 Taiping Liao
Taiping Liao Yongjun Long
Yongjun Long- Department of Nuclear Medicine, The Third Hospital of Mianyang (Sichuan Mental Health Center), Mianyang, China
Primary thyroid squamous cell carcinoma is extremely rare. We report a case of primary thyroid squamous cell carcinoma diagnosed using 18F-FDG PET/CT. The patient presented with left axillary lymphadenopathy as the initial symptom. Fine-needle aspiration of the axillary lymph nodes indicated metastatic squamous cell carcinoma. To identify the primary tumor, the patient underwent an 18F-FDG PET/CT scan, which revealed a mass in the thyroid and multiple enlarged lymph nodes with abnormal FDG uptake. Pathological examination of the axillary lymph nodes and thyroid biopsy confirmed the diagnosis of primary thyroid squamous cell carcinoma with lymph node metastasis.
Introduction
Primary thyroid squamous cell carcinoma is extremely rare, with an incidence rate of less than 1% (1), and it is a subtype of anaplastic thyroid carcinoma (2). It mostly occurs in elderly males (3), progresses rapidly, and has a very poor prognosis, with a survival period mostly shorter than one year (4, 5). In this case, we describe a rare instance of primary thyroid squamous cell carcinoma with multiple systemic lymph node metastases.
Case presentation
Nine months ago, the 74-year-old male patient discovered a lump in the left axilla and did not pay much attention to it. Recently, the lump has gradually enlarged and become painful.One week ago, the patient visited our hospital. Ultrasound and CT scans revealed multiple enlarged lymph nodes in the neck and left axilla. Physical examination confirmed multiple enlarged lymph nodes in the neck, which were hard, poorly mobile, and mildly tender (Figures 1A–D). Fine-needle aspiration of the left axillary lymph nodes indicated metastatic squamous cell carcinoma, Immunohistochemistry results indicate: PCK (+), P40 (+), P63 (+), CD56 (+), PAX-8 (-), TTF-1 (-), CgA (-), S100 (-), NUT (-), P53 (+), Ki67 (+, 60%), EBER1/2-ISH (-). The tumor marker test results for this patient are as follows: SCC 5.13 ng/mL (reference range: 0-1.8 ng/mL), CYFRA 21-1 8.42 ng/mL (reference range: 0-3.30 ng/mL), NSE 28.70 ng/mL (reference range: 0-16.5 ng/mL), CA125 82.10 U/mL (reference range: 0-30.2 U/mL). The levels of CA199, CA724, AFP, and CEA are within normal limits. The patient has a history of appendectomy and a 10-year history of coronary artery disease.
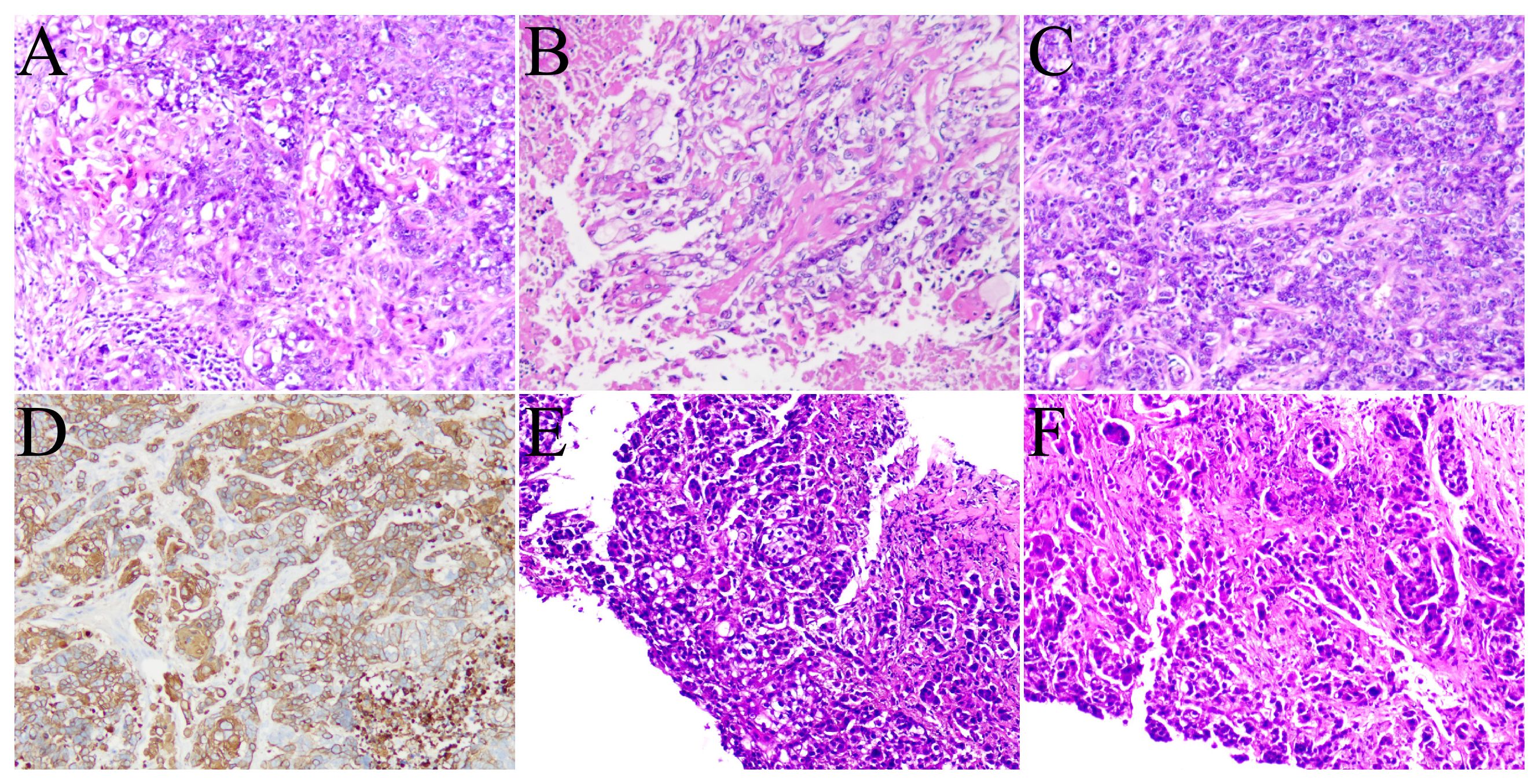
Figure 1 Images (A–D) show the pathological pictures of the left axillary lymph node biopsy. Images (E, F) show the pathological pictures of the thyroid biopsy.
To identify the primary tumor, the patient underwent 18F-FDG PET/CT at our hospital. The PET/CT images showed a heterogeneous mass in the thyroid with significantly increased FDG uptake (Figures 2A–G, arrow), with an SUVmax of 10.0. Multiple enlarged lymph nodes in the neck, right supraclavicular fossa, left axilla, and abdomen,with an abnormally high FDG uptake, with an SUVmax of 15.3. No abnormal morphology or FDG metabolism was observed in other organs. Subsequently, the patient underwent fine-needle aspiration biopsy of the thyroid (Figures 1E, F), which revealed cancer cells with immunohistochemistry positive for P40. Based on the 18F-FDG PET/CT and pathological findings, the patient was diagnosed with primary thyroid squamous cell carcinoma with multiple systemic lymph node metastases. The patient is currently undergoing the first cycle of chemotherapy with paclitaxel and carboplatin.
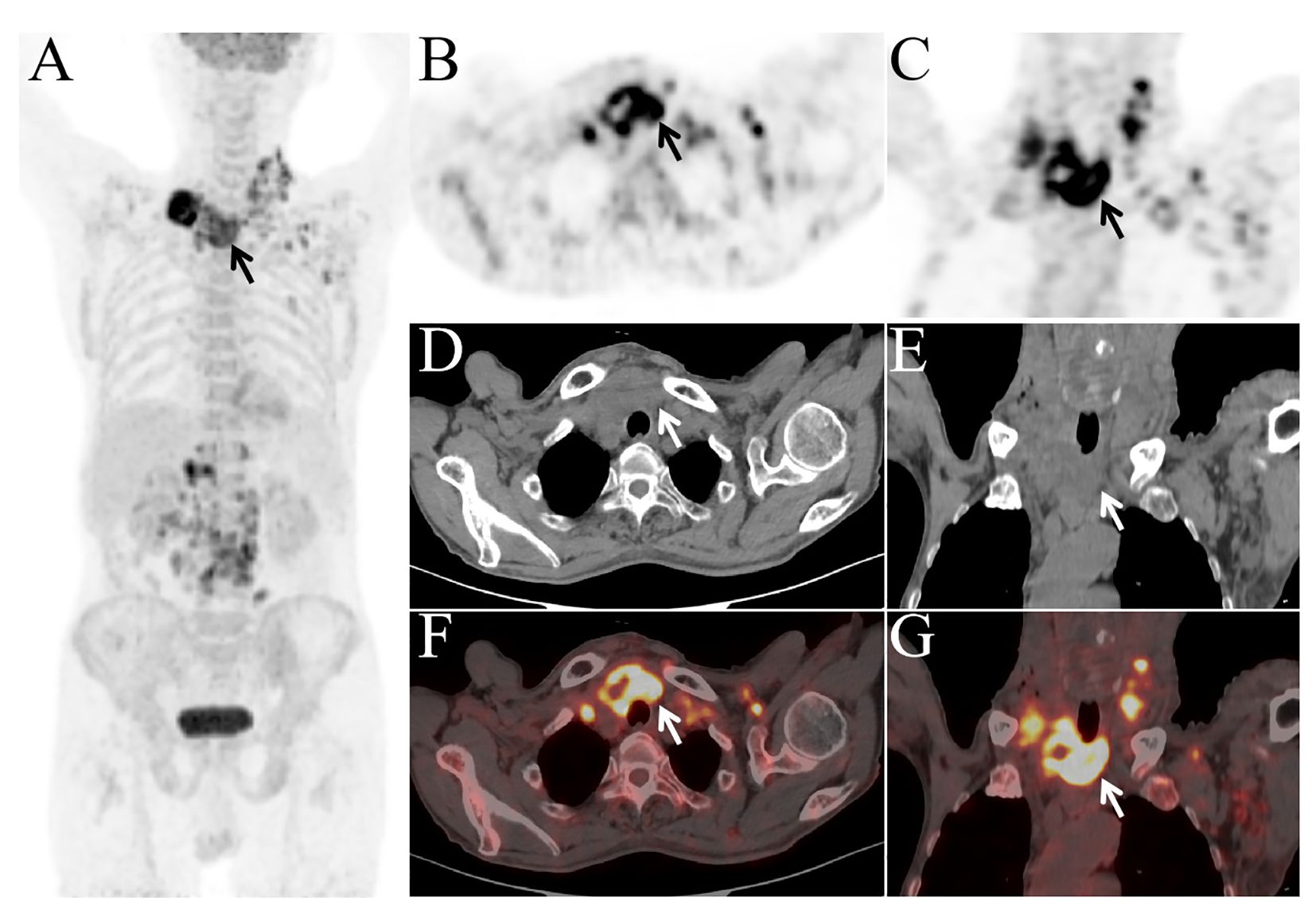
Figure 2 Whole-body imaging (A) revealed multiple areas of increased FDG metabolism in the thyroid region (arrow), neck, and abdomen. The axial and coronal images (B, C), axial and coronal view of PET; (D, E), axial and coronal view of CT; (F, G), axial and coronal view of fusion images) showed a mass in the thyroid with increased FDG metabolism [(B–G), arrow].
Discussion
Primary thyroid squamous cell carcinoma is a malignant tumor originating from thyroid tissue. In the latest World Health Organization classification of endocrine and neuroendocrine tumors, primary thyroid squamous cell carcinoma is included in anaplastic thyroid carcinoma,because squamous cell carcinoma of the thyroid often displays BRAF p.V600E mutations (87%) and exhibits positive immunohistochemical staining for the follicular cell markers PAX8 (91%) and TTF1 (38%) (6). Its incidence is extremely low, accounting for less than 1% of thyroid malignancies. Patients are mostly elderly males. However, it exhibits a high degree of malignancy, progresses rapidly, and carries a poor prognosis, with most patients surviving less than one year. 18F-FDG PET/CT can simultaneously display the glucose metabolism level and morphological information of lesions (7), which is valuable in the diagnosis and staging of thyroid cancer (8). There are few reports on 18F-FDG PET/CT imaging of primary thyroid squamous cell carcinoma (9, 10).
In this case, 18F-FDG PET/CT was crucial in distinguishing primary thyroid squamous cell carcinoma from secondary squamous cell carcinoma. Secondary squamous cell carcinoma could originate from other squamous cell carcinomas outside the thyroid, such as those in the lungs, esophagus, or head and neck region. By showing increased FDG uptake in the thyroid gland and the absence of abnormal FDG uptake in other common sites of squamous cell carcinoma, 18F-FDG PET/CT helped exclude the possibility of a metastatic origin. Additionally, the morphological information provided by PET/CT supported the localization of the tumor to the thyroid. Combined with pathological results showing squamous differentiation in the thyroid tissue, the diagnosis of primary thyroid squamous cell carcinoma was confirmed.
Conclusion
Primary thyroid squamous cell carcinoma is extremely rare,this case emphasizes the value of 18F-FDG PET/CT in identifying primary tumor lesions and is also of great value in distinguishing between primary and secondary thyroid squamous cell carcinoma,which is of great significance for the diagnosis and staging of primary thyroid squamous cell carcinoma.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of The Third Hospital of Mianyang. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
LT: Writing – original draft, Writing – review & editing. LY: Writing – review & editing. LXL: Writing – review & editing. QQ: Writing – review & editing. LL: Writing – review & editing. FG: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sharma PSA, Ranjith J, Murali Mohan BV, Kannan S. Paraneoplastic manifestation of primary squamous cell cancer of the thyroid gland. Cureus. (2023) 15:e39415. doi: 10.7759/cureus.39415
2. Baloch ZW, Asa SL, Barletta JA, Ghossein RA, Juhlin CC, Jung CK, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocr Pathol. (2022) 33:27–63. doi: 10.1007/s12022-022-09707-3
3. Ou D, Ni C, Yao J, Lai M, Chen C, Zhang Y, et al. Clinical analysis of 13 cases of primary squamous-cell thyroid carcinoma. Front Oncol. (2022) 12:956289. doi: 10.3389/fonc.2022.956289
4. Ding W, Gao X, Ran X. Progress in diagnosing and treating thyroid squamous cell carcinoma under the 5th edition of WHO classification. Front Endocrinol (Lausanne). (2024) 14:1273472. doi: 10.3389/fendo.2023.1273472
5. Syed MI, Stewart M, Syed S, Dahill S, Adams C, McLellan DR, et al. Squamous cell carcinoma of the thyroid gland: primary or secondary disease? J Laryngol Otol. (2011) 125:3–9. doi: 10.1017/S0022215110002070
6. Chiba T. Molecular pathology of thyroid tumors: Essential points to comprehend regarding the latest WHO classification. Biomedicines. (2024) 12:712. doi: 10.3390/biomedicines12040712
7. Krause BJ, Schwarzenböck S, Souvatzoglou M. FDG PET and PET/CT. Recent Results Cancer Res. (2013) 187:351–69. doi: 10.1007/978-3-642-10853-2_12
8. Chandekar KR, Satapathy S, Bal C. Positron emission tomography/computed tomography in thyroid cancer: An updated review. PET Clin. (2024) 19:131–45. doi: 10.1016/j.cpet.2023.12.001
9. Caballero Gullón L, Carmona González E, Martínez Estévez A, Gómez Camarero MP, Corral JJ, Borrego Dorado I. Primary squamous cell carcinoma of the thyroid. Initial assessment and follow-up using 18F-FDG PET/CT. Carcinoma epidermoide primario de tiroides. Valoración inicial y control evolutivo mediante 18F-FDG PET/TC. Rev Esp Med Nucl Imagen Mol. (2017) 36:257–9. doi: 10.1016/j.remn.2017.01.001
Keywords: 18F, FDG, PET/CT, thyroid, squamous cell carcinoma
Citation: Liao T, Long Y, Li L, Qi Q, Li L and Fu G (2024) Primary thyroid squamous cell carcinoma diagnosed with 18F-FDG PET/CT: a case report. Front. Oncol. 14:1434811. doi: 10.3389/fonc.2024.1434811
Received: 18 May 2024; Accepted: 27 June 2024;
Published: 08 July 2024.
Edited by:
Alla Reznik, Lakehead University, CanadaReviewed by:
Bilgin Kadri Aribas, Bülent Ecevit University, TürkiyeRong Niu, The Third Affiliated Hospital of Soochow University, China
Copyright © 2024 Liao, Long, Li, Qi, Li and Fu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guoxu Fu, NzQ0NTE1NTQ4QHFxLmNvbQ==