 Paula T. Bradley1*
Paula T. Bradley1* Ying Ki Lee2Abigail Albutt3John Hardman4Ian Kellar5Chinasa Odo6Rebecca Randell6
Ying Ki Lee2Abigail Albutt3John Hardman4Ian Kellar5Chinasa Odo6Rebecca Randell6 Nikki Rousseau3Theofano Tikka7Joanne M. Patterson8
Nikki Rousseau3Theofano Tikka7Joanne M. Patterson8 Vinidh Paleri9
Vinidh Paleri9- 1Population Health, Newcastle University, Newcastle upon Tyne, United Kingdom
- 2Department of Otolaryngology, Guy’s and St Thomas’ National Health Service (NHS) Foundation Trust, London, United Kingdom
- 3Faculty of Medicine and Health, University of Leeds, Leeds, United Kingdom
- 4Department of Otolaryngology, Barts Health NHS Trust, London, United Kingdom
- 5Department of Psychology, The University of Sheffield, Sheffield, United Kingdom
- 6Faculty of Health Studies, University of Bradford, Bradford, United Kingdom
- 7Department of Otolaryngology, Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom
- 8School of Allied Health Professions & Nursing, Institute of Population Health / Liverpool Head and Neck Centre, University of Liverpool, Liverpool, United Kingdom
- 9Head and Neck Unit, Royal Marsden NHS Foundation Trust, London, United Kingdom
Introduction: Evolution of a patient-reported symptom-based risk stratification system to redesign the suspected head and neck cancer (HNC) referral pathway (EVEREST-HN) will use a broad and open approach to the nomenclature and symptomatology. It aims to capture and utilise the patient reported symptoms in a modern way to identify patients’ clinical problems more effectively and risk stratify the patient.
Method: The review followed the PRISMA checklist for scoping reviews. A search strategy was carried out using Medline, Embase and Web of Science between January 1st 2012 and October 31st 2023. All titles, abstracts and full paper were screened for eligibility, papers were assessed for inclusion using predetermined criteria. Data was extracted pertaining to the aims, type of study, cancer type, numbers of patients included and symptoms, presenting complaints or signs and symptoms.
Results: There were 9,331 publications identified in the searches, following title screening 350 abstracts were reviewed for inclusion and 120 were considered for eligibility for the review. 48 publications met the eligibility criteria and were included in the final review. Data from almost 11,000 HNC patients was included. Twenty-one of the publications were from the UK, most were retrospective examination of patient records. Data was extracted and charted according to the anatomical area of the head and neck where the symptoms are subjectively and objectively found, and presented according to lay terms for symptoms, clinical terms for symptoms and the language of objective clinical findings.
Discussion: Symptoms of HNC are common presenting complaints, interpreting these along with clinical history, examination and risk factors will inform a clinician’s decision to refer as suspected cancer. UK Head and Neck specialists believe a different way of triaging the referrals is needed to assess the clinical risk of an undiagnosed HNC. EVEREST-HN aims to achieve this using the patient history of their symptoms. This review has highlighted issues in terms of what is considered a symptom, a presenting complaint and a clinical finding or sign.
Introduction
Head and neck cancer (HNC) are a group of cancers affecting the head and neck including the nose, mouth, throat, voice box (larynx), and salivary glands. HNC presents in multiple anatomical sites and tissue types because of this it presents with; physical changes which are noticed by a patient and objectively detectable like an ulcer or a neck lump, symptoms like pain or discomfort which a patient experiences (locally or referred), altered function of the voice, swallowing, or breathing or a combination of physical signs, symptoms and change in function. Some of the symptoms of HNC are very commonly experienced in the general population, like an earache, a sore throat or hoarseness. In health systems where clinical gatekeepers act to determine access to clinical specialist services, decisions about who and how urgently to refer patients relies on the assessment by primary care clinicians (GP, general dental practitioners (GDP) and allied clinical staff with referral privileges). Currently there is no screening test to detect, or risk stratify suspected cases of HNC, instead patients are referred for diagnosis based on presenting signs and symptoms often with no objective clinical findings because sites are out view of examining clinicians (pharynx, larynx) or in areas with which they have little clinical experience (oral cavity). EVEREST-HN (1) aims to develop and assess the success of a system to harness responses from the patient who has been referred as a suspected HNC, to standardised questions to establish the risk of undiagnosed HNC. It is hoped that this will be suitable to help triage referrals so that specialists can better direct the patient to initial investigations, most suitable clinical assessment and determine the urgency of that assessment.
Amongst countries with a gatekeeper to specialist referrals (half of Europe, Australia, New Zealand and Canada) only the UK, Denmark, Sweden, Norway, Spain, New Zealand and Australia have guidelines for organ specific suspected cancer referrals (2, 3) including suspected HNC (4). One Danish centre (Odense) reports a conversion rate from referral to cancer diagnosis as 29.2% (1 July 2012 to 1st September 2015) (5). In the UK referral to cancer diagnosis conversion rates for head and neck cancer, reported by multiple audits of specialist centres, commonly fall below 10% (6). The suspected cancer referral to diagnosis conversion rates for head and neck cancers in the UK is one of the lowest amongst the country’s organ specific suspected cancer referral pathways despite the changes to the clinical referral criteria since 2000 (7). The most recent version of the English suspected HNC referral guidelines, determined by the National Institute of Clinical Excellence (NICE NG12) (now nearly a decade old), has been implemented in some but not all the cancer alliances in England.
In the UK the where referrals for suspected cancer come from primary care, the changing nature of the workforce, issues with patient access to dentistry and the cancer agenda set by the NHS are all drivers to the increase in suspected HNC referral volumes, which now stands at just over 200,000 referrals per annum (8). Problems peculiar to the NHS derive from government determined clinical targets and a commitment to prioritise early cancer detection (because of comparatively poor outcomes when compared to those of similarly socioeconomic status countries). In the UK this means suspected cancer referrals come without financial tariff for primary care (unlike referrals for specialist opinion about clinical issues not associated with a cancer suspicion), but targets and fines are imposed on secondary care if they miss time to diagnosis targets. This places a huge burden when it comes to delivery of outpatient services and diagnostic imaging on specialist services.
Referrals to suspected HNC services depends on a primary care clinician’s interpretation of the patient history, along with risk factors and clinical assessment. The difficulty for primary care in recognising HNC exist in large part because they will see a case of HNC so rarely, HNC originates from multiple tissue types across neighbouring anatomical sites which are often outside the examination field without specialist equipment and cancers can cause overlapping symptoms. The interpretation and misinterpretation of, particularly, the symptoms and physical signs of HNC have been a source of frustration for Ear Nose and Throat (ENT) and maxillofacial surgeons (OMFS) alike (9). The comparative ease with which the Two week wait (TWW) and Urgent Suspicion of Cancer (USOC) pathway (in Scotland) can be accessed in primary care for referrals and the emphasis on early cancer recognition and detection issued from the NHS, government and charitable bodies has decidedly changed the referral practices and subsequently resources required to meet the volume of patient referrals.
A recent publication of the analysis of UK General Practice (GP) Cancer Diagnosis Audit in 2018, exploring the signature symptoms of incident cancers, found the signature symptoms for HNC were neck lump, ulceration and, hoarseness (10). The audit was retrospective, making it subject to recall bias, and those submitting data had access to the full medical records; hence there is potential for diagnostic findings to be declared as the first symptom prompting suspicion of cancer and possibly not reflective of the true clinical course from first presentation in primary care to diagnosis in secondary care.
Much retrospective work has been conducted since the introduction of the suspected cancer pathway by UK head and neck specialists (6). Published audits examine compliance with referral guidelines and consider ways which might reduce the volume of referrals whilst maintaining the yield of cancer from the referrals. The most notable contribution to this debate is the HaNC-RC (head and neck cancer – risk calculator) which was proposed initially as a tool to be used in primary care to help determine the route of referral for patients with symptoms considered suspicious for HNC (11–13).
Covid-19 and its consequences on healthcare delivery offered an opportunity for ENT surgeons to use HaNC-RC tool to triage the suspected HNC referrals (14). This ENT UK endorsed project demonstrated that secondary care could successfully triage over the telephone using the risk calculator as part of a consultation. Those specialists involved found this an effective way to determine the risk of an undiagnosed HNC, reduce patient anxiety and arrange appropriate investigations ahead of a time appropriate face to face assessment (15). As services opened up as lockdown restrictions relaxed telephone triage was gradually phased out and so a new solution to a long term problem was sought.
EVEREST-HN takes a multidisciplinary approach and includes public and patient involvement (from inception to completion) and will use a broad and open approach to the nomenclature and symptomatology aiming to capture and utilise the patient’s responses to questions posed in appropriate language. The aim is to identify patients’ clinical problems more effectively and risk stratify, rather than by way of a simple box tick on a referral form. The hope is that it will necessitate a move away from an automatic one size fits all specialist out-patient appointment within two weeks.
Aims of scoping review
The aim of the scoping review was to produce a comprehensive collection of the terminology related to the symptoms associated with head and neck patient presentation to help inform the development of the EVEREST-HN patient facing platform.
This scoping review will explore the literature to 1) identify the symptoms associated with the presentation of HNC, 2) provide a collection of terms and identify the source of this language to describe the patient experience of symptoms which could be caused by an undiagnosed HNC.
Scoping reviews allow an exploration of the available literature in a complex area which has perhaps not been comprehensively reviewed, they enable mapping of the main sources and available evidence about a topic (16).
The review is not concerned with risk factors of HNC nor does it not aim to assess sensitivity of the symptoms as this was done in the development of the HaNC-RC and its use during Covid-19, which has informed the development of the EVEREST-HN project and is already in the public domain.
Method
The review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension for Scoping Reviews (PRISMA-ScR) (17). A protocol was developed by PB with agreement from VP and JP. The anticipated heterogenous nature of the data (a large proportion of the literature was not research but reports of audit and reports of retrospective patient note review) meant that there was no intention to critically appraise the publications.
The lead researcher (PB) and an Information Specialist developed a search strategy for electronic databases using MeSH terms (see Appendix for search strategies). An electronic search for relevant published material was done using Medline, Embase and Web of Science between January 1st 2012 and October 31st 2023. The only limits on the searches were that they were dated after 1st January 2012 (pilot searches over a decade found more results than could be managed in the available time and resources). Publications included those which were considered quantitative, qualitative, or mixed methods, as not all publications could be regarded as empirical studies, it was decided that audits, surveys, and descriptive cohort publications could be included as this was a scoping not a systematic review or meta-analysis. Reviews, commentaries, conference abstracts and editorials were excluded but foreign language papers were not excluded from the searches.
Search results were saved into an Excel® (Microsoft® 365) spreadsheet and references downloaded to EndNote ™ citation manager (Clarivate) and duplicates were removed.
All titles identified in the electronic database searches were screened by PB with 10% of the titles checked by YL, PB reviewed all selected abstracts with a 10% check by YL again. Any decisions about inclusion which were not in agreement were discussed and reviewed. The full papers were obtained for all abstracts considered eligible and both PB and YL reviewed all full papers for inclusion using the predetermined criteria, any disagreements at any point in the process were discussed between PB and YL until agreement was reached.
Papers were included which had information about a cohort or case series of HNC patients with terms/vocabulary/language pertaining to their symptoms, signs, or presenting complaints, no limits were applied in terms of type of health care system (public, private or gatekeeper system with specific referral criteria), following full paper selection, PB extracted data using criteria agreed by PB and YL.
Data was extracted from the articles about the aims, type of study, cancer type, numbers of patients included along with patients’ symptoms and presenting complaints or signs and symptoms pertinent to referral criteria, YL checked the data extraction table completed by PB against the full papers and any additions or corrections were agreed between PB and YL.
Once the data was extracted and charted, the main author summarised the results in a narrative synthesis and categorised the symptoms, signs, lay and medicalised language of the presenting symptoms, complaints, and signs of HNC in a table according to anatomical functional sites.
Results
The searches yielded a total of 9,810 publications. When duplicates were removed, there were 9,331 titles to screen. Following title screening there were 350 abstracts to review for inclusion in the scoping review (Figure 1).
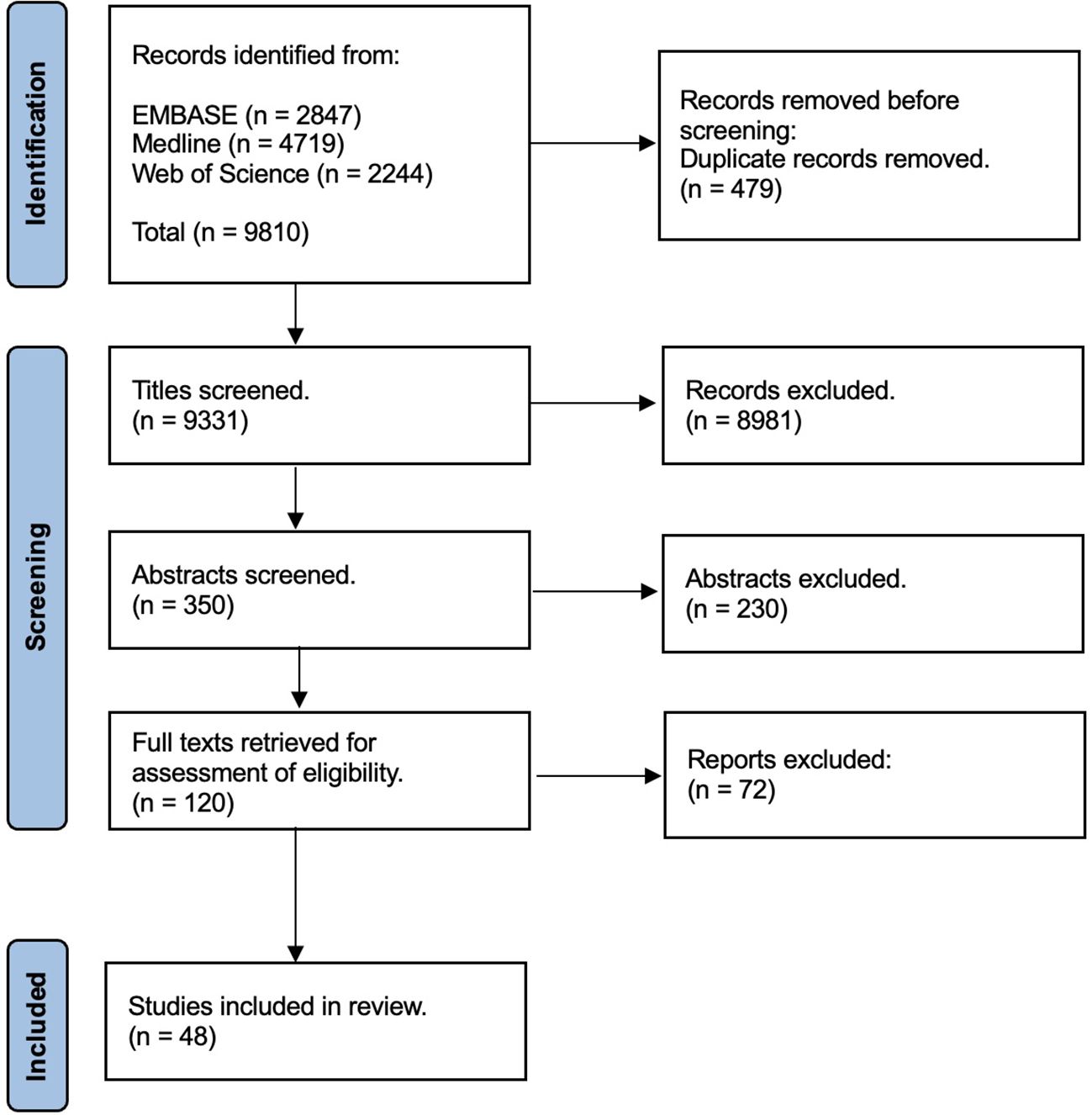
Figure 1 PRISMA flow diagram.
Following abstract screening there were 120 full papers considered for eligibility for the review. Forty-eight publications were considered to meet the eligibility criteria and therefore included in the final review.
Summarising the results
Forty-eight publications were selected to inform the review (5, 11–13, 18–61) which included data from nearly 11,000 patients with a diagnosis of cancer (number of HNC cases included in the reviewed publications = 10,808) (Table 1).

Table 1 Summary of included publications.
Most of the publications present European data (5, 11–13, 19, 22–28, 35, 42, 43, 45–48, 50–52, 55–58, 61) of which the majority were from the UK (11–13, 19, 22–24, 26–28, 43, 45–47, 49–51, 55, 56, 58, 61). Eight of the selected papers were from lower or middle income countries (18, 20, 21, 30, 31, 33, 34, 36), seven from the USA (32, 37–39, 41, 54, 60), three from Canada (40, 44, 53) and one from Australia (59).
The majority of the papers selected were retrospective studies using data from patient records. These explored characteristics of a cohort or case series of patients with a particular HNC (for example nasopharyngeal carcinoma (54, 60), HPV positive oropharyngeal carcinoma) or a group of cancers arising in the head and neck [for example a cohort including oral, oropharynx, larynx and hypopharyngeal (27)] (11–13, 18, 21–26, 32–35, 37, 38, 41–43, 46, 48, 50, 52, 54, 56–58, 60, 61).
Seventeen papers (5, 11–13, 24, 26, 28, 43–45, 49–52, 55, 58, 61) included retrospective analysis of patients referred on a suspected HNC referral pathway; most of these were from the UK (England TWW (11, 24, 43, 49, 50, 55, 58, 61) or Scotland USOC route (12, 13, 26, 28, 45, 51). Three were from outside the UK (4, 44, 52). These papers included analysis of the signs, symptoms, and risk factors more common amongst the patients who were diagnosed with HNC.
Of the retrospective cohort series reports most were from the UK. Five studies used data to statistically model the presenting signs and symptoms with which patients are referred to specialist care for suspected cancer, and defined the symptoms associated with a diagnostic outcome of a HNC (11–13, 43, 49, 56). These papers aimed for a clinically applicable risk stratification system which might be used to make decisions on urgency of referrals or to triage referrals. There was only one prospective study from Denmark (5), arising from the HNC fast track referral programme in Odense.
There were six qualitative studies (20, 30, 31, 44, 53, 59), all of which were from outside the UK. These explored the patient and health system factors related to the delays in presentation and diagnosis associated with HNCs (20, 30, 31, 44, 59). One explored patient symptom appraisal (53) and its role in timing of presentation to health care services.
Four selected articles presented the results of patient questionnaires, three explored factors determining delay in presentation and diagnosis (29, 36, 45), and one was concerned with patient expectations of a suspected cancer referral and appointment (51).
Three papers used a non-traditional mixed method approach (19, 40, 47), two using retrospective notes examination with patient questionnaires (19, 40) [one from the UK (19)] and a third included data from patient interviews (47) from a UK sarcoma cohort which included 9 patients diagnosed with a head and neck sarcoma. All aimed to explore the reasons behind delay in diagnosis and presentation.
Some papers referred specifically to a type of HNC, often rare like sino-nasal (46, 48) and nasopharyngeal carcinoma (18, 21, 30, 33, 60); a number of studies concentrated on HPV positive and negative oropharyngeal cancer (22, 25, 32, 39, 41, 54) and oral cancers (20, 29, 36), with one including both (35). Studies on multiple HNC subtypes based on suspected cancer referrals often had a small minority with diagnosed cancer (5, 11–13, 24, 26, 28, 43–45, 50–52, 55, 58, 61). Three studies were based on laryngeal cancers (37, 38, 56), two of which were rare types of laryngeal cancers [non-epithelial (37) and salivary gland cancers of the larynx (38)]. The selected data included papers on some cancers which are not regarded as HNCs in the traditional sense but which frequently present with important symptoms related to the function and anatomy of the head and neck e.g. lymphoma (34, 42, 57) and sarcoma (47). These patients are likely to present/be referred to ENT for clinical assessment in the first instance.
The aims of the studies can be categorised into the following: explorations for the reasons for delay in diagnosis or presentation (19, 20, 22, 23, 29–32, 36, 39, 40, 44, 45, 47, 59, 60), the relationship between presenting symptoms and outcomes (18, 21, 25–28, 37, 38, 42, 46, 48, 49, 51–54, 56, 57), the predictive factors (including symptoms and risk factors) for an eventual diagnosis of a HNC (33–35, 41), development of statistical models to assist referrals for suspected cancer (11–13, 43). A small number of the published papers present an assessment of the fast track referral systems for suspected cancer (5, 24, 50, 55, 58, 61) (only one from outside the UK (5)).
When it comes to the symptoms of HNC in these papers, it is important to consider the perspective and the language. There are five papers where the data is based on primary care coding or referral category (5, 22, 52, 56, 58); in others, the presenting symptoms and referral criteria from primary care have been used to explore the strength of the relationship between various signs and symptoms and a cancer outcome.
When the selected studies discussed symptoms, these tended to be in terms of medical language (5, 11–13, 18, 21–24, 28, 29, 32–35, 38–40, 42–44, 48, 53, 54, 56, 58, 61) with some including clinical signs or findings and other using diagnostic terminology but referring to it in the same category as a symptom (25–27, 36, 37, 41, 45, 46, 49, 50, 52, 55, 57, 60).
The patient perspective and language is presented in just seven papers (20, 30, 31, 47, 51, 53, 59). Five papers focus on the language used by patients to describe their head and neck symptoms (20, 30, 31, 47, 59). One paper used medical terminology to discuss patient level of concern (51) the other grouped patient symptoms into medicalised groups (for example voice/speech problem and pain or bleeding (53).
In those papers which present a retrospective assessment of the clinical notes the authors fail to clarify whether data included objective examination findings noted by the specialist and diagnoses which a primary care clinician had not made or included as part of their referral (globus as opposed to dysphagia and the physical presence or absence of a neck lump for example) (11–13, 24).
Because most the publications included in this scoping review were internal departmental retrospective case note reviews there is no external funding reported. Where there is funding declared it is all from academic non-commercial research grants (20, 29–31, 53, 56).
The symptoms of head and neck cancer
The extracted data related to signs, symptoms and referral criteria were categorised in terms of the type of language: patient or lay terms for symptoms, clinical terms for symptoms and the language of clinical examination findings, signs, and diagnostic terms. The results are displayed in Table 2 and are divided into the anatomical areas of the head and neck which the symptoms affect along with some of the systemic symptoms associated with cancers in general derived from the literature. Table 2 includes columns which contains the site to which symptoms are related the physical signs which patients may complain of and the medical language of both signs and symptoms.
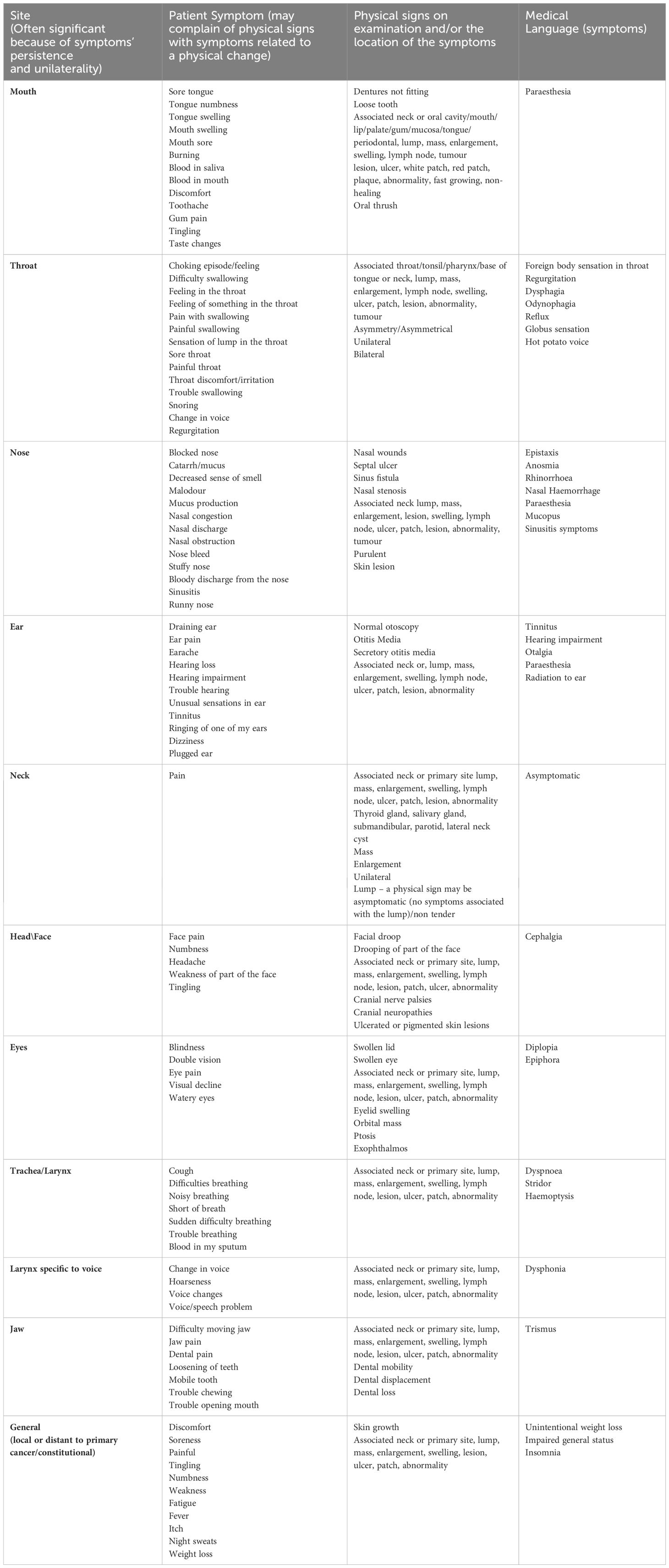
Table 2 Summary of symptoms, presenting complaints, clinical findings and medical language of head and neck cancer.
In the literature, signs are sometimes conflated with symptoms such as a mouth ulcer or a neck lump, these are objective clinical findings. A patient may notice an asymptomatic neck or salivary gland lump and this might be the reason they present to primary care or a specialist (where there is no gatekeeper system), however, the assumption is that if a patient is referred from primary care there is, on clinical examination, a palpable neck or salivary gland lump. The term symptom is sometimes used in the reviewed literature when the language refers to a clinically determined diagnosis such as globus pharyngeus.
Despite some of the symptoms being rarely associated with an eventual diagnosis of cancer (fewer than those with a benign cause), some patients will experience and describe these symptoms in the journey to their cancer diagnosis and so these are included in Table 2.
Discussion
This scoping review aimed to produce a comprehensive collection of terminology in the literature related to the symptoms associated with HNC patient presentations. Forty-eight publications were identified, and the data extracted has been presented, organised according to anatomical and functional sites of the head and neck, in terms of patient and clinical language of the symptoms and those which are considered a presenting complaint which is subject to an objective clinical examination. This summary will be used and expanded upon in the EVEREST-HN project with the aim of harnessing the patient narrative in estimating risk of undiagnosed HNC.
The language pertaining to the symptoms of HNC is important because successful diagnosis depends on effective communication regarding signs and symptoms between patients and clinicians and between different health care professionals: unfortunately, what a term like odynophagia means to a specialist is different to that which a GP might understand (62). It is also true that how a patient communicates symptoms can be re/mis-interpreted by a GP leading to over or under emphasising the clinical significance (63). UK ENT surgeons complain that some primary care clinicians misinterpret a neck lump as a lump in the throat when a patient has no palpable neck lump (64). An ulcer is a physical sign found on examination and can be associated with symptoms like bleeding or pain but findings in the mouth might be interpreted differently by a GDP compared to a GP or a nurse practitioner with no dental experience. Fear of missing a cancer may drive referrals along with lack of relevant clinical experience, pressures related to capacity to book follow up appointments, continuity of care and difficulty accessing alternatives to the urgent cancer pathway (such as dental care and routine hospital appointments).
There are important issues drawn out of this literature review in terms of what is considered a sign and what is a symptom. When patients present to primary care they do not say “I have been experiencing hoarseness, haemoptysis, dyspnoea, odynophagia, unilateral sore throat with ipsilateral otalgia, with normal otoscopy and level IV cervical lymphadenopathy”; instead, they might say “my throat has been sore for weeks and my ear hurts on the same side, I can’t swallow my food properly so am having soups, my voice is croaky and my breathing is noisy”. They might say “there’s a painful white patch on the roof of my mouth which has been bleeding” as opposed to “leukoplakia of the hard palate” and a primary care clinician may not have the confidence to describe it as such either.
In the UK, odynophagia, dysphagia, and hoarseness are the commonest “symptoms” for which patients are referred to ENT from GPs and yet very few of these patients will be diagnosed with a cancer (conversion from referral to cancer diagnosis of less than 3% (7). The fact that GPs are referring patients with these symptoms because they suspect a HNC implies that they do not have the confidence to clinically reassure themselves or patients that an underlying cancer does not exist. For some GPs, excluding a cancer may necessitate a referral much to the chagrin of head and neck surgeons (both ENT and OMFS) many of the swallowing issues (referred as dysphagia and odynophagia) are given a benign diagnosis of globus pharyngeus it is also notable that these symptoms no longer appear on the NICE referral criteria for suspected HNC (are part of upper gastrointestinal pathway) yet some English Cancer Alliances have retained these symptoms on their local referral proformas. A recent review of the diagnosis and investigation of globus by the joint European and American Society of Neurogastroenterology and Motility describe it as a “clinical challenge” diagnosed “when the clinical history is supportive and after alternate medical conditions have been excluded using prudent and specific investigation” (65) such expertise and appropriate investigations are not routinely accessible, without significant delay, to primary care in the UK.
Triage of suspicious oral lesions seen by primary care (GPs), for which NICE recommend a general dental opinion (increasingly difficult to access in the NHS) prior to a TWW referral from GPs, might be facilitated using teledentistry alongside clinical history and physical examination performed in the community by both GPs and GDPs (66). Teledentistry could improve communication between primary care and secondary care and provide a timely expert opinion about the route of referral and or appropriate management in the community, this is particularly pertinent given the current crisis in dental care provision in the UK (8). It could certainly be an adjunct to the patient reported symptom questions proposed by the EVEREST-HN programme for lesions visible in the mouth and oropharynx.
The HaNC-RC work and retrospective studies into HNC patients highlights that there are combinations of risk factors, symptoms and signs which make a cancer more likely to be causing symptoms. The sources exploring the links between signs and symptoms and an outcome of a diagnosis of HNC are mostly from secondary care and predominantly from UK sources (two authors dominate these sources Tikka and Douglas). It appears an almost uniquely UK preoccupation with the sensitivity of the referrals and compliance with the clinical criteria pertaining to these referrals. The reasons for this are justified by the poor yield of cancer from this referral route (7) and demands on secondary care services to meet the NHS Faster Diagnosis Framework Pathway Standard (67). Publications from other countries are more concerned with reasons for late presentation, delayed diagnosis, and patient symptom appraisal. When it comes to HNC, the suspected cancer referral routes in both England and Scotland are a source of frustration to secondary care as its existence does not appear to be affecting the yield or the treatment outcomes of HNCs.
Remote triage using HaNC-RC was not a perfect tool even in the hands of senior specialists (68) and when used by GPs increased rather than decreased the volumes referred (69). EVEREST-HN aims to further explore these relationships and potentially integrate digital images and voice recordings to develop a system which stratifies patients in a way that benefits the NHS, the patients and cancer outcomes better than the current system.
Limitations
Because of resources and time constraints it was not possible to complete grey searches or to gather international clinical guidelines and HNC referral criteria. Other sources such as patient facing cancer websites and patient forums would be another source of valuable data in terms of the lay perspective and language around the symptoms of HNC.
This review has not subdivided the nomenclature of the symptoms and signs of HNC into head and neck site specific areas but rather into function and anatomical areas. There is undoubtedly cross over between symptoms which occur in several subsites where cancers of the head and neck originate which will sometimes depend on the stage of the cancer at which the patient presents because it may invade local tissues affecting function, EVEREST-HN aspires to expose some of these relationships with the aim to utilise this information for future triaging of referrals.
The review includes symptoms of rare HNCs and the more common ones including oral, oropharyngeal, and laryngeal cancers. EVEREST-HN will gather data on the rare and the common symptoms and identify ways in which these can be stratified into high and low risk using the patient reported symptoms so that the vast majority can be investigated or assessed quickly by the most appropriate clinician. EVEREST-HN will capture data to use in the future to target questions about symptoms, signs, and risk factors to triage more effectively those most likely to have cancer to appropriate services with the aim to improve the patient journey (for the vast majority without a cancer and those with an underlying cancer) and best optimise the finite NHS resources.
Conclusions
Symptoms of HNC are common presenting complaints in primary care, interpreting these along with clinical history, examination and risk factors will inform a clinician’s decision to refer as suspected cancer. The TWW suspected cancer referral criteria have evolved over the years as specialists consider a different way of triaging the volume of referrals that is needed to assess the clinical risk of an undiagnosed HNC over and above the referral based on primary care assessment. EVEREST-HN aims to achieve this using the patient history of their symptoms. This review has highlighted issues in terms of what is considered a symptom, a presenting complaint and a clinical finding or sign. Difficulties remain in terms of interpretation, of the language of signs and symptoms and the physical findings, by both patients as well as generalists. The way patients report their own symptoms will be crucial along in combination with other modalities like digital photography, voice recordings and the potential of artificial intelligence, to develop a more a more sensitive triage system.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
PB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. YL: Data curation, Writing – review & editing. AA: Writing – review & editing. JH: Writing – review & editing. IK: Writing – review & editing. CO: Writing – review & editing. RR: Writing – review & editing. NR: Writing – review & editing. TT: Writing – review & editing. JP: Writing – review & editing. VP: Writing – review & editing
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. National Institute for Health and Care Research Programme Grant for Applied Research NIHR 202862.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. RMH. EVEREST-HN - Evolution of a patient-reported symptom-based risk stratification system to redesign the suspected head and neck cancer referral pathway (2022). Available at: https://www.royalmarsden.nhs.uk/everest-hn.
2. Koo MM, Unger-Saldaña K, Mwaka AD, Corbex M, Ginsburg O, Walter FM, et al. Conceptual framework to guide early diagnosis programs for symptomatic cancer as part of global cancer control. JCO Glob Oncol. (2021) 7:35–45. doi: 10.1200/GO.20.00310
3. Grønnemose RB, Hansen PS, Worsøe Laursen S, Gerke O, Kjellberg J, Lykkegaard J, et al. Risk of cancer and serious disease in Danish patients with urgent referral for serious non-specific symptoms and signs of cancer in Funen 2014–2021. Br J Cancer. (2024) 130(8):1304–15. doi: 10.1038/s41416-024-02620-y
4. Tikka T. Development and validation of a head and neck cancer risk calculator. Available at: https://stax.strath.ac.uk/concern/theses/g445cd76k?locale=en.
5. Roennegaard AB, Rosenberg T, Bjorndal K, Sorensen JA, Johansen J, Godballe C. The Danish Head and Neck Cancer fast-track program: a tertiary cancer centre experience. Eur J Cancer. (2018) 90:133–9. doi: 10.1016/j.ejca.2017.10.038
6. Langton S, Siau D, Bankhead C. Two-week rule in head and neck cancer 2000–14: a systematic review. Br J Oral Maxillofac Surg. (2016) 54:120–31. doi: 10.1016/j.bjoms.2015.09.041
7. Smith L, Sansom N, Hemphill S, Bradley SH, Shinkins B, Wheatstone P, et al. Trends and variation in urgent referrals for suspected cancer 2009/2010–2019/2020. Br J Gen Pract. (2022) 72:34–7. doi: 10.3399/bjgp22x718217
8. Watt RG, Heilmann A, Conway DI. Oral cancers are rising in the UK. Bmj. (2023) 383:2907. doi: 10.1136/bmj.p2907
9. Rovira A, Russell B, Trivedi P, Ojo O, Oakley R, Byrne E, et al. The impact of 2 weeks wait referral on survival of head and neck cancer patients. Eur Arch Otorhinolaryngol. (2023) 280:5557–64. doi: 10.1007/s00405-023-08152-0
10. Zakkak N, Barclay ME, Swann R, McPhail S, Rubin G, Abel GA, et al. The presenting symptom signatures of incident cancer: evidence from the English 2018 National Cancer Diagnosis Audit. Br J Cancer. (2023) 130(2):297–307. doi: 10.1038/s41416-023-02507-4
11. Tikka T, Pracy P, Paleri V. Refining the head and neck cancer referral guidelines: A two-centre analysis of 4715 referrals. Clin Otolaryngology. (2016) 41:66–75. doi: 10.1111/coa.12597
12. Tikka T, Paleri V, MacKenzie K. External validation of a cancer risk prediction model for suspected head and neck cancer referrals. Clin Otolaryngol. (2018) 43:714–7. doi: 10.1111/coa.13019
13. Tikka T, Kavanagh K, Lowit A, Pan JF, Burns H, Nixon IJ, et al. Head and neck cancer risk calculator (HaNC-RC)-V.2. Adjustments and addition of symptoms and social history factors. Clin Otolaryngol. (2020) 45:380–8. doi: 10.1111/coa.13511
14. Paleri V, Hardman J, Tikka T, Bradley P, Pracy P, Kerawala C. Rapid implementation of an evidence-based remote triaging system for assessment of suspected referrals and patients with head and neck cancer on follow-up after treatment during the COVID-19 pandemic: Model for international collaboration. Head Neck. (2020) 42:1674–80. doi: 10.1002/hed.26219
15. Hardman JC, Tikka T, Paleri V, Ent Uk B. Integrate. Remote triage incorporating symptom-based risk stratification for suspected head and neck cancer referrals: A prospective population-based study. Cancer. (2021) 127:4177–89. doi: 10.1002/cncr.33800
16. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodology. (2005) 8:19–32. doi: 10.1080/1364557032000119616
17. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-scR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
18. Adham M, Kurniawan AN, Muhtadi AI, Roezin A, Hermani B, Gondhowiardjo S, et al. Nasopharyngeal carcinoma in Indonesia: epidemiology, incidence, signs, and symptoms at presentation. Chin J Cancer. (2012) 31:185–96. doi: 10.5732/cjc.011.10328
19. Allgar VL, Oliver SE, Chen H, Oviasu O, Johnson MJ, Macleod U. Time intervals from first symptom to diagnosis for head and neck cancers: An analysis of linked patient reports and medical records from the UK. Cancer Epidemiol. (2019) 59:37–45. doi: 10.1016/j.canep.2019.01.008
20. Azhar N, Doss JG. Health-seeking behaviour and delayed presentation of oral cancer patients in a developing country: A qualitative study based on the self-regulatory model. Asian Pacific J Cancer Prevention: Apjcp. (2018) 19:2935–41. doi: 10.22034/apjcp.2018.19.10.2935
21. Aziz A, Ramli RR, Mohamad I, Bhavaraju VMK. Young nasopharyngeal carcinoma: a review of an 8-year experience in the East Coast Malaysia Hospital. Egyptian J Otolaryngology. (2017) 33:490–4. doi: 10.4103/1012-5574.206021
22. Bannister M, Ah-See KW. Is oropharyngeal cancer being misdiagnosed as acute tonsillitis? Br J Gen Pract. (2014) 64:e742–4. doi: 10.3399/bjgp14X682537
23. Bannister M, Vallamkondu V, Ah-See KW. Emergency presentations of head and neck cancer: A modern perspective. J Laryngology Otology. (2016) 130:571–4. doi: 10.1017/S0022215116001043
24. Bhamra N, Gorman B, Arnold W, Rajah A, Jolly K, Nieto H, et al. The impact of coronavirus disease 2019 on suspected head and neck cancer two-week-wait referrals. J Laryngology Otology. (2022) 136:248–51. doi: 10.1017/S0022215121001717
25. Carpen T, Sjoblom A, Lundberg M, Haglund C, Markkola A, Syrjanen S, et al. Presenting symptoms and clinical findings in HPV-positive and HPV-negative oropharyngeal cancer patients. Acta Oto-Laryngologica. (2018) 138:513–8. doi: 10.1080/00016489.2017.1405279
26. Douglas CM, Carswell V, Montgomery J. Outcomes of urgent suspicion of head and neck cancer referrals in Glasgow. Ann R Coll Surgeons Engl. (2019) 101:103–6. doi: 10.1308/rcsann.2018.0168
27. Douglas CM, Ingarfield K, McMahon AD, Savage SA, Conway DI, MacKenzie K. Presenting symptoms and long-term survival in head and neck cancer. J Laryngology Otology. (2018) 132:1. doi: 10.1111/coa.13053
28. Douglas CM, Middleton C, Sim P, Wight M, Young D, MacKenzie K, et al. Patterns of urgent hoarseness referrals to ENT-When should we be suspicious of cancer? Clin Otolaryngology. (2021) 46:562–9. doi: 10.1111/coa.13712
29. Esmaelbeigi F, Hadji M, Harirchi I, Omranipour R, vand Rajabpour M, Zendehdel K. Factors affecting professional delay in diagnosis and treatment of oral cancer in Iran. Arch Iranian Med. (2014) 17:253–7.
30. Fles R, Bos A, Rachmawati D, Waliyanti E, Tan IB, Haryana SM, et al. The role of Indonesian patients' health behaviors in delaying the diagnosis of nasopharyngeal carcinoma. BMC Public Health. (2017) 17:510. doi: 10.1186/s12889-017-4429-y
31. Ganesan S, Sivagnanganesan S, Thulasingam M, Karunanithi G, Ravichandran S, Saxena S, et al. Diagnostic delay for head and neck cancer in South India: A Mixed-methods Study. Asian Pacific J Cancer Prevention: Apjcp. (2020) 21:1673–8. doi: 10.31557/apjcp.2020.21.6.1673
32. Gilde J, Song B, Masroor F, Darbinian JA, Ritterman Weintraub ML, Salazar J, et al. The diagnostic pathway of oropharyngeal squamous cell carcinoma in a large U.S. healthcare system. Laryngoscope. (2018) 128:1867–73. doi: 10.1002/lary.27038
33. Hasnaoui M, Lahmar R, Ben Mabrouk A, Masmoudi M, Mighri K, Driss N. Predictive epidemiological and clinical factors of nasopharyngeal carcinoma diagnosis: Adult versus pediatric population. Int J Pediatr Otorhinolaryngology. (2020) 137:110203. doi: 10.1016/j.ijporl.2020.110203
34. Hu ZZ, Wang Y. The factors associated with the early diagnosis of nasal NK/T-cell lymphoma with prominent ocular symptoms and general nasal NKTL. Am J Otolaryngol. (2019) 40:353–7. doi: 10.1016/j.amjoto.2019.01.012
35. Jehannin-Ligier K, Dejardin O, Lapotre-Ledoux B, Bara S, Coureau G, Grosclaude P, et al. Oral cancer characteristics in France: Descriptive epidemiology for early detection. J Stomatology Oral Maxillofac Surg. (2017) 118:84–9. doi: 10.1016/j.jormas.2017.02.003
36. Joshi P, Nair S, Chaturvedi P, Nair D, Agarwal JP, D'Cruz AK. Delay in seeking specialized care for oral cancers: experience from a tertiary cancer center. Indian J Cancer. (2016) 51:95–7. doi: 10.4103/0019-509x.137934
37. Karatayli-Ozgursoy S, Bishop JA, Hillel AT, Akst LM, Best SR. Non-epithelial tumors of the larynx: a single institution review. Am J Otolaryngology. (2016) 37:279–85. doi: 10.1016/j.amjoto.2016.01.005
38. Karatayli-Ozgursoy S, Bishop JA, Hillel AT, Akst LM, Best SR. Malignant salivary gland tumours of the larynx: a single institution review. Acta Otorhinolaryngologica Italica. (2016) 36:289–94. doi: 10.14639/0392-100X-807
39. Karp EE, Yin LX, Moore EJ, Elias AJ, O'Byrne TJ, Glasgow AE, et al. Barriers to obtaining a timely diagnosis in human papillomavirus-associated oropharynx cancer. Otolaryngol - Head Neck Surg. (2021) 165:300–8. doi: 10.1177/0194599820982662
40. Kassirian S, Dzioba A, Hamel S, Patel K, Sahovaler A, Palma DA, et al. Delay in diagnosis of patients with head-and-neck cancer in Canada: impact of patient and provider delay. Curr Oncol. (2020) 27:e467–e77. doi: 10.3747/co.27.6547
41. Khalid MB, Ting P, Pai A, Russo JL, Bakst R, Chai RL, et al. Initial presentation of human papillomavirus-related head and neck cancer: A retrospective review. Laryngoscope. (2019) 129:877–82. doi: 10.1002/lary.27296
42. Kiessling SY, Soyka MB, Huber GF, Holzmann D, Laske RD. Delayed diagnosis of sinonasal lymphoma due to bilateral manifestation. Eur Arch Oto-Rhino-Laryngology. (2017) 274:823–7. doi: 10.1007/s00405-016-4275-z
43. Lau K, Wilkinson J, Moorthy R. A web-based prediction score for head and neck cancer referrals. Clin Otolaryngology. (2018) 43:1043–9. doi: 10.1111/coa.13098
44. Lee JJ, Dhepnorrarat C, Nyhof-Young J, Witterick I. Investigating patient and physician delays in the diagnosis of head and neck cancers: a Canadian perspective. J Cancer Education. (2016) 31:8–14. doi: 10.1007/s13187-014-0777-9
45. Lim AE, Douglas CM, Montgomery J. An open structure questionnaire on reasons for delay in presentation: a study of patients attending clinic with red flag symptoms of head and neck cancer. Eur Arch Oto-Rhino-Laryngology. (2020) 277:1801–6. doi: 10.1007/s00405-020-05897-w
46. Mahalingappa YB, Khalil HS. Sinonasal Malignancy: presentation and outcomes. J Laryngology Otology. (2014) 128:654–7. doi: 10.1017/s0022215114001066
47. Martin S, Clark SE, Gerrand C, Gilchrist K, Lawal M, Maio L, et al. Patients' Experiences of a sarcoma diagnosis: A process mapping exercise of diagnostic pathways. Cancers. (2023) 15. doi: 10.3390/cancers15153946
48. Martinez-Rodriguez N, Dorado CB, Brinkmann JCB, Ares MM, Alonso JS, Martinez-Gonzalez JM. Dental considerations in diagnosis of maxillary sinus carcinoma A patient series of 24 cases. J Am Dental Assoc. (2018) 149:976–82. doi: 10.1016/j.adaj.2018.07.016
49. Metcalfe C, Dailey Y, Lowe D, Rogers SN. Introduction of a referral pathway guide for general dental practitioners in Cheshire & Merseyside: the effect on two-week suspected cancer referrals. Br Dental J. (2019) 227:1058–62. doi: 10.1038/s41415-019-1003-2
50. Mettias B, Charlton A, Ashokkumar S. Outcome of two-week head and neck cancer pathway for the otolaryngology department in a tertiary centre. J Laryngology Otology. (2021) 135:869–73. doi: 10.1017/S0022215121002061
51. Montgomery J, Douglas CM, Begbie F, Hitchings A, MacKenzie K. 'Urgent suspicion of cancer' referrals to a head and neck clinic-what do patients expect? J Laryngology Otology. (2019) 133:782–7. doi: 10.1017/S0022215119001543
52. Nieminen M, Aro K, Makitie A, Harlin V, Kainulainen S, Jouhi L, et al. Challenges in diagnosing head and neck cancer in primary health care. Ann Med. (2021) 53:26–33. doi: 10.1080/07853890.2020.1802060
53. Queenan JA, Gottlieb BH, Feldman-Stewart D, Hall SF, Irish J, Groome PA. Symptom appraisal, help seeking, and lay consultancy for symptoms of head and neck cancer. Psycho-Oncology. (2018) 27:286–94. doi: 10.1002/pon.4458
54. Raman A, Sen N, Ritz E, Fidler MJ, Revenaugh P, Stenson K, et al. Heterogeneity in the clinical presentation, diagnosis, and treatment initiation of p16-positive oropharyngeal cancer. Am J Otolaryngol. (2019) 40:626–30. doi: 10.1016/j.amjoto.2019.05.004
55. Rovira A, Brar S, Munroe-Gray T, Ofo E, Rodriguez C, Kim D. Telephone consultation for two-week-wait ENT and head and neck cancer referrals: initial evaluation including patient satisfaction. J Laryngology Otology. (2022) 136:615–21. doi: 10.1017/S0022215121003157
56. Shephard EA, Parkinson MA, Hamilton WT. Recognising laryngeal cancer in primary care: a large case-control study using electronic records. Br J Gen Pract. (2019) 69:e127–e33. doi: 10.3399/bjgp19X700997
57. Storck K, Brandstetter M, Keller U, Knopf A. Clinical presentation and characteristics of lymphoma in the head and neck region. Head Face Med. (2019) 15. doi: 10.1186/s13005-018-0186-0
58. Talwar C, McClune A, Kelly D, Lowe D, Rogers SN. Two-week rule: suspected head and neck cancer referrals from a general medical practice perspective. Br J Oral Maxillofac Surgery. (2020) 58:981–5. doi: 10.1016/j.bjoms.2020.05.004
59. Venchiarutti RL, Pho L, Clark JR, Palme CE, Young JM. A qualitative exploration of the facilitators and barriers to early diagnosis and treatment of head and neck cancer: Perceptions of patients and carers. Eur J Cancer Care. (2022) 31:e13718. doi: 10.1111/ecc.13718
60. Wang KH, Austin SA, Chen SH, Sonne DC, Gurushanthaiah D. Nasopharyngeal carcinoma diagnostic challenge in a nonendemic setting: our experience with 101 patients. Permanente J. (2017) 21:16–180. doi: 10.7812/tpp/16-180
61. Williams C, Byrne R, Holden D, Sherman I, Srinivasan VR. Two-week referrals for suspected head and neck cancer: two cycles of audit, 10 years apart, in a district general hospital. J Laryngology Otology. (2014) 128:720–4. doi: 10.1017/s0022215114001406
62. Rosendal M, Jarbøl DE, Pedersen AF, Andersen RS. Multiple perspectives on symptom interpretation in primary care research. BMC Family Practice. (2013) 14:167. doi: 10.1186/1471-2296-14-167
63. Hardy V, Usher-Smith J, Archer S, Barnes R, Lancaster J, Johnson M, et al. Agreement between patient's description of abdominal symptoms of possible upper gastrointestinal cancer and general practitioner consultation notes: a qualitative analysis of video-recorded UK primary care consultation data. BMJ Open. (2023) 13:e058766. doi: 10.1136/bmjopen-2021-058766
64. Bradley PT. A Qualitative Exploration of the prospective implementation of a primary care clinical referral decision tool for patients with suspected head and neck cancer. (2022). Available at: https://sure.sunderland.ac.uk/id/eprint/15552/.
65. Zerbib F, Rommel N, Pandolfino J, Gyawali CP. ESNM/ANMS Review. Diagnosis and management of globus sensation: A clinical challenge. Neurogastroenterol Motil. (2020) 32:e13850. doi: 10.1111/nmo.13850
66. Bradley P, Deane J, O’Hara J, Kennedy M, Carrard VC, Cheong SC, et al. Teledentistry may help in detecting oral cancers in current GP and dentist shortages. BMJ. (2024) 384:q512. doi: 10.1136/bmj.q512
67. NHS E. Faster diagnosis framework (2024). Available at: https://www.england.nhs.uk/cancer/faster-diagnosis/#:~:text=The%20Faster%20Diagnostic%20Framework%20aims,community%2C%20primary%20and%20secondary%20care.
68. Lau KL, Wilson M, Oozeer N, Cocks H. Coronavirus disease 2019 pandemic telephone two-week-wait referrals in head and neck cancer - how safe were they? J Laryngol Otol. (2024) 138:321–4. doi: 10.1017/S0022215123001238
69. Li L, Tikka T, Morton C, Chan C, Hayois L, Henderson M, et al. Primary care triaging of head and neck cancer referrals using the head and neck cancer risk calculator version 2: impact on a tertiary head and neck service. J Laryngol Otol. (2023) 137:763–8. doi: 10.1017/S002221512200192X
Appendices
Database searches
EMBASE
1. “head and neck neoplasms”/or “squamous cell carcinoma of head and neck”/or mouth neoplasms/or gingival neoplasms/or lip neoplasms/or palatal neoplasms/or salivary gland neoplasms/or parotid neoplasms/or sublingual gland neoplasms/or submandibular gland neoplasms/or tongue neoplasms/or otorhinolaryngologic neoplasms/or ear neoplasms/or laryngeal neoplasms/or nose neoplasms/or paranasal sinus neoplasms/or pharyngeal neoplasms/or hypopharyngeal neoplasms/or nasopharyngeal neoplasms/or nasopharyngeal carcinoma/or oropharyngeal neoplasms/or tonsillar neoplasms/or thyroid neoplasms/or thyroid cancer, papillary/.
2. “predictive value of tests”/or roc curve/.
3. diagnosis/or clinical decision-making/or delayed diagnosis/or “early detection of cancer”/.
4. “Referral and Consultation”/mt, td [Methods, Trends].
5. clinical audit/or dental audit/or medical audit/or practice guidelines as topic/.
6. Symptom Assessment/sn [Statistics & Numerical Data].
7. 2 or 3 or 4 or 5 or 6.
8. 1 and 7.
9. limit 8 to yr=“2012 -Current”.
MEDLINE
1. (Head and Neck Neoplasms).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
2. Otorhinolaryngologic Neoplasms.mp. or Otorhinolaryngologic Neoplasms/.
3. exp Mouth Neoplasms/di [Diagnosis].
4. Thyroid Neoplasms/or Thyroid Carcinoma, Anaplastic/or Carcinoma/.
5. Pharyngeal Neoplasms.mp. or Pharyngeal Neoplasms/.
6. Laryngeal Neoplasms.mp. or Laryngeal Neoplasms/.
7. Tongue Neoplasms.mp. or Tongue Neoplasms/.
8. Salivary Gland Neoplasms.mp. or Salivary Gland Neoplasms/.
9. Oropharyngeal Neoplasms.mp. or Oropharyngeal Neoplasms/.
10. (Squamous Cell Carcinoma of Head and Neck).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
11. Paranasal Sinus Neoplasms.mp. or Paranasal Sinus Neoplasms/.
12. Maxillary Sinus Neoplasms.mp. or Maxillary Sinus Neoplasms/.
13. Nose Neoplasms.mp. or Nose Neoplasms/.
14. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13.
15. oropharyngeal cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
16. (head and neck cancer).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
17. (head and neck cancer).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
18. mouth cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
19. thyroid cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
20. pharyngeal cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
21. pharynx cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
22. tongue cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
23. salivary gland cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
24. parotid cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
25. submandibular cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
26. (Squamous Cell Carcinoma head and neck).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
27. oropharyngeal cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
28. sinus cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
29. paranasal sinus cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
30. maxillary sinus cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
31. nose cancer.mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
32. 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31.
33. 14 or 32.
34. (Signs and Symptoms).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
35. Predictive Value of Tests.mp. or “Predictive Value of Tests”/.
36. Diagnosis/or Diagnosis.mp.
37. Early Diagnosis.mp. or Early Diagnosis/.
38. Physical Examination.mp. or Physical Examination/.
39. Diagnosis, Oral.mp. or Diagnosis, Oral/.
40. (Referral and Consultation).mp. [mp=title, book title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms].
41. 34 or 35 or 36 or 37 or 38 or 39 or 40.
42. 33 and 41.
43. Quality Improvement/or Medical Audit/or Clinical Audit Clinical Audit Clinical Audit.mp.
44. guideline.mp. or Guideline/.
45. 43 or 44.
46. 42 and 45.
47. Logistic Models.mp. or Logistic Models/.
48. 33 and 47.
49. 46 or 48.
Web of Science
1. TS=(prediction) 1,545,739.
2. TS=(signs symptoms) 94,033.
3. TS=(early diganosis) 2.
4. #1 OR #2 OR #3 1,638,130.
5. head and neck cancer (Topic) 79,998.
6. #4 AND #5 1,922.
Keywords: head and neck cancer, symptom assessment, risk assessment scoring system, gatekeeper, referral
Citation: Bradley PT, Lee YK, Albutt A, Hardman J, Kellar I, Odo C, Randell R, Rousseau N, Tikka T, Patterson JM and Paleri V (2024) Nomenclature of the symptoms of head and neck cancer: a systematic scoping review. Front. Oncol. 14:1404860. doi: 10.3389/fonc.2024.1404860
Received: 21 March 2024; Accepted: 03 May 2024;
Published: 17 June 2024.
Edited by:
Gyorgy B. Halmos, University Medical Center Groningen, NetherlandsReviewed by:
Jenny Montgomery, NHS Greater Glasgow and Clyde, United KingdomCatriona M. Douglas, NHS Greater Glasgow and Clyde, United Kingdom
Copyright © 2024 Bradley, Lee, Albutt, Hardman, Kellar, Odo, Randell, Rousseau, Tikka, Patterson and Paleri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paula T. Bradley, cGF1bGEuYnJhZGxleUBuZXdjYXN0bGUuYWMudWs=