
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 27 January 2025
Sec. Cardio-Oncology
Volume 15 - 2025 | https://doi.org/10.3389/fonc.2025.1520725
 Marte Svalastoga1
Marte Svalastoga1 Trine-Lise Larsen1,2Jorunn Brekke3Tone Enden4Hege Frøen5Herish Garresori6Eva Marie Jacobsen7Alina Carmen Porojnicu8
Trine-Lise Larsen1,2Jorunn Brekke3Tone Enden4Hege Frøen5Herish Garresori6Eva Marie Jacobsen7Alina Carmen Porojnicu8 Anne Hansen Ree1,9
Anne Hansen Ree1,9 Dag Torfoss10Elin Osvik Velle11Hilde Skuterud Wik7Waleed Ghanima1,12
Dag Torfoss10Elin Osvik Velle11Hilde Skuterud Wik7Waleed Ghanima1,12 Per Morten Sandset1,7
Per Morten Sandset1,7 Anders Erik Astrup Dahm1,2*
Anders Erik Astrup Dahm1,2*Introduction: It is unclear how drug-interaction with apixaban influences recurrent venous thromboembolism (VTE) and bleedings in cancer patients.
Methods: A post-hoc analysis of a single-arm interventional clinical trial on apixaban treatment of cancer patients with VTE to investigate whether the occurrence of any of the endpoints could be associated with the concurrent use of an interacting drug. Drugs taken by the patients during the trial period were categorized as either increasing bleeding risk, increasing thrombosis risk, both or neither.
Results: 298 patients were divided into groups based on whether they used no interacting drugs (controls, n=74), drugs increasing bleeding risk (n=55), drugs increasing thrombosis risk (n=8), or both (n=161). Odds ratios (OR) were calculated for recurrent VTE, clinically relevant non-major bleeding (CRNMB), and major bleeding during the 36-month follow-up period. Each patient took a median of 13 different drugs over the study period. 67% of the patients used drugs expected to both increase bleeding and thrombosis. The use of fluconazole appeared associated with CRNMB (OR 3.6, 95% confidence interval (CI) 0.99-13), but not with major bleeding (OR 0.56, 95% CI 0.06 - 4.8). Non-steroid anti-inflammatory drugs were not associated with CRNMB (OR 1.0, 95% CI 0.25-4.1) or major bleedings (OR 0.72, 95% CI 0.14 - 3.6). Use of antiplatelet therapy was not associated with CRNMB (OR 0.75, 95% CI, 0.22 - 2.58) or major bleeding (OR 0.2, 95% CI, 0.02-1.6). There were no major bleedings in 23 patients using aprepitant nor in the 10 patients taking macrolides. We found no association between drugs and recurrent VTE, except that there were no recurrent VTE in 19 patients using bevacizumab.
Conclusions: Despite the high number of drugs taken that could potentially interact with apixaban, none were found to clearly influence clinical outcomes, except that fluconazole may increase the risk of CRNMB.
Patients with cancer are known to be at higher risk of venous thromboembolism (VTE) than the general population (1, 2). In recent years, several studies have shown that direct-acting oral anticoagulants (DOACs) edoxaban, rivaroxaban, and apixaban are as effective as low-molecular-weight heparin (LMWH) in prevention of recurrent thrombosis. DOACs were generally found to be non-inferior to LMWH (3–6), and are currently an alternative to LMWH for cancer patients (7). Apixaban is a substrate of cytochrome P450 3A4 (CYP3A4) (8) and permeability glycoprotein 1 (P-gp) (9), which makes it susceptible to pharmacokinetic interactions with inducers or inhibitors of these pathways. Such interaction can reduce or increase the plasma concentration of apixaban, respectively. Accordingly, DOACs are not recommended for cancer patients taking anticancer therapies that significantly affect these pathways (10). Less is, however, known about how changes in the plasma concentration translate into clinical outcomes, and how real-world combinations of both inducers and inhibitors of CYP3A4 and/or P-gp affect the efficacy of apixaban.
In addition to drugs with pharmacokinetic interactions, many drugs commonly taken by cancer patients can increase the risk of bleeding or thrombosis in apixaban users through pharmacodynamic interactions, by directly influencing the hemostasis. Examples are the increased risk of bleeding seen with non-steroid anti-inflammatory drugs (NSAIDs) or platelet inhibitors, and the increased thrombosis risk associated with antihormonal treatments like tamoxifen (11, 12).
A systematic review of drug-drug interactions with DOACs found that interactions between amiodarone and dabigatran were the most frequently associated with bleeding events (13). Amiodarone, fluconazole, rifampicin, and phenytoin were found to increase the risk of major bleeding when taken in combination with one of the DOACs dabigatran, rivaroxaban, or apixaban (14). Hanigan et al. reported a trend towards increased bleeding risk in patients taking rivaroxaban or apixaban combined P-gp and CYP3A4 inhibitors like amiodarone, dronedarone, diltiazem, and verapamil (15).
In a post-hoc analysis of the Caravaggio study, which compared dalteparin with apixaban in cancer patients with VTE, no association was found between anti-cancer treatment and the risk of recurrent VTE or major bleeding (16). Likewise, drug-drug interactions did now influence recurrent VTE or major bleeding in a cohort of patients treated for cancer (17).
The aim of the current report is to describe how drugs expected to interact with apixaban influenced recurrent VTE and bleedings in cancer patients participating in a multicenter single-arm interventional study of apixaban (CAP study) (18).
A post-hoc analysis was be performed on data collected from the CAP study, which was originally designed to investigate the safety and efficacy of apixaban for treating VTE in cancer patients. The study was carried out from April 2016 until May 2018, and included 298 patients across nine Norwegian hospitals. The inclusion and exclusion criteria for the study have previously been reported (18). In short, the patients were 18 years or older and either had a diagnosis of cancer or were treated for cancers other than basal cell or squamous cell carcinoma of the skin, had an objectively verified VTE, and did not use strong inhibitors or inducers of CYP3A4 or P-gp. Interacting drugs that were not allowed in the study according to the protocol were voriconazole, posaconazole, itraconazole, idelalisib, several drugs against HIV and hepatitis C, phenytoin, carbamazepine, phenobarbital, primidone, enzalutamide, dabrafenib, and rifampicin. Drugs that were considered moderate interactors or with an unknown degree of interaction were allowed. The patients received apixaban 10 mg twice daily the first week, then 5 mg twice daily for 6 months. If there were indication of continued anticoagulation after 6 months, they received apixaban 2.5 mg twice daily. Clinical endpoints and a complete list of medications taken were registered at inclusion, after 3, 6, and 12 months, and then every 12th month for a total of 36 months. Ethics approval was obtained from the Norwegian Regional Committees for Medical and Health Research Ethics and the local data protection officer at each participating hospital. The study was carried out in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice.
Interactions of both pharmacokinetic (mainly through CYP3A4 or P-gp interference) and pharmacodynamic nature were considered, i.e. drugs with a known effect on hemostasis, either as effects or side effects. For the pharmacokinetic interactions, categorization of drugs as either strong, moderate, or weak inducers or inhibitors of CYP enzymes was based on FDA’s 2020 Guidance for Industry on clinical drug interaction studies (19), summarized in Table 1. The guidance used measured differences in area under concentration-time curve (AUC) when an index substrate was combined with an interactor to describe the magnitude of effect.
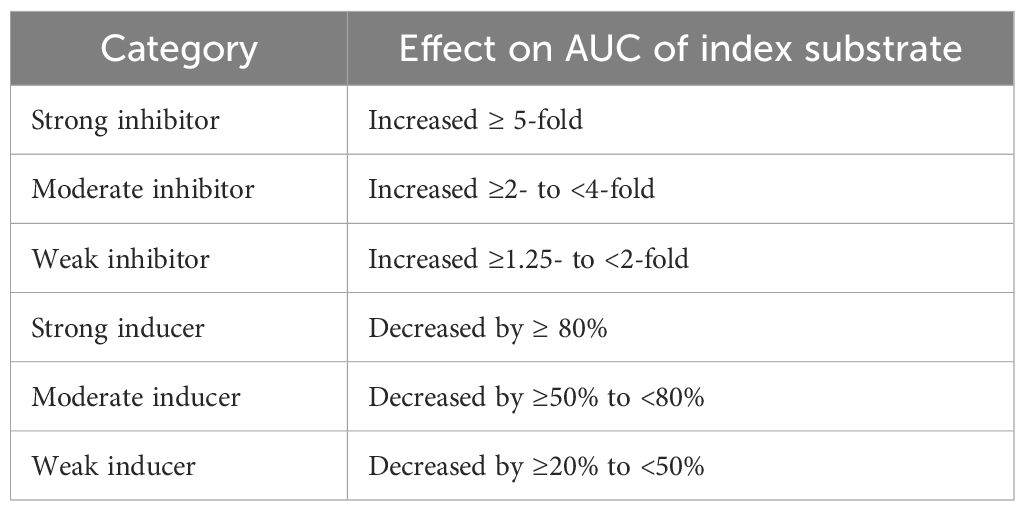
Table 1. Definitions of weak to strong inhibitors and inducers of CYP enzymes, from FDA’s 2020 Guidance for Industry on clinical drug interaction studies (19).
While drugs with strong pharmacokinetic interactions with apixaban were exclusion criteria for the study, the study population could use mild/moderate interactors, as well as some groups of medications that increase the risk of bleeding and/or thrombosis. Lists of potentially interacting drugs were sourced from previous reports on the topic (15, 20), and the appendix of the initial report from the CAP study (18). All patients that had taken at least one dose of an interacting drug during the study were considered users of that drug.
Potentially interacting drugs were categorized as: i) drugs where a higher risk of bleeding was assumed, either because the drugs inhibit the metabolism of apixaban, thus potentially increasing its potency, or because of other features, e.g., platelet inhibition; ii) drugs assumed to have a higher risk of thrombosis, either because of induction of the metabolic paths of apixaban, or because of other features, e.g., cisplatin; iii) drugs with a combination of interactions or effects from both previous groups.
Patients were correspondingly categorized as taking drugs from the first group “expected only increased bleeding risk”, the second group “expected only increased thrombosis risk”, or from the third group “expected both increased bleeding risk and thrombosis risk”. Patients taking drugs from both the first and second group were placed in the third group. Patients not exposed to drugs in either of the three interacting drug groups served as control group. For each group, odds ratio (OR) for each of the outcomes were calculated and compared with the control group.
Three main clinical outcomes were defined in the CAP study for the efficacy and safety assessments of apixaban: recurrent VTE, major bleeding, and clinically relevant non-major bleeding (CRNMB).
Recurrent VTE was defined as objectively verified progression of the thrombosis following start of treatment (18). CRNMB was defined by the recommended criteria by the International Society on Thrombosis and Haemostasis (21). Major bleeding was defined according to the Control of Anticoagulation Subcommittee as fatal bleeding, and/or symptomatic bleeding in a critical area or organ, and/or bleeding causing a fall of hemoglobin level of 2 g/dL or more, or leading to transfusion of two or more units of whole blood or red cells (22).
The number of outcomes were counted for the control group and each group of patients taking the potentially interacting drugs. ORs and 95% confidence intervals (CI) were calculated, comparing the frequencies between the control group and interaction groups. An OR of 1 means no difference between groups of patients, an OR >1 means increased risk for the outcome, while and OR <1 means decreased risk for the outcome. If the 95% CI includes 1 it means that the odds ratio is not statistically significant. Descriptive statistics were used to summarize the baseline characteristics of the study population. We did simple counts of occurrences of categorical variables. Continuous data were expressed as means with standard deviation (SD) or median with range. Among the potentially interacting drugs, those used by five or more study patients were subject to further comparison of outcomes compared to the control group. Potentially interacting drugs used by 1-4 patients were only included in analysis of groups of drugs. IBM SPSS statistics software was used to do the statistical calculations.
The median number of unique drugs taken per patient in addition to apixaban during the trial period was 13 (range 0-58).
A list of the selected individual drugs, the number of patients taking each drug and their expected interactions is detailed in Supplementary Table 1. Four patients were prescribed medications considered exclusion criteria during the study period (enzalutamide and dabrafenib) and were taken out of the study for safety reasons.
The study population and subgroups are summarized in Table 2. Of the 298 enrolled patients, 26 (9%) patients experienced recurrent venous thrombosis, 42 (14%) had one or more CRNMB and 22 (7%) had a major bleeding during the 36-month study period. Upon reviewing the data, 2 patients had one or more CRNMB as well as a major bleeding, 4 patients had one or more CRNMB and a recurrent VTE. These 6 patients were included in both the CRNMB group and the major bleeding or recurrent VTE group, respectively.
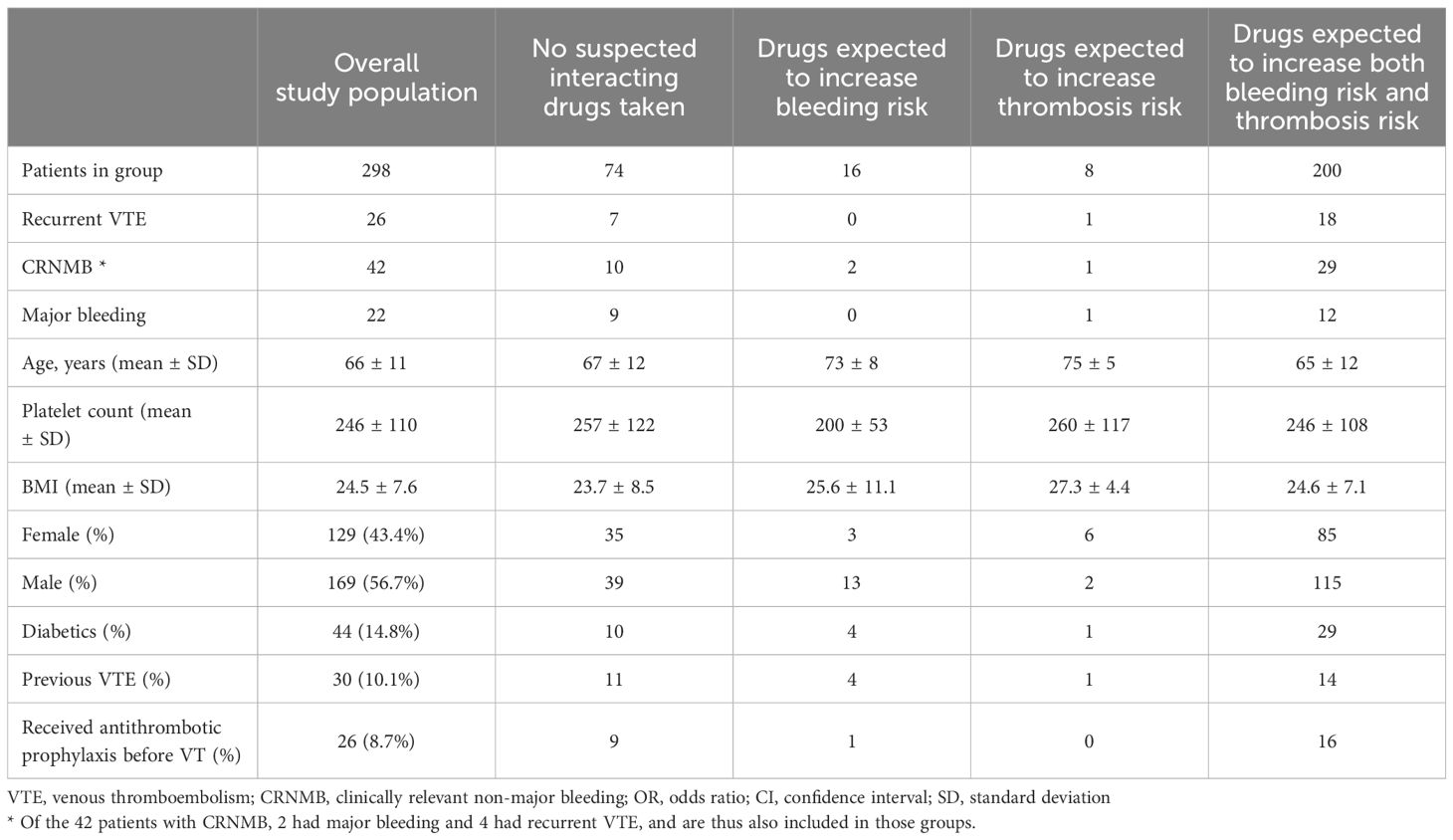
Table 2. Endpoints and baseline characteristics for the different groups of interacting drugs.
Two hundred patients (67%) used drugs expected to reduce the anticoagulant effect of apixaban as well as drugs expected to increase the bleeding risk. Only 8 patients (3%) were exposed only to drugs suspected to reduce the anticoagulant effect of apixaban without any other known interfering drugs, while 16 patients (5%) received only one or more of the drugs with expected bleeding interactions. Finally, 74 patients (25%) did not use any of the suspected interactors.
We did not find any association between categories of interacting drugs and the risk of recurrent VTE or any type of clinically relevant bleeding compared with patients who took no interacting drugs (Table 3).
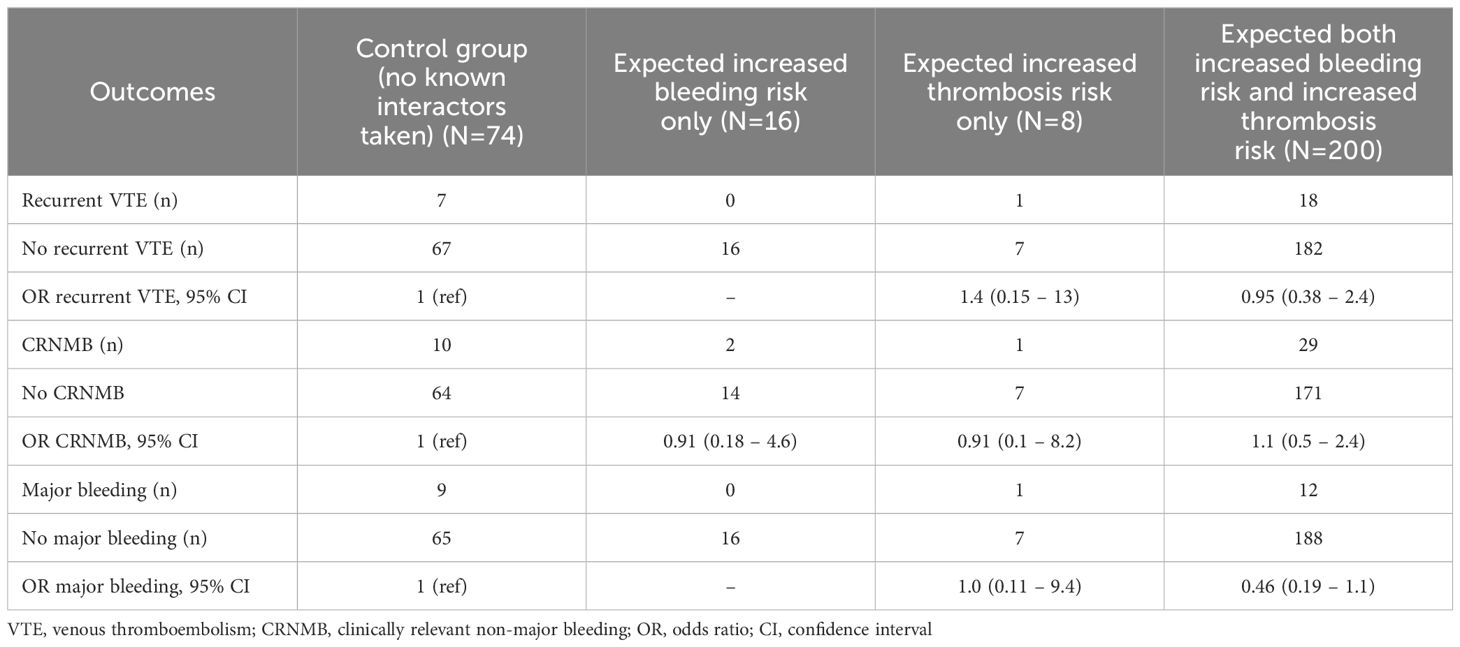
Table 3. Odds ratios for recurrent VTE, CRNMB and major bleeding according to group of interacting drugs.
We found no association between use of any of the suspected drugs and recurrent VTE (Table 4). The highest point estimates of the OR for VTE were seen for aprepitant, gemcitabine, macrolide antibiotics, and NSAIDs, with broad confidence intervals. No OR could be calculated for bevacizumab as none of the 19 patients taking bevacizumab had a recurrent VTE.
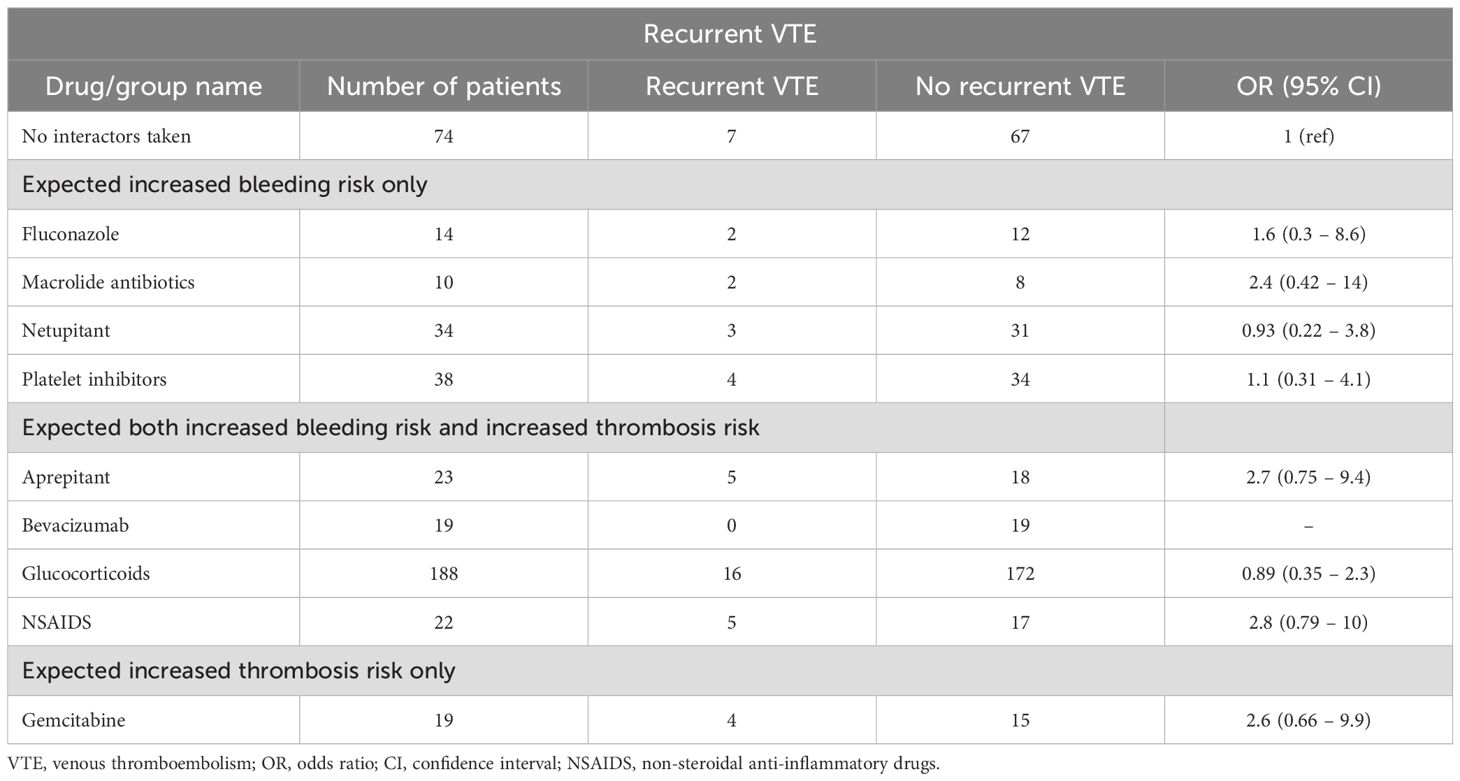
Table 4. Odds ratio for recurrent venous thromboembolism.
Regarding CRNMB (Table 5) and major bleedings (Table 6) we found no association with any drugs, except that the use of fluconazole perhaps was associated with CRNMB. Neither the use of NSAIDs nor antiplatelet therapy were associated with bleeding. No major bleeding was registered for the 10 patients taking macrolides nor for the 23 patients taking aprepitant, thus no OR could be calculated.
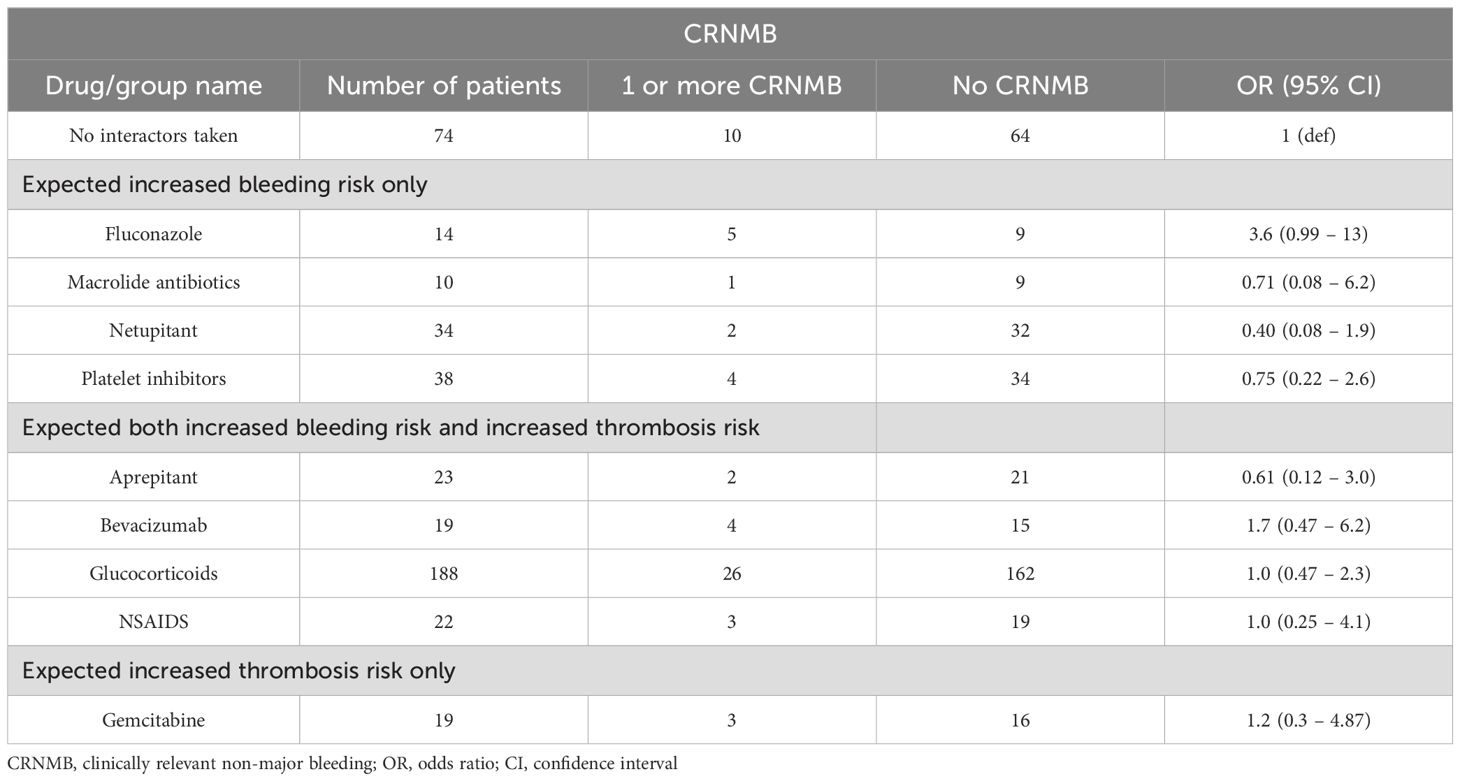
Table 5. Odds ratio for clinically relevant non-major bleeding.
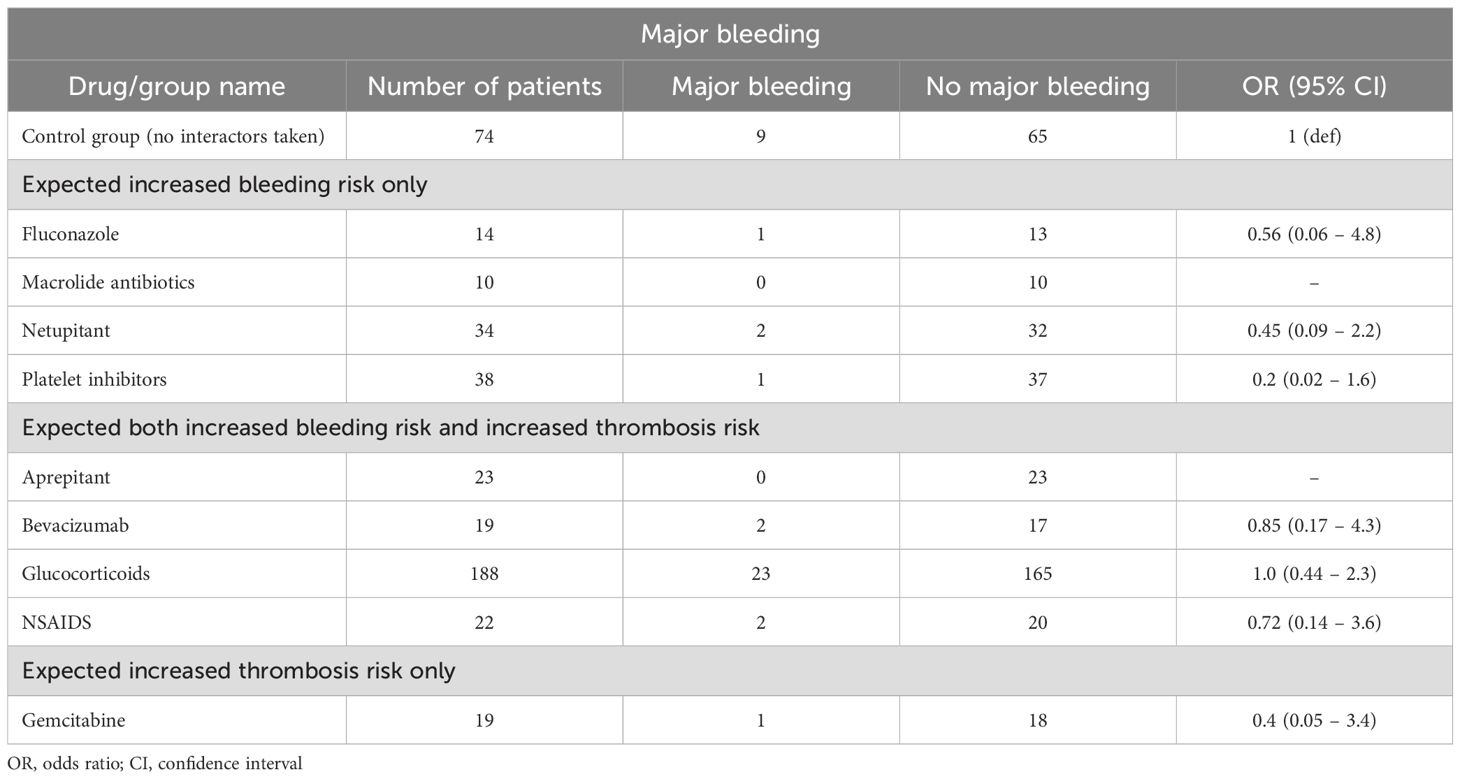
Table 6. Odd ratio for major bleeding.
More than half of the cancer patients treated with apixaban for VTE in the current study used interacting drugs expected to increase the risk of thrombosis as well as bleeding. None of the potentially interacting drugs, or groups of drugs with similar interactions, were associated with recurrent VTE or clinically relevant bleeding. Although fluconazole perhaps increased the risk of CRNMB. Thus, a number of drugs expected to increase the risk of bleeding or thrombosis did not do so in our study. This included NSAIDs, platelet inhibitors, glucocorticoids, and bevacizumab. We found a high level of polypharmacy, with each patient taking a median of 13 different drugs at some time during the 36 month period.
Other studies of interaction with apixaban and other DOACs have focused on specific drugs or families of drugs, and most studies are done in the non-cancer population. In contrast, the current study investigated the clinical effects of interactions with all potentially interacting drugs used by cancer patients. A recent study by Wang et al. (17) looked at drug-drug interactions with DOACs or LMWH in cancer patients using LexiComp® data, grouping patients as either using interacting drugs or not. Like us, they found that many cancer patients used drugs interacting with anticoagulant treatment (42%), but there were no differences in recurrent VTE or bleeding events between patients with or without drug-drug interactions.
A 2013 study by Mueck et al. (23) found a significant increase in AUC and maximum drug concentration in plasma in co-administration of rivaroxaban and CYP3A4/P-gp inhibitors like fluconazole, erythromycin, and clarithromycin (23). In our study, fluconazole seemed to be associated with CRNMB, but not with major bleedings. Interestingly, we see that another study have found the same, apparently contradicting, result between CRNMB and major bleeding (24). We found no convincing effects on clinical outcomes for macrolides. As the number of patients taking macrolides was low, we did not perform analysis on the separate macrolide drugs. Within the group of macrolides, azithromycin is a weak interactor, leading to the possibility that it somewhat masked the interactions of stronger interactors in the macrolide group. A previous study assessed the bleeding risk of older adults taking a DOAC (apixaban, dabigatran or rivaroxaban) and either azithromycin and clarithromycin (25), and found an increased risk of hospital admission because of major bleeding in patients on clarithromycin compared with those taking azithromycin. In our study, none of the 10 patients taking macrolides experienced major bleeding.
There are many previous studies of interaction between DOACs and single drugs, some of those drugs were used by patients in our study. Verapamil and diltiazem have been investigated without finding any interaction with DOACs (15, 26, 27), while our study only had one patient taking each of these drugs, so we were not able to add any new information. The APPRAISE-2 trial found increased bleeding in patients with acute coronary syndromes taking apixaban with aspirin alone or aspirin and clopidogrel compared with placebo (28). The current study had 38 patients taking aspirin and two of those were also taking clopidogrel, but no association with CRNMB or major bleeding was found. A theoretical interaction between aprepitant and DOACs has been described (29), with the potential to cause both increased and decreased effect of anticoagulation, depending on the timing. Our results suggest that, if there is an effect, aprepitant may increase the risk of VTE and reduce the risk of bleeding since no patients taking aprepitant had major bleeding and only two patients had CRNMB, while five patients had recurrent VTE. Bevacizumab has previously been associated with a higher risk of VTE in cancer patients (30), while more recent studies indicate that it can protect against VTE (31). Our results are in line with the latter as none of the 19 patients taking bevacizumab experienced recurrent VTE.
Glucocorticoids are frequently used by cancer patients receiving chemotherapy. They are both associated with increased risk of VTE (32, 33) and with increased gastrointestinal bleeding when taken together with DOAC (34). In our study, 126 of the 298 participants used glucocorticoids. A convincing result was the lack of association with bleeding or recurrent VTE among these patients. The lack of bleeding risk may be related to prophylactic use of proton pump inhibitors.
There are several methodological challenges in investigating clinical effects of drug-drug interactions. One problem is that many drugs are used for short periods of time, e.g., antiemetic drugs, dexamethasone, or antifungal drugs. Thus, the increased risk of an adverse outcome is limited to a few days. We have defined users of interacting drugs as patients who used the interacting drug at any duration of time during the study, not factoring in the time for potential interactions to occur nor the timing in relation to endpoints. A second challenge are the patients who use drugs that can both increase and decrease the efficacy of apixaban and other drugs metabolized through CYP3A4 and P-pg. Thus, the sum of apparently contradicting effects is very difficult to estimate. On the other hand, the data from our study may indicate that polypharmacy could be beneficial, i.e., that the summation of the effects of drugs working opposite on the hemostatic system may reduce the risk of bleeding and recurrent VTE.
The main limitation of the current study is the low number of endpoint events, which resulted in broad CIs of a number of the risk estimates. Thus, there might be drugs increasing the risk of thrombosis or bleeding, where we found no association. Another possible limitation is that there may have been patients in what we have used as the control group, assumed to take no interacting drugs, but still doing so, who we did not consider in our analyses. In addition, we did not have information on intake of food that could possibly interact with apixaban. From the list of potentially interacting drugs, only gemcitabine, dabrafenib, enzalutamide, and tamoxifen were suspected to increase thrombosis risk without any increased bleeding risk. Of the 28 patients taking one or more of these drugs, 20 were also taking one or more drugs that could increase the risk of bleeding, leaving the group of “increased thrombosis risk” with only eight patients. This naturally caused lower confidence in any results from this group, due to the small size.
Apixaban interact with drugs inducing or inhibiting both CYP3A4 and P-gp. It is common among cancer patients to use drugs that potentially interact with apixaban. Despite this concern for drug-drug interaction, drugs with moderate or unknown interacting potential were not found to increase the risk for bleeding or recurrent VTE in cancer patients treated for VTE with apixaban. A possible exception was interaction with fluconazole, which perhaps increases the risk for CRNMB. The results of our study together with the results of previous studies, indicate that drug-drug interactions with drugs of moderate or unknown interacting potential is not a major problem in cancer patients treated with apixaban. We suggest that a possible explanation for this is polypharmacy where drugs with opposite interacting effects on bleeding or thrombosis neutralize each other.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the regional ethical committee of South-East Norway (REC South-East D, Norway). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MS: Data curation, Investigation, Writing – original draft. T-LL: Data curation, Investigation, Supervision, Writing – review & editing. JB: Investigation, Resources, Writing – review & editing. TE: Project administration, Resources, Writing – review & editing. HF: Investigation, Resources, Writing – review & editing. HG: Investigation, Resources, Writing – review & editing. EJ: Investigation, Resources, Writing – review & editing. AP: Investigation, Resources, Writing – review & editing. AR: Investigation, Resources, Writing – review & editing. DT: Writing – review & editing, Investigation, Resources. EV: Investigation, Resources, Writing – review & editing. HW: Project administration, Validation, Writing – review & editing. WG: Investigation, Project administration, Resources, Supervision, Writing – review & editing. PS: Funding acquisition, Project administration, Supervision, Writing – review & editing. AD: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by grants from the Norwegian South-Eastern health authority (Grant number 243861), Akershus University Hospital (Grant number 296910), Pfizer Norway, and the University of Oslo. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
We acknowledge the skills and hard work of the research nurses Christin Johansen, Nina Hviding, Eli Førsund, Torill Våge, Turid Neverdahl Almvik, Margrete Friestad Anne-Karin Eap, Hilde Larhammer, and Elin Sandanger Haugen, as well as study coordinator Line-Theres Carolin.
T-LL: Lecture honoraria from Pfizer and Bristol Myers Squibb. HG: Honorary for organizing meetings from Amgen AB Norway, Bristol Myers Squibb and Pierre Fabre. Honorary for professional support and presentations from Ipsen Norway, Pfizer Norway, AstraZeneca. AP: Lecture honoraria from Bristol Myers Squibb. WG: Fees for participation in Advisory board from Amgen, Novartis, Pfizer, Principia Biopharma Inc- a Sanofi Company, Sanofi, SOBI, Grifols, UCB, Argenx, Cellphire. Lecture honoraria from Amgen, Novartis, Pfizer, Bristol Myers Squibb, SOBI, Grifols, Sanofi and Bayer. Research grants from Bayer, BMS/Pfizer and UCB. AD: Lecture honoraria from Pfizer, Novartis, Bayer, Bristol Myers Squibb. Consultancy honoraria from Pfizer, Bristol Myers Squibb, MSD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1520725/full#supplementary-material
1. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O'Fallon WM, Melton LJ. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Internal Med. (2000) 160:809–15. doi: 10.1001/archinte.160.6.809
2. Blom JW, Doggen CJ, Osanto S, Rosendaal FR. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. Jama. (2005) 293:715–22. doi: 10.1001/jama.293.6.715
3. Raskob GE, van Es N, Segers A, Angchaisuksiri P, Oh D, Boda Z, et al. Edoxaban for venous thromboembolism in patients with cancer: results from a non-inferiority subgroup analysis of the Hokusai-VTE randomised, double-blind, double-dummy trial. Lancet Haematology. (2016) 3:e379–e87. doi: 10.1016/S2352-3026(16)30057-6
4. Young AM, Marshall A, Thirlwall J, Chapman O, Lokare A, Hill C, et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J Clin Oncol. (2018) 36:2017–23. doi: 10.1200/JCO.2018.78.8034
5. McBane RD, Wysokinski WE, Le-Rademacher JG, Zemla T, Ashrani A, Tafur A, et al. Apixaban and dalteparin in active Malignancy-associated venous thromboembolism: The ADAM VTE trial. J Thromb Haemostasis. (2020) 18:411–21. doi: 10.1111/jth.14662
6. Agnelli G, Becattini C, Meyer G, Muñoz A, Huisman MV, Connors JM, et al. Apixaban for the treatment of venous thromboembolism associated with cancer. New Engl J Med. (2020) 382:1599–607. doi: 10.1056/NEJMoa1915103
7. Lyman GH, Carrier M, Ay C, Di Nisio M, Hicks LK, Khorana AA, et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood advances. (2021) 5:927–74. doi: 10.1182/bloodadvances.2020003442
8. Wang L, Zhang D, Raghavan N, Yao M, Ma L, Frost CA, et al. In vitro assessment of metabolic drug-drug interaction potential of apixaban through cytochrome P450 phenotyping, inhibition, and induction studies. Drug Metab Disposition. (2010) 38:448–58. doi: 10.1124/dmd.109.029694
9. Foerster KI, Hermann S, Mikus G, Haefeli WE. Drug–drug interactions with direct oral anticoagulants. Clin Pharmacokinetics. (2020) 59:967–80. doi: 10.1007/s40262-020-00879-x
10. O'Connell C, Escalante CP, Goldhaber SZ, McBane R, Connors JM, Raskob GE. Treatment of cancer-associated venous thromboembolism with low-molecular-weight heparin or direct oral anticoagulants: patient selection, controversies, and caveats. Oncologist. (2021) 26:e8–e16. doi: 10.1002/onco.13584
11. Olsen A-MS, Gislason GH, McGettigan P, Fosbøl E, Sørensen R, Hansen ML, et al. Association of NSAID use with risk of bleeding and cardiovascular events in patients receiving antithrombotic therapy after myocardial infarction. Jama. (2015) 313:805–14. doi: 10.1001/jama.2015.0809
12. Meier CR, Jick H. Tamoxifen and risk of idiopathic venous thromboembolism. Br J Clin Pharmacol. (1998) 45:608–12. doi: 10.1046/j.1365-2125.1998.00733.x
13. Li A, Li MK, Crowther M, Vazquez SR. Drug-drug interactions with direct oral anticoagulants associated with adverse events in the real world: a systematic review. Thromb Res. (2020) 194:240–5. doi: 10.1016/j.thromres.2020.08.016
14. Chang S-H, Chou I-J, Yeh Y-H, Chiou M-J, Wen M-S, Kuo C-T, et al. Association between use of non–vitamin K oral anticoagulants with and without concurrent medications and risk of major bleeding in nonvalvular atrial fibrillation. Jama. (2017) 318:1250–9. doi: 10.1001/jama.2017.13883
15. Hanigan S, Das J, Pogue K, Barnes GD, Dorsch MP. The real world use of combined P-glycoprotein and moderate CYP3A4 inhibitors with rivaroxaban or apixaban increases bleeding. J Thromb Thrombolysis. (2020) 20:1–8. doi: 10.1007/s11239-020-02037-3
16. Verso M, Munoz A, Bauersachs R, Huisman MV, Mandalà M, Vescovo G, et al. Effects of concomitant administration of anticancer agents and apixaban or dalteparin on recurrence and bleeding in patients with cancer-associated venous thromboembolism. Eur J Cancer. (2021) 148:371–81. doi: 10.1016/j.ejca.2021.02.026
17. Wang T-F, Hill M, Mallick R, Chaudry H, Unachukwu U, Delluc A, et al. The prevalence of relevant drug-drug interactions and associated clinical outcomes in patients with cancer-associated thrombosis on concurrent anticoagulation and anticancer or supportive care therapies. Thromb Res. (2023) 231:128–34. doi: 10.1016/j.thromres.2023.10.004
18. Hannevik T-L, Brekke J, Enden T, Frøen H, Garresori H, Jacobsen EM, et al. Thrombosis and bleedings in a cohort of cancer patients treated with apixaban for venous thromboembolism. Thromb Res. (2020) 196:238–44. doi: 10.1016/j.thromres.2020.08.042
19. Food, Administration D. Guidance for industry: clinical drug interaction studies—cytochrome P450 enzyme-and transporter-mediated drug interactions. In: Center for drug evaluation and research. Silver Spring, MD: Office of Communications, Division of Drug Information Center for Drug Evaluation and Research Food and Drug Administration (2020).
20. Fralick M, Juurlink DN, Marras T. Bleeding associated with coadministration of rivaroxaban and clarithromycin. Cmaj. (2016) 188:669–72. doi: 10.1503/cmaj.150580
21. Kaatz S, Ahmad D, Spyropoulos A, Schulman S. Anticoagulation SoCo. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: communication from the SSC of the ISTH. J Thromb Haemostasis. (2015) 13:2119–26. doi: 10.1111/jth.13140
22. Schulman S, Kearon C, SoCoAot S. Thrombosis SCotISo, Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb haemostasis. (2005) 3:692–4. doi: 10.1111/j.1538-7836.2005.01204.x
23. Mueck W, Kubitza D, Becka M. Co-administration of rivaroxaban with drugs that share its elimination pathways: pharmacokinetic effects in healthy subjects. Br J Clin Pharmacol. (2013) 76:455–66. doi: 10.1111/bcp.2013.76.issue-3
24. Cid A, Smetana ME, Hebert C, Coe K, Smith JM. Impact of concomitant fluconazole on direct oral anticoagulant bleeding risk. Pharmacotherapy. (2022) 42:880–9. doi: 10.1002/phar.v42.12
25. Hill K, Sucha E, Rhodes E, Carrier M, Garg AX, Harel Z, et al. Risk of hospitalization with hemorrhage among older adults taking clarithromycin vs azithromycin and direct oral anticoagulants. JAMA Internal Med. (2020) 180:1052–60. doi: 10.1001/jamainternmed.2020.1835
26. Bistervels IM, Bavalia R, Gebel M, Lensing AW, Middeldorp S, Prins MH, et al. Effect of polypharmacy on bleeding with rivaroxaban versus vitamin K antagonist for treatment of venous thromboembolism. J Thromb Haemostasis. (2022) 20:1376–84. doi: 10.1111/jth.15692
27. Pham P, Schmidt S, Lesko L, Lip GY, Brown JD. Association of oral anticoagulants and verapamil or diltiazem with adverse bleeding events in patients with nonvalvular atrial fibrillation and normal kidney function. JAMA network Open. (2020) 3:e203593–e. doi: 10.1001/jamanetworkopen.2020.3593
28. Hess CN, James S, Lopes RD, Wojdyla DM, Neely ML, Liaw D, et al. Apixaban plus mono versus dual antiplatelet therapy in acute coronary syndromes: insights from the APPRAISE-2 trial. J Am Coll Cardiol. (2015) 66:777–87. doi: 10.1016/j.jacc.2015.06.027
29. Dushenkov A, Kalabalik J, Carbone A, Jungsuwadee P. Drug interactions with aprepitant or fosaprepitant: review of literature and implications for clinical practice. J Oncol Pharm Practice. (2017) 23:296–308. doi: 10.1177/1078155216631408
30. Nalluri SR, Chu D, Keresztes R, Zhu X, Wu S. Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: a meta-analysis. Jama. (2008) 300:2277–85. doi: 10.1001/jama.2008.656
31. Ades S, Pulluri B, Holmes CE, Lal I, Kumar S, Littenberg B. Risk factors for venous thromboembolism in metastatic colorectal cancer with contemporary treatment: A SEER-Medicare analysis. Cancer Med. (2022) 11:1817–26. doi: 10.1002/cam4.v11.8
32. Johannesdottir SA, Horváth-Puhó E, Dekkers OM, Cannegieter SC, Jørgensen JOL, Ehrenstein V, et al. Use of glucocorticoids and risk of venous thromboembolism: a nationwide population-based case-control study. JAMA Internal Med. (2013) 173:743–52. doi: 10.1001/jamainternmed.2013.122
33. Orsi FA, Lijfering WM, Geersing GJ, Rosendaal FR, Dekkers OM, le Cessie S, et al. Glucocorticoid use and risk of first and recurrent venous thromboembolism: self-controlled case-series and cohort study. Br J haematology. (2021) 193:1194–202. doi: 10.1111/bjh.v193.6
Keywords: venous thromboembolism, apixaban, cancer, drug-drug interaction, bleeding
Citation: Svalastoga M, Larsen T-L, Brekke J, Enden T, Frøen H, Garresori H, Jacobsen EM, Porojnicu AC, Ree AH, Torfoss D, Velle EO, Wik HS, Ghanima W, Sandset PM and Dahm AEA (2025) Effect of drug interactions with apixaban on clinical outcomes in cancer patients with venous thromboembolism. Front. Oncol. 15:1520725. doi: 10.3389/fonc.2025.1520725
Received: 31 October 2024; Accepted: 02 January 2025;
Published: 27 January 2025.
Edited by:
Jose Luis Ramirez-GarciaLuna, McGill University Health Centre, CanadaReviewed by:
Yoshinori Imamura, University of Fukui Hospital, JapanCopyright © 2025 Svalastoga, Larsen, Brekke, Enden, Frøen, Garresori, Jacobsen, Porojnicu, Ree, Torfoss, Velle, Wik, Ghanima, Sandset and Dahm. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anders Erik Astrup Dahm, YWVhZGFobUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.