
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 26 August 2024
Sec. Hematologic Malignancies
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1405467
 Valentín García-Gutiérrez1
Valentín García-Gutiérrez1 María Teresa Gómez-Casares2
María Teresa Gómez-Casares2 Blanca Xicoy3
Blanca Xicoy3 Felipe Casado-Montero4
Felipe Casado-Montero4 Guillermo Orti5
Guillermo Orti5 Pilar Giraldo6
Pilar Giraldo6 Juan Carlos Hernández-Boluda7*
Juan Carlos Hernández-Boluda7*Chronic myeloid leukemia (CML), characterized by the presence of the BCR::ABL1 fusion gene, has undergone a transformative shift with the introduction of tyrosine kinase inhibitors (TKIs). The current availability of six different TKIs (imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and asciminib) in clinical practice makes it important to know their efficacy and toxicity profile for treatment optimization. This review examines the latest insights regarding the use of bosutinib in CML treatment. Clinical trials have demonstrated the effectiveness of bosutinib, positioning it as a first-line treatment that can induce sustained molecular responses. Importantly, it can also be effective in patients who have experienced treatment failure or intolerance with prior TKIs, revealing the potential of bosutinib also in second- and later-line settings. Even in the advanced phase of CML, bosutinib has demonstrated its capacity to achieve molecular responses, expanding its usefulness. Real-world evidence studies echo these findings, emphasizing bosutinib’s effectiveness in achieving deep molecular responses, maintaining remissions, and serving as an alternative for patients intolerant or resistant to other TKIs as a second-line therapy. Notably, one of the greatest strengths of bosutinib is its favorable safety profile, in particular the low incidence of vascular complications with its use, which is undoubtedly a comparative advantage over other TKIs. In summary, the latest research highlights the versatility of bosutinib in CML treatment and underscores its pivotal role in optimizing patient management in challenging cases. Continuing research and investigation will further establish bosutinib’s place in the evolving landscape of CML therapy, offering an alternative for CML patients across different treatment stages.
Chronic myeloid leukemia (CML) is a clonal hematopoietic stem cell (HSC) disease that accounts for approximately 30% of the incidence of adult leukemia (1). It is characterized by the presence of the Philadelphia (Ph1) chromosome, which results from a reciprocal chromosomal translocation between chromosome 22 and chromosome 9 [t(9;22)(q34;q11)] (2). This produces fusion of the BCR and ABL1 genes into the pathogenic BCR::ABL1 oncogene, generating a truncated hybrid protein with uncontrolled tyrosine kinase activity, which results in a proliferative advantage for mutant HSCs over normal HSCs (3). CML was classically classified into three stages: chronic (CP), accelerated (AP), and blast phase (BP) (4). Left untreated, the annual rate of disease progression to the advanced phases is about 10% (4). However, the risk of progression has been dramatically reduced with the introduction of tyrosine kinase inhibitor (TKI) therapy. As a result, the updated World Health Organization diagnostic criteria no longer recognize the AP, instead focusing on high risk features such as the presence of ABL1 kinase mutations and/or additional cytogenetic abnormalities (5). By contrast, the International Consensus Classification (ICC) maintains the traditional three-phase model for classifying CML (6).
Historically, the only curative therapeutic option for CML was allogeneic stem cell transplant (7). However, the CML treatment scenario was transformed by the development of TKIs. TKIs effectively block the interaction between the BCR::ABL1 oncoprotein and adenosine triphosphate (ATP), halting the cellular growth of the malignant clone. This “targeted” therapy altered the normal course of CML, raising the 10-year survival rate from 20% to 80%-90% (8, 9). The first-in-class TKI medicine licensed for the treatment of CML is imatinib mesylate more than 20 years ago (10). Nevertheless, some patients experienced treatment resistance or intolerance with imatinib, resulting in therapy failure in approximately 30%–35% of cases (11). Consequently, second- and third-generation TKIs such as dasatinib, nilotinib, bosutinib, and ponatinib were developed (12).
Current guidelines recommend a TKI (imatinib, dasatinib, nilotinib or bosutinib) as the frontline therapy for CML, while imatinib being the most commonly utilized, particularly in patients with comorbidities (11, 13, 14). Second-generation TKIs have been proposed for patients requiring a second line of treatment. While available evidence shows similar efficacy in comparison to imatinib, it is important to note that no head-to-head trials comparing second generation TKIs have been conducted to date (15). Therefore, the choice of therapy in this scenario is determined by the patient’s specific condition, particularly the existence of comorbidities, management of the side effects associated with each TKI, and how they impact the patient’s quality of life.
Bosutinib (also known as SKI-606) is an oral, second-generation TKI that binds to the kinase domain of BCR::ABL1 (16). Preclinical studies indicate that over the oral dosage range of 200-800 mg, it induces dose-proportional increases in plasma concentration and Cmax (17, 18). In addition, it has 34% absolute bioavailability in healthy people with a single 500-mg dose (17). Bosutinib inhibits 16 of 18 imatinib-resistant forms of BCR::ABL1 kinase in murine models (16). In preclinical safety trials, bosutinib had no effect on respiratory function or blood pressure, and had no/minimal effect on cardiac function (16, 19). It has also been shown to be non-mutagenic, non-carcinogenic, non-phototoxic, and non-clastogenic (16, 19). Some reproductive and developmental damage, as well as impaired fertility, was observed following bosutinib treatment in studies in rats and rabbits (16, 19).
Bosutinib 400 mg once daily (QD) is authorized for the treatment of individuals with newly diagnosed CP Ph1 CML, and 500 mg QD is approved for patients with CP, AP, or BP Ph1 CML who have developed resistance or intolerance to prior treatments (16). Since bosutinib was approved for the treatment of CML in 2012, numerous additional studies have been conducted, generating new data on its real-world and population-specific performance. In this review, we compile the latest available data on the efficacy and safety of bosutinib in the treatment of CML, in order to identify the patient profile that might potentially benefit more from this medication.
Approval of bosutinib as a first-line therapy for CML was based on the results of two pivotal phase 3 studies (summarized in Table 1). The BELA trial results were first published in 2012 and compared bosutinib 500 mg QD to imatinib 400 mg QD (15, 20). Although this trial did not meet its primary objective (complete cytogenetic response, CCyR, at 12 months), with a CCyR rate of 70% for patients on bosutinib vs. 68% for imatinib, it found a significantly higher major molecular response (MMR) rate (41% vs. 27%), faster times to CCyR and MMR, and a trend toward fewer on-treatment transformations to AP/BP with bosutinib compared to imatinib (20). The BELA trial also reported Kaplan-Meier estimates of overall survival at 12 months, which were greater than 99% in the bosutinib arm and 97% in the imatinib arm. Some factors might potentially have influenced the primary outcome of this trial, most notably the higher dose administered, which resulted in high rates of adverse event (AE)-related dose interruptions during the first few months (61% vs. 42%) and discontinuations (19% vs. 6%) in the bosutinib group versus imatinib group. The safety profile of bosutinib in this trial was consistent with previous reports and no new safety signals were identified (15).
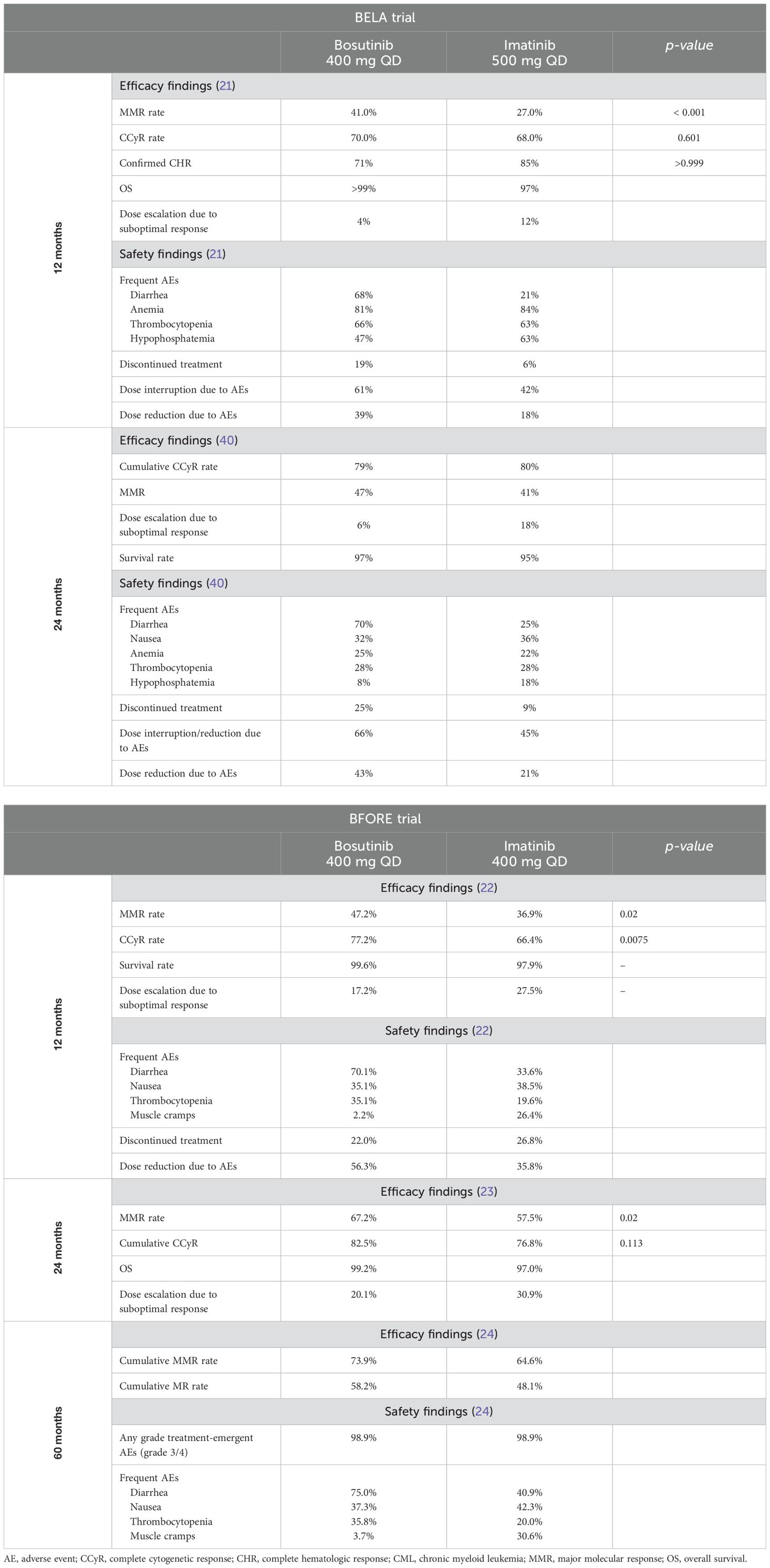
Table 1. Summary of major findings from phase III studies of bosutinib as first-line therapy for patients with newly diagnosed CP-CML.
The results of the BFORE trial comparing bosutinib 400 mg QD to imatinib 400 mg QD were first published in 2018 (21). At 12 months, patients who received bosutinib had substantially greater rates of MMR and CCyR than patients who did not receive bosutinib (MMR: 47% vs. 37%; CCyR: 77% vs. 66%, respectively). Furthermore, as compared to imatinib-treated patients, bosutinib demonstrated quicker responses at 24 months (Table 1) (22). The safety findings were consistent with prior studies, and no new safety signals were identified. Long-term efficacy and safety of bosutinib were demonstrated in the final analysis of the BFORE trial after 5 years of follow-up (23). Bosutinib was superior to imatinib in terms of MMR rates (47.4% vs. 36.6%; 1.57 [1.11–2.22]) (23). This data was also confirmed in the Japanese population (24). Regarding its safety profile, both bosutinib and imatinib treatment showed an increase in the incidence of cardiac, effusion, renal, and vascular treatment-emergent adverse events (TEAEs) after 5 years of follow-up, but no new safety signals were observed (23). Overall survival rates in the BFORE study demonstrated the long-term efficacy of bosutinib. After 5 years of follow-up, both bosutinib and imatinib had excellent overall survival rates (94.5% and 94.6%, respectively), highlighting the effectiveness of bosutinib in producing long-term responses.
These data support the use of bosutinib 400 mg QD in newly diagnosed CP-CML patients. In current practice, first-line treatment is determined on the basis of the estimated risk-benefit ratio in each particular patient. Although no direct comparisons of bosutinib vs. dasatinib or nilotinib have been made, indirect comparisons have shown that bosutinib is as effective as nilotinib and dasatinib in the treatment of individuals with newly diagnosed CP-CML (25). Thus, in those patients considered candidates for treatment with second-generation TKIs, the choice is determined by the patient’s comorbidities and drug safety profile. The selection of second-generation TKIs may also be influenced by the availability of dasatinib as a generic medication. Treatment with dasatinib or nilotinib is not indicated in individuals with significant cardiovascular risk, so bosutinib is a better option since it has a better cardiovascular profile (26). On the other hand, patients who have had or are having gastrointestinal (GI) issues or hepatotoxicity for any reason would not be good candidates for bosutinib treatment.
Bosutinib is also approved for patients with Ph1 CML who are resistant/intolerant to prior therapy (16). The approval of bosutinib 500 mg QD for patients with CML who were previously treated with ≥1 TKI was based on the results of a multicenter, open-label phase 1/2 study that investigated bosutinib’s performance in patients with imatinib-resistant or -intolerant CML. The study had distinct cohorts for CP-, AP-, and BP-CML (27–29). Most of the participants in the study (69%) were patients with imatinib-resistant CP-CML (27–29). Cumulative major cytogenetic response (MCyR) and CCyR rates (newly acquired or maintained from baseline) were 60% and 50%, respectively, by year 5 (29). The Kaplan-Meier probability of maintaining an MCyR or CCyR response after 5 years was 71% and 69%, respectively (29). Most AEs occurred within the first 2 years (29). Overall, GI disturbances were the most prevalent (diarrhea 86%, nausea 46%, and vomiting 37%), with thrombocytopenia (25%) being the most common grade 3/4 toxicity (29). From years 3 to 5, none of the four on-treatment reported fatalities were linked to bosutinib. In summary, bosutinib demonstrated long-term efficacy and a tolerable safety profile in patients with CML treated for up to 5 years in the second-line setting (27–29). A summarized comparison of the efficacy of other second-generation TKIs (dasatinib and nilotinib) after imatinib failure at 24 months is shown in Table 2. In general, the three second-generation TKIs exhibited comparable efficacy, with probabilities of achieving CCyR around 50% (28, 30, 31).
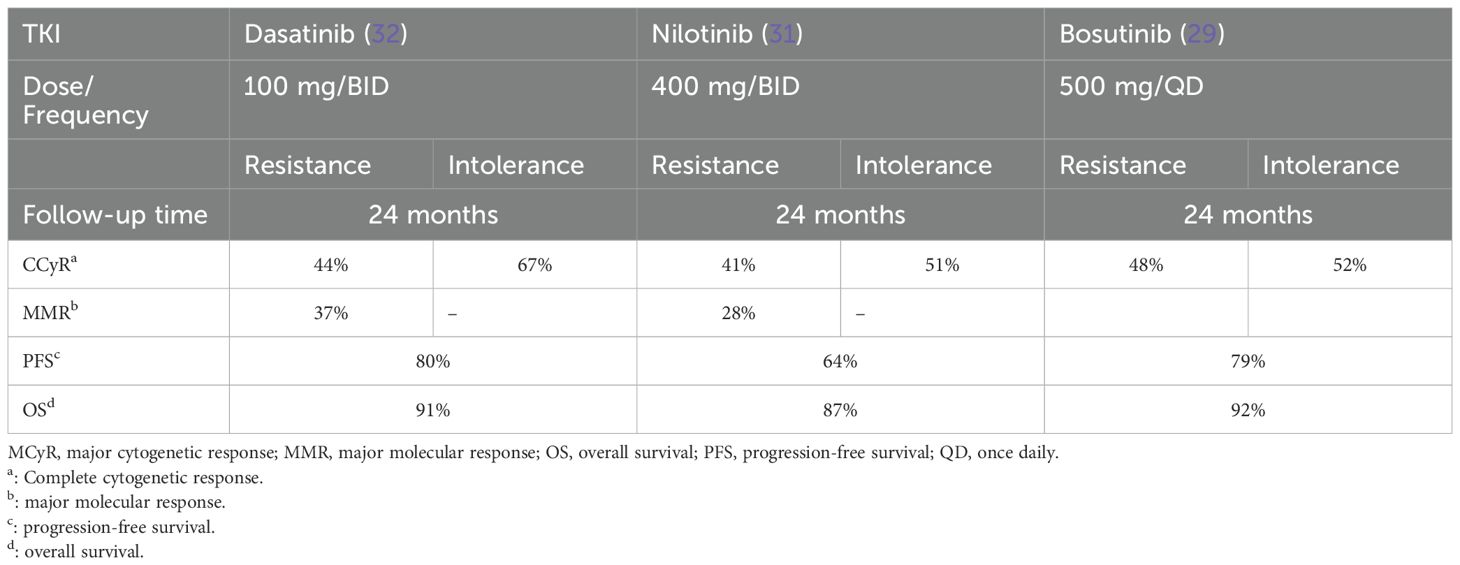
Table 2. Efficacy of second-generation TKIs after imatinib failure.
The efficacy and safety of bosutinib 500 mg QD was further evaluated in patients with CML who had previously failed TKI therapy and were otherwise ineligible for other TKIs in the post-approval phase 4 BYOND trial (32, 33). This was a single-arm, open-label, non-randomized study assessing the efficacy of second-, third-, and fourth-line bosutinib treatment (32, 33). To be considered a responder, the patient must have had maintenance of baseline response for ≥52 weeks for cytogenic response or an improvement from baseline (32, 33). Bosutinib was able to induce a cumulative MMR rate by 1 year of 70.5% in the overall Ph1 CP-CML cohort (32). After 3 years of follow-up, bosutinib continued to show efficacy in previously treated patients with Ph1 CP CML, with 71.8% of patients achieving or maintaining MMR (33). Among responders, the estimated probability of maintaining CCyR, MMR, or deep molecular response (DMR) was 96.5%, 87.2%, and 80.7%, respectively (33).
While there are no head-to-head comparative trials between bosutinib and other second-generation TKIs in the second- and later-line settings, a matching-adjusted indirect comparison analysis in patients receiving second-line treatment for CP-CML found that bosutinib had a longer progression-free survival (PFS) (hazard ratio 0.63) and overall survival (OS) (hazard ratio 0.82) than either dasatinib or nilotinib (34). However, it is worth noting that dasatinib and nilotinib showed higher rates of MCyR than bosutinib (34).
The safety and efficacy of bosutinib 500 mg QD in the setting of third-line CP-CML treatment was evaluated in patients who had previously been treated with imatinib, followed by dasatinib and/or nilotinib (35, 36). This phase 1/2 study included 118 individuals, most of them in the third-line setting (n=115) and the rest in the fourth-line setting (n=3). Patients were followed up for a median of 28.5 months and responses were divided according to resistance/intolerance to previous treatments (35). Among these patients, 32% achieved MCyR and 24% attained CCyR. Notably, bosutinib treatment resulted in CCyR in 1 out of 3 patients who had failed to respond to three prior TKIs (35). Patients with dasatinib intolerance (76%) and nilotinib resistance (86%) had a higher probability of maintaining MCyR at 2 years, compared to those with dasatinib resistance (34%) and nilotinib intolerance/prior treatment with all three TKIs (50%) (35). The 2-year estimated PFS was 73%, and estimated OS was 83% (36). The safety profile of bosutinib was deemed acceptable; the majority of TEAEs were GI issues of mild to moderate severity and rash (35). Long-term efficacy and tolerability results of this trial were consistent, demonstrating durable efficacy and a toxicity profile similar to previous bosutinib studies (36).
Regarding the specific findings of the BYOND trial, cumulative CCyR rates by 1 year were 83.9% and 73.3% for patients in the third-line and fourth-line settings, respectively (32). Cumulative MMR rate by 1 year was 74.5% for the patients in the third-line setting, and 56.3% for those in the fourth-line setting (32).
ASCEMBL is a phase 3, open-label, randomized study of asciminib vs. bosutinib in CML after two or more prior TKIs (37). In this study, asciminib demonstrated superior efficacy vs. bosutinib. One striking aspect was that bosutinib outcomes in ASCEMBL were worse than in the prior BYOND study (28, 29). Two factors could explain these findings. First, there was a higher proportion of resistant patients in the bosutinib arm; and second, patients failing bosutinib treatment due to a lack of efficacy were offered the possibility of switching to asciminib. However, patients who discontinued treatment with bosutinib because of intolerance (or any reason other than lack of efficacy) were not allowed to switch to asciminib. This might have impacted negatively on the percentage of patients who discontinued bosutinib.
Understanding their different modes of action is important for comprehending the efficacy and toxicity profile of each medication. Bosutinib is a second-generation TKI that inhibits the BCR::ABL1 protein by binding to its ATP-binding site, thereby blocking its tyrosine kinase activity (38). In contrast, asciminib is a first-in-class STAMP (Specifically Targeting the ABL Myristoyl Pocket) inhibitor that binds to the myristoyl pocket of the BCR::ABL1 protein, leading to its inactivation through an allosteric mechanism (39). The binding of asciminib outside of the ATP site may account for the greater efficacy demonstrated by this agent in the ASCEMBL study.
In our opinion, although asciminib has been shown to provide superior results, bosutinib remains a valid option in patients failing second-generation TKIs, with a high likelihood of treatment success, especially in cases with intolerance to prior TKIs. In patients who have previously been intolerant to TKIs, bosutinib may be a better alternative than asciminib due to its established safety profile, which showed a lower incidence of cardiovascular events in the ASCEMBL trial. This makes it a potential option for people who have pre-existing cardiovascular issues or are at high risk of such complications. Furthermore, while asciminib has shown higher effectiveness, bosutinib may still be useful in individuals who have developed resistance to several second-generation TKIs. The choice of treatment may be determined by the specific mutation profile and prior response patterns. Furthermore, due to its demonstrated efficacy in eliciting rapid cytogenetic and molecular responses, bosutinib may be considered in situations requiring a prompt treatment response. Of note, in the ASCEMBL study, bosutinib showed fewer cardiovascular events than asciminib, a topic that will be further explored in the management of AEs section of this review.
A subanalysis of the phase 1/2 open-label study evaluating the efficacy and safety of bosutinib as second-line therapy in CP-CML patients evaluated for the first time the durability of response and long-term safety of bosutinib in the fully enrolled advanced leukemia cohort (AP-CML, BP-CML, and Ph1 acute lymphoblastic leukemia {ALL]) during a follow-up of up to 4 years (40). Bosutinib demonstrated a durable response among the 167 patients included in the study, with 50% of AP responders sustaining an MCyR at 4 years (40). Furthermore, 25% of BP responders sustained their response to therapy after 1 year. Despite the small number of ALL patients that were included, some of them responded (40, 41).
Another study looked at the safety of combining inotuzumab ozogamicin (an antiCD22 recombinant humanized monoclonal antibody) with bosutinib as treatment for lymphoid BP-CML (42). The trial studied the role of this combination with three dose levels of bosutinib (300 mg/d, 400 mg/and 500 mg/d) in 18 patients with a median follow-up of 44 months. The maximum tolerated dose of bosutinib was 400 mg daily and dose limiting toxicities included grade 3 skin rashes (42). CMR was seen in 56% of patients (42). Thus, this drug combination resulted in high rates of morphologic and molecular response with an acceptable toxicity profile in this population.
Several reports on the real-world use of bosutinib have been published since its marketing approval (Table 3). The efficacy and safety of real-life bosutinib administration were retrospectively investigated in a cohort of 85 Italian patients who were resistant, refractory, or intolerant to multiple TKIs (43). The median age of this group was 60 years, as reported by Attolico et al. in 2018 (43). MMR/DMR was achieved by 46% of evaluable patients (43). In terms of safety, 88% of patients completed the study after a median follow-up of 26 months (range: 3-49 months). Fourteen patients (16%) experienced hematological toxicity, while 48% experienced extra-hematological toxicity. Dose reductions were required in four patients (5%) due to side effects, with diarrhea being the most common (43). Another study conducted in the United Kingdom and the Netherlands found that bosutinib, when used in routine clinical practice in CML patients in the third and fourth lines of treatment, achieved high rates of cumulative CCyR and MMR similar to those observed in clinical trials (67% and 55%, respectively) (44, 45). Remarkably, despite the fact that most patients had preexisting comorbidities, bosutinib was generally well tolerated, with the majority of patients not experiencing grade 3/4 AEs (45). The real-world performance of bosutinib in fourth-line treatment was also assessed in a Spanish cohort (46). Sixty-two patients with CP-CML who had been previously treated with imatinib, nilotinib, and dasatinib were retrospectively reviewed (46). The probability of either maintaining or improving CCyR was 25% in the subgroup of patients without CCyR at baseline and 94% in patients with CCyR at baseline (46). The probability of achieving MMR in patients who did not respond at baseline was 14% or 42% in patients with or without CCyR at baseline, respectively. Additionally, bosutinib had an acceptable safety profile in patients who had been intolerant to prior TKI therapy (46).
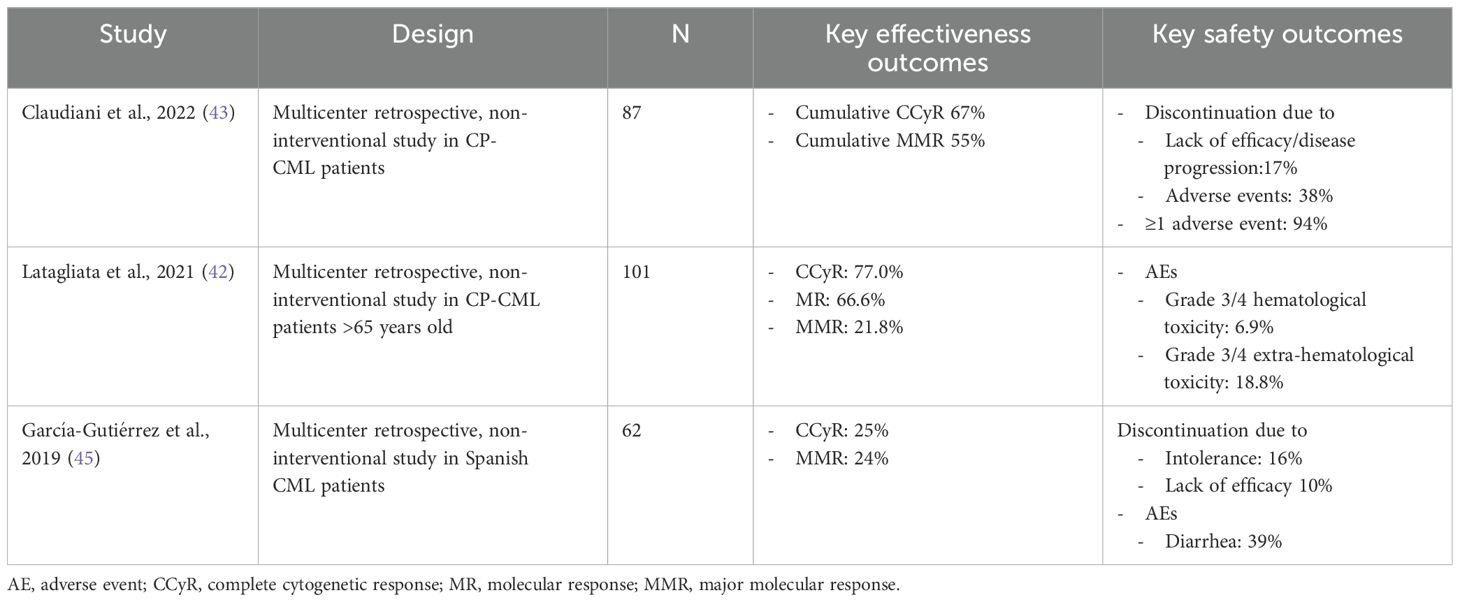
Table 3. Summary of effectiveness and safety results in a real-world setting after bosutinib treatment in CML patients.
In summary, findings from clinical trials and real-world evidence indicate that bosutinib is a viable therapeutic option for CP-CML patients who are resistant/intolerant to multiple TKIs.
Multiple studies on bosutinib dose optimization in CML patients have been reported (Table 4). In frontline treatment of CP-CML, an analysis including patients participating in the BFORE trial who had a bosutinib dose reduction to 300 mg for toxicity-related issues (or to 200 mg QD for four weeks maximum, after which dose escalation or treatment discontinuation was required) (47) evaluated the effectiveness of a lower dose of bosutinib. Thirty-one percent of the patients in the bosutinib arm had their dosage reduced to 300 mg QD (without further reduction) and 12% to 200 mg (47). Among patients who had a dose reduction to 300 mg QD, 62% had maintained MMR for >6 months afterwards, in comparison to 78% of the patients who remained on 400 mg achieving MMR (47). In fact, 17% of patients who reduced the dose to 300 mg QD maintained MMR before and after dose reduction, and 45% of them achieved MMR for the first time after decreasing the dose (47). In patients who had their bosutinib dosage reduced to 200 mg QD, 36% obtained MMR >6 months later, 21% maintained MMR before and after the decrease, and 15% achieved MMR for the first time after the dose was lowered (47). At the safety level, the incidence of diarrhea, thrombocytopenia, nausea, vomiting, and anemia decreased by more than 10% in individuals whose bosutinib dosage was reduced to 300 mg QD or 200 mg QD, with additional decreases in abdominal pain, fatigue, and rash after dose reduction to 200 mg QD (47). Thus, the study showed that management of AEs through bosutinib dose reduction enabled patients to continue on treatment, maintaining its efficacy while improving tolerability.
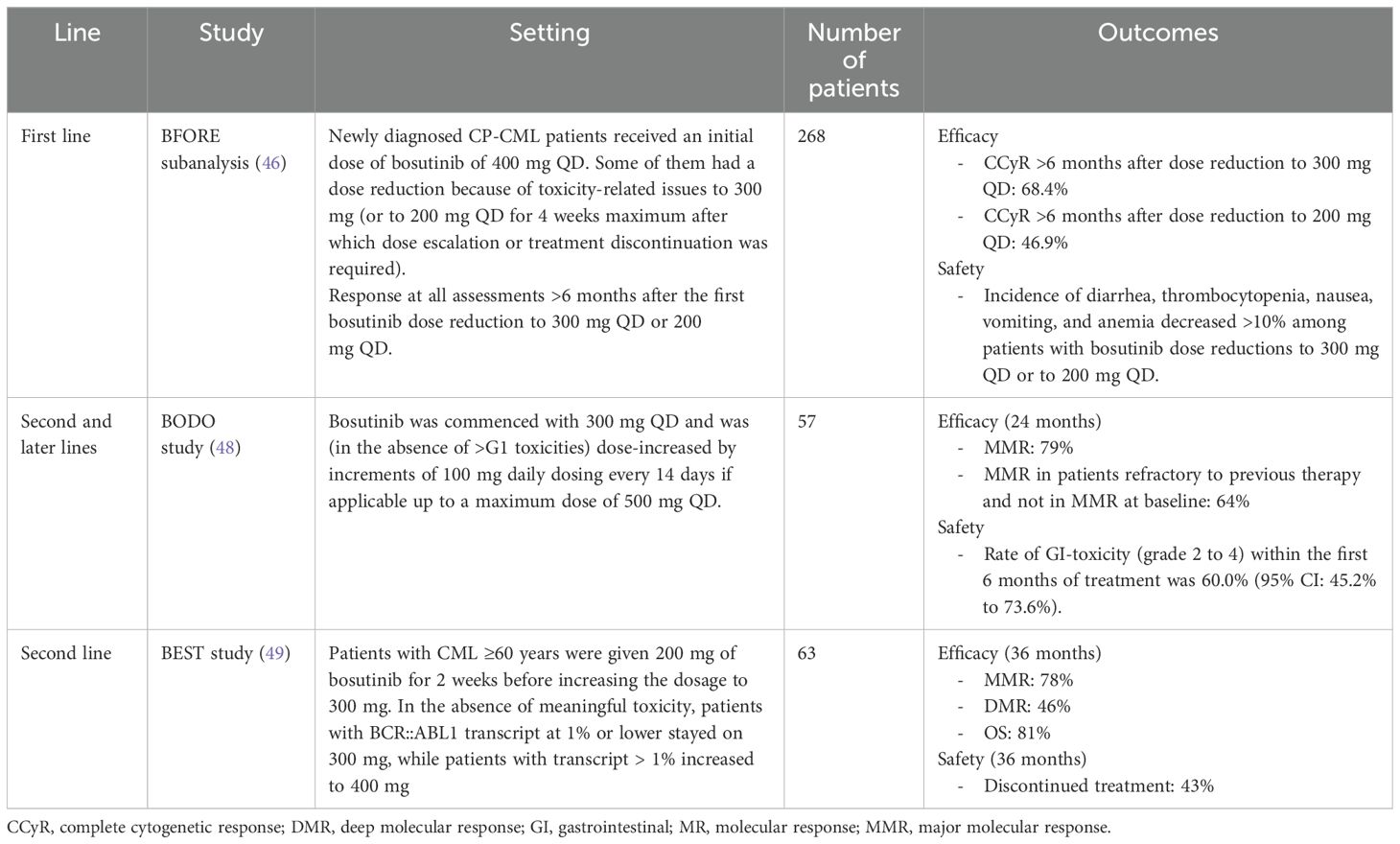
Table 4. Summary of dose optimization studies with bosutinib.
More recently, pharmacokinetic population modeling was conducted to quantify the impact of reducing the initial dosage of bosutinib from 500 to 400 mg QD (48). The analysis integrated data from the BELA and BFORE studies and from trial B1871048 (a phase 2 study of first-line bosutinib in CP-CML in a newly diagnosed Japanese cohort).The exposure-response efficacy analysis revealed that cumulative MMR and CCyR were comparable in patients in the BFORE and B1871048 trials who had a starting dosage of 400 mg QD and those in the BELA trial who were given a starting dose of 500 mg QD (48). Additionally, in terms of safety, patients in the BFORE and B1871048 trials who received a starting dose of 400 mg QD had a lower rate of permanent discontinuation due to AEs (48). Overall, the results suggest that a bosutinib starting dose of 400 mg QD improves tolerability without affecting the efficacy in newly diagnosed adult CP-CML patients.
Another trial investigating the effect of a bosutinib step-in dosing regimen in reducing GI toxicity was focused in patients with CML after failure or intolerance to other second-generation TKIs (49). In this phase 2 trial, the “Bosutinib Dose Optimization Study” (BODO; NCT02577926), the bosutinib starting dose was 300 mg QD and was increased by increments of 100 mg daily dosing every 14 days in the absence of grade 1 or higher toxicities up to a maximum dose of 500 mg (49). Although the advantage of the step-in dosing concept in lowering the frequency of GI toxicity could not be demonstrated because of incomplete recruitment, this regimen of bosutinib administration, with a mean bosutinib dosage of 403 mg/day, induced optimal responses in 64% of patients refractory to previous therapy and not in MMR at baseline, while GI toxicity rarely led to treatment discontinuation (49).
A subanalysis of the BEST study sought to determine the effectiveness of initial low-dose bosutinib in elderly CML patients in the second-line setting, considering that the fixed starting dosage of 500 mg QD may still be too high for this subpopulation (50). The study was designed so that participants over the age of 60 were given 200 mg of bosutinib for 2 weeks before increasing the dosage to 300 mg (50). In the absence of meaningful toxicity, patients with BCR::ABL1 transcript at 1% or lower stayed on 300 mg, while patients with transcript >1% increased to 400 mg (50). The study revealed that the likelihood of reaching or maintaining MR by 36 months was 78% (36). Moreover, the majority of patients stayed on 300 mg or less of bosutinib (50).
The appropriate management of low-grade persistent AEs is becoming increasingly important in CML patients, particularly given the possibility of lifetime TKI therapy. However, data is limited as regards the timing and management of AEs associated with long-term TKI therapy.
The low incidence of adverse effects related to bosutinib treatment is worth noting, although GI AEs, specifically diarrhea, are expected. The incidence of moderate-grade adverse effects has not exceeded 20% in clinical trials and in routine clinical practice, particularly within the first 12 months of treatment initiation (51).
Although diarrhea is frequent in CML patients taking bosutinib as second- or later-line therapy (around 85% of patients) (51), the prevalence of grade 3/4 diarrhea episodes is lower (approximately 9.5% of patients) (36, 52). Nausea, vomiting, and abdominal discomfort are also among other GI TEAEs associated with bosutinib (36, 52). It is recommended that all patients receiving bosutinib be assessed for diarrhea and signs of dehydration (53, 54). Non-pharmacological treatment options include dose reduction, increased fiber consumption, and abstaining from foods or ingredients that can cause loose stools (such as alcohol, lactose-containing products, laxatives/stool softeners, raw fruits and vegetables, spicy or fatty meals, caffeine, etc.) (51). Proton pump inhibitors should be avoided due to the potential reduction in bosutinib exposure (19). Pharmacological therapies include mostly drugs that reduce stool discharge, such as antidiarrheals; antiemetics and/or fluid replacement are also used (51). In practice, the majority of affected individuals are treated for diarrhea with concomitant antidiarrheal drugs, most often loperamide (51).
Studies concerning the concomitant administration of symbiotics to mitigate the incidence of GI disorders remain limited in the scientific literature. However, a preliminary exploration conducted in a small-scale pilot study (55) detailed the clinical observations derived from the treatment of 35 patients with bosutinib concomitantly supplemented with a symbiotic regimen. Notably, the findings demonstrated a statistically significant reduction in GI adverse effects associated with bosutinib administration (55). Furthermore, the symbiotic intervention exhibited a beneficial impact on treatment adherence and quality of life parameters pertaining to GI health (55). While further research is needed, these findings suggest the potential of symbiotics in mitigating bosutinib-induced GI complications, offering avenues for improved patient outcomes and therapeutic compliance.
Hepatotoxicity TEAEs are seen in around 25% of patients receiving bosutinib as a second-line therapy, with occurrence of grade 3/4 hepatotoxicity, specifically increased alanine and aspartate aminotransferase (ALT/AST) levels observed in 11% of patients (51). Transient dosage pauses in 37% of patients, dose reductions, or concomitant medicines were used to manage patients with high ALT/AST levels (51). These TEAEs had an average duration of 26 days, indicating that bosutinib hepatotoxicity can be reversed with a change in dosage or a temporary discontinuation in therapy. Of note, 74% of patients who resumed bosutinib after ALT/AST elevations did not experience additional ALT/AST events (51). However, permanent discontinuation should be considered if the patient does not respond to dose adjustment or continues.
Cardiac and vascular AEs are infrequent with bosutinib, as only 3.9% of patients have been reported to develop grade III-IV cardiovascular toxicities (56). In the ASCMBL trial comparing asciminib with bosutinib, a higher number of patients developed cardiovascular disease in the asciminib arm (3.2%) compared with the bosutinib cohort (1.3%) (37). Furthermore, these incidence rates seem to be lower than other second-generation TKI historic data (56). Dose interruption has been demonstrated to be effective in the management of those patients who develop cardiac TEAEs (51). Indeed, the majority of the patients whose bosutinib was interrupted were successfully retreated (56). Concomitant medication (47%) or dose reduction (5%) were other management strategies (51).
Regarding hematological toxicities, thrombocytopenia is the most frequently reported (around 40% of patients) and the most common reason for temporary treatment discontinuation or dosage reduction (15, 51).
Bosutinib has been associated with pulmonary side effects, such as pleural effusion (PE), occurring at a rate of 4% to 8% in long-term safety trials (27, 28, 41). Interestingly, it has been shown that, in certain individuals, bosutinib might worsen dasatinib-induced pulmonary arterial hypertension and PE (57). However, a recent retrospective study found that 70% of patients who were treated with bosutinib in second or subsequent lines after having one or more PE events while on dasatinib therapy did not develop PE during the study treatment (58), suggesting that bosutinib may be a valid therapeutic choice in CML in a selected population of patients who developed PE while on dasatinib treatment.
In the context of renal dysfunction, the prevalence of elevated blood creatinine levels, irrespective of severity, among patients in the CP second-line cohort undergoing bosutinib treatment was increased during years 3 and 4 compared to the initial 2 years (36, 52). Similarly, within the CP third-line cohort, the incidence was notably elevated in the fourth year relative to preceding years (36, 52). Nevertheless, long-term administration of bosutinib appears to induce a reversible decline in renal function, demonstrating a frequency and characteristics akin to those observed with prolonged imatinib use (59). Nevertheless, optimal management necessitates vigilant patient assessment for manifestations of renal dysfunction, such as alterations in urinary frequency, polyuria, or oliguria (51). Continuous monitoring of renal function, especially in patients with preexisting renal impairment or predisposing factors for renal dysfunction should be performed (51). The recommended starting dose of bosutinib varies based on creatinine clearance (CrCL) levels: for CrCL 30–50 ml/min, the recommended starting dose is 400 mg/day, while for CrCL <30 ml/min, the starting dose is reduced to 300 mg/day (51).
TKI therapy should be discontinued in case of pregnancy (19). Despite this general recommendation, some patients require treatment with a TKI during pregnancy. Clinical data has been reported mostly with imatinib, mainly in the third trimester. As regards experience with bosutinib in this setting, despite preclinical studies showing reproductive toxicity (16, 19), clinical data on the risk of teratogenesis or miscarriage is scarce. In clinical practice, a recent report including 33 pregnancies noted that 15 of them (45.5%) resulted in healthy newborns, and nine resulted in abortions, although none of these were considered by the healthcare provider to be related to bosutinib treatment (60). Moreover, there is also a risk of diminished fertility (female/male) with bosutinib, according to preclinical studies (16, 19). Female patients should have a pregnancy test before beginning bosutinib medication, and adequate contraception should be used during treatment and for ≥1 month after the last dose to avoid becoming pregnant while receiving bosutinib (16). Patients should also be informed about the risks of using bosutinib during pregnancy (19). For male patients, there are no current restrictions. Despite limited published experience, no association has been identified between men on bosutinib treatment and the occurrence of miscarriages in their partners or malformations in full-term pregnancies (60). On the other hand, although there are safety reports on the use of imatinib in the third trimester, the National Comprehensive Cancer Network and European Leukemia Net guidelines clearly advise against using any TKI during pregnancy (53, 54).
Imatinib is the first-line treatment recommended in pediatric CML patients (61). However, 30% of children have suboptimal response to imatinib (61). Bosutinib is not currently licensed for use in children in Europe, although it has been recently approved in the USA for use in children starting from the age of 1 year (62). Pediatric patients who are intolerant or do not respond to imatinib or second-generation TKIs may benefit from the approval of bosutinib. A phase 1/2 study of bosutinib in 23 patients with newly diagnosed or resistant/intolerant Ph1 CML (63) established 300 mg/m2 QD as the recommended phase 2 dose (63). For resistant or intolerant individuals, 400 mg/m2 QD provided exposure equivalent to 500 mg QD in adults, with comparable preliminary effectiveness to other second-generation TKIs (63).
Drug interactions also need to be considered when choosing a TKI in CML patients. Bosutinib has been shown to have a particular interaction profile (64). All second-generation TKIs block the BCR::ABL1 tyrosine kinase, and are often non-selective medications that can inhibit other tyrosine kinases, such as cKIT or PDGFR (64). These medications are taken orally and have intermediate bioavailability, a large volume of distribution, strong protein binding, and elimination following extensive metabolism involving different cytochrome P450 (64). Because all BCR::ABL1 inhibitors are cytochrome P450 substrates, their rate of elimination can be influenced by other medications that enhance or decrease the activity of these isoenzymes. Furthermore, dasatinib, imatinib, nilotinib, and ponatinib control CYP450 interaction by inhibiting the enzyme activity of several of the isoenzymes (64). Bosutinib does not share this property, suggesting that it might be a good treatment option for patients who are polymedicated as it prevents possible drug-drug interactions, although no specific recommendations have been published in this regard.
A retrospective review of CP-CML patients receiving bosutinib or ponatinib who discontinued treatment in a real-life single-center study in the USA showed that among the eight patients who discontinued bosutinib (65), safety was similar to discontinuation with other TKIs. Patients who had lost MMR responded after restarting treatment (65). In Spain, a discontinuation study (BOSUTRF) is ongoing.
As previously mentioned, both controlled trials [BEST study (50)] and real-world data (43) show that bosutinib is effective and safe in older patients with significant comorbidities and resistance or intolerance to earlier TKIs. Efficacy results are comparable to those in younger patients, with a reported CCyR of 77% in the real-world setting (43). Tolerability in the elderly is also comparable to the younger population (43). Nevertheless, the use of bosutinib in this age group depends on various factors: comorbidities, other drug interactions and supportive care. Ultimately, the use of bosutinib in older adults is determined on a case-by-case basis and should be evaluated by the patient’s healthcare team.
Based on data reviewed in the present document, our conclusions on the use of bosutinib in clinical practice are as follows:
● Among second-generation TKIs, bosutinib could provide a clinical advantage in patients with cardiovascular risk factors.
● Long-term data demonstrate the safety of bosutinib in this setting.
● In cases of resistance or intolerance to imatinib, bosutinib has shown similar efficacy to other second-generation TKIs, with an optimal safety profile and low incidence of adverse events.
● In third-line treatment, bosutinib has proven effective in sustaining previous responses in patients who discontinued treatment due to intolerance following prior second-generation TKI failure.
● Bosutinib has proven to be effective in older individuals. Due to its favorable drug interaction profile, bosutinib is an adequate therapeutic option for patients with multiple medications.
● As bosutinib does not contain lactose in its formulation, it should be recommended in patients with lactose intolerance.
● The recommended dosage for first-line treatment is 400 mg, while for second and subsequent lines, it is 500 mg. If intolerance is the reason for therapeutic failure, doses lower than 500 mg are recommended from treatment initiation. In certain cases, especially in older patients, starting with 300 mg and escalating to 400 mg may be considered to improve drug tolerance and achieve favorable molecular responses.
VG-G: Writing – review & editing, Writing – original draft, Methodology, Conceptualization. MG-C: Project administration, Investigation, Data curation, Writing – review & editing, Writing – original draft. BX: Writing – review & editing, Writing – original draft, Validation, Methodology, Investigation, Data curation. FC-M: Writing – review & editing, Writing – original draft, Supervision, Investigation, Conceptualization. GO: Writing – review & editing, Writing – original draft, Investigation, Data curation. PG: Writing – review & editing, Writing – original draft, Validation, Investigation, Data curation. JH-B: Writing – review & editing, Writing – original draft, Conceptualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Miranda-Filho A, Piñeros M, Ferlay J, Soerjomataram I, Monnereau A, Bray F. Epidemiological patterns of leukaemia in 184 countries: a population-based study. Lancet Haematology. (2018) 5:e14–24. doi: 10.1016/S2352-3026(17)30232-6
2. Rinaldi I, Winston K. Chronic myeloid leukemia, from pathophysiology to treatment-free remission: A narrative literature review. J Blood Med. (2023) 14:261–77. doi: 10.2147/JBM.S382090
3. Younes S, Ismail MA, Al-Jurf R, Ziyada A, Nasrallah GK, Abdulrouf PV, et al. Management of chronic myeloid leukaemia: current treatment options, challenges, and future strategies. Hematology. (2023) 28:2196866. doi: 10.1080/16078454.2023.2196866
4. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. WHO classification of tumours of haematopoietic and lymphoid tissues Vol. 2. Lyon, France: International agency for research on cancer (2008).
5. Khoury JD, Solary E, Abla O, Akkari Y, Alaggio R, Apperley JF, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia. (2022) 36:1703–19. doi: 10.1038/s41375-022-01613-1
6. Arber DA, Orazi A, Hasserjian RP, Borowitz MJ, Calvo KR, Kvasnicka HM, et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood J. (2022) 140:1200–28. doi: 10.1182/blood.2022015850
7. Niederwieser C, Kroger N. Transplantation in CML in the TKI era: who, when, and how? Hematol Am Soc Hematol Educ Program. (2022) 2022:114–22. doi: 10.1182/hematology.2022000329
8. Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. Am J Hematol. (2020) 95:691–709. doi: 10.1002/ajh.25792
9. Sasaki K, Strom SS, O'Brien S, Jabbour E, Ravandi F, Konopleva M, et al. Relative survival in patients with chronic-phase chronic myeloid leukaemia in the tyrosine-kinase inhibitor era: analysis of patient data from six prospective clinical trials. Lancet Haematol. (2015) 2:e186–93. doi: 10.1016/S2352-3026(15)00048-4
10. Koschmieder S, Keller VA. Profile of bosutinib and its clinical potential in the treatment of chronic myeloid leukemia. OncoTargets Ther. (2013) p:99. doi: 10.2147/OTT
11. Hochhaus A, Baccarani M, Silver RT, Schiffer C, Apperley JF, Cervantes F, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. (2020) 34:966–84. doi: 10.1038/s41375-020-0776-2
12. Apperley JF. Chronic myeloid leukaemia. Lancet. (2015) 385:1447–59. doi: 10.1016/S0140-6736(13)62120-0
13. Hochhaus A, Saussele S, Rosti G, Mahon FX, Janssen JJWM, Hjorth-Hansen H, et al. Chronic myeloid leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2018) 29:iv261. doi: 10.1093/annonc/mdy159
14. Vener C, Banzi R, Ambrogi F, Ferrero A, Saglio G, Pravettoni G, et al. First-line imatinib vs second- and third-generation TKIs for chronic-phase CML: a systematic review and meta-analysis. Blood Adv. (2020) 4:2723–35. doi: 10.1182/bloodadvances.2019001329
15. Gambacorti-Passerini C, Cortes JE, Lipton JH, Dmoszynska A, Wong RS, Rossiev V, et al. Safety of bosutinib versus imatinib in the phase 3 BELA trial in newly diagnosed chronic phase chronic myeloid leukemia. Am J Hematol. (2014) 89:947–53. doi: 10.1002/ajh.23788
16. European Medicines Agency (EMA). Summary of product characteristics. EupreaBosulif: EPAR - Product Information. Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/bosulif. (accessed May 17, 2023)
17. Abbas R, Hsyu PH. Clinical pharmacokinetics and pharmacodynamics of bosutinib. Clin Pharmacokinet. (2016) 55:1191–204. doi: 10.1007/s40262-016-0391-6
18. Abbas R, Hug BA, Leister C, Gaaloul ME, Chalon S, Sonnichsen D. A phase I ascending single-dose study of the safety, tolerability, and pharmacokinetics of bosutinib (SKI-606) in healthy adult subjects. Cancer Chemother Pharmacol. (2012) 69:221–7. doi: 10.1007/s00280-011-1688-7
20. Cortes JE, Kim DW, Kantarjian HM, Brümmendorf TH, Dyagil I, Griskevicius L, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: results from the BELA trial. J Clin Oncol. (2012) 30:3486–92. doi: 10.1200/JCO.2011.38.7522
21. Cortes JE, Gambacorti-Passerini C, Deininger MW, Mauro MJ, Chuah C, Kim DW, et al. Bosutinib versus imatinib for newly diagnosed chronic myeloid leukemia: results from the randomized BFORE trial. J Clin Oncol. (2018) 36:231–7. doi: 10.1200/JCO.2017.74.7162
22. Cortes JE, Mauro MJ, Deininger MW, Chuah C, Kim DW, Kota V, et al. Bosutinib vs imatinib for newly diagnosed chronic myeloid leukemia in the BFORE trial: 24-month follow-up. J Clin Oncol. (2018) 36:7002–2. doi: 10.1200/JCO.2018.36.15_suppl.7002
23. Brummendorf TH, Cortes JE, Milojkovic D, Gambacorti-Passerini C, Clark RE, et al. Bosutinib versus imatinib for newly diagnosed chronic phase chronic myeloid leukemia: final results from the BFORE trial. Leukemia. (2022) 36:1825–33. doi: 10.1038/s41375-022-01589-y
24. Ono T, Hino M, Matsumura I, Fujisawa S, Ishizawa K, Sakaida E, et al. Bosutinib in Japanese patients with newly diagnosed chronic-phase chronic myeloid leukemia: final 3-year follow-up results of a phase 2 study. Int J Hematol. (2022) 116:871–82. doi: 10.1007/s12185-022-03435-4
25. Muresan B, Mamolo C, Cappelleri JC, Leip E, Viqueira A, Heeg B. An indirect comparison between bosutinib, nilotinib and dasatinib in first-line chronic phase chronic myeloid leukemia. Curr Med Res Opin. (2021) 37:801–9. doi: 10.1080/03007995.2021.1896489
26. Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. (2022) 43:4229–361. doi: 10.1093/eurheartj/ehac244
27. Cortes JE, Kantarjian HM, Brümmendorf TH, Kim DW, Turkina AG, Shen ZX, et al. Safety and efficacy of bosutinib (SKI-606) in chronic phase Philadelphia chromosome-positive chronic myeloid leukemia patients with resistance or intolerance to imatinib. Blood. (2011) 118:4567–76. doi: 10.1182/blood-2011-05-355594
28. Gambacorti-Passerini C, Brümmendorf TH, Kim DW, Turkina AG, Masszi T, Assouline S, et al. Bosutinib efficacy and safety in chronic phase chronic myeloid leukemia after imatinib resistance or intolerance: Minimum 24-month follow-up. Am J Hematol. (2014) 89:732–42. doi: 10.1002/ajh.23728
29. Gambacorti-Passerini C, Cortes JE, Lipton JH, Kantarjian HM, Kim DW, Schafhausen P, et al. Safety and efficacy of second-line bosutinib for chronic phase chronic myeloid leukemia over a five-year period: final results of a phase I/II study. Haematologica. (2018) 103:1298–307. doi: 10.3324/haematol.2017.171249
30. Giles FJ, le Coutre PD, Pinilla-Ibarz J, Larson RA, Gattermann N, Ottmann OG, et al. Nilotinib in imatinib-resistant or imatinib-intolerant patients with chronic myeloid leukemia in chronic phase: 48-month follow-up results of a phase II study. Leukemia. (2013) 27:107–12. doi: 10.1038/leu.2012.181
31. Shah NP, Guilhot F, Cortes JE, Schiffer CA, le Coutre P, Brümmendorf TH, et al. Long-term outcome with dasatinib after imatinib failure in chronic-phase chronic myeloid leukemia: follow-up of a phase 3 study. Blood. (2014) 123:2317–24. doi: 10.1182/blood-2013-10-532341
32. Hochhaus A, Gambacorti-Passerini C, Abboud C, Gjertsen BT, Brümmendorf TH, Smith BD, et al. Bosutinib for pretreated patients with chronic phase chronic myeloid leukemia: primary results of the phase 4 BYOND study. Leukemia. (2020) 34:2125–37. doi: 10.1038/s41375-020-0915-9
33. Gambacorti-Passerini C, Brümmendorf TH, Abruzzese E, Kelly KR, Oehler VG, Garcia-Gutierrez V, et al. Efficacy and safety of bosutinib in previously treated patients with chronic myeloid leukemia: final results from the byond trial. Blood. (2021) 138:1475. doi: 10.1182/blood-2021-150352
34. Cortes JE, Muresan B, Mamolo C, Cappelleri JC, Crescenzo RJ, Su Y, et al. Matching-adjusted indirect comparison of bosutinib, dasatinib and nilotinib effect on survival and major cytogenetic response in treatment of second-line chronic phase chronic myeloid leukemia. Curr Med Res Opin. (2019) 35:1615–22. doi: 10.1080/03007995.2019.1605239
35. Khoury HJ, Cortes JE, Kantarjian HM, Gambacorti-Passerini C, Baccarani M, Kim DW, et al. Bosutinib is active in chronic phase chronic myeloid leukemia after imatinib and dasatinib and/or nilotinib therapy failure. Blood. (2012) 119:3403–12. doi: 10.1182/blood-2011-11-390120
36. Cortes JE, Khoury HJ, Kantarjian HM, Lipton JH, Kim DW, Schafhausen P, et al. Long-term bosutinib for chronic phase chronic myeloid leukemia after failure of imatinib plus dasatinib and/or nilotinib. Am J Hematol. (2016) 91:1206–14. doi: 10.1002/ajh.24536
37. Rea D, Mauro MJ, Boquimpani C, Minami Y, Lomaia E, Voloshin S, et al. A phase 3, open-label, randomized study of asciminib, a STAMP inhibitor, vs bosutinib in CML after 2 or more prior TKIs. Blood. (2021) 138:2031–41. doi: 10.1182/blood.2020009984
38. Isfort S, Crysandt M, Gezer D, Koschmieder S, Brümmendorf TH, Wolf D. Bosutinib: A Potent Second-Generation Tyrosine Kinase Inhibitor. Recent results in cancer research. Fortschritte der Krebsforschung. Progres dans les recherches sur le Cancer. (2018) 212:87–108. doi: 10.1007/978-3-319-91439-8_4
39. Hochhaus A, Réa D, Boquimpani C, Minami Y, Cortes JE, Hughes TP, et al. Asciminib vs bosutinib in chronic-phase chronic myeloid leukemia previously treated with at least two tyrosine kinase inhibitors: longer-term follow-up of ASCEMBL. Leukemia. (2023) 37:617–26. doi: 10.1038/s41375-023-01829-9
40. Gambacorti-Passerini C, Kantarjian HM, Kim DW, Khoury HJ, Turkina AG, Brümmendorf TH, et al. Long-term efficacy and safety of bosutinib in patients with advanced leukemia following resistance/intolerance to imatinib and other tyrosine kinase inhibitors. Am J Hematol. (2015) 90:755–68. doi: 10.1002/ajh.24034
41. Brummendorf TH, Cortes JE, de Souza CA, Guilhot F, Duvillié L, Pavlov D, et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukaemia: results from the 24-month follow-up of the BELA trial. Br J Haematol. (2015) 168:69–81. doi: 10.1111/bjh.13108
42. Jain N, Maiti A, Ravandi F, Konopleva M, Daver N, Kadia T, et al. Inotuzumab ozogamicin with bosutinib for relapsed or refractory Philadelphia chromosome positive acute lymphoblastic leukemia or lymphoid blast phase of chronic myeloid leukemia. Am J Hematol. (2021) 96:1000–7. doi: 10.1002/ajh.26238
43. Costa A, Abruzzese E, Latagliata R, Mulas O, Carmosino I, Scalzulli E, et al. Real life evaluation of efficacy and safety of bosutinib therapy in chronic myeloid leukemia patients. Blood. (2018) 132:3021–1. doi: 10.1182/blood-2018-99-113427
44. Claudiani S, Janssen JJWM, Byrne J, Smith G, Blijlevens N, Raghavan M, et al. A retrospective observational research study to describe the real-world use of bosutinib in patients with chronic myeloid leukemia in the United Kingdom and the Netherlands. Eur J Haematol. (2022) 109:90–9. doi: 10.1111/ejh.13775
45. Apperley JF, Byrne JL, Smith G, Claudiani S, Viqueira A, Ferdinand R, et al. The real world use of bosutinib in patients with chronic myeloid leukaemia. Blood. (2016) 128:5435. doi: 10.1182/blood.V128.22.5435.5435
46. Garcia-Gutierrez V, Milojkovic D, Hernandez-Boluda JC, Claudiani S, Martin Mateos ML, Casado-Montero LF, et al. Safety and efficacy of bosutinib in fourth-line therapy of chronic myeloid leukemia patients. Ann Hematol. (2019) 98:321–30. doi: 10.1007/s00277-018-3507-2
47. Deininger MW, Brümmendorf TH, Milojkovic D, Cervantes F, Huguet F, Viqueira A, et al. Outcomes before and after dose reduction in patients with newly diagnosed chronic myeloid leukemia receiving bosutinib or imatinib. J Clin Oncol. (2021) 39:7039–9. doi: 10.1200/JCO.2021.39.15_suppl.7039
48. Garrett M, Knight B, Cortes JE, Deininger MW. Population modeling of bosutinib exposure-response in patients with newly diagnosed chronic phase chronic myeloid leukemia. Cancer Med. (2023) 12(17):17981–92. doi: 10.1002/cam4.6439
49. Isfort S, Manz K, Teichmann LL, Crysandt M, Burchert A, Hochhaus A, et al. Step-in dosing of bosutinib in pts with chronic phase chronic myeloid leukemia (CML) after second-generation tyrosine kinase inhibitor (TKI) therapy: results of the Bosutinib Dose Optimization (BODO) Study. Ann Hematol. (2023) 102:2741–52. doi: 10.1007/s00277-023-05394-0
50. Castagnetti F, Bocchia M, Abruzzese E, Capodann I, Bonifacio M, Rege Cambrin G, et al. P698: Bosutinib dose optimization in the second-line treatment of elderly cml patients: extended 3-year follow-up and final results of the best study. HemaSphere. (2022) 6:593–4. doi: 10.1097/01.HS9.0000845676.81208.c2
51. Khoury HJ, Gambacorti-Passerini C, Brummendorf TH. Practical management of toxicities associated with bosutinib in patients with Philadelphia chromosome-positive chronic myeloid leukemia. Ann Oncol. (2018) 29:578–87. doi: 10.1093/annonc/mdy019
52. Brümmendorf TH, Cortes JE, Khoury HJ, Kantarjian HM, Kim DW, Schafhausen P, et al. Factors influencing long-term efficacy and tolerability of bosutinib in chronic phase chronic myeloid leukaemia resistant or intolerant to imatinib. Br J Haematology. (2016) 172:97–110. doi: 10.1111/bjh.13801
53. Steegmann JL, Baccarani M, Breccia M, Casado LF, García-Gutiérrez V, Hochhaus A, et al. European LeukemiaNet recommendations for the management and avoidance of adverse events of treatment in chronic myeloid leukaemia. Leukemia. (2016) 30:1648–71. doi: 10.1038/leu.2016.104
54. Radich JP, Deininger M, Abboud CN, Altman JK, Berman E, Bhatia R, et al. Chronic myeloid leukemia, version 1.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2018) 16:1108–35. doi: 10.6004/jnccn.2018.0071
55. Medrano-Engay B, Gomez-Notario CJ, Alcedo J, Giraldo P. POSTER PC-353-Simbiótico conteniendo Bacillus Coagulans lmg-s-24828 y prebióticos en la reducción de trastornos gastrointestinales secundarios al tratamiento farmacológico de enfermedades hematológicas crónicas. Estudio piloto. In: LX Congreso Nacional de la Sociedad Española de Hematología y Hemoterapia. GRANADA: Sociedad Española de Hematologia y Hemoterapia (2018).
56. Cortes JE, Kantarjian HM, Mauro MJ, An F, Nick S, Leip E, et al. Long-term cardiac, vascular, hypertension, and effusion safety of bosutinib in patients with Philadelphia chromosome-positive leukemia resistant or intolerant to prior therapy. Eur J Haematol. (2021) 106:808–20. doi: 10.1111/ejh.13608
57. Riou M, Seferian A, Savale L, Chaumais MC, Guignabert C, Canuet M, et al. Deterioration of pulmonary hypertension and pleural effusion with bosutinib following dasatinib lung toxicity. Eur Respir J. (2016) 48:1517–9. doi: 10.1183/13993003.01410-2016
58. Tiribelli M, Abruzzese E, Capodanno I, Sorà F, Trabacchi E, Iurlo A, et al. Efficacy and safety of bosutinib in chronic phase CML patients developing pleural effusion under dasatinib therapy. Ann Hematol. (2019) 98:2609–11. doi: 10.1007/s00277-019-03802-y
59. Cortes JE, Gambacorti-Passerini C, Kim DW, Kantarjian HM, Lipton JH, Lahoti A, et al. Effects of bosutinib treatment on renal function in patients with philadelphia chromosome-positive leukemias. Clin Lymphoma Myeloma Leuk. (2017) 17:684–695 e6. doi: 10.1016/j.clml.2017.06.001
60. Cortes JE, Gambacorti-Passerini C, Deininger M, Abruzzese E, DeAnnuntis L, Brümmendorf TH. Pregnancy outcomes in patients treated with bosutinib. Int J Hematol Oncol. (2020) 9:IJH26. doi: 10.2217/ijh-2020-0004
61. Suttorp M, Schulze P, Glauche I, Göhring G, von Neuhoff N, Metzler M, et al. Front-line imatinib treatment in children and adolescents with chronic myeloid leukemia: results from a phase III trial. Leukemia. (2018) 32:1657–69. doi: 10.1038/s41375-018-0179-9
62. Brivio E, Pennesi E, Willemse ME, Huitema ADR, Jiang Y, van Tinteren HDR, et al. Bosutinib in resistant and intolerant pediatric patients with chronic phase chronic myeloid leukemia: results from the phase I part of study ITCC054/COG AAML1921. J Clin Oncol. (2023), JCO2300897. doi: 10.1200/JCO.23.00897
63. Pennesi E, Brivio E, Willemse ME, Huitema ADR, Chandra S, Vijayakumar A, et al. A phase I/II study of bosutinib in pediatric patients with resistant/intolerant or newly diagnosed philadelphia chromosome-positive chronic myeloid leukemia, study ITCC (Innovative therapies for children with cancer european consortium) 054 and COG (Children’s oncology group consortium) AAML1921: results from the phase I trial in resistant/intolerant patients. Blood. (2021) 138:2558–8. doi: 10.1182/blood-2021-145709
64. Azanza JR, Sadaba B, Díez N. Comparative pharmacology of tyrosine kinase inhibitors for the treatment of chronic myeloid leukemia. Int J Clin Pharmacol Pharmacother. (2018) 3:134. doi: 10.15344/2456-3501/2018/134
Keywords: chronic myeloid leukemia, tyrosine kinase inhibitors, bosutinib, adverse event, real world evidence
Citation: García-Gutiérrez V, Gómez-Casares MT, Xicoy B, Casado-Montero F, Orti G, Giraldo P and Hernández-Boluda JC (2024) Critical review of clinical data and expert-based recommendations for the use of bosutinib in the treatment of chronic myeloid leukemia. Front. Oncol. 14:1405467. doi: 10.3389/fonc.2024.1405467
Received: 22 March 2024; Accepted: 06 August 2024;
Published: 26 August 2024.
Edited by:
Mario Tiribelli, University of Udine, ItalyReviewed by:
Dennis Kim, Princess Margaret Hospital, Hong Kong SAR, ChinaCopyright © 2024 García-Gutiérrez, Gómez-Casares, Xicoy, Casado-Montero, Orti, Giraldo and Hernández-Boluda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Carlos Hernández-Boluda, aGVybmFuZGV6X2pjYUBndmEuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.