 Jiamin Xu
Jiamin Xu Shukun Mu2
Shukun Mu2 Suchun Yu
Suchun Yu Zhongming Wang
Zhongming Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 16 July 2024
Sec. Cancer Immunity and Immunotherapy
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1400193
This article is part of the Research Topic Immunology and Immunotherapy of Skin Cancer View all 14 articles
The incidence of melanoma is increasing year by year and is highly malignant, with a poor prognosis. Its treatment has always attracted much attention. Among the more clinically applied immunotherapies are immune checkpoint inhibitors, bispecific antibodies, cancer vaccines, adoptive cell transfer therapy, and oncolytic virotherapy. With the continuous development of technology and trials, in addition to immune monotherapy, combinations of immunotherapy and radiotherapy have shown surprising efficacy. In this article, we review the research progress of immune monotherapy and combination therapy for advanced melanoma, with the aim of providing new ideas for the treatment strategy for advanced melanoma.
Melanoma is one of the most lethal and aggressive malignant tumors in the world. Its morbidity and mortality are increasing year by year, and the incidence of melanoma in men is slightly higher than that in women (1). Melanoma mostly occurs in the skin but also in mucous membranes, the uveal tract, and leptomeninges (2). Moreover, melanoma is prone to exhibit microsatellite, satellite, lymph node, or distant metastasis patterns to the lungs, brain, liver, and soft tissues and has a high local recurrence ability (3).
Immunotherapy is a treatment method that activates the human immune system and relies on its own immune function to cause cancer cells to die. For patients with melanoma that is surgically resectable, immunotherapy can serve as an adjuvant treatment to improve the prognosis. For patients with inoperable melanoma, immunotherapy can replace surgery, providing a new treatment direction (4, 5). Common clinical immunotherapies include immune checkpoint inhibitors, bispecific antibodies, cancer vaccines, adoptive cell therapy, and oncolytic virotherapy. This article reviews the clinical application of immunotherapy for advanced (unresectable or metastatic) melanoma, as well as the latest progress of combined radiotherapy.
The immune checkpoint includes cytotoxic T lymphocyte-associated antigen-4 (CTLA-4), programmed death-1 (PD-1) and its ligand (PD-L1), and lymphocyte activation gene-3 (LAG-3). They negatively regulate CD8+ T cells, and cancer cells may make use of this pathway to downregulate T cell responses, thereby avoiding immune attacks (6). Immune checkpoint inhibitors (ICIs), on the other hand, activate immune cell activity by blocking immune checkpoint molecules, thereby achieving anti-tumor effects. There are many factors that affect the efficacy of ICIs, including tumor microenvironment (TME), age, diet, genetics, intestinal microbiota, antibiotics, and infusion time of ICIs (7, 8). Among them, a study found that injecting ICIs during the day (before 3 p.m.) may better integrate with the intrinsic circadian rhythm of the immune system to prolong the overall survival (OS) of patients (9). In addition, the efficacy of different ICIs varies, and with the deepening of research, drugs are constantly being updated and upgraded.
Ipilimumab is a monoclonal antibody that blocks the binding of CTLA-4 to its ligand on antigen-presenting cells. In addition to poor physical condition and elevated lactate dehydrogenase and C-reactive protein levels, endostatin and galactin-3-binding proteins may serve as prognostic biomarkers for advanced melanoma patients receiving ipilimumab treatment (10). When using ipilimumab monotherapy, the dosage has an impact on the efficacy of advanced melanoma. A study showed that 10 mg/kg of ipilimumab brings more significant survival benefits to patients than 3 mg/kg of ipilimumab, with median OS of 15.7 months and 11.5 months, respectively (p = 0.04), and 5-year OS rates of 25% and 19%, respectively. However, the incidence of level 3 or 4 treatment-related adverse events (AEs) is also higher (36% vs. 20%) (11). Besides clinical trials, the Ipi4 study showed similar efficacy in real-world advanced melanoma patients receiving an intravenous injection of 3 mg/kg of ipilimumab, with a median OS of 12.1 months and a 5-year OS rate of 20% (12). Although ipilimumab was the first ICI, with the continuous development of drugs, ipilimumab monotherapy is no longer the preferred first-line treatment for advanced melanoma.
Humanized IgG4 kappa monoclonal antibodies that target PD-1 are nivolumab, pembrolizumab, cetrelimab, toripalimab, and camrelizumab. Nivolumab proved to be a highly durable first-line therapy for advanced melanoma in the CheckMate 066 trial, with a median overall survival of 37.3 months, a 5-year OS of 43%, and a progression-free survival (PFS) rate of 32% (13). In 151 previously untreated patients with unresectable advanced melanoma, pembrolizumab demonstrated sustained anti-tumor activity and tolerability in the KEYNOTE-001 study, with a five-year OS rate of up to 41% and a median OS of 38.6 months (14). Pembrolizumab had a lower incidence of 3–4 grade adverse events than ipilimumab, according to the KEYNOTE–006 research, and it has higher clinical efficacy in treating advanced melanoma. The two patient groups had respective median OS of 32.7 months and 15.9 months (p = 0.00049), and respective median PSFs of 8.4 months and 3.4 months (p < 0.0001) (15). Furthermore, research indicated that patients who achieve early disease stabilization with pembrolizumab have a fair likelihood of long-term survival and a high chance of establishing a complete or partial remission with ongoing pembrolizumab treatment (16). In the LUC1001 study, the results of cetrelimab’s first treatment for advanced solid tumors were encouraging, with an overall response rate of 28% for melanoma patients and a median PFS of 5.4 months (17). Similarly, camrelizumab showed preliminary anti-tumor activity in the first treatment of advanced solid tumor patients in Australia (18). Moreover, in the subsequent Phase I study on patients with advanced melanoma in Asia, the efficacy of camrelizumab was similar to that of toripalimab in the POLARIS-01 study, with objective response rates (ORRs) of 15.2% and 17.3%, respectively (19, 20).
Prolgolimab is an IgG1 anti-PD-1 monoclonal antibody with Fc-silenced LALA (L234A/L235A) mutations. The MIRACULUM study was the first to evaluate the clinical efficacy of prolgolimab in advanced melanoma. The overall response rates of intravenous injections of 1 mg/kg prolgolimab (Group 1) and 3 mg/kg prolgolimab (Group 2) were 38.1% and 28.6%, respectively. Among them, the efficacy of primary skin melanoma patients in Group 1 was more significant, with ORR and median PFS of 48.9% and 8.84 months, respectively (21).
Atezolizumab, avelumab, and durvalumab are anti-PD-L1 agents that are mostly used in combination with targeted agents for the treatment of advanced BRAF-mutant melanoma. In a phase I trial, atezolizumab was safe and well tolerated as a first-line monotherapy in patients with advanced BRAF-mutant melanoma, with an ORR and median PSF of 35% and 3.7 months, respectively (22). The international phase III trial IMspire170 found that atezolizumab in combination with cobimetinib (a MEK inhibitor) did not improve PSF in patients with advanced melanoma compared to pembrolizumab monotherapy, with 5.5 and 5.7 months, respectively (23). However, the IMspire150 trial showed that a triple combination with atezolizumab significantly prolonged PFS in patients with BRAF-mutated melanoma compared to a combination of vemurafenib (a BRAF inhibitor) and cobimetinib (15.1 months vs. 10.6 months, p = 0.025) (24). A phase I trial found durvalumab in combination with dabrafenib (a BRAF inhibitor) and trametinib (a MEK inhibitor) to be feasible for the treatment of BRAF-mutant melanoma (25). And avelumab showed a durable response in previously treated patients with metastatic melanoma, with an ORR of 21.6% and median PSF and OS of 3.1 and 17.2 months, respectively (26).
Bispecific antibodies have been extensively studied as an effective immunotherapy for advanced melanoma (Table 1).
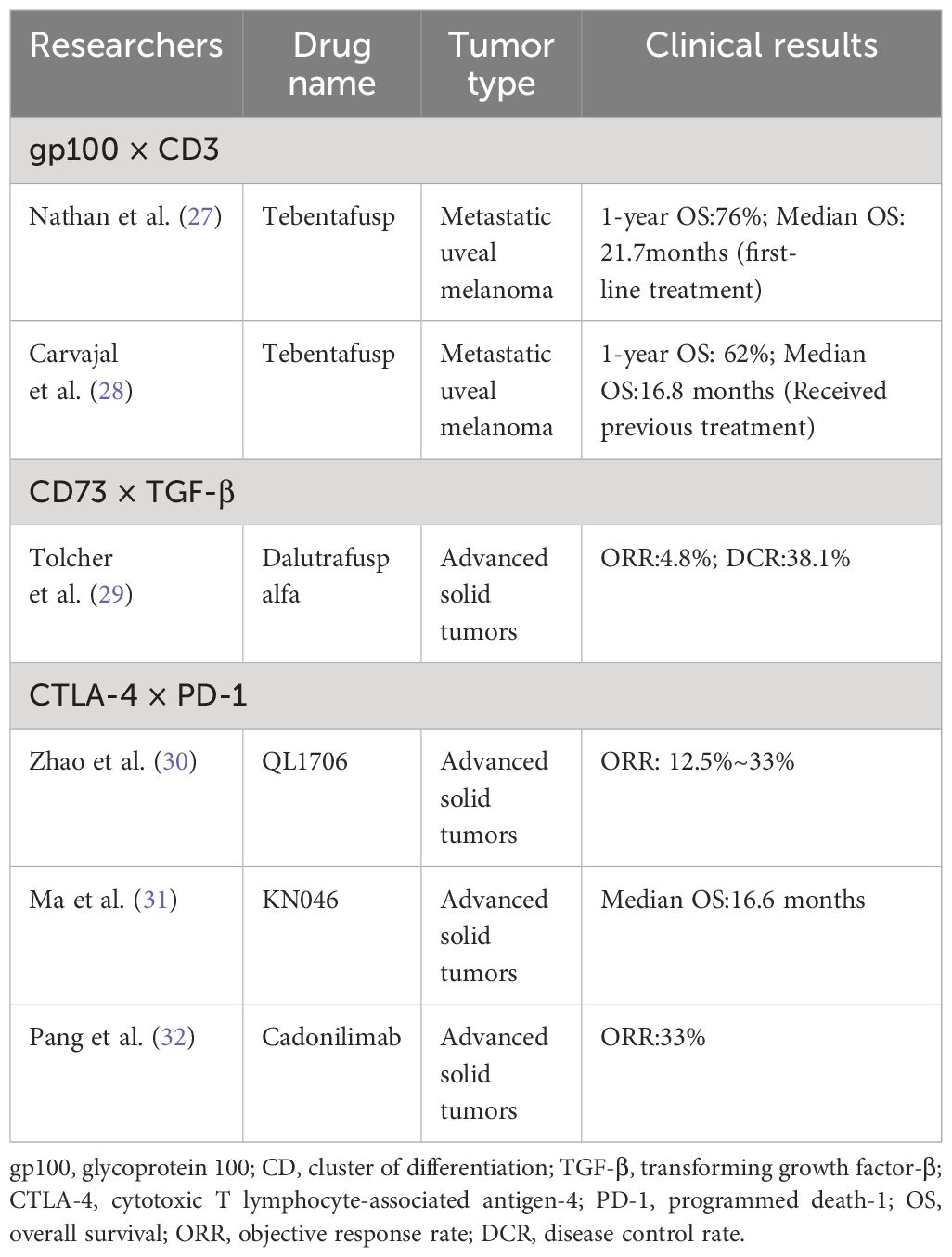
Table 1 Clinical application of bispecific antibody in advanced tumors.
Tebentafusp is a bispecific fusion protein composed of soluble high-affinity T cell receptors, targeting glycoprotein 100 (gp100) and cluster of differentiation (CD) 3 (33). In 2022, tebentafusp was approved by the Food and Drug Administration for the treatment of advanced uveal melanoma (34). For patients with metastatic uveal melanoma, tebentafusp as a first-line treatment has a 1-year OS rate of up to 73%, bringing significant survival benefits to patients (27). And for patients who have received previous treatment, tebentafusp also exhibits strong anti-tumor activity. By using a gradual dosing regimen (20 μg on Day 1, 30 μg on Day 8, 68 μg on Day 15, then injecting 68 μg intravenously once a week), the median OS was 16.8 months. Treatment-related AEs mostly occurred in the early stages of treatment, and the incidence and severity of AE decreased with repeated administration (28, 35). IMA401 is a T-cell antigen receptor bispecific drug targeting MAGEA4/8, co-developed by Bristol Myers Squibb and Immatics. The drug has demonstrated complete remission in a variety of in vivo tumor models, and the therapy is currently undergoing a Phase I trial in solid tumors in anticipation of the results being announced.
Dalutrafusp alfa is a bifunctional humanized antibody that targets both CD73-adenosine and transforming growth factor-β (TGF-β), and patients with advanced solid tumors have good tolerance to it (29). From this, it can be seen that dalutrafusp alfa has certain therapeutic potential for patients with advanced melanoma.
QL1706 is a bispecific antibody generated by MabPair technology that also targets CTLA-4 and PD-1. In a phase I trial targeting patients with advanced solid tumors (including advanced melanoma), QL1706 showed good anti-tumor efficacy and tolerance (30). Based on the promising preliminary efficacy of QL1706, it is worth further clinical research in advanced melanoma. KN046 is a novel bispecific antibody produced by Chinese hamster ovarian cells that can simultaneously block CTLA-4 and PD-1. In a multicenter phase I study, KN046 showed encouraging anti-tumor activity and controllable safety in the treatment of advanced solid cancer, and patients with high expression of CD8 and PD-1 had a longer median OS (31). However, the sample size of advanced melanoma is relatively small, and its efficacy needs to be verified in a large sample size. Cadonilimab is a symmetric tetravalent bispecific antibody against CTLA-4 and PD-1 with lower toxicity than the combination of CTLA-4 inhibitors and PD-1 inhibitors. It exhibits good clinical activity in advanced gastric esophageal cancer and metastatic cervical cancer (32). For advanced melanoma, there is still a lack of clinical trials to verify the efficacy of cadonilimab, but it is worth a try.
Cancer vaccines are a promising immunotherapy consisting of tumor-related antigens and vaccine adjuvants. Common vaccines for treating melanoma include peptide vaccines, nucleic acid vaccines, cell vaccines, and nano vaccines.
Dendritic cell (DC) vaccines have been widely studied in melanoma. A team in the United States developed a DC-based genetically engineered vaccine using a recombinant adenovirus that co-expresses three melanoma antigens (tyrosinase, MART-1, and MAGE-A6). The study found that the expression of an inducible co-stimulator ligand on DCs in melanoma patients was positively correlated with the patient survival rate (36). This suggests that the treatment outcomes of patients can be improved by regulating the expression of an inducible co-stimulator ligand. The allogeneic plasmacytoid dendritic cells (PDCs) vaccine can initiate and amplify tumor-specific T cells. In the GeniusVac-Mel4 clinical trial, allogeneic PDC vaccines were subcutaneously injected into patients with metastatic melanoma, and the patients showed good tolerance (37). The tumor lysate particle-loaded dendritic cell vaccine is a personalized vaccine made by loading autologous tumor lysate into yeast cell wall particles and introducing patient DCs. Upregulation of genes related to DC maturation in tumor lysate particle-loaded dendritic cell vaccines that did not harvest DC using granulocyte colony stimulating factors can bring outstanding survival benefits to patients with advanced melanoma (3-year disease-free survival and OS rates of 55.8% and 94.2%, respectively) (38).
In addition to the DCs vaccine, there are other vaccines that exhibit anti-tumor activity against advanced melanoma. For example, vaccines developed for major histocompatibility complex-restricted phosphopeptides have been used for the first time in patients with advanced melanoma. Among them, the pIRS21097–1105 and pBCAR3126–134 phosphopeptide vaccines have good tolerance and clinical benefit prospects (39). A recombinant HSP110–gp100 vaccine was prepared from heat shock proteins 110 (HSP110) derived from autologous tumors and melanoma-associated antigen gp100. The lower dose (30–60 mcg) of the recombinant HSP110–gp100 vaccine showed clinical activity and low toxicity in patients with advanced melanoma (40). These vaccines are worth further research to improve the prognosis of patients.
Oncolytic virotherapy is a new type of immunotherapy. The use of natural or genetically recombinant viruses, through a dual mechanism of selective killing of tumor cells and inducing systemic anti-tumor immunity, brings clinical benefits to cancer patients (41). It has a good therapeutic effect in treating advanced melanoma (Table 2).
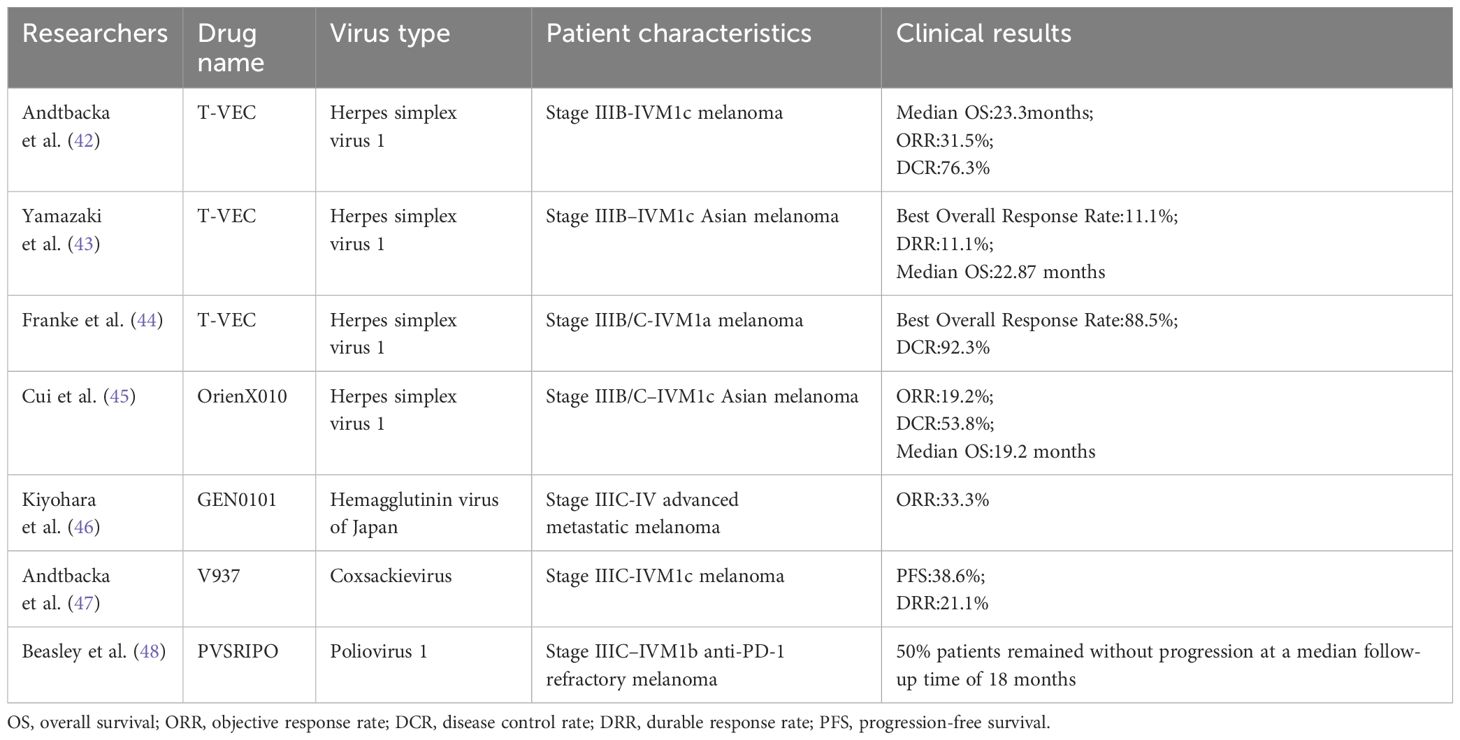
Table 2 Clinical application of Oncolytic virotherapy in the treatment of advanced melanoma.
Talimogene laherparepvec (T-VEC) is a type 1 genetically modified herpes simplex virus. Through genetic modification, the deletion of the infected cell protein (ICP) 34.5 gene and the ICP47 gene, as well as the addition of granulocyte macrophage colony stimulating factor (GM-CSF), enhances the anti-tumor effect (49). Research has found that increasing the infection of T-VEC on susceptible tumor cells can improve the therapeutic effect of T-VEC, and overexpression of GM-CSF may have a negative impact on the curative effect of T-VEC. Therefore, the activation rate of GM-CSF is worth considering when designing T-VEC (50). For non-Asian populations, the OPTiM study found that compared to subcutaneous injection of GM-CSF, T-VEC had a more pronounced impact on OS in patients with advanced melanoma (23.3 months vs. 18.9 months, p = 0.0494), with ORRs of 31.5% and 6.4%, respectively, and a durable response rate (DRR) of 19.0% and 1.4%, respectively (42). For the Asian population, a multicenter Phase I trial in Japan showed that T-VEC exhibited similar clinical activity in patients with unresectable advanced melanoma, with a DRR of 11.1%. Among them, 77.8% of patients had treatment-related AEs, but their tolerance is good (43). For patients with early-stage metastatic melanoma, the optimal overall response rate of T-VEC is as high as 88.5%, and the disease control rate (DCR) is 92.3% (44). A clinical prediction model in the Netherlands further validated the above results, and patients with lower tumor burden showed better efficacy in using T-VEC (51).
OrienX010is also a type 1 herpes simplex virus that has undergone genetic modification. Its main operations include deleting the ICP34.5 gene and the ICP47 gene and inserting the inactivated ICP6 gene (which can reduce the potential neurotoxicity of injection) and GM-CSF. Intratumoral injection of OrienX010has a positive anti-tumor effect on Asian advanced melanoma patients, with an ORR of 19.2% and a DCR of 53.8% (45). And for patients with heavier tumor loads, higher doses of OrienX010may have more remarkable survival benefits.
The Hemagglutinin virus of Japan (HVJ) is a single-negative-stranded RNA virus. RNA fragments in the HVJ-envelope (HVJ-E) are absorbed into cells through membrane fusion, which can induce cancer cell death and stimulate anti-tumor immunity (52). In the Phase I clinical trial, HVJ-E (GEN0101) with 30000 mNAU and 60000 mNAU was administered to patients with advanced melanoma without dose-limiting toxicity. The anti-tumor activity increased in a dose-dependent manner, and the target lesion response rate increased from 44% in the low-dose group to 78% in the high-dose group (46).
Coxsackievirus A21 (V937) is a single-positive-stranded RNA enterovirus that can enter cells through overexpressed intercellular adhesion molecule-1 and decay-accelerating factor receptors in melanoma. The use of V937 in the CALM trial for the treatment of unresectable advanced melanoma resulted in a 6-month PFS rate of 38.6% and a DRR of 21.1%, with good patient tolerance and no treatment-related AEs of grade 3 or above (47).
PVSRIPO is a genetically modified type 1 poliovirus that can infect CD155-expressing antigen-presenting cells, thereby triggering an immune response targeting tumors. For advanced melanoma patients who are difficult to treat with PD-1, injection of PVSRIPO into the tumor shows clinical activity and good tolerance (48).
Adoptive cell therapy refers to the separation of immune-active cells from tumor patients, followed by in vitro culture, amplification, and functional identification before re-infusion into the patient’s body, achieving the goal of directly killing the tumor or activating the immune response in the body to eliminate the tumor (53). Immune cells mainly include tumor-infiltrating lymphocytes (TILs), natural killer cells, lymphokine-activated killer cells, etc. TIL therapy has been extensively studied in advanced melanoma and usually requires a combination of immune regulatory factors to stimulate TIL activity. Interleukin-2 (IL-2) is a cytokine stimulator for T cells, natural killer cells, lymphokine-activated killer cells, and B cells, which can promote lymphocyte growth, proliferation, and differentiation and is often used in combination with TIL.
In a phase III multicenter trial (NCT02278887) in the Netherlands, the median PFS of 84 patients receiving TIL (intravenous high-dose IL-2) treatment for unresectable advanced melanoma was significantly higher than that of ipilimumab treatment (7.2 months vs. 3.1 months, p < 0.001), but the incidence of treatment-related AEs also increased (54). However, in a phase II trial, subcutaneous injections of low-dose IL-2 (125000 IU/kg/day) were administered to patients with advanced melanoma using TIL therapy. Although reducing the toxicity caused by IL-2, the curative effect also decreased (55). For advanced melanoma patients who have failed ICIs treatment, TIL therapy (intravenous high-dose IL-2) has shown clinical activity in different subtypes (mucosal, superficial diffusion, and limb), but there are reversible AEs of grade 3 and grade 4 (56). In addition, there are also studies using low-dose interferon alpha to replace the previous pretreatment process (nonmyeloablative lymphodepleting chemotherapy combined with high-dose IL-2) for TIL therapy. The clinical benefits to patients are long-lasting, with a 3-year OS of 46.7% in responsive patients. Nevertheless, interferon alpha can lead to a decrease in white blood cells, neutrophils, and lymphocytes (57). Lifileucel (LN-144), a TIL therapy developed by Iovance Biotherapeutics, is produced from harvested tumor specimens using a simplified 22-day process in a centralized Good Manufacturing Practices facility, and in the Phase 2 C-144–01 trial, lifileucel demonstrated sustained clinical activity in the treatment of patients with advanced melanoma who had received prior ICI therapy (58). The therapy is currently in the FDA review stage and is expected to be the world’s first immunocellular therapy for the treatment of solid tumors (59).
In addition to using TIL for adoptive cell therapy, the MELSORT trial selected T lymphocytes with specificity for Melan-A and MELOE-1 antigens and high-dose IL-2. This combination has shown clinical activity in advanced melanoma patients and is expected to be used in conjunction with ICIs to enhance efficacy (60). IMA203 is an autologous T-cell receptor-engineered T-cell therapy developed on Immatics’ proprietary ACTengine platform targeting the melanoma antigen PRAME presented by HLA-A*02. The company has now announced clinical data from its ongoing 1b-dose expansion cohort A. The data showed that IMA203 was well tolerated and resulted in confirmed objective remissions in melanoma. The trial of IMA203 in combination with ICIs is ongoing, and the results are expected to be announced.
The combination of CTLA-4 inhibitors and PD-1 inhibitors has shown more lasting clinical benefits than single therapy in unresectable advanced melanoma. In the Phase III CheckMate 067 trial (NCT01844505), the 5-year OS rate of ipilimumab combined with nivolumab for advanced skin melanoma was 52%, with a median PFS of 11.5 months and an ORR of 58%. 59% of patients experienced grade 3 or 4 treatment-related AEs (61). Wolchok et al. (62) further studied on the basis of this experiment and found that the 6.5-year median OS was 72.1 months, and the median melanoma-specific survival period was not reached at 77 months. The drug tolerance was good, and no new AE occurred. In addition to clinical trials, the combination of ipilimumab and nivolumab also brings long-term survival benefits to patients in the real world, with a 4-year OS of 50% for patients similar to the CheckMate 067 trial (63). For patients with metastatic uveal melanoma, ipilimumab combined with nivolumab as first-line treatment also showed outstanding clinical activity, significantly improving the patient’s OS compared to monotherapy (64, 65). In addition, the dosage of ICIs has a certain impact on anti-tumor activity and safety. The KEYNOTE-029 study showed that, compared with standard-dose ipilimumab (3 mg/kg) plus reduced-dose nivolumab (1 mg/kg) in the treatment of advanced melanoma, the combination of reduced-dose ipilimumab (1 mg/kg) and standard-dose pembrolizumab (2 mg/kg) significantly reduced the toxicity associated with the combination therapy and provided survival benefits to patients (66). This dose combination mode is also applicable to advanced melanoma patients who have failed PD-1 inhibitor treatment, with a median OS of 24.7 months and controllable safety (67).
The combination of LAG-3 inhibitors and PD-1 inhibitors is also more effective than monotherapy in the treatment of advanced melanoma and has the potential to become a first-line treatment. Relatlimab is a humanized monoclonal antibody targeting LAG-3. In the RELATIVITY-047 trial, a median PFS of 10.1 months was observed in untreated patients with advanced melanoma who received a single intravenous infusion of relatlimab (160 mg) and nivolumab (480 mg), which was significantly prolonged by 5.5 months compared to nivolumab monotherapy (p = 0.006). Although the incidence of AE was slightly higher, it was well tolerated (68). Schadendorf et al. (69) further demonstrated the above results by studying the health-related quality of life of patients based on this experiment. For advanced melanoma patients who have progressed after receiving previous treatment (including anti-PD-1 therapy), relatlimab combined with nivolumab can also bring long-lasting survival benefits. And Opdualag, a fixed-dose combination of relatlimab and nivolumab, has been approved by the FDA in March 2022 for the treatment of unresectable or metastatic melanoma (70). Efftilagimod alpha is a soluble LAG-3 fusion protein that can activate antigen-presenting cells, thereby activating CD8+ T cells. In a multicenter Phase I trial, for the first time, efftilagimod alpha combined with pembrolizumab was used to treat advanced melanoma. The treatment mode showed strong anti-tumor activity in both pembrolizumab refractory and pembrolizumab initially treated patients, with overall remission rates of 33% and 50% and DCR of 55.6% and 83%, respectively (71).
UV1 is a human telomerase reverse transcriptase vaccine composed of three synthetic long peptides, which can enhance anti-tumor activity when combined with ICIs. In the phase I/II single-center clinical trial (NCT02275416), the combination of UV1 and ipilimumab showed controllable safety in the treatment of metastatic melanoma with no additional toxicity. The ORR was 33%, the 5-year OS was 50%, and the median PFS was 6.7 months (72, 73). In addition, a multicenter phase I trial (NCT03538314) is underway for the treatment of advanced melanoma using UV1 combined with pembrolizumab.
Six melanoma helper peptide vaccines, limited by the class II major histocompatibility complex, can induce CD4+ T helper cell responses. Combined with pembrolizumab, they can increase the number of T cells, B cells, and Th1 cells in the tumor. Especially for advanced melanoma patients who did not receive other immunotherapies before the combination therapy, the clinical benefits were more significant (74).
The vaccine developed for the tumor associated-antigen NY-ESO-1 can induce CD4+ and CD8+ T cells, as well as antibody responses. Ipilimumab can also enhance the immunity of the NY-ESO-1 vaccine. The combination of the two can have a beneficial effect on TME in the treatment of advanced melanoma, increasing the proliferation of CD8+ T cells within the tumor and ensuring controllable safety (75).
NEO-PV-01 is a personalized vaccine made based on new antigens generated by cancer cell mutations. Its induced T cells have a cytotoxic phenotype and can be transported to tumors and kill cancer cells. The combination of NEO-PV-01 and nivolumab has shown strong potential in the treatment of advanced melanoma. In a phase Ι clinical trial, the ORR of patients after combination therapy was 59%, the 1-year OS rate was 96%, and there were no severe treatment-related AEs (76).
The phase 2 KEYNOTE-942 trial evaluated the efficacy of mRNA-4157/V940, a personalized cancer vaccine developed by Moderna, in combination with pembrolizumab for patients with advanced melanoma. The results showed a significant improvement in recurrence-free survival compared to pembrolizumab monotherapy, resulting in a 44% reduction in the risk of postoperative recurrence or death (77). These findings are encouraging and have led to the therapy being granted breakthrough therapy designation by the FDA.
A study has found that new epitope-specific CD8+ T cells affect the efficacy of TIL adoptive cell therapy in treating melanoma (78). Using ICIs to increase the frequency of CD8+ T cells may improve clinical outcomes. In a phase I trial, TIL adoptive cell therapy combined with nivolumab was safe and feasible for the treatment of metastatic melanoma patients who had not received PD-1 inhibitors, with an ORR of 36% and a median OS of 23 months. The use of CD137 agonists during TIL generation in vitro can reduce culture time and increase tumor-specific activity (79). TILVANCE-301 is a multicenter Phase 3 trial designed to evaluate the efficacy and safety of lifileucel in combination with pembrolizumab versus pembrolizumab alone in patients with untreated advanced melanoma. The trial is currently ongoing, and the results are promising.
T-VEC can overcome adaptive resistance by inducing systemic immune activity and altering TME, and its combination with ICIs has shown excellent clinical efficacy in the treatment of advanced melanoma (80). A multicenter phase II trial with a 5-year follow-up showed that the ORR of T-VEC combined with ipilimumab for unresectable stage IIIB-IV melanoma was more than twice that of ipilimumab monotherapy (35.7% vs. 16.0%, p = 0.0003), with DRRs of 33.7% and 13.0%, respectively, and no additional toxicity (81). T-VEC in combination with pembrolizumab showed some improvement in efficacy in patients with advanced melanoma, with an ORR of 48.6% and a DRR of 42.2% (82).
The combination of V937 and ICIs has shown encouraging results in the treatment of advanced melanoma. The ORR of advanced melanoma patients in the CAPRA study receiving intratumoral injection of V937 combined with pembrolizumab treatment was 47%, with a median PFS of 11.9 months, both higher than monotherapy, and the safety was controllable (83). In the MITCI trial, the ORR and DRR of intratumoral injections of V937 and ipilimumab for advanced melanoma patients were 30% and 14%, respectively. Among them, patients who had previously undergone PD-1 inhibitor treatment and experienced disease progression also had clinical benefits (median OS of 29.7 months) (84). In addition to intratumoral injection of V937, the STORM trial showed that intravenous injection of V937 in combination with pembrolizumab has controllable safety in patients with advanced solid tumors (85). However, in the CLEVER study, intravenous injection of V937 combined with ipilimumab did not bring significant survival benefits to patients with advanced uveal melanoma (86).
RP1, a herpes simplex virus-based lysosomal viral therapy developed by Replimune, showed activity in combination with nivolumab in melanoma that failed PD-1 immunotherapy in the Phase 2 IGNYTE trial (NCT03767348), promising to provide patients with a novel treatment option. In addition to this, the team has developed RP2 (adding CTLA-4 antibody-like molecules to RP1) and RP3 (adding 4–1BBL and CD40L to RP2) and launched clinical trials in solid tumors.
For melanoma patients with ICI resistance (primary or secondary resistance), in addition to the aforementioned immune combination therapy, new therapies are also needed to improve the condition. The DC vaccine can effectively activate T lymphocytes, and its combination with TIL therapy may improve patient prognosis. In a phase I trial, this combination therapy showed clinical activity (87). Furthermore, the feasibility of DC plus TIL was further demonstrated in the Phase II trial, with a patient’s ORR of 50% (88). However, only DC vaccines targeting multiple antigens have shown efficacy, and both trials have small sample sizes, requiring further validation in more patients. In addition to being used in combination with TIL, the DC vaccines can also be combined with T-VEC. In a phase I trial, T-VEC and CD1c (BDCA-1) + bone marrow DC vaccine +/- CD141 (BDCA-3) + bone marrow DC vaccine were injected into advanced melanoma patients who failed ICIs treatment. The results were satisfactory, with 66.7% of patients (n = 3) experiencing persistent complete remission (89).
During the occurrence and development of tumors, TME interacts with tumor cells, jointly mediating the immune tolerance of tumors, thereby affecting the therapeutic effect of immunotherapy. Radiotherapy is the use of energy emitted by radiation to cause structural changes and loss of biological activity in tumor cells, leading to tumor apoptosis and necrosis, thus achieving the goal of treatment. Research has shown that radiotherapy can induce immunogenic cell death, leading to a large number of damages-related molecular patterns and cytokine expression and release, activating anti-tumor immune responses (90). In addition, radiation therapy can also promote the infiltration of effector immune cells into TME, thereby enhancing the immune system’s ability to recognize and kill tumor cells (91, 92). And in some cases, local radiotherapy may also trigger a systemic anti-tumor response (distant effect) in unirradiated areas, which may be related to immune activation triggered by DNA damage induced by radiotherapy (93). Therefore, radiotherapy may enhance the effectiveness of immunotherapy and improve the prognosis of patients.
The combination of immunotherapy and radiotherapy has great potential in the treatment of advanced melanoma (Table 3).
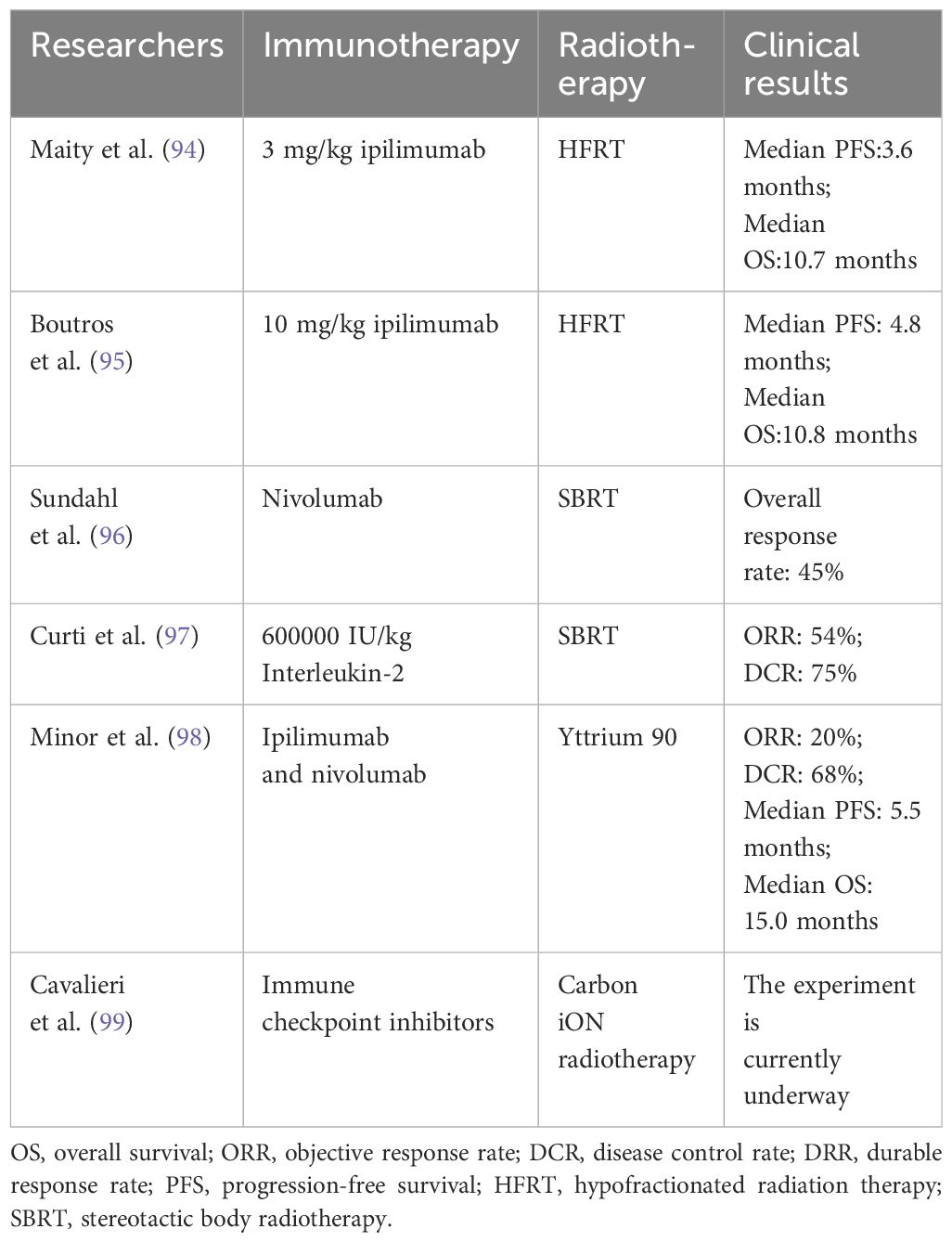
Table 3 Clinical application of immunotherapy combined with radiotherapy in advanced melanoma.
Hypofractionated radiation therapy combined with ipilimumab has also shown clinical activity in the treatment of metastatic melanoma. The median PSF and OS of 3 mg/kg ipilimumab combined with hypofractionated radiation therapy were 3.6 months and 10.7 months, respectively, and there was no dose-limiting toxicity caused by the combination therapy (94). The median PSF and OS of 10 mg/kg ipilimumab combined with hypofractionated radiation therapy were 4.8 months and 10.8 months, respectively (95). Although the doses of ipilimumab in the two Phase I trials mentioned above were different and the radiotherapy regimen was also different, the clinical results were similar.
Studies have found that stereotactic body radiation therapy (SBRT) combined with immunotherapy can alter the immune phenotype of blood T cells in patients with advanced melanoma (100). In a phase II trial, the overall response rate of SBRT combined with nivolumab for advanced melanoma was 45%, and it was found through circulating tumor DNA that the combination of SBRT can bring survival benefits to patients with lower PD-1 comprehensive positive scores (96). In addition, the combination of SBRT and high-dose IL-2 (600000 IU/kg) also showed satisfactory results, with ORR and DCR of 54% and 75%, respectively, in patients with metastatic melanoma (97). And the immune activity of this combination was further confirmed in a phase II experiment (101).
In a multicenter prospective clinical trial, patients with uveal melanoma with liver metastasis were treated with sequential hepatic arterial infusion of Yttrium 90 resin microspheres with a normal liver radiation limit dose of 35 Gy and combined with ipilimumab (1 mg/kg) and nivolumab (1 mg/kg or 3 mg/kg). The results of the study were promising. The ORR and DCR of patients were 20% and 68%, respectively. The median PFS and median OS are 5.5 and 15.0 months, respectively, and the toxicity is tolerable (98).
The ICONIC study is the first to combine carbon-ion radiation therapy with ICIs for the treatment of advanced solid tumor patients. The trial is currently underway, and its results may provide new treatment options for advanced melanoma patients (99).
Tumors evade the immune system through a synergistic process of central and peripheral tolerance. ICIs can overcome peripheral tolerance and bring survival benefits to cancer patients. However, for immunocompromised patients, long-term benefits cannot be achieved due to insufficient tumor-specific CD8+ T cells or insufficient new antigenicity. In addition to ICIs, bispecific immunotherapy, cancer vaccines, adoptive cell therapy, and oncolytic virotherapy are all immunotherapies that are currently being studied in advanced melanoma. The combination of different immunotherapies has brought new hope to patients who have not received immunotherapy or who have previously received immunotherapy but have progressed, and it has greatly improved the prognosis of patients with advanced melanoma. Based on the synergy between radiotherapy and immunotherapy, the combination of the two is promising. Further studies are needed on the selection of immunotherapy, dosage, and route of administration, as well as the choice of radiotherapy technique and radiation dose in combination therapy, in order to improve the survival rate of patients without adding additional toxic reactions.
JX: Writing – original draft, Writing – review & editing. SM: Writing – review & editing. YW: Writing – review & editing. SY: Writing – review & editing. ZW: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Elder DE, Bastian BC, Cree IA, Massi D, Scolyer RA. The 2018 world health organization classification of cutaneous, mucosal, and uveal melanoma: detailed analysis of 9 distinct subtypes defined by their evolutionary pathway. Arch Pathol Lab Med. (2022) 144:500–22. doi: 10.5858/arpa.2019-0561-RA
3. Amalinei C, Grigoraş A, Lozneanu L, Căruntu ID, Giuşcă SE, Balan RA. The interplay between tumour microenvironment components in Malignant melanoma. Medicina (Kaunas). (2022) 58:365. doi: 10.3390/medicina58030365
4. Amaria RN, Postow M, Burton EM, Tetzlaff MT, Ross MI, Torres-Cabala C, et al. Neoadjuvant relatlimab and nivolumab in resectable melanoma. Nature. (2021) 611:155–60. doi: 10.1038/s41586-022-05368-8
5. McQuade JL, Homsi J, Torres-Cabala CA, Bassett R, Popuri RM, James ML, et al. A phase II trial of recombinant MAGE-A3 protein with immunostimulant AS15 in combination with high-dose Interleukin-2 (HDIL2) induction therapy in metastatic melanoma. BMC Cancer. (2018) 18:1274. doi: 10.1186/s12885-018-5193-9
6. Marei HE, Hasan A, Pozzoli G, Cenciarelli C. Cancer immunotherapy with immune checkpoint inhibitors (ICIs): potential, mechanisms of resistance, and strategies for reinvigorating T cell responsiveness when resistance is acquired. Cancer Cell Int. (2023) 23:64. doi: 10.1186/s12935-023-02902-0
7. Li YZ, Zhang HM. Recent advances in primary resistance mechanisms against immune checkpoint inhibitors. Curr Opin Oncol. (2022) 34:95–106. doi: 10.1097/CCO.0000000000000802
8. Spyrou N, Vallianou N, Kadillari J, Dalamaga M. The interplay of obesity, gut microbiome and diet in the immune check point inhibitors therapy era. Semin Cancer Biol. (2021) 73:356–76. doi: 10.1016/j.semcancer.2021.05.008
9. Qian DC, Kleber T, Brammer B, Xu KM, Switchenko JM, Janopaul-Naylor JR, et al. Effect of immunotherapy time-of-day infusion on overall survival among patients with advanced melanoma in the USA (MEMOIR): a propensity score-matched analysis of a single-centre, longitudinal study. Lancet Oncol. (2021) 22:1777–86. doi: 10.1016/S1470-2045(21)00546-5
10. Nyakas M, Aamdal E, Jacobsen KD, Guren TK, Aamdal S, Hagene KT, et al. Prognostic biomarkers for immunotherapy with ipilimumab in metastatic melanoma. Clin Exp Immunol. (2019) 197:74–82. doi: 10.1111/cei.13283
11. Ascierto PA, Del Vecchio M, Mackiewicz A, Robert C, Chiarion-Sileni V, Arance A, et al. Overall survival at 5 years of follow-up in a phase III trial comparing ipilimumab 10 mg/kg with 3 mg/kg in patients with advanced melanoma. J Immunother Cancer. (2020) 8:e000391. doi: 10.1136/jitc-2019-000391
12. Aamdal E, Jacobsen KD, Straume O, Kersten C, Herlofsen O, Karlsen J, et al. Ipilimumab in a real-world population: A prospective Phase IV trial with long-term follow-up. Int J Cancer. (2022) 150:100–11. doi: 10.1002/ijc.33768
13. Robert C, Long GV, Brady B, Dutriaux C, Di Giacomo AM, Mortier L, et al. Five-year outcomes with nivolumab in patients with wild-type BRAF advanced melanoma. J Clin Oncol. (2022) 38:3937–46. doi: 10.1200/JCO.20.00995
14. Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann Oncol. (2019) 30:582–8. doi: 10.1093/annonc/mdz011
15. Robert C, Ribas A, Schachter J, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. (2019) 20:1239–51. doi: 10.1016/S1470-2045(19)30388-2
16. Hamid O, Robert C, Daud A, Carlino MS, Mitchell TC, Hersey P, et al. Long-term outcomes in patients with advanced melanoma who had initial stable disease with pembrolizumab in KEYNOTE-001 and KEYNOTE-006. Eur J Cancer. (2021) 157:391–402. doi: 10.1016/j.ejca.2021.08.013
17. Felip E, Moreno V, Morgensztern D, Curigliano G, Rutkowski P, Trigo JM, et al. First-in-human, open-label, phase 1/2 study of the monoclonal antibody programmed cell death protein-1 (PD-1) inhibitor cetrelimab (JNJ-63723283) in patients with advanced cancers. Cancer Chemother Pharmacol. (2022) 89:499–514. doi: 10.1007/s00280-022-04414-6
18. Lickliter JD, Gan HK, Voskoboynik M, Arulananda S, Gao B, Nagrial A, et al. A first-in-human dose finding study of camrelizumab in patients with advanced or metastatic cancer in Australia. Drug Des Devel Ther. (2020) 14:1177–89. doi: 10.2147/DDDT.S243787
19. Zhou L, Wu X, Chi Z, Si L, Sheng X, Kong Y, et al. Safety, activity, and pharmacokinetics of camrelizumab in advanced Asian melanoma patients: a phase I study. BMC Cancer. (2022) 22:565. doi: 10.1186/s12885-022-09663-5
20. Tang B, Chi Z, Chen Y, Liu X, Wu D, Chen J, et al. Safety, efficacy, and biomarker analysis of toripalimab in previously treated advanced melanoma: results of the POLARIS-01 multicenter phase II trial. Clin Cancer Res. (2020) 26:4250–9. doi: 10.1158/1078-0432.CCR-19-3922
21. Tjulandin S, Demidov L, Moiseyenko V, Protsenko S, Semiglazova T, Odintsova S, et al. Novel PD-1 inhibitor prolgolimab: expanding non-resectable/metastatic melanoma therapy choice. Eur J Cancer. (2021) 149:222–32. doi: 10.1016/j.ejca.2021.02.030
22. de Azevedo SJ, de Melo AC, Roberts L, Caro I, Xue C, Wainstein A. First-line atezolizumab monotherapy in patients with advanced BRAFV600 wild-type melanoma. Pigment Cell Melanoma Res. (2021) 34:973–7. doi: 10.1111/pcmr.12960
23. Gogas H, Dréno B, Larkin J, Demidov L, Stroyakovskiy D, Eroglu Z, et al. Cobimetinib plus atezolizumab in BRAF wild-type melanoma: primary results from the randomized phase III IMspire170 study. Ann Oncol. (2021) 32:384–94. doi: 10.1016/j.annonc.2020.12.004
24. Gutzmer R, Stroyakovskiy D, Gogas H, Robert C, Lewis K, Protsenko S, et al. Atezolizumab, vemurafenib, and cobimetinib as first-line treatment for unresectable advanced BRAFV600 mutation-positive melanoma (IMspire150): primary analysis of the randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. (2020) 395:1835–44. doi: 10.1016/S0140-6736(20)30934-X
25. Ribas A, Algazi A, Ascierto PA, Butler MO, Chandra S, Gordon M, et al. PD-L1 blockade in combination with inhibition of MAPK oncogenic signaling in patients with advanced melanoma. Nat Commun. (2020) 11:6262. doi: 10.1038/s41467-020-19810-w
26. Keilholz U, Mehnert JM, Bauer S, Bourgeois H, Patel MR, Gravenor D, et al. Avelumab in patients with previously treated metastatic melanoma: phase 1b results from the JAVELIN Solid Tumor trial. J Immunother Cancer. (2019) 7:12. doi: 10.1186/s40425-018-0459-y
27. Nathan P, Hassel JC, Rutkowski P, Baurain JF, Butler MO, Schlaak M, et al. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N Engl J Med. (2021) 385:1196–206. doi: 10.1056/NEJMoa2103485
28. Carvajal RD, Butler MO, Shoushtari AN, Hassel JC, Ikeguchi A, Hernandez-Aya L, et al. Clinical and molecular response to tebentafusp in previously treated patients with metastatic uveal melanoma: a phase 2 trial. Nat Med. (2022) 28:2364–73. doi: 10.1038/s41591-022-02015-7
29. Tolcher AW, Gordon M, Mahoney KM, Seto A, Zavodovskaya M, Hsueh CH, et al. Phase 1 first-in-human study of dalutrafusp alfa, an anti-CD73-TGF-β-trap bifunctional antibody, in patients with advanced solid tumors. J Immunother Cancer. (2023) 11:e005267. doi: 10.1136/jitc-2022-005267
30. Zhao Y, Ma Y, Zang A, Cheng Y, Zhang Y, Wang X, et al. First-in-human phase I/Ib study of QL1706 (PSB205), a bifunctional PD1/CTLA4 dual blocker, in patients with advanced solid tumors. J Hematol Oncol. (2023) 16:50. doi: 10.1186/s13045-023-01445-1
31. Ma Y, Xue J, Zhao Y, Zhang Y, Huang Y, Yang Y, et al. Phase I trial of KN046, a novel bispecific antibody targeting PD-L1 and CTLA-4 in patients with advanced solid tumors. J Immunother Cancer. (2023) 11:e006654. doi: 10.1136/jitc-2022-006654
32. Pang X, Huang Z, Zhong T, Zhang P, Wang ZM, Xia M, et al. Cadonilimab, a tetravalent PD-1/CTLA-4 bispecific antibody with trans-binding and enhanced target binding avidity. MAbs. (2023) 15:2180794. doi: 10.1080/19420862.2023.2180794
33. Middleton MR, McAlpine C, Woodcock VK, Corrie P, Infante JR, Steven NM, et al. Tebentafusp, A TCR/anti-CD3 bispecific fusion protein targeting gp100, potently activated antitumor immune responses in patients with metastatic melanoma. Clin Cancer Res. (2020) 26:5869–78. doi: 10.1158/1078-0432.CCR-20-1247
34. Dhillon S. Tebentafusp: first approval. Drugs. (2022) 82:703–10. doi: 10.1007/s40265-022-01704-4
35. Carvajal RD, Nathan P, Sacco JJ, Orloff M, Hernandez-Aya LF, Yang J, et al. Phase I study of safety, tolerability, and efficacy of tebentafusp using a step-up dosing regimen and expansion in patients with metastatic uveal melanoma. J Clin Oncol. (2022) 40:1939–48. doi: 10.1200/JCO.21.01805
36. Maurer DM, Adamik J, Santos PM, Shi J, Shurin MR, Kirkwood JM, et al. Dysregulated NF-κB-dependent ICOSL expression in human dendritic cell vaccines impairs T-cell responses in patients with melanoma. Cancer Immunol Res. (2020) 8:1554–67. doi: 10.1158/2326-6066.CIR-20-0274
37. Charles J, Chaperot L, Hannani D, Bruder Costa J, Templier I, Trabelsi S, et al. An innovative plasmacytoid dendritic cell line-based cancer vaccine primes and expands antitumor T-cells in melanoma patients in a first-in-human trial. Oncoimmunology. (2020) 9:1738812. doi: 10.1080/2162402X.2020.1738812
38. Adams AM, Carpenter EL, Clifton GT, Vreeland TJ, Chick RC, O'Shea AE, et al. Divergent clinical outcomes in a phase 2B trial of the TLPLDC vaccine in preventing melanoma recurrence and the impact of dendritic cell collection methodology: a randomized clinical trial. Cancer Immunol Immunother. (2023) 72:697–705. doi: 10.1007/s00262-022-03272-8
39. Engelhard VH, Obeng RC, Cummings KL, Petroni GR, Ambakhutwala AL, Chianese-Bullock KA, et al. MHC-restricted phosphopeptide antigens: preclinical validation and first-in-humans clinical trial in participants with high-risk melanoma. J Immunother Cancer. (2020) 8:e000262. doi: 10.1136/jitc-2019-000262
40. Wach MM, Subjeck JR, Wang XY, Repasky E, Matsuzaki J, Yu H, et al. Recombinant human Hsp110-gp100 chaperone complex vaccine is nontoxic and induces response in advanced stage melanoma patients. Melanoma Res. (2022) 32:88–97. doi: 10.1097/CMR.0000000000000796
41. Goradel NH, Alizadeh A, Hosseinzadeh S, Taghipour M, Ghesmati Z, Arashkia A, et al. Oncolytic virotherapy as promising immunotherapy against cancer: mechanisms of resistance to oncolytic viruses. Future Oncol. (2022) 18:245–59. doi: 10.2217/fon-2021-0802
42. Andtbacka RHI, Collichio F, Harrington KJ, Middleton MR, Downey G, Őhrling K, et al. Final analyses of OPTiM: a randomized phase III trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in unresectable stage III-IV melanoma. J Immunother Cancer. (2019) 7:145. doi: 10.1186/s40425-019-0623-z
43. Yamazaki N, Isei T, Kiyohara Y, Koga H, Kojima T, Takenouchi T, et al. A phase I study of the safety and efficacy of talimogene laherparepvec in Japanese patients with advanced melanoma. Cancer Sci. (2022) 113:2798–806. doi: 10.1111/cas.15450
44. Franke V, Berger DMS, Klop WMC, van der Hiel B, van de Wiel BA, Ter Meulen S, et al. High response rates for T-VEC in early metastatic melanoma (stage IIIB/C-IVM1a). Int J Cancer. (2019) 145:974–8. doi: 10.1002/ijc.32172
45. Cui C, Wang X, Lian B, Ji Q, Zhou L, Chi Z, et al. OrienX010, an oncolytic virus, in patients with unresectable stage IIIC-IV melanoma: a phase Ib study. J Immunother Cancer. (2022) 10:e004307. doi: 10.1136/jitc-2021-004307
46. Kiyohara E, Tanemura A, Sakura K, Nakajima T, Myoui A, Yamazaki N, et al. A phase I dose-escalation, safety/tolerability, and preliminary efficacy study of the intratumoral administration of GEN0101 in patients with advanced melanoma. Cancer Immunol Immunother. (2022) 71:2041–9. doi: 10.1007/s00262-021-03122-z
47. Andtbacka RHI, Curti B, Daniels GA, Hallmeyer S, Whitman ED, Lutzky J, et al. Clinical responses of oncolytic coxsackievirus A21 (V937) in patients with unresectable melanoma. J Clin Oncol. (2021) 39:3829–38. doi: 10.1200/JCO.20.03246
48. Beasley GM, Nair SK, Farrow NE, Landa K, Selim MA, Wiggs CA, et al. Phase I trial of intratumoral PVSRIPO in patients with unresectable, treatment-refractory melanoma. J Immunother Cancer. (2021) 9:e002203. doi: 10.1136/jitc-2020-002203
49. Raman SS, Hecht JR, Chan E. Talimogene laherparepvec: review of its mechanism of action and clinical efficacy and safety. Immunotherapy. (2019) 11:705–23. doi: 10.2217/imt-2019-0033
50. Ahamadi M, Kast J, Chen PW, Huang X, Dutta S, Upreti VV. Oncolytic viral kinetics mechanistic modeling of Talimogene Laherparepvec (T-VEC) a first-in-class oncolytic viral therapy in patients with advanced melanoma. CPT Pharmacometrics Syst Pharmacol. (2023) 12:250–60. doi: 10.1002/psp4.12898
51. Stahlie EHA, Franke V, Zuur CL, Klop WMC, van der Hiel B, Van de Wiel BA, et al. T-VEC for stage IIIB-IVM1a melanoma achieves high rates of complete and durable responses and is associated with tumor load: a clinical prediction model. Cancer Immunol Immunother. (2021) 70:2291–300. doi: 10.1007/s00262-020-02839-7
52. Kiyohara E, Tanemura A, Nishioka M, Yamada M, Tanaka A, Yokomi A, et al. Intratumoral injection of hemagglutinating virus of Japan-envelope vector yielded an antitumor effect for advanced melanoma: a phase I/IIa clinical study. Cancer Immunol Immunother. (2020) 69:1131–40. doi: 10.1007/s00262-020-02509-8
53. Kirtane K, Elmariah H, Chung CH, Abate-Daga D. Adoptive cellular therapy in solid tumor Malignancies: review of the literature and challenges ahead. J Immunother Cancer. (2021) 9:e002723. doi: 10.1136/jitc-2021-002723
54. Rohaan MW, Borch TH, van den Berg JH, Met Ö, Kessels R, Geukes Foppen MH, et al. Tumor-infiltrating lymphocyte therapy or ipilimumab in advanced melanoma. N Engl J Med. (2022) 387:2113–25. doi: 10.1056/NEJMoa2210233
55. Nguyen LT, Saibil SD, Sotov V, Le MX, Khoja L, Ghazarian D, et al. Phase II clinical trial of adoptive cell therapy for patients with metastatic melanoma with autologous tumor-infiltrating lymphocytes and low-dose interleukin-2. Cancer Immunol Immunother. (2019) 68:773–85. doi: 10.1007/s00262-019-02307-x
56. Hirai I, Funakoshi T, Kamijuku H, Fukuda K, Mori M, Sakurai M, et al. Adoptive cell therapy using tumor-infiltrating lymphocytes for melanoma refractory to immune-checkpoint inhibitors. Cancer Sci. (2021) 112:3163–72. doi: 10.1111/cas.15009
57. Verdegaal E, van der Kooij MK, Visser M, van der Minne C, de Bruin L, Meij P, et al. Low-dose interferon-alpha preconditioning and adoptive cell therapy in patients with metastatic melanoma refractory to standard (immune) therapies: a phase I/II study. J Immunother Cancer. (2020) 8:e000166. doi: 10.1136/jitc-2019-000166
58. Larkin J, Sarnaik A, Chesney JA, Khushalani NI, Kirkwood JM, Weber JS, et al. Lifileucel (LN-144), a cryopreserved autologous tumor infiltrating lymphocyte (TIL) therapy in patients with advanced melanoma: evaluation of impact of prior anti-PD-1 therapy. JCO. (2021) 39:9505–05. doi: 10.1200/JCO.2021.39.15_suppl.9505
59. Mullard A. Tumour-infiltrating lymphocyte cancer therapy nears FDA finish line. Nat Rev Drug Discovery. (2024) 23:3–7. doi: 10.1038/d41573-023-00206-6
60. Dréno B, Khammari A, Fortun A, Vignard V, Saiagh S, Beauvais T, et al. Phase I/II clinical trial of adoptive cell transfer of sorted specific T cells for metastatic melanoma patients. Cancer Immunol Immunother. (2021) 70:3015–30. doi: 10.1007/s00262-021-02961-0
61. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. (2019) 381:1535–46. doi: 10.1056/NEJMoa1910836
62. Wolchok JD, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J Clin Oncol. (2022) 40:127–37. doi: 10.1200/JCO.21.02229
63. van Zeijl MCT, van Breeschoten J, de Wreede LC, Wouters MWJM, Hilarius DL, Blank CU, et al. Real-world outcomes of ipilimumab plus nivolumab combination therapy in a nation-wide cohort of advanced melanoma patients in the Netherlands. J Immunother. (2023) 46:197–204. doi: 10.1097/CJI.0000000000000468
64. Pelster MS, Gruschkus SK, Bassett R, Gombos DS, Shephard M, Posada L, et al. Nivolumab and ipilimumab in metastatic uveal melanoma: results from a single-arm phase II study. J Clin Oncol. (2021) 39:599–607. doi: 10.1200/JCO.20.00605
65. Piulats JM, Espinosa E, de la Cruz Merino L, Varela M, Alonso Carrión L, Martín-Algarra S, et al. Nivolumab plus ipilimumab for treatment-naïve metastatic uveal melanoma: an open-label, multicenter, phase II trial by the spanish multidisciplinary melanoma group (GEM-1402). J Clin Oncol. (2021) 39:586–98. doi: 10.1200/JCO.20.00550
66. Carlino MS, Menzies AM, Atkinson V, Cebon JS, Jameson MB, Fitzharris BM, et al. Long-term follow-up of standard-dose pembrolizumab plus reduced-dose ipilimumab in patients with advanced melanoma: KEYNOTE-029 part 1B. Clin Cancer Res. (2020) 26:5086–91. doi: 10.1158/1078-0432.CCR-20-0177
67. Olson DJ, Eroglu Z, Brockstein B, Poklepovic AS, Bajaj M, Babu S, et al. Pembrolizumab plus ipilimumab following anti-PD-1/L1 failure in melanoma. J Clin Oncol. (2021) 39:2647–55. doi: 10.1200/JCO.21.00079
68. Tawbi HA, SChadendorf D, Lipson EJ, Ascierto PA, Matamala L, Castillo Gutiérrez E, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. (2022) 386:24–34. doi: 10.1056/NEJMoa2109970
69. SChadendorf D, Tawbi H, Lipson EJ, Stephen Hodi F, Rutkowski P, Gogas H, et al. Health-related quality of life with nivolumab plus relatlimab versus nivolumab monotherapy in patients with previously untreated unresectable or metastatic melanoma: RELATIVITY-047 trial. Eur J Cancer. (2023) 87:164–73. doi: 10.1016/j.ejca.2023.03.014
70. Ascierto PA, Lipson EJ, Dummer R, Larkin J, Long GV, Sanborn RE, et al. Nivolumab and Relatlimab in Patients with Advanced Melanoma That Had Progressed on Anti-Programmed Death-1/Programmed Death Ligand 1 Therapy: Results from the Phase I/IIa RELATIVITY-020 Trial. J Clin Oncol. (2023) 41:2724–35. doi: 10.1200/JCO.22.02072
71. Atkinson V, Khattak A, Haydon A, Eastgate M, Roy A, Prithviraj P, et al. Eftilagimod alpha, a soluble lymphocyte activation gene-3 (LAG-3) protein plus pembrolizumab in patients with metastatic melanoma. J Immunother Cancer. (2020) 8:e001681. doi: 10.1136/jitc-2020-001681
72. Aamdal E, Inderberg EM, Ellingsen EB, Rasch W, Brunsvig PF, Aamdal S, et al. Combining a universal telomerase based cancer vaccine with ipilimumab in patients with metastatic melanoma - five-year follow up of a phase I/IIa trial. Front Immunol. (2021) 12:663865. doi: 10.3389/fimmu.2021.663865
73. Ellingsen EB, Bounova G, Kerzeli I, Anzar I, Simnica D, Aamdal E, et al. Characterization of the T cell receptor repertoire and melanoma tumor microenvironment upon combined treatment with ipilimumab and hTERT vaccination. J Transl Med. (2022) 20:419. doi: 10.1186/s12967-022-03624-z
74. Vavolizza RD, Petroni GR, Mauldin IS, Chianese-Bullock KA, Olson WC, Smith KT, et al. Phase I/II clinical trial of a helper peptide vaccine plus PD-1 blockade in PD-1 antibody-naïve and PD-1 antibody-experienced patients with melanoma (MEL64). J Immunother Cancer. (2022) 10:e005424. doi: 10.1136/jitc-2022-005424
75. Slingluff CL, Zarour HM, Tawbi HA, Kirkwood JM, Postow MA, Friedlander P, et al. A phase 1 study of NY-ESO-1 vaccine + anti-CTLA4 antibody Ipilimumab (IPI) in patients with unresectable or metastatic melanoma. Oncoimmunology. (2021) 10:1898105. doi: 10.1080/2162402X.2021.1898105
76. Ott PA, Hu-Lieskovan S, Chmielowski B, Govindan R, Naing A, Bhardwaj N, et al. A phase ib trial of personalized neoantigen therapy plus anti-PD-1 in patients with advanced melanoma, non-small cell lung cancer, or bladder cancer. Cell. (2020) 183:347–362.e24. doi: 10.1016/j.cell.2020.08.053
77. mRNA vaccine slows melanoma recurrence. Cancer Discovery. (2023) 13:1278. doi: 10.1158/2159-8290.CD-NB2023-0028
78. Kristensen NP, Heeke C, Tvingsholm SA, Borch A, Draghi A, Crowther MD, et al. Neoantigen-reactive CD8+ T cells affect clinical outcome of adoptive cell therapy with tumor-infiltrating lymphocytes in melanoma. J Clin Invest. (2022) 132:e150535. doi: 10.1172/JCI150535
79. Hall MS, Mullinax JE, Cox CA, Hall AM, Beatty MS, Blauvelt J, et al. Combination nivolumab, CD137 agonism, and adoptive cell therapy with tumor-infiltrating lymphocytes for patients with metastatic melanoma. Clin Cancer Res. (2022) 28:5317–29. doi: 10.1158/1078-0432.CCR-22-2103
80. Malvehy J, Samoylenko I, SChadendorf D, Gutzmer R, Grob JJ, Sacco JJ, et al. Talimogene laherparepvec upregulates immune-cell populations in non-injected lesions: findings from a phase II, multicenter, open-label study in patients with stage IIIB-IVM1c melanoma. J Immunother Cancer. (2021) 9:e001621. doi: 10.1136/jitc-2020-001621
81. Chesney JA, Puzanov I, Collichio FA, Singh P, Milhem MM, Glaspy J, et al. Talimogene laherparepvec in combination with ipilimumab versus ipilimumab alone for advanced melanoma: 5-year final analysis of a multicenter, randomized, open-label, phase II trial. J Immunother Cancer. (2023) 11:e006270. doi: 10.1136/jitc-2022-006270
82. Chesney JA, Ribas A, Long GV, Kirkwood JM, Dummer R, Puzanov I, et al. Randomized, double-blind, placebo-controlled, global phase III trial of talimogene laherparepvec combined with pembrolizumab for advanced melanoma. J Clin Oncol. (2023) 41:528–40. doi: 10.1200/JCO.22.00343
83. Silk AW, O'Day SJ, Kaufman HL, Bryan J, Norrell JT, Imbergamo C, et al. A phase 1b single-arm trial of intratumoral oncolytic virus V937 in combination with pembrolizumab in patients with advanced melanoma: results from the CAPRA study. Cancer Immunol Immunother. (2023) 72:1405–15. doi: 10.1007/s00262-022-03314-1
84. Curti BD, Richards J, Hyngstrom JR, Daniels GA, Faries M, Feun L, et al. Intratumoral oncolytic virus V937 plus ipilimumab in patients with advanced melanoma: the phase 1b MITCI study. J Immunother Cancer. (2022) 10:e005224. doi: 10.1136/jitc-2022-005224
85. Rudin CM, Pandha HS, Zibelman M, Akerley WL, Harrington KJ, Day D, et al. Phase 1, open-label, dose-escalation study on the safety, pharmacokinetics, and preliminary efficacy of intravenous Coxsackievirus A21 (V937), with or without pembrolizumab, in patients with advanced solid tumors. J Immunother Cancer. (2023) 11:e005007. doi: 10.1136/jitc-2022-005007
86. Lutzky J, Sullivan RJ, Cohen JV, Ren Y, Li A, Haq R. Phase 1b study of intravenous coxsackievirus A21 (V937) and ipilimumab for patients with metastatic uveal melanoma. J Cancer Res Clin Oncol. (2023) 149:6059–66. doi: 10.1007/s00432-022-04510-3
87. Lövgren T, Wolodarski M, Wickström S, Edbäck U, Wallin M, Martell E, et al. Complete and long-lasting clinical responses in immune checkpoint inhibitor-resistant, metastasized melanoma treated with adoptive T cell transfer combined with DC vaccination. Oncoimmunology. (2020) 9:1792058. doi: 10.1080/2162402X.2020.1792058
88. Saberian C, Amaria RN, Najjar AM, Radvanyi LG, Haymaker CL, Forget MA, et al. Randomized phase II trial of lymphodepletion plus adoptive cell transfer of tumor-infiltrating lymphocytes, with or without dendritic cell vaccination, in patients with metastatic melanoma. J Immunother Cancer. (2021) 9:e002449. doi: 10.1136/jitc-2021-002449
89. Schwarze JK, Tijtgat J, Awada G, Cras L, Vasaturo A, Bagnall C, et al. Intratumoral administration of CD1c (BDCA-1) + and CD141 (BDCA-3) + myeloid dendritic cells in combination with talimogene laherparepvec in immune checkpoint blockade refractory advanced melanoma patients: a phase I clinical trial. J Immunother Cancer. (2022) 10:e005141. doi: 10.1136/jitc-2022-005141
90. Vaes RDW, Hendriks LEL, Vooijs M, De Ruysscher D. Biomarkers of radiotherapy-induced immunogenic cell death. Cells. (2021) 10:930. doi: 10.3390/cells10040930
91. Patel RR, He K, Barsoumian HB, Chang JY, Tang C, Verma V, et al. High-dose irradiation in combination with non-ablative low-dose radiation to treat metastatic disease after progression on immunotherapy: Results of a phase II trial. Radiother Oncol. (2021) 162:60–7. doi: 10.1016/j.radonc.2021.06.037
92. Newton JM, Hanoteau A, Liu HC, Gaspero A, Parikh F, Gartrell-Corrado RD, et al. Immune microenvironment modulation unmasks therapeutic benefit of radiotherapy and checkpoint inhibition. J Immunother Cancer. (2019) 7:216. doi: 10.1186/s40425-019-0698-6
93. Craig DJ, Nanavaty NS, Devanaboyina M, Stanbery L, Hamouda D, Edelman G, et al. The abscopal effect of radiation therapy. Future Oncol. (2021) 17:1683–94. doi: 10.2217/fon-2020-0994
94. Maity A, Mick R, Rengan R, Mitchell TC, Amaravadi RK, Schuchter LM, et al. A stratified phase I dose escalation trial of hypofractionated radiotherapy followed by ipilimumab in metastatic melanoma: long-term follow-up and final outcomes. Oncoimmunology. (2021) 10:1863631. doi: 10.1080/2162402X.2020.1863631
95. Boutros C, Chaput-Gras N, Lanoy E, Larive A, Mateus C, Routier E, et al. Dose escalation phase 1 study of radiotherapy in combination with anti-cytotoxic-T-lymphocyte-associated antigen 4 monoclonal antibody ipilimumab in patients with metastatic melanoma. J Immunother Cancer. (2020) 8:e000627. doi: 10.1136/jitc-2020-000627
96. Sundahl N, Seremet T, Van Dorpe J, Neyns B, Ferdinande L, Meireson A, et al. Phase 2 trial of nivolumab combined with stereotactic body radiation therapy in patients with metastatic or locally advanced inoperable melanoma. Int J Radiat Oncol Biol Phys. (2019) 104:828–35. doi: 10.1016/j.ijrobp.2019.03.041
97. Curti B, Crittenden M, Seung SK, Fountain CB, Payne R, Chang S, et al. Randomized phase II study of stereotactic body radiotherapy and interleukin-2 versus interleukin-2 in patients with metastatic melanoma. J Immunother Cancer. (2020) 8:e000773. doi: 10.1136/jitc-2020-000773
98. Minor DR, Kim KB, Tong RT, Wu MC, Kashani-Sabet M, Orloff M, et al. A pilot study of hepatic irradiation with yttrium-90 microspheres followed by immunotherapy with ipilimumab and nivolumab for metastatic uveal melanoma. Cancer Biother Radiopharm. (2022) 37:11–6. doi: 10.1089/cbr.2021.0366
99. Cavalieri S, Vitolo V, Barcellini A, Ronchi S, Facoetti A, Campo C, et al. Immune checkpoint inhibitors and Carbon iON radiotherapy In solid Cancers with stable disease (ICONIC). Future Onco. (2023) 19:193–203. doi: 10.2217/fon-2022-0503
100. Ratnayake G, Reinwald S, Edwards J, Wong N, Yu D, Ward R, et al. Blood T-cell profiling in metastatic melanoma patients as a marker for response to immune checkpoint inhibitors combined with radiotherapy. Radiother Oncol. (2022) 173:299–305. doi: 10.1016/j.radonc.2022.06.016
101. Bulgarelli J, Piccinini C, Petracci E, Pancisi E, Granato AM, de Rosa F, et al. Radiotherapy and high-dose interleukin-2: clinical and immunological results of a proof of principle study in metastatic melanoma and renal cell carcinoma. Front Immunol. (2021) 12:778459. doi: 10.3389/fimmu.2021.778459
Keywords: melanoma, immune checkpoint inhibitors, radiotherapy, combination therapy, oncolytic virus
Citation: Xu J, Mu S, Wang Y, Yu S and Wang Z (2024) Recent advances in immunotherapy and its combination therapies for advanced melanoma: a review. Front. Oncol. 14:1400193. doi: 10.3389/fonc.2024.1400193
Received: 13 March 2024; Accepted: 01 July 2024;
Published: 16 July 2024.
Edited by:
Selma Ugurel, Essen University Hospital, GermanyReviewed by:
Yoshiaki Yura, Osaka University, JapanCopyright © 2024 Xu, Mu, Wang, Yu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhongming Wang, d3ptMTI5MUAxMzkuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.