 Marlen Haderlein1,2*
Marlen Haderlein1,2* Jens von der Grün3,4
Jens von der Grün3,4 Panagiotis Balermpas3,4
Panagiotis Balermpas3,4 Claus Rödel3
Claus Rödel3 Matthias G. Hautmann5Felix Steger5Christopher Bohr6
Matthias G. Hautmann5Felix Steger5Christopher Bohr6 Thomas Hehr7
Thomas Hehr7 Carmen Stromberger8Volker Budach8Markus Schymalla9Rita Engenhart-Cabillic9Lukas Kocik10Hans Geinitz10Ursula Nestle11,12Gunter Klautke13
Carmen Stromberger8Volker Budach8Markus Schymalla9Rita Engenhart-Cabillic9Lukas Kocik10Hans Geinitz10Ursula Nestle11,12Gunter Klautke13 Claudia Scherl14
Claudia Scherl14 Christine Gall15
Christine Gall15 Benjamin Frey1,2
Benjamin Frey1,2 Philipp Schubert1,2
Philipp Schubert1,2 Sabine Semrau1,2Oliver Ott1,2Marco Kesting16Heinrich Iro2,17
Sabine Semrau1,2Oliver Ott1,2Marco Kesting16Heinrich Iro2,17 Sarina K. Mueller2,17†Rainer Fietkau1,2†
Sarina K. Mueller2,17†Rainer Fietkau1,2†- 1Department of Radiotherapy and Radiation Oncology, University Hospital Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
- 2Comprehensive Cancer Center Erlangen-EMN (CCC ER-EMN), Universitätsklinikum Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
- 3Department of Radiotherapy and Radiation Oncology, University Hospital Frankfurt, Goethe-Universitat Frankfurt am Main, Frankfurt am Main, Germany
- 4Department of Radiation Oncology, Zurich University Hospital, Zurich, Switzerland
- 5Department of Radiotherapy and Radiation Oncology, University Hospital of Regensburg, Regensburg, Germany
- 6Department of Otorhinolaryngology, University Hospital Regensburg, Regensburg, Germany
- 7Department of Radiotherapy and Radiation Oncology, Marienhospital, Stuttgart, Germany
- 8Department of Radiotherapy and Radiation Oncology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 9Department of Radiotherapy and Radiation Oncology, University Hospital of Marburg, Marburg, Germany
- 10Department of Radiation Oncology and Radiotherapy, Ordensklinikum Linz Barmherzige Schwestern, Linz, Austria
- 11Department of Radiotherapy and Radiation Oncology, Kliniken Maria Hilf, Moenchengladbach, Germany
- 12Department of Radiation Oncology, Freiburg University Medical Center, Freiburg, Germany
- 13Department of Radiation Oncology, Chemnitz Hospital, Chemnitz, Germany
- 14Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Mannheim, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany
- 15Department of Medical Informatics, Biometry and Epidemiology, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
- 16Department of Oral and Maxillofacial Surgery, University Hospital Erlangen, Erlangen, Germany
- 17Department of Otolaryngology - Head & Neck Surgery, University Hospital Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany
Background: Current standard treatment concepts in head and neck squamous cell carcinoma (HNSCC) are based on former studies using 2D and 3D treatment plans. However, modern radiation techniques allow for a more precise and individual dose application. Therefore, in a clearly defined patient population, de-intensified risk-adapted radiation is investigated.
Methods: Patients with newly diagnosed HNSCC after surgery (with resection margins ≥1 mm and cM0) with the following tumor stages (TNM 7th Edition) were eligible for the study: oral cavity, oropharynx, or larynx: pT1–3, pN0–pN2b; hypopharynx: pT1–2, pN1. The patients should have either a low risk of local recurrence [≤pT2, resection margin ≥5 mm, no peritumoral lymphangiosis (L0), and no perineural invasion] or contralateral lymph node metastasis (≤3 ipsilateral lymph node metastases, in case of well-lateralized oropharyngeal or oral cavity cancer contralateral cN0, otherwise pN0). Patients were assigned to three different treatment regimes with reduction of the treated volume, radiation dose, or both, according to tumor stage and results of surgery performed. The primary objective was to show an LRR of <10% after 2 years.
Findings: A total of 150 patients were enrolled. Tumor localizations were as follows: n = 53 (35.3%), oral cavity; n = 94 (62.7%), oropharynx (82% HPV-positive); n = 2 (1.3%), hypopharynx; and n = 1 (0.7%), larynx. A total of 61 patients (41.0%) were stage IVA, 81 (54.0%) were stage III, and 8 (5.3%) were stage II. Median follow-up was 36 months. Cumulative incidence of 2y-LRR was 5.6% (95% CI: 1.7%–9.2%) in the whole study population and 14.1% (95% CI: 3.8%–23.2%) in patients with oral cavity cancer. Cumulative incidence of 2y-LRR in non-irradiated or dose-reduced regions was 3.5% (95% CI: 0.4%–6.5%). After 2 years, disease-free survival was 92% (95% CI: 87%–96%) and overall survival was 94% (95% CI: 90%–98%) for the complete study cohort. Acute III° toxicity was as follows: dysphagia, 30%; xerostomia, 7%; mucositis, 19%; and dermatitis, 4%. Dysphagia and xerostomia decrease over time. After 27 months, late dysphagia III° and xerostomia II° were 1% and 9%, respectively.
Interpretation: The study met its primary objective. De-intensification of postoperative radiotherapy irrespective of HPV status in a predefined patient population is associated with a favorable toxicity profile without compromising LRR. In an unplanned subgroup analysis, a significantly increased risk of LRR was observed in patients with oral cavity cancer. In these patients, de-intensified radiotherapy should be applied with caution.
Background
In low- and intermediate-risk patient populations with head and neck cancer, 5-year locoregional control rates of over 90% have been achieved, but approximately 30% of the patients suffer from grade III therapy-related side effects, like xerostomia, dysphagia, and trismus, leading to a reduced quality of life (1–7).
Long-term toxicity is highly relevant for cancer survivors. In the last decades, head and neck surgeons significantly de-intensified the extent of surgery in an effort to preserve functionality, e.g., preferring selective or modified radical neck dissection over radical neck dissections. Modern radiation techniques allow a more precise and individual dose application. However, current standard radiotherapy treatment concepts in head and neck squamous cell carcinoma (HNSCC) are based on former studies using 2D and 3D treatment plans. To achieve reduced long-term toxicity rates while maintaining locoregional control, individualized risk-adapted therapy de-intensification is of great interest.
To date, several studies investigated de-intensification of therapy in HPV-associated head and neck carcinomas, but only few studies included patients with HPV-negative head and neck cancer. There are only small prospective studies (8–10) and some retrospective studies (11–13) investigating the possibility of treating ipsilateral elective neck nodes only in the postoperative situation of head and neck cancer. Moreover, the primary tumor region was usually treated with a dose of up to 60–66 Gy (14–16).
To overcome this shortcoming, the objective of this study, the prospective non-randomized multicentric DIREKHT-Trial, was the investigation of an individual de-escalation of the radiotherapy dose and volume in a predefined patient population irrespective of HPV status. The aim was to reduce late toxicity without compromising the oncological outcome defined as locoregional control.
Methods
We performed a prospective multicenter non-randomized phase II trial in a highly selected patient population. Patients should have either a low risk for local recurrence or a low risk for contralateral neck metastases as defined below.
Eligibility criteria were as follows:
- Newly diagnosed HNSCC after resection of the primary tumor and neck dissection.
- No distant metastases.
- Resection margin (R) ≥1 mm.
- According to TNM 7th Edition, the following tumor stages were eligible: oral cavity, oropharynx, or larynx: pT1–3, pN0–pN2b; hypopharynx: pT1–2, pN1.
- Moreover, patients had to fulfill one or both of the following criteria:
► Either low risk for local recurrence defined as ≤pT2 and resection margin ≥ 5 mm and no peritumoral lymphangiosis (L0) and PNI negative (without perineural invasion).
or
► Low risk for contralateral neck node metastases defined as ≤3 ipsilateral lymph node metastases in the setting of adequate contralateral neck dissection of at least six negative nodes (according to WHO) or well-lateralized oropharynx or oral cavity cancers with a minimum of 5 mm from midline in which contralateral neck dissection was not performed.
HPV status in patients with oropharyngeal cancer was tested, but study inclusion and treatment de-intensification were independent of HPV status.
Depending on individual risk factors (low risk for local and/or contralateral neck recurrence), three different de-intensification regimes were possible:
A. Dose reduction in primary tumor region to 56 Gy
B. Omitting elective contralateral neck
C. Dose reduction in primary tumor region and omitting contralateral elective neck
For more detailed information, see Figure 1.
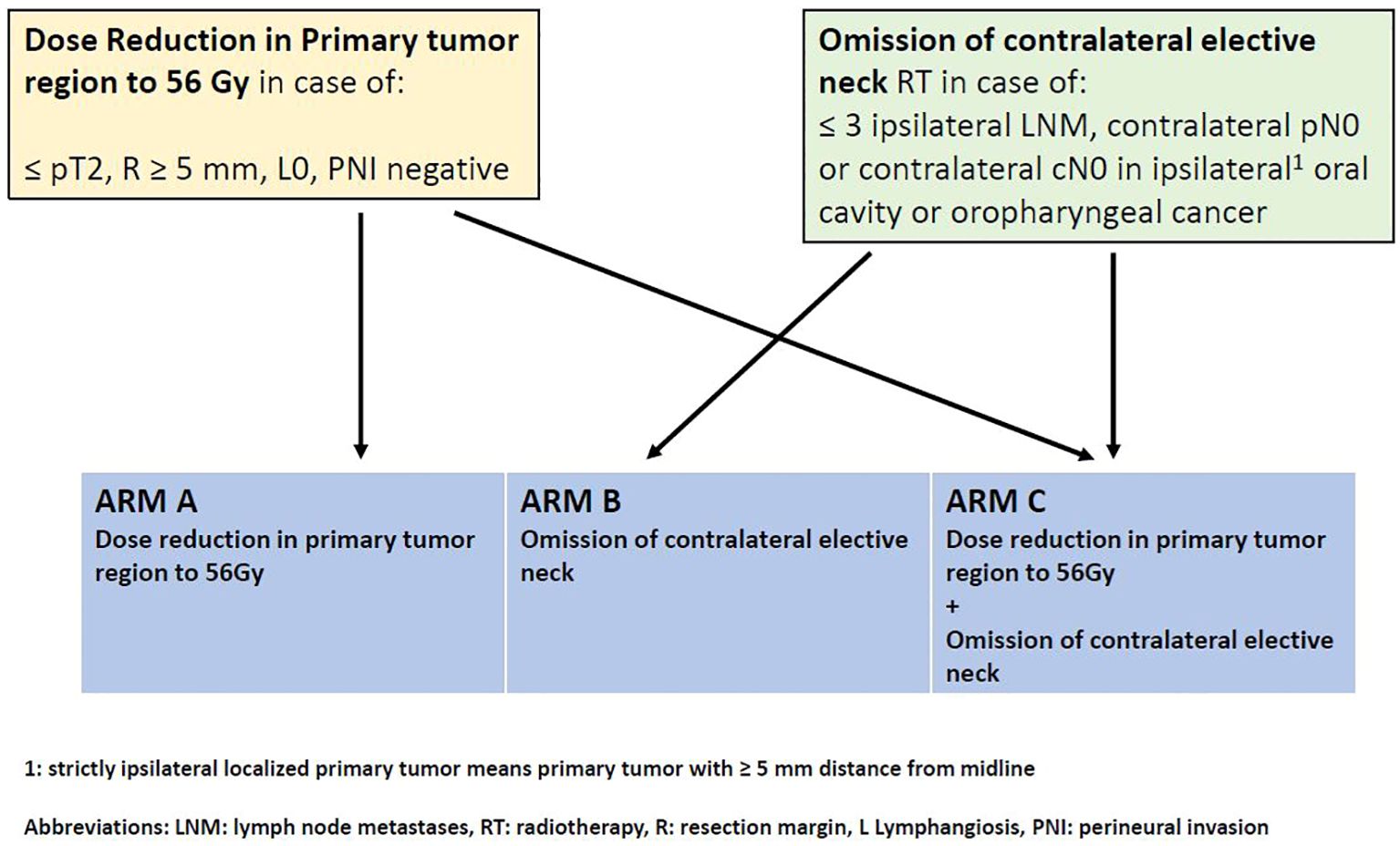
Figure 1. Study scheme.
The study protocol was approved by the local ethics committee No.195_14B and registered in clinicaltrials.gov NCT02528955.
Target volume definition, dose prescription, and radiotherapy planning
Target volume definition and dose prescription were already published in detail (17).
In short, target volumes and dose prescriptions were as follows:
Clinical target volume (CTV)1 included the former primary tumor region or space after resection (in case of ≥pT3 L1 Pn1 or resection margin <5 mm) and lymph node levels with resected lymph node metastases with extranodal extension (ENE).
CTV2 always included the former primary tumor region or space after resection and lymph node levels with resected lymph node metastases.
CTV3, in addition to CTV2, includes elective neck nodes.
Planning target volume (PTV) 1, 2, and 3 resulted by giving a safety margin of 3–5 mm (according to individual setup errors) around each of CTV1, 2, and 3.
The prescribed dose in PTV1, PTV2, and PTV3 was 64 Gy, 56 Gy, and 50 Gy, respectively. Single fraction dose was 2 Gy. One fraction per day and five fractions per week were delivered.
Radiotherapy was delivered as intensity-modulated radiotherapy (IMRT) or volumetric-intensity modulated arc therapy (VMAT) with daily image guidance, using the standard of the institution, e.g., cone beam computer tomography (CBCT) or ExacTRac.
Concurrent chemotherapy
Chemotherapy consisted of 5-FU 800 mg/m² BSA d1–5, cisplatin 20 mg/m² BSA d1–5, qd29 as used in the ARO96-3 trial (16) and was applied according to standard indications in the ARO96-3 trial (close resection margins ≤5 mm, lymph node metastases with ENE, ≥3 lymph node metastases).
In cisplatin-ineligible patients, carboplatin AUC1 d1–5 and 5-FU 800 mg/m² BSA d1–5, qd29 were applied.
Endpoints
The primary endpoint was the LRR after 2 years. Based on previous results of the ARO96-3 study, a 2-year LRR of 10% was expected. In areas with de-intensified radiation, an additional 6% of recurrences was assumed.
The sample size was calculated based on the predicted width of the confidence interval in a binomial distributed hit rate assuming an LRR of 10% (with a likelihood of 80%). As the estimation of the 2-year LRR was based on cumulative incidence rates and the longitudinal character of the data, the calculated sample size was then raised by 15%.
Initially, the half-width of the confidence intervall was planned to be maximally 4.8%, which leads to a sample size of 200. However, the study protocol includes the option of early stopping at a sample size of 150 patients in case of delayed recruitment. Then, the half-width rises to 5.6%.
Secondary endpoints were overall/disease-free survival (OS/DFS) and late toxicity according to common toxicity criteria for adverse events (CTC-AE) version 4.0.
Statistical analysis
Data were collected and restored in an electronic case report form (eCRF) called Secutrial.
The statistical analysis was carried out using the R software (version 4.2.2) (25).
Event times were calculated from the time of first diagnosis (defined as the date of biopsy of the primary tumor). DFS was defined as the absence of locoregional or distant disease recurrence and death from any cause.
We addressed the primary endpoint LRR and the secondary endpoints DFS and OS, as well as the cumulative incidence of distant metastases (DM) and the occurrence of secondary cancer(SC) by the Kaplan–Meier method estimating cumulative incidences and survival. The log-rank test was used for comparison.
As most recurrences occurred in oral cavity cancer patients treated according to de-intensification regime B, an exploratory analysis to identify risk factors for LRR was carried out in this subgroup.
Results
Between November 2014 and April 2021, 150 patients were enrolled in eight different study centers in Germany and Austria. Seven (4.7%) patients received dose reduction in primary tumor region only (regime A); in 95 (63.3%) patients, radiotherapy of the elective contralateral neck was omitted (regime B), and in 48 (32.0%) patients, dose in the primary tumor region was reduced and radiotherapy of the elective contralateral neck was omitted (regime C).
Median age was 59 years (range, 21–81 years). Tumor localizations were as follows: n = 53 patients (35.3%), oral cavity; n = 94 patients (62.7%), oropharynx (82% HPV-positive); n = 2 patients (1.3%), hypopharynx; and n = 1 (0.7%) patients, larynx. A total of 61 patients (40.7%) were stage IVA, 81 (54.0%) were stage III, and 8 (5.3%) were stage II according to AJCC, Seventh Edition (2010). For more detailed information on patient characteristics, see Table 1.
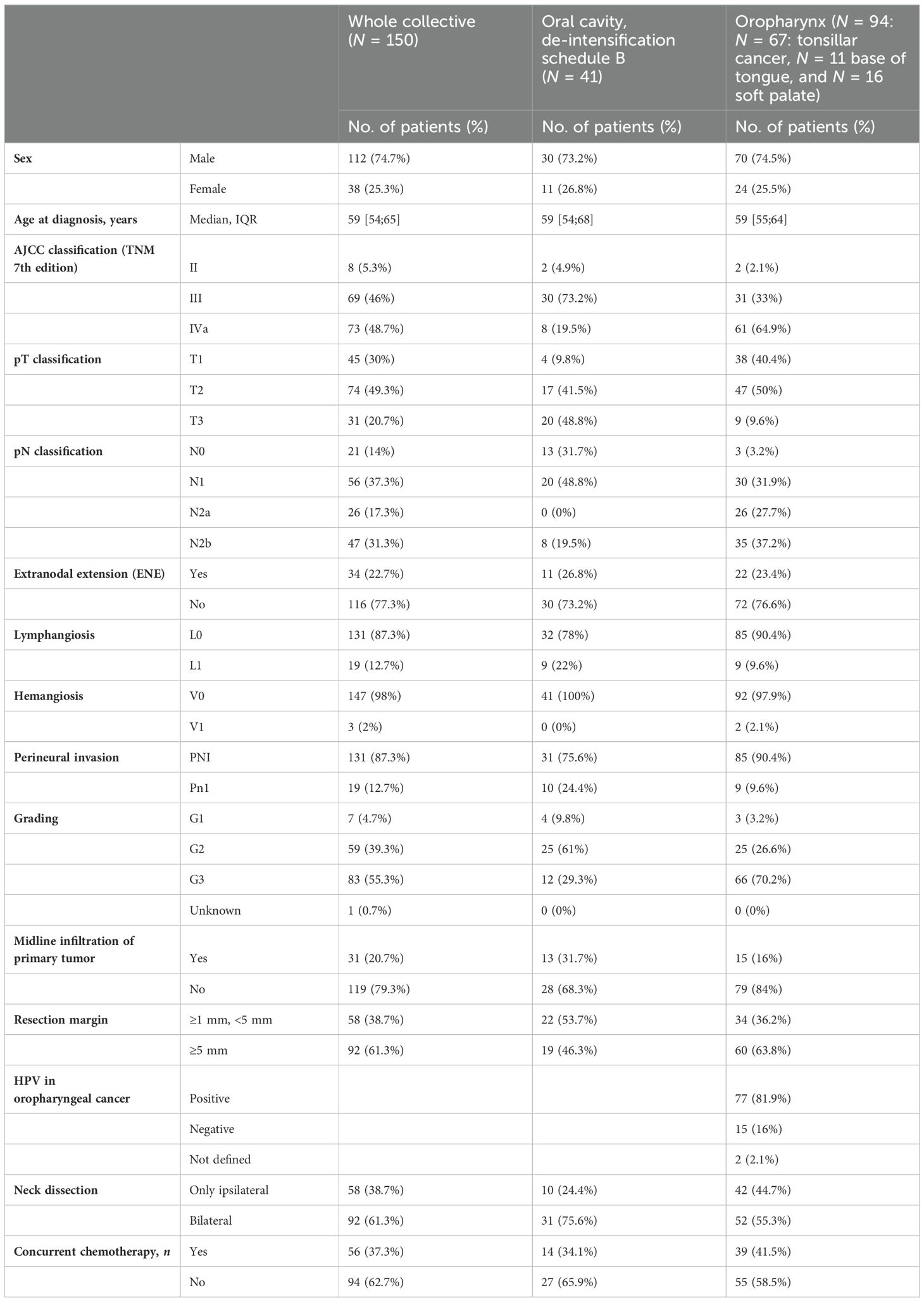
Table 1. Patient characteristics.
Locoregional recurrences
Cumulative incidence of LRR after 1, 2, and 3 years was 5.6%, 5.6%, and 5.6% (95% CI: 1.7%–9.2%), respectively, in the whole study population (see Figure 2). For detailed information on locoregional recurrences, see Table 2.
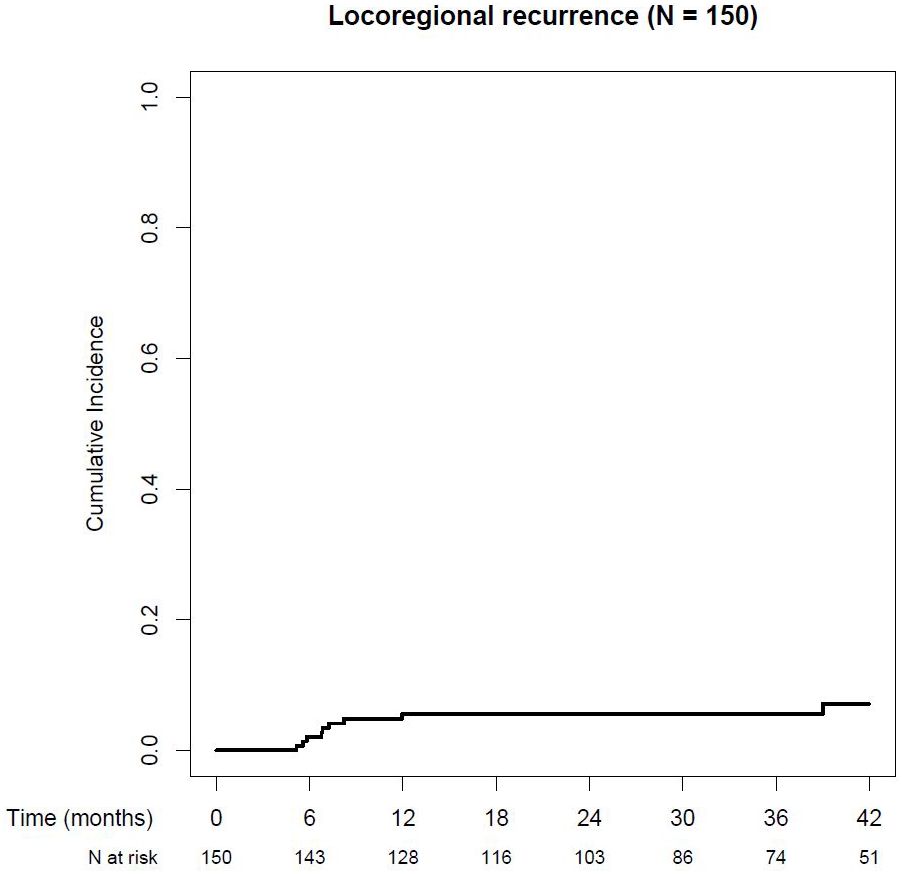
Figure 2. Cumulative locoregional recurrence rate.
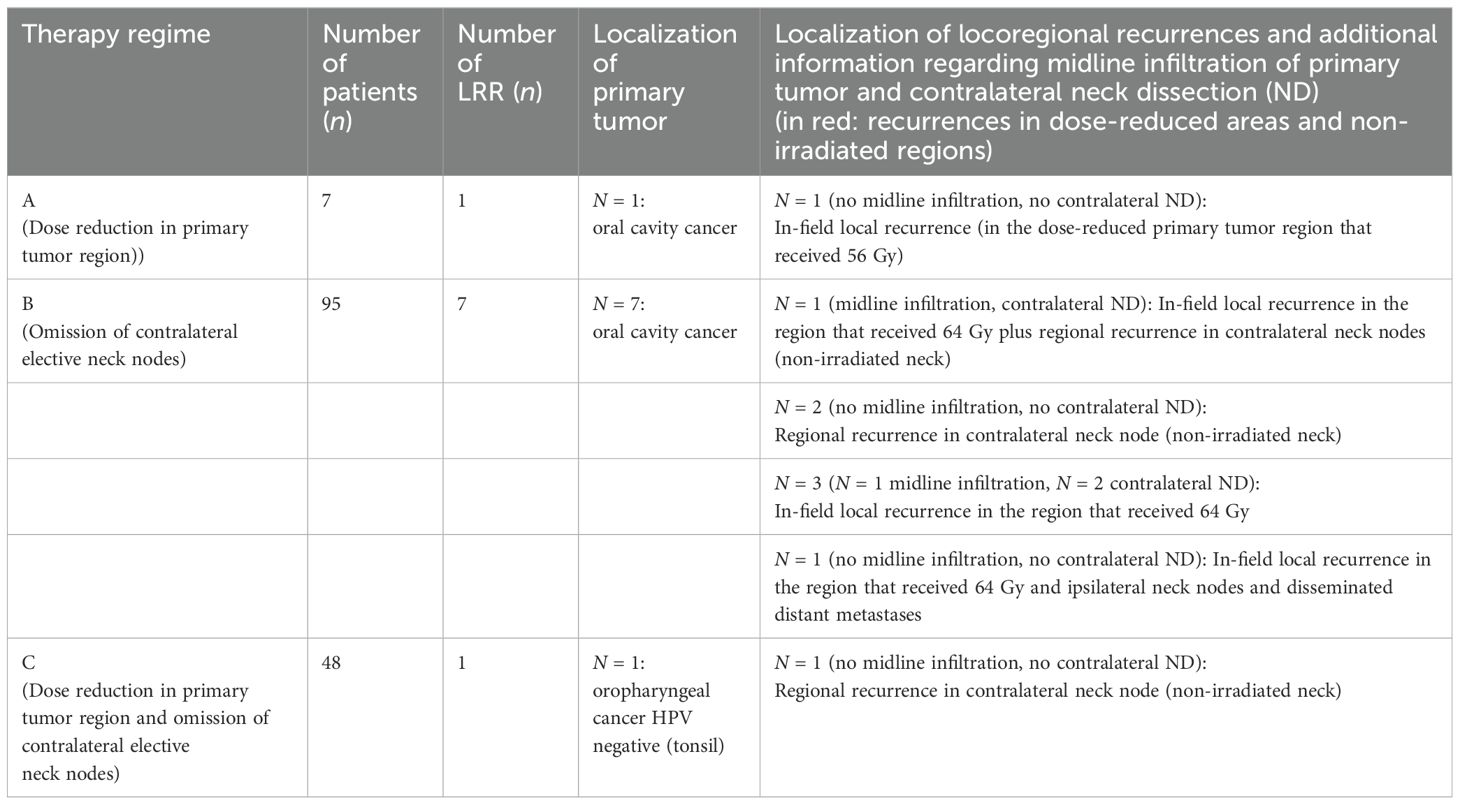
Table 2. Detailed information on locoregional recurrences.
Locoregional recurrences in non-irradiated and/or dose-reduced regions
Cumulative incidence of locoregional recurrences in non-irradiated or dose-reduced regions was seen in 3.5% of all patients (95% CI: 0.4%–6.5%) after 1, 2, and 3 years (see Figure 3). For detailed information, see Table 2.
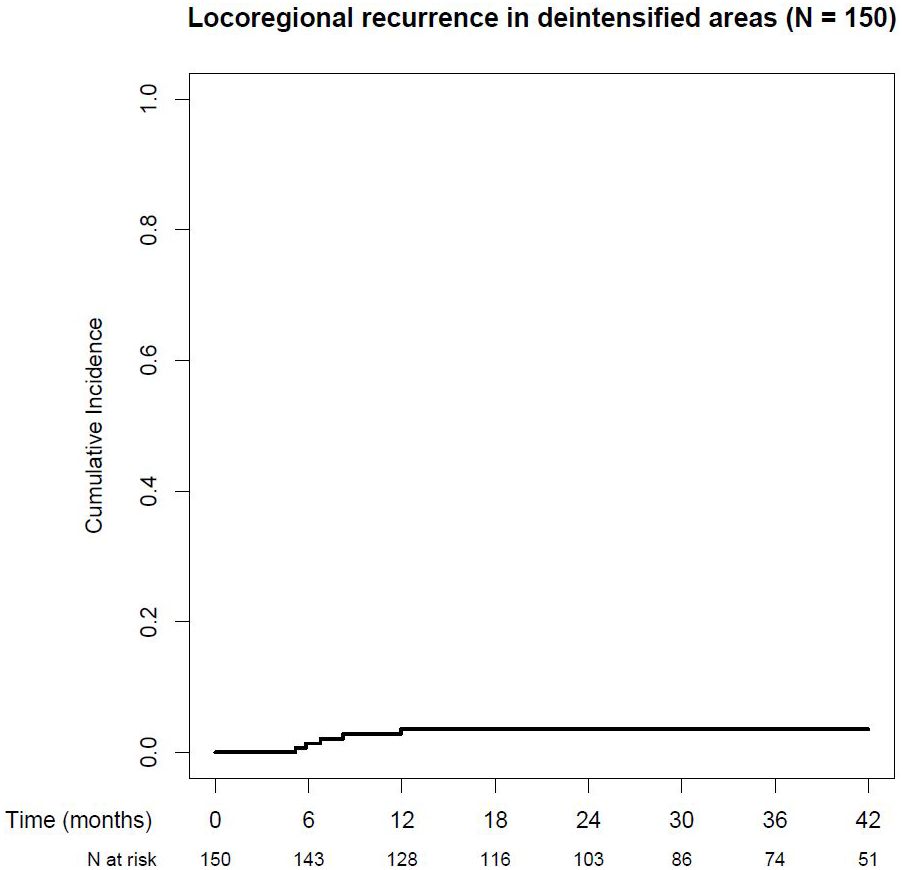
Figure 3. Cumulative locoregional recurrence rate in deintensified areas.
A total of 55 patients were irradiated with a reduced dose in the primary tumor region. One of these 55 patients (1.8%) developed a local recurrence in the dose-reduced region.
Only ipsilateral elective neck was irradiated in 143 patients. From these 143 patients, 4 (2.8%) patients developed a contralateral neck recurrence.
Cumulative incidence of locoregional recurrences in non-irradiated and/or dose-reduced areas was 8.2% in oral cavity cancer and 1.1% in oropharyngeal cancer after 1, 2, and 3 years.
Prognostic factors for locoregional recurrences
In patients with oral cavity cancer, the cumulative incidence of LRR was 14.1% after 1, 2, and 3 years (95% CI: 3.8%–23.2%) and therefore significantly higher compared to patients with oropharyngeal cancer (1.1% after 1, 2, and 3 years, 95% CI: 0%–3.2%), see Figure 4.

Figure 4. Cumulative locoregional recurrence according to tumor localisation.
Most locoregional recurrences occurred in oral cavity patients treated according to de-intensification regime B. In this patient population, univariate statistical analysis showed a trend toward a higher incidence of LRR in patients with a close (>1 mm, but <5 mm) resection margin, with perineural spread and peritumoral lymphangiosis. Midline infiltration, N status and lymph node metastases with ENE showed no correlation with LRR, see Table 3.
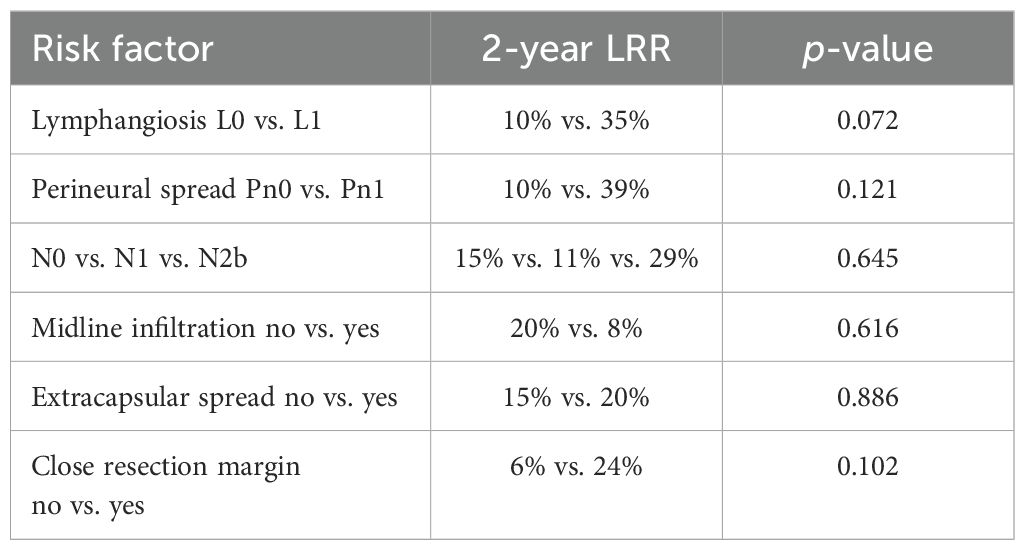
Table 3. Prognostic factors for locoregional recurrences in patients with oral cavity cancer treated in arm B.
Disease-free and overall survival
The 1-, 2-, and 3-year disease-free survival rates (see Figure 5) were 95% (95% CI: 91%–98%), 92% (95% CI: 87%–96%), and 89% (95% CI: 84%–95%), and the corresponding overall survival rates were 96% (95% CI: 93%–99%), 94% (95% CI: 90%–98%), and 94% (95% CI: 90%–98%), respectively.
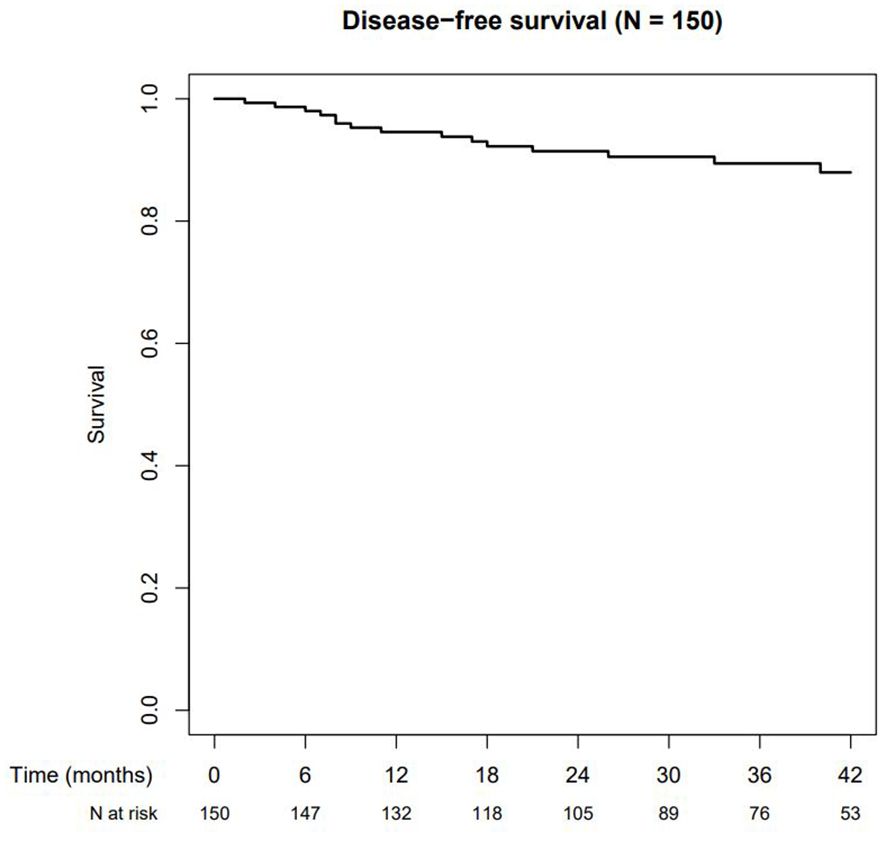
Figure 5. Disease-free survival.
Distant metastases
Cumulative incidence of distant metastases was 4.2% (95% CI: 0.8%–7.4%), 4.2% (95% CI: 0.8%–7.4%), and 5.3% (95% CI: 1.3%–9.1%) after 1, 2 and 3 years, respectively.
During the follow-up time, eight patients developed distant metastases in the following localizations: n = 6, lung; n = 1, bone; and n = 1, disseminated lung, pleura, and liver.
Secondary cancer
Cumulative incidence of a second cancer was 3.6% (95% CI: 0.4%–0.67%), 6.9% (95% CI: 2.4%–11.1%), and 9% (95% CI: 3.7%–14.0%) after 1, 2, and 3 years, respectively.
A total of 17 patients developed a second cancer in the following localizations: n = 3, lung; n = 3, prostate; n = 2, oral cavity; n = 2, renal cell carcinoma; n = 2, contralateral tonsil; n = 1, colon; n = 1, breast cancer; n = 1, cholangiocarcinoma; and n = 1, sarcoma.
Acute toxicity
At the beginning of radiotherapy, dysphagia according to CTC-AE v.4.0 was grade 2: 8% and grade 3: 11%, and xerostomia was grade 2: 4% and grade 3: 1%.
In the last week of radiotherapy, acute toxicity according to CTC-AE version 4.0. was as follows: dysphagia grades 2 and 3: 33% and 30%, weight loss grades 2 and 3: 8% and 10% (see Figures 6A, B).
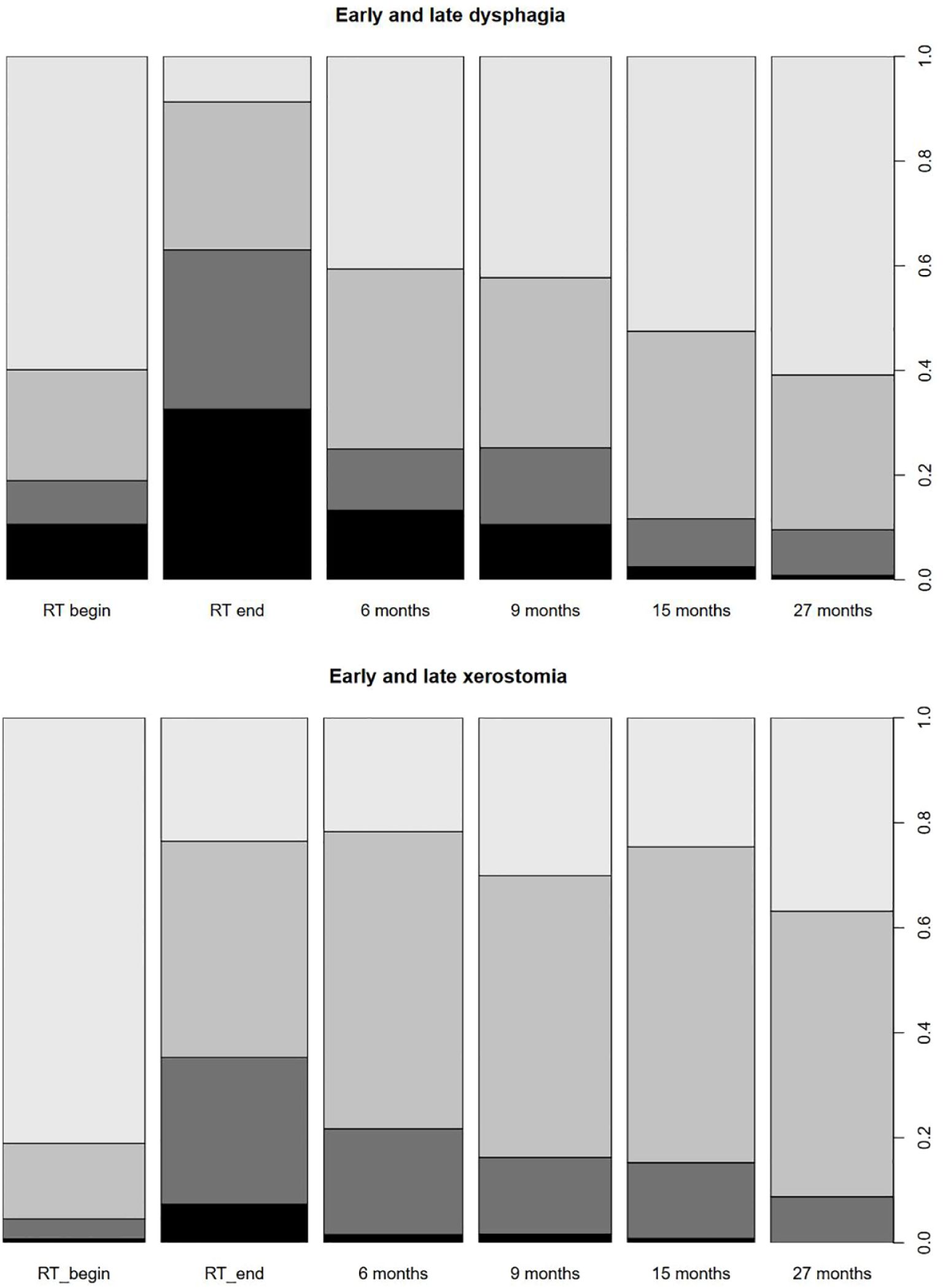
Figure 6. (A) Early and late dysphagia. (B) Early and late xerostomia.
Dermatitis grades 2 and 3: 40% and 4%, xerostomia grades 2 and 3: 28% and 7%, oral mucositis grades 2 and 3: 38% and 19%, and oral pain grades 2 and 3: 29% and 7%.
No grade 4 toxicity was observed.
Late toxicity
Grade of dysphagia and xerostomia decreased over time (see Figures 6A, B). After a follow-up of 9 months, grade 0, 1, 2, and 3 dysphagia was 42%, 33%, 15%, and 11% and decreased after 27 months as follows: grade 0, 1, 2, and 3 dysphagia was 61%, 30%, 9%, and 1%, respectively. After 9 months, late xerostomia was as follows: grade 0: 30%, grade 1: 54%, grade 2: 15%, and grade 3: 2%, and after 27 months, it was as follows: grade 0: 37%, grade 1: 54%, grade 2: 9%, and grade 3: 0%.
Other grade ≥3 toxicities were as follows: esophageal stenosis, 2.0%, and osteonecrosis of the mandible, 0.7%. No further grade ≥3 toxicities occurred.
Grade III° dysphagia was significantly increased in patients with concomitant chemotherapy at the end of RT [55% (with chemo) vs. 20% (without chemo)], but not late dysphagia (3% vs. 1%).
Discussion
In this study, we investigated de-intensification of postoperative radiotherapy in 150 selected patients with HNSCC. A total of 55 patients received a dose reduction in the primary tumor region, and in 143 patients, contralateral elective neck irradiation was omitted.
Our trial showed that de-intensification of radiotherapy in a predefined patient population with head and neck cancer is possible irrespective of HPV status. Cumulative LRR after 2 years was 5.6% (95% CI 1.7%–9.2%) and therefore lower than expected. Moreover, cumulative incidence of LRR in dose-reduced or non-irradiated regions was 3.5%, whereas 2.6% of these recurrences were isolated recurrences. Therefore, the primary objective of the study was met.
Previous data showed that de-intensification of radiotherapy by dose reduction in primary tumor region or target volume reduction leads to significantly reduced dose in salivary glands and swallowing apparatus compared to standard treatment (17). Yet, it was unclear if this dose reduction is clinically relevant. Regarding late toxicity, our data show a comparably low rate of II° and III° late toxicities. Dysphagia III° decreased over time and was by 1% after a follow-up of 27 months. In comparison, in a retrospective population (6) treated with standard radiotherapy, approximately 30% of the patients suffered from grade III° late dysphagia.
An unplanned subgroup analysis showed that LRR in patients with oral cavity carcinomas who were treated with the full dose in the primary tumor region but omitting contralateral elective neck was relatively high, with most of the recurrences occurring in the primary tumor region. Locoregional recurrence in non-irradiated or dose-reduced regions was 8.2% in oral cavity cancer. There was a trend toward a higher incidence of LRR in patients with perineural spread, close resection margin, and/or peritumoral lymphangiosis. In the literature, 5-year locoregional control rates of 78% after surgery plus postoperative radiotherapy are reported (18). Other studies also show that in oral cavity cancer, LRR increases in patients with positive/close resection margins, lymphangiosis, or perineural spread (19). Therefore, it can be assumed that higher LRR in oral cavity carcinomas is because of the tumor biology. Nevertheless, de-intensified radiotherapy should be used with caution, especially dose reduction in the primary tumor region. Rather, in oral cavity cancer, consideration should be given to applying a higher dose in the primary tumor region in the presence of risk factors like close resection margin and perineral spread or lymphangiosis, even in the postoperative situation.
In tonsillar carcinoma, the NCCN guideline recommends in locally limited tumors (pT1–2pN1–N2a according to TNM classification v.7) only ipsilateral elective neck irradiation due to retrospective data (11, 13). There are only two prospective studies (8, 9) with a small sample size including 8 patients with oropharyngeal carcinoma in the definitive setting and 12 patients with oral cavity cancer in the postoperative situation investigating ipsilateral neck irradiation only (8), (9) and 37 patients with oropharyngeal cancer without midline infiltration (9). In both studies, there was no contralateral neck failure, but patients (T1–2 and N0–N2b tumor stage) were highly selected, e.g., all patients had well-lateralized tumor without midline infiltration.
Because of this paucity of prospective data, we also included patients with locally limited oropharyngeal cancer in our study. As a consequence, the retrospective data of O’Sullivan et al. (11, 13) have now been confirmed prospectively.
Moreover, data of our study show that omitting radiotherapy to the contralateral elective neck is possible not only in tonsillar carcinoma but also in other oropharyngeal carcinomas including cancer of the base of tongue and soft palate, even with midline infiltration in case of adequate selective contralateral neck dissection. In a review of Al-Mamgani et al. (12), 1,116 patients with oropharyngeal carcinomas from 11 different studies showed 2.4% of contralateral neck failure after ipsilateral radiotherapy only. However, in 9 of these 11 studies, only patients with tonsillar carcinoma were included, and in 2 of these 11 studies, only patients with tonsillar and soft palate carcinoma were included. Patients with base of tongue tumors have been excluded. In our study, we showed that 2-year locoregional control rate in patients with oropharyngeal carcinoma in all localizations and independent of HPV status is 99% (95% CI: 96.8%–100%) if strictly applying the predefined inclusion criteria.
Unfortunately, patients with laryngeal and hypopharyngeal carcinomas were underrepresented in this study and therefore our results do not allow to draw conclusions for postoperative de-intensification of radiotherapy in laryngeal or hypopharyngeal regions.
Because of the slow recruitment, the study was closed after 150 patients. The slow recruitment could have been due to the complex inclusion criteria and study design.
A shortcoming of the trial is that chemotherapy and radiotherapy were applied according to the ARO96-3 trial, which is a common therapy concept in many institutions in Germany.
The chemotherapy consists of cisplatin and 5-FU and was administered in cases of close resection margins, the presence of ECS, and with three or more affected lymph nodes. According to guidelines, mandatory indications for concurrent chemotherapy (usually with cisplatin alone) are positive resection margins and ECS. Therefore, generalizing the study data should be viewed critically.
Applied dose in the primary tumor region is 64 Gy independent of resection margin (in the current guidelines, 60 Gy in patients with complete resection and 66 Gy in patients with microscopic residual disease). In case of low risk for local recurrence, dose in the primary tumor region was reduced to 56 Gy. A dose of 56 Gy was chosen because in a previous study, we were able to demonstrate that the rate of dysphagia in HNSCC decreases the more the mean dose to the swallowing apparatus falls below 60 Gy (20). In the meantime, we know that a significantly greater dose reduction might be possible in selected patients.
Most of the published and ongoing studies investigating the de-intensification of postoperative radiotherapy are studies in patients with HPV+ oropharyngeal cancer only. ECOG-ACRIN E3311 (21), a prospective phase II study, showed that it might be possible to omit radiotherapy in low-risk patients (pT1–2pN0–N1, negative margins, according to TNM classification v.7) and to reduce radiation dose to 50 Gy in intermediate-risk patients (close margin, ECE ≤1 mm, two to four metastatic lymph nodes, perineural spread, lymph- or hemangiosis) with HPV+ oropharyngeal cancer.
In the MC1675 study (22), a prospective phase III trial, standard radiotherapy versus dose-reduced radiotherapy (30 Gy in 1.5 Gy twice daily in patients with ENE− and 36 Gy in 1.8 Gy twice daily in patients with ENE+) in combination with docetaxel on d1 and d8 was compared to standard-of-care RT (60 Gy and weekly cisplatin). The primary endpoint was toxicity (and not locoregional control) after 3 months, and the difference was not statistically significant, but regarding locoregional control in patients with more than four lymph nodes and ECE, a significantly worse locoregional control rate and reduced PFS were described.
In the AVOID Trial (23), a prospective phase II trial, omission of radiotherapy to the primary tumor region and only irradiation of involved and elective lymph node regions in tumors with pT1–2 stage and a resection margin of ≥2 mm without evidence of perineural spread were investigated. From 60 patients, 1 patient developed local recurrence in the primary tumor region, resulting in a local control rate of 98.3% after 2 years. The “incidental” median dose in the primary tumor region was 39.6 Gy and therefore much lower than the standard radiation dose.
In our trial, patients have been included independent of HPV status, but 82% of all patients with oropharyngeal cancer were HPV positive. Thus, in this patient population, according to other phase II trials (ECOG-Acrin, AVOID), radiation dose in the primary tumor region might be reduced more than we did (e.g., 50 or 40 Gy).
Contreras et al. (10) also included all kinds of HNSCC (n = 14: oral cavity cancer, n = 37: oropharyngeal cancer, n = 4: hypopharyngeal cancer, n = 16: laryngeal cancer, n = 1: CUP) independent of HPV status (HPV+: 49%, 43% not tested). In this prospective phase II study, omitting radiotherapy of the node negative neck was investigated. Patients with tonsillar cancer T1–2 pN0–N2a were excluded in this study. LRR in this patient population (70% mid-line infiltration) was 4%, but PFS was only 60% after 5 years. In this study, all patients had ipsilateral neck dissection and a contralateral neck dissection (92%) or a FDG-PET-CT scan (8%).
From this study and other small prospective phase II studies, we know that de-escalation of postoperative radiotherapy in selected patients is possible. However, the best strategy of de-intensification (radiation dose and/or volume reduction) remains unclear. Moreover, in all published studies, the sample size was limited and prospective phase III data with a primary endpoint regarding locoregional control rate are lacking, but may be impossible to perform as all phase II studies showed a better quality of life following de-escalation.
The fact that the cumulative incidence of second cancer after 3 years is 9% and therefore higher than the cumulative incidence of locoregional recurrence (5.6%) is in line with previous studies (6, 24).
Summarizing, we showed that target volume (omitting contralateral elective neck) and/or dose reduction in a strictly predefined patient population is safe and associated with low late toxicity rates. Therefore, de-intensification of radiotherapy should be performed if clearly defined surgical, pathological, radiological, and radiation oncological standards are fulfilled. To the best of our knowledge, this is the first study to include the biggest patient population with oropharyngeal and oral cavity cancer and investigate de-intensification of radiotherapy in the postoperative situation independent of HPV status.
As a next step, future trials may need to explore updated eligibility criteria that exclude patients who would typically be spared contralateral neck as common practice (e.g., well-lateralized tonsillar carcinoma) already, and it should be investigated if further de-escalation (e.g., only irradiation of the lymph node areas with metastatic disease and no elective neck irradiation) could be performed.
Conclusion
The trial met its primary objective. De-intensification of radiotherapy independent of HPV status in a predefined low-risk patient population appears to result in very low rates of late toxicity without compromising locoregional control. However, in an unplanned subgroup analysis, a significantly increased risk of locoregional recurrence was observed in patients with oral cavity cancer. In these patients, de-intensified radiotherapy should be applied with caution.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the University of Erlangen-Nuremberg. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MH: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. Jv: Investigation, Writing – review & editing. PB: Investigation, Writing – review & editing. CR: Investigation, Writing – review & editing. MH: Investigation, Writing – review & editing. FS: Investigation, Writing – review & editing. CB: Conceptualization, Investigation, Writing – review & editing. TH: Investigation, Writing – review & editing. CS: Investigation, Writing – review & editing. VB: Investigation, Writing – review & editing. MS: Investigation, Writing – review & editing. RE: Investigation, Writing – review & editing. LK: Investigation, Writing – review & editing. HG: Investigation, Writing – review & editing. UN: Investigation, Writing – review & editing. GK: Investigation, Writing – review & editing. CS: Investigation, Writing – review & editing. CG: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. BF: Investigation, Writing – review & editing. PS: Investigation, Writing – review & editing. SS: Investigation, Writing – review & editing. OO: Investigation, Writing – review & editing. MK: Investigation, Writing – review & editing. HI: Conceptualization, Investigation, Methodology, Writing – review & editing. SM: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft. RF: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bjordal K, de Graeff A, Fayers PM, Hammerlid E, van Pottelsberghe C, Curran D, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. (2000) 36:1796–807. doi: 10.1016/S0959-8049(00)00186-6
2. Mehanna HM, Morton RP. Deterioration in quality-of-life of late (10-year) survivors of head and neck cancer. Clin Otolaryngol. (2006) 31:204–11. doi: 10.1111/j.1749-4486.2006.01188.x
3. Mowry SE, Ho A, Lotempio MM, Sadeghi A, Blackwell KE, Wang MB. Quality of life in advanced oropharyngeal carcinoma after chemoradiation versus surgery and radiation. Laryngoscope. (2006) 116:1589–93. doi: 10.1097/01.mlg.0000233244.18901.44
4. Oskam IM, Verdonck-de Leeuw IM, Aaronson NK, Witte BI, de Bree R, Doornaert P, et al. Prospective evaluation of health-related quality of life in long-term oral and oropharyngeal cancer survivors and the perceived need for supportive care. Oral Oncol. (2013) 49:443–8. doi: 10.1016/j.oraloncology.2012.12.005
5. Rathod S, Livergant J, Klein J, Witterick I, Ringash J. A systematic review of quality of life in head and neck cancer treated with surgery with or without adjuvant treatment. Oral Oncol. (2015) 51:888–900. doi: 10.1016/j.oraloncology.2015.07.002
6. Onbasi Y, Lettmaier S, Hecht M, Semrau S, Iro H, Kesting M, et al. Is there a patient population with squamous cell carcinoma of the head and neck region who might benefit from de-intensification of postoperative radiotherapy?: A monocentric retrospective analysis of a previously defined low-risk patient population treated with standard-of-care radiotherapy. Strahlenther Onkol. (2019) 195(6):482–95. doi: 10.1007/s00066-018-1415-y
7. Loser A, Grohmann M, Finger A, Greinert F, Krause L, Molwitz I, et al. Impact of dosimetric factors on long-term percutaneous enteral gastrostomy (PEG) tube dependence in head and neck cancer patients after (chemo)radiotherapy-results from a prospective randomized trial. Strahlenther Onkol. (2022) 198:1016–24. doi: 10.1007/s00066-022-01992-5
8. Cerezo L, Martin M, Lopez M, Marin A, Gomez A. Ipsilateral irradiation for well lateralized carcinomas of the oral cavity and oropharynx: results on tumor control and xerostomia. Radiat Oncol. (2009) 4:33. doi: 10.1186/1748-717X-4-33
9. Hu KS, Mourad WF, Gamez M, Safdieh J, Lin W, Jacobson AS, et al. Low rates of contralateral neck failure in unilaterally treated oropharyngeal squamous cell carcinoma with prospectively defined criteria of lateralization. Head Neck. (2017) 39:1647–54. doi: 10.1002/hed.24806
10. Contreras JA, Spencer C, Dewees T, Haughey B, Henke LE, Chin RI, et al. Eliminating postoperative radiation to the pathologically node-negative neck: long-term results of a prospective phase II study. J Clin Oncol. (2019) 37(28):JCO1900186. doi: 10.1200/JCO.19.00186
11. O'Sullivan B, Warde P, Grice B, Goh C, Payne D, Liu FF, et al. The benefits and pitfalls of ipsilateral radiotherapy in carcinoma of the tonsillar region. Int J Radiat Oncol Biol Phys. (2001) 51:332–43. doi: 10.1016/S0360-3016(01)01613-3
12. Al-Mamgani A, van Werkhoven E, Navran A, Karakullukcu B, Hamming-Vrieze O, Machiels M, et al. Contralateral regional recurrence after elective unilateral neck irradiation in oropharyngeal carcinoma: A literature-based critical review. Cancer Treat Rev. (2017) 59:102–8. doi: 10.1016/j.ctrv.2017.07.004
13. Huang SH, Waldron J, Bratman SV, Su J, Kim J, Bayley A, et al. Re-evaluation of ipsilateral radiation for T1-T2N0-N2b tonsil carcinoma at the princess margaret hospital in the human papillomavirus era, 25 years later. Int J Radiat Oncol Biol Phys. (2017) 98:159–69. doi: 10.1016/j.ijrobp.2017.01.018
14. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefebvre JL, Greiner RH, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. (2004) 350:1945–52. doi: 10.1056/NEJMoa032641
15. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. (2004) 350:1937–44. doi: 10.1056/NEJMoa032646
16. Fietkau R., Lautenschläger C., Sauer R., Dunst J., Becker A., Baumann M., et al. Postoperative concurrent radiochemotherapy versus radiotherapy in high-risk SCCA of the head and neck: Results of the German phase III trial ARO 96–3. J Clin Oncol. (2006) 24:5507–. doi: 10.1200/jco.2006.24.18_suppl.5507
17. Haderlein M, Speer S, Ott O, Lettmaier S, Hecht M, Semrau S, et al. Dose reduction to the swallowing apparatus and the salivary glands by de-intensification of postoperative radiotherapy in patients with head and neck cancer: first (Treatment planning) results of the prospective multicenter DIREKHT trial. Cancers (Basel). (2020) 12. doi: 10.3390/cancers12030538
18. Wennerberg J, Gebre-Medhin M, Nilsson P, Brun E, Kjellen E, Carlwig K, et al. Results from a prospective, randomised study on (accelerated) preoperative versus (conventional) postoperative radiotherapy in treatment of patients with resectable squamous cell carcinoma of the oral cavity - The ARTSCAN 2 study. Radiother Oncol. (2022) 166:26–32. doi: 10.1016/j.radonc.2021.11.008
19. Slieker FJB, Rombout DAA, de Bree R, van Cann EM. Local recurrence and survival after treatment of oral squamous cell carcinoma of the maxilla: A systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. (2022) 133:626–38. doi: 10.1016/j.oooo.2021.10.003
20. Haderlein M, Semrau S, Ott O, Speer S, Bohr C, Fietkau R. Dose-dependent deterioration of swallowing function after induction chemotherapy and definitive chemoradiotherapy for laryngopharyngeal cancer. Strahlenther Onkol. (2014) 190:192–8. doi: 10.1007/s00066-013-0493-0
21. Ferris RL, Flamand Y, Weinstein GS, Li S, Quon H, Mehra R, et al. Phase II randomized trial of transoral surgery and low-dose intensity modulated radiation therapy in resectable p16+ Locally advanced oropharynx cancer: an ECOG-ACRIN cancer research group trial (E3311). J Clin Oncol. (2022) 40:138–49. doi: 10.1200/JCO.21.01752
22. Ma DMEA. MC1675, a phase III evaluation of de-escalated adjuvant radiation therapy (DART) vs. Standard adjuvant treatment for human papillomavirus associated oropharyngeal squamous cell carcinoma. Internation Joural Radiat Oncol Biol Phys. (2021) 111:1324. doi: 10.1016/j.ijrobp.2021.09.012
23. Swisher-McClure S, Lukens JN, Aggarwal C, Ahn P, Basu D, Bauml JM, et al. A phase 2 trial of alternative volumes of oropharyngeal irradiation for de-intensification (AVOID): omission of the resected primary tumor bed after transoral robotic surgery for human papilloma virus-related squamous cell carcinoma of the oropharynx. Int J Radiat Oncol Biol Phys. (2020) 106:725–32. doi: 10.1016/j.ijrobp.2019.11.021
24. Bukovszky B, Fodor J, Szekely G, Kocsis SZ, Oberna F, Major T, et al. Mutagen sensitivity and risk of second cancer in younger adults with head and neck squamous cell cancer: 15-year results. Strahlenther Onkol. (2022) 198:820–7. doi: 10.1007/s00066-022-01917-2
Keywords: head and neck cancer, radiotherapy, HPV, de-intensification, postoperative
Citation: Haderlein M, von der Grün J, Balermpas P, Rödel C, Hautmann MG, Steger F, Bohr C, Hehr T, Stromberger C, Budach V, Schymalla M, Engenhart-Cabillic R, Kocik L, Geinitz H, Nestle U, Klautke G, Scherl C, Gall C, Frey B, Schubert P, Semrau S, Ott O, Kesting M, Iro H, Mueller SK and Fietkau R (2024) De-intensification of postoperative radiotherapy in head and neck cancer irrespective of human papillomavirus status—results of a prospective multicenter phase II trial (DIREKHT Trial). Front. Oncol. 14:1447123. doi: 10.3389/fonc.2024.1447123
Received: 11 June 2024; Accepted: 25 July 2024;
Published: 19 August 2024.
Edited by:
Takumi Kumai, Asahikawa Medical University, JapanReviewed by:
John Lukens, University of Pennsylvania, United StatesCarla Pisani, Azienda Ospedaliero Universitaria Maggiore della Carità, Italy
Dominic Moon, University of Texas Southwestern Medical Center, United States
Alicia Lozano, Catalan Institute of Oncology, Spain
Copyright © 2024 Haderlein, von der Grün, Balermpas, Rödel, Hautmann, Steger, Bohr, Hehr, Stromberger, Budach, Schymalla, Engenhart-Cabillic, Kocik, Geinitz, Nestle, Klautke, Scherl, Gall, Frey, Schubert, Semrau, Ott, Kesting, Iro, Mueller and Fietkau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marlen Haderlein, bWFybGVuLmhhZGVybGVpbkB1ay1lcmxhbmdlbi5kZQ==
†These authors have contributed equally to this work and share last authorship