 Rubén E. Lasso-Palomino1,2*
Rubén E. Lasso-Palomino1,2* Inés Elvira Gómez3,4María José Soto-Aparicio4
Inés Elvira Gómez3,4María José Soto-Aparicio4 Andrés Gempeler3,4
Andrés Gempeler3,4 Andrés Pombo-Jiménez4Melissa Gómez-Toro3Valentina Rojas-Robledo3
Andrés Pombo-Jiménez4Melissa Gómez-Toro3Valentina Rojas-Robledo3 María Alejandra Jiménez-Arévalo3Karla Alejandra Bastidas-Toro3Jimena Sierra2Sofía Martínez-Betancur4,5Camila Ariza-Insignares2Isabella Montaño-Vivas2Ximena Castro2,6Anita V. Arias7
María Alejandra Jiménez-Arévalo3Karla Alejandra Bastidas-Toro3Jimena Sierra2Sofía Martínez-Betancur4,5Camila Ariza-Insignares2Isabella Montaño-Vivas2Ximena Castro2,6Anita V. Arias7- 1Fundación Valle del Lili, Unidad de Cuidado Intensivo Pediátrico, Unidad Materno Infantil, Cali, Colombia
- 2Universidad Icesi, Facultad de Ciencias de la Salud, Departamento de Pediatría, Cali, Colombia
- 3Universidad Icesi, Facultad de Ciencias de la Salud, Departamento de Salud Pública, Cali, Colombia
- 4Fundación Valle del Lili, Centro de Investigaciones Clínicas (CIC), Cali, Colombia
- 5Universidad Tecnológica de Pereira, Facultad de Ciencias de la Salud, Departamento de Pediatría, Pereira, Colombia
- 6Fundación Valle del Lili, Unidad de Atención de Cáncer Infantil, Unidad Materno Infantil, Cali, Colombia
- 7Division of Critical Care and Pulmonary Medicine, Department of Pediatrics, St Jude Children’s Research Hospital, Memphis, TN, United States
Introduction: Central nervous system (CNS) tumors are the second most prevalent malignant neoplasms in childhood, with surgical resection as the primary therapeutic approach. The immediate postoperative period following CNS tumor resection requires intensive care to mitigate complications associated with high morbidity and mortality.
Objective: The primary aim of this study is to comprehensively describe the postoperative complications observed in pediatric patients who underwent primary CNS tumor resection and were subsequently admitted to the pediatric intensive care unit (PICU) at Hospital Universitario Fundación Valle del Lili in Colombia.
Methods: We conducted a cross-sectional observational analysis of pediatric patients who underwent surgery for CNS tumors and were admitted to our PICU from January 2011 to December 2021. Clinical, histopathologic, and postoperative complication data were collected. A descriptive statistical analysis was performed using measures of dispersion and central tendency with a 95% confidence interval.
Results: A total of 114 patients were included, of whom 55.3% were male. The median PICU stay was 4 days (2–7). The most common tumor type was embryonal (25.4%), followed by low-grade glioma (20.1%) and high-grade glioma (14.9%). Mechanical ventilation was required in 24.5% of patients, with a median extubation time of 3 days (2–9). In the immediate postoperative period, 6.14% of patients experienced CNS hemorrhage and 3.5% experienced intracranial hypertension. Common complications included motor deficits, facial paralysis, and sensory deficits. The mortality rate was 3.5%.
Conclusion: This study describes the postoperative complications, clinical challenges, and interventions observed in pediatric patients after CNS tumor resection in a resource-limited country. Our findings emphasize the importance of tailored interventions and multidisciplinary collaboration to optimize clinical outcomes. Future data comparison from centers sharing similar characteristics will play a crucial role in identifying best practices and enhancing outcomes globally.
1 Introduction
Pediatric central nervous system (CNS) tumors are the most common solid tumors in childhood and the leading cause of cancer-related death, accounting for 15%–20% of deaths among children aged 0 to 14 years globally (1–4). According to the Central Brain Tumor Registry of the United States, the incidence of primary CNS tumors is 6.14 cases per 100,000 children and adolescents (1, 5, 6), with 58% of these cases classified as malignant.
In high-income countries, the 5-year survival for pediatric patients with cancer exceeds 80%, reflecting the impact of early diagnosis and access to specialized healthcare services (7). However, global disparities exist, including in Latin America where the prevalence of childhood cancer is 11%, which is lower than that of Asian and African countries (8). In Colombia, CNS cancer in children is a significant health burden. The reported prevalence is 22.1% and it is the second leading cause of cancer-related death, with 47.4% of cases involving solid tumors (1, 2, 7). Moreover, 7,769 cases of childhood cancer were reported between January 2020 and January 2021, including 876 new cases. In southwestern Colombia, where our institution is geographically located, the prevalence of childhood cancer is 575 (95% CI, 545–606) per 1,000,000 individuals under the age of 18 years (2).
Precise tumor diagnosis and staging play a crucial role in determining treatment and prognosis. The World Health Organization (WHO) classification, with its 2021 update, places a strong emphasis on molecular diagnostics to distinguish tumors affecting adults from those affecting children, as this differentiation may influence treatment strategies and disease progression (9). CNS tumors in children, which originate from the brain, spinal cord, and meninges, are predominantly of primary origin, with gliomas comprising half of these tumors in children and adolescents (10, 11).
Surgical resection is the preferred treatment for CNS tumors in children. In Colombia, surgery has been the main treatment for children with CNS tumors since 2020, with an adoption rate of 98.7%. The surgical approach is tailored to the patient’s clinical condition and imaging findings (3, 12), with a focus on tumor mass reduction, intracranial hypertension management, hydrocephalus relief, or obtaining tumor samples for accurate classification. Postoperative care in a pediatric intensive care unit (PICU) is essential for continuous monitoring and early detection of complications such as infections, seizures, endocrine disturbances, or stroke (12).
Outcome data, including postsurgical data, provide valuable insights into care, risks, and opportunities for improvement in patient care. Despite Colombia’s effort to conduct epidemiological surveillance of pediatric cancer, there is limited information on postoperative outcomes following tumor resection. This study aims to describe the clinical outcomes and most common complications during the postoperative period for pediatric patients admitted to a PICU between 2011 and 2021 in a resource-limited setting that manages complex pediatric cases in southwestern Colombia.
2 Materials and methods
2.1 Study design and population
A descriptive, cross-sectional study with retrospective data collection was conducted. The study included patients aged 1 to 18 years who underwent resection of CNS tumors at our tertiary university hospital between January 2011 and December 2021 and were subsequently admitted to the PICU during the postoperative period. Patients whose surgical resections or diagnoses were conducted outside our institution without histopathologic review performed at our hospital, as well as those who underwent solely diagnostic biopsies, were excluded from the study. Data were extracted from the patients’ medical records and tabulated using a standardized form.
2.2 Setting
Hospital Universitario Fundación Valle del Lili is a general hospital with a significant portion of its services (25% to 30%) dedicated to pediatric patients. It serves as a referral center for high-complexity pathology in the southwestern region of Colombia. The hospital contains a PICU with 40 beds, including 10 designated for pediatric cardiovascular surgery and 30 for general medical-surgical and oncologic conditions. On average, the PICU admits approximately 200 patients per month, with 20% to 30% experiencing critical oncologic conditions. Colombia is classified as a middle-income country according to the Global Burden of Disease Study 2019 Socio-Demographic Index (13), which is an indicator of development status that correlates with health outcomes. Hospitals in this region encounter therapeutic and resource constraints and high patient volumes, resulting in frequent resource limitations.
2.3 Variables
The diagnoses of eligible patients are listed in Appendix 1. Sociodemographic factors such as age, sex, city of residence, and type of health insurance were recorded. Clinical characteristics prior to surgery were also documented, including tumor classification based on the 2016 WHO classification, medical history, and neurologic symptoms. Supplementary Material 1 provides the complete World Health Organization (WHO) classification system used for tumor categorization in this study. Postoperative outcomes including complications such as the need for advanced interventions (e.g., invasive mechanical ventilation or vasopressors) and mortality were also analyzed. The functional status score (FSS) was used to evaluate patients’ functionality upon admission to and discharge from the PICU. Postoperative complications were categorized based on their occurrence within 24 hours (immediate), between 24 and 48 hours (early), between 48 hours and 7 days (intermediate), and beyond 7 days during the PICU stay (late). All patients were examined by pediatric intensivists, neurosurgeons, neurologists, and critical care nurses.
2.4 Statistical analysis
Variables were described based on their nature and distribution. The type of distribution for quantitative variables was determined using the Shapiro-Wilk test. Quantitative variables exhibiting a normal distribution were characterized using the mean and standard deviation, whereas those with non-normal distributions were described using median and interquartile range (IQR). The incidence of complications was calculated by defining the numerator as the number of cases with complications and the denominator as the total number of patients admitted to the PICU with a history of surgical tumor resection during the study period. Qualitative variables were summarized by frequencies and percentages. A 95% confidence interval was calculated. The statistical software STATA SE v18 was used for the analysis.
2.5 Ethical considerations
This study was approved by the Research Ethics Committee of Hospital Universitario Fundación Valle del Lili. Informed consent was not required for this study due to its retrospective nature and the use of electronic medical records. Data confidentiality was maintained throughout the study.
3 Results
This study included 114 patients who were admitted to the PICU immediately after undergoing CNS tumor resection. There were 63 males (55.3%) and 51 females (44.7%), with a median age of 8 years (IQR, 4–12) at the time of the first surgery. The median time from symptom onset to diagnosis was 29.5 days (IQR, 8–121), and the median time from diagnosis to surgery was 2 days (IQR, 1–8).
Before surgery, 21.1% (n=24) of patients experienced intracranial hypertension, with 12.2% (n=14) requiring emergent ventriculostomy prior to tumor resection. Due to cerebral edema pre-surgery, 78.7% (n=89) of patients received treatment with dexamethasone, and 79.8% (n=91) continued corticosteroid therapy for up to 5 days postoperatively. Only 15.7% (n=18) of patients required corticosteroid administration beyond the initial 5 days after surgery.
Regarding surgical outcomes, all patients underwent primary surgery, with 49.1% (n=56) achieving total tumor resection and 28.1% (n=32) undergoing partial resection (less than 90% resection), as documented in the neurosurgeon’s surgical notes. Surgical outcome information was not available in the medical records of 26 patients (22.8%). Tumor localization was primarily infratentorial in 51.7% of cases (n=59). The most prevalent tumor type by histology was embryonal (25.4%, n=29), followed by low-grade glioma (20.1%, n=23). Tumors were graded according to the 2016 WHO CNS Tumor Classification (14) as outlined in Table 1. During surgery, 19.3% (n=22) of patients required blood transfusions. Additionally, 50% (n=57) of patients had ventriculostomy placement, either concurrently with tumor resection or in the early postoperative period.
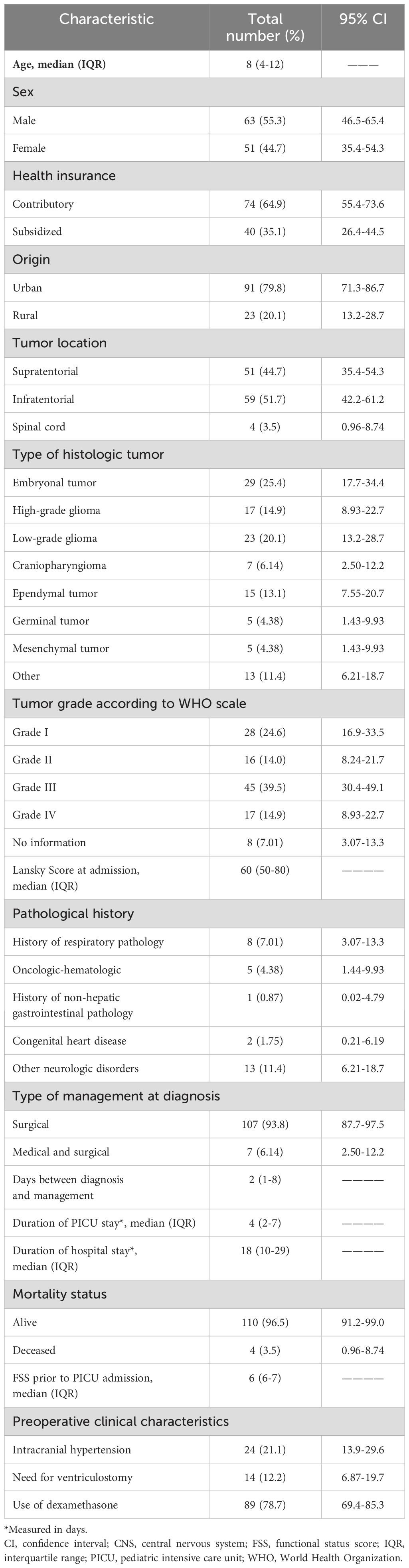
Table 1. Demographics and clinical characteristics of pediatric patients admitted to the PICU following CNS tumor resection (n=114).
After surgery, 33 patients (28.9%) had an uneventful postoperative phase. In some cases, multiple complications occurred in a single patient. Regarding the therapeutic interventions performed during the immediate postoperative phase (<24 hours), 32.5% (n=37) of patients required anticonvulsants, 17.5% (n=20) received antibiotics, 7.89% (n=9) were administered vasopressors, and 6.24% (n=7) received hyperosmolar therapy. Throughout their PICU stay, 24.5% (n=28) of patients required invasive mechanical ventilation (IMV) with a median duration of 3 days (IQR, 2–9). Additional details are shown in Table 2.
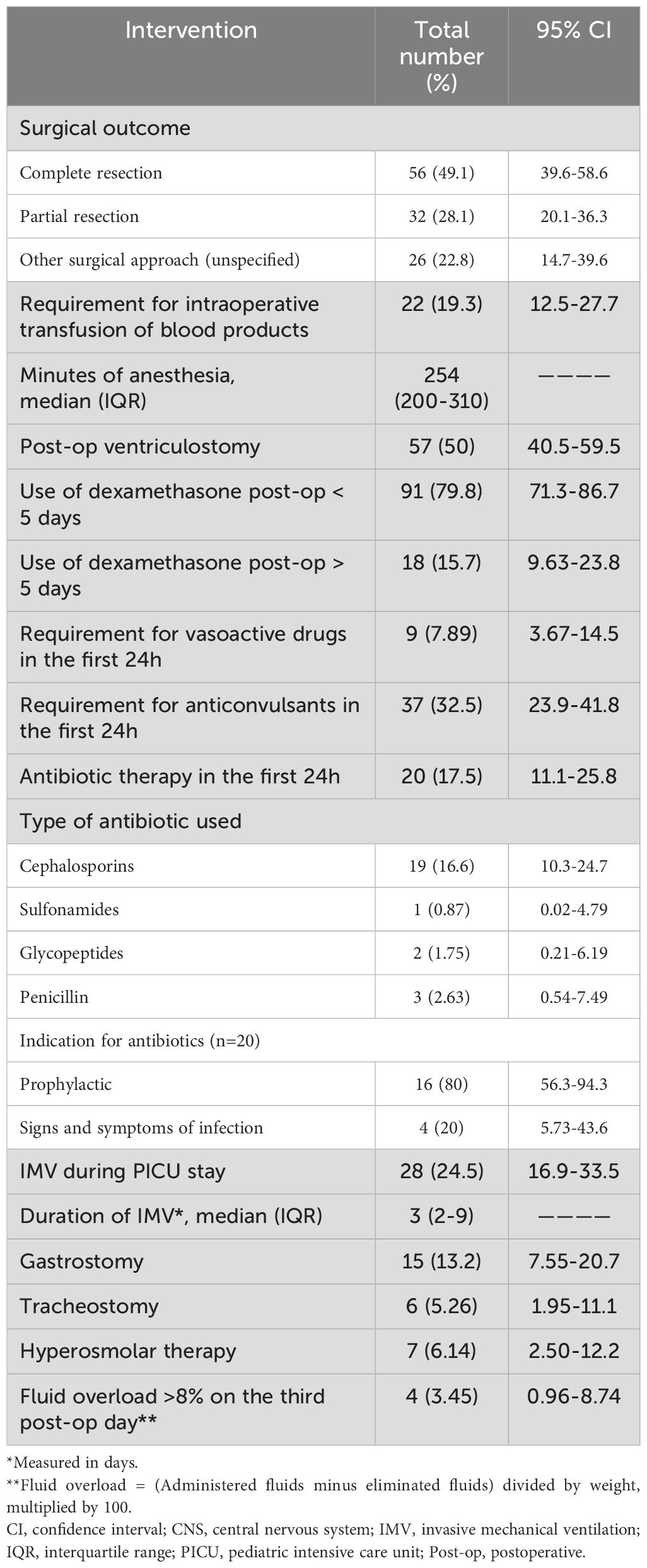
Table 2. Clinical conditions and interventions for pediatric patients admitted to the PICU following CNS tumor resection (n=114).
Table 3 outlines the clinical characteristics and complications during early and late postoperative periods, grouped according to their timing. In the initial 24 hours following surgery, complications included surgical bed hemorrhage (6.14%, n=7), intracranial hypertension (3.50%, n=4), and septic shock (0.87%, n=1). Regarding neurologic status at 24 hours postoperatively, 89 (78%) patients had a Glasgow Coma Scale (GCS) score between 14 and 15, 10 (8.8%) had a score between 9 and 13, and 3 (2.6%) scored below 9. In 12 patients (10.5%), the GCS score was not available due to sedation and IMV at that time. Within the first 48 hours, the most common complications were motor deficits (36.8% of patients, n=42), facial paralysis (12.2%, n=14), and sensory deficits (11.4%, n=13). Diabetes insipidus, cerebellar syndrome, seizures, and hypothalamic insufficiency occurred in fewer patients. Between 2 and 7 days postoperatively, motor deficits persisted in 30.7% of patients (n=35), with notable occurrences of facial paralysis and sensory deficits. CNS infection was reported in 1 patient (0.87%). After 7 days, the incidence of motor deficits decreased to 13.2% (n=15), but sensory deficits, facial paralysis, seizures, and endocrine disorders remained. During this period, 3 patients (2.63%) developed infectious complications.
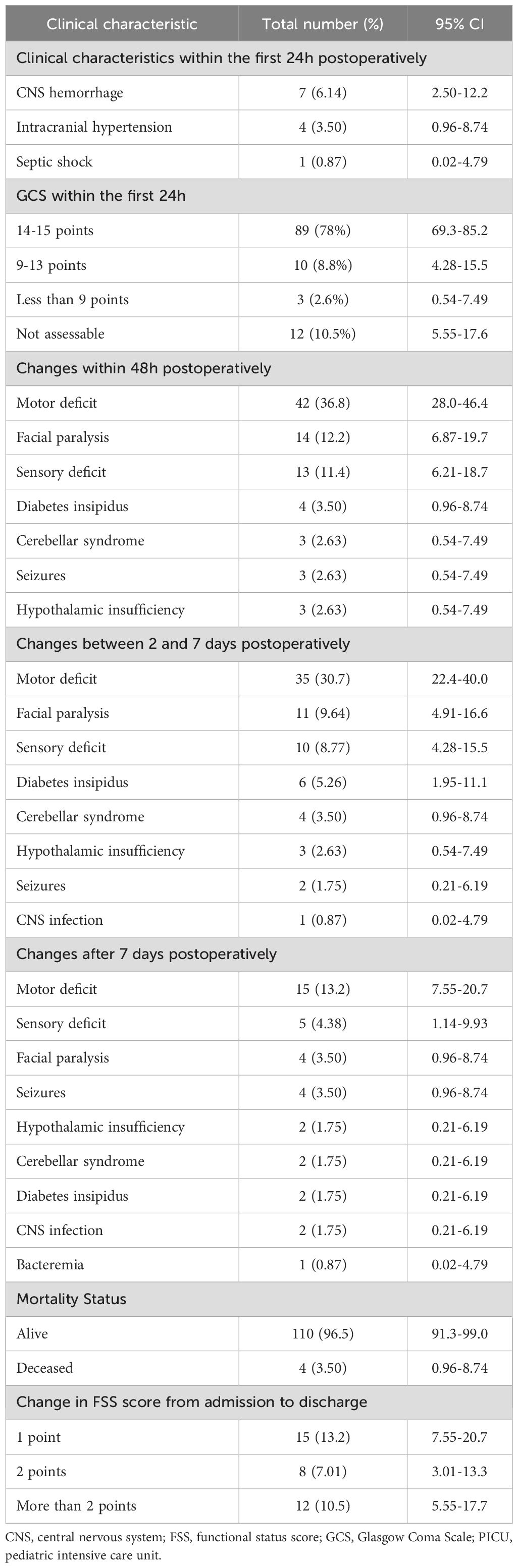
Table 3. Postoperative clinical characteristics of pediatric patients admitted to the PICU following CNS tumor resection (n=114).
During the study period, 3.5% of patients died (n=4) during PICU stay. Although the causes of death were multifactorial, they were primarily related to complications that developed during the postoperative period rather than to the underlying disease. The majority of these deaths were due to CNS infections, sepsis, respiratory failure, and brain death. The FSS changed in some patients between admission and discharge, with 13.2% (n=15) of patients exhibiting a 1-point increase, 7.01% (n=8) showing a 2-point increase, and 10.5% (n=12) experiencing an increase of more than 2 points. Additionally, 5.26% (n=6) required tracheostomy and 13.2% (n=15) required gastrostomy during the PICU stay due to functional impairment and residual morbidity resulting from the primary disease and/or the surgical intervention. Patients received adjuvant chemotherapy and/or radiotherapy as part of their oncologic treatment after discharge from the PICU, but data on these additional treatments were not collected.
4 Discussion
Postoperative complications in children after CNS tumor resection are critical and require intensive monitoring and continuous follow-up as many factors contribute to recovery and prognosis, including the patient’s preoperative condition and the type of surgery (15, 16). To date, limited data are available on the postsurgical outcomes following CNS tumor resections in Colombia. Our study reports the surgical morbidity and mortality of pediatric patients treated in a PICU of a tertiary referral center in Cali, Colombia.
The distribution of age and sex of our patients aligned with previous research conducted by Ramírez et al. and with the VIGICANCER report published in 2024 for this patient population in Colombia (17), as well as with data from other countries (1, 2, 5, 6, 11). Similarly, the anatomical location and WHO histopathologic classification were consistent with previous reports indicating that among gliomas, astrocytomas, medulloblastomas, and ependymomas are the most prevalent histologic subtypes (6, 9–11). The median PICU stay was 4 days (IQR, 2–7), which was comparable to that of other conditions managed in the PICU and did not involve prolonged stays (18, 19).
Immediate postoperative complications included surgical site hemorrhage (6.14%), intracranial hypertension (3.5%), and septic shock (0.87%). Hemodynamic complications were infrequent, with 7.89% of patients requiring vasopressor support and 6.14% receiving hyperosmolar therapy. Notably, no patients required reoperation, indicating effective clinical management and monitoring by a multidisciplinary team of pediatric intensivists, neurosurgeons, anesthesiologists, and nurses specialized in the care of critically ill children.
Neurologic assessment at 24 hours postoperatively revealed that 78% of patients were alert and oriented (GCS >14). Only a small proportion of patients (13%) had a GCS score below 9 at 24 hours, likely due to orotracheal intubation and sedation in the early postoperative period. Despite an average anesthesia duration of 4 hours, 24.5% of patients required IMV with a median duration of 3 days, which is considered a relatively short period of ventilatory support. This need was likely due to the complexity of the procedure rather than to pulmonary complications. Of these patients, 5.2% required tracheostomy placement prior to their PICU discharge.
In our study, we found that neurologic and endocrinologic complications were the most prominent complications, consistent with the existing literature (20). Specifically, motor deficits affected 36.8% of patients within 48 hours postoperatively, followed by facial paralysis (12.2%), sensory deficits (11.4%), and cerebellar syndrome (2.63%). These findings resemble those reported by Zhang et al., who documented a motor deficit prevalence of 56.8% in pediatric patients admitted to the PICU following tumor resection (21). A small proportion of our patients experienced seizures following surgery: 2.63% within the first 48 hours and 3.5% in the late postoperative period. These findings are also consistent with the existing literature, in which the reported prevalence ranges from 1.1% to 10.5% and often correlates with substantial bleeding or electrolyte imbalances, resulting in prolonged ICU stays (20, 22–24). The prophylactic use of anticonvulsants likely contributed to the reduced frequency of this complication in our pediatric cohort.
Endocrine disorders included diabetes insipidus in 5.26% of patients and hypothalamic insufficiency in 2.63% of patients within 48 hours post-surgery. The lower prevalence of these endocrine disorders in our study compared to the reported 37.1% in other studies (25) could be attributed to the limited evaluation period during the PICU stay, which may have excluded delayed-onset conditions. Other studies have linked endocrine disorders with prolonged PICU stay and increased risk of neurologic morbidity (16, 22, 26).
Postoperative infections were relatively rare in our study. One patient developed a CNS infection (0.87%) on the fifth day post-surgery, while 2 patients experienced CNS infection (1.75%) and 1 had bacteremia (0.87%) with pneumonia and surgical site infection in the late postoperative period (>7 days). These findings are consistent with publications reporting a 2.5% prevalence of CNS infection in neurosurgical patients (15, 24). Despite only 17.5% of our patients receiving immediate postoperative antibiotics, 20% displayed clear signs of infection. Although guidelines caution against postoperative antibiotic use as they do not decrease the frequency of infections (27), our findings support the use of prophylactic antibiotics to reduce the risk of surgical site infections and meningitis associated with ventriculostomy, emergent craniotomies, and early reinterventions in specific contexts (16, 22, 28).
Based on the FSS as a measurement of long-term sequelae, 10.5% of patients had residual functional morbidity after discharge, defined as more than a 2-point difference between PICU admission and discharge scores (29). Additionally, 5.26% of patients required tracheostomy and 13.2% required gastrostomy before discharge. These advanced interventions were conducted in adherence to clinical practice guidelines and adapted to each patient’s specific clinical complexity (30). Despite the low overall long-term morbidity, we must not underestimate the impact of morbidity on the quality of life and survival of pediatric patients. This is supported by findings from previous studies and further evidenced by the need for gastrostomy and tracheostomy due to severe neurologic impairment in this specific patient population (31). Therefore, proactive consideration of early tracheostomy and gastrostomy placement is crucial to facilitate timely rehabilitation and improve overall outcomes.
The mortality rate for our patient cohort was 3.5% and was attributed to various causes, including CNS infections, sepsis, ventilatory failure, and brain death, consistent with expected complications in this vulnerable population. Mortality in high-income countries has shown a decreasing trend over recent decades due to advancements in therapeutic technologies within ICUs (24, 32, 33). However, in low- and middle-income countries like Colombia, mortality remains relatively unchanged (34). Furthermore, the observed mortality in our study was higher than that from other international studies but consistent with data from countries with similar epidemiologic profiles, highlighting challenges related to healthcare access and economic constraints faced by our population.
4.1 Study limitations
A primary limitation of this study is its cross-sectional design involving analysis at a single time point, which limits our ability to establish causality between the studied variables. To mitigate potential information biases, rigorous quality controls were enforced during data collection and analysis. Although the sample size was adequate for this study’s objectives, future research could benefit from larger sample sizes to enhance the generalizability of the findings. These limitations emphasize the need for additional studies that can provide further insights and relevance to comparable clinical settings, especially in hospitals with resource limitations.
4.2 Conclusions
This study highlights the most common postoperative complications observed in pediatric patients after resection of CNS tumors and admission to the PICU. Although relatively rare, CNS hemorrhage was an immediate complication within the initial 24 hours, whereas motor deficits were the most common complications after 48 hours. Long-term sequelae included residual morbidity in 10.5% of patients and a mortality rate of 3.5%. These findings underscore the critical importance of vigilant monitoring of pediatric patients with CNS tumors post-resection. Early detection and prompt interventions are essential in mitigating residual morbidity and mortality risks. Furthermore, these data will facilitate future comparison across institutions to improve local and global outcomes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Teresa Gómez-Rodríguez, Comité de Ética en Investigación Biomédica, Fundación Valle del Lili, Cali, Colombia. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
RL: Conceptualization, Investigation, Project administration, Supervision, Interpretation of results, Writing – original draft, Writing – review & editing. IG: Conceptualization, Methodology, Formal analysis, Interpretation of results, Writing – original draft, Writing – review & editing. MS: Investigation, Data collection, Writing – original draft, Writing – review & editing. AG: Conceptualization, Methodology, Formal analysis, Interpretation of results, Writing – review & editing. AP: Investigation, Data collection, Writing – original draft, Writing – review & editing. MG: Conceptualization, Investigation, Data collection, Interpretation of results, Writing – original draft, Writing – review & editing. VR: Conceptualization, Investigation, Data collection, Interpretation of results, Writing – original draft, Writing – review & editing. MJ: Investigation, Data collection, Writing – original draft, Writing – review & editing. KB: Investigation, Data collection, Writing – original draft, Writing – review & editing. JS: Conceptualization, Data collection, Investigation, Writing – review & editing. SM: Conceptualization, Data collection, Investigation, Writing – review & editing. CA: Investigation, Data collection, Writing & original draft, Writing – review & editing, Data curation. IM: Investigation, Data collection, Writing – original draft, Writing – review & editing. XC: Conceptualization, Interpretation of results, Investigation, Writing – review & editing. AA: Interpretation of results, Investigation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded by the Division of Critical Care and Pulmonary Medicine, Department of Pediatrics, St. Jude Children’s Research Hospital.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1491943/full#supplementary-material
References
2. Costo C deA. Situación del cáncer en la población pediátrica atendida en el SGSSS de Colombia 2020. In: CUENTA DE ALTO COSTO Fondo Colombiano de Enfermedades de Alto Costo, Bogota D. C. (2021).
3. Hanson DR, Atlas MP. Central nervous system Malignancies. Lanzkowskys Man Pediatr Hematol Oncol. (2016), 453–72. doi: 10.1016/B978-0-12-801368-7.00023-5
4. Alegría-Loyola MA, Galnares-Olalde JA, Mercado M. Artículos de revisión Tumores del sistema nervioso central. Rev Med Inst Mex Seguro Soc. (2017) 55:330–70.
5. Ostrom QT, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2014-2018. Neuro-Oncol. (2021) 23:III1–105. doi: 10.1093/neuonc/noab200
6. Nieves-Cuervo GM, Manrique-Hernández EF, Ojeda-Rincón SA, Galvis-Pabón S. Tumores del sistema nervioso central en población pediátrica entre 0 y 14 años. UNAB. (2016) 19(2):124–33. doi: 10.29375/01237047.2191
7. Ortega FV, García AA, Pérez TM. Tumores cerebrales en niños. Pediatría Integral. (2016) 10:401–11.
8. Laso EL, González MEM. Tumores cerebrales infantiles, semiología neurológica y diagnóstico. Asocación Esp Pediatría. (2022), 151–8.
9. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro-Oncol. (2021) 23:1231–51. doi: 10.1093/neuonc/noab106
10. Toro-Moreno AC, Serna-Velez L, Gallego-González D, Jaramillo-Jaramillo LI, Martínez-Sánchez LM, Álvarez-Hernández LF. Central nervous system tumors in pediatrics: Present and future of diagnostic approach, Tumores de sistema nervioso central en pediatría: Presente y futuro del abordaje diagnóstico. Revista Ecuatoriana de Neurologia. (2017) 26.
11. Gómez FV, Ortega EC, Atienza ÁL. Tumores cerebrales en niños. Pediatría Integral. (2021) 15:357–66.
12. Linabery AM, Ross JA. Trends in childhood cancer incidence in the U.S. (1992-2004). Cancer. (2008) 112:416–32. doi: 10.1002/cncr.v112:2
13. Global burden of Disease Study 2019 (GBD 2019) Socio-Demographic Index (SDI) 1950–2019. United States: GHDx. (2024). Available at: https://ghdx.healthdata.org/record/ihme-data/gbd-2019-socio-demographic-index-sdi-1950-2019.
14. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 world health organization classification of tumors of the central nervous system: a summary. Acta Neuropathologica. (2016) 131:803–20. doi: 10.1007/s00401-016-1545-1
15. Wach J, Banat M, Borger V, Vatter H, Haberl H, Sarikaya-Seiwert S. Intraoperative MRI-guided resection in pediatric brain tumor surgery: A meta-analysis of extent of resection and safety outcomes. J Neurological Surgery Part A: Cent Eur Neurosurg. (2021) 82:64–74. doi: 10.1055/s-0040-1714413
16. Fernández de Sevilla Estrach M, Lasaosa FJC, Matute SS, Quesada AG, Rico AP. Postoperatorio de tumores cerebrales en la unidad de cuidados intensivos pediátricos. Pediatr marzo. (2009) 70:282–6. doi: 10.1016/j.anpedi.2008.10.015
17. Ramirez O, Piedrahita V, Ardila J, Pardo C, Cabrera-Bernal E, Lopera J, et al. Primary central nervous system tumors survival in children in ten Colombian cities: a VIGICANCER report. Front Oncol. (2024) 13. doi: 10.3389/fonc.2023.1326788
18. Kirk AHP, Sng QW, Zhang LQ, Wong JJM, Puthucheary J, Lee JH. Characteristics and outcomes of long-stay patients in the pediatric intensive care unit. J Pediatr Intensive Care. (2018) 7(1):1–6. doi: 10.1055/s-0037-1601337
19. Shrestha AK, Bhattarai S, Paudel P, Basel PL. Paediatric intensive care unit of tertiary level hospital of Nepal. J Nepal Paediatr Soc. (2020) 40(1):28–33. doi: 10.3126/jnps.v40i1.28853
20. Sangtongjaraskul S, Lerdsirisopon S, Sae-Phua V, Kanta S, Kongkiattikul L. Factors influencing prolonged intensive care unit length of stay after craniotomy for intracranial tumor in children: A 10-year analysis from A university hospital. Indian J Crit Care Med. (2023) 27:205–11. doi: 10.5005/jp-journals-10071-24418
21. Zhang Z, Wu Y, Zhao X, Ji W, Li L, Zhai X, et al. Neurosurgical short-term outcomes for pediatric medulloblastoma patients and molecular correlations: a 10-year single-center observation cohort study. Neurosurg Rev. (2024) 47:283. doi: 10.1007/s10143-024-02526-6
22. Mishra N, Rath GP, Rajagopalan V, Doddamani R, Chaturvedi A. Perioperative management of pediatric brain tumors: A retrospective analysis. Neurol India. (2022) 70:1095–101. doi: 10.4103/0028-3886.349578
23. Spentzas T, Escue JE, Patters AB, Varelas PN. Brain tumor resection in children: Neurointensive care unit course and resource utilization. Pediatr Crit Care Med. (2010) 11:718–22. doi: 10.1097/PCC.0b013e3181d907fa
24. Lassen B, Helseth E, Egge A, Due-Tønnessen BJ, Rønning P, Meling TR. Surgical mortality and selected complications in 273 consecutive craniotomies for intracranial tumors in pediatric patients. Neurosurgery. abril. (2012) 70:936–43. doi: 10.1227/NEU.0b013e31823bcc61
25. Heo J, Lee HS, Hwang JS, Noh OK, Kim L, Park JE. Prevalence of endocrine disorders in childhood brain tumor survivors in South Korea. In Vivo. (2019) 33:2287–91. doi: 10.21873/invivo.11735
26. Manzanares W, Aramendi I, Langlois PL, Biestro A. Hiponatremias en el paciente neurocrítico: Enfoque terapéutico basado en la evidencia actual. Medicina Intensiva. (2015) 39:234–43. doi: 10.1016/j.medin.2014.11.004
27. de Jonge SW, Boldingh QJJ, Solomkin JS, Dellinger EP, Egger M, Salanti G, et al. Effect of postoperative continuation of antibiotic prophylaxis on the incidence of surgical site infection: a systematic review and meta-analysis. Lancet Infect Dis. (2020) 20:1182–92. doi: 10.1016/S1473-3099(20)30084-0
28. Korinek AM, Baugnon T, Golmard JL, Effenterre RV, Coriat P, Puybasset L. Risk factors for adult nosocomial meningitis after craniotomy: Role of antibiotic prophylaxis. Neurosurgery. (2006) 59:126–32. doi: 10.1227/01.neu.0000243291.61566.21
29. Pollack MM, Holubkov R, Glass P, Dean JM, Meert KL, Zimmerman J, et al. The functional status score (FSS): A new pediatric outcome measure. Pediatrics. (2009) 124:e18. doi: 10.1542/peds.2008-1987
30. Ramos-Clason EC, Tuñón-Pitalua MC, Rivas-Muñoz FA, Veloza-Cabrera LA. Tumores primarios del sistema nervioso central en Cartagena, 2001– 2006. Rev salud pública [Internet]. (2010) 12:257–6.
31. Masoudi MS, Taheri R, Zoghi S. Predictive factors for postoperative tracheostomy requirement in children undergoing surgical resection of medulloblastoma. World Neurosurg. (2021) 150:e746–9. doi: 10.1016/j.wneu.2021.03.129
32. Chalif EJ, Morshed RA, Oh T, Ore CD, Aghi MK, Gupta N. Neurosurgical outcomes for pediatric central nervous system tumors in the United States. Neurosurgery. (2024) 92:407–20. doi: 10.1227/neu.0000000000002215
33. Smith ER, Butler WE, Barker FG, Pollack IF, Sutton LN, Ellenbogen RG, et al. Craniotomy for resection of pediatric brain tumors in the United States, 1988 to 2000: effects of provider caseloads and progressive centralization and specialization of care. Neurosurgery. (2004) 54:553–65. doi: 10.1227/01.NEU.0000108421.69822.67
34. Riaño I, Bravo P, Bravo LE, García LS, Collazsos P, Carrascal E. Incidence, mortality, and survival trends of primary CNS tumors in cali, Colombia, from 1962 to 2019. JCO Glob Oncol. (2020) 6:1712–20. doi: 10.1200/GO.20.00368
Appendix 1. Tumor diagnoses
ICD-10 Codes:
● C700 Malignant neoplasm of cerebral meninges.
● C701 Malignant neoplasm of spinal meninges.
● C709 Malignant neoplasm of meninges, unspecified.
● C710 Malignant neoplasm of cerebrum, except lobes and ventricles.
● C711 Malignant neoplasm of frontal lobe.
● C712 Malignant neoplasm of temporal lobe.
● C713 Malignant neoplasm of parietal lobe.
● C714 Malignant neoplasm of occipital lobe.
● C715 Malignant neoplasm of cerebral ventricle.
● C716 Malignant neoplasm of cerebellum.
● C717 Malignant neoplasm of brainstem.
● C718 Malignant neoplasm of overlapping sites of brain.
● C719 Malignant neoplasm of brain, unspecified part.
● C720 Malignant neoplasm of spinal cord.
● C721 Malignant neoplasm of cauda equina.
● C722 Malignant neoplasm of olfactory nerve.
● C723 Malignant neoplasm of unspecified optic nerve.
● C724 Malignant neoplasm of unspecified acoustic nerve.
● C725 Malignant neoplasm of other and unspecified cranial nerves.
● C728 Lesion of contiguous sites of the brain and other parts of the central nervous system.
● C729 Malignant neoplasm of the central nervous system, unspecified.
● D320 Benign neoplasm of cerebral meninges.
● D321 Benign neoplasm of spinal meninges.
● D329 Benign neoplasm of meninges, unspecified.
● D330 Benign neoplasm of brain, supratentorial.
● D331 Benign neoplasm of brain, infratentorial.
● D332 Benign neoplasm of brain, unspecified.
● D333 Benign neoplasm of cranial nerves.
● D334 Benign neoplasm of spinal cord.
● D337 Benign neoplasm of other specified parts of the central nervous system.
● D339 Benign neoplasm of central nervous system, unspecified.
Keywords: pediatric, cancer, central nervous system neoplasms, tumor, pediatric intensive care unit, postoperative complications, resource-limited settings
Citation: Lasso-Palomino RE, Gómez IE, Soto-Aparicio MJ, Gempeler A, Pombo-Jiménez A, Gómez-Toro M, Rojas-Robledo V, Jiménez-Arévalo MA, Bastidas-Toro KA, Sierra J, Martínez-Betancur S, Ariza-Insignares C, Montaño-Vivas I, Castro X and Arias AV (2024) Postoperative complications after central nervous system tumor resection in pediatric patients admitted to an intensive care unit in Colombia. Front. Oncol. 14:1491943. doi: 10.3389/fonc.2024.1491943
Received: 05 September 2024; Accepted: 22 October 2024;
Published: 06 December 2024.
Edited by:
Christian Dohna-Schwake, Essen University Hospital, GermanyReviewed by:
Andrea Carai, Bambino Gesù Children’s Hospital (IRCCS), ItalyMichael Schwake, University Hospital Münster, Germany
Copyright © 2024 Lasso-Palomino, Gómez, Soto-Aparicio, Gempeler, Pombo-Jiménez, Gómez-Toro, Rojas-Robledo, Jiménez-Arévalo, Bastidas-Toro, Sierra, Martínez-Betancur, Ariza-Insignares, Montaño-Vivas, Castro and Arias. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rubén E. Lasso-Palomino, cnViZW4ubGFzc29AZnZsLm9yZy5jbw==