 Karim Amrane1,2*
Karim Amrane1,2* Coline Le Meur3
Coline Le Meur3 Pierre Alemany4Clémence Niel1David Renault1Inès Peillon1Valentin Tissot5
Pierre Alemany4Clémence Niel1David Renault1Inès Peillon1Valentin Tissot5 Ronan Abgral6,7
Ronan Abgral6,7- 1Department of Oncology, Regional Hospital of Morlaix, Morlaix, France
- 2Inserm, UMR1227, Lymphocytes B et Autoimmunité, Univ Brest, Inserm, LabEx IGO, Brest, France
- 3Department of Radiotherapy, University Hospital of Brest, Brest, France
- 4Department of Pathology, Ouest-Pathologie, Brest, France
- 5Department of Radiology, University Hospital of Brest, Brest, France
- 6Department of Nuclear Medicine, University Hospital of Brest, Brest, France
- 7UMR Inserm 1304 groupe d'étude de la thrombose de bretagne occidentale (GETBO), Instituts Fédératifs de Recherche (IFR) 148, University of Western Brittany, Brest, France
We report increased 18F-FDG uptake in the right posterior mediastinal region in a 70-year-old woman following the discovery of a mass in the aftermath of a bronchitis episode. We also report increased 18F-Choline uptake in the right posterior mediastinal region in a 66-year-old man with newly discovered prostate cancer, which may indicate the presence of mediastinal metastases. Both patients had a thoracic MRI showing an intense gadolinium enhancement in the same region, consistent with thoracic schwannomas, which were subsequently proven histologically. This case highlights that schwannoma is a diagnostic pitfall in both 18F-FDG and 18F-Choline PET/CT.
Introduction
A schwannoma is a generally benign soft tissue tumor that arises from Schwann cell myelin in the peripheral nervous system. It can be difficult to distinguish from malignant soft tissue tumours. The number of malignant peripheral nerve sheath tumors is relatively small, and the incidence rate is 3-10% of soft tissue sarcomas (1). Thoracic schwannomas are usually located in the posterior mediastinum (2, 3) and are often large in size (4), but rarely intrapulmonary (5, 6). On imaging, schwannomas appear in the path of a nerve, are well limited, often oval and single. MRI shows low to intermediate signal intensity on T1-weighted images, high signal intensity on T2-weighted images and intense enhancement of solid components on gadolinium-enhanced imaging. Regions of very high T2-weighted signal intensity correspond to cystic degeneration and may show only peripheral enhancement or no enhancement associated with very high signal intensity. Overall, the larger the schwannoma, the more heterogeneous it appears on all sequences (including gadolinium-enhanced images) due to cystic degeneration, hemorrhage or both (3). The metabolic characteristics of schwannomas on 18F-FDG PET-CT are not well described in the literature to differentiate benign or malignant forms. There is no association between SUV and benign or malignant schwannomas (7, 8) moreover lesions with heterogeneous FDG activity had higher SUVmax and more frequent internal non-enhancement on MRI (9). Radiolabeled choline is becoming a promising tracer in the diagnosis of glial tumors due to its low distribution rate in normal white and gray matter, leading to a high background signal-to-noise ratio compared with 18F-FDG PET/CT (10). Thus, patients with suspected recurrent glial tumors have been shown to have a more clearly defined abnormal accumulation on 18F-Choline PET/CT (11).
Case description
We first present a 70-year-old woman with no significant past medical history other than 15 pack-years of smoking. Following severe bronchitis, a right paravertebral mass measuring 62 x 49 mm was seen on chest radiography. This corresponded to a hypermetabolic lesion (SUVmax 6.7) on 18F-FDG PET, without locoregional extension. Figures 1A–C.

Figure 1. FDG PET/CT (A, B, C) MRI (D, E, F) and (G) (schwanomma histology).
We then present the case of a 66-year-old man with a particular history of Gleason 8 prostatic adenocarcinoma. 18F-Choline PET/CT for disease extension revealed a right posterobasal lung mass almost 5 cm long with moderate uptake (SUVmax 6.4) at the posterior pleural contact. Figures 2A’-C’.
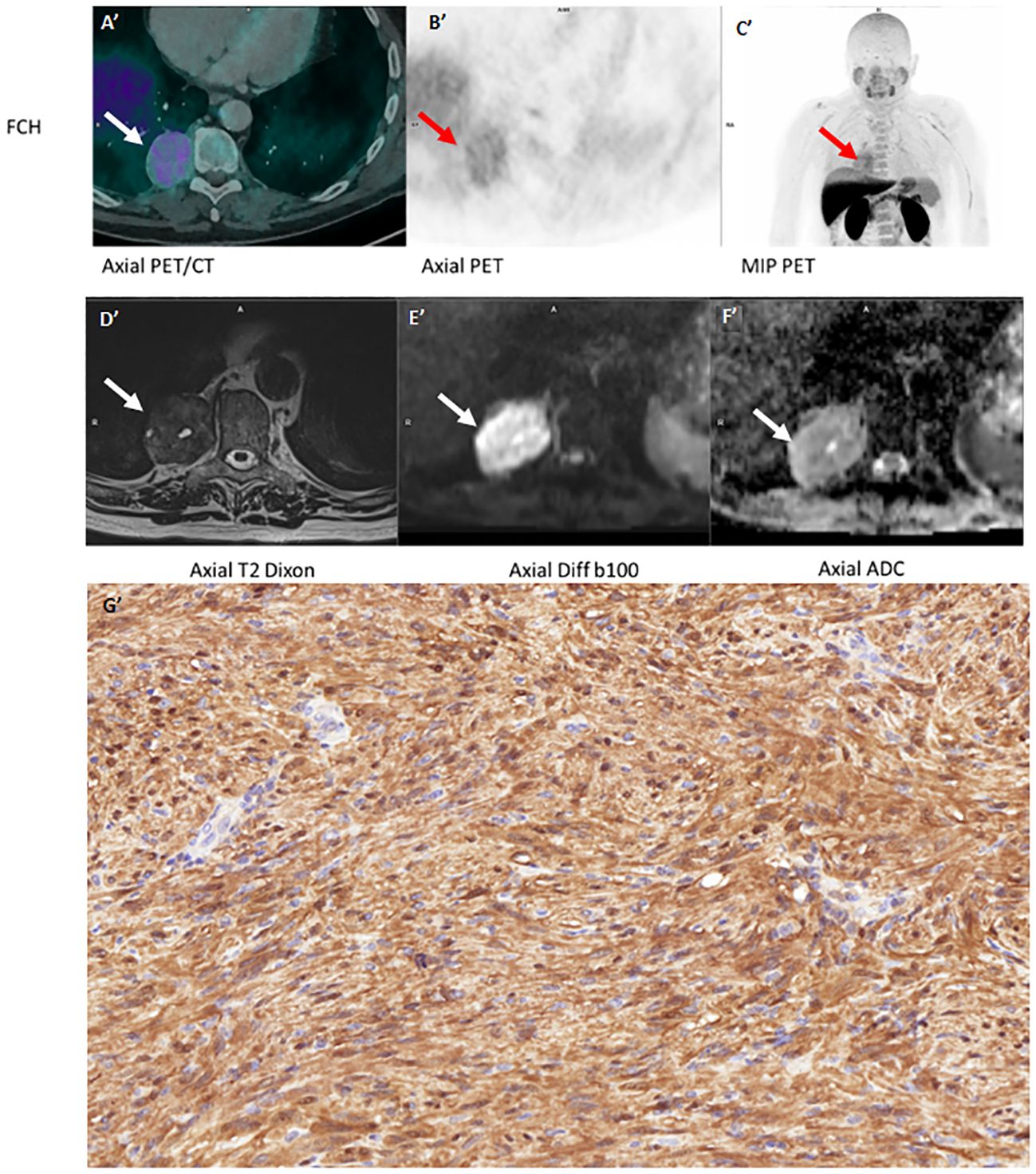
Figure 2. FCH PET/CT (A', B', C') MRI (D', E', F') and (G') (schwanomma histology).
Complementary MRI was performed for both two lesions (panel of different MRI sequence both two cases). It showed same characteristics: heterogeneous T2 hypersignal with some microcystic areas, T1 isosignal to muscle and moderate diffusion restriction; gadolinium injection resulted in early, intense and relatively homogeneous enhancement outside cystic (or myxoid) areas. Figures 1D–F and Figures 2D’-F’.
Both patients (Figure 1G’ and Figure 2G’) were operated on with complete excision in favor of a benign schwannomatous nerve lesion, with a tumor proliferation rate (Ki-67 index) of 3% for both lesions. (Figure 1G: In the pleura, tumor characterised by spindle cells intermingled in bundles. Absence of cytonuclear atypia. Magnification x20. Figure 2G’: High magnification image (x40) of the tumor expressing the positive S100 protein in immunochemistry with strongly and diffusely signal over the entire lesion).
Discussion
18F-FDG PET/CT is used to differentiate between benign and malignant tumors (12). However, false-positive and false-negative results with 18F-FDG PET/CT are relatively common. 18F-FDG uptake in benign schwannomas varies considerably, and benign schwannomas with high FDG uptake can easily be misdiagnosed as malignant. Indeed, even with low levels of Ki-67, the lesion may be avid for 18F-FDG, as there is no correlation between Ki-67 expression and 18F-FDG uptake in schwannomas (13), and this avidity for 18F-FDG could be due to overexpression of GLUT1 or GLUT3, although this is not certain as studies give different results (14, 15).
However, 18F-Choline avidity is less controversial in suspected schwannomas as it is a precursor of phosphatidylcholine, one of the main components of the cell membrane. Its specific pathophysiological pathway allows it to be used as a marker of cell proliferation in PET, helping to detect tumors that synthesize a lot of cell wall, such as prostate cancer (16). Schwannomas are composed of myelin, the precursor of which is phosphatidylcholine (17), which explains their detection on 18F-Choline PET/CT. Although it remains difficult to distinguish between a metastasis and a schwannoma in the case of 18F-Choline uptake, the unusual location of this uptake in the context of a prostate cancer metastasis could more easily point to another etiology, such as a benign tumor.
Conclusion
It seems difficult to conclude a diagnosis of schwannoma on the basis of PET-CT SUV characteristics alone, as their SUVmax seems to vary enormously. There are also several other causes of false positives, such as infectious and inflammatory processes.
Although promising, 18F-Choline PET/CT cannot play a role in the management of newly diagnosed glial lesions, as it is a non-tumor-specific tracer. Biopsy remains the gold standard for accurate diagnosis.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
KA: Writing – original draft, Writing – review & editing. CL: Writing – original draft, Writing – review & editing. AP: Writing – original draft, Writing – review & editing. CN: Writing – original draft, Writing – review & editing. DR: Writing – original draft, Writing – review & editing. IP: Writing – original draft, Writing – review & editing. VT: Writing – original draft, Writing – review & editing. RA: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wang S-Y, Liu J-H, Yao S, Wang S-X, Shao D. PET/CT and contrast-enhanced CT imaging findings in benign solitary schwannomas. Eur J Radiol. (2021) 141:109820. doi: 10.1016/j.ejrad.2021.109820
2. Davis RD, Oldham HN, Sabiston DC. Primary cysts and neoplasms of the mediastinum: recent changes in clinical presentation, methods of diagnosis, management, and results. Ann Thorac Surg. (1987) 44:229–37. doi: 10.1016/s0003-4975(10)62059-0
3. Pavlus JD, Carter BW, Tolley MD, Keung ES, Khorashadi L, Lichtenberger JP. Imaging of thoracic neurogenic tumors. AJR Am J Roentgenol. (2016) 207:552–61. doi: 10.2214/AJR.16.16018
4. Lapierre F, Rigoard P, Wager M. Peripheral nerve tumors. Neurochirurgie. (2009) 55:413–20. doi: 10.1016/j.neuchi.2009.09.004
5. Gonzalez M, Prior JO, Rotman S, Ris H-B, Krueger T. Benign intrapulmonary schwannoma: aspect on F-18 fluorodeoxyglucose PET/CT. Clin Nucl Med. (2011) 36:465–7. doi: 10.1097/RLU.0b013e31820aa268
6. Takeda S-I, Miyoshi S, Minami M, Matsuda H. Intrathoracic neurogenic tumors–50 years’ experience in a Japanese institution. Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg. (2004) 26:807–12. doi: 10.1016/j.ejcts.2004.07.014
7. Ahmed AR, Watanabe H, Aoki J, Shinozaki T, Takagishi K. Schwannoma of the extremities: the role of PET in preoperative planning. Eur J Nucl Med. (2001) 28:1541–51. doi: 10.1007/s002590100584
8. Boré P, Descourt R, Ollivier L, Le Roux P-Y, Abgral R. False positive 18F-FDG positron emission tomography findings in schwannoma-A caution for reporting physicians. Front Med. (2018) 5:275. doi: 10.3389/fmed.2018.00275
9. Dewey BJ, Howe BM, Spinner RJ, Johnson GB, Nathan MA, Wenger DE, et al. FDG PET/CT and MRI features of pathologically proven schwannomas. Clin Nucl Med. (2021) 46:289–96. doi: 10.1097/RLU.0000000000003485
10. Mertens K, Slaets D, Lambert B, Acou M, De Vos F, Goethals I. PET with (18)F-labelled choline-based tracers for tumour imaging: a review of the literature. Eur J Nucl Med Mol Imaging. (2010) 37:2188–93. doi: 10.1007/s00259-010-1496-z
11. DeGrado TR, Baldwin SW, Wang S, Orr MD, Liao RP, Friedman HS, et al. Synthesis and evaluation of (18)F-labeled choline analogs as oncologic PET tracers. J Nucl Med Off Publ Soc Nucl Med. (2001) 42:1805–14.
12. Xu R, Kido S, Suga K, Hirano Y, Tachibana R, Muramatsu K, et al. Texture analysis on (18)F-FDG PET/CT images to differentiate Malignant and benign bone and soft-tissue lesions. Ann Nucl Med. (2014) 28:926–35. doi: 10.1007/s12149-014-0895-9
13. Beaulieu S, Rubin B, Djang D, Conrad E, Turcotte E, Eary JF. Positron emission tomography of schwannomas: emphasizing its potential in preoperative planning. AJR Am J Roentgenol. (2004) 182:971–4. doi: 10.2214/ajr.182.4.1820971
14. Miyake KK, Nakamoto Y, Kataoka TR, Ueshima C, Higashi T, Terashima T, et al. Clinical, morphologic, and pathologic features associated with increased FDG uptake in schwannoma. AJR Am J Roentgenol. (2016) 207:1288–96. doi: 10.2214/AJR.15.14964
15. Pliszka M, Szablewski L. Glucose transporters as a target for anticancer therapy. Cancers. (2021) 13:4184. doi: 10.3390/cancers13164184
16. Tian M, Zhang H, Oriuchi N, Higuchi T, Endo K. Comparison of 11C-choline PET and FDG PET for the differential diagnosis of Malignant tumors. Eur J Nucl Med Mol Imaging. (2004) 31:1064–72. doi: 10.1007/s00259-004-1496-y
Keywords: prostate cancer, thoracic schwannoma, 18 F-choline PET/CT, MRI, FDG-PET/CT
Citation: Amrane K, Le Meur C, Alemany P, Niel C, Renault D, Peillon I, Tissot V and Abgral R (2024) Case report: Thoracic schwannoma as a diagnostic pitfall in both 18F-Choline PET/CT and 18F-FDG PET/CT. Front. Oncol. 14:1467344. doi: 10.3389/fonc.2024.1467344
Received: 19 July 2024; Accepted: 09 September 2024;
Published: 08 October 2024.
Edited by:
Carmelo Caldarella, Fondazione Policlinico Universitario A. Gemelli IRCCS, ItalyReviewed by:
Corina Millo, National Institutes of Health (NIH), United StatesCorinna Altini, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, Italy
Copyright © 2024 Amrane, Le Meur, Alemany, Niel, Renault, Peillon, Tissot and Abgral. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Karim Amrane, a2FtcmFuZUBjaC1tb3JsYWl4LmZy