 Jessica Prunaretty*
Jessica Prunaretty* Laura Lopez†Morgane Cabaillé†
Laura Lopez†Morgane Cabaillé† Céline BourgierAurélie Morel
Céline BourgierAurélie Morel David AzriaPascal Fenoglietto
David AzriaPascal Fenoglietto- Radiotherapy Department, Montpellier Regional Cancer Institute, Montpellier, France
Purpose: To evaluate the feasibility to use a standard Ethos planning template to treat left-sided breast cancer with regional lymph nodes.
Material/Methods: The tuning cohort of 5 patients was used to create a planning template. The validation cohort included 15 patients treated for a locally advanced left breast cancer randomly enrolled. The Ethos planning template was tuned using standard 3 partial arc VMAT and two collimator rotation configurations: 45/285/345° and 30/60/330°. Re-planning was performed automatically using the template without editing. The study was conducted with a schedule of 42.3 Gy in 18 fractions to the breast/chestwall, internal mammary chain (IMC) and regional lymph nodes (“Nodes”). The PTV was defined as a 3D extension of the CTV with a margin of 7 mm, excluding the 5mm below the skin. The manual treatment plans were performed using Eclipse treatment planning system with AAA and PO algorithms (v15.6) and a manual arc VMAT configuration and imported in Ethos TPS (v1.1) for a dose calculation with Ethos Acuros algorithm. The automated plans were compared with the manual plans using PTV and CTV coverage, homogeneity and conformity indices (HI and CN) and doses to organs at risk (OAR) via DVH metrics. For each plan, the patient quality assurance (QA) were performed using Mobius3D and gamma index. Finally, two breast radiation oncologists performed a blinded assessment of the clinical acceptability of each of the three plans (manual and automated) for each patient.
Results: The manual and automated plans provided suitable treatment planning as regards dose constraints. The dosimetric comparison showed the CTV_breast D99% were significantly improved with both automated plans (p< 0,002) while PTV coverage was comparable. The doses to the organs at risk were equivalent for the three plans. Concerning treatment delivery, the Ethos-45° and Ethos-30° plans led to an increase in MUs compared to the manual plans, without affecting the beam on time. The average gamma index pass rates remained consistently above 98% regardless of the type of plan utilized. In the blinded evaluation, clinicians 1 and 2 assessed 13 out of 15 plans for Ethos 45° and 11 out of 15 plans for Ethos 30° as clinically acceptable.
Conclusion: Using a standard planning template for locally advanced breast cancer, the Ethos TPS provided automated plans that were clinically acceptable and comparable in quality to manually generated plans. Automated plans also dramatically reduce workflow and operator variability.
1 Introduction
Breast-conserving surgery followed by whole breast irradiation (WBI) is the current standard of care for patients with early stage breast cancer (BC) (1). Although the American Society for Radiation Oncology (ASTRO) does not recommend intensity modulated radiation therapy (IMRT) for the routine delivery of WBI after breast-conserving surgery, some studies have shown that the use of IMRT is increasing worldwide (2, 3). In recent decades, IMRT has played a crucial role in improving plan quality. However, it has also introduced complexity into the treatment planning process leading to an inter-operator variability (4, 5) and an increased planning time.
The strategy of planning automation has shown promising results in standardizing treatment planning while maintaining plan quality and reducing workload (6, 7). Three methods are currently commercially available. First, knowledge-based planning (KBP) relies on knowledge from previous cases to predict an achievable dose in a new case of a similar population (8, 9). Apaza Blanco et al. (10) evaluated two knowledge-based VMAT models for breast cancer using the C-arm accelerator and demonstrated a plan quality equivalent to the planner’s experience. Esposito et al. (11) published similar results using Tomotherapy. The multicriteria optimization (MCO) is based on pareto-optimal plan proposals where one criterion cannot be improved without worsening at least one other criterion (12, 13). Finally, the template-based planning uses an iterative approach of progressive optimization that mimics the planning process by a skilled planner. This method requires the creation of a wish‐list including beam setup, dose prescriptions and planning objectives for each treatment site‐specific clinical data. The Ethos Treatment Planning System (TPS) uses the latter strategy. Ethos® Therapy, marketed by Varian Medical System, includes a Halcyon® linac upgraded with fully integrated and automated online ART using CBCT images and artificial intelligence (14). The Ethos TPS uses an Intelligent Optimization Engine (IOE) that automatically drives the Photon Optimizer algorithm. The IOE is designed to perform all the necessary steps to produce high quality dose distributions that match the clinical expectations for the plan, to ensure dosimetric accuracy. The performance of the IOE has been evaluated for pelvis (15–18), head and neck (19, 20), partial breast (21), and lung (22). However, to our knowledge, it has not yet been evaluated for breast cancer including regional lymph nodes. The aim of this study was to evaluate the quality of whole breast treatment plans automatically generated by the Ethos IOE using a planning directive template. The automatically generated plans will be compared to manual plans using dose metrics. A blinded assessment will be performed for a clinical approval.
2 Materials and methods
2.1 Patient description
Patients underwent a 2.5 mm slice thickness computed tomography (CT) scan (GE Optima CT580, General Electric Healthcare, Waukesha, WI, USA) in the supine position with free breathing, and with both arms above the head with personalized foam cushions.
The ESTRO consensus guidelines (23, 24) were used to delineate the target volumes, breast/wall, and axillary (Berg I), subclavicular (Berg II, III) and supraclavicular (Berg IV) lymph nodes (hereafter Nodes); and the internal mammary chain (IMC). The PTV was defined as a 3D extension of the CTV with a margin of 7 mm. All PTVs and CTVs were limited to 5 mm under the skin. Organs at risk were delineated according to the French RecoRad recommendations (25) using TheraPanacea software (26) and AW Server (General Electric). PTV volumes are listed in Table 1 and two examples of patient CT images are shown in Figure 1.
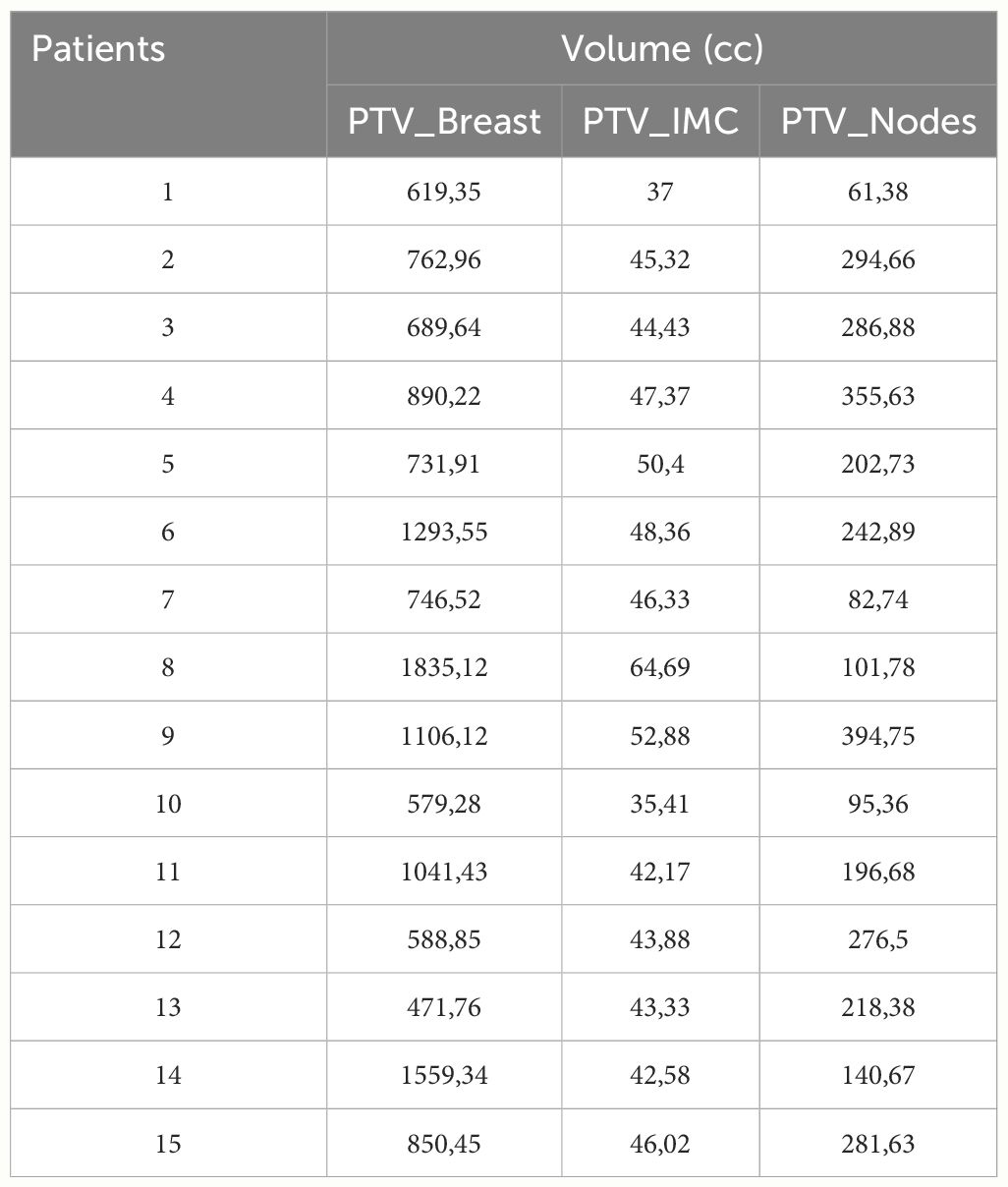
Table 1 Volume descriptions of PTV breast, PTV_IMC and PTV_Nodes.
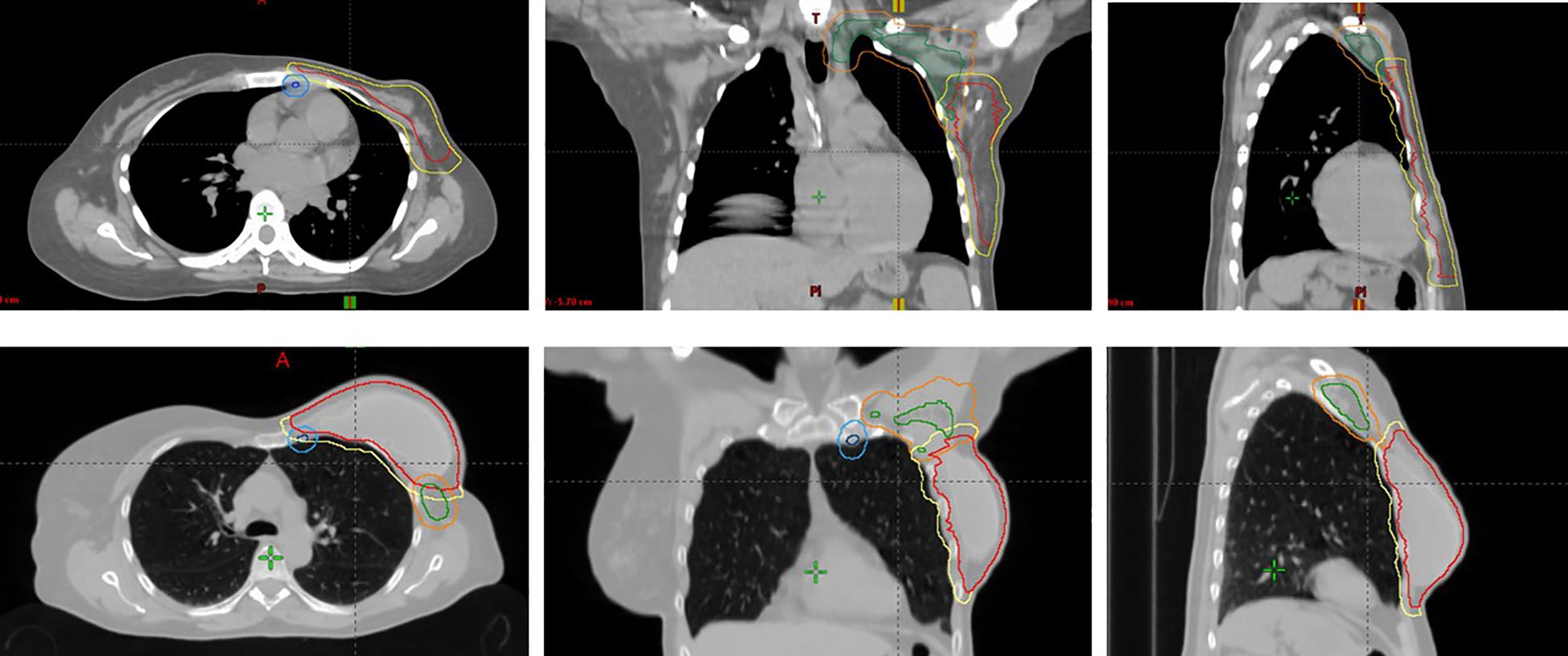
Figure 1 Two examples of patient CT images in axial (left), coronal (center), and sagittal (right) views showing PTV breast/chestwall (yellow), PTV_IMC (light blue), PTV_nodes (orange), CTV breast/chestwall (red), CTV_IMC (dark blue) and CTV_nodes (green).
2.2 Departmental treatment planning workflow
The Ethos treatment planning system (TPS) offers a choice of 5 fixed beam configurations: 7–9-12 IMRT fields and 2–3 full-arc VMAT (14). However, these configurations are not adapted for breast irradiation with regional nodes where partial-arc VMAT is preferred (27, 28). Therefore, a beam geometry using the Eclipse TPS is required. The current departmental workflow consists of a manual planning with the Eclipse treatment planning system (Varian, Medical Systems, Palo Alto, CA, USA) using the Photon Optimizer and AAA algorithms (PO, AAA, v15.6, Varian, Medical Systems, Palo Alto, CA, USA). Once the treatment plan is clinically acceptable on the Eclipse TPS, it is then imported into the Ethos TPS (v1.1) and calculated with the Ethos Acuros algorithm for clinical approval. Renormalization of the plan was necessary to compensate for the dose differences between the two algorithms (29, 30). The departmental workflow is detailed in Figure 2.
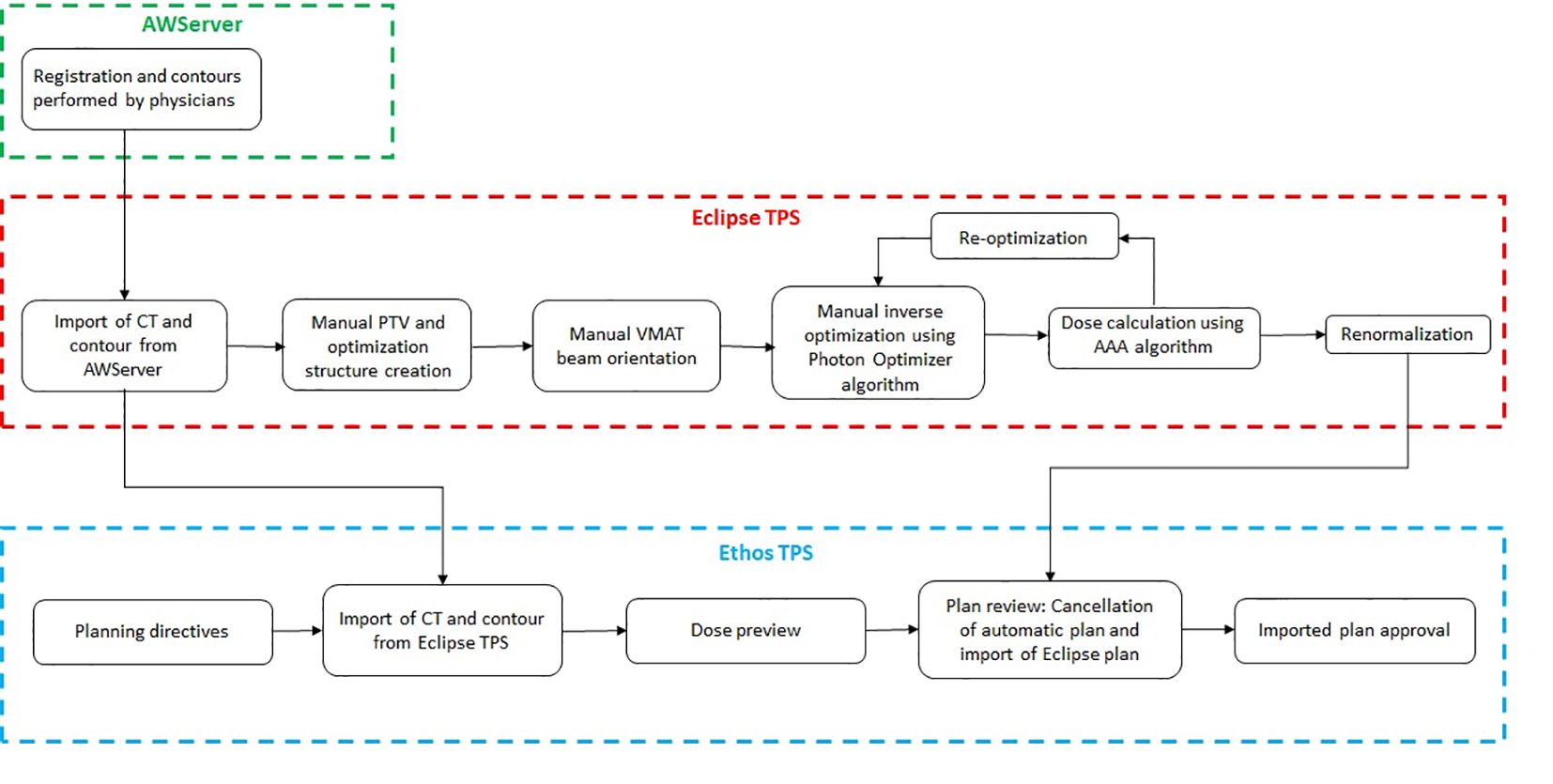
Figure 2 Departmental workflow for the Ethos breast treatment planning.
2.3 Manual treatment planning
The study was conducted with a schedule of 42.3 Gy in 18 fractions to the breast/chestwall, internal mammary chain (IMC) and regional lymph nodes (“Nodes”) according to the HYPOG-01 clinical trial (6). The dose constraints for CTVs and organs at risk (OAR) are shown in Table 2. No PTV dose constraints are defined in this protocol. Patients were treated with the Ethos linear accelerator using Volumetric Modulated Arctherapy (VMAT) technique. The arc amplitude was 240° (from 179° to 300°, and vice versa). Treatment descriptions are detailed in Table 3. The number of arcs and collimator angles are defined according to the operator and the anatomical complexity of the patient. The manual plans will be referred to as “Eclipse” throughout the rest of the study.
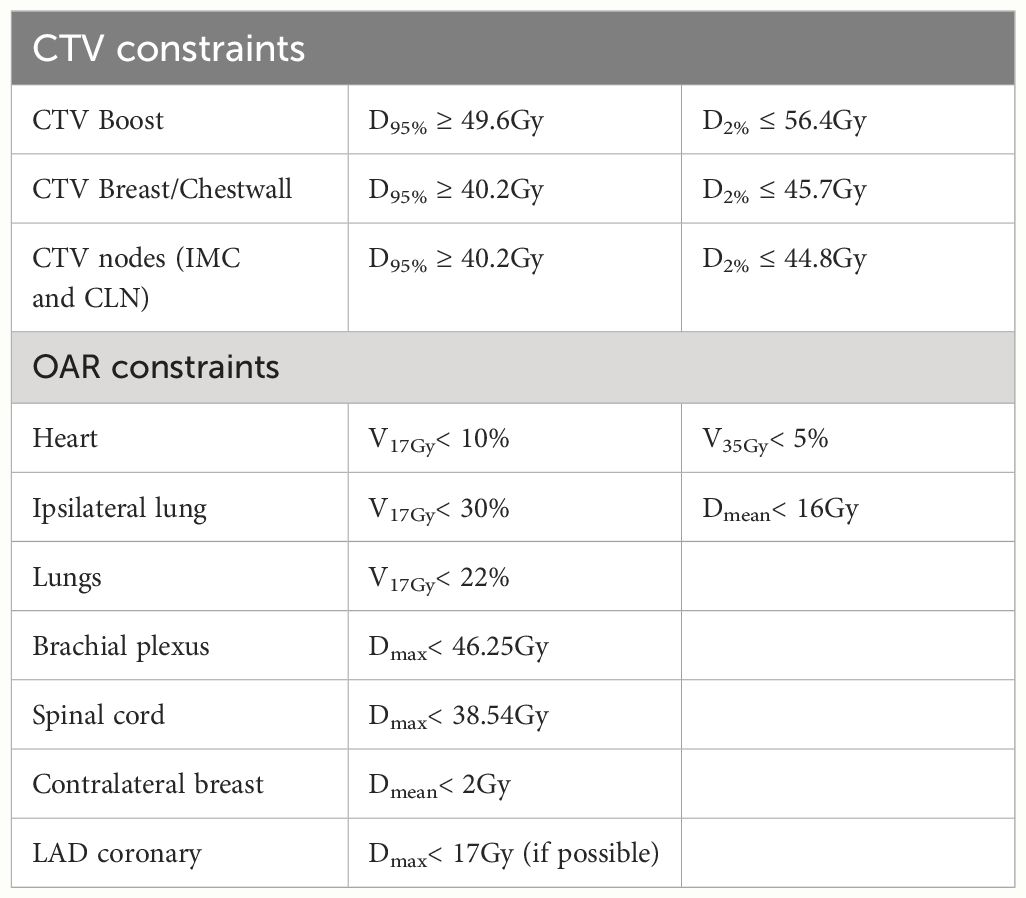
Table 2 Dose constraints for CTVs and organs at risk.
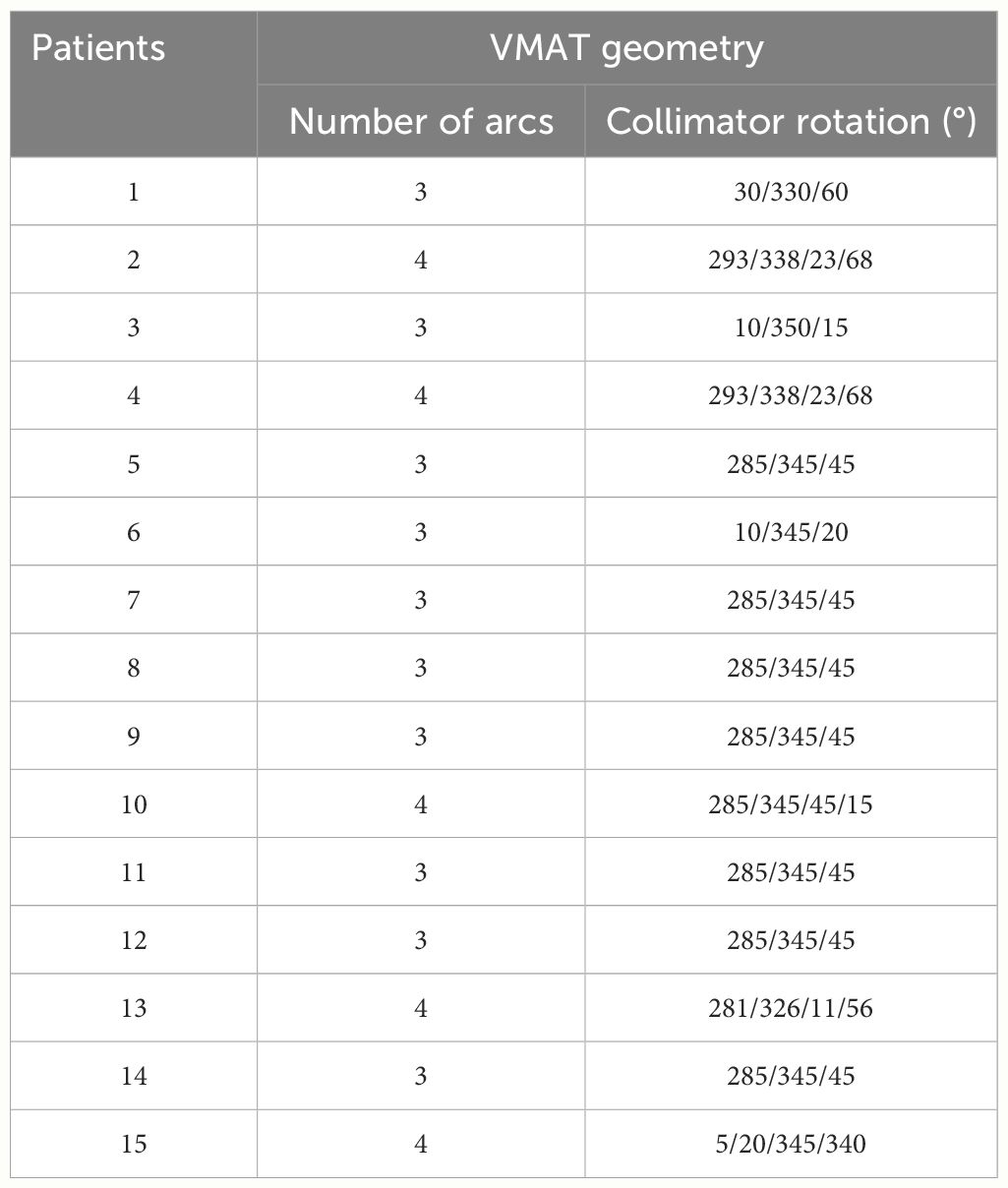
Table 3 Treatment description including VMAT geometry for each patient.
2.4 Automated treatment planning
An Ethos optimization template was tuned using standard 3 partial arc volumetric modulated arc therapy and two collimator rotation configurations: 45/285/345° (referred to as Ethos-45°) and 30/60/330° (referred to as Ethos-30°). The collimator rotation configurations were selected based on the clinical practice. Five patients previously treated with Ethos were randomly selected for the tuning cohort. The tuning cohort was used to create a template for planning guidelines. Clinical experience from the other centers (19, 21) and iterative planning were adapted to achieve a standard template and ensure dosimetric accuracy. Finally, fifteen patients were automatically replanned using the template without editing.
2.5 Plan comparison
All the treatment plans were transferred to Eclipse TPS for the purpose of conducting a side-by-side comparison. Dose metrics were compared between the three plans using some dose constraints provided by the HYPOG-01 protocol and some additional relevant parameters. Target volume coverage was assessed using more demanding parameters than those used in the clinical protocol according to our clinical practice, i.e the doses received at 99% and 95% of the volume (D99% D95%) for the CTVs and PTVs (breast, IMC and nodes), respectively. For the ipsilateral lung, the mean dose (Dmean) and the volume receiving 17Gy (V17Gy) were calculated. Mean doses to the heart, the contralateral lung and the right breast and maximum doses (Dmax) to the brachial plexus and LAD coronary arteries were also recorded. The homogeneity index within the whole PTV is defined by the following formula (31):
The dose conformity was evaluated using the conformity index (CI) defined as (32):
Where V95%(PTV) and V95(Body) are the volumes receiving at least 95% of the prescribed dose for the whole PTV (breast, IMC and Nodes) and body, respectively. VPTV is the volume of the whole PTV. The total number of monitor units (MU) was reported for each plan. Finally, the optimization and calculation times for Ethos plans were extracted from the treatment report. Due to the retrospective nature of the study, we were unable to collect these values for Eclipse plans.
2.6 Quality assurance
Ethos includes Mobius3D (version 3.1, Varian Medical System), an integrated and independent quality assurance (QA) tool for dose calculation using an independent collapsed cone convolution algorithm. Pre-treatment QA was performed for each plan. The assessment metric was the global gamma pass rate with a 3%/3mm criterion and a 10% threshold. In addition, the beam-on time was estimated for each plan using Mobius3D.
2.7 Physician review
Two radiation oncologists specializing in breast cases thoroughly reviewed the Ethos and Eclipse plans. They performed a blinded assessment of the clinical acceptability of each of the two automated plans for each patient. During plan review, the physicians made binary decisions regarding the clinical acceptability of the plan. The Ethos optimization template was not shown to the clinicians prior to the assessment to avoid decision bias. The clinicians then blindly selected the best plan from the three proposed plans (Eclipse, Ethos-45°, Ethos-30°).
2.8 Statistical analyses
The Wilcoxon signed rank test was used to determine the significant difference between the Eclipse and Ethos plan metrics. A Bonferroni correction was applied and the significance level was set at 0.003.
3 Results
This study evaluated the viability of employing an Ethos standard planning template for treating left-sided breast cancer involving regional lymph nodes. Table 4 provides a summary of the structures and objectives utilized, along with their corresponding priorities for the standard template. The primary objective was to control the hotspot, set at 107% of the prescribed dose. Subsequently, the template emphasized avoidance of the ipsilateral lung, coverage of the clinical target volume (CTV), protection of the heart, and coverage of the planning target volume (PTV). Lower priority was assigned to contralateral organs, with no specific avoidance strategy implemented.
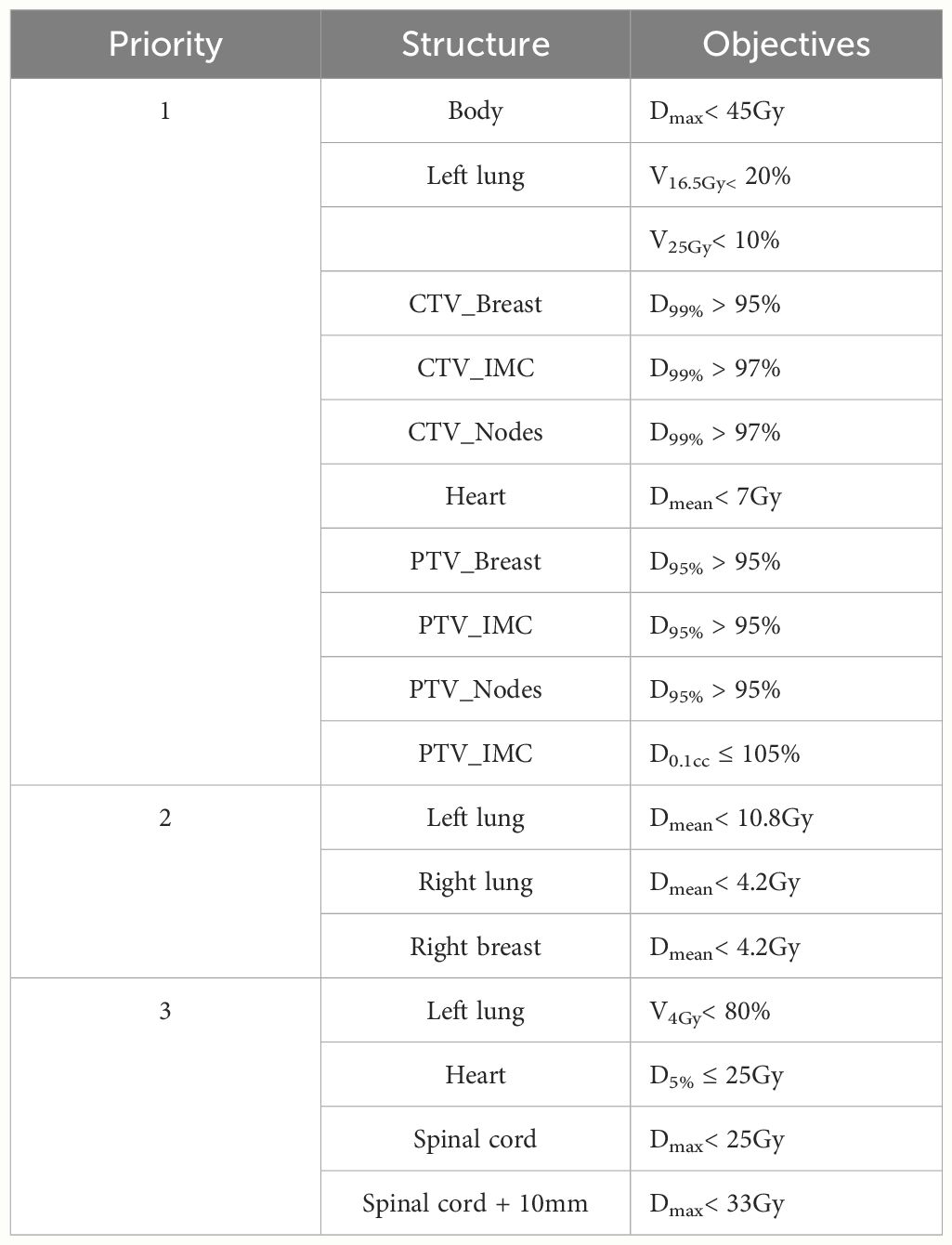
Table 4 Summary of the objectives used in the standard template.
The manual and automated plans provided suitable treatment planning in terms of HYPOG-01 dose constraints (Figure 3 and Table 5). PTV coverage was similar between the Eclipse (manual) and both Ethos (automated) plans. The conformity and homogeneity indices were not statistically different between the three plans. Only the CTV_breast coverage were significantly improved with both Ethos plans (p< 0,002). The mean dose to the organs at risk was equivalent between the three plans. However, the dose distributions were different. For protection of the heart and both lungs, ΔDVH showed that the Eclipse plans delivered fewer low doses than the Ethos plans while the Ethos plan provided better protection at intermediate and high doses (Figure 2). For the contralateral breast, however, the trend was reversed.
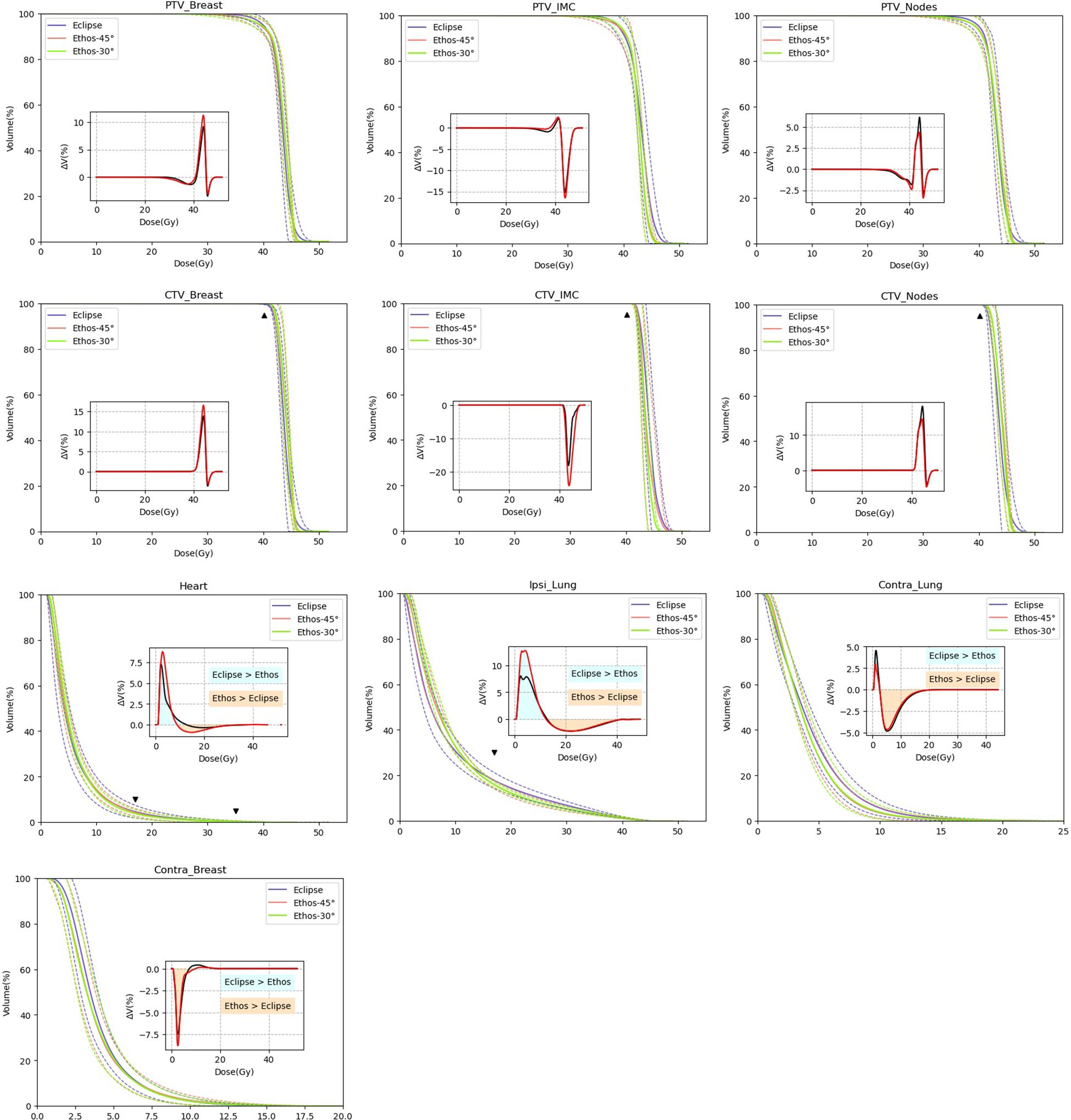
Figure 3 Comparison of mean DVH (solid line) of Eclipse (blue) and Ethos automatic plan (red and green for Ethos-45° and Ethos-30°, respectively). Dashed lines show the standard deviation. The triangle figures show the HYPOG constraints. Insets show the mean of DVH difference between Ethos-45° minus Eclipse (black) and Ethos-30° minus Eclipse (red).

Table 5 Dose metric results (mean ± standard deviation) for PTVs and organs at risk (OAR) for Eclipse, Ethos-45° and Ethos-30° treatment plans.
Regarding the treatment delivery, the Ethos-45° and Ethos-30° plans resulted in MU increases of 15.5 and 17.3%, respectively, compared to the Eclipse plans, with no impact on the beam on time (Table 6). Pre-treatment verification with mobius3D showed that mean gamma index pass rates remained above 98% regardless of the plans used. Ethos plan generation (including optimization and dose calculation) was in the range of 14 to 15 minutes.

Table 6 Mean [Min-Max] of total MUs, gamma passing rates, plan generation time and beam on time for Eclipse, Ethos-45° and Ethos-30° treatment plans.
In the blinded assessment, both clinicians 1 and 2 found 13/15 and 11/15 of the plans clinically acceptable for Ethos 45° and Ethos 30°, respectively. Furthermore, if an Ethos plan was not clinically acceptable, the second Ethos geometry was acceptable. Finally, Figure 4 shows the physician’s choice of treatment plan in the blinded comparison between manual (Eclipse) and automatic (Ethos-45° and Ethos-30°) plans. Physician 1 selected 86.7% of the Ethos plans (Ethos-45° and Ethos-30°combined) while the physician 2 selected 80% of the Ethos plans.
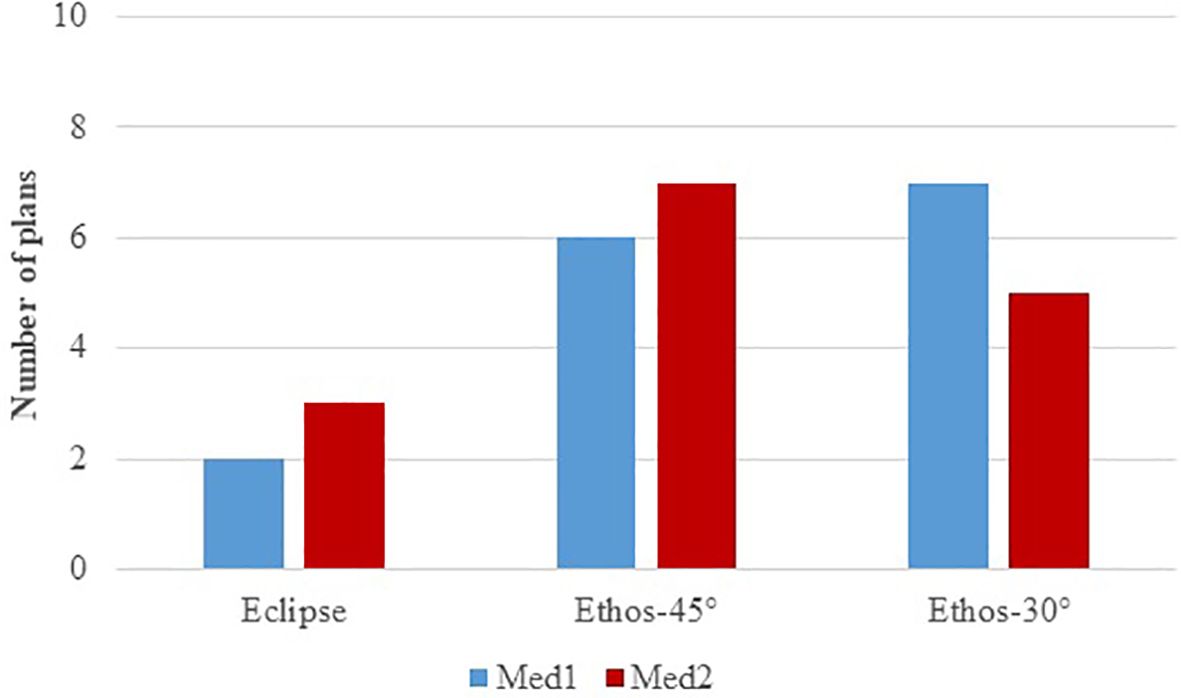
Figure 4 Physicians’ choice of treatment plan during the blinded comparison between manual (Eclipse) and automatic (Ethos-45° and Ethos-30°) plans.
4 Discussion
This study presents the first investigation of Ethos treatment planning for left-sided locally advanced breast cancer. We conduct a comprehensive assessment, both quantitative and qualitative, of treatment plans generated automatically.
The automated plans provided an adequate treatment plan with respect to the HYPOG-01 dose constraints, and the quality of the plans was similar to the manual plans. These results are consistent with the literature for other disease sites (16, 21, 22). Furthermore, a difference in dose distribution between low and high dose was observed between manual and automated treatment plans. Pogue et al. (22) developed an Ethos treatment plan template for locally advanced lung cancer and reported similar results for the organs at risk. In their study, they compared the initial treatment plan using C-arm accelerators with the Ethos treatment plans. Due to the different multi-leaf collimator (MLC) design between the accelerators, they could not determine how much of the difference in the Ethos plan was due to the Ethos double-banked MLC and how much was due to the IOE. In contrast, our study was performed with the Ethos accelerator only. Therefore, the dosimetric differences observed cannot be attributed to the MLC.
In addition, blinded physician review showed that at least 73% of the automated plans were clinically acceptable without edits, demonstrating the robustness of the standard template.
In terms of planning and treatment efficiency, automated treatment planning resulted in an increase in MUs, consistent with findings from another automated planning engine (16, 20). This suggests an increase in plan complexity, but without any impact on the quality assurance.
In addition to the high plan quality achieved with the automated treatment plan, the interest of this work was to reduce the workload caused by switching back and forth between two TPSs. Although the time savings have not been fully quantified, it is reasonable to assume that plan preparation time will be reduced. In our clinical experience, the time required for a planner to manually generate a clinically acceptable breast VMAT plan ranged from 60 to 180 minutes, depending on anatomical complexity. The two Ethos plans optimized for each patient took 30 minutes without intervention. Note that the time required to select the planning directive and planning image, and then manually associate the structure set, remains unchanged between the two workflows.
There was no significant difference in dose metrics between the two collimator rotation configurations for the automated plans. However, in some cases where an Ethos plan was clinically unacceptable in the blinded assessment, the second Ethos geometry was acceptable. The interest of the two geometries is to propose two different plans without editing the planning template.
Finally, we have chosen to maintain this VMAT geometry despite several studies reporting that the Ethos optimization time is significantly longer with VMAT than with IMRT (16, 17). The two main reasons for this are our extensive experience with breast VMAT (33–36) and the fact that all our patients are treated with Ethos in the IGRT mode for breast cancer: the planning time is affected but not the length of the session. In the context of an adaptive session with a daily re-optimization, an IMRT beam geometry should be considered in order not to increase session times (37). In addition, only a single isocenter was examined in this study. Due to the limited maximum field size of the Ethos (28 x 28 cm²), the larger whole breast with regional nodes could not be covered by a mono-isocenter technique. In this case, the standard planning template with a specific multi-isocenter technique should be investigated.
Future research will encompass the clinical integration and prospective application of this standard template. Moreover, the methodology outlined in this study will be employed for other treatment protocols (such as simultaneous integrated boost for breast cancer) and extended to other disease sites.
5 Conclusion
This study demonstrated the feasibility of the Ethos Intelligent Optimization Engine to generate high quality automated plans using a standard planning template for left-sided locally advanced breast cancer. Planning automation reduces the need for human intervention, thereby reducing both the workload and operator variability.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
JP: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft. LL: Investigation, Writing – review & editing. MC: Investigation, Writing – review & editing. CB: Writing – review & editing. AM: Writing – review & editing. DA: Writing – review & editing. PF: Conceptualization, Methodology, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Maughan KL, Lutterbie MA, Ham PS. Treatment of breast cancer. Am Fam Physician. (2010) 81:1339–46.
2. Huh SJ, Park W, Choi DH. Recent trends in intensity-modulated radiation therapy use in Korea. Radiat Oncol J. (2019) 37:249–53. doi: 10.3857/roj.2019.00577
3. Chang JS, Chang JH, Kim N, Kim YB, Shin KH, Kim K. Intensity modulated radiotherapy and volumetric modulated arc therapy in the treatment of breast cancer: an updated review. J Breast Cancer. (2022) 25:349–65. doi: 10.4048/jbc.2022.25.e37
4. Peters LJ, O’Sullivan B, Giralt J, Fitzgerald TJ, Trotti A, Bernier J, et al. Critical impact of radiotherapy protocol compliance and quality in the treatment of advanced head and neck cancer: results from TROG 02.02. J Clin Oncol Off J Am Soc Clin Oncol. (2010) 28:2996–3001. doi: 10.1200/JCO.2009.27.4498
5. Nelms BE, Robinson G, Markham J, Velasco K, Boyd S, Narayan S, et al. Variation in external beam treatment plan quality: An inter-institutional study of planners and planning systems. Pract Radiat Oncol. (2012) 2:296–305. doi: 10.1016/j.prro.2011.11.012
6. Hussein M, Heijmen BJM, Verellen D, Nisbet A. Automation in intensity modulated radiotherapy treatment planning-a review of recent innovations. Br J Radiol. (2018) 91:20180270. doi: 10.1259/bjr.20180270
7. Nguyen D, Lin MH, Sher D, Lu W, Jia X, Jiang S. Advances in automated treatment planning. Semin Radiat Oncol. (2022) 32:343–50. doi: 10.1016/j.semradonc.2022.06.004
8. Ge Y, Wu QJ. Knowledge-based planning for intensity-modulated radiation therapy: A review of data-driven approaches. Med Phys. (2019) 46:2760–75. doi: 10.1002/mp.13526
9. Momin S, Fu Y, Lei Y, Roper J, Bradley JD, Curran WJ, et al. Knowledge-based radiation treatment planning: A data-driven method survey. J Appl Clin Med Phys. (2021) 22:16–44. doi: 10.1002/acm2.13337
10. Apaza Blanco OA, Almada MJ, Garcia Andino AA, Zunino S, Venencia D. Knowledge-based volumetric modulated arc therapy treatment planning for breast cancer. J Med Phys. (2021) 46:334–40. doi: 10.4103/jmp.JMP_51_21
11. Esposito PG, Castriconi R, Mangili P, Broggi S, Fodor A, Pasetti M, et al. Knowledge-based automatic plan optimization for left-sided whole breast tomotherapy. Phys Imaging Radiat Oncol. (2022) 23:54–9. doi: 10.1016/j.phro.2022.06.009
12. Thieke C, Küfer KH, Monz M, Scherrer A, Alonso F, Oelfke U, et al. A new concept for interactive radiotherapy planning with multicriteria optimization: first clinical evaluation. Radiother Oncol J Eur Soc Ther Radiol Oncol. (2007) 85:292–8. doi: 10.1016/j.radonc.2007.06.020
13. Schreibmann E, Lahanas M, Xing L, Baltas D. Multiobjective evolutionary optimization of the number of beams, their orientations and weights for intensity-modulated radiation therapy. Phys Med Biol. (2004) 49:747–70. doi: 10.1088/0031-9155/49/5/007
14. Archambault Y, Boylan C, Bullock D, Morgas T, Peltola J, Ruokokoski E, et al. Making on-line adaptive radiotherapy possible using artificial intelligence and machine learning for efficient daily re-planning. Med Phys Intl J. (2020).
15. Roberfroid B, Barragán-Montero AM, Dechambre D, Sterpin E, Lee JA, Geets X. Comparison of Ethos template-based planning and AI-based dose prediction: General performance, patient optimality, and limitations. Phys Med PM Int J Devoted Appl Phys Med Biol Off J Ital Assoc BioMed Phys AIFB. (2023) 116:103178. doi: 10.1016/j.ejmp.2023.103178
16. Calmels L, Sibolt P, Åström LM, Serup-Hansen E, Lindberg H, Fromm AL, et al. Evaluation of an automated template-based treatment planning system for radiotherapy of anal, rectal and prostate cancer. Tech Innov Patient Support Radiat Oncol. (2022) 22:30–6. doi: 10.1016/j.tipsro.2022.04.001
17. Pokharel S, Pacheco A, Tanner S. Assessment of efficacy in automated plan generation for Varian Ethos intelligent optimization engine. J Appl Clin Med Phys. (2022) 23:e13539. doi: 10.1002/acm2.13539
18. Sibolt P, Andersson LM, Calmels L, Sjöström D, Bjelkengren U, Geertsen P, et al. Clinical implementation of artificial intelligence-driven cone-beam computed tomography-guided online adaptive radiotherapy in the pelvic region. Phys Imaging Radiat Oncol. (2021) 17:1–7. doi: 10.1016/j.phro.2020.12.004
19. Visak J, Inam E, Meng B, Wang S, Parsons D, Nyugen D, et al. Evaluating machine learning enhanced intelligent-optimization-engine (IOE) performance for ethos head-and-neck (HN) plan generation. J Appl Clin Med Phys. (2023) 24:e13950. doi: 10.1002/acm2.13950
20. El-Qmache A, McLellan J. Investigating the feasibility of using Ethos generated treatment plans for head and neck cancer patients. Tech Innov Patient Support Radiat Oncol. (2023), 27:100216. doi: 10.1016/j.tipsro.2023.100216
21. Pogue JA, Cardenas CE, Cao Y, Popple RA, Soike M, Boggs DH, et al. Leveraging intelligent optimization for automated, cardiac-sparing accelerated partial breast treatment planning. Front Oncol. (2023) 13:1130119. doi: 10.3389/fonc.2023.1130119
22. Pogue JA, Cardenas CE, Harms J, Soike MH, Kole AJ, Schneider CS, et al. Benchmarking automated machine learning-enhanced planning with ethos against manual and knowledge-based planning for locally advanced lung cancer. Adv Radiat Oncol. (2023) 8:101292. doi: 10.1016/j.adro.2023.101292
23. Offersen BV, Boersma LJ, Kirkove C, Hol S, Aznar MC, Biete Sola A, et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother Oncol J Eur Soc Ther Radiol Oncol. (2015) 114:3–10. doi: 10.1016/j.radonc.2014.11.030
24. Offersen BV, Boersma LJ, Kirkove C, Hol S, Aznar MC, Sola AB, et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer, version 1.1. Radiother Oncol J Eur Soc Ther Radiol Oncol. (2016) 118:205–8. doi: 10.1016/j.radonc.2015.12.027
25. Noël G, Antoni D, Barillot I, Chauvet B. [Delineation of organs at risk and dose constraints]. Cancer Radiother J Soc Francaise Radiother Oncol. (2016) 20 Suppl:S36–60. doi: 10.1016/j.canrad.2016.07.032
26. Ung M, Rouyar-Nicolas A, Limkin E, Petit C, Sarrade T, Carre A, et al. Improving radiotherapy workflow through implementation of delineation guidelines & AI-based annotation. Int J Radiat Oncol Biol Phys. (2020) 108:e315. doi: 10.1016/j.ijrobp.2020.07.753
27. Cozzi L, Lohr F, Fogliata A, Franceschini D, De Rose F, Filippi AR, et al. Critical appraisal of the role of volumetric modulated arc therapy in the radiation therapy management of breast cancer. Radiat Oncol Lond Engl. (2017) 12:200. doi: 10.1186/s13014-017-0935-4
28. Popescu CC, Olivotto IA, Beckham WA, Ansbacher W, Zavgorodni S, Shaffer R, et al. Volumetric modulated arc therapy improves dosimetry and reduces treatment time compared to conventional intensity-modulated radiotherapy for locoregional radiotherapy of left-sided breast cancer and internal mammary nodes. Int J Radiat Oncol Biol Phys. (2010) 76:287–95. doi: 10.1016/j.ijrobp.2009.05.038
29. Sayah R, Felefly T, Zouein L, El Barouky J, Khater N, Farah N, et al. Dosimetric impact of switching from AAA to Acuros dose-to-water and dose-to-medium for RapidArc plans of nasopharyngeal carcinomas. Cancer/Radiothérapie. (2020) 24:842–50. doi: 10.1016/j.canrad.2020.05.014
30. Guebert A, Conroy L, Weppler S, Alghamdi M, Conway J, Harper L, et al. Clinical implementation of AXB from AAA for breast: Plan quality and subvolume analysis. J Appl Clin Med Phys. (2018) 19:243–50. doi: 10.1002/acm2.12329
31. Hodapp N. Der ICRU-Report 83: Verordnung, Dokumentation und Kommunikation der fluenzmodulierten Photonenstrahlentherapie (IMRT) [The ICRU Report 83: prescribing, recording and reporting photon-beam intensity-modulated radiation therapy (IMRT)]. Strahlenther Onkol. (2012) 188(1):97–9. doi: 10.1007/s00066-011-0015-x
32. van't Riet A, Mak AC, Moerland MA, Elders LH, van der Zee W. A conformation number to quantify the degree of conformality in brachytherapy and external beam irradiation: application to the prostate. Int J Radiat Oncol Biol Phys. (1997) 37(3):731–6. doi: 10.1016/s0360-3016(96)00601-3
33. Fenoglietto P, Bourgier C, Riou O, Lemanski C, Azria D. [Impact of intensity-modulated radiotherapy on node irradiation for breast cancer]. Cancer Radiother J Soc Francaise Radiother Oncol. (2015) 19:265–70.
34. Lauche O, Kirova YM, Fenoglietto P, Costa E, Lemanski C, Bourgier C, et al. Helical tomotherapy and volumetric modulated arc therapy: New therapeutic arms in the breast cancer radiotherapy. World J Radiol. (2016) 8:735–42. doi: 10.4329/wjr.v8.i8.735
35. Quesada S, Fenoglietto P, Gourgou S, Lemanski C, Draghici R, Ailleres N, et al. Efficacy, safety, and feasibility of volumetric modulated arc therapy for synchronous bilateral breast cancer management. Front Oncol. (2022) 12:967479. doi: 10.3389/fonc.2022.967479
36. Riou O, Fenoglietto P, Bourgier C, Lauche O, Boulbair F, Charissoux M, et al. Feasibility of accelerated partial breast irradiation with volumetric-modulated arc therapy in elderly and frail patients. Radiat Oncol Lond Engl. (2015) 10:209. doi: 10.1186/s13014-015-0516-3
Keywords: ethos, IOE, automation, AI, breast cancer
Citation: Prunaretty J, Lopez L, Cabaillé M, Bourgier C, Morel A, Azria D and Fenoglietto P (2024) Evaluation of Ethos intelligent optimization engine for left locally advanced breast cancer. Front. Oncol. 14:1399978. doi: 10.3389/fonc.2024.1399978
Received: 12 March 2024; Accepted: 13 June 2024;
Published: 01 July 2024.
Edited by:
Guang Li, Memorial Sloan Kettering Cancer Center, United StatesReviewed by:
Hong Qi Tan, National Cancer Centre Singapore, SingaporeYibo Xie, Duke University, United States
Copyright © 2024 Prunaretty, Lopez, Cabaillé, Bourgier, Morel, Azria and Fenoglietto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica Prunaretty, SmVzc2ljYS5wcnVuYXJldHR5QGljbS51bmljYW5jZXIuZnI=
†These authors have contributed equally to this work