 Yungang Hu
Yungang Hu Lu Yu
Lu Yu Yuming Shen
Yuming Shen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 26 August 2024
Sec. Radiation Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1430802
Background: Radiation therapy has become an important treatment for many malignant tumours after surgery and for palliative tumour care. Although modern radiotherapy technology is constantly improving, radiation damage to normal tissues is often difficult to avoid, and radiation-induced skin injury (RSI) is a common complication, manifested as skin erythema, peeling, ulceration, and even bone and deep organ damage, seriously affect the quality of life for patients. Basic research and clinical trials related to RSI have achieved certain results, while no researchers have conducted comprehensive bibliometric studies.
Objective: A comprehensive bibliometric analysis of publications on RSI published between 2004 and 2023 was conducted to identify current hotspots and future directions in this area of study.
Methods: RSI-related publications published between January 1, 2004, and December 31, 2023, were retrieved from the Web of Science Core Collection (WoSCC) database for analysis using VOSviewer and CiteSpace analytics.
Results: A total of 1009 publications on RSI from 2004 to 2023 were included in the WoSCC database. The United States had the highest productivity with 299 papers, accounting for 29.63% of the total production, followed by China with 193 papers (19.13%) and Japan with 111 papers (11.00%). In terms of research institutions and journals, the University of Toronto and Journal of Supportive Care in Cancer published the highest number of papers. Professor Edward Chow published the most articles, while Professor Shuyu Zhang was the most cited. The top ten most-cited papers focused on the pathogenesis, prevention, and management of RSI. Keyword co-occurrence analysis and the top 25 keywords with the strongest citation bursts suggest that current research focuses on the pathogenesis, prevention, and treatment management of RSI.
Conclusion: This study conducted a systematic bibliometric analysis of RSI publications from 2004 to 2023; identified the trends in RSI publications, major research countries, major research institutions, major research journals, major research authors, and major research keywords; and revealed the future development direction and research hotspots of this field. This study provides a valuable reference for future RSI research.
Radiation therapy has become an important treatment for many malignant tumours after surgery and for palliative tumour care (1). Over half of the patients with malignant tumours require radiation therapy (2). Although modern radiotherapy technology is constantly improving, radiation damage to normal tissues is often difficult to avoid, and radiation-induced skin injury (RSI) is a common complication. Approximately 95% of radiotherapy patients experience moderate to severe skin damage, resulting in skin erythema and peeling, and approximately 20%-25% of patients experience skin erosion and ulcers (Figure 1) (3–5). RSI caused by interventional therapy can also simultaneously occur (6). Owing to the cumulative effect of radiation on the skin, RSI is progressive, and complications can easily occur including secondary infection, aggravated tissue damage, ulcer wound deepening, and even bone and deep organ damage, which creates great difficulties in clinical treatment (7). With the increasing annual incidence of malignant tumours, RSI is gradually becoming the main factor affecting the quality of life and prognosis of patients with tumours (8).
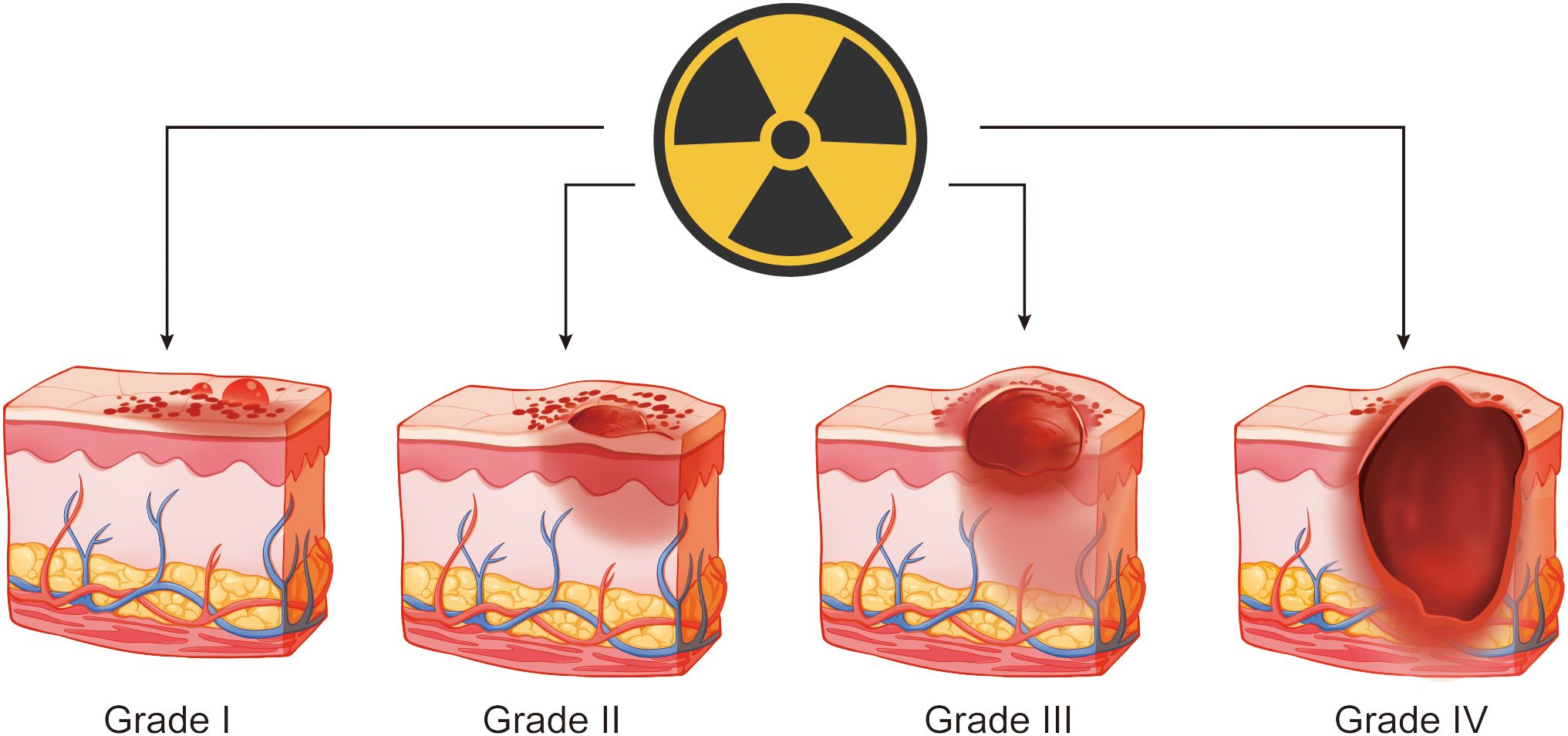
Figure 1. Schematic diagram of radiation-induced skin injury.
However, no clear standard exists for the treatment of RSI, and the prevention and management of RSI in clinical practice are usually based on personal experience, while evidence-based treatments are lacking (9). Therefore, a comprehensive analysis of the global development status, research hotspots, and future development trends of RSI is immensely significant.
Bibliometrics is a scientific discipline that employs metering methods, including mathematics and statistics, to conduct comprehensive research on both quantitative and qualitative aspects of the literature (10). The analysis enables the identification of developmental laws and of research hotspots within the research field, as well as prediction of future directions and trends. VOSviewer and CiteSpace are two widely used bibliometric analysis tools for quantitatively describing and visually analysing literature (11). In recent years, numerous bibliometric analyses have been conducted in the fields of diabetes and hypertension; however, no such studies have been conducted on RSI (12, 13). Therefore, we employ bibliometric methodologies along with these two tools to systematically analyse RSI-related literature within the Web of Science Core Collection (WoSCC) database. The objective of this study is to explore the global research status quo and identify hotspots and frontiers in RSI research while predicting future development trends to provide a novel perspective for clinical prevention and treatment.
We searched for RSI-related literature between 2004 and 2023 collected from the WoSCC database. The following retrieval formula was used: Topic = (“radiation-induced skin injury” OR “radiation skin injury” OR “radiation-induced skin ulcer” OR “radiation ulcer” OR “Radiation-induced dermatitis” OR “Radiation dermatitis”) AND Publication Data = (2004-01-01 to 2023-12-31). First, 1283 papers were retrieved. After excluding conference abstracts, letters, and other types of papers, as well as non-English literature, a total of 1,009 papers were included in the analysis. The information gathered from the selected articles encompassed the annual count of publications and citations, contributing authors, their affiliations, the year of publication, originating country, publishing journal, utilized keywords, and the H-index. Figure 2 shows the search keywords and strategies used.
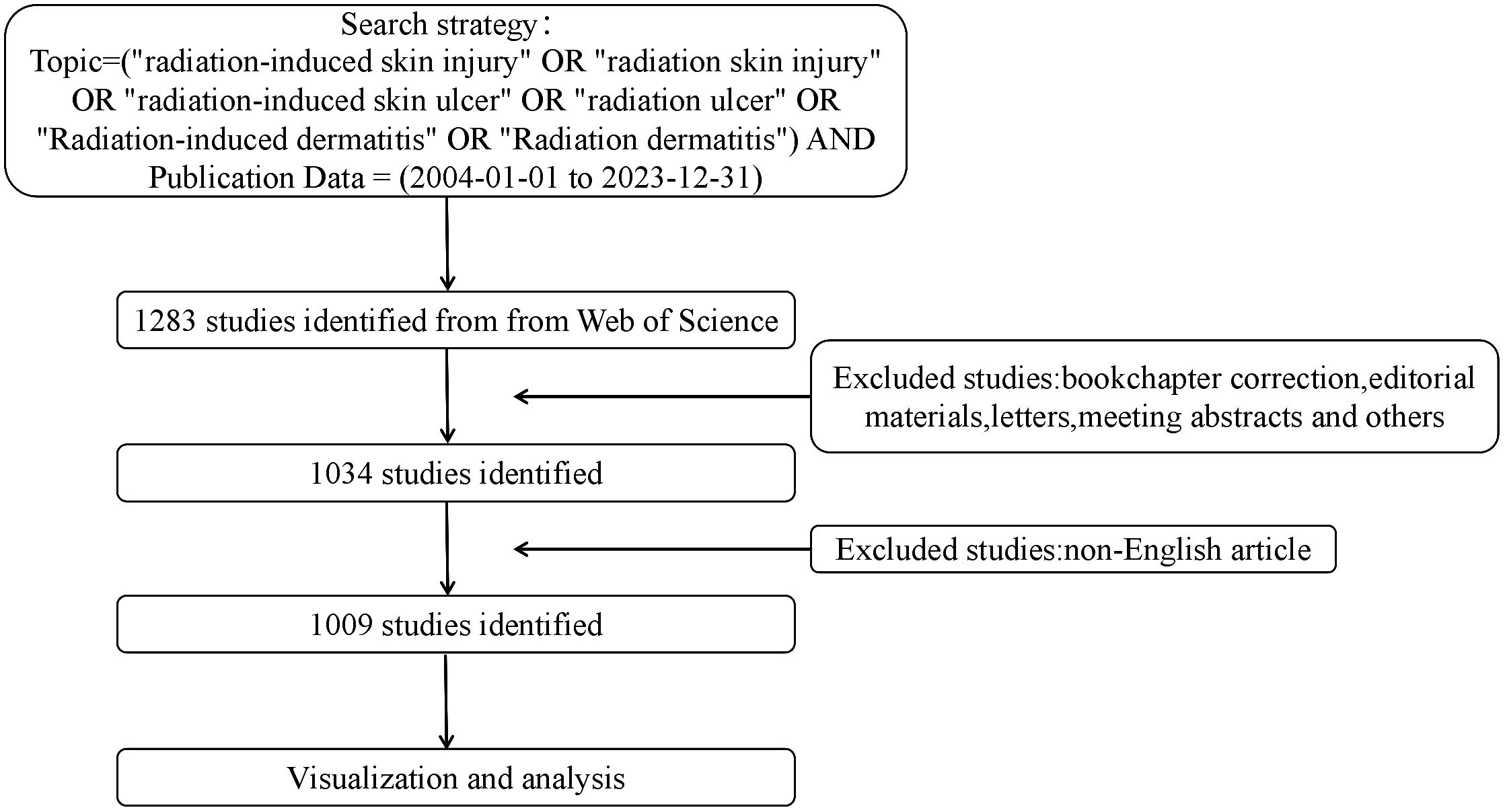
Figure 2. Research screening flow chart.
The data were analysed using CiteSpace (6.2.4R Premium) and VOSviewer (1.6.18), which was created by Waltman et al. in 2009 and is a Java-based free software for analysing large amounts of documentary data and displaying them in map format. The results of research in a certain field can then be visualised by mapping literature co-citation networks (14). Professor Chaomei Chen created CiteSpace software, which envisions the use of an experimental framework to investigate new concepts and evaluate existing techniques (15). This enables users to better understand knowledge areas, research frontiers and trends, and predict their future research progress. The number of publication reflects the research heat of the field, while the number of citations reflects the influence of the publication in the academic community.
In total, 1009 publications were included in this study, including 866 original articles and 143 review articles. Among the 1009 articles, the top three producing countries are the United States (= 299,29.63%), China (= 193,19.13%), and Japan (= 111,11.00%). Together, these three countries contributed 59.76% of the publications in the RSI field (Figure 3A). Over the past 20 years, the number of RSI-related publications per year has gradually increased globally from 17 publications in 2004 to 113 in 2023, reaching a peak of 129 in 2022. A strong relationship exists between the number of citations and the year of publication (R2 = 0.9268) (Figure 3B). These results indicate that RSI has attracted the attention of researchers worldwide.
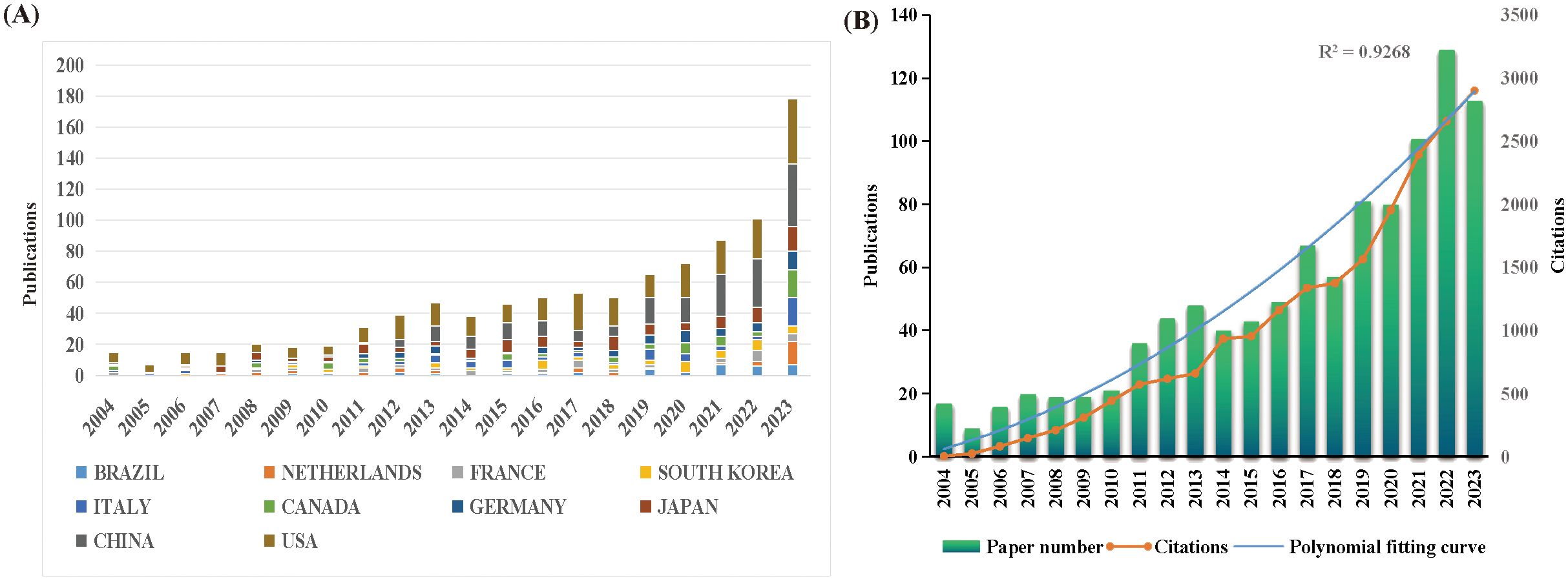
Figure 3. (A) The number of publications by country during the past 20 years. (B) The Number of annual publications and citations from 2004 to 2023.
Over the past 20 years, RSI research has been published in 66 countries and regions worldwide. The global distribution of RSI publications is shown in Figure 4. The top ten countries with the largest number of publications are the United States, China, Japan, Germany, Canada, Italy, South Korea, France, the Netherlands, and Brazil, with the top three countries accounting for more than half of the total (Table 1). The United States has the highest number of references, up to 9694, which is significantly ahead of other countries. In addition, we analysed global RSI research international partnerships. As shown in Figure 5A, international cooperation is closely linked, especially between China and the United States. Countries that publish fewer publications have less international cooperation.
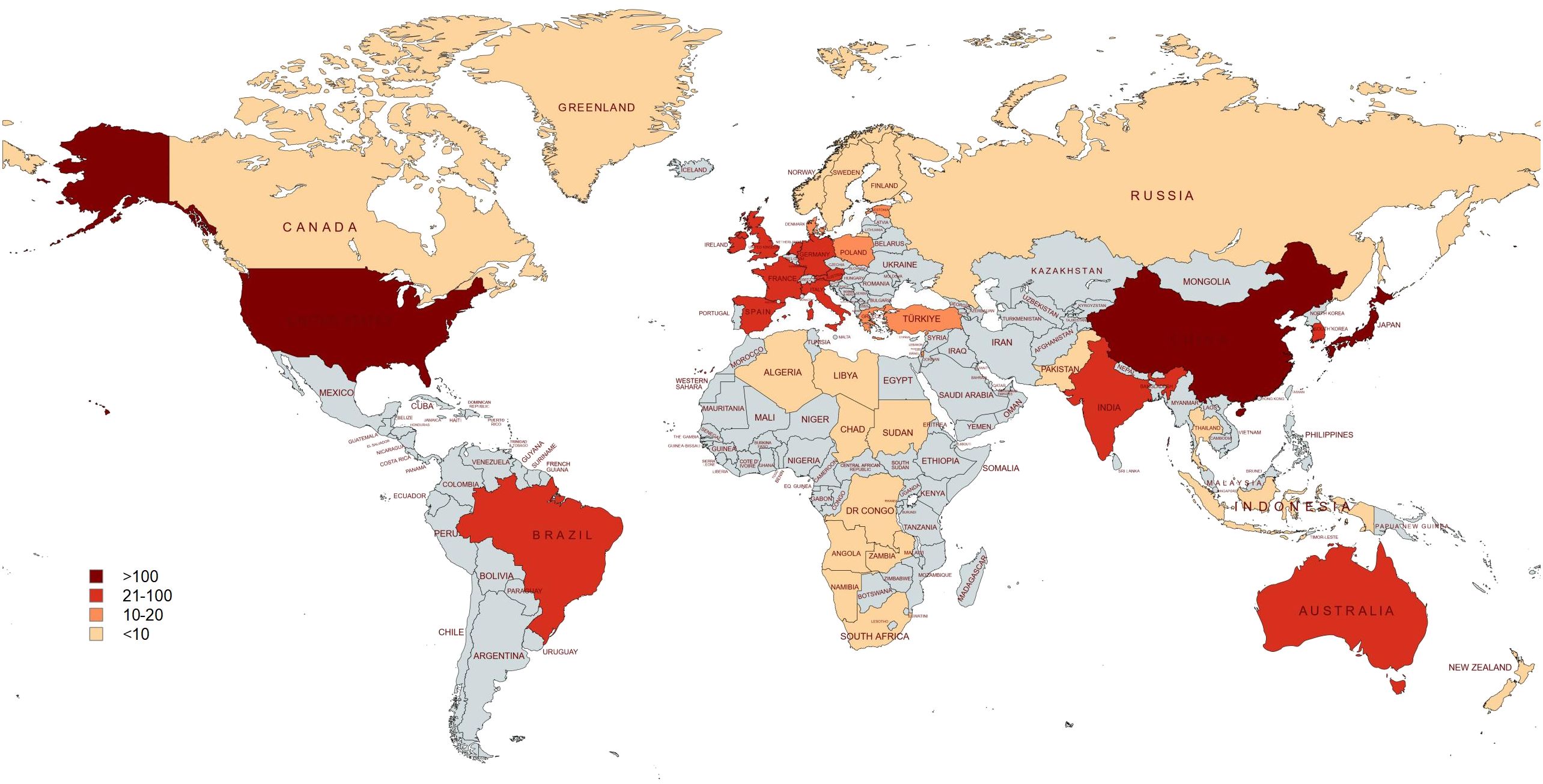
Figure 4. Visualization of the global distribution of RSI publications.
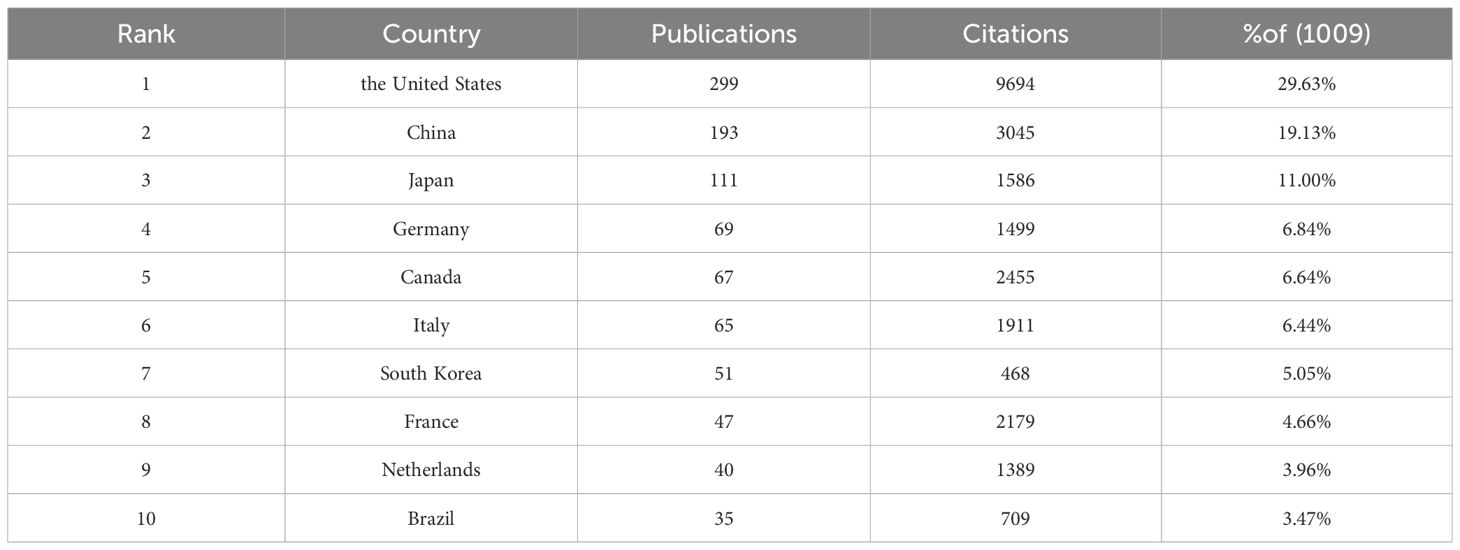
Table 1. Top 10 countries with the highest number.

Figure 5. (A) Network of RSI research international cooperation. (B) Visualisation network of RSI research institution collaboration.
The top ten institutions with the highest publication volume are distributed across six different countries: Canada, the United States, China, Belgium, the Netherlands, and Italy (Table 2). The University of Toronto published the most papers, followed by the Mayo Clinic and University of Rochester. In addition, two cancer institutions are present in the mix: the Memorial Sloan Kettering Cancer Center and the Netherlands Comprehensive Cancer Organisation. To further analyse the collaboration between different institutions, we used VOSviewer to map the RSI research institution collaboration visualisation network (Figure 5B).
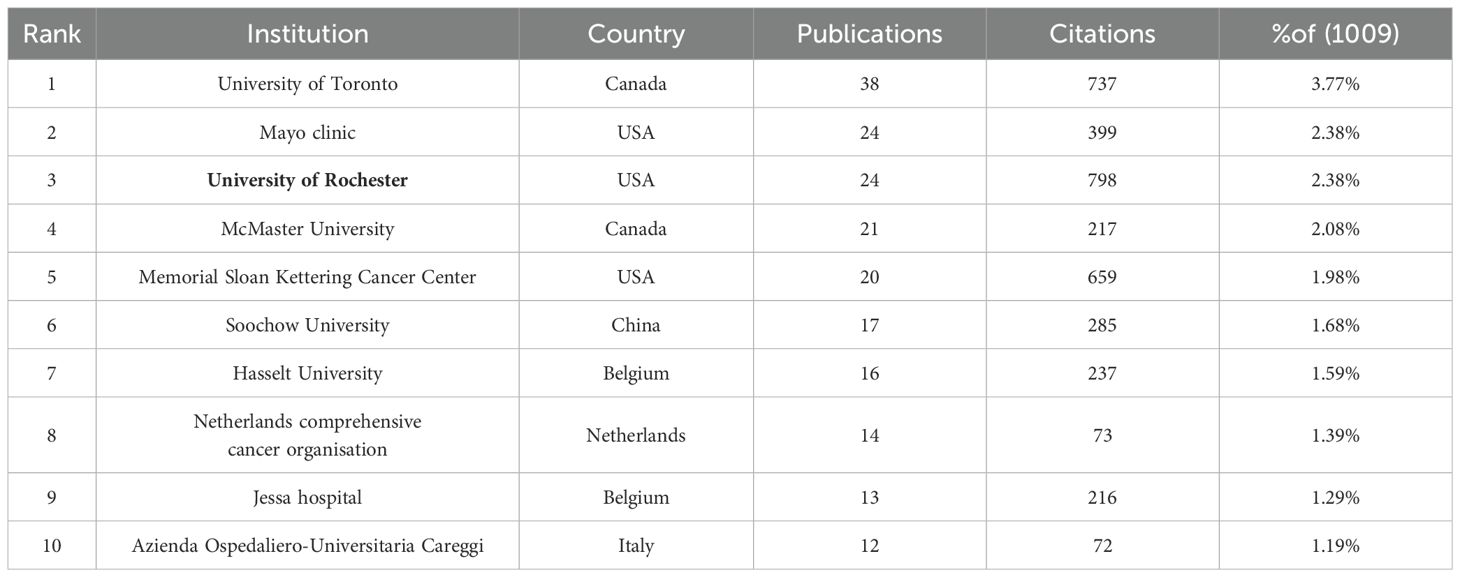
Table 2. Top 10 institutions with the highest volume of publications.
Supportive Care in Cancer, a leading publisher of RSI research, was followed by the International Journal of Radiation Oncology Biology Physics and Radiation Oncology (Table 3). From 2004 to 2023, the top ten journals with the most publications accounted for 22.50% of the total. In addition, we used co-citation analysis to further study the cooperative relationships between journals (Figure 6A).
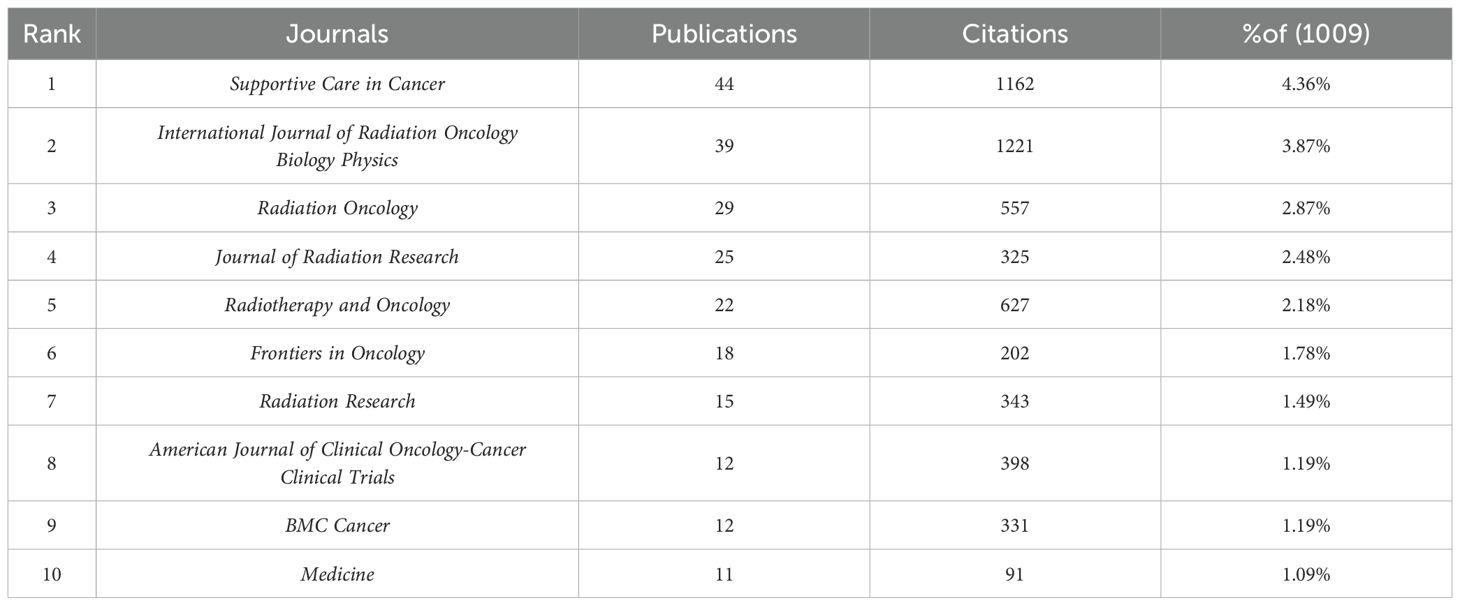
Table 3. Top 10 journals with the highest volume of publications.
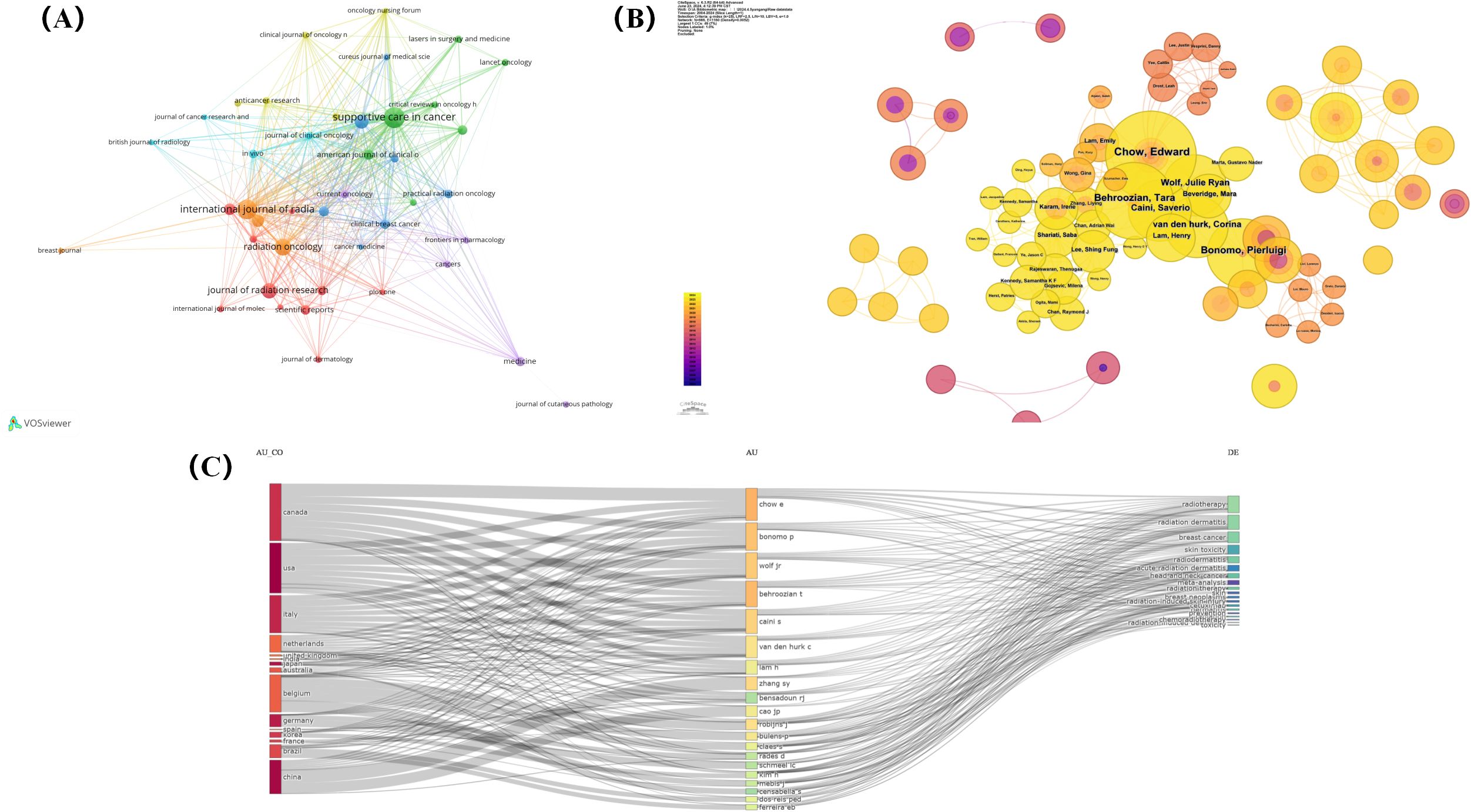
Figure 6. (A) Co-citation network visualisation of journals. (B) Co-citation network visualisation of authors. (C)Country, author and keywords Sankey diagram.
The 10 authors who have published the most in the field of RSI worldwide from six different countries, published 164 articles, representing 16.25% of all publications in the last 20 years (Table 4). Professor Edward Chow from the University of Toronto is the most prolific author in the field, followed by Prof. Pierluigi Bonomo from Azienda Ospedaliero-Universitaria Careggi, and Prof. Tara Behroozian from McMaster University. The most cited author is Shuyu Zhang, a professor at Sichuan University, China (Figure 6B). In addition, although Professor Jianping Cao from Soochow University in China has the lowest number of publications among the top 10, his citation counts are only lower than those of Shuyu Zhang and Edward Chow (Figure 6C). Hence, the achievements of Chinese scholars in the field of RSI have been recognized by scholars worldwide.
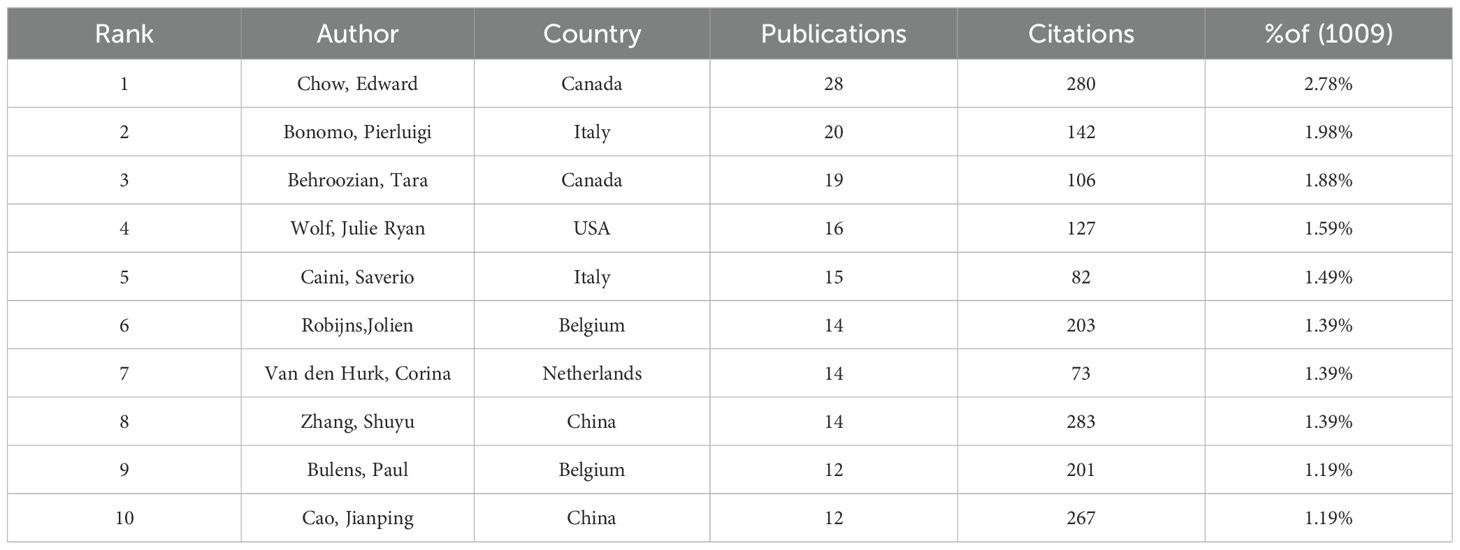
Table 4. Top 10 authors with the highest volume of publications.
Of the top 10 cited articles, the most-cited is ‘A multicentre randomised trial of breast intensity-modulated radiation therapy to reduce acute radiation dermatitis’ published by Professor Jean-Philippe Pignol, with as many as 552 citations. The lowest is Professor Lynda D. Woodruff’s ‘The efficacy of laser therapy in wound repair: A meta-analysis of the literature’, which has been cited 249 times (Table 5). These articles are mainly concerned with RSI prevention and treatment management.
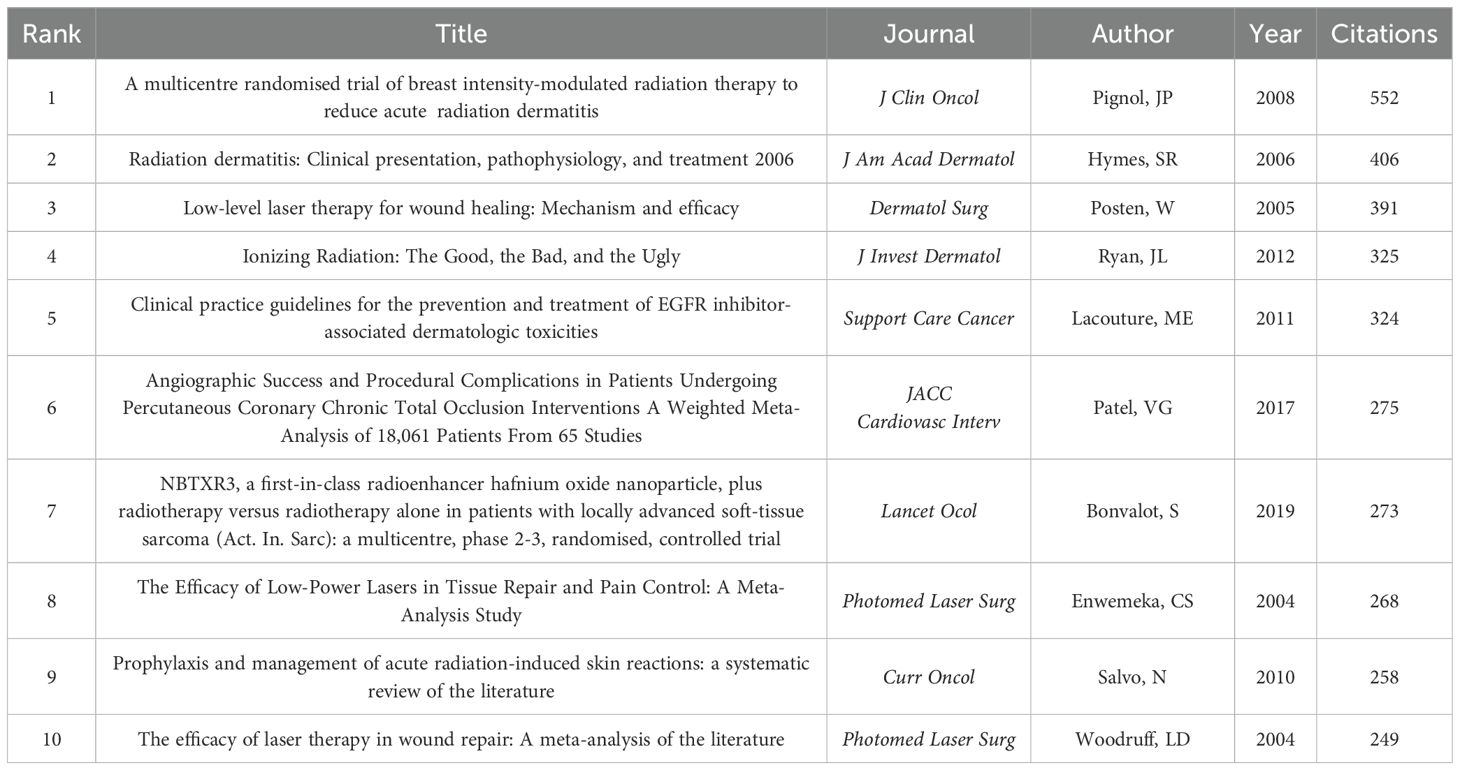
Table 5. Top 10 articles with the highest number of citations.
CiteSpace software was used to generate a co-citation network diagram depicting the relationships among the references (Figure 7A). The articles with the highest co-citation frequency include Manni Singh’s ‘Radiodermatitis: A Review of Our Current ‘Understanding’, Julie L Ryan’s ‘Ionizing radiation: the good, the bad, and the ugly’, and Fleta N Bray’s publication titled ‘Acute and Chronic Cutaneous Reactions to Ionizing Radiation Therapy’ (3, 16, 17). These three reviews comprehensively describe the pathogenesis, clinical manifestations, differential diagnosis, prevention, and treatment of skin injuries caused by ionising radiation.
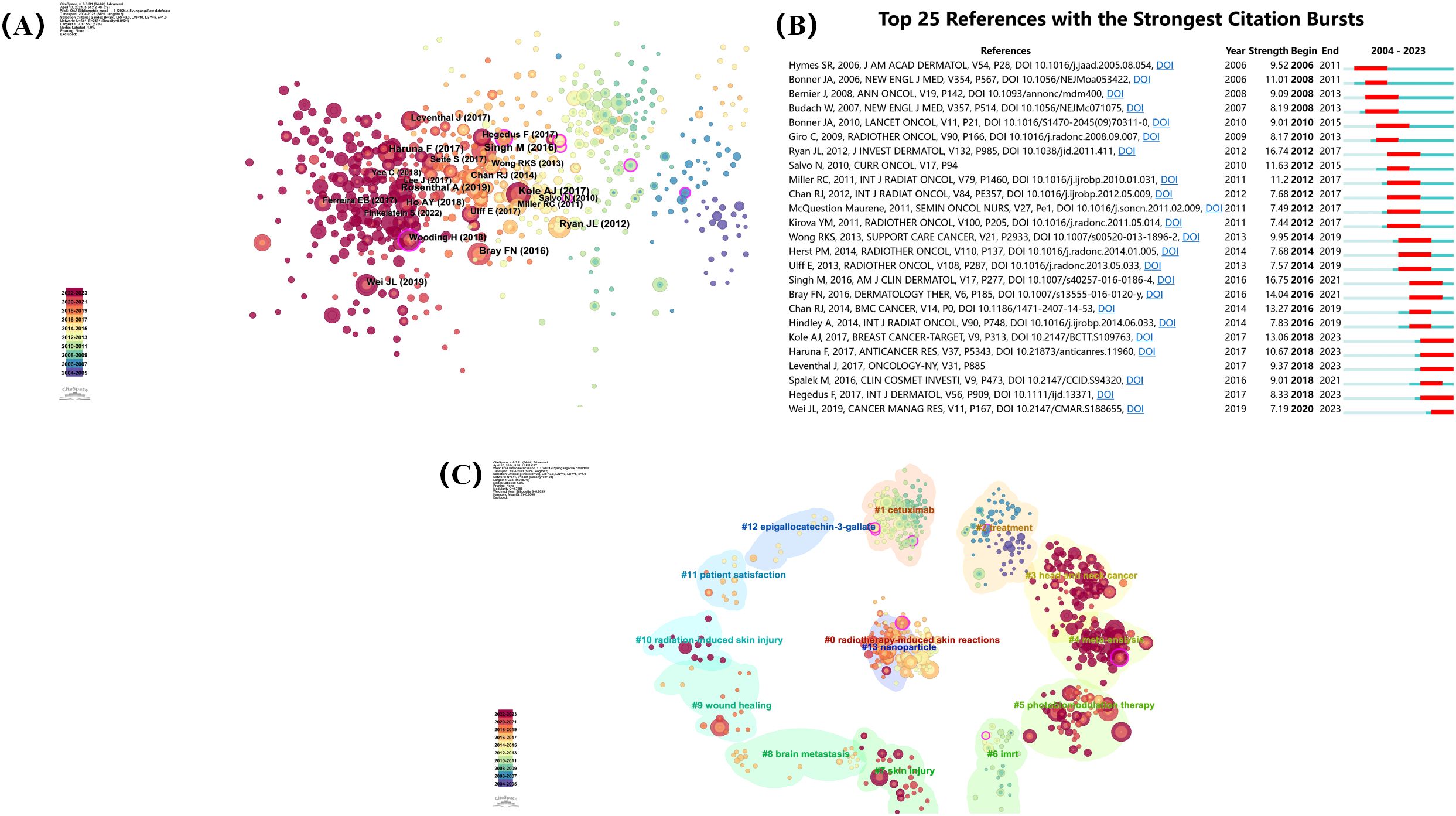
Figure 7. (A) Co-citation network visualization of references. (B) Top 25 references with the strongest citation bursts. (C) Co-citation references topic analysis.
A reference citation burst refers to a phenomenon in which the number of citations surges after an article is published. This indicates that scholars have paid significant attention to related topics. We analysed the top 25 references with the strongest citation bursts over the past 20 years using CiteSpace’s burst detection function (Figure 7B). In addition, we divided the reference co-citation titles into 14 topics. These are ‘radiotherapy-induced skin reactions’, ‘cetuximab’, ‘treatment’, ‘head and neck cancer’, ‘meta-analysis’, ‘photobiomodulation therapy’, ‘IMRT’, ‘skin injury’, ‘brain metastasis’, ‘wound healing’, ‘radiation-induced skin injury’, ‘patient satisfaction’, ‘epigallocatechin-3-gallate’, and ‘nanoparticle’ (Figure 7C). Research on RSI has mainly focused on radiotherapy-induced skin reactions and treatment after skin injury.
In addition, we also conducted co-cited reference clustering and temporal clustering analysis (Figure 8). We found that medical care (cluster 4) and clinical presentation pathophysiology (cluster 6) were early research hotspots. epidermal growth factor receptor inhibitor (cluster 1), current understanding (cluster 2), low-level laser (cluster 7), future clinical trial (cluster 8), Platinate-based chemotherapy (cluster 9), conventional radiotherapy (cluster 11), recall phenomena (cluster 12) is a research hotspot in the middle period. acute radiation dermatitis (cluster 0), containing nanoparticle (cluste 3), non-invasive physical plasma (cluster 5), stromal vascular fraction (cluster10), high-quality healing (cluster 13), single-institution retrospective analysis (cluster 15) is a hot topic and trend in the field.
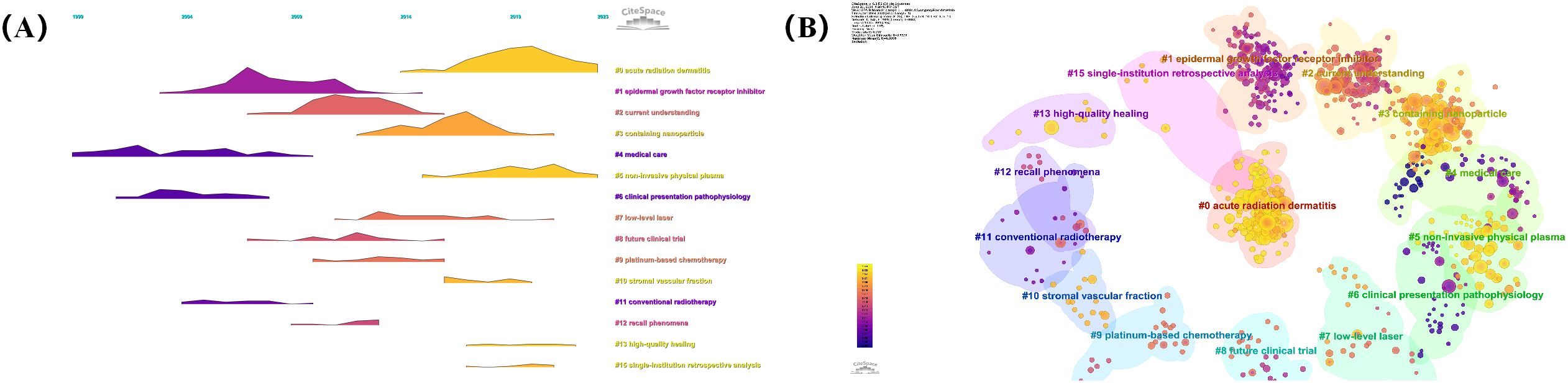
Figure 8. (A) Volcano map of co-cited references. (B) Cluster map of co-cited references.
Keyword co-occurrence analysis can identify current research hotspots in the field of RSI, which is of great significance for the development of future research trends. By drawing a co-occurrence network of keywords, we divided them into four categories (Figure 9A).
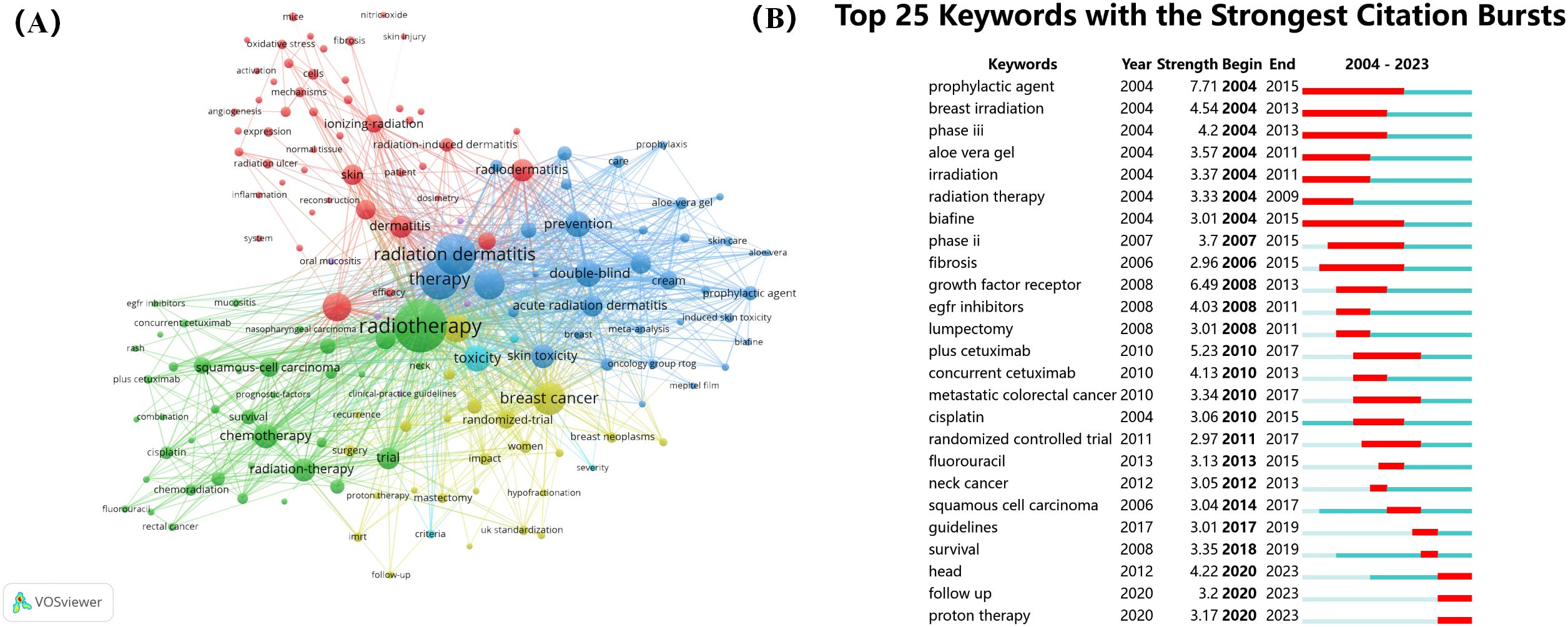
Figure 9. (A) Co-occurrence network visualization of keywords. (B) Top 25 keywords with the strongest citation bursts.
Cluster 1 (indicated in green) mainly involves radiotherapy, Cluster 2 (indicated in blue) mainly focuses on radiation dermatitis therapy, Cluster 3 (indicated in red) mainly focuses on dermatitis, and Cluster 4 (indicated in red) mainly focuses on breast cancer. In addition, we analysed the top 25 keywords with the strongest citation bursts over the last 20 years (Figure 9B). These results indicate that the current research focus is still on RSI prevention and treatment, mainly including growth factors, aloe vera gel, and related randomised controlled trials, among which the most common causes are radiotherapy for breast cancer and head and neck cancer. In order to more directly display the change of research hotspot over time, we drew the keyword clustering and time clustering analysis volcano map through CiteSpace (Figure 10).
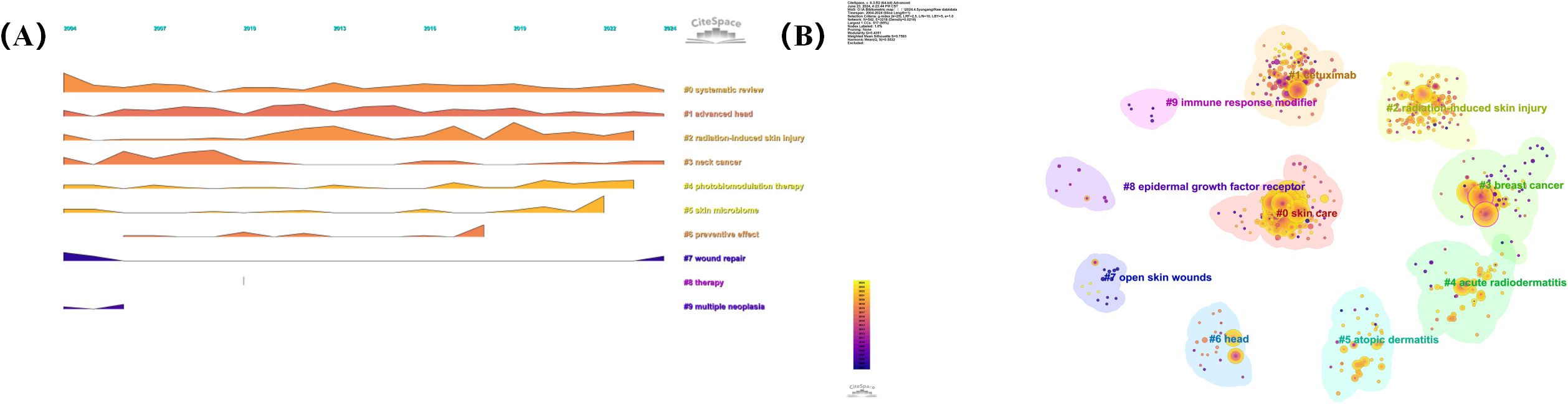
Figure 10. (A) Volcano map of keywords. (B) Cluster map of keywords.
To further analyse the differences in research hotspots among different countries, we compare the top three countries with the largest volume of publications: the United States, China, and Japan (Figure 11). We found that the three countries re very close to each other in terms of research focus, mainly covering the pathogenesis, prevention, and treatment of RSI. However, the United States has paid more attention to the pathogenesis of RSI, such as radiation dermatitis and skin toxicity. China focuses on RSI prevention and wound healing mechanisms such as antioxidants and angiogenesis. However, Japan has been paying more attention to RSI treatments.

Figure 11. (A) Co-occurrence network visualization of keywords in the United States. (B) Co-occurrence network visualization of keywords in China. (C) Co-occurrence network visualization of keywords in Japan.
Bibliometrics is often used to evaluate the research output and influence of researchers, institutions, and countries in a certain field, as well as changing trends in the research field. This helps researchers understand the current research hotspots and future development directions. In this study, we analysed 866 original articles and 143 review articles related to RSI from 2004 to 2023, showing an overall upward trend in the number of publications and citations per year. This indicates that global understanding of RSI is gradually increasing, which may be related to an increase in the number of patients with malignant tumours requiring radiation therapy. The United States leads in both the number of publications and citations in the field of RSI, far exceeding other countries. At the same time, among the top 10 institutions with the highest number of publications, three are from the United States, which shows that this country is in a leading position in research in this field. The most widely published RSI journal is Supportive Care in Cancer. This journal deals primarily with interventions to reduce symptoms and side effects in patients with cancer throughout their lives. The journal with the highest number of RSI citations is the International Journal of Radiation Oncology Biology Physics, which is mainly publishes articles concerning radiation oncology, radiobiology, medical physics, and original laboratory and clinical research related to education and health policies in this field. In the field of RSI, the most published author is Professor Edward Chow from the Department of Radiation Oncology at the University of Toronto in Canada, while the most cited author is Professor Shuyu Zhang from the School of Basic Medicine of Sichuan University, China. Hence, Canadian and Chinese scholars have conducted in-depth research in this field and have been recognized by domestic scholars. The top ten most-cited articles predominantly focused on the pathogenesis, treatment, and prevention of RSI. This is the current research hotspot and future focus of RSI.
Skin injuries caused by radiation include acute and chronic radiation dermatitis. The pathogenic mechanisms include oxidative stress, inflammatory fibrosis, and cell senescence.
When tissues are exposed to ionizing radiation, water molecules in the skin ionise and produce large amounts of reactive oxygen species (ROS). ROS can bind to lipid molecules in the cell membrane and cause lipid peroxidation, which destroys cell structure and function (18). In addition, ionising radiation can directly damage cell DNA, causing DNA strand breaks and producing ROS, resulting in persistent oxidative stress that affects the repair of the DNA double-helix structure, resulting in cell function impairment and cell necrosis (19). Continuous oxidative stress hinders basal cell division, proliferation, migration to the surface, and keratinisation (20). Oxidative stress causes vascular endothelial cell damage, resulting in dermal microvascular occlusion, ischaemia, and hypoxia (21).
After the tissue is exposed to ionising radiation, neutrophils are recruited to the irradiated site to release inflammatory mediators and stimulate an inflammatory response. Simultaneously, DNA damage, cell death, and ROS production further aggravate the inflammatory response (22). The acute inflammatory response is primarily triggered by pro-inflammatory cytokines [such as interleukin (IL)-1, IL-3, IL-5, IL-6, tumour necrosis factor-alpha (TNF-α)], chemokines (such as IL-3, eosinophil chemotactic factor), tyrosine kinase receptors, and adhesion molecules (ICAM-1, VCAM) (23). The chronic inflammatory phase predominantly involves macrophages, fibroblasts, and epithelial cells secreting transforming growth factor-beta (TGF-β) (24). TGF-β, a pro-fibrotic factor, stimulates fibroblasts to differentiate into myofibroblasts post-radiation, leading to an overproduction of extracellular matrix components such as collagen and fibronectin (25). TGF-β also reduces matrix metalloproteinase (MMP) activity in fibroblasts, affecting the degradation of the extracellular matrix (26). Accumulation of the extracellular matrix leads to increased skin tissue hardness and thickness, resulting in fibrosis. Skin fibrosis is a characteristic manifestation of chronic radiative injury. Fibrosis disrupts lymphatic and local blood circulation, reduces tissue perfusion, exacerbates the quality and functional impairment of post-radiation skin, and causes skin injuries that hinder wound healing.
Cell senescence is an evolutionarily conserved state of stable replication stagnation induced by pro-aging stressors. ROS and DNA damage caused by ionising radiation lead to cell cycle arrest and induce cell senescence (27). Senescent cells typically promote the secretion of a range of pro-inflammatory cytokines, growth factors, chemokines, and matrix metalloproteinases, collectively known as the senescence-associated secretory phenotype (SASP), and can induce tissue dysfunction via paracrine means (28). Chen et al. (29) found that in an animal model of RSI, the number of senescent cells gradually increased with the progression of radiation damage, and exogenous injection of senescent cells significantly promoted the progression of RSI in a rat model, indicating that senescent cells play a key role in the progression of RSI. Wang et al. (30) confirmed that cordycepin inhibited cell senescence in rat radiation ulcers and reduced the progression of radiation damage. Similarly, the removal of senescent cells can alleviate RSI. Dasatinib plus quercetin can selectively remove senescent cells by inducing apoptosis, reducing DNA damage, and maintaining the proliferative ability of tissue cells, thus preventing the development of RSI (31). Therefore, inhibiting cell senescence or removing senescent cells is expected to be a new strategy for reducing RSI.
At present, the pathogenesis of RSI is still studied at the cellular and molecular levels, but further studies are needed on the genes related to susceptibility to radioactive skin injury, the effects of radiation injury on epigenetic modification, and the interaction between immune response and microenvironment. By continuously improving the understanding of the pathogenesis, finding biomarkers for early prediction and diagnosis of RSI, and providing basis for personalized precision treatment, it is expected to become the main treatment strategy in the future.
Skin damage can occur in any part of the body after exposure to radiation and is more common in moist areas of the body and folds of the skin, such as the head and neck, mammary glands, armpits, perineum, and groin. RSI is common in patients with head and neck tumours, breast cancer, lung cancer, and sarcoma because of the higher radiation doses received by the skin. Risk factors for RSI mainly include patient-related and treatment-related factors.
The anterior neck area, limbs, chest, abdomen, facial skin, and scalp are sensitive to radiation and are at a higher risk of RSI (32). Obesity, malnutrition, chronic sun exposure, and smoking may increase the risk of RSI (33). Patients with genetic disorders associated with impaired DNA repair, such as ataxic capillary dilatation, Bloom syndrome, Fanconi anaemia, Gorlin syndrome, and xeroderma chromatica, are at a higher risk of RSI (21).
The total dose of radiotherapy, dose/number of splits, irradiation volume, and skin surface area affect the degree of skin damage (34). Radiotherapy techniques (intensity-modulated radiotherapy and conventional two-dimensional radiotherapy), ray particle type, and energy also affect skin toxicity. Intensity-modulated radiotherapy (IMRT) can protect normal tissues and reduce the dose and volume of skin exposure, and the dose distribution is more uniform than that in traditional two-dimensional radiotherapy technology, which can reduce the hot spots of high doses to the skin, effectively reducing the incidence of acute wet peeling reactions and late reactions such as telangiectasia (17). Both concurrent and adjuvant chemotherapy can increase skin toxicity associated with radiotherapy. Traditional chemotherapy drugs (such as doxorubicin, methotrexate, fluorouracil, and bleomycin), paclitaxel, and epidermal growth factor receptor inhibitors increase the risk of RSI (35).
The initial symptoms of RSI are mild, and with the accumulation of radiation in the skin, wet dermatitis appears, which can easily progress to chronic radioactive skin ulcers that do not heal and even cause deep tissue damage, such as radiation pneumonia and radiation cystitis (36, 37). Therefore, early prevention of RSI is very important. The main preventive measures against RSI include topical and systemic drugs, and modern radiotherapy techniques.
Topical corticosteroids are effective for preventing RSI. Regular use of topical corticosteroids during and weeks after radiotherapy may reduce the incidence of severe dermatitis, prevent severe radiation dermatitis, and reduce discomfort and itching (38). Shukla et al. (39) found that corticosteroids could effectively prevent radiation-induced skin toxicity. The incidence of wet peeling was 13% in the corticosteroid prevention group and 37% in the control group (without drug treatment). Although topical corticosteroids have shown some efficacy in RSI, there are some long-term limitations and potential side effects, including skin thinning, pigment changes, telangiectasia and drug dependence, and even local infections (40). Therefore, when selecting local topical drugs, short-term use should be tried to avoid long-term dependence; Choose low or medium acting corticosteroids to reduce the risk of side effects; Evaluate skin status regularly and adjust treatment regimen in time. Additionally, recombinant human granulocyte macrophage-stimulating factor and epidermal growth factor promote cell proliferation, reduce inflammation, improve skin barrier function and repair damaged skin (41). However, growth factor is relatively expensive, poor in vitro stability and easy to degrade, especially after long-term use of growth factor in the skin after radiotherapy, whether there is abnormal cell proliferation and increase the potential possibility of tumour needs further investigation (42). In general, growth factors have significant efficacy and multiple advantages in the prevention of radioactive skin injury, but at the same time, there are certain limitations. Future research is needed to further optimize the stability and application methods of growth factors, reduce costs, and increase their clinical penetration. At the same time, more clinical studies are needed to evaluate the long-term safety and efficacy of growth factors. Silicone film-forming gel dressings, silver ion dressings, and triethanolamine also play vital roles in preventing radiation dermatitis (43).
Oral pentoxifylline is beneficial in reducing delayed skin changes, such as skin fibrosis and necrosis, after radiation therapy; however, the preventive effect against acute radiation dermatitis is similar to that of placebo (44). Small randomised trials have evaluated egg white hydrolytic enzymes, antioxidants, zinc supplements, sulfoalumin, and gingerin, but few have documented their effectiveness in whole-body prevention (45, 46). Therefore, full-body medications are not recommended to reduce RSI.
The continuous development and improvement of modern radiotherapy technology are fundamental measures to prevent RSI. Precision radiotherapy is gradually replacing traditional radiotherapy techniques. IMRT and volumetric modulated arc therapy (VMAT) use precise positioning, planning, and illumination formulas, which can significantly reduce the radiation of normal tissues outside the target area and reduce the incidence of skin reactions (47). The use of hyperfractionation radiotherapy for the treatment of milk adenocarcinoma is increasing. Raising the total equal-effect dose with a higher fractional dose in a short course of therapy, compared with standard fractionation therapy, can reduce acute radiative dermatitis, such as diamantus, the incidence of itching, pigmentation, and pain (48).
During radiation therapy, the skin at the site of radiation should be evaluated at least once a week, and the colour, texture, and sensation of the skin should be carefully observed. The therapeutic management of RSI is guided by the severity of skin injury, and treatment depends on the severity of the skin injury.
Grade I radiation dermatitis is characterised by mild erythema and dry peeling, and generally requires application of a moisturiser. Low- and medium-efficiency topical steroid hormones can be used (49). Grade II–III radiation dermatitis is characterised by wet peeling of the skin folds or other parts of the skin. Treatment includes prevention of secondary skin staining and promotion of wet peeling healing. Silicone gel dressings, hydrogels, and hydrocolloidal dressings can keep the wound moist, promote wound healing, and effectively relieve dermatitis above grade II (9, 20). At present, there are many kinds of gel dressings, and how to choose the right dressing according to the type of radioactive skin injury is a problem that needs to be solved in clinical management. For wounds combined with infection, dressings containing antibacterial agents or silver ions can be selected to prevent infection and accelerate wound healing (50). However, the pathogenesis of radioactive skin injury is complex, and single-function dressings are not sufficient to meet clinical needs. The development of multifunctional dressings that can adapt to radioactive wounds will be the main research direction in the future. Co-infections should be treated with topical or systemic antibiotics. Grade IV radiation dermatitis may result in skin necrosis and refractory ulceration. Treatment methods mainly include surgical debridement, musculocutaneous flaps with abundant blood flow, and flap transplantation to cover the wound. Physical treatment should be based on individual conditions (22). Platelet-rich plasma, hyperbaric oxygen, and negative pressure closed drainage can be used as adjuvant treatments to improve the basic condition of the wound and promote wound regeneration and repair (51, 52).
Manifestations of chronic radiation dermatitis include dermal shrinkage, pigmentation and hypopigmentation, dermal hardiness, dermal ulceration, capillary dilatation, and fibrinisation (53). Due to poor local blood flow, radiation ulcers can easily lead to infection and the wound progressively deepens. Conservative treatment is often ineffective (54). Clinical treatment requires complete debridement to remove ulcer tissue and surrounding fibrotic skin in the first stage, and a musculocutaneous flap with abundant blood flow to fill the wound in the second stage to achieve functional reconstruction and aesthetic appearance (55). Different from other wounds, radiation ulcer has the possibility of recurrence, mostly caused by incomplete debridement. In addition to necrotic tissue and surrounding fibrotic tissue, radioactive injury involving bone, blood vessels and other important tissues should also be resected accordingly, rather than palliative debridement. Of course, this debridement mode will cause large skin soft tissue defects and bone defects. According to the defect site, extent and depth, the corresponding flap and artificial material were selected to reconstruct the bone contour and soft tissue coverage. Histological biopsies may be required for slow refractory skin ulcerations and suspected neoplasms to confirm the diagnosis and rule out the possibility of secondary skin tumours. In addition, fat transplantation can effectively improve skin fibrosis and prevent ulcers (56).
At present, the prevention and treatment of RSI are limited, and there is an urgent need to develop new drugs, such as antioxidants and senescent cell scavengers that scavenge free radicals and reduce oxidative stress damage. In recent years, the field of regenerative medicine has made significant progress, and the application of stem cells and exosomes in RSI therapy has great potential. At the same time, the use of biological materials and regenerative medicine technology to develop multi-functional wound dressings to protect the wound and accelerate healing is also a new method that many scholars are exploring. In addition, the study of low-dose radiation therapy to reduce the occurrence of radioactive skin damage at the source is a key issue that we need to pay attention to.
Using VOSviewer and CiteSpace, this study conducted a systematic bibliometric analysis; evaluated research trends, major research countries, major research institutions, and authors in the RSI field; identified the current research hotspots of RSI; and provided valuable insights for future research directions. However, this study had some limitations. The included studies were only from the WoSCC database and published between 2004 and 2023. This may have uncovered insufficient research literature, affecting the accuracy of the results.
This study conducted a systematic bibliometric analysis of RSI publications from 2004 to 2023 and identified trends in RSI publications, major research countries, institutions, journals, authors, and keywords, thus revealing the future development directions and research hotspots of this field. This study provides a valuable reference for future RSI research.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
YH: Formal analysis, Methodology, Visualization, Writing – original draft. LY: Data curation, Investigation, Methodology, Writing – original draft. WD: Conceptualization, Data curation, Investigation, Software, Writing – review & editing. XH: Project administration, Resources, Writing – review & editing. YS: Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by National Key Research and Development Program of China (2022YFC2403004).
The assistance provided by the members of the Department of Burns and Plastic Surgery at Beijing Jishuitan Hospital, Capital Medical University, is greatly appreciated.
The authors declare that the research was conducted without any existing commercial or financial affiliations that could potentially be perceived as a conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang Y, Chen S, Bao S, Yao L, Wen Z, Xu L, et al. Deciphering the fibrotic process: mechanism of chronic radiation skin injury fibrosis. Front Immunol. (2024) 15:1338922. doi: 10.3389/fimmu.2024.1338922
2. Allen C, Her S, Jaffray DA. Radiotherapy for cancer: present and future. Adv Drug Delivery Rev. (2017) 109:1–2. doi: 10.1016/j.addr.2017.01.004
3. Singh M, Alavi A, Wong R, Akita S. Radiodermatitis: A review of our current understanding. Am J Clin Dermatol. (2016) 17:277–92. doi: 10.1007/s40257-016-0186-4
4. Burnett LR, Hughes RT, Rejeski AF, Moffatt LT, Shupp JW, Christy RJ, et al. Review of the terminology describing ionizing radiation-induced skin injury: A case for standardization. Technol Cancer Res Treat. (2021) 20:15330338211039681. doi: 10.1177/15330338211039681
5. Abdlaty R, Doerwald-Munoz L, Farrell TJ, Hayward JE, Fang Q. Hyperspectral imaging assessment for radiotherapy induced skin-erythema: Pilot study. Photodiagnosis Photodyn Ther. (2021) 33:102195. doi: 10.1016/j.pdpdt.2021.102195
6. Liao JB, Chen W, Lee HS, Wu SR, Wei KC. Histopathology of fluoroscopy-induced radiation ulcer: a case series study in comparison with morphea. J Dtsch Dermatol Ges. (2020) 18:447–54. doi: 10.1111/ddg.14092
7. Kim JM, Kim SA, Kwon HJ, Moon SH, Oh DY, Rhie JW, et al. Reconstruction of radiation-induced ulcers with free flaps using the perforating vessel as a recipient vessel. Microsurgery. (2019) 39:613–20. doi: 10.1002/micr.30504
8. Rübe CE, Freyter BM, Tewary G, Roemer K, Hecht M, Rübe C. Radiation dermatitis: radiation-induced effects on the structural and immunological barrier function of the epidermis. Int J Mol Sci. (2024) 25:3320. doi: 10.3390/ijms25063320
9. Yang X, Ren H, Guo X, Hu C, Fu J. Radiation-induced skin injury: pathogenesis, treatment, and management. Aging (Albany NY). (2020) 12:23379–93. doi: 10.18632/aging.103932
10. Ninkov A, Frank JR, Maggio LA. Bibliometrics: Methods for studying academic publishing. Perspect Med Educ. (2022) 11:173–6. doi: 10.1007/s40037-021-00695-4
11. Liu Z, Yu Q, Liu H. Mesenchymal stem cells in heterotopic ossification in ankylosing spondylitis: A bibliometric study based on citeSpace and VOSViewer. J Inflammation Res. (2023) 16:4389–98. doi: 10.2147/JIR.S421962
12. Lang X, Li L, Li Y, Feng X. Effect of diabetes on wound healing: A bibliometrics and visual analysis. J Multidiscip Healthc. (2024) 17:1275–89. doi: 10.2147/JMDH.S457498
13. Jiao Y, Li W, Zhang Q, Jiang Q. Gut microbiota and hypertension: a bibliometric analysis of recent research (2014-2023). Front Nutr. (2023) 10:1253803. doi: 10.3389/fnut.2023.1253803
14. Arruda H, Silva ER, Lessa M, Proença D Jr, Bartholo R. VOSviewer and bibliometrix. J Med Libr Assoc. (2022) 110:392–5. doi: 10.5195/jmla.2022.1434
15. Han X, Wei D. Advances in research on abused women in China: bibliometric analysis by citeSpace. Trauma Violence Abuse. (2023) 24:966–80. doi: 10.1177/15248380211050562
16. Ryan JL. Ionizing radiation: the good, the bad, and the ugly. J Invest Dermatol. (2012) 132:985–93. doi: 10.1038/jid.2011.411
17. Bray FN, Simmons BJ, Wolfson AH, Nouri K. Acute and chronic cutaneous reactions to ionizing radiation therapy. Dermatol Ther (Heidelb). (2016) 6:185–206. doi: 10.1007/s13555-016-0120-y
18. Khodamoradi E, Hoseini-Ghahfarokhi M, Amini P, Motevaseli E, Shabeeb D, Musa AE, et al. Targets for protection and mitigation of radiation injury. Cell Mol Life Sci. (2020) 77:3129–59. doi: 10.1007/s00018-020-03479-x
19. Danforth JM, Provencher L, Goodarzi AA. Chromatin and the cellular response to particle radiation-induced oxidative and clustered DNA damage. Front Cell Dev Biol. (2022) 10:910440. doi: 10.3389/fcell.2022.910440
20. Hegedus F, Mathew LM, Schwartz RA. Radiation dermatitis: an overview. Int J Dermatol. (2017) 56:909–14. doi: 10.1111/ijd.13371
21. Wei J, Meng L, Hou X, Qu C, Wang B, Xin Y, et al. Radiation-induced skin reactions: mechanism and treatment. Cancer Manag Res. (2019) 11:167–77. doi: 10.2147/CMAR.S188655
22. Xie G, Ao X, Lin T, Zhou G, Wang M, Wang H, et al. E-Cadherin-Mediated Cell Contact Controls the Epidermal Damage Response in Radiation Dermatitis. J Invest Dermatol. (2017) 137:1731–9. doi: 10.1016/j.jid.2017.03.036
23. Müller K, Meineke V. Radiation-induced alterations in cytokine production by skin cells. Exp Hematol. (2007) 35:96–104. doi: 10.1016/j.exphem.2007.01.017
24. Wei KC, Lai SF, Huang WL, Yang KC, Lai PC, Wei WJ, et al. An innovative targeted therapy for fluoroscopy-induced chronic radiation dermatitis. J Mol Med (Berl). (2022) 100:135–46. doi: 10.1007/s00109-021-02146-3
25. Borrelli MR, Shen AH, Lee GK, Momeni A, Longaker MT, Wan DC. Radiation-induced skin fibrosis: pathogenesis, current treatment options, and emerging therapeutics. Ann Plast Surg. (2019) 83:S59–59S64. doi: 10.1097/SAP.0000000000002098
26. King SN, Al-Quran Z, Hurley J, Wang B, Dunlap N. Cytokine and growth factor response in a rat model of radiation induced injury to the submental muscles. Dysphagia. (2021) 36:457–64. doi: 10.1007/s00455-020-10162-7
27. Khan M, Wang Y. Advances in the current understanding of how low-dose radiation affects the cell cycle. Cells. (2022) 11:356. doi: 10.3390/cells11030356
28. Laberge RM, Sun Y, Orjalo AV, Patil CK, Freund A, Zhou L, et al. MTOR regulates the pro-tumorigenic senescence-associated secretory phenotype by promoting IL1A translation. Nat Cell Biol. (2015) 17:1049–61. doi: 10.1038/ncb3195
29. Chen W, Wang Y, Zheng J, Chen Y, Zhang C, Yang W, et al. Characterization of cellular senescence in radiation ulcers and therapeutic effects of mesenchymal stem cell-derived conditioned medium. Burns Trauma. (2023) 11:tkad001. doi: 10.1093/burnst/tkad001
30. Wang Z, Chen Z, Jiang Z, Luo P, Liu L, Huang Y, et al. Cordycepin prevents radiation ulcer by inhibiting cell senescence via NRF2 and AMPK in rodents. Nat Commun. (2019) 10:2538. doi: 10.1038/s41467-019-10386-8
31. Wang H, Wang Z, Huang Y, Zhou Y, Sheng X, Jiang Q, et al. Senolytics (DQ) mitigates radiation ulcers by removing senescent cells. Front Oncol. (2019) 9:1576. doi: 10.3389/fonc.2019.01576
32. Dzul S, Ninia J, Jang H, Kim S, Dominello M. Predictors of acute radiation dermatitis and esophagitis in african american patients receiving whole-breast radiation therapy. Pract Radiat Oncol. (2022) 12:52–9. doi: 10.1016/j.prro.2021.08.004
33. Córdoba EE, Lacunza E, Güerci AM. Clinical factors affecting the determination of radiotherapy-induced skin toxicity in breast cancer. Radiat Oncol J. (2021) 39:315–23. doi: 10.3857/roj.2020.00395
34. Hymes SR, Strom EA, Fife C. Radiation dermatitis: clinical presentation, pathophysiology, and treatment 2006. J Am Acad Dermatol. (2006) 54:28–46. doi: 10.1016/j.jaad.2005.08.054
35. Tejwani A, Wu S, Jia Y, Agulnik M, Millender L, Lacouture ME. Increased risk of high-grade dermatologic toxicities with radiation plus epidermal growth factor receptor inhibitor therapy. Cancer. (2009) 115:1286–99. doi: 10.1002/cncr.24120
36. Viso Vidal D, Jiménez Palacios M, Jorquera Plaza F. A huge rectal ulcer due to argon plasma coagulation in a patient with radiation proctitis. Rev Esp Enferm Dig. (2020) 112:661–2. doi: 10.17235/reed.2020.6798/2019
37. Zhou Y, Zhang Y. Single- versus 2-stage reconstruction for chronic post-radiation chest wall ulcer: A 10-year retrospective study of chronic radiation-induced ulcers. Med (Baltimore). (2019) 98:e14567. doi: 10.1097/MD.0000000000014567
38. Tam S, Zhou G, Trombetta M, Caini S, Ryan Wolf J, van den Hurk C, et al. Topical corticosteroids for the prevention of severe radiation dermatitis: a systematic review and meta-analysis. Support Care Cancer. (2023) 31:382. doi: 10.1007/s00520-023-07820-5
39. Shukla PN, Gairola M, Mohanti BK, Rath GK. Prophylactic beclomethasone spray to the skin during postoperative radiotherapy of carcinoma breast: a prospective randomized study. Indian J Cancer. (2006) 43:180–4. doi: 10.4103/0019-509x.29424
40. Finkelstein S, Kanee L, Behroozian T, Wolf JR, van den Hurk C, Chow E, et al. Comparison of clinical practice guidelines on radiation dermatitis: a narrative review. Support Care Cancer. (2022) 30:4663–74. doi: 10.1007/s00520-022-06829-6
41. Liu S, Wang YL, Shi ST, Zeng GD, Song YW, Zhang XD, et al. The effect of recombinant human epidermal growth factor on radiation dermatitis in rectal and anal cancer patients: a self-controlled study. BMC Cancer. (2022) 22:1140. doi: 10.1186/s12885-022-10226-x
42. Zarei F, Soleimaninejad M. Role of growth factors and biomaterials in wound healing. Artif Cells Nanomed Biotechnol. (2018) 46:906–11. doi: 10.1080/21691401.2018.1439836
43. Behroozian T, Bonomo P, Patel P, Kanee L, Finkelstein S, van den Hurk C, et al. Multinational Association of Supportive Care in Cancer (MASCC) clinical practice guidelines for the prevention and management of acute radiation dermatitis: international Delphi consensus-based recommendations. Lancet Oncol. (2023) 24:e172–172e185. doi: 10.1016/S1470-2045(23)00067-0
44. Patel V, McGurk M. Use of pentoxifylline and tocopherol in radiation-induced fibrosis and fibroatrophy. Br J Oral Maxillofac Surg. (2017) 55:235–41. doi: 10.1016/j.bjoms.2016.11.323
45. Ryan Wolf J, Heckler CE, Guido JJ, Peoples AR, Gewandter JS, Ling M, et al. Oral curcumin for radiation dermatitis: a URCC NCORP study of 686 breast cancer patients. Support Care Cancer. (2018) 26:1543–52. doi: 10.1007/s00520-017-3957-4
46. Lin LC, Que J, Lin LK, Lin FC. Zinc supplementation to improve mucositis and dermatitis in patients after radiotherapy for head-and-neck cancers: a double-blind, randomized study. Int J Radiat Oncol Biol Phys. (2006) 65:745–50. doi: 10.1016/j.ijrobp.2006.01.015
47. Kawamura M, Yoshimura M, Asada H, Nakamura M, Matsuo Y, Mizowaki T. A scoring system predicting acute radiation dermatitis in patients with head and neck cancer treated with intensity-modulated radiotherapy. Radiat Oncol. (2019) 14:14. doi: 10.1186/s13014-019-1215-2
48. Fang M, Marta GN. Hypofractionated and hyper-hypofractionated radiation therapy in postoperative breast cancer treatment. Rev Assoc Med Bras (1992). (2020) 66:1301–6. doi: 10.1590/1806-9282.66.9.1301
49. Rosenthal A, Israilevich R, Moy R. Management of acute radiation dermatitis: A review of the literature and proposal for treatment algorithm. J Am Acad Dermatol. (2019) 81:558–67. doi: 10.1016/j.jaad.2019.02.047
50. Kraemer J, Momm F. Decrease of radiation-induced skin reactions in breast cancer patients by preventive application of film dressings-a systematic review. Strahlenther Onkol. (2024) 200:109–22. doi: 10.1007/s00066-023-02151-0
51. Lee J, Jang H, Park S, Myung H, Kim K, Kim H, et al. Platelet-rich plasma activates AKT signaling to promote wound healing in a mouse model of radiation-induced skin injury. J Transl Med. (2019) 17:295. doi: 10.1186/s12967-019-2044-7
52. Lin ZC, Bennett MH, Hawkins GC, Azzopardi CP, Feldmeier J, Smee R, et al. Hyperbaric oxygen therapy for late radiation tissue injury. Cochrane Database Syst Rev. (2023) 8:CD005005. doi: 10.1002/14651858.CD005005.pub5
53. Spałek M. Chronic radiation-induced dermatitis: challenges and solutions. Clin Cosmet Investig Dermatol. (2016) 9:473–82. doi: 10.2147/CCID.S94320
54. Dong W, Zhang X, Luo X, Chen Y, Bi H, An Y, et al. Regional flap: A reliable coverage for post-radiation ulcer. Int Wound J. (2023) 20:2224–32. doi: 10.1111/iwj.14103
55. Li X, Zhang F, Liu X, Cao Z, Liu P, Xia L, et al. Staged treatment of chest wall radiation-induced ulcer with negative pressure wound therapy and latissimus dorsi myocutaneous flap transplantation. J Craniofac Surg. (2019) 30:e450–450e453. doi: 10.1097/SCS.0000000000005514
Keywords: radiation-induced skin injury, radiotherapy, bibliometric analysis, Citespace, VOSviewer
Citation: Hu Y, Yu L, Du W, Hu X and Shen Y (2024) Global hotspots and research trends of radiation-induced skin injury: a bibliometric analysis from 2004 to 2023. Front. Oncol. 14:1430802. doi: 10.3389/fonc.2024.1430802
Received: 10 May 2024; Accepted: 12 August 2024;
Published: 26 August 2024.
Edited by:
Tsair-Fwu Lee, National Kaohsiung University of Science and Technology, TaiwanReviewed by:
Ramy Abdlaty, Military Technical College, EgyptCopyright © 2024 Hu, Yu, Du, Hu and Shen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuming Shen, c2hlbnl1bWluZ2pzdEAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.