 Ralph Wendt1*†
Ralph Wendt1*† Marie Heller1Daniel Härtwig1Sven Oliver Ullmann1Heike Bisanz2
Marie Heller1Daniel Härtwig1Sven Oliver Ullmann1Heike Bisanz2 Daniela Geister2Luisa Mantovani3Ulrike Hoffmann1
Daniela Geister2Luisa Mantovani3Ulrike Hoffmann1- 1Department of Nephrology, St. Georg Hospital, Leipzig, Germany
- 2Department of Pathology, St. Georg Hospital, Leipzig, Germany
- 3Department of Oncology and Hematology, St. Georg Hospital, Leipzig, Germany
Background: Malignant hypercalcemia is usually caused by osteolytic processes of metastases, production of parathormone-related peptide, or secretion of 1,25-dihydroxyvitamin D. Ectopic PTH (parathyroid hormone) production by malignancy is very unusual.
Methods: Case report and review of the literature.
Results: We present a case of a malignant hypercalcemia with a presentation that mimicked primary hyperparathyroidism in a patient with endometrial carcinoma. Finally, ectopic production of PTH by a rapidly progressive neuroendocrine tumor was proven. Systematic literature review revealed ectopic PTH production by malignancies as an extremely rare cause of hypercalcemia and that most cases were initially misdiagnosed as primary hyperparathyroidism and underwent unnecessary surgical neck exploration in almost all cases.
Conclusion: In patients even with a suggestive constellation of primary hyperparathyroidism, an ectopic paraneoplastic PTH source should be considered if the localization diagnostics are without abnormalities or if the PTH values are unusually high. Concomitant elevated LDH levels should also raise concern about an ectopic malignant source.
The case
A 59-year-old female patient presented to the emergency department with weakness, slowness, and impaired consciousness. Routine laboratory investigation showed severe hypercalcemia (5.61 mmol/L) and acute renal failure (complete lab values in Table 1). The history of the patient was remarkable of a locally removed endometrial cancer (pT1a pNx R0 L1 V0 Pn0) 4 weeks ago at another hospital. It was described as a localized process which was completely removed. Brachytherapy was already scheduled. Hypercalcemia of malignancy was nevertheless the first differential diagnosis in the emergency department, and the patient was referred to intermediate care and treated with volume expansion, furosemide, and zoledronate. When the surprisingly elevated intact PTH (PTH) values (619 ng/L) were reported, the diagnosis was changed to primary hyperparathyroidism, given the typical constellation and the supposedly cancer-free patient. Parathormone-related peptide (PTHrP) levels were not increased. Parathyroid gland investigations with ultrasound and technetium (99mTc) sestamibi scan did not show an adenoma or any other pathology. A PTH staining from the tissue of the removed endometrial carcinoma showed a negative result. Due to persisting severe hypercalcemia, surgery with exploration of the parathyroid gland was performed on day 13. Histology confirmed normal parathyroid tissue with no evidence of malignancy. After parathyroidectomy, intraoperative intact parathyroid hormone (iPTH) results showed a surprising and massive increase in iPTH levels compared with admission values (iPTH 2,798 ng/L, Figure 1). Given those results, an ectopic production of iPTH became obvious. As an incidental finding, a papillary thyroid carcinoma was found in the removed thyroid tissue. Further investigations showed multiple spread of tumor masses, among others also in lung and liver. Liver biopsy revealed a neuroendocrine tumor with histological staining showing a negative result for synaptophysin and chromogranin, but a positive result for PTH (Figure 2).
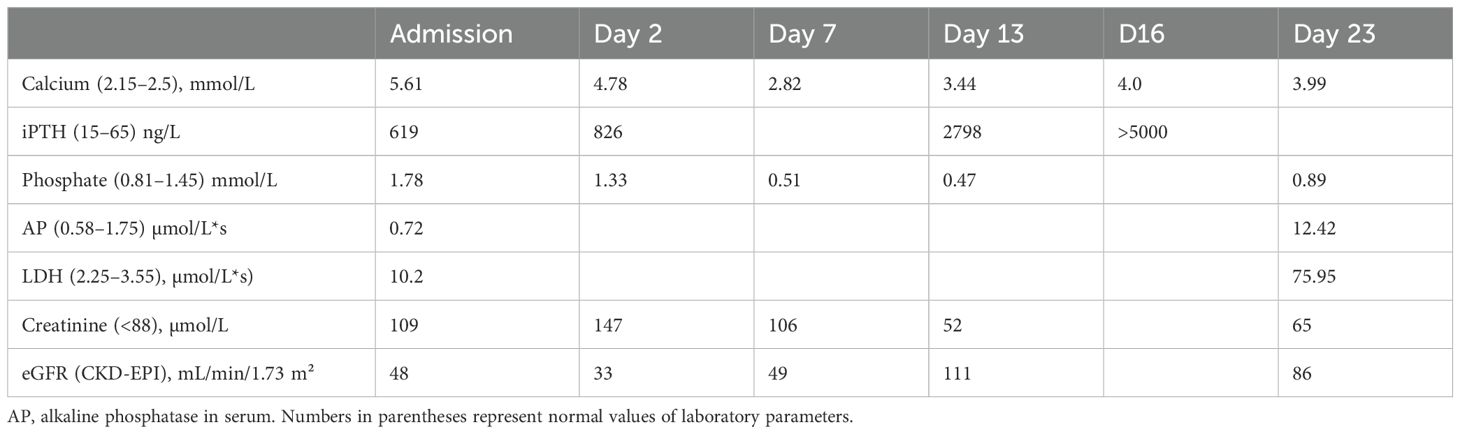
Table 1. Laboratory values from admission to day 23.
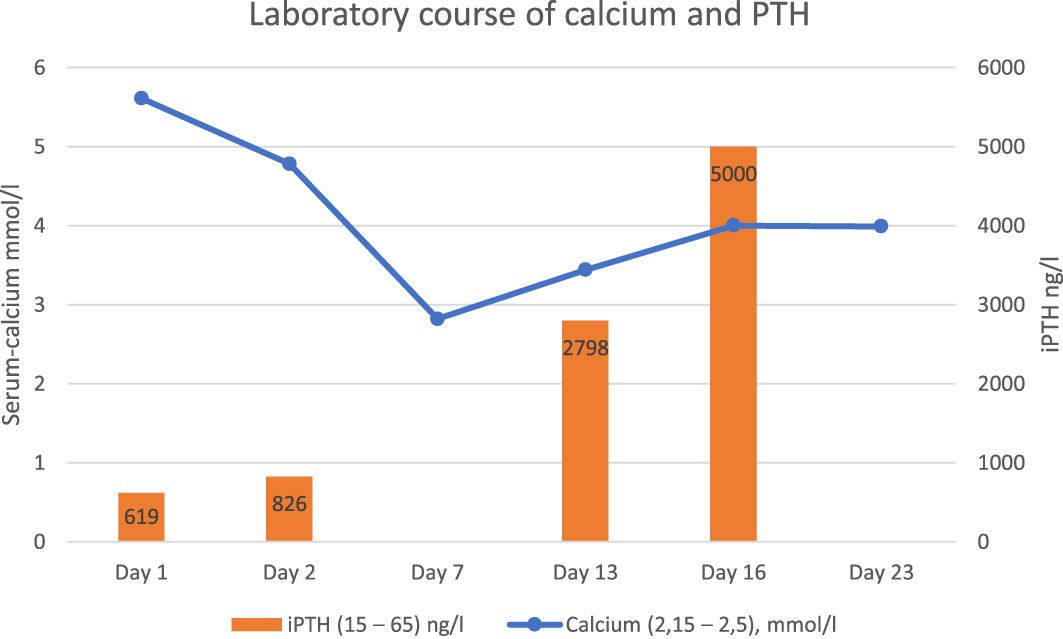
Figure 1. Course of serum calcium and iPTH during hospitalization. Numbers in parentheses represent normal values of laboratory parameters.
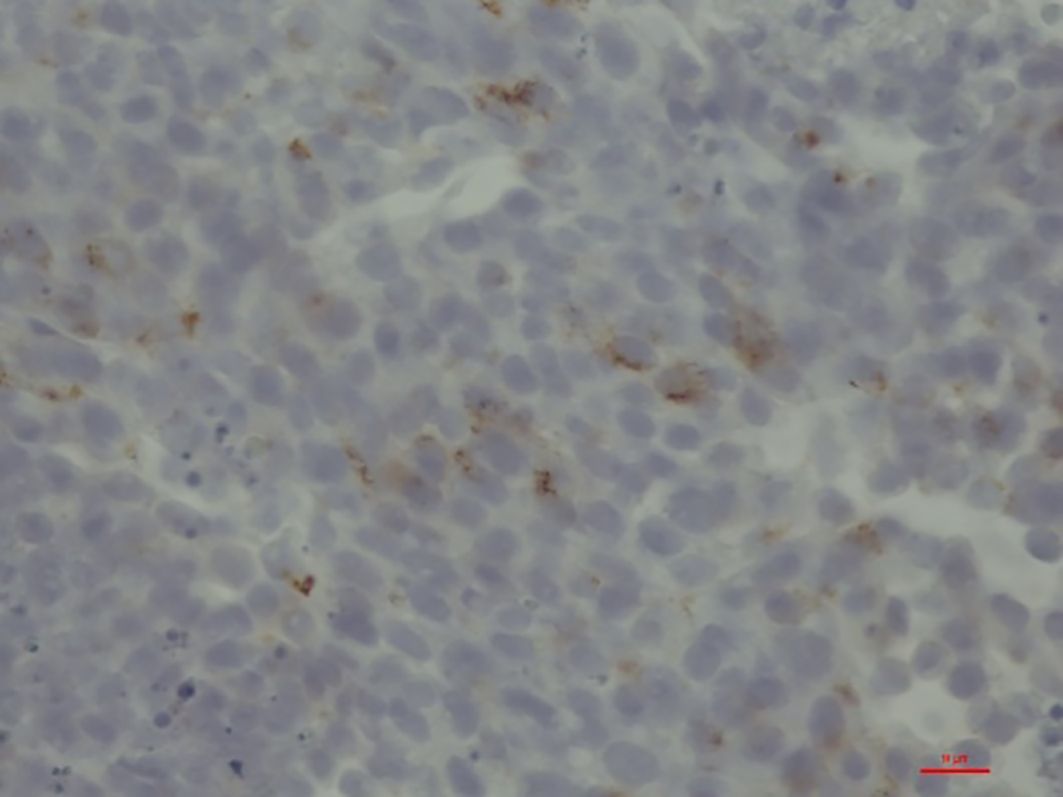
Figure 2. Liver biopsy with large cell, neuroendocrine carcinoma and positive immunostaining for PTH (brown-colored stains).
Despite repeated bisphosphonate therapy and chemotherapy, the patient died of her serious illness within a short time (day 36 of hospitalization).
Discussion and review of the literature
Hypercalcemia of malignancy is usually caused by osteolytic processes of metastases, production of parathormone-related peptide, or secretion of 1,25-dihydroxyvitamin D. Here, we present a case of ectopic PTH production by malignancy and have identified further 11 published cases in the literature.
Cancer-associated hypercalcemia has been classified into four subtypes: humoral, local osteolytic, 1,25-dihydroxyvitamin D-mediated, and ectopic hyperparathyroidism (1).
Humoral hypercalcemia of malignancy is typically caused by tumor secretion of parathyroid hormone-related protein (PTHrP). This increases osteoclastic bone resorption and renal tubular reabsorption of calcium by binding the parathyroid hormone (PTH)-PTHrP type 1 receptor in the bones and kidneys.
Local osteolytic hypercalcemia, which is characterized by extensive bone metastasis, is due to tumor cells in bone producing cytokines that increase osteoclastic bone resorption and suppress osteoblastic bone formation.
In ectopic hyperparathyroidism, tumors produce parathyroid hormone (PTH), which can act alone or in concert with PTHrP to stimulate bone resorption (5–15).
With hypercalcemia mediated by excess production of 1,25-dihydroxyvitamin D, tumors upregulate the expression 1-alpha-hydroxylase, the enzyme that converts 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D. Excess 1,25-dihydroxyvitamin D increases intestinal calcium absorption and bone resorption.
Primary hyperparathyroidism (pHPT) is the most frequent cause for hypercalcemia in the general population. Even in patients with cancer who had hypercalcemia, 6% to 21% had concomitant primary hyperparathyroidism (2, 3). In 675 consecutive patients with a biochemical diagnosis of PHPT who underwent surgical parathyroidectomy, the majority of patients had preoperative PTH levels of 100 pg/mL–400 pg/mL (433 patients), but 55 patients (8.1%) had PTH levels >400 pg/mL with maximum values up to 1,521 pg/mL (4). Therefore, the high values of iPTH in our case (619 ng/L) together with severe hypercalcemia was suggestive of pHPT and not very unusual. As depicted in Table 2, PTH levels in the published cases with ectopic PTH production were in at least 50% of the cases lower than 10× the ULN. The normal serum phosphate was confounded by acute renal failure. After improvement and normalization of renal function, serum phosphate levels dropped tremendously as expected with high iPTH levels. Remarkedly, the elevated value for lactate dehydrogenase (LDH 10.2 µmol/L*s (2.25–3.55)) already at admission should have raised suspicion for another cause of hypercalcemia other than pHPT.
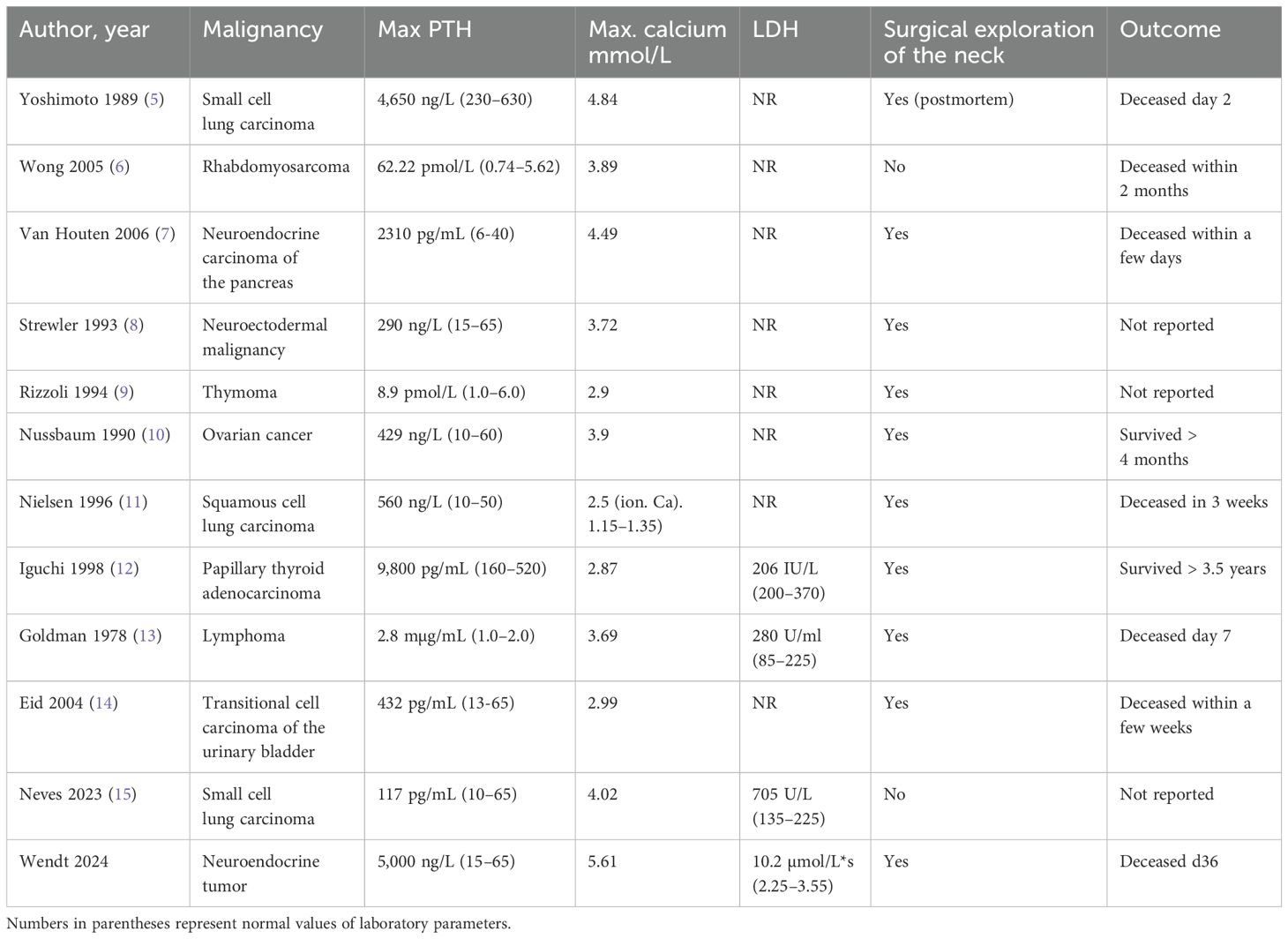
Table 2. Summary of all published cases with ectopic PTH production in malignancies with addition of our present case.
Conclusion
In conclusion of our case and after the extensive review of all published cases of ectopic PTH production by malignancies, we propose the following:
1. In cases of high iPTH (>400 pg/mL or ng/L) with suspicion of PHPT, but no signs of pathology of the parathyroid gland on ultrasound or parathyroid technetium (99mTc) sestamibi scan, we advise to undergo an extensive screening for malignancies before neck exploration.
2. In cases with suspicion of PHPT, but no signs of pathology of the parathyroid gland on ultrasound or parotid technetium (99mTc) sestamibi scan, and an elevated LDH (>3× ULN) and no other obvious reason for LDH elevation, do an extensive screening for malignancies before neck exploration.
Data availability statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans because retrospective case report of routine clinical management. The report was conducted in accordance with the local legislation and institutional requirements. Written informed consent was obtained from the next of kin for the publication of the data included in this article.
Author contributions
RW: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. MH: Writing – review & editing. DH: Writing – review & editing. SU: Writing – review & editing. HB: Writing – review & editing. DG: Writing – review & editing. LM: Writing – review & editing. UH: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Guise TA, Wysolmerski JJ. Cancer-associated hypercalcemia. N Engl J Med. (2022) 386:1443–51. doi: 10.1056/nejmcp2113128
2. Strodel WE, Thompson NW, Eckhauser FE, Knol JA. Malignancy and concomitant primary hyperparathyroidism. J Surg Oncol. (1988) 37:10–2. doi: 10.1002/jso.2930370104
3. Hutchesson ACJ, Bundred NJ, Ratcliffe WA. Survival in hypercalcaemic patients with cancer and co-existing primary hyperparathyroidism. Postgrad Méd J. (1995) 71:28–31. doi: 10.1136/pgmj.71.831.28
4. Hargitai L, Bereuter CM, Dunkler D, Geroldinger A, Scheuba C, Niederle B, et al. The value of intraoperative parathyroid hormone monitoring in patients with primary hyperparathyroidism and varying baseline parathyroid hormone levels. BJS Open. (2022) 6:zrac118. doi: 10.1093/bjsopen/zrac118
5. Yoshimoto K, Yamasaki R, Sakai H, Tezuka U, Takahashi M, Iizuka M, et al. Ectopic production of parathyroid hormone by small cell lung cancer in a patient with hypercalcemia. J Clin Endocrinol Metab. (1989) 68:976–81.
6. Wong K, Tsuda S, Mukai R, Sumida K, Arakaki R. Parathyroid hormone expression in a patient with metastatic nasopharyngeal rhabdomyosarcoma and hypercalcemia. Endocrine. (2005) 27:83–6. doi: 10.1385/endo:27:1:083
7. VanHouten JN, Yu N, Rimm D, Dotto J, Arnold A, Wysolmerski JJ, et al. Hypercalcemia of Malignancy due to ectopic transactivation of the parathyroid hormone gene. J Clin Endocrinol Metab. (2006) 91:580–3. doi: 10.1210/jc.2005-2095
8. Strewler GJ, Budayr AA, Clark OH, Nissenson RA. Production of parathyroid hormone by a Malignant nonparathyroid tumor in a hypercalcemic patient. J Clin Endocrinol Metab. (1993) 76:1373–5. doi: 10.1210/jcem.76.5.7684395
9. Rizzoli R, Pache JC, Didierjean L, Bürger A, Bonjour JP. A thymoma as a cause of true ectopic hyperparathyroidism. J Clin Endocrinol Metab. (1994) 79:912–5. doi: 10.1210/jcem.79.3.8077382
10. Nussbaum SR, Gaz RD, Arnold A. Hypercalcemia and ectopic secretion of parathyroid hormone by an ovarian carcinoma with rearrangement of the gene for parathyroid hormone. N Engl J Med. (1990) 323:1324–8. doi: 10.1056/nejm199011083231907
11. Nielsen PK, Rasmussen AK, Feldt-Rasmussen U, Brandt M, Christensen L, Olgaard K. Ectopic production of intact parathyroid hormone by a squamous cell lung carcinoma. Vivo vitro. J Clin Endocrinol Metab. (1996) 81:3793–6. doi: 10.1210/jcem.81.10.8855839
12. Iguchi H, Miyagi C, Tomita K, Kawauchi S, Nozuka Y, Tsuneyoshi M, et al. Hypercalcemia caused by ectopic production of parathyroid hormone in a patient with papillary adenocarcinoma of the thyroid gland. J Clin Endocrinol Metab. (1998) 83:2653–7. doi: 10.1210/jcem.83.8.5025
13. Goldman JW, Becker FO. Ectopic parathyroid hormone syndrome. Occurrence in a case undifferentiated lymphoma with bone marrow involvement. Arch Intern Med. (1978) 138:1290–1. doi: 10.1001/archinte.138.8.1290
14. Eid W, Wheeler TM, Sharma MD. Recurrent hypercalcemia due to ectopic production of parathyroid hormone-related protein and intact parathyroid hormone in A single patient with multiple Malignancies. Endocr Pr. (2004) 10:125–8. doi: 10.4158/ep.10.2.125
Keywords: IPTH, parathyroid hormone, malignancy, ectopic, primary hyperparathyroidism (pHPT), hypercalcemia
Citation: Wendt R, Heller M, Härtwig D, Ullmann SO, Bisanz H, Geister D, Mantovani L and Hoffmann U (2024) Case report: Ectopic production of intact parathyroid hormone (iPTH) by malignoma mimicking primary hyperparathyroidism. Front. Oncol. 14:1422131. doi: 10.3389/fonc.2024.1422131
Received: 23 April 2024; Accepted: 15 November 2024;
Published: 05 December 2024.
Edited by:
Hui Lu, Zhejiang University, ChinaReviewed by:
Sudhaker D. Rao, Henry Ford Hospital, United StatesClaudiu Eduard Nistor, Carol Davila University of Medicine and Pharmacy, Romania
Copyright © 2024 Wendt, Heller, Härtwig, Ullmann, Bisanz, Geister, Mantovani and Hoffmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ralph Wendt, cmFscGgud2VuZHRAc2Fua3RnZW9yZy5kZQ==
†ORCID: Ralph Wendt, orcid.org/0000-0003-1600-6581