
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 07 October 2024
Sec. Cancer Molecular Targets and Therapeutics
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1433179
This article is part of the Research Topic DNA Damage, Repair and Mutagenesis: Targeting Cancer’s Achilles Heel View all 6 articles
 Laura del Puerto-Nevado1*†
Laura del Puerto-Nevado1*† María J. Fernández-Aceñero2†
María J. Fernández-Aceñero2† Arancha Cebrián1Yuliia Fatych3Luis I. Díez-Valladares4
Arancha Cebrián1Yuliia Fatych3Luis I. Díez-Valladares4 Elia Pérez-Aguirre4Sofía de la Serna4Alejandra García-Botella3,4Javier Martínez-Useros1
Elia Pérez-Aguirre4Sofía de la Serna4Alejandra García-Botella3,4Javier Martínez-Useros1 Jesús García-Foncillas1
Jesús García-Foncillas1 Pedro A. Mateos-Gómez3*
Pedro A. Mateos-Gómez3*Background: DNA polymerase theta (POLQ) is a translesion synthesis polymerase essential for the repair of double strand breaks by the error-prone TMEJ (Theta Mediated End Joining) pathway. Although POLQ participates in maintaining genome stability, several studies have shown that its overexpression correlates with cancer progression and poor prognosis. Due to the fact that its role as a biomarker in pancreatic cancer remains unexplored, we aimed to study the usefulness of POLQ H-score as a prognostic factor in a pancreatic cancer patient cohort.
Methods: We evaluated POLQ gene expression using a web-based tool to deliver gene expression profiling and interactive analyses based on TCGA and GTEx (GEPIA) and we examined the POLQ immunostaining in 152 biliopancreatic cancer surgical specimens using tissue microarrays. Association with survival was evaluated by Kaplan Meier curves and uni-multivariate Cox regression.
Results: GEPIA analysis showed statistical differences according to POLQ mRNA levels in Disease Free Survival (DFS) (log rank 0.023, HR 2.8, p=0.029) and Overall Survival (OS) (log rank 0.011, HR 3.1, p=0.016). For immunohistochemistry (IHC) evaluation, POLQ H-score was calculated, and showed statistical differences for OS in Kaplan Meier curves (log rank 0.001) and uni-multivariate analysis (HR 2.27; 95% CI 1.24-4.15, p=0.008).
Conclusions: Our results indicate that POLQ is an independent prognostic factor in pancreatic cancer when analyzed by immunostaining, which is in agreement with the results shown by the POLQ gene expression analysis (GEPIA).
Pancreatic cancer is one of the most aggressive human tumors because of its rapid growth and its ability to form metastases. Due to these characteristics, diagnosis is usually only possible at advanced stages, leading to a high mortality rate. Despite its relatively low incidence, pancreatic cancer ranks seventh in terms of cancer-related death worldwide (1). Only 20% of patients with pancreatic cancer present surgically resectable tumors at diagnosis, and despite successful surgical resection, 5-year survival remains at 27% (2). Hence, it is important to evaluate new strategies to improve the management and outcome of these patients, concentrating the efforts on the search for valuable biomarkers that could also have therapeutic impact for its clinical application.
DNA replication stress and genomic instability are one of the hallmarks of cancer, helping tumor cells to escape from cell death under uncontrolled proliferation, what makes targeting the DNA damage response (DDR) an effective antitumoral strategy (3, 4). Therefore, the cellular pathways for DNA repair are one of the fields of intense research, of course also related to pancreatic cancer.
Among the DNA repair mechanisms, there is a double strand breaks (DSBs) repair pathway in which the DNA polymerase theta (POLQ) has an essential role, the Theta Mediated End Joining (TMEJ) (5, 6). This is a protein encoded by the POLQ gene and this pathway is crucial for some cancers with deficiencies in homologous recombination (HR), given their reported dependence on TMEJ for survival and tumor growth (5, 7). In addition, POLQ depletion sensitizes cells to several agents that induce DSBs such as camptothecin, bleomycin, etoposide and irradiation (8).
POLQ is a unique DNA polymerase with an N-terminal helicase-like domain, a central domain with no similarities to other enzymes, and a C-terminal A-family DNA polymerase domain (9, 10). Recently it was confirmed that POLQ can dimerize to facilitate the approximation of DNA ends in order to form synapsed intermediates using microhomologies in the sequence, which is the previous step for DNA synthesis (11). In normal cells POLQ is absent or its activity is low, and polq knock-out has a minor impact on development. In addition to its previously reported requirement for survival in BRCA1/2 mutated cells, POLQ would protect cancer cells with functional canonical DSBs repair mechanism from the accumulation of DNA replication associated DSBs (12).
Several studies have shown the association of POLQ expression with outcome in other tumor entities such breast cancer (13, 14), ovarian (7) colorectal cancer (15) or lung cancer (16), and also its relation with pathogenesis in lung adenocarcinoma (17, 18), hepatocellular carcinoma (19) and esophageal squamous cell carcinoma (20, 21). Very recently, the involvement of TMEJ has been implicated in the development and metastasis of KRAS mutated pancreatic cancer (22) and its expression has been associated with a better response to immunotherapy in a subset of bladder cancer patients (23). Additionally, POLQ inhibition in this type of cancer with BRCA2 deficiency is synthetically lethal as expected, but also stimulates the immune response (24).
Since GEPIA (Gene Expression Profiling Interactive Analysis) (25) data showed differences in expression and patient survival, we decided to study whether this DNA polymerase could serve as biomarker in pancreatic cancer. Despite evidence reported in other tumors, there is little data regarding either the impact of POLQ in pancreatic cancer, or the usefulness of immunohistochemistry staining of POLQ as a valuable technique to associate its expression level with patient outcome.
In this report we evaluate the usefulness of POLQ expression analysis for outcome prediction in pancreatic cancer. Additionally, we tested the potential of POLQ immunostaining as a valid technique for this analysis in formalin-fixed, paraffin-embedded (FFPE) tissue sections. Our results indicate that the POLQ H-score obtained from immunohistochemistry is a valuable prognostic biomarker for pancreatic cancer outcomes, which may also contribute to the future design of more personalized therapies that improve patient prognoses.
The GEPIA (Gene Expression Profiling Interactive Analysis) website (http://gepia.cancer-pku.cn/) offers an online tool for analyzing the RNA sequencing expression data of 9,736 tumors from the TCGA and GTEx projects, using a standard processing pipeline. GEPIA allows many interactive and customizable functions including patient survival analysis (25). In our study, GEPIA was used to obtain data about the potential impact of POLQ gene expression in terms DFS and OS in pancreatic adenocarcinoma patients. For both analyses we used a cut off point for POLQ expression of 10%.
A total of 182 biliopancreatic cancer patients who underwent surgery from 2006 to 2012 at the Surgery Department of University Hospital Clínico San Carlos were included in the database. Patients were followed until March 2019 and their clinicopathological characteristics regarding tumor location, stage, histologic type, tumor grade, tumor size, vessel invasion, perineural infiltration and margin status were recorded. The outcome measurements were progression-free survival, defined as the time in months between surgery with a curative intent and disease recurrence shown with imaging methods; and overall survival, defined as the time in months elapsed between surgery with a curative intent and death due to disease.
FFPE samples from 182 biliopancreatic cancer surgical specimens were used for tissue microarray (TMA) construction. Representative tumor regions from samples were identified by a pathologist (MJFA) on hematoxylin- and eosin-stained tissue sections. After pathologist review, TMAs were assembled from triplicate 0.6-mm cores of FFPE tumor samples using the TMA workstation MTA-1 (Beecher Instruments).
For the immunohistochemical techniques the antigen retrieval was performed in a PT-Link (Dako, Glostrup, Denmark) for 20 min at 95 °C in citrate buffer (Dako). Endogenous peroxidase was blocked by adding 0.03% hydrogen peroxide for 5 min. Slides were then washed for 5 min with Tris-buffered saline solution containing Tween 20 at pH 7.6 and incubated with the primary antibody (1:100 POLQ, Thermofisher PA5-115130) for 1.5 hours at room temperature, followed by 30 min incubation with the appropriate anti-Ig horseradish peroxidase-conjugated polymer (EnVision, Dako) to detect antigen–antibody. Sections were then visualized with 3,3′-diaminobenzidine as a chromogen and counterstained with haematoxylin. Only 152 patient samples reached enough quality for immunohistochemical evaluation.
We scanned the TMA stained slide at low power and selected the case showing the highest intensity of staining, which was graded as 3. Then we chose two patterns of staining of moderate (graded as 2) and weak intensity (graded as 1) in the cases, observing a negative staining pattern as well. After marking these cases as reference, we compared all the other cores with the references for grading. Once the grade of each case was assigned, the Histoscore (H-score) of POLQ nuclear staining was determined as the percentage of positive cells in every case multiplied by the intensity of the grade assigned (0=negative; 1=weak; 2=moderate; 3=strong); hence the H-score values could range between 0 and 300.
The cases were blindly graded. Pathologist was unaware of the outcome of the patients.
Clinicopathological patients’ characteristics were reported as frequency (and percentage). The relationship between POLQ H-score and survival (DFS and OS) was estimated using the Kaplan Meier method and significant survival differences between groups were determined by the log rank test.
The relationship between each variable and survival (DFS and OS) was investigated by resorting to a Cox proportional hazards regression model in both univariate and multivariate fashion. Those variables that had potential prognostic significance in univariate analysis (significant variables or variables trending to significance) were subjected to multivariate analysis.
The H-score cutoff point used for this analysis was established in first quartile (Low POLQ H-score ≤ 10 vs High POLQ H-score>10). A p-value < 0.05 was considered statistically significant. All statistical analysis was performed using SPSS software version 20.0 (SPSS Inc., Chicago, IL).
To assess the prognostic potential of POLQ gene expression in patients with pancreatic adenocarcinoma, we conducted a survival analysis using Gene Expression Profiling Interactive Analysis (GEPIA) (25). We studied the prognostic impact of POLQ gene expression in terms of PFS and OS in these samples (N=178) using a cutoff point of 10%. Results obtained with Kaplan Meier method were the following: log-rank=0.023, Hazard Ratio=2.8 and p-value 0.029 for PFS and log-rank=0.011, Hazard Ratio=3.1 and p-value 0.016 for OS, suggesting a predictive and prognostic role of POLQ gene expression in this group of patients (Figure 1).

Figure 1. POLQ mRNA expression is upregulated in pancreatic adenocarcinoma and associated with survival. The expression of POLQ in pancreatic adenocarcinoma tissues was collected from TCGA database. Kaplan Meier survival analysis of patients with low and high POLQ mRNA expression using the Mantel–Cox [log rank] test, n = 178; p value is indicated for comparison of patients with higher or lower POLQ expression. In the left is shown the analysis for disease free survival and in the right is shown the analysis for overall free survival.
We conducted a retrospective study with cohort of 152 patients with resectable biliopancreatic cancer, comprising only cancer stages I and II. In Table 1 we summarized the baseline patient’s characteristics. Most patients included were over 60 years old (79.6%). The distribution of sex across the cohort was similar (47.4% males vs 52.6% females). The predominant tumor location was pancreas and bile duct with few cases of ampullary carcinomas (13.2%); most neoplasms were ductal adenocarcinomas (73%). Regarding sample characteristics, most of the tumors were categorized as high grade (59.9%), and the size of 48.7% of them was over 20 mm. Around half of the tumors (48.7%) presented desmoplastic stroma and 29.6% showed positive disease resection margins in the microscopic analysis, mainly the superior mesenteric vein margin (R1 disease). Regarding tumor aggressive features, 39.5% of patients presented vascular invasion and 65.8% perineural infiltration. Due to the lack of standardization of adjuvant therapy after surgery in this kind of tumor, only 34.9% of patients received adjuvant treatment.
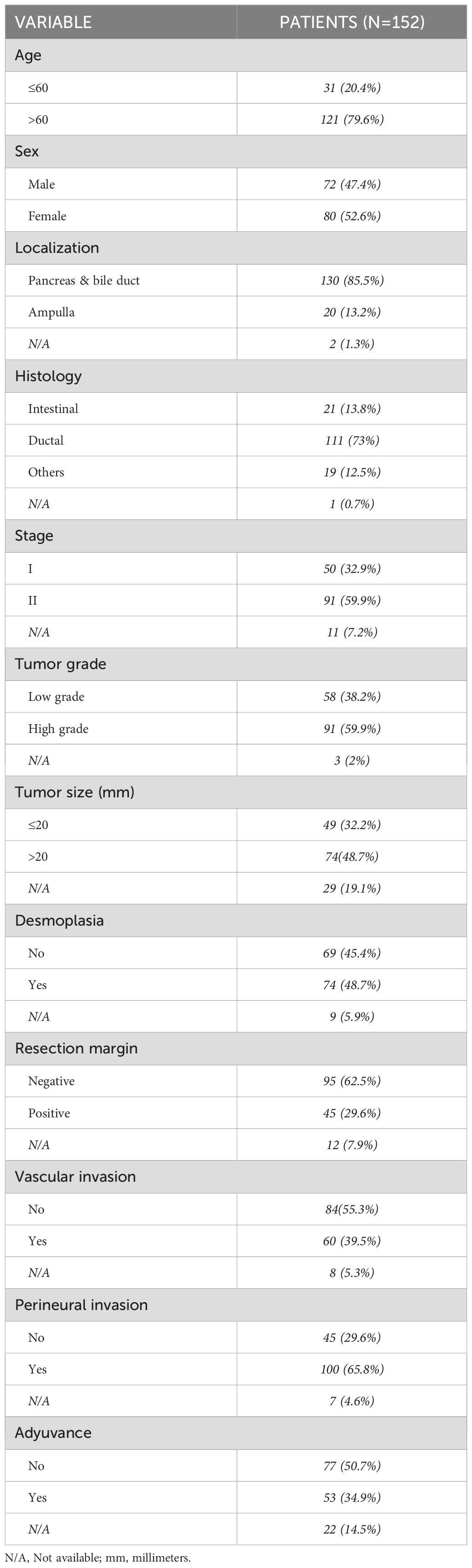
Table 1. Baseline characteristics of included patients.
POLQ protein expression was assessed by immunohistochemistry. The final value to calculate H-score was stablished in terms of percentage of positive cells and staining intensity for each case, evaluating samples in triplicate and representing the value as the mean of the three results.
We also examined the expression localization pattern of POLQ, that was detected in the nucleus and the cytoplasm as shown in Figure 2A. However, considering its role in TMEJ, only nuclear staining was recorded for later H-score calculation. After POLQ expression analysis H-scores were calculated and plotted in a histogram. The H-score values obtained from the cohort revealed a median interquartile range (IQR) value of 40 (10, 80) (Figure 2B).
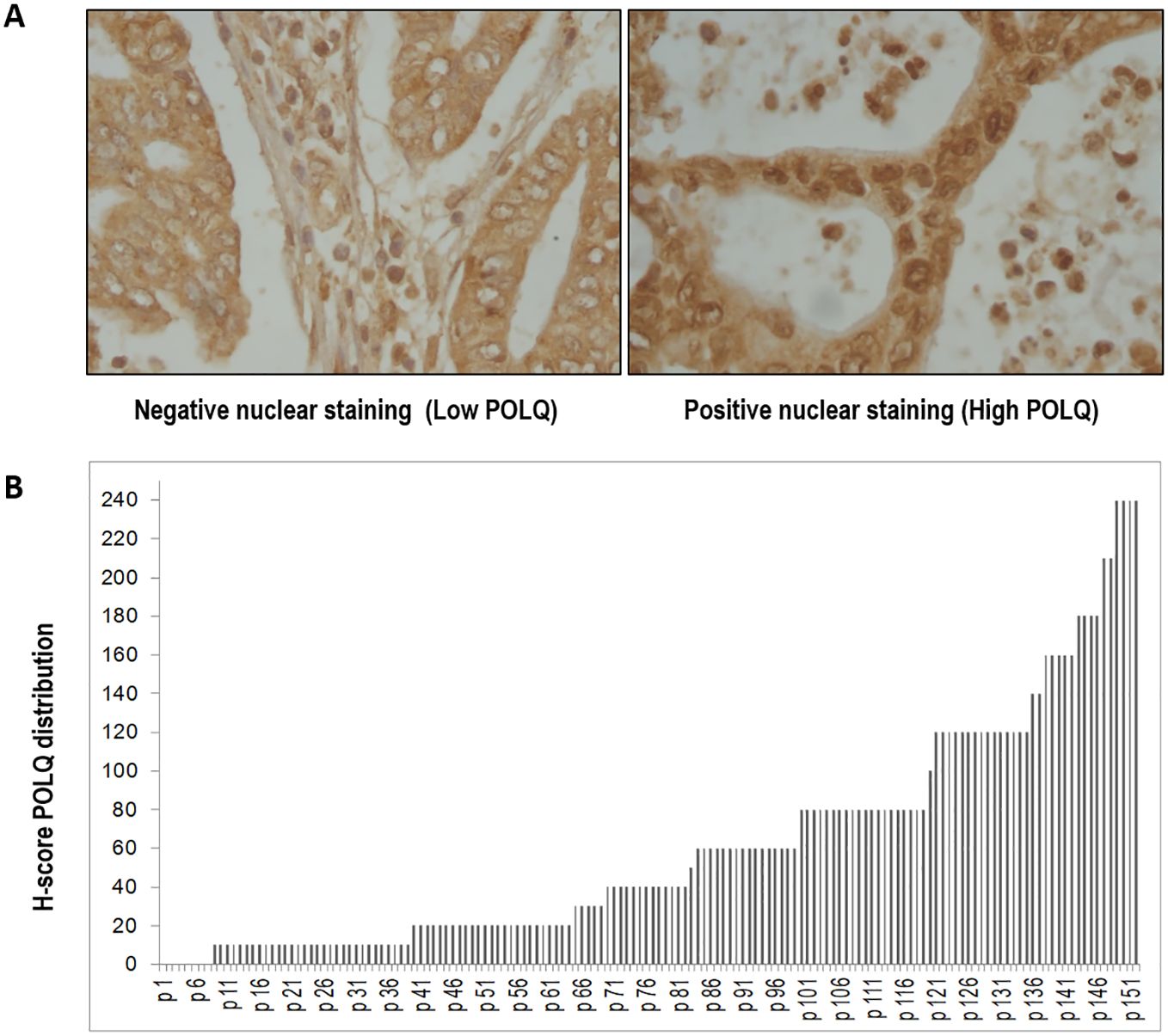
Figure 2. The expression of POLQ in pancreatic adenocarcinoma tissues was detected by IHC. (A) representative images of pancreatic tissues after POLQ immunostaining (x400 magnification). (B) distribution of POLQ H-scores of pancreatic adenocarcinoma tissues analyzed. H-score of POLQ nuclear staining was determined as the percentage of positive cells multiplied by the intensity of the case (0=negative; 1=weak; 2=moderate; 3=strong); hence the H-score values range between 0 and 300.
In terms of overall survival, log rank test showed statistical differences for the staining of this biomarker (log rank. 0.001). The median survival time for the patients with low POLQ was 28 months (IQR, 16 – 74) whereas those cases with high POLQ, showed a worse outcome, with a significantly lower median survival time of 17 months for OS (IQR, 7.5 – 31.5) (Figure 3). These results were in agreement with those obtained with GEPIA and POLQ gene expression.
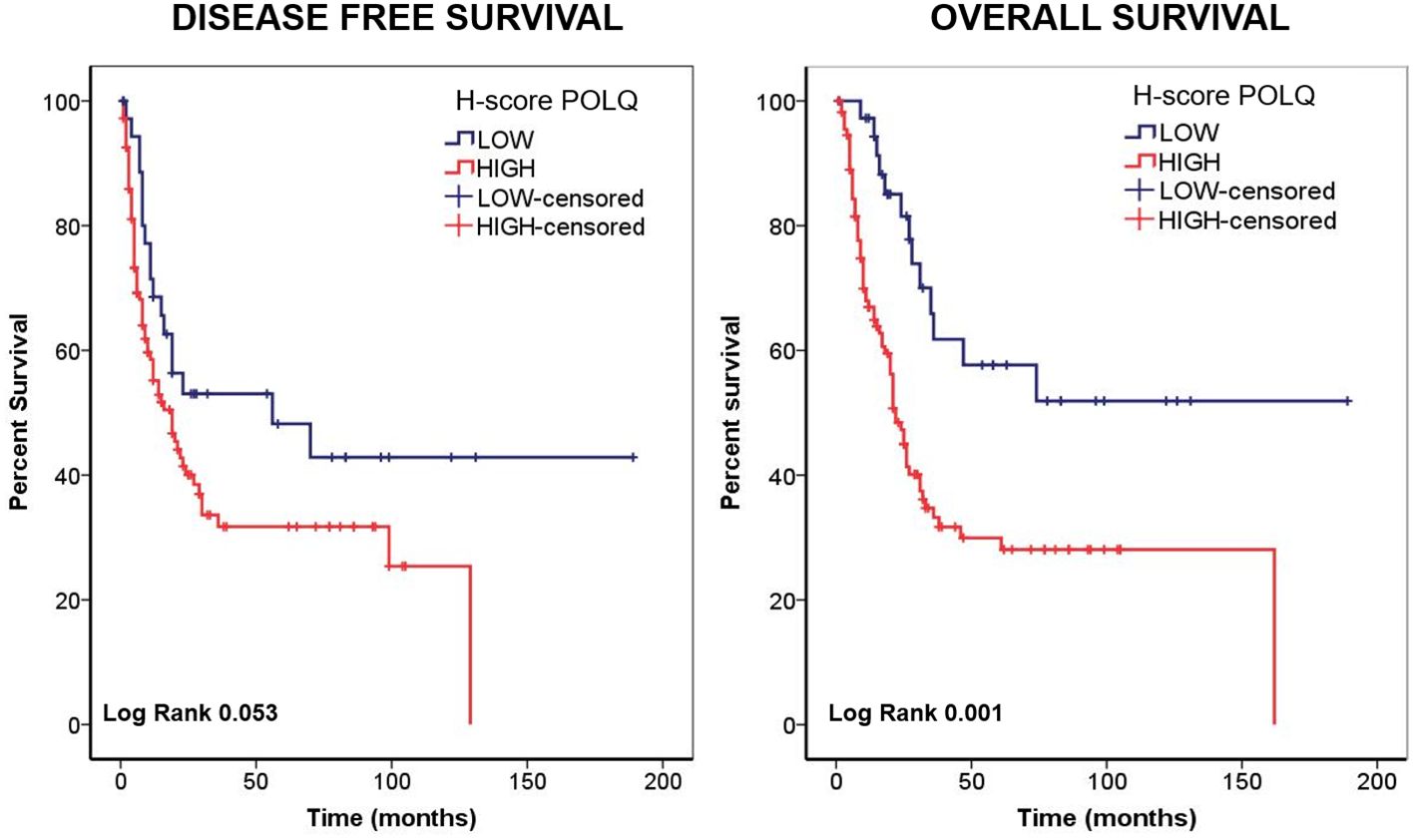
Figure 3. The expression of POLQ in pancreatic adenocarcinoma tissues detected by IHC predicts patient survival. The relationship between POLQ expression in pancreatic adenocarcinoma tissues detected by IHC and patient survival analyzed by Kaplan Meier. In the left is shown the analysis for disease free survival and in the right is shown the analysis for overall survival.
Based on the cutoff point established for POLQ H-score nuclear staining, Kaplan Meier analysis for POLQ as marker was performed in terms of disease-free survival and overall survival, and the correlation between the expression levels of POLQ and prognosis status in patients with pancreatic adenocarcinoma was determined. Regarding the first parameter evaluated, DFS, log rank test derived from Kaplan Meier curve showed a nonsignificant, but strong trend to significance (log rank. 0.053); the median survival time for the patients with low POLQ was 19 months (interquartile range, IQR, 9 – 58) whereas those cases with high POLQ, presented a median survival time of 10 for OS (IQR, 5 – 25).
Considering the results obtained in Kaplan Meier curves, Cox regression was also performed for DFS and OS; multivariate analysis did not show statistical significance for DFS as expected (Data not shown).
However, results for OS were more robust. In univariate analysis, stage and perineural infiltration were significant (HR, 1.66; 95% CI 1.02-2.71, p = 0.04 and HR, 2.21 95% CI 1.29-3.78, p = 0.004, respectively). Sex, histology and tumor grade showed a trend to significance (HR, 1.56; 95% CI 0.99-2.45, p=0.05; HR, 2.08; 95% CI 0.99-4.34, p=0.05 and HR,1.56; 95% CI 0.98-2.49, p=0.06). The molecular marker, POLQ, also showed statistical significance in univariate analysis, (HR, 2.62; 95% CI 1.44-4.76, p=0.002).
As shown in Table 2, in multivariate analysis, performed with univariate significant variables, only the result for POLQ H-score remained statistically significant (HR, 2.27; 95% CI 1.24-4.15, p=0.008), suggesting that POLQ could be an independent predictive factor of outcome for patients with biliopancreatic cancer, in agreement with the results of the POLQ gene expression analysis (GEPIA).
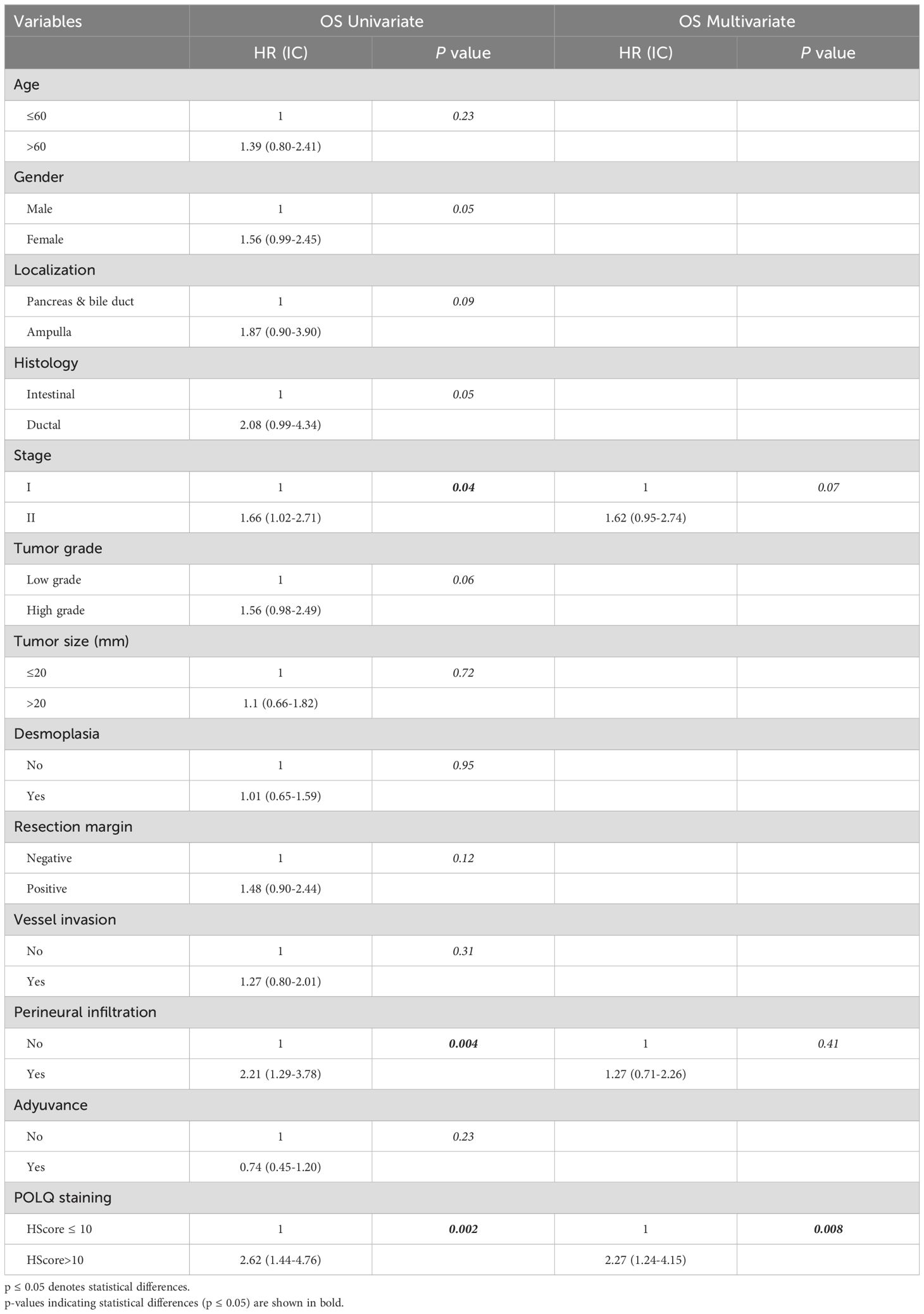
Table 2. Analysis of the relation between POLQ H-score and tumor characteristics in patients with pancreatic adenocarcinoma by uni and multivariate analysis for overall survival.
Recent studies have demonstrated that DNA polymerase theta, encoded by the POLQ gene, plays an important role in DSBs repair pathways, given its essential role in TMEJ. Previous research indicates that POLQ helps to maintain genome stability while its expression correlates with cancer progression and poor prognosis (6). Cancer cells usually show increased expression of POLQ, which would favor their survival. In contrast, normal cells express low levels or do not express POLQ (26). Many studies have also shown that POLQ activity in DNA damage repair is frequently accompanied by deletions and insertions of nucleotides (6, 11, 27, 28). Despite the mutation rate associated with POLQ, this enzyme is involved in preserving genome stability as it can be observed in its absence (12). In addition, it was shown that POLQ promotes the survival of cells deficient in homologous recombination genes, where a synthetically lethal correlation was revealed (5, 7), even very recently in pancreatic cancer cells (22, 24). The higher expression of POLQ mRNA observed in breast, colorectal and lung cancer, correlates with reduced patient survival (13, 15, 16, 18, 20), and may be helping cancer cells to counteract replication stress and genome instability, preventing large deletions and genomic rearrangements (29, 30). In addition, the mutations associated with TMEJ repair could serve as an adaptive mechanism favoring further clonal diversity and evolutionary resistance to treatments (31). Therefore, the differences in expression between cancer and normal tissues, and its role in survival and evolution of cancer cells have made POLQ a potential therapeutic target in cancer treatment. Furthermore, three inhibitors have been developed very recently, and although they inhibit POLQ in vitro, they show low potency in vivo and in xenograft models. One of these inhibitors targets the polymerase activity and two of them the helicase activity of POLQ (32–34).
One can say that great efforts have been made to understand how POLQ works and its functions in cells, and to develop chemical inhibitors for this unusual enzyme. On the other hand, the potential of POLQ as a biomarker in cancer remains poorly explored, aside from the mRNAs level studies that were mentioned above.
There are some reports regarding mutations in the POLQ gene, all found in familiar pancreatic cancer and in the undifferentiated sarcomatoid carcinoma, but both represent the minority of the cases (35–37). Likewise, not much is known regarding the relationship of POLQ mRNA expression and patient outcome. In agreement with our observations, two studies showed that pancreatic ductal adenocarcinoma (PDAC) patients with low POLQ expression have higher survival rates (22, 24). In addition, in one of them, the results indicated that this correlation is independent of KRAS status, but that there is an increase in expression of some proteins of the TMEJ pathway in pancreatic cancer cells, both in tumor samples and in cell lines carrying the activating KRAS mutation G12D (22).
Hence, in this work we evaluated the impact of POLQ in a pancreatic cancer cohort and we tested the usefulness of immunostaining as a valid technique for this type of analysis.
The data obtained in this study analyzing tumor samples by IHC from a cohort of pancreatic adenocarcinoma patients, allowed us to show that there is a strong impact of POLQ expression in the outcome of patients with this type of tumors. POLQ nuclear staining was the only variable that remained statistically significant in the multivariate analysis. Other variables such as stage and perineural infiltration, although in univariate analysis they were statistically significant, they did not remain as that in the multivariate analysis. These results indicate that POLQ may be a useful prognostic biomarker in this type of tumor, with more potential and more robust that other variables. A fact that is supported also with the results obtained from the GEPIA (Figure 1), that also showed the same correlation using the mRNA levels. This correlation between survival of patients with pancreatic adenocarcinoma and POLQ mRNA levels was also confirmed recently (22, 24). In addition, GEPIA data showed that POLQ mRNA is on average twenty times more abundant in pancreatic adenocarcinoma tumor samples than in normal pancreatic tissues (data not shown), which enhances the potential of POLQ as a therapeutic target and prognostic biomarker.
These findings indicate that POLQ expression is a prognostic factor of patient survival and suggest that its evaluation should be considered to guide the application of a treatment based on TMEJ inhibition. While the new POLQ inhibitors are in an early stage of development, the extensive research in this field will undoubtedly lead to the generation of new ones with higher potential. Finally, this method of POLQ analysis by IHC could be very useful for future POLQ inhibitors clinical trials.
The development of protocols to analyze POLQ expression by IHC could be helpful in other cancers, since the increase in POLQ abundance takes place in most of the tumors analyzed (7, 13–17, 19–22) and in the different tumor data included in GEPIA. In addition, IHC performed in Hepatocellular carcinoma (HCC) samples also showed that POLQ was expressed higher than in normal tissues (19). In this study they also analyzed the correlation between samples from patients with high POLQ expression in the IHC and the tumor recurrence or patient survival, finding that high POLQ expression in tumor samples predicted poorer prognosis (19). These results suggest that POLQ expression has potential as a prognostic marker in HCC when analyzed by IHC, in agreement with our results in pancreatic cancer. In the other hand, the recently published POLQ IHQ analysis performed for muscle-invasive bladder cancer patients, showed that high POLQ expression correlated with better overall survival. Although these results seem to disagree with ours, they evaluated the response to immunotherapy treatment in patients with also high PD-L1, but did not directly correlate POLQ expression and patient survival (38).
Our results indicated that high POLQ H-score was associated with poor survival, therefore, POLQ could be considered an independent prognostic factor for patients with pancreatic cancer.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Clinical research ethical committee from the Hospital Clínico San Carlos. Madrid, Spain. Sample collection was carried out with the approval of the Institutional Review Board (IRB-HCSC) under approval code CI 17/091-E. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LD: Formal analysis, Investigation, Writing – original draft, Conceptualization, Data curation, Writing – review & editing. MF-A: Conceptualization, Methodology, Supervision, Writing – original draft, Data curation, Writing – review & editing. AC: Data curation, Investigation, Writing – review & editing. YF: Formal analysis, Writing – review & editing, Data curation. LD-V: Writing – review & editing, Resources. EP-A: Resources, Writing – review & editing. SD: Resources, Writing – review & editing. AG-B: Resources, Writing – review & editing. JM-U: Resources, Writing – review & editing. JG-F: Resources, Writing – review & editing. PAM-G: Conceptualization, Data curation, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Comunidad de Madrid within the program V PRICIT, Grant Number CM/JIN/2021-020 (to PAM-G); and Ministerio de Ciencia y Universidades Grant Number RTI2018-097016-A-I00 (to PAM-G).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. McGuigan A, Kelly P, Turkington RC, Jones C, Coleman HG, McCain RS. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J Gastroenterol. (2018) 24:4846–61. doi: 10.3748/wjg.v24.i43.4846
3. Patterson-Fortin J, D'Andrea AD. Exploiting the microhomology-mediated end-joining pathway in cancer therapy. Cancer Res. (2020) 80:4593–600. doi: 10.1158/0008-5472.CAN-20-1672
4. Dalmasso B, Puccini A, Catalano F, Borea R, Iaia ML, Bruno W, et al. Beyond BRCA: the emerging significance of DNA damage response and personalized treatment in pancreatic and prostate cancer patients. Int J Mol Sci. (2022) 23:4709. doi: 10.3390/ijms23094709
5. Mateos-Gomez PA, Gong F, Nair N, Miller KM, Lazzerini-Denchi E, Sfeir A. Mammalian polymerase θ promotes alternative NHEJ and suppresses recombination. Nature. (2015) 518:254–7. doi: 10.1038/nature14157
6. Ramsden DA, Carvajal-Garcia J, Gupta GP. Mechanism, cellular functions and cancer roles of polymerase-theta-mediated DNA end joining. Nat Rev Mol Cell Biol. (2022) 23:125–40. doi: 10.1038/s41580-021-00405-2
7. Ceccaldi R, Liu JC, Amunugama R, Hajdu I, Primack B, Petalcorin MI, et al. Homologous-recombination-deficient tumours are dependent on Polθ-mediated repair. Nature. (2015) 518:258–62. doi: 10.1038/nature14184
8. Wood RD, Doublié S. DNA polymerase θ (POLQ), double-strand break repair, and cancer. DNA Repair (Amst). (2016) 44:22–32. doi: 10.1016/j.dnarep.2016.05.003
9. Seki M, Marini F, Wood RD. POLQ (Pol theta), a DNA polymerase and DNA-dependent ATPase in human cells. Nucleic Acids Res. (2003) 31:6117–26. doi: 10.1093/nar/gkg814
10. Mateos-Gomez PA, Kent T, Deng SK, McDevitt S, Kashkina E, Hoang TM, et al. The helicase domain of Polθ counteracts RPA to promote alt-NHEJ. Nat Struct Mol Biol. (2017) 24:1116–23. doi: 10.1038/nsmb.3494
11. Black SJ, Ozdemir AY, Kashkina E, Kent T, Rusanov T, Ristic D, et al. Molecular basis of microhomology-mediated end-joining by purified full-length Polθ. Nat Commun. (2019) 10:4423. doi: 10.1038/s41467-019-12272-9
12. Hwang T, Reh S, Dunbayev Y, Zhong Y, Takata Y, Shen J, et al. Defining the mutation signatures of DNA polymerase θ in cancer genomes. NAR Cancer. (2020) 2:zcaa017. doi: 10.1093/narcan/zcaa017
13. Lemée F, Bergoglio V, Fernandez-Vidal A, MaChado-Silva A, Pillaire MJ, Bieth A, et al. DNA polymerase theta up-regulation is associated with poor survival in breast cancer, perturbs DNA replication, and promotes genetic instability. Proc Natl Acad Sci U S A. (2010) 107:13390–5. doi: 10.1073/pnas.0910759107
14. Higgins GS, Harris AL, Prevo R, Helleday T, McKenna WG, Buffa FM. Overexpression of POLQ confers a poor prognosis in early breast cancer patients. Oncotarget. (2010) 1:175–84. doi: 10.18632/oncotarget.v1i3
15. Pillaire MJ, Selves J, Gordien K, Gourraud PA, Gouraud PA, Gentil C, et al. A 'DNA replication' signature of progression and negative outcome in colorectal cancer. Oncogene. (2010) 29:876–87. doi: 10.1038/onc.2009.378
16. Allera-Moreau C, Rouquette I, Lepage B, Oumouhou N, Walschaerts M, Leconte E, et al. DNA replication stress response involving PLK1, CDC6, POLQ, RAD51 and CLASPIN upregulation prognoses the outcome of early/mid-stage non-small cell lung cancer patients. Oncogenesis. (2012) 1:e30. doi: 10.1038/oncsis.2012.29
17. Shinmura K, Kato H, Kawanishi Y, Yoshimura K, Tsuchiya K, Takahara Y, et al. POLQ overexpression is associated with an increased somatic mutation load and PLK4 overexpression in lung adenocarcinoma. Cancers (Basel). (2019) 11:722. doi: 10.3390/cancers11050722
18. Rao X, Xing B, Wu Z, Bin Y, Chen Y, Xu Y, et al. Targeting polymerase θ impairs tumorigenesis and enhances radiosensitivity in lung adenocarcinoma. Cancer Sci. (2023) 114:1943–57. doi: 10.1111/cas.v114.5
19. Pan Q, Wang L, Liu Y, Li M, Zhang Y, Peng W, et al. Knockdown of POLQ interferes the development and progression of hepatocellular carcinoma through regulating cell proliferation, apoptosis and migration. Cancer Cell Int. (2021) 21:482. doi: 10.1186/s12935-021-02178-2
20. Li J, Ko JM, Dai W, Yu VZ, Ng HY, Hoffmann JS, et al. Depletion of DNA Polymerase Theta Inhibits Tumor Growth and Promotes Genome Instability through the cGAS-STING-ISG Pathway in Esophageal Squamous Cell Carcinoma. Cancers (Basel). (2021) 13:3204. doi: 10.3390/cancers13133204
21. Lessa RC, Campos AH, Freitas CE, Silva FR, Kowalski LP, Carvalho AL, et al. Identification of upregulated genes in oral squamous cell carcinomas. Head Neck. (2013) 35:1475–81. doi: 10.1002/hed.v35.10
22. Smolinska A, Singer K, Golchert J, Smyczynska U, Fendler W, Sendler M, et al. DNA polymerase theta plays a critical role in pancreatic cancer development and metastasis. Cancers (Basel). (2022) 14:4077. doi: 10.3390/cancers14174077
23. Liu G, Jin K, Liu Z, Su X, Xu Z, Li B, et al. POLQ identifies a better response subset to immunotherapy in muscle-invasive bladder cancer with high PD-L1. Cancer Med. (2024) 13:e6962. doi: 10.1002/cam4.v13.4
24. Oh G, Wang A, Wang L, Li J, Werba G, Weissinger D, et al. POLQ inhibition elicits an immune response in homologous recombination-deficient pancreatic adenocarcinoma via cGAS/STING signaling. J Clin Invest. (2023) 133:e165934. doi: 10.1172/JCI165934
25. Tang Z, Li C, Kang B, Gao G, Zhang Z. GEPIA: a web server for cancer and normal gene expression profiling and interactive analyses. Nucleic Acids Res. (2017) 45:W98–W102. doi: 10.1093/nar/gkx247
26. Kawamura K, Bahar R, Seimiya M, Chiyo M, Wada A, Okada S, et al. DNA polymerase theta is preferentially expressed in lymphoid tissues and upregulated in human cancers. Int J Cancer. (2004) 109:9–16. doi: 10.1002/ijc.v109:1
27. Schaub JM, Soniat MM, Finkelstein IJ. Polymerase theta-helicase promotes end joining by stripping single-stranded DNA-binding proteins and bridging DNA ends. Nucleic Acids Res. (2022) 50:3911–21. doi: 10.1093/nar/gkac119
28. Kent T, Mateos-Gomez PA, Sfeir A, Pomerantz RT. Polymerase θ is a robust terminal transferase that oscillates between three different mechanisms during end-joining. Elife. (2016) 5:e13740. doi: 10.7554/eLife.13740
29. Goullet de Rugy T, Bashkurov M, Datti A, Betous R, Guitton-Sert L, Cazaux C, et al. Excess Polθ functions in response to replicative stress in homologous recombination-proficient cancer cells. Biol Open. (2016) 5:1485–92. doi: 10.1242/bio.018028
30. Feng W, Simpson DA, Carvajal-Garcia J, Price BA, Kumar RJ, Mose LE, et al. Genetic determinants of cellular addiction to DNA polymerase theta. Nat Commun. (2019) 10:4286. doi: 10.1038/s41467-019-12234-1
31. Brambati A, Barry RM, Sfeir A. DNA polymerase theta (Polθ) - an error-prone polymerase necessary for genome stability. Curr Opin Genet Dev. (2020) 60:119–26. doi: 10.1016/j.gde.2020.02.017
32. Bubenik M, Mader P, Mochirian P, Vallée F, Clark J, Truchon JF, et al. Identification of RP-6685, an orally bioavailable compound that inhibits the DNA polymerase activity of polθ. J Med Chem. (2022) 65:13198–215. doi: 10.1021/acs.jmedchem.2c00998
33. Zatreanu D, Robinson HMR, Alkhatib O, Boursier M, Finch H, Geo L, et al. Polθ inhibitors elicit BRCA-gene synthetic lethality and target PARP inhibitor resistance. Nat Commun. (2021) 12:3636. doi: 10.1038/s41467-021-23463-8
34. Zhou J, Gelot C, Pantelidou C, Li A, Yücel H, Davis RE, et al. A first-in-class Polymerase Theta Inhibitor selectively targets Homologous-Recombination-Deficient Tumors. Nat Cancer. (2021) 2:598–610. doi: 10.1038/s43018-021-00203-x
35. Earl J, Galindo-Pumariño C, Encinas J, Barreto E, Castillo ME, Pachón V, et al. A comprehensive analysis of candidate genes in familial pancreatic cancer families reveals a high frequency of potentially pathogenic germline variants. EBioMedicine. (2020) 53:102675. doi: 10.1016/j.ebiom.2020.102675
36. Slater EP, Wilke LM, Böhm LB, Strauch K, Lutz M, Gercke N, et al. Combinations of low-frequency genetic variants might predispose to familial pancreatic cancer. J Pers Med. (2021) 11:631. doi: 10.3390/jpm11070631
37. Gkountakos A, Mafficini A, Lou E, Malleo G, Salvia R, Calicchia M, et al. Genomic characterization of undifferentiated sarcomatoid carcinoma of the pancreas. Hum Pathol. (2022) 128:124–33. doi: 10.1016/j.humpath.2022.07.011
Keywords: POLQ, pancreatic carcinoma, immunostaining, overall survival, prognostic factor
Citation: del Puerto-Nevado L, Fernández-Aceñero MJ, Cebrián A, Fatych Y, Díez-Valladares LI, Pérez-Aguirre E, de la Serna S, García-Botella A, Martínez-Useros J, García-Foncillas J and Mateos-Gómez PA (2024) POLQ immunostaining behaves as a prognostic factor for pancreatic carcinoma. Front. Oncol. 14:1433179. doi: 10.3389/fonc.2024.1433179
Received: 15 May 2024; Accepted: 16 September 2024;
Published: 07 October 2024.
Edited by:
Sumeet Nayak, KSQ Therapeutics, United StatesReviewed by:
Chinnadurai Mani, Texas Tech University Health Sciences Center, United StatesCopyright © 2024 del Puerto-Nevado, Fernández-Aceñero, Cebrián, Fatych, Díez-Valladares, Pérez-Aguirre, de la Serna, García-Botella, Martínez-Useros, García-Foncillas and Mateos-Gómez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro A. Mateos-Gómez, cGVkcm9hbnRvbmlvLm1hdGVvc0B1YWguZXM=; Laura del Puerto-Nevado, bHB1ZXJ0b0BvbmNvaGVhbHRoLmV1
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.