 İvo Gökmen1*†
İvo Gökmen1*† Nazan Demir2†Pınar Peker3†Erkan Özcan1†Fahri Akgül1†İsmail Bayrakçı1†Didem Divriklioğlu1†
Nazan Demir2†Pınar Peker3†Erkan Özcan1†Fahri Akgül1†İsmail Bayrakçı1†Didem Divriklioğlu1† Bülent Erdoğan1†
Bülent Erdoğan1† Sernaz Topaloğlu1†Muhammet Bekir Hacıoğlu1†
Sernaz Topaloğlu1†Muhammet Bekir Hacıoğlu1†- 1Division of Medical Oncology, Department of Internal Medicine, Trakya University School of Medicine, Edirne, Türkiye
- 2Department of Medical Oncology, Sultan I. Murat Public Hospital, Edirne, Türkiye
- 3Division of Medical Oncology, Department of Internal Medicine, Ege University School of Medicine, Izmir, Türkiye
Objective: The aim of our study was to assess the impact of the combination of HALP score with TTCR score on OS and PFS in PC patients who developed castration resistance.
Patients and methods: The study enrolled 152 patients with metastatic disease who had received either ARTAs or docetaxel as first-line treatment. The median cut-off was 30.83 months for the HALP score and 16.1 months for TTCR determined by ROC analysis. Based on these cut-off values, patients were categorized into low-high HALP score and TTCR <16.1 months-TTCR ≥16.1 months groups. The combination of HALP score and TTCR was then stratified by risk into three new groups: Factor 0, Factor 1, and Factor 2.
Results: PFS was significantly shorter in the TTCR <16.1 months group compared to the TTCR ≥16.1 months group, as well as in the low-HALP score group compared to the high-HALP score group. Furthermore, as the number of factors increased, a significant increase in OS and PFS was observed in the groups formed by the combination of HALP score and TTCR.
Conclusion: We have validated the predictive capability of combining low HALP score (<30.38) and short TTCR (<16.1 months) parameters in estimating the OS and PFS durations of mCRPC patients, both recognized as unfavorable prognostic indicators.
1 Introduction
Prostate cancer (PC) stands as the most prevalent solid organ tumor among males and ranks as the second leading cause of cancer-related mortality in this demographic (1). Upon diagnosis, approximately 78% of patients present with early-stage disease confined to the prostate capsule, while 12% exhibit regional lymph node metastases and 6% showcase distant metastases. Nevertheless, a majority of patients progress to develop distant metastases over time (2).
Current guidelines now state that monotherapy with androgen deprivation therapy (ADT) is no longer the standard initial treatment for hormone-sensitive prostate cancer (mHSPC) and should not be favored (3, 4). However, in countries where the use of androgen receptor-targeting agents (ARTAs) is restricted due to reimbursement limitations by public health insurance systems, many patients still receive ADT monotherapy. Although initial response rates to ADT range from 80% to 90%, treatment response is often transient, and cancer progression occurs in a significant number of patients within 6 months to several years, leading to metastatic castration-resistant prostate cancer (mCRPC), which is fatal (5, 6). In this population, docetaxel or ARTAs (abiraterone acetate or enzalutamide) may be considered as first-line treatment alongside ADT. Estimated survival ranges from 13.2 to 23.2 months, although some patients may respond favorably to these treatments (7).
mCRPC is a heterogeneous disease with variable characteristics and prognosis, representing a large patient population. The classification of these patients relies on common indicators such as prostate-specific antigen (PSA), alkaline phosphatase (ALP), lactate dehydrogenase (LDH), Eastern Cooperative Oncology Group erformance status (ECOG PS), Gleason score (GS), and tumor size (T), nodal involvement (N), and metastasis (M) stage (TNM stage) (8, 9). Unfortunately, these indicators have limited prognostic accuracy. Clinicians still require novel prognostic patterns and biomarkers to aid in the classification and management of these patients. Some prognostic indices based on inflammation and/or nutritional scores, such as the neutrophil-lymphocyte ratio (NLR) (10), platelet-lymphocyte ratio (PLR) (11), C-reactive protein/albumin ratio (CAR) (12), hemoglobin (HGB) level (13), and prognostic nutritional index (PNI) (14), have previously been utilized to predict the prognosis of patients with mCRPC who develop castration resistance following ADT treatment. Combinations of these parameters are known to provide better predictions of disease prognosis compared to single indices.
In this context, the HALP score—based on HGB, albumin, lymphocyte, and platelet levels—has recently emerged as a marker that evaluates both immune and nutritional status. Many studies have reported the HALP score’s utility as a reliable prognostic index in various types of cancer (15–22). However, data on PC patients are limited (23, 24), and to our knowledge, no study has yet evaluated the HALP score in mCRPC patients.
Given the importance of identifying reliable prognostic markers in prostate cancer, particularly in advanced stages, research has shown that a shorter time to castration resistance (TTCR) is linked to poorer overall survival (OS) in PC patients, both after diagnosis and after developing castration resistance (25–27). Wenzel et al. (27) suggested that the duration of treatment response before castration resistance is influenced by both patient and tumor characteristics. They further hypothesized that genetic mutations or alterations in the host or tumor may also contribute.
A previous study has shown that the combination of the CAR and TTCR can be used as a prognostic marker in mCRPC patients (12). In our study, we investigated the prognostic value of the HALP score and TTCR in mCRPC patients who developed resistance after ADT treatment. We aimed to determine whether their combination could be utilized to predict prognosis more accurately than current methods.
2 Materials and methods
2.1 Data collection, assessments, and follow-up
We adhered to the ethical standards of institutional and national research committees, as well as the 1964 Declaration of Helsinki and its subsequent revisions. The method and procedure of the study were approved by the Ethics Committee of Trakya University Faculty of Medicine (protocol code TÜTF-GOBAEK 2023/362) on October 9, 2023.
Patients histopathologically diagnosed with prostate adenocarcinoma in our medical oncology department between January 2010 and September 2023, who had previously failed ADT, were retrospectively reviewed. A total of 152 patients were enrolled, receiving docetaxel or ARTAs such as their primary treatment, with metastatic disease at the time of castration resistance development. Treatment decisions were made based on disease progression, toxicity, patient rejection of treatment, and physician preference. PSA levels at diagnosis of GS, mHSPC, and mCRPC, along with age before initial treatment for mCRPC, ECOG PS, and patient demographics, were recorded. In mCRPC patients, laboratory parameters including HGB, lymphocyte count, platelet count, serum albumin, ALP, and LDH levels were recorded if obtained within 2 weeks before the initiation of treatment. Lymphocyte and platelet counts, as well as serum HGB and albumin levels, were retrieved from the laboratory information system to calculate the HALP score. The HALP score was calculated using the following formula: [HGB (g/L) × albumin (g/L) × lymphocytes (/L)]/platelets (/L). Patients with factors that could potentially affect inflammatory parameters (e.g., active infection, inadequate organ function, or those receiving anti-inflammatory treatment) were excluded from the analysis.
The clinical stage was determined using standardized TNM criteria based on digital rectal examination, computed tomography, magnetic resonance imaging, and bone scintigraphy. Risk stratification was based on the criteria utilized in the CHAARTED and LATITUDE trials at the time of mCRPC diagnosis. Patients demonstrating evidence of disease progression (e.g., increased PSA levels, new metastases, or progression of existing metastases) with castrate serum testosterone levels (<50 ng/dl or <1.7 nmol/l) were classified as having developed mCRPC. TTCR was defined as the duration from the initiation of ADT treatment in mHSPC patients to the first reported date of mCRPC. This duration reflects the time it takes for the disease to develop resistance to ADT therapy. Regarding PSA progression, three consecutive increases of 50% or more in nadir PSA (2.0 ng/ml) were considered as a reference. Disease progression was determined by an increase in the number or size of lesions assessable according to the Response Evaluation Criteria in Solid Tumors 1.1 (RECIST 1.1) or the presence of new lesions on imaging studies.
The primary and secondary endpoints of the study were OS and progression-free survival (PFS) after the development of mCRPC, respectively. OS was defined as the duration from the diagnosis of mCRPC until the patient’s death or the final visit. PFS was calculated from the initiation of the first treatment for mCRPC until the last day of the study or evidence of progressive disease.
2.2 Statistical analyses
All analyses were conducted using the IBM (International Business Machines) SPSS (Statistical Package for the Social Sciences) Statistics for Windows, Version 27.0 (Armonk, N.Y., USA) and MedCalc Statistical Software Ltd. (Ostend, Belgium; https://www.medcalc.org; 2020). Receiver operating characteristic (ROC) curve analysis was utilized to plot the curves for the HALP score and TTCR. Subsequently, sensitivity and specificity values were transferred to Microsoft Excel, where the cut-off value was determined as the point at which the sensitivity and specificity values reached the highest total score. The cohort was stratified into three groups based on HALP score and TTCR, and differences between them were analyzed using ANOVA or chi-square tests. The Kruskal-Wallis test was employed to assess continuous variables without a normal distribution across groups. Survival curves were constructed using the Kaplan-Meier method, and differences were analyzed using the log-rank test. Univariate and multivariate analyses for OS were performed using the Cox proportional hazards regression model. All tests were two-sided, with differences considered statistically significant if the p-value was less than 0.05.
3 Results
3.1 Patient characteristics
In our study, the median age of the 152 patients was 70 years (range: 53-82 years). Among them, 52 patients (34.2%) had a pre-treatment ECOG PS of 0, while the remaining 100 patients (65.8%) had a ECOG PS of 1 or 2. The mean pre-treatment levels of HGB, albumin, lymphocytes, and platelets were 12.8 g/dL, 4.4 g/dL, 1.4 × 10^3/μL, and 225 × 10^3/mm^3, respectively, with a mean HALP score of 30.83 (range: 1.95-82.24). Among the patients, 109 (71.1%) met the CHAARTED criteria for high-volume disease, while 92 (60.5%) met the LATITUDE criteria for high-risk disease. Distant metastases were most commonly observed in the bone (n=123, 80.9%), with visceral metastases detected in 49 patients (32.2%). The median TTCR was 14.4 months (range: 4.3-53.7 months). Docetaxel was administered as the first-line treatment for mCRPC in 94 patients (61.8%), while ARTAs were used in 58 patients (38.2%). Throughout the observation period of the study, 146 patients (96.1%) received ARTAs, and 140 patients (92.1%) underwent docetaxel therapy (see Table 1).
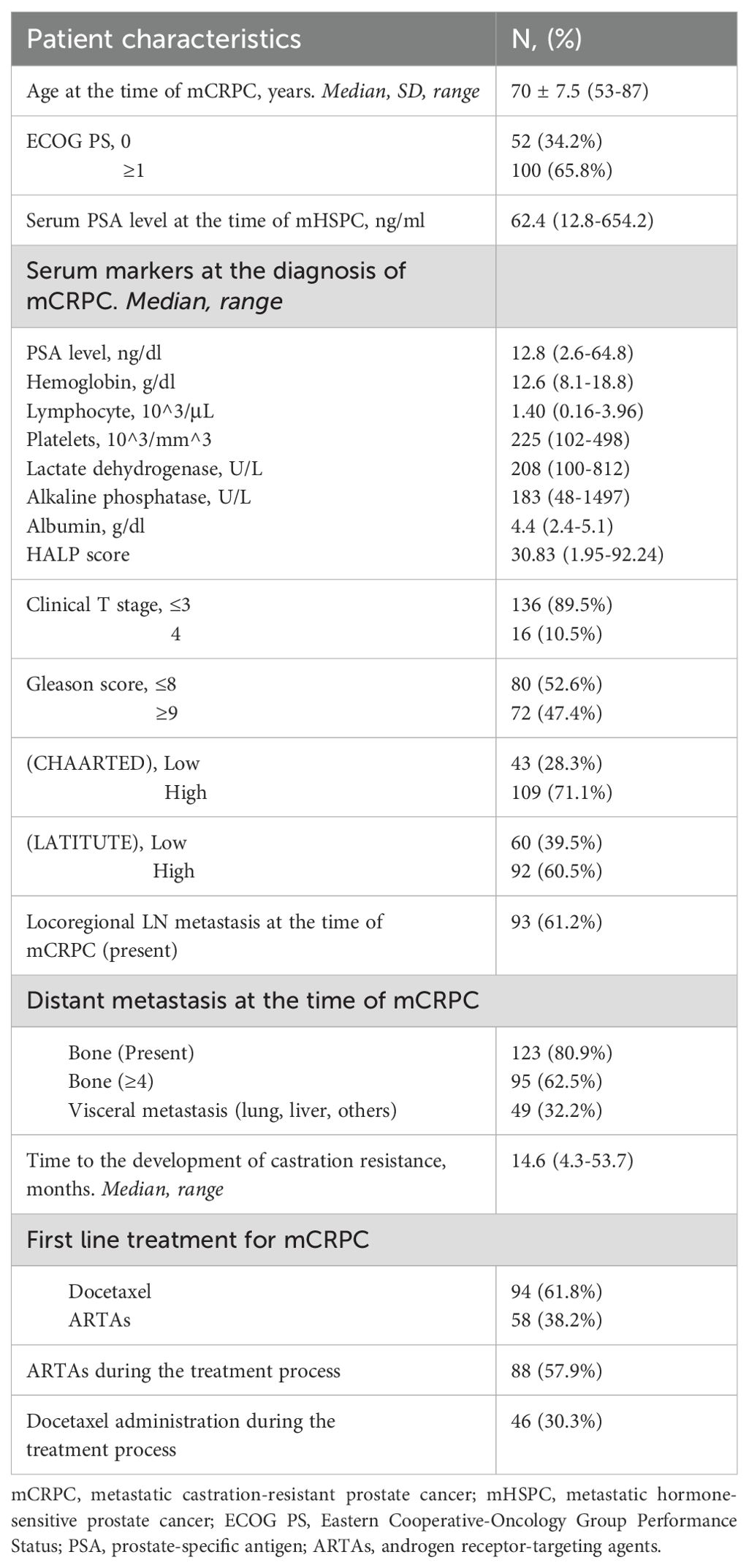
Table 1. Clinicopathological characteristics and treatment data of 152 patients diagnosed with mCRPC.
3.2 Evaluation of the HALP score and TTCR as prognostic factors
We examined the optimal cut-off points for both the HALP score and TTCR in predicting mortality in mCRPC. The optimal cut-off point for mortality prediction, as determined by ROC curve analysis, was ≥32.13 months for the HALP score (area under the curve 0.712, sensitivity 66.18%, and specificity 61.77%) and ≥16.1 months for TTCR (area under the curve 0.732, sensitivity 62.71%, and specificity 61.77%). When comparing these values with the cut-off points determined by the median using Cox analysis, the results indicated that the hazard ratio (HR) was superior to the median cut-off for TTCR but not for the HALP score (see Figure 1).
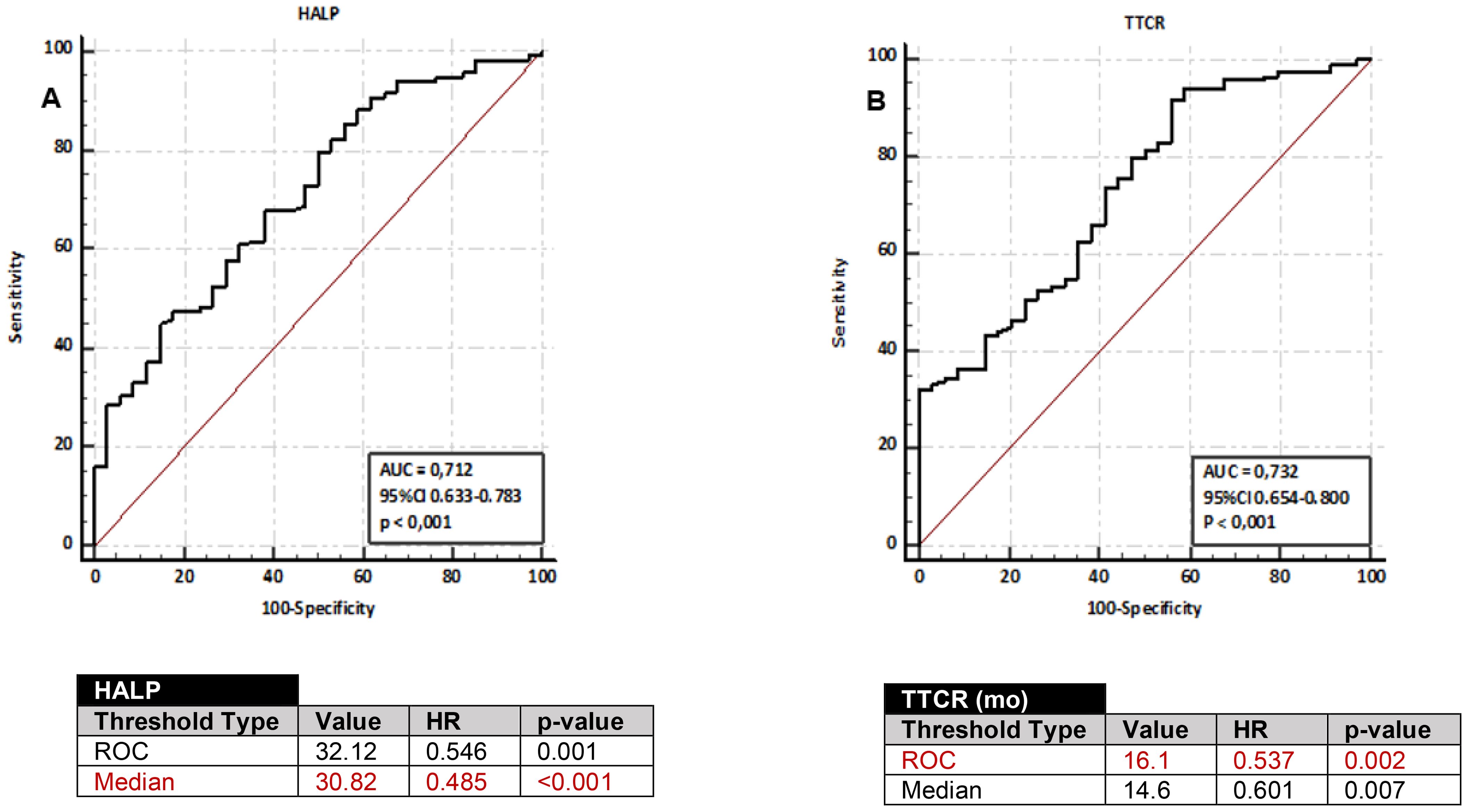
Figure 1. ROC curves for predicting overall survival in mCRPC patients using HALP score (A) and TTCR (B). Cut-off values derived from ROC analysis and median-based cut-offs, along with performance metrics (HR and p-values) for OS, obtained through Cox regression analysis, are displayed in the accompanying tables.
Based on this data analysis, the median cut-off value was utilized for the HALP score. Patients were categorized into two groups: a low HALP score group (<30.83, n=77) and a high HALP score group (≥30.83, n=75). The cut-off value from the ROC analysis was applied for TTCR, and patients were categorized into two groups: TTCR≥16.1 months (n=70) and TTCR<16 months (n=82). Kaplan-Meier analysis revealed that the low HALP score group had significantly inferior OS compared to the high HALP score group (median 19.8 months (95%CI 16.1-23.4) vs. 33.3 months (95%CI 27.9-38.7), p<0.001). Similarly, the TTCR<16.1 months group exhibited worse OS compared to the TTCR≥16.1 months group (median 23.5 months (95%CI 19.2-26.8) vs. 36.8 months (95%CI 30.1-43.6), p=0.002). Moreover, PFS was notably shorter in the low HALP score group compared to the high HALP score group and in the TTCR<16.1 months group compared to the TTCR≥16 months group (p=0.017, p=0.018, respectively) (see Figure 2).
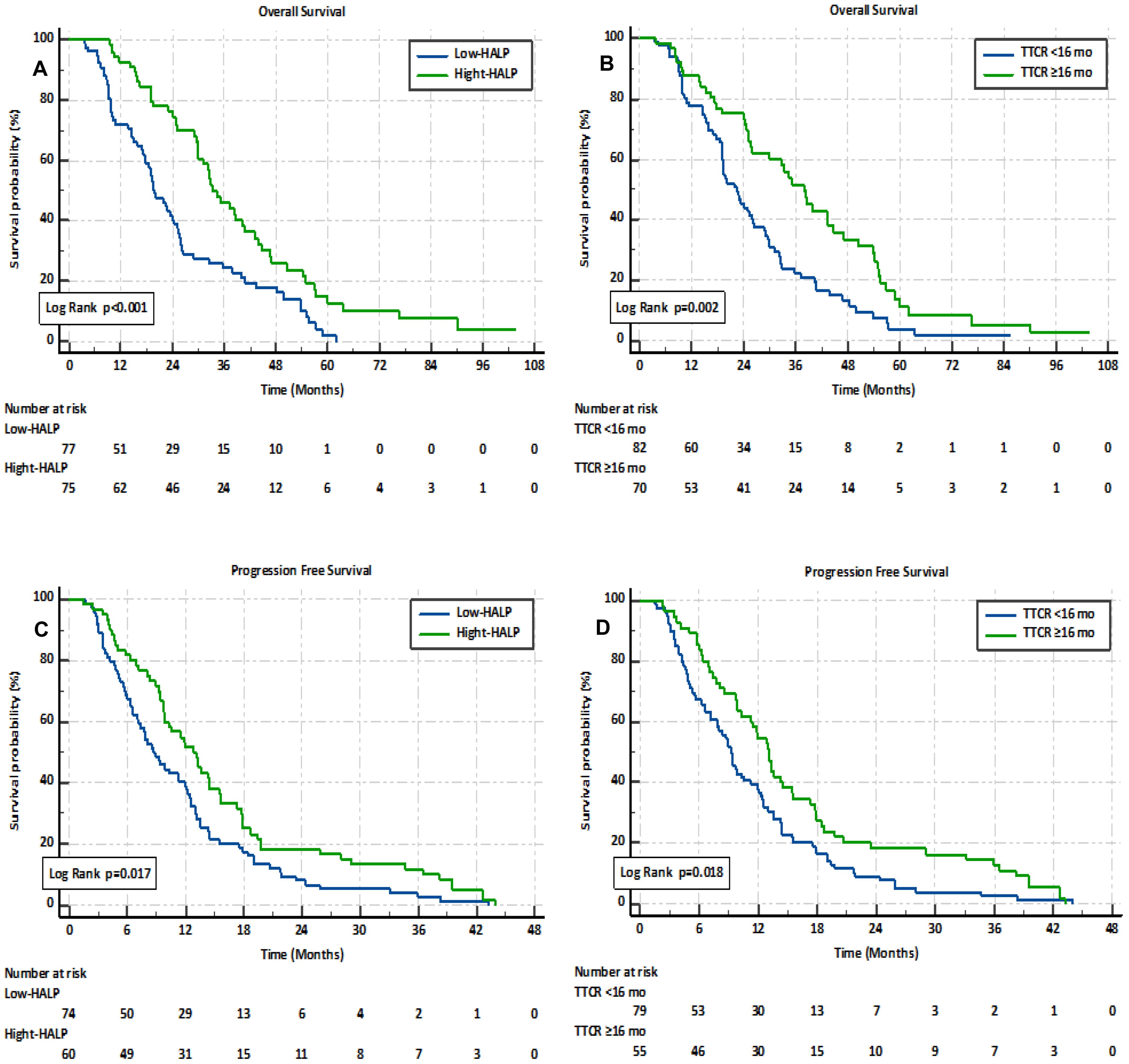
Figure 2. Kaplan–Meier analysis of overall survival and progression-free survival in mCRPC patients, stratified by HALP score (A, C) and TTCR (B, D).
Univariate and multivariate Cox analyses were conducted to further explore the prognostic significance of the HALP score and TTCR. The univariate analysis revealed that both the HALP score (HR 0.485, 95% CI 0.334-0.706, p<0.001) and TTCR (HR 0.537, 95% CI 0.369-0.784, p=0.002) were significantly associated with OS. Similarly, factors such as age ≥75 years, ECOG PS ≥1, HGB ≥12.8 g/dl, lymphocyte count ≥1.40 x 10^3/μL, high-volume disease, high-risk disease, bone metastases, and visceral metastases were identified as potential prognostic factors significantly correlated with OS. Although not statistically significant, albumin ≥4.1 g/dl and ALP ≥183 U/L were considered potential prognostic factors for OS (see Table 2). Additionally, both the HALP score (HR 0.499, 95% CI 0.338-0.737, p=0.001) and TTCR (HR 0.643, 95% CI 0.436-0.948, p=0.026) consistently demonstrated independent prognostic value for OS in multivariate analysis, controlling for uncorrelated prognostic factors including age, ECOG PS, ALP, high-risk disease, HALP score, and TTCR.
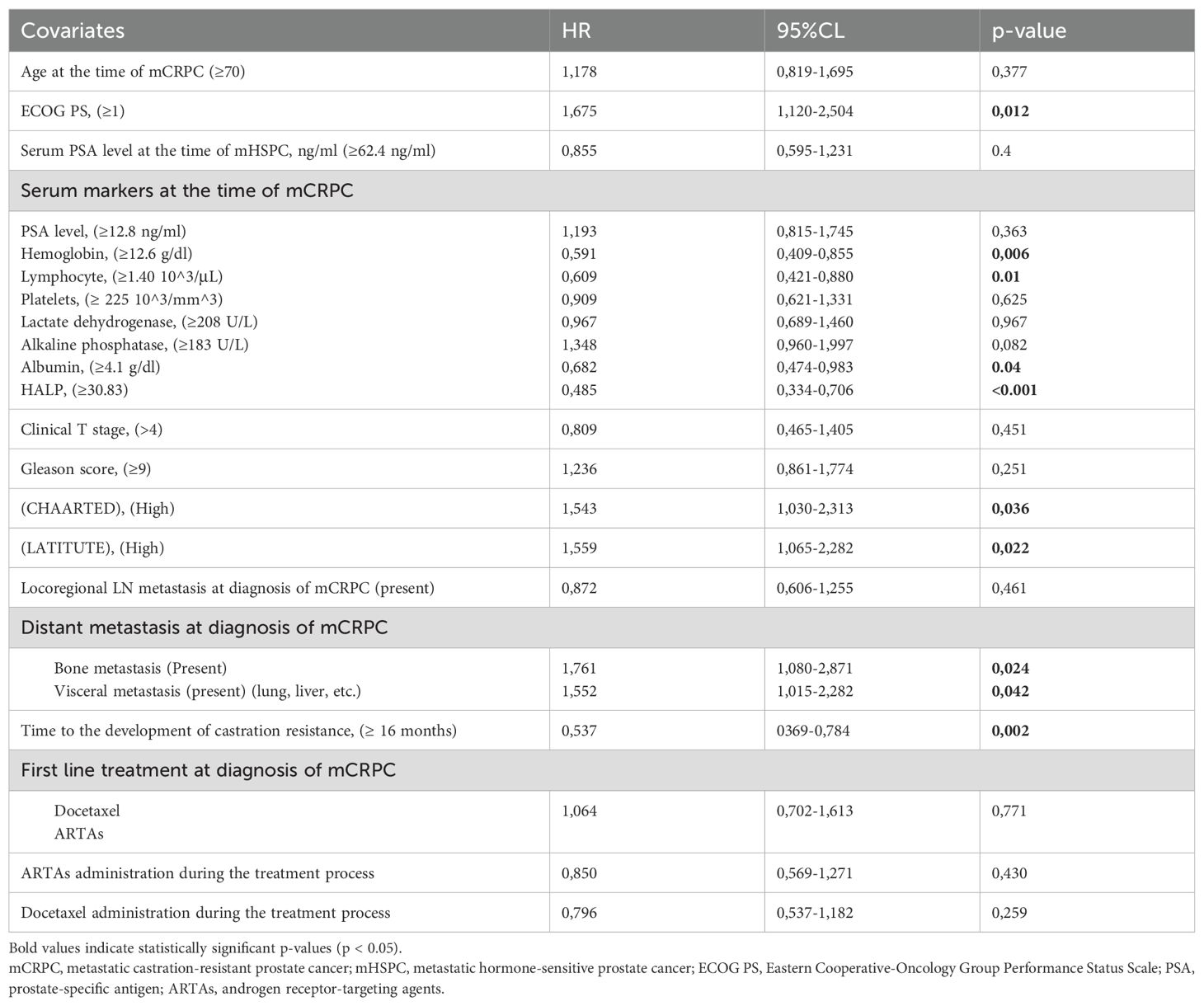
Table 2. Univariate Cox proportional hazards analysis of factors affecting overall survival in patients with mCRPC.
3.3 Evaluation of the combination between the HALP score and TTCR
We assessed whether combining the HALP score and TTCR could enhance accuracy in predicting patient prognosis. The study population was divided into three groups based on this new combination. The factor 0 “0F” group comprised patients with a low HALP score and TTCR<16.1 months; the factor 1 “1F” group included those with a high HALP score and TTCR<16.1 months, or a low HALP score and TTCR≥16.1 months; and the factor 2 “2F” group consisted of patients with a high HALP score and TTCR≥16.1 months. By combining the HALP score and TTCR, there was a significant gradual increase in both OS (0F: median 19.5 months (95% CI 17.8-21); 1F: 25.4 (95% CI 19.2-31.7); 2F: 43.2 (95% CI 33.7-52.6); p<0.001) and PFS (p=0.007) as the number of factors increased (see Figure 3). Significant differences were observed between the groups in various blood markers, including HGB, lymphocytes, platelets, and albumin. The presence of bone metastases, visceral metastases, high-risk disease, and an ECOG PS of 0 were also found to have an inverse correlation with the number of available factors (see Table 3).
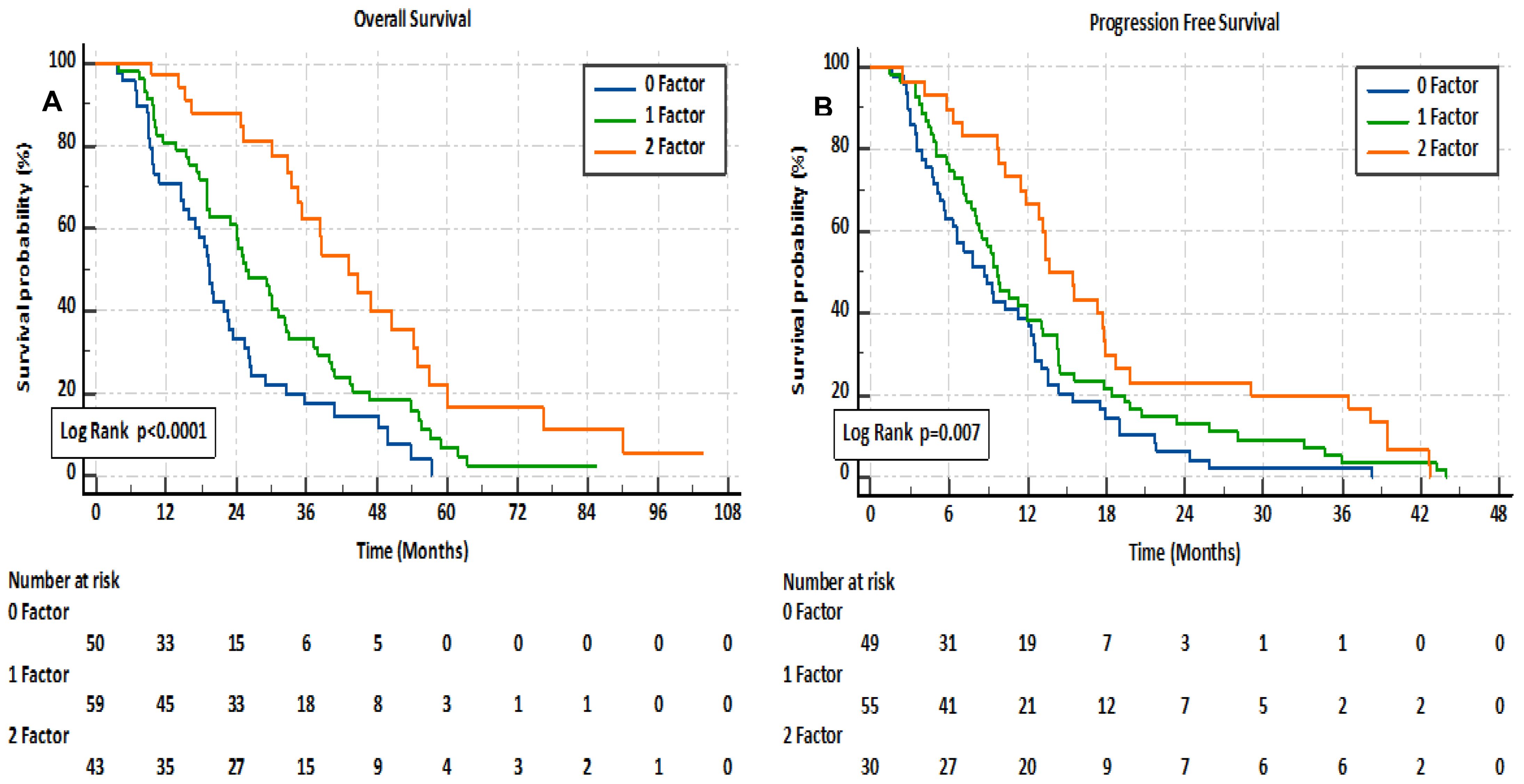
Figure 3. Kaplan–Meier analysis of overall survival (A) and progression-free survival (B) in mCRPC patients, based on a combination of HALP score and TTCR.
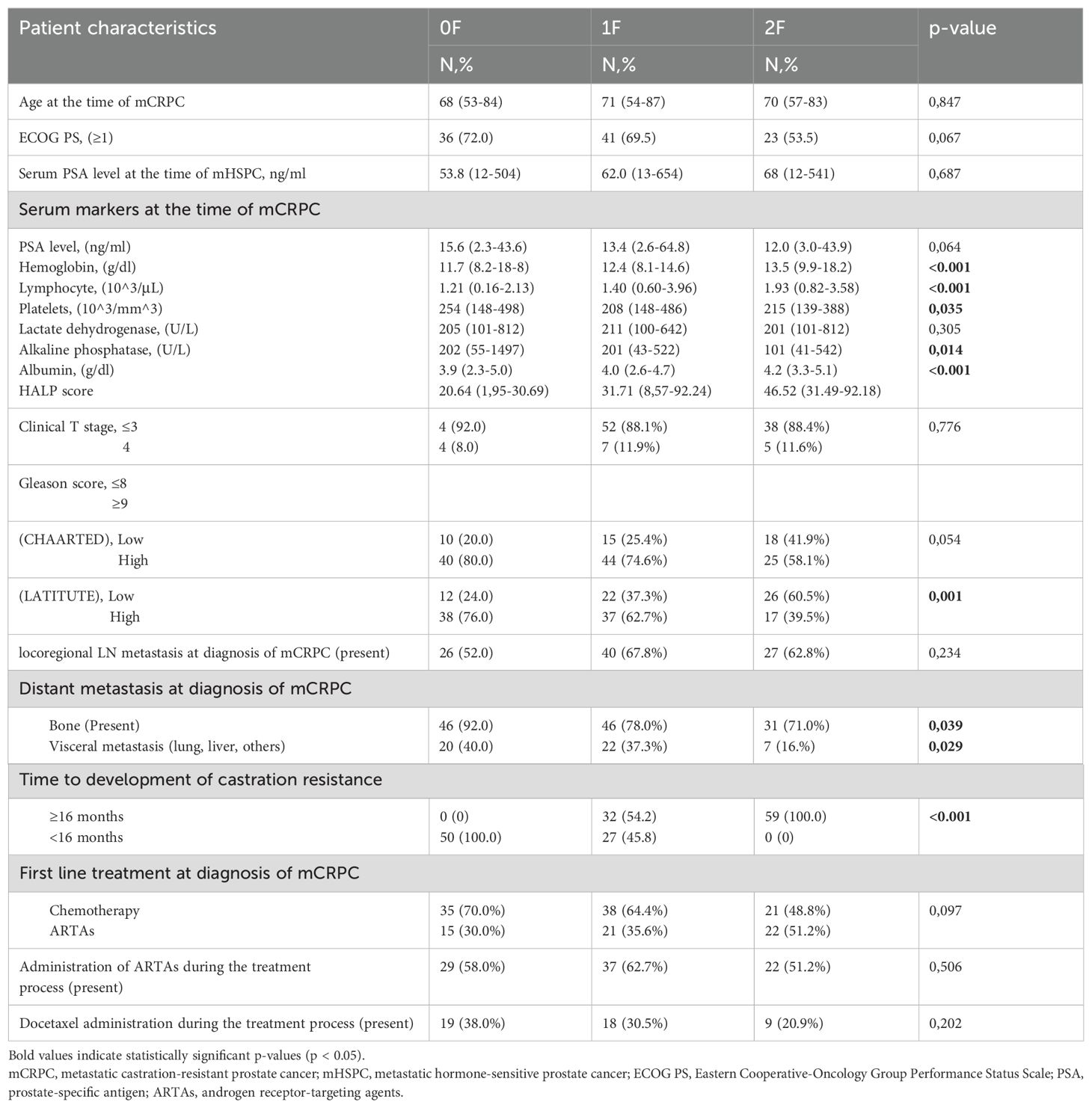
Table 3. Clinicopathologic characteristics of mCRPC patients stratified into three groups based on HALP score and TTCR.
4 Discussion
In our study, we aimed to investigate the prognostic value of pre-treatment HALP score, TTCR, and their combination in predicting both OS and PFS in patients diagnosed with mCRPC who developed resistance following ADT and were subsequently treated with ARTAs or docetaxel as first-line therapy. This retrospective analysis focused on patients treated at our clinic after developing castration resistance. The key findings are detailed below.
Recent advances in the treatment of mCRPC with new therapeutic options have underscored the increased need for predictive and prognostic markers to inform individualized treatment selection. In recent years, there has been a growing number of studies focusing on the roles of inflammatory response and nutritional status in predicting prognosis in mCRPC (10, 11, 14, 28, 29). These factors may reflect the onset and progression of cancer, indirectly forecast response to anti-tumor therapy, and determine survival duration in clinical practice (30). Serum albumin, a negative acute-phase marker synthesized in the liver, serves as an indicator of nutritional status. Hypoalbuminemia, which frequently occurs in cancer patients, may be linked to compromised oral intake and catabolic processes, as well as systemic inflammation and heightened cytokine release. Consequently, this may weaken the immune response against cancer cells (31). Numerous studies have highlighted that hypoalbuminemia in mCRPC is associated with shorter survival outcomes (32, 33).
Lymphocytes play a crucial role in the immune system. They can secrete cytokines such as interferon-γ and tumor necrosis factor-alpha (TNF-α), which may enhance prognosis by inducing apoptosis and suppressing cancer cell proliferation, invasion, and migration (34, 35). In summary, lymphocytopenia may contribute to tumor growth. Several studies have demonstrated a direct relationship between HGB levels and both survival and tumor development in cancer patients (36, 37). Platelets are pivotal in the metastatic potential of tumor cells, with tumor cell-induced platelet aggregation (TCIPA) being associated with high metastatic potential across various cancer types. Additionally, platelets may shield tumor cells from immune attack. They can also facilitate tumor angiogenesis through vascular endothelial growth factor (VEGF) and other inflammatory mediators, while inhibiting tumor necrosis via TNF-α (38, 39).
In light of these data, the HALP score, derived from HGB, albumin, lymphocyte, and platelet values, may be regarded as a comprehensive index measuring the nutritional status and immune health of patients. In 2015, Chen et al. initially reported that a higher pre-operative HALP score (cut-off value of 58.8) was associated with improved survival outcomes in gastric cancer patients (15). Shortly thereafter, Jiang et al. identified a higher mortality risk in locally advanced colorectal cancer patients with a low pre-operative HALP score (cut-off value of 26.5) (16). Subsequent studies have confirmed the HALP score as a useful prognostic tool for predicting the prognosis of patients with various cancer types, including pancreatic and biliary tract cancer (17, 18), lung cancer (19, 20), and urologic cancers such as renal cell carcinoma (21, 22). To date, the HALP score has been investigated in two distinct studies within the context of PC, yielding differing results. In a 2019 study by Guo et al. the pre-operative HALP score was significantly correlated with PFS in both metastatic and oligometastatic PC subgroups in patients undergoing cytoreductive radical prostatectomy for PC (23). Subsequently, a study conducted by Kaya et al. in 2020 explored the pre-operative diagnostic significance of the HALP score in patients with PC but found no correlation (24). To our knowledge, there have been no previously reported studies on the prognostic significance of the HALP score in patients with mCRPC.
Nearly all previous studies have utilized X-tile or ROC curves to determine the cut-off value of the HALP score, which predominantly fell between 15.5 and 56.8 (40). There is no evidence indicating a correlation between the HALP score cut-off and tumor type. A single, fixed value may not represent the optimal threshold across all tumor types. In our study, the median cut-off value (30.83) was employed for the HALP score. Kaplan-Meier survival analysis confirmed a significant disparity in OS between the high and low HALP score groups. Patients with a high pre-treatment HALP score (≥30.83) exhibited a median OS of 33.3 months, whereas those with a low HALP score (<30.83) experienced a notably shorter OS of 19.8 months (p<0.001). This significance was also evident for PFS. The HALP score maintained its independent prognostic value for OS in both univariate analysis (HR 0.485, 95% CI 0.334-0.706, p<0.001) and multivariate analysis encompassing various patient and tumor factors (HR 0.499, 95% CI 0.338-0.737, p=0.001). These findings highlight that improvements in the HALP score could greatly improve survival outcomes in mCRPC patients.
The cut-off value for TTCR from the ROC analysis (16.1 months) was used in our study. TTCR was also confirmed to be an independent predictor for OS in mCRPC in both univariate and multivariate analyses. Patients with TTCR ≥16.1 months had a mean OS of 36.8 months, whereas those with TTCR <16.1 months had a significantly shorter OS (23.3 months). This trend was also observed for PFS. Many studies have used a 12-month cut-off as the optimal threshold for TTCR in patients treated with ADT during the mHSPC period who subsequently developed castration resistance. Miyake et al. in their study stratifying TTCR, found that those with a TTCR of ≤6 months had the worst prognosis (25, 26, 41). Additionally, it has been demonstrated that short TTCR durations were strongly associated with poor prognosis following the development of mCRPC in patients undergoing combination therapy (ARTAs, docetaxel) with ADT during the mHSPC period (27).
Finally, this study confirmed that it is possible to predict both OS and PFS durations more accurately by categorizing mCRPC patients into three groups based on parameters defined as poor prognostic factors: low HALP score (<30.38) and short TTCR (<16.1 months). In the newly established prognostic model, a gradual increase in survival was observed for both OS (0F: median 19.5 months; 1F: 25.4 months; 2F: 43.2 months; p<0.001) and PFS (p=0.007) as the number of factors increased. Harrel’s 0.701 c-index value can be indicative of the combined score’s superior performance in distinguishing patients within the best prognostic group compared to the individual use of HALP score (c-index 0.641) and TTCR (c-index 0.639). These results are not surprising, as the combination of these factors incorporates variations in various host and tumor-related poor prognostic factors such as low ECOG PS, anemia, lymphopenia, hypoalbuminemia, high-risk disease, and metastasis.
This study has several limitations. Firstly, although it is the first study to demonstrate both the HALP score and the HALP score in combination with TTCR for OS as independent prognostic factors in patients with mCRPC, its retrospective design spanning 13 years and the potential for bias in patient selection reduce the study’s reliability. Secondly, the evaluation of patients treated at a single center and the small number of patients are limitations. The small sample size and the HALP score and TTCR cut-off values used may not be sufficient to reflect prognosis in other cohorts. Additionally, the results cannot be generalized to all mCRPC patients, as we did not focus on patients receiving combination therapy during a castration-sensitive phase. Finally, the failure to evaluate other potential prognostic markers such as NLR (10) and PLR (11), and PNI (14) is another limitation.
5 Conclusion
In conclusion, the HALP score emerges as a reliable, simple, easily accessible, and cost-effective index for predicting prognosis in mCRPC patients. A low HALP score may serve as a clinical indicator for implementing nutritional support in mCRPC patients. Moreover, the combined utilization of the HALP score and TTCR may enhance the accuracy of prognosis prediction in mCRPC patients. This approach is believed to effectively identify patients who could benefit from therapy. Multicenter studies involving larger cohorts are warranted to provide a more conclusive assessment.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Trakya University. (Protocol code TÜTF-GOBAEK 2023/362 and date of application 9 October 2023).
Author contributions
İG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing, Project administration. ND: Conceptualization, Writing – review & editing. PP: Conceptualization, Writing – review & editing. EÖ: Data curation, Writing – review & editing. FA: Data curation, Writing – review & editing. İB: Data curation, Writing – review & editing. DD: Data curation, Writing – review & editing. BE: Data curation, Writing – review & editing. ST: Writing – review & editing. MH: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763
2. SEER*Explorer:. an interactive website for SEER cancer statistics. Surveillance Res Program. (2021). https://seer.cancer.gov.
3. Schaeffer EM, Srinivas S, Adra N, An Y, Barocas D, Bitting R, et al. Prostate cancer, version 4.2023, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2023) 21:1067–96. doi: 10.6004/jnccn.2023.0050
4. Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer. Part II-2020 update: treatment of relapsing and metastatic prostate cancer. Eur Urol. (2021) 79:263–82. doi: 10.1016/j.eururo.2020.09.046
5. Annala M, Taavitsainen S, Khalaf DJ, Vandekerkhove G, Beja K, Sipola J, et al. Evolution of Castration-Resistant Prostate Cancer in ctDNA during Sequential Androgen Receptor Pathway Inhibition. Clin Cancer Res. (2021) 27:4610–23. doi: 10.1158/1078-0432.CCR-21-1625
6. Sumanasuriya S, Seed G, Parr H, Christova R, Pope L, Bertan C, et al. Elucidating prostate cancer behaviour during treatment via low-pass whole-genome sequencing of circulating tumour DNA. Eur Urol. (2021) 80:243–53. doi: 10.1016/j.eururo.2021.05.030
7. Aly M, Leval A, Schain F, Liwing J, Lawson J, Vágó E, et al. Survival in patients diagnosed with castration-resistant prostate cancer: a population-based observational study in Sweden. Scand J Urol. (2020) 54:115–21. doi: 10.1080/21681805.2020.1739139
8. Shariat SF, Semjonow A, Lilja H, Savage C, Vickers AJ, Bjartell A. Tumor markers in prostate cancer I: blood-based markers. Acta Oncol. (2011) 50 Suppl 1:61–75.
9. Čapoun O, Mikulová V, Jančíková M, Honová H, Kološtová K, Sobotka R, et al. Prognosis of castration-resistant prostate cancer patients - use of the adnaTest® System for detection of circulating tumor cells. Anticancer Res. (2016) 36:2019–26.
10. Meisel A, de Wit R, Oudard S, Sartor O, Stenner-Liewen F, Shun Z, et al. Neutropenia, neutrophilia, and neutrophil-lymphocyte ratio as prognostic markers in patients with metastatic castration-resistant prostate cancer. Ther Adv Med Oncol. (2022) 14:17588359221100022. doi: 10.1177/17588359221100022
11. Sciarra A, Gentilucci A, Cattarino S, Salsiccia S, Mariotti G. Prognostic role of platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in patients with metastatic castration resistant prostate cancer treated with abiraterone or enzalutamide. Minerva Urol Nephrol. (2021) 73:863–5.
12. Mitsui Y, Yamabe F, Hori S, Uetani M, Aoki H, Sakurabayashi K, et al. Combination of C-reactive protein/albumin ratio and time to castration resistance enhances prediction of prognosis for patients with metastatic castration-resistant prostate cancer. Front Oncol. (2023) 13:1162820. doi: 10.3389/fonc.2023.1162820
13. Dai D, Han S, Li L, Guo Y, Wei Y, Jin H, et al. Anemia is associated with poor outcomes of metastatic castration-resistant prostate cancer, a systematic review and meta-analysis. Am J Transl Res. (2018) 10:3877–86.
14. Zheng Y, Wang K, Ou Y, Hu X, Wang Z, Wang D, et al. Prognostic value of a baseline prognostic nutritional index for patients with prostate cancer: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. (2023). doi: 10.1038/s41391-023-00689-9
15. Chen XL, Xue L, Wang W, Chen HN, Zhang WH, Liu K, et al. Prognostic significance of the combination of preoperative hemoglobin, albumin, lymphocyte and platelet in patients with gastric carcinoma: a retrospective cohort study. Oncotarget. (2015) 6:41370–82. doi: 10.18632/oncotarget.v6i38
16. Jiang H, Li H, Li A, Tang E, Xu D, Chen Y, et al. Preoperative combined hemoglobin, albumin, lymphocyte and platelet levels predict survival in patients with locally advanced colorectal cancer. Oncotarget. (2016) 7:72076–83. doi: 10.18632/oncotarget.12271
17. Xu SS, Li S, Xu HX, Li H, Wu CT, Wang WQ, et al. Haemoglobin, albumin, lymphocyte and platelet predicts postoperative survival in pancreatic cancer. World J Gastroenterol. (2020) 26:828–38. doi: 10.3748/wjg.v26.i8.828
18. Sun L, Guan A, Jin Y, Liu M, Xiao Y, Xu H, et al. Comparison of prognostic value of red cell-related parameters of biliary tract cancer after surgical resection and integration of a prognostic nomogram: A retrospective study. Adv Ther. (2021) 38:1227–44. doi: 10.1007/s12325-020-01595-5
19. Shen XB, Zhang YX, Wang W, Pan YY. The hemoglobin, albumin, lymphocyte, and platelet (HALP) score in patients with small cell lung cancer before first-line treatment with etoposide and progression-free survival. Med Sci Monit. (2019) 25:5630–9. doi: 10.12659/MSM.917968
20. Zhai B, Chen J, Wu J, Yang L, Guo X, Shao J, et al. Predictive value of the hemoglobin, albumin, lymphocyte, and platelet (HALP) score and lymphocyte-to-monocyte ratio (LMR) in patients with non-small cell lung cancer after radical lung cancer surgery. Ann Transl Med. (2021) 9:976. doi: 10.21037/atm-21-2120
21. Peng D, Zhang CJ, Gong YQ, Hao H, Guan B, Li XS, et al. Prognostic significance of HALP (hemoglobin, albumin, lymphocyte and platelet) in patients with bladder cancer after radical cystectomy. Sci Rep. (2018) 8:794. doi: 10.1038/s41598-018-19146-y
22. Ekinci F, Balcik OY, Oktay E, Erdogan AP. HALP score as a new prognostic index in metastatic renal cell cancer. J Coll Physicians Surg Pak. (2022) 32:313–8. doi: 10.29271/jcpsp.2022.03.313
23. Guo Y, Shi D, Zhang J, Mao S, Wang L, Zhang W, et al. The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is a novel significant prognostic factor for patients with metastatic prostate cancer undergoing cytoreductive radical prostatectomy. J Cancer. (2019) 10:81–91. doi: 10.7150/jca.27210
24. Kaya C, Caliskan S, Sungur M, Aydın C. HALP score and albumin levels in men with prostate cancer and benign prostate hyperplasia. Int J Clin Pract. (2021) 75:e13766. doi: 10.1111/ijcp.13766
25. Uchimoto T, Komura K, Fujiwara Y, Saito K, Tanda N, Matsunaga T, et al. Prognostic impact of C-reactive protein-albumin ratio for the lethality in castration-resistant prostate cancer. Med Oncol. (2019) 37:9. doi: 10.1007/s12032-019-1332-7
26. Miyake H, Matsushita Y, Watanabe H, Tamura K, Motoyama D, Ito T, et al. Prognostic significance of time to castration resistance in patients with metastatic castration-sensitive prostate cancer. Anticancer Res. (2019) 39:1391–6. doi: 10.21873/anticanres.13253
27. Wenzel M, Preisser F, Hoeh B, Schroeder M, Würnschimmel C, Steuber T, et al. Impact of time to castration resistance on survival in metastatic hormone sensitive prostate cancer patients in the era of combination therapies. Front Oncol. (2021) 11:659135. doi: 10.3389/fonc.2021.659135
28. Stangl-Kremser J, Mari A, Suarez-Ibarrola R, D'Andrea D, Korn SM, Pones M, et al. Development of a prognostic model for survival time prediction in castration-resistant prostate cancer patients. Urol Oncol. (2020) 38:600.e9–.e15. doi: 10.1016/j.urolonc.2019.11.005
29. Yamada Y, Sakamoto S, Rii J, Yamamoto S, Kamada S, Imamura Y, et al. Prognostic value of an inflammatory index for patients with metastatic castration-resistant prostate cancer. Prostate. (2020) 80:559–69. doi: 10.1002/pros.23969
30. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. (2019) 51:27–41. doi: 10.1016/j.immuni.2019.06.025
31. Lucijanic M, Veletic I, Rahelic D, Pejsa V, Cicic D, Skelin M, et al. Assessing serum albumin concentration, lymphocyte count and prognostic nutritional index might improve prognostication in patients with myelofibrosis. Wien Klin Wochenschr. (2018) 130:126–33. doi: 10.1007/s00508-018-1318-z
32. Pei XQ, He DL, Tian G, Lv W, Jiang YM, Wu DP, et al. Prognostic factors of first-line docetaxel treatment in castration-resistant prostate cancer: roles of neutrophil-to-lymphocyte ratio in patients from Northwestern China. Int Urol Nephrol. (2017) 49:629–35. doi: 10.1007/s11255-017-1524-z
33. Linton A, Pond G, Clarke S, Vardy J, Galsky M, Sonpavde G. Glasgow prognostic score as a prognostic factor in metastatic castration-resistant prostate cancer treated with docetaxel-based chemotherapy. Clin Genitourin Cancer. (2013) 11:423–30. doi: 10.1016/j.clgc.2013.04.020
34. Lim JA, Oh CS, Yoon TG, Lee JY, Lee SH, Yoo YB, et al. The effect of propofol and sevoflurane on cancer cell, natural killer cell, and cytotoxic T lymphocyte function in patients undergoing breast cancer surgery: an in vitro analysis. BMC Cancer. (2018) 18:159. doi: 10.1186/s12885-018-4064-8
35. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. (2008) 454:436–44. doi: 10.1038/nature07205
36. Belcher DA, Ju JA, Baek JH, Yalamanoglu A, Buehler PW, Gilkes DM, et al. The quaternary state of polymerized human hemoglobin regulates oxygenation of breast cancer solid tumors: A theoretical and experimental study. PloS One. (2018) 13:e0191275. doi: 10.1371/journal.pone.0191275
37. Xia L, Hu G, Guzzo TJ. Prognostic significance of preoperative anemia in patients undergoing surgery for renal cell carcinoma: A meta-analysis. Anticancer Res. (2017) 37:3175–81.
38. Jurasz P, Alonso-Escolano D, Radomski MW. Platelet–cancer interactions: mechanisms and pharmacology of tumour cell-induced platelet aggregation. Br J Pharmacol. (2004) 143:819–26. doi: 10.1038/sj.bjp.0706013
40. Farag CM, Antar R, Akosman S, Ng M, Whalen MJ. What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP's prognostic ability in different cancer types. Oncotarget. (2023) 14:153–72. doi: 10.18632/oncotarget.28367
Keywords: prostate cancer, castration resistance, HALP score, time to castration resistance, prognostic tools
Citation: Gökmen İ, Demir N, Peker P, Özcan E, Akgül F, Bayrakçı İ, Divriklioğlu D, Erdoğan B, Topaloğlu S and Hacıoğlu MB (2024) Prognostic value of the HALP score in metastatic castration-resistant prostate cancer: an analysis combined with time to castration resistance. Front. Oncol. 14:1431629. doi: 10.3389/fonc.2024.1431629
Received: 31 May 2024; Accepted: 29 October 2024;
Published: 05 December 2024.
Edited by:
Marcus Sadi, Federal University of São Paulo, BrazilReviewed by:
Prathibha Ranganathan, Centre for Human Genetics (CHG), IndiaShangwei Zhong, University of South China, China
Copyright © 2024 Gökmen, Demir, Peker, Özcan, Akgül, Bayrakçı, Divriklioğlu, Erdoğan, Topaloğlu and Hacıoğlu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: İvo Gökmen, aXZvX2dlb3JnaWV2MUBob3RtYWlsLmNvbQ==
†ORCID: İvo Gökmen, orcid.org/0000-0002-0382-5396
Nazan Demir, orcid.org/0009-0000-2988-4450
Pınar Peker, orcid.org/0009-0004-8769-1584
Erkan Özcan, orcid.org/0000-0003-1562-6340
Fahri Akgül, orcid.org/0000-0003-1422-1093
İsmail Bayrakçı, orcid.org/0000-0002-5785-8273
Didem Divriklioğlu, orcid.org/0000-0001-9956-3900
Bülent Erdoğan, orcid.org/0000-0002-2158-3490
Sernaz Topaloğlu, orcid.org/0000-0001-5387-8309
Muhammed Bekir Hacıoğlu, orcid.org/0000-0001-8490-3239