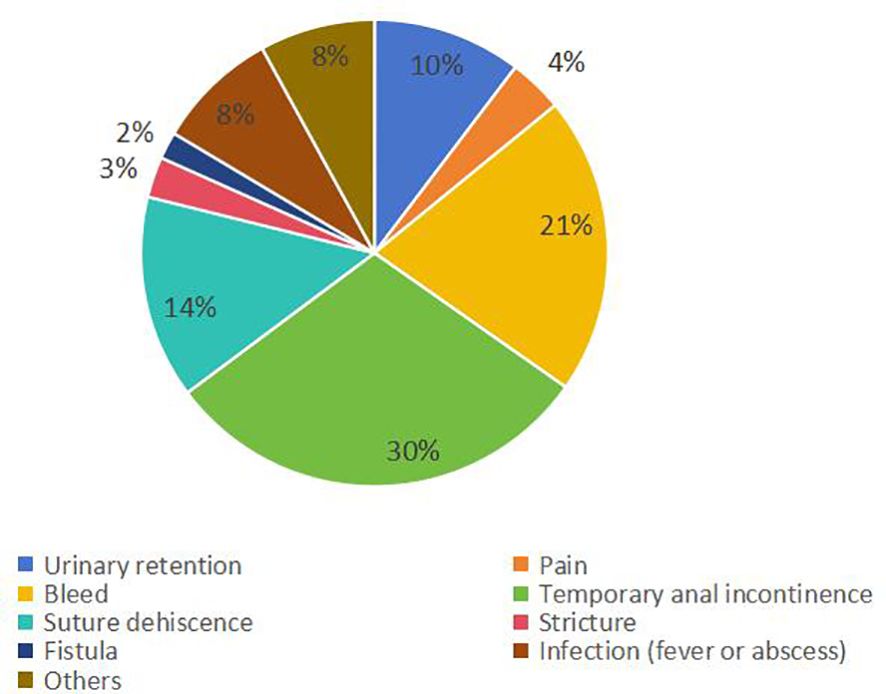
Figure 7. Type and proportion of complications.
Early stage rectal cancer refers to the rectal infiltrating adenocarcinoma that only invaded the submucosa or muscularis propria, with no lymph node metastasis or distant metastasis (T1N0M0, T2N0M0), accounting for about 11% of rectal cancer. T0 refers to the absence of evidence of a primary tumor, and Tis refers to carcinoma in situ (the tumor invades the proper muc layer but does not penetrate the muscularis mucosae) (56). Salinas HM et al. found that 89% of T1 patients and 72% of T2 patients experienced unnecessary radical resection (57). TEM combines endoscopic techniques and minimally invasive techniques, with the advantages of less trauma, sufficient visual field exposure, and precise surgical resection (58). TEM removes only the local tumor tissue and cannot clear occult metastatic lymph nodes, while the probability of lymph node metastasis was considered to be 0%–15% in T1 and 16%–28% in T2 (59). The results of the clinical study by Stornes T et al. showed that the 5-year local recurrence rate of TEM patients was 14.5% (T1), and 11.4% (T2), which was significantly higher than the 1.4% (T1) and 4.4% (T2) of total mesorectal excision (TME) (60). Therefore, although many physicians advocate the use of TEM for early rectal cancer, its safety and efficacy remain controversial.
The results of our analysis showed that the recurrence rate was 0.5% for T0 stage, 1.9% for Tis stage, and 11.9% for early stage rectal cancer patients (8.1% for T1 and 19.7% for T2). The weighted average recurrence rate was 7% for all stage patients. Junginger T et al. believe that local tumor recurrence after rectal cancer surgery is related to residual postoperative tumor tissue, and they think that the integrity of tumor resection and negative resection margin are key factors in reducing the local recurrence rate (61). Chen YY et al. suggested that local tumor recurrence after rectal cancer surgery is related to lymphatic metastasis due to incomplete regional lymph node resection, and they think that potential lymph node metastasis in the mesentery is the main cause of local recurrence (22). Weiser M R agrees with Chen YY et al. and believes that preoperative classification of lymph node metastasis is a key factor in patient selection of treatment (62). This may explain why the results of this study show that the recurrence rate of T2 stage rectal cancer is significantly higher than that of T1 stage. Morino M et al. believe that tumor size is also one of the reasons for the recurrence of rectal cancer after surgery; the larger the tumor, the higher the risk of postoperative recurrence (38). McCloud et al. found that the recurrence rate of rectal tumors with >5cm was significantly higher than that of smaller tumors (25.9% vs. 8.9%) (63). In addition, some studies believe that the degree of tumor differentiation and nerve vascular invasion around the tumor is associated with postoperative recurrence (61, 64). Local resection is a minimum resection of the rectal wall under the premise of ensuring radical treatment. The traditional transanal local resection after the surgical margin positive rate is 27%, and the local recurrence rate is as high as 39% (65). By combining minimally invasive surgical techniques with endoscopic microscopy, TEM can better expose the surgical field, achieve complete resection of the tumor, and reduce the positive margin rate. Currently, patients with rectal masses that are assessed as T0 or Tis stage after thorough preoperative evaluation, or T1 stage rectal cancer with tumor invasion <30% of the intestinal circumference, tumor size <3 cm, good differentiation, first layer of the submucosa, no vascular or neural invasion, and exclusion of lymph node metastasis and distant metastasis, are considered to have low-risk features for local recurrence (61, 66). Unfortunately, few of the articles we included (26, 32, 33, 38, 39, 54) distinguished and analyzed the pathological factors and depth of submucosal invasion associated with poor prognosis in T1 rectal cancer. Among all the patients with T1 rectal cancer who had a recurrence and whose tumor invasion depth was recorded, the Sm2+Sm3 recurrence rate was 83.3%. The study by Kapiteijn E et al. reported that the local recurrence rate after TEM in patients with T1-2N0 rectal cancer was 0.7% (67). In our analysis, the recurrence rate after TEM for T2 rectal cancer was 19.7%, which was higher than the 11.4% reported by Stornes T et al., and much higher than the 4.4% recurrence rate after TME (60). Such a high recurrence is unacceptable therefore, for such patients, TME is more frequently recommended.
Our study showed that the overall survival rate was 100% for T0 stage, 98.1% for Tis stage, and 80.2% for early stage rectal cancer patients (83.9% for T1 and 72.4% for T2). The weighted overall survival rate was 94% for all stage patients, the weighted disease-free survival rate was 91%, and the disease-specific survival rate was 97%. How to improve the survival rate of cancer patients and avoid their death has always been one of the important purposes pursued by clinicians. Patients with early rectal cancer have a lower risk of lymph node metastasis and distant metastasis, and whether it is necessary to carry on radical resection is still quite controversial. Through complete resection of local tumor tissue, TEM is now favored by the majority of clinicians and early rectal cancer patients. Zaheer et al. showed that the overall survival after radical resection of stage I tumors was 85% (68). Hazard et al. showed that the 5-year disease-specific survival rate of T1 and T2 after radical resection was 97% and 95% (69). The results of this study showed that disease-specific survival after TEM was comparable to radical resection without significant differences. Furthermore, there was no significant difference in disease-free survival between local excision and radical resection, as shown by Tan S et al. (70).
Middleton PF et al. reported a complication rate of 0% to 28% after TEM (71). The results of this study showed that the weighted complication rate was 11% for all patients, with Clavien-Dindo grade I accounting for 77.7%, Clavien-Dindo grade II accounting for 8%, and Clavien-Dindo grade III accounting for 14.3%. Simon P Bach et al. reported that common complications of radical resection include genitourinary function impairment and irregular defecation (72). Unlike radical resection, TEM, as a surgical method of local resection, combining the advantages of minimally invasive surgery and endoscopic surgery, can avoid autonomic nerve injury in the pelvic cavity, thus avoiding injury to patients’ urogenital function (73). Our study showed that most patients have Clavien-Dindo I postoperative complications, which generally do not require special treatment, with only a minority of Clavien-Dindo II–III patients needing interventions such as blood transfusions or surgery. The most common complication after TEM was temporary anal incontinence, accounting for 3.8% of the total population (30% of the complication). Cataldo PA et al. believe that the reason may be the thicker diameter of the endoscope used by TEM (4 cm), which leads to overstretching injury of the anal sphincter, resulting in the occurrence of temporary anal incontinence, but the symptoms will disappear within three months (74). Our study showed that the bleeding complications after TEM represented 2.6% of the total population (21% of the complications). The reason may come from the surgical wound or anal enlargement causing anal skin tear and internal hemorrhoid bleeding, which is usually controllable. Furthermore, our study showed that 1.8% of patients had postoperative suture dehiscence (14% of the complication), and the possible reason is the large wound surface and the excessive postoperative suture tension. Wei Li et al. by meta-analysis showed that the complication rate after TEM is lower than after radical resection (75).
Of course, our study also has some limitations. First, some of the included literature are retrospective studies, and the authenticity and accuracy of the collected data were low; second, due to differences in inclusion criteria, there is a certain degree of heterogeneity; third, the different follow-up times of patients in different literature may affect the postoperative recurrence rate and survival outcomes. Therefore, more prospective studies with uniform criteria are needed.
In conclusion, limited evidence indicates that TEM, as an alternative to radical resection of rectal cancer, has a low rate of postoperative complications in treat of T1 rectal cancer, T0 stage and Tis stage tumors, consistent with the minimally invasive surgical treatment philosophy. TEM has a high-postoperative survival rate and a low recurrence rate, consistent with the management goal of rectal tumor patients. For the treatment of T2 rectal cancer, the overall survival rate is low and the recurrence rate is high, it is not recommended to use TEM alone as a radical treatment.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
CW: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. TH: Data curation, Validation, Writing – review & editing. XW: Data curation, Supervision, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Everyone who contributed significantly to this study has been listed.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. (2023) 73:233–54. doi: 10.3322/caac.21772
3. Wang F, Chen G, Zhang Z, Yuan Y, Wang Y, Gao YH, et al. The Chinese Society of Clinical Oncology (CSCO): Clinical guidelines for the diagnosis and treatment of colorectal cancer, 2024. Cancer Commun (Lond). (2024). doi: 10.1002/cac2.12639
4. Heald RJ, Santiago I, Pares O, Carvalho C, Figueiredo N. The perfect total mesorectal excision obviates the need for anything else in the management of most rectal cancers. Clin Colon Rectal Surg. (2017) 30:324–32. doi: 10.1055/s-0037-1606109
5. Zhang X, Gao Y, Dai X, Zhang H, Shang Z, Cai X, et al. Short- and long-term outcomes of transanal versus laparoscopic total mesorectal excision for mid-to-low rectal cancer: a meta-analysis. Surg Endosc. (2018) 33:972–85. doi: 10.1007/s00464-018-6527-z
6. Kauff DW, Roth YDS, Bettzieche RS, Kneist W. Fecal incontinence after total mesorectal excision for rectal cancer-impact of potential risk factors and pelvic intraoperative neuromonitoring. World J Surg Oncol. (2020) 18:12. doi: 10.1186/s12957-020-1782-6
7. Nguyen TH, Chokshi RV. Low anterior resection syndrome. Curr Gastroenterol Rep. (2020) 22:48. doi: 10.1007/s11894-020-00785-z
8. Celentano V, Cohen R, Warusavitarne J, Faiz O, Chand M. Sexual dysfunction following rectal cancer surgery. Int J Colorectal Dis. (2017) 32:1523–30. doi: 10.1007/s00384-017-2826-4
9. Bleier JI, Maykel JA. Outcomes following proctectomy. Surg Clin North Am. (2013) 93:89–106. doi: 10.1016/j.suc.2012.09.012
10. Park IJ, Choi GS, Lim KH, Kang BM, Jun SH. Laparoscopic resection of extraperitoneal rectal cancer: a comparative analysis with open resection. Surg Endosc. (2009) 23:1818–24. doi: 10.1007/s00464-008-0265-6
11. Nastro P, Beral D, Hartley J, Monson JR. Local excision of rectal cancer: review of literature. Dig Surg. (2005) 22:6–15. doi: 10.1159/000084345
12. Xiong X, Wang C, Wang B, Shen Z, Jiang K, Gao Z, et al. Can transanal endoscopic microsurgery effectively treat T1 or T2 rectal cancer?A systematic review and meta-analysis. Surg Oncol. (2021) 37:101561. doi: 10.1016/j.suronc.2021.101561
13. Park SU, Min YW, Shin JU, Choi JH, Kim YH, Kim JJ, et al. Endoscopic submucosal dissection or transanal endoscopic microsurgery for nonpolypoid rectal high grade dysplasia and submucosa-invading rectal cancer. Endoscopy. (2012) 44:1031–6. doi: 10.1055/s-0032-1310015
14. Woo JS, Cho MJ, Park IK, Im YC, Kim GY, Park DJ, et al. Initial case series experience with robotic-assisted transanal minimally invasive surgery performed with da Vinci single-port system for the excision of rectal cancer. Surg Endosc. (2024) 38:6762–70. doi: 10.1007/s00464-024-11142-w
15. Han J, Noh GT, Cheong C, Cho MS, Hur H, Min BS, et al. Transanal endoscopic operation versus conventional transanal excision for rectal tumors: case-matched study with propensity score matching. World J Surg. (2017) 41:2387–94. doi: 10.1007/s00268-017-4017-4
16. Buess G, Hutterer F, Theiss J, Böbel M, Isselhard W, Pichlmaier H. A system for a transanal endoscopic rectum operation. Chirurg. (1984) 55:677–80.
17. Flexer SM, Durham-Hall AC, Steward MA, Robinson JM. TEMS: results of a specialist centre. Surg Endosc. (2014) 28:1874–8. doi: 10.1007/s00464-013-3407-4
18. Marinello FG, Curell A, Tapiolas I, Pellino G, Vallribera F, Espin E. Systematic review of functional outcomes and quality of life after transanal endoscopic microsurgery and transanal minimally invasive surgery: a word of caution. Int J Colorectal Dis. (2020) 35:51–67. doi: 10.1007/s00384-019-03439-3
19. Ondhia M, Tamvakeras P, O'Toole P, Montazerri A, Andrews T, Farrell C, et al. Transanal endoscopic microsurgery for rectal lesions in a specialist regional early rectal cancer centre: the Mersey experience. Colorectal Dis. (2019) 21:1164–74. doi: 10.1111/codi.14730
20. Sajid MS, Leung P, Sains P, Miles WF, Baig MK. Systematic review and meta-analysis of published trials comparing the effectiveness of transanal endoscopic microsurgery and radical resection in the management of early rectal cancer. Colorectal Dis. (2014) 16:2–14. doi: 10.1111/codi.12474
21. Saclarides TJ. TEM/local excision: indications, techniques, outcomes, and the future. J Surg Oncol. (2007) 96:644–50. doi: 10.1002/jso.20922
22. Chen YY, Liu ZH, Zhu K, Shi PD, Yin L. Transanal endoscopic microsurgery versus laparoscopic lower anterior resection for the treatment of T1-2 rectal cancers. Hepatogastroenterology. (2013) 60:727–32. doi: 10.5754/hge12868
23. Allaix ME, Arezzo A, Caldart M, Festa F, Morino M. Transanal endoscopic microsurgery for rectal neoplasms: experience of 300 consecutive cases. Dis Colon Rectum. (2009) 52:1831–6. doi: 10.1007/DCR.0b013e3181b14d2d
24. Baatrup G, Breum B, Qvist N, Wille-Jørgensen P, Elbrønd H, Møller P, et al. Transanal endoscopic microsurgery in 143 consecutive patients with rectal adenocarcinoma: results from a Danish multicenter study. Colorectal Dis. (2009) 11:270–5. doi: 10.1111/j.1463-1318.2008.01600.x
25. Borschitz T, Heintz A, Junginger T. Transanal endoscopic microsurgical excision of pT2 rectal cancer: results and possible indications. Dis Colon Rectum. (2007) 50:292–301. doi: 10.1007/s10350-006-0816-7
26. Bretagnol F, Merrie A, George B, Warren BF, Mortensen NJ. Local excision of rectal tumours by transanal endoscopic microsurgery. Br J Surg. (2007) 94:627–33. doi: 10.1002/bjs.5678
27. Floyd ND, Saclarides TJ. Transanal endoscopic microsurgical resection of pT1 rectal tumors. Dis Colon Rectum. (2005) 49:164–8. doi: 10.1007/s10350-005-0269-4
28. Gao H, Li SY, Zhang QH, Zhang XP. Clinical analysis on transanal endoscopic microsurgery in the treatment of early rectal carcinoma. Chin J Colorec Dis(Electronic Edition). (2014) 3:286–7. doi: 10.3877/cma.j.issn.2095-3224.2014.04.14
29. Guerrieri M, Feliciotti F, Baldarelli M, Zenobi P, De Sanctis A, Lezoche G, et al. Sphincter-saving surgery in patients with rectal cancer treated by radiotherapy and transanal endoscopic microsurgery: 10 years' experience. Dig Liver Dis. (2004) 35:876–80. doi: 10.1016/j.dld.2003.07.004
30. Hart A, Clifford K, Thompson-Fawcett M. Recurrence after transanal endoscopic microsurgery for benign and Malignant rectal tumours: experience of a single New Zealand centre. ANZ J Surg. (2023) 94:412–7. doi: 10.1111/ans.18780
31. Jeong WK, Park JW, Choi HS, Chang HJ, Jeong SY. Transanal endoscopic microsurgery for rectal tumors: experience at Korea's National Cancer Center. Surg Endosc. (2009) 23:2575–9. doi: 10.1007/s00464-009-0466-7
32. Jones HJS, Hompes R, Mortensen N, Cunningham C. Modern management of T1 rectal cancer by transanal endoscopic microsurgery: a 10-year single-centre experience. Colorectal Dis. (2018) 20:586–92. doi: 10.1111/codi.14029
33. Kanehira E, Tanida T, Kamei A, Nakagi M, Hideshima A. A single surgeon's experience with transanal endoscopic microsurgery over 20 years with 153 early cancer cases. Minim Invasive Ther Allied Technol. (2013) 23:5–9. doi: 10.3109/13645706.2013.868814
34. Khoury W, Dauod M, Khalefah M, Duek SD, Issa N. The outcome of transanal endoscopic microsurgery and adjuvant radiotherapy in patients with high-risk T1 rectal cancer. J Minim Access Surg. (2022) 18:212–7. doi: 10.4103/jmas.JMAS_67_21
35. Lezoche G, Guerrieri M, Baldarelli M, Paganini A, D'Ambrosio G, Campagnacci R, et al. Transanal endoscopic microsurgery for 135 patients with small nonadvanced low rectal cancer (iT1-iT2, iN0): short- and long-term results. Surg endoscopy. (2011) 25:1222–9. doi: 10.1007/s00464-010-1347-9
36. Maslekar S, Pillinger SH, Monson JR. Transanal endoscopic microsurgery for carcinoma of the rectum. Surg Endosc. (2006) 21:97–102. doi: 10.1007/s00464-005-0832-z
37. Mentges B, Buess G, Effinger G, Becker HD. Local therapy of early rectal carcinoma with curative intent: implications for a change in oncologic strategy. Langenbecks Arch Chir Suppl Kongressbd. (1996) 113:543–6.
38. Morino M, Allaix ME, Caldart M, Scozzari G, Arezzo A. Risk factors for recurrence after transanal endoscopic microsurgery for rectal Malignant neoplasm. Surg Endosc. (2011) 25:3683–90. doi: 10.1007/s00464-011-1777-z
39. Osman KA, Ryan D, Afshar S, Mohamed ZK, Garg D, Gill T. Transanal endoscopic microsurgery (TEM) for rectal cancer: university hospital of north tees experience. Indian J Surg. (2016) 77:930–5. doi: 10.1007/s12262-014-1067-9
40. O'Neill CH, Platz J, Moore JS, Callas PW, Cataldo PA. Transanal endoscopic microsurgery for early rectal cancer: A single-center experience. Dis Colon Rectum. (2017) 60:152–60. doi: 10.1097/DCR.0000000000000764
41. Perez RO, Habr-Gama A, Lynn PB, São Julião GP, Bianchi R, Proscurshim I, et al. Transanal endoscopic microsurgery for residual rectal cancer (ypT0-2) following neoadjuvant chemoradiation therapy: another word of caution. Dis Colon Rectum. (2012) 56:6–13. doi: 10.1097/DCR.0b013e318273f56f
42. Ramirez JM, Aguilella V, Valencia J, Ortego J, Gracia J, Escudero P, et al. Transanal endoscopic microsurgery for rectal cancer. Long-term oncologic results. Int J colorectal disease. (2011) 26:437–43. doi: 10.1007/s00384-011-1132-9
43. Ren CC, Li F, Chen XL, Zhang YR, Zhao TJ, Qi SL. Transanal endoscopic microsurgery for early rectal cancer in patients over 70 years old. Colorectal Anal Surg department. (2021) 27:53–6. doi: 10.19668/j.cnki.issn1674-0491.2021.01.012
44. Samalavicius N, Ambrazevicius M, Kilius A, Petrulis K. Transanal endoscopic microsurgery for early rectal cancer: single center experience. Wideochir Inne Tech Maloinwazyjne. (2015) 9:603–7. doi: 10.5114/wiitm.2014.44138
45. Serra-Aracil X, Vallverdú H, Bombardó-Junca J, Pericay-Pijaume C, Urgellés-Bosch J, Navarro-Soto S. Long-term follow-up of local rectal cancer surgery by transanal endoscopic microsurgery. World J Surg. (2008) 32:1162–7. doi: 10.1007/s00268-008-9512-1
46. Smart CJ, Korsgen S, Hill J, Speake D, Levy B, Steward M, et al. Multicentre study of short-course radiotherapy and transanal endoscopic microsurgery for early rectal cancer. Br J Surg. (2016) 103:1069–75. doi: 10.1002/bjs.10171
47. Stipa F, Giaccaglia V, Burza A. Management and outcome of local recurrence following transanal endoscopic microsurgery for rectal cancer. Dis Colon Rectum. (2012) 55:262–9. doi: 10.1097/DCR.0b013e318241ef22
48. Sun N, Xia LJ, Liu QG. Curative effect analysis of transanal endoscopic microsurgery operation(TEM) in rectal carcinoma. Qingdao J Med Health Care. (2014) 46:99–101. doi: 10.3969/j.issn.1006-5571.2014.02.006
49. Sun CY. Clinical analysis of transanal endoscopic microsurgery in the t reatment of early rectal cancer. Chin Pract Med J. (2016) 11:23–4. doi: 10.14163/j.cnki.11-5547/r.2016.05.014
50. Tsai BM, Finne CO, Nordenstam JF, Christoforidis D, Madoff RD, Mellgren A. Transanal endoscopic microsurgery resection of rectal tumors: outcomes and recommendations. Dis Colon Rectum. (2009) 53:16–23. doi: 10.1007/DCR.0b013e3181bbd6ee
51. Whitehouse PA, Armitage JN, Tilney HS, Simson JN. Transanal endoscopic microsurgery: local recurrence rate following resection of rectal cancer. Colorectal Dis. (2007) 10:187–93. doi: 10.1111/j.1463-1318.2007.01291.x
52. Xia LJ, Shi B. Experince of transanal endoscopic microsurgery(TEM) in the treatment for early rectal cancer. J Surg Theory Practice. (2010) 15:357–60.
53. Xu K, Liu Y, Yu P, Shang W, Zhang Y, Jiao M, et al. Oncological outcomes of transanal endoscopic microsurgery plus adjuvant chemoradiotherapy for patients with high-risk T1 and T2 rectal cancer. J Of Laparoendoscopic Advanced Surg Techniques. (2020) 31:1006–13. doi: 10.1089/lap.2020.0706
54. Yu HH, Liu B, Chen JB, Xia LJ. Summary of the clinical data of fifty patients with pT1 rectal cancer teeated by transanal endoscopic microsurgery. Chin J Cancer Prev Treat. (2013) 20:695–98.
55. Zhuang JF, Ye JX, Huang YJ. Efficacy of transanal endoscopic microsurgery in the treatment for 32 patients with rectal cancer. J Chin Med Guide. (2013) 11:299–301.
56. Cunningham C. Local excision for early rectal cancer. Clin Oncol (R Coll Radiol). (2022) 35:82–6. doi: 10.1016/j.clon.2022.08.030
57. Salinas HM, Dursun A, Klos CL, Shellito P, Sylla P, Berger D, et al. Determining the need for radical surgery in patients with T1 rectal cancer. Arch Surg. (2011) 146:540–3. doi: 10.1001/archsurg.2011.76
58. Whiteford MH. Transanal endoscopic microsurgery (TEM) resection of rectal tumors. J Gastrointest Surg. (2007) 11:155–7. doi: 10.1007/s11605-007-0104-4
59. Sengupta S, Tjandra JJ. Local excision of rectal cancer: what is the evidence? Dis Colon Rectum. (2001) 44:1345–61. doi: 10.1007/BF02234796
60. Stornes T, Wibe A, Nesbakken A, Myklebust TÅ, Endreseth BH. National early rectal cancer treatment revisited. Dis Colon Rectum. (2016) 59:623–9. doi: 10.1097/DCR.0000000000000591
61. Junginger T, Goenner U, Hitzler M, Trinh TT, Heintz A, Roth W, et al. Analysis of local recurrences after transanal endoscopic microsurgery for low risk rectal carcinoma. Int J Colorectal Dis. (2016) 32:265–71. doi: 10.1007/s00384-016-2715-2
62. Weiser MR. AJCC 8th edition: colorectal cancer. Ann Surg Oncol. (2018) 25:1454–5. doi: 10.1245/s10434-018-6462-1
63. McCloud JM, Waymont N, Pahwa N, Varghese P, Richards C, Jameson JS, et al. Factors predicting early recurrence after transanal endoscopic microsurgery excision for rectal adenoma. Colorectal Dis. (2006) 8:581–5. doi: 10.1111/j.1463-1318.2006.01016.x
64. Glynne-Jones R, Wyrwicz L, Tiret E, Brown G, Rödel C, Cervantes A, et al. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2017) 28:22–40. doi: 10.1093/annonc/mdx224
65. Pigot F, Bouchard D, Mortaji M, Castinel A, Juguet F, Chaume J, et al. Local excision of large rectal villous adenomas: long-term results. Dis colon rectum. (2003) 46:1345–50. doi: 10.1007/s10350-004-6748-1
66. Benson AB, Venook AP, Al-Hawary MM, Cederquist L, Chen YJ, Ciombor KK, et al. Rectal cancer, version 2.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2018) 16:874–901. doi: 10.6004/jnccn.2018.0061
67. Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. (2001) 345:638–46. doi: 10.1056/NEJMoa010580
68. Zaheer S, Pemberton JH, Farouk R, Dozois RR, Wolff BG, Ilstrup D. Surgical treatment of adenocarcinoma of the rectum. Ann Surg. (1998) 227:800–11. doi: 10.1097/00000658-199806000-00003
69. Hazard LJ, Shrieve DC, Sklow B, Pappas L, Boucher KM. Local excision vs. Radical resection in T1-2 rectal carcinoma: results of a study from the surveillance, epidemiology, and end results (SEER) registry data. Gastrointest Cancer Res. (2009) 3:105–14.
70. Tan S, Xu C, Ma H, Chen S, Yang Y, Zhan Y, et al. Local resection versus radical resection for early-stage rectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis. (2022) 37:1467–83. doi: 10.1007/s00384-022-04186-8
71. Serra-Aracil X, Pericay C, Badia-Closa J, Golda T, Biondo S, Hernández P, et al. Short-term outcomes of chemoradiotherapy and local excision versus total mesorectal excision in T2-T3ab,N0,M0 rectal cancer: a multicentre randomised, controlled, phase III trial (the TAU-TEM study). Ann Oncol. (2022) 34:78–90. doi: 10.1016/j.annonc.2022.09.160
72. Bach SP, Gilbert A, Brock K, Korsgen S, Geh I, Hill J, et al. Radical surgery versus organ preservation via short-course radiotherapy followed by transanal endoscopic microsurgery for early-stage rectal cancer (TREC): a randomised, open-label feasibility study. Lancet Gastroenterol Hepatol. (2021) 6:92–105. doi: 10.1016/S2468-1253(20)30333-2
73. Serra-Aracil X, Labró-Ciurans M, Rebasa P, Mora-López L, Pallisera-Lloveras A, Serra-Pla S, et al. Morbidity after transanal endoscopic microsurgery: risk factors for postoperative complications and the design of a 1-day surgery program. Surg Endosc. (2018) 33:1508–17. doi: 10.1007/s00464-018-6432-5
74. Cataldo PA, O'Brien S, Osler T. Transanal endoscopic microsurgery: a prospective evaluation of functional results. Dis Colon Rectum. (2005) 48:1366–71. doi: 10.1007/s10350-005-0031-y
Keywords: early rectal cancer, transanal endoscopic microsurgery, local excision, endoscopic surgery, safety and efficacy
Citation: Wang C, Huang T and Wang X (2025) Efficacy and safety of transanal endoscopic microsurgery for early rectal cancer: a meta-analysis. Front. Oncol. 15:1545547. doi: 10.3389/fonc.2025.1545547
Received: 15 December 2024; Accepted: 17 January 2025;
Published: 10 February 2025.
Edited by:
Carlos Cerdán, Princess University Hospital, SpainReviewed by:
Jialin Jiang, McGill University, CanadaCopyright © 2025 Wang, Huang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chunqiang Wang, d2FuZ2NodW5xaWFuZzkzQDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.