 Dazhen Jiang†
Dazhen Jiang† Chunxu Yang†
Chunxu Yang† Shaoxing Sun†
Shaoxing Sun† Dajiang WangZhizhi XiaoJie Hu
Dajiang WangZhizhi XiaoJie Hu Zijie MeiConghua XieHui Liu
Zijie MeiConghua XieHui Liu Hui Qiu*†
Hui Qiu*† Xiaoyong Wang*†
Xiaoyong Wang*†- Department of Radiation and Medical Oncology, Hubei Key Laboratory of Tumor Biological Behaviors, Hubei Cancer Clinical Study Center, Zhongnan Hospital of Wuhan University, Wuhan, China
Purpose: To assess the dosimetric effectiveness of image-guided radiation treatment (IGRT) and online adaptive radiation therapy (oART) for cervical cancer. As well as survival follow-up was conducted to validated the safety and efficacy of oART.
Methods: A total of 15 cervical cancer patients were enrolled. oART was performed on a CT-integrated linear accelerator. The initial plan was revised to include the distribution of IGRT dose using daily fan-beam CT (FBCT) images, after which the distinctions between ART and IGRT in terms of target coverage and organs at risk (OARs) sparing were analyzed. Survival follow-up was conducted to validated the safety and efficacy of oART in this group.
Results: PTV Dmax value decreased by 1.23 Gy in the ART plan when compared to that in the IGRT plan; PTV D95 increased by 1.34 Gy; PTV V50 coverage increased by 4.86%; CTV coverage increased by 3.02%; PTV D2cc of the colon, rectum, and small intestine decreased by 1.24 Gy, 1.29 Gy, and 1.12 Gy, respectively. The V10 and V30 of the pelvis increased by 1.27% and 0.56%, respectively, while the V30 of the left and right femoral heads dropped by 2.82% and 3.41%, respectively. Except for the pelvic changes, all other differences were statistically significant (p < 0.01). The average time for the ART procedure was 21.22 min (range: 18.72–24.90 min). The median follow-up time is 28.0 months. Median event-free survival and overall survival were not reached. EFS rate and OS rate at 3 years were 79.4% and 92.9%.
Conclusion: Online ART for cervical cancer can minimize the dose of OARs and enhance the target volume coverage significantly when compared to IGRT with satisfied survival time.
Introduction
Globally, the fourth most prevalent malignancy in women is cervical cancer (1). For the past 15 years, intensity-modulated radiotherapy (IMRT) and image-guided radiation (IGRT) have been used as modifications to the external beam radiation treatment for gynecological cancer. IGRT has made personalized treatment (2, 3), dose escalation, better clinical outcomes, and less toxicity to normal tissues (4, 5) possible. The capacity to adhere to target quantities, which decreases the dose administered to organs at risk (OARs), also motivates the clinical use of these modifications (6). Clinical improvements are evident as a decrease in acute and chronic gastrointestinal and hematological toxicities have been observed with the switch from pelvic three-dimensional conformal radiation (3DCRT) to IMRT (7, 8). The risk of geographical miss arising from the complex and varying inter- and intrafractional mobility observed with the cervix-uterus complex was an initial cause of concern for the application of IMRT for gynecological cancer treatment (9). This depends on tumor regression during radiation therapy and bladder and rectal filling (9, 10). A mean interfractional cervical motion of 2.3–16 mm in the anterioposterior direction, 2.7–8 mm in the superior–inferior direction, and 0.3–10 mm in the lateral direction was reported in a systematic review (11). According to Tyagi et al. (12), a margin of >35 mm would be necessary to cover the clinical target volume (CTV) for every fraction. However, one-third of the cases failed to cover the CTV as a 15-mm margin was used. Cervical cancer treatment needs to be more personalized so as to address this interpatient variability. However, due to the special anatomical position of the cervix, adjacent to the bladder and rectum with obvious changes in physiological status (varying due to the degree of filling), coupled with random factors such as tumor retraction, the target area may be deformed and moved between fractional treatments, which may lead to dose distribution deviation.
Online adaptive radiotherapy (online ART) is another development in adaptive radiation therapy (ART) methods. OART can modify plans based on real-time images and can be executed immediately to accommodate random transfer of target volume (TV) and organs, as well as the deformation of OARs in the fractional treatments, to ensure the coverage of the target dose and to control the dose of OARs (13–15). With daily replanning and oART, the issue of interfractional mobility may be reduced. Ten years’ worth of technological and computational developments in radiotherapy have thankfully made oART a clinical potential (13, 15). This therapeutic approach relies on daily anatomical fluctuations in target volumes and OARs and changes in tumor volume. Therefore, planning treatment volume (PTV) margins may decrease (16). Most commercially available oART systems are guided by magnetic resonance imaging (MRI); however, recent developments have resulted in the development of a cone beam computed tomography (CBCT)-guided system. Table 1 presents the possible advantages of oART in cervical cancer external beam radiation treatment with CBCT and MRI guidance.
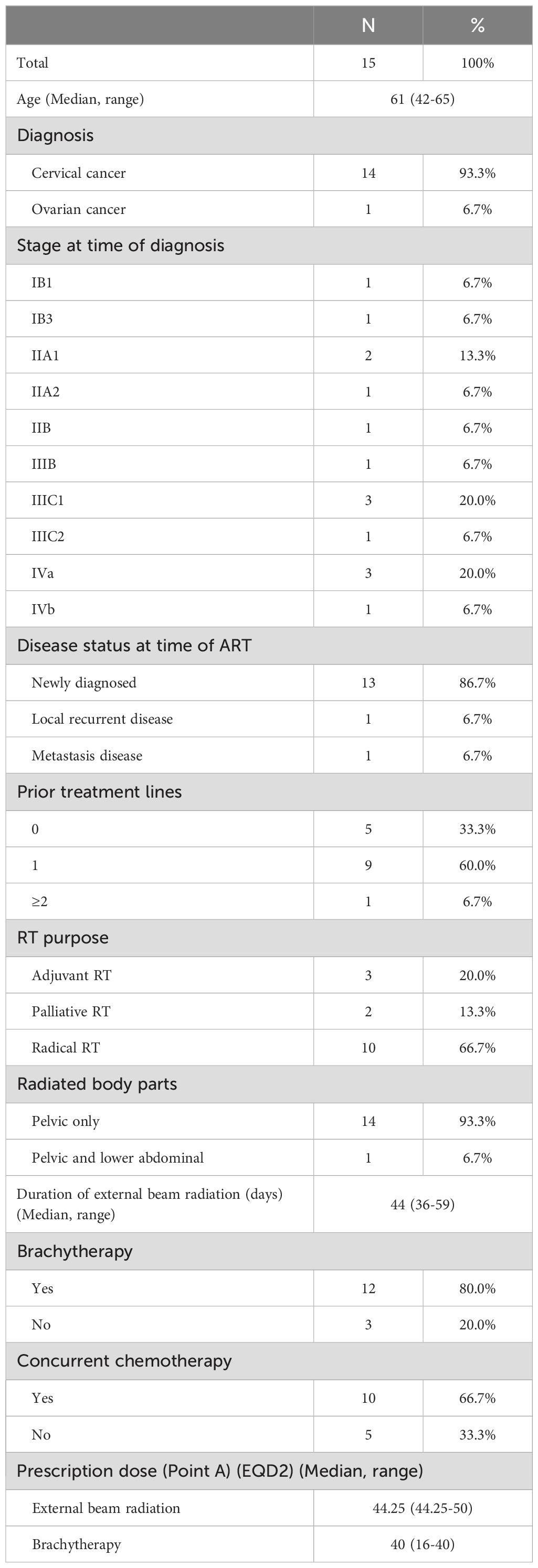
Table 1. Patients’ characteristics.
The currently used oART is based on transforming CBCT and MRI images into pseudo-CT images for radiotherapy planning design, which increases the time of oART and introduces certain errors. The FBCT-linac accelerator, a fan-beam computed tomography (CT), which may be used directly in radiotherapy planning design, is the basis for the present investigation. This accelerator considerably shortens the time of oART and improves the dose accuracy.
This study compared oART and a clinically implemented plan selection technique to quantify the added value of oART performed for cervical cancer by using the FBCT-linac accelerator. The benefit was measured in terms of target volume coverage and dose to OARs. The aim of this study was to evaluate the long-term clinical results of oART in a single center and contribute to the rare evidence in that field.
Methods
Patient selection and simulation
We enrolled 15 cervical cancer patients received pelvic IMRT treatment at our facility between January 2022 and November 2022 in this study. According to FIGO stage classification (17), the patients information were presented in Table 1. A 3-mm slice thickness helical CT scanner (Sensation Cardiac 64x, Siemens, Munich, Bavaria, Germany) was used to perform CT simulation. Before the simulation was started, the patients were placed in a supine position, and a vacuum-formed cradle, a comfortably full bladder, and no bowel preparation were ensured.
15 patients radiated with ART technique were enrolled. 14 of them were diagnosed as cervical cancer. 10 received radical concurrent chemoradiation and 3 received adjuvant radiotherapy. The median prescription dose at point A was 44.25Gy for external beam radiation. 12 of them received brachytherapy with median dose of 40Gy. Patients characteristics were listed in Table 1.
Normal tissue definition
In this study, the rectum, small bowel, bladder, femoral heads, and bone marrow were all considered normal tissue. The small bowel, which encompasses the entire peritoneal cavity from L4 to L5, was contoured for each patient. This contour, along with the others, was defined by a single radiation oncologist so as to ensure consistency in target definition and treatment planning. GTVp refers to the primary lesion of cervical tumors. GTVn refers to pelvic metastatic lymph nodes. From the L4-L5 vertebra to the inferior border of the obturator foramen, CTV generally includes vaginal stumps, common iliac, internal iliac, external iliac, obturator and presacral lymphatic drainage areas, cervix, uterine body, parauterine and partial vagina. Delineations method of target volumn complied with ICRU report 50 and 62 and consensus guidelines developed by RTOG (18). The PTV was produced by applying a uniform 5-mm margin to the CTV (19).
To ensure consistency, each treatment planning technique was created by the same radiation physicist. Figure 1 illustrates how United Imaging TPS (United Imaging HealthCare Co., LTD, Shanghai, China) was used to design the inverse planned dynamic IMRT plans. Using the analytic CC algorithm with a grid size of 2.0 mm, the dosage to be administered to the irradiated zone was calculated. With 6 MV photon beams, sliding-window fields, and a multileaf collimator leaf size of 5 mm, we applied the machine parameter optimization approach.
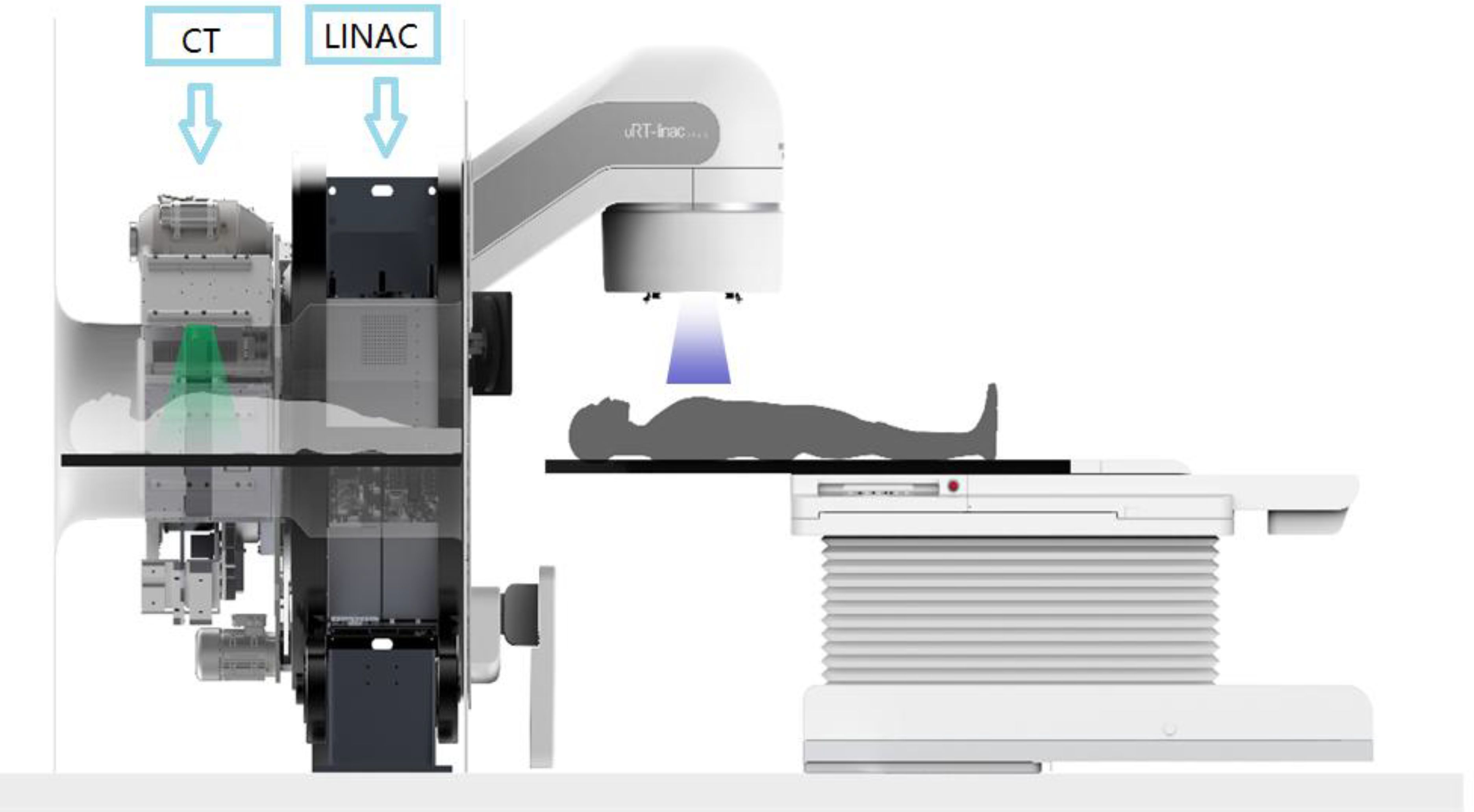
Figure 1. The linear accelerator of United Imaging Healthcare’s CT linac URT-Linac 506C.
IMRT therapy planning
By using the initial radiotherapy CT scans of all patients, a radiation treatment plan was designed at the United Imaging FBCT-Linac workstation for each patient. This plan was prescribed as a 25-day IMRT session. A 9-field coplanar static intensity-modulated radiation treatment plan was implemented with a 50-Gy prescribed dose for PTV-CTV.
Online ART plan
After the patient was positioning, the FBCT images were acquired based on the oART process. The simulation CT was registered to the FBCT by using a deformable alignment. Normal organs were delineated by TPS based on the outputs of the coimage automatic contour system. An experienced clinician modified the CTV after deformable registration. The PTV was generated by expanding the 5-mm margin from the GTV and CTV. Based on FBCT, oART plans were automatically generated using TPS algorithms and were evaluated by physicists and clinicians. After the plans were evaluated, they were transmitted to the treatment terminal for FBCT guidance and treatment.
Evaluation indicators
The plans of patients receiving IGRT and ART must be assessed for the actual target coverage rate and OAR sparing. The IGRT parameter values can be obtained as follows. The treatment plan for the simulation FBCT was first strictly copied to the FBCT on each treatment day to calculate the dose as the IGRT dose received by the patient in each treatment fraction. The dose parameters of each IGRT plan were statistically analyzed, and the final average IGRT values were then obtained. Similarly, the final average ART values.
The dose and coverage of PTV and OARs were compared. Dx% was the maximum dose of volume accepted by x% of PTV or OARs, and Vx% was the volume of the prescribed dose line for x% of PTV or OARs. The plan had to be approved with at least 95% of the PTV receiving 100% of the prescribed dose, and the PTV’s maximum dosage had to be <110% of the prescribed dose. Some dosimetric parameters were collected for the OARs, namely small bowel, rectum, femoral heads, bone marrow, and colon sigmoid, including the V30 (the percent of volume that received 30 Gy) for the femoral heads and bone marrow. These values also included the maximum dose of 2 cc (D2cc) of the structure representing the significant maximum dosage for the colon sigmoid, rectum, and small bowel.
Statistical analysis
The Statistical Package for Social Sciences (version 22.0, IBM Corporation, Armonk, NY, USA) was used for data analysis. The Shapiro−Wilk method was used to test the normality of the data. A paired sample t test was performed for data lines with a normal distribution, while the Wilcoxon signed rank test was performed with a significance level of 0.05.
Results
Table 2 presents all values. Compared with those of the IGRT plan, the PTV Dmax of the ART plan decreased by 1.23 Gy; its PTV D95 increased by 1.34 Gy; its PTV coverage V50 increased by 4.86%; its CTV coverage increased by 3.02%; and its D2cc of the small intestine, rectum, and colon decreased by 1.24 Gy, 1.29 Gy, and 1.12 Gy, respectively. The V30 of the left and right femoral heads decreased by 2.82% and 3.41%, respectively. The V10 and V30 of the pelvis increased by 1.27% and 0.56%, respectively. Except for the pelvis, statistically significant differences were observed for all other organs (P < 0.01).

Table 2. Depicts the parametric statistics of PTV, CTV, and each OAR.
Table 3 presents the average time taken for imaging, contouring, planning, delivery and the time it takes for patients to enter and leave the treatment room.
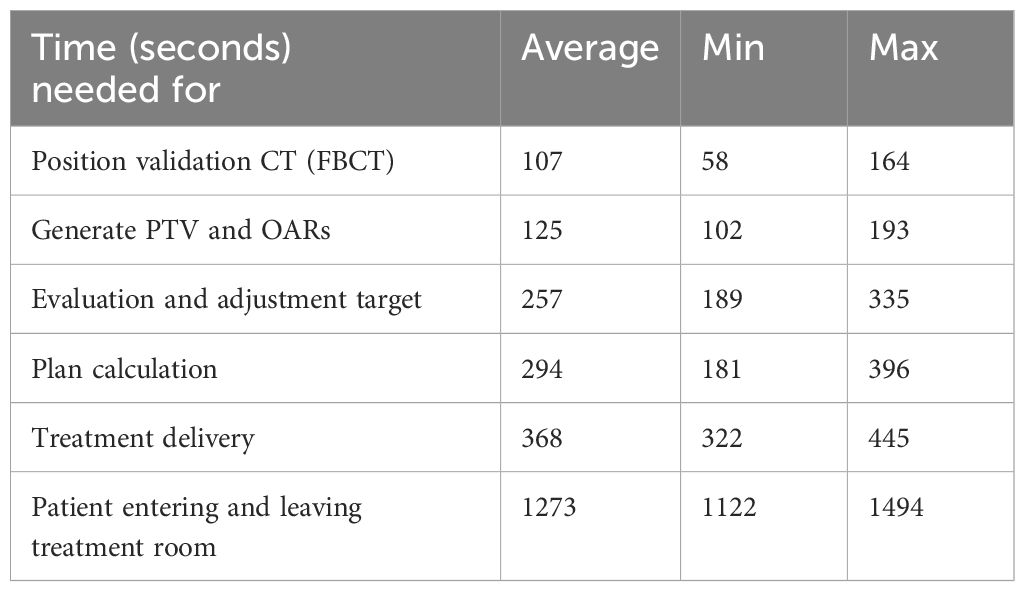
Table 3. Overview of steps and duration.
From Figure 2, we can see that the changes among fractional treatments were irregular. However, it can be seen that as the number of treatments increases, the patient’s urine retention decreases, which may be due to a certain degree of cystitis.
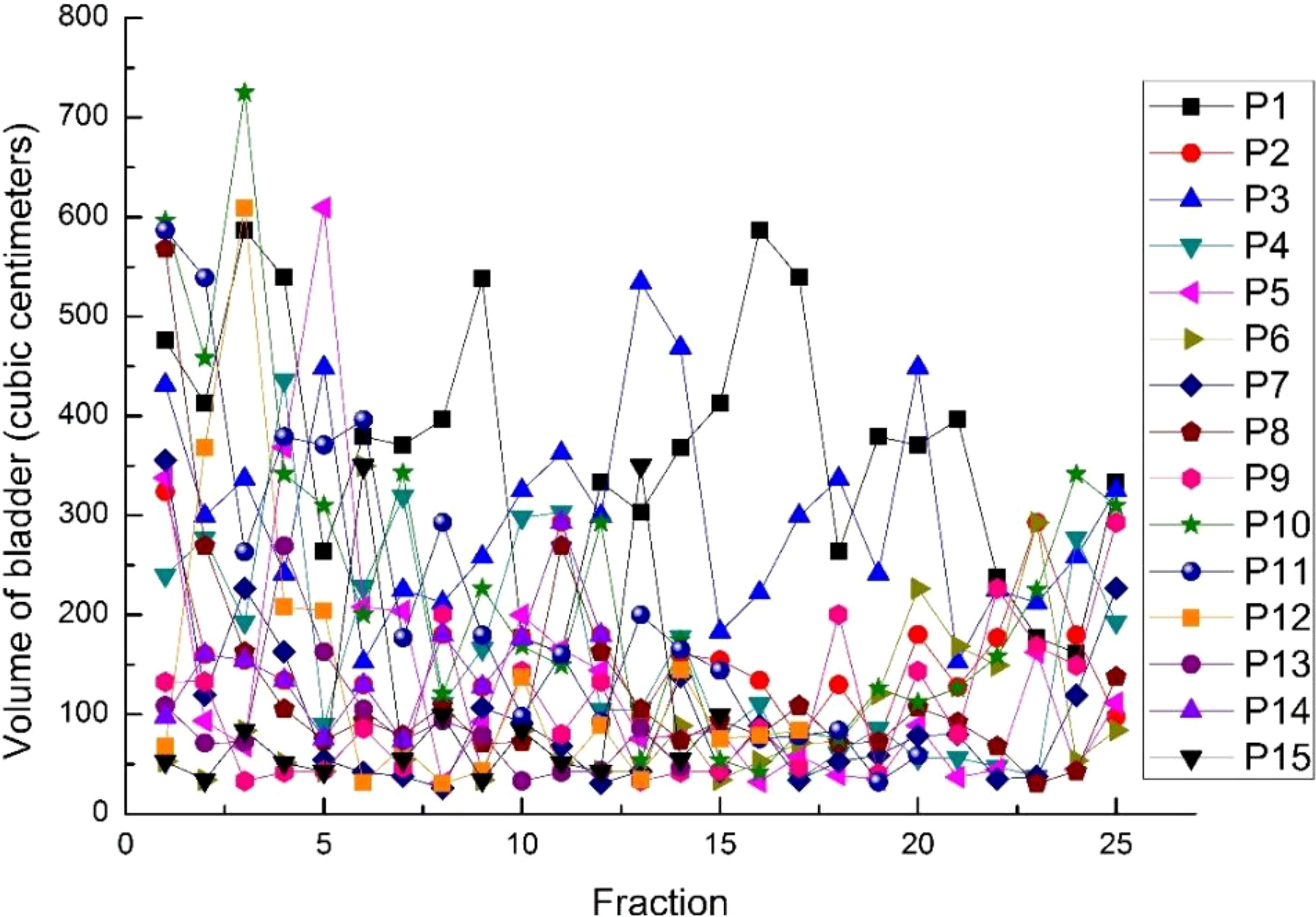
Figure 2. The volumes of the bladder in 15 cases for every fraction.
From Figures 3, 4, we can see that compared to the IGRT plan, the ART plan can significantly improve the coverage of the target area while better protecting organs at risk.

Figure 3. The ART plan dose distribution for one of the patients with (A) 100% (50 Gy), (B) 80% (40 Gy), (C) 60% (30 Gy) and (D) 40% (20 Gy) on coronal views.

Figure 4. The IGRT plan dose distribution for one of the patients with (A) 100% (50 Gy), (B) 80% (40 Gy), (C) 60% (30 Gy) and (D) 40% (20 Gy) on coronal views.
In this study, Figures 5–9 present PTV and OAR DVH parameters for both IGRT selection and oART. Compared with the IGRT plan, target coverage rate parameters for the ART plan were improved. Significant differences in V50 and D95 (P < 0.05) were observed for PTV parameters between the two groups. The V50 values of GTV significantly differed between the two groups (P < 0.05). For the colon, rectum, and small intestine, the D2cc values of IGRT were higher than those of ART.
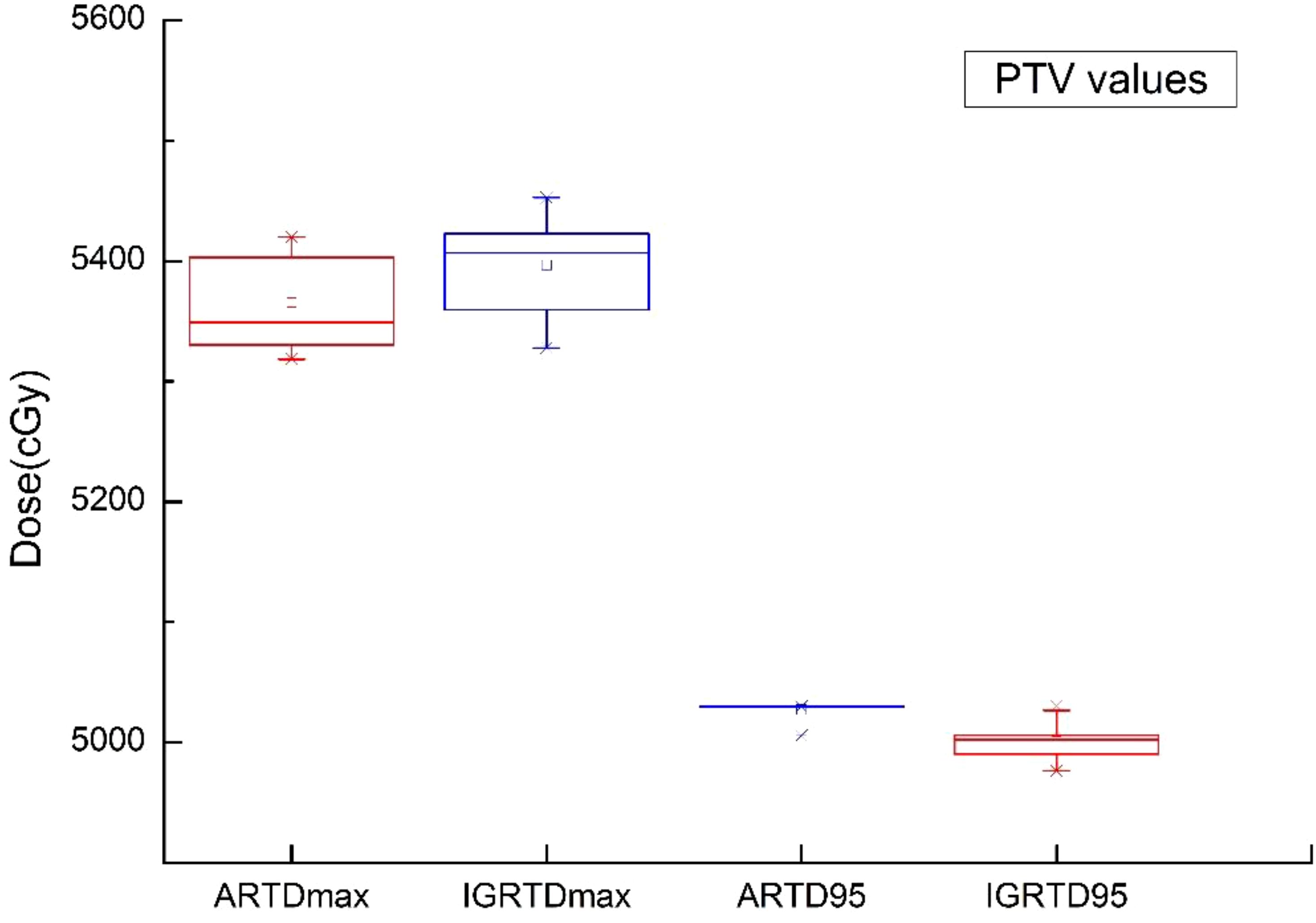
Figure 5. Boxplot showed the values of PTV different DVH parameters for both IGRT selection and online ART.

Figure 6. Boxplot showed the coverage rate of PTV different DVH parameters for both IGRT selection and online ART.
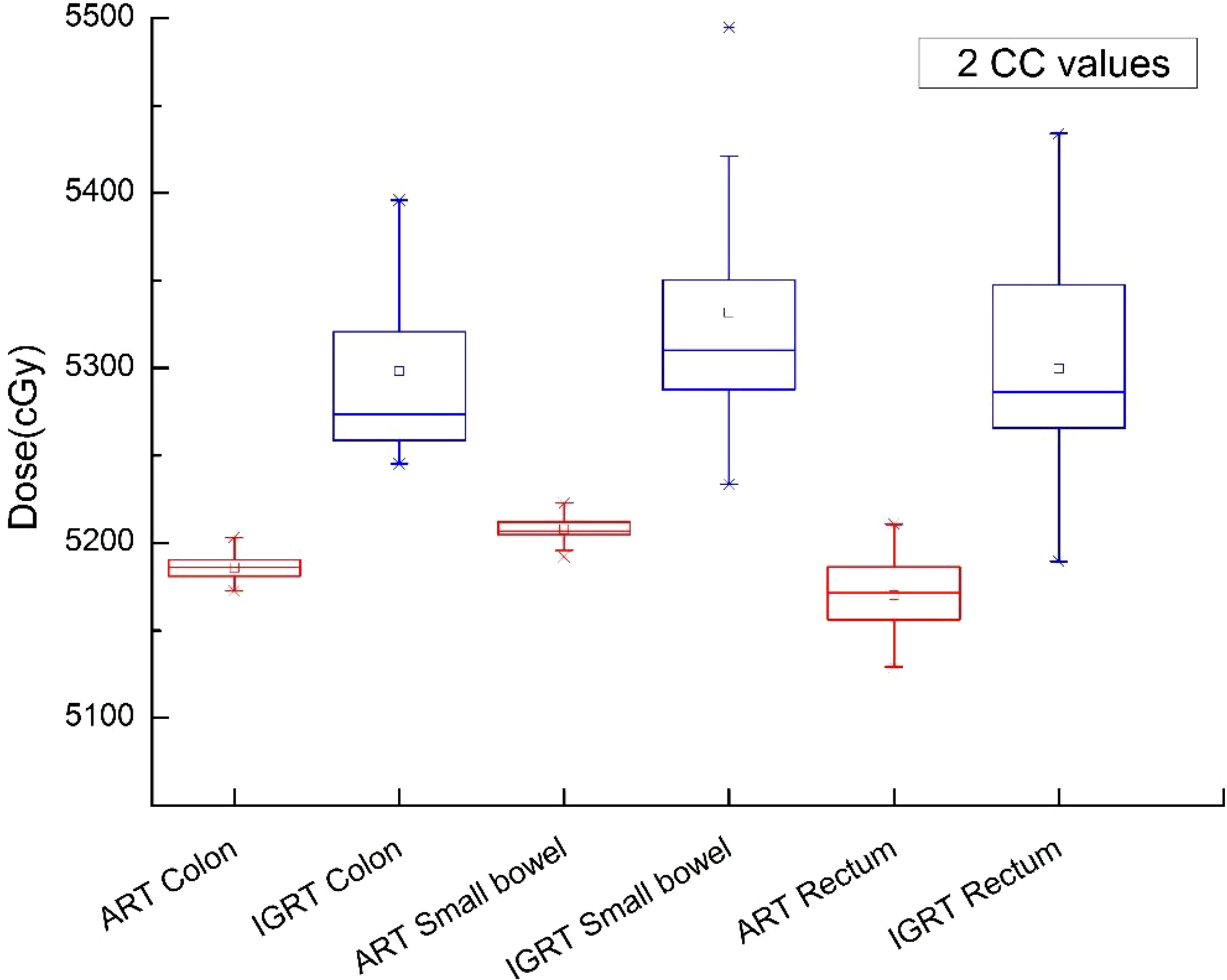
Figure 7. Boxplot showed the 2cc values of OAR different DVH parameters for both IGRT selection and online ART.
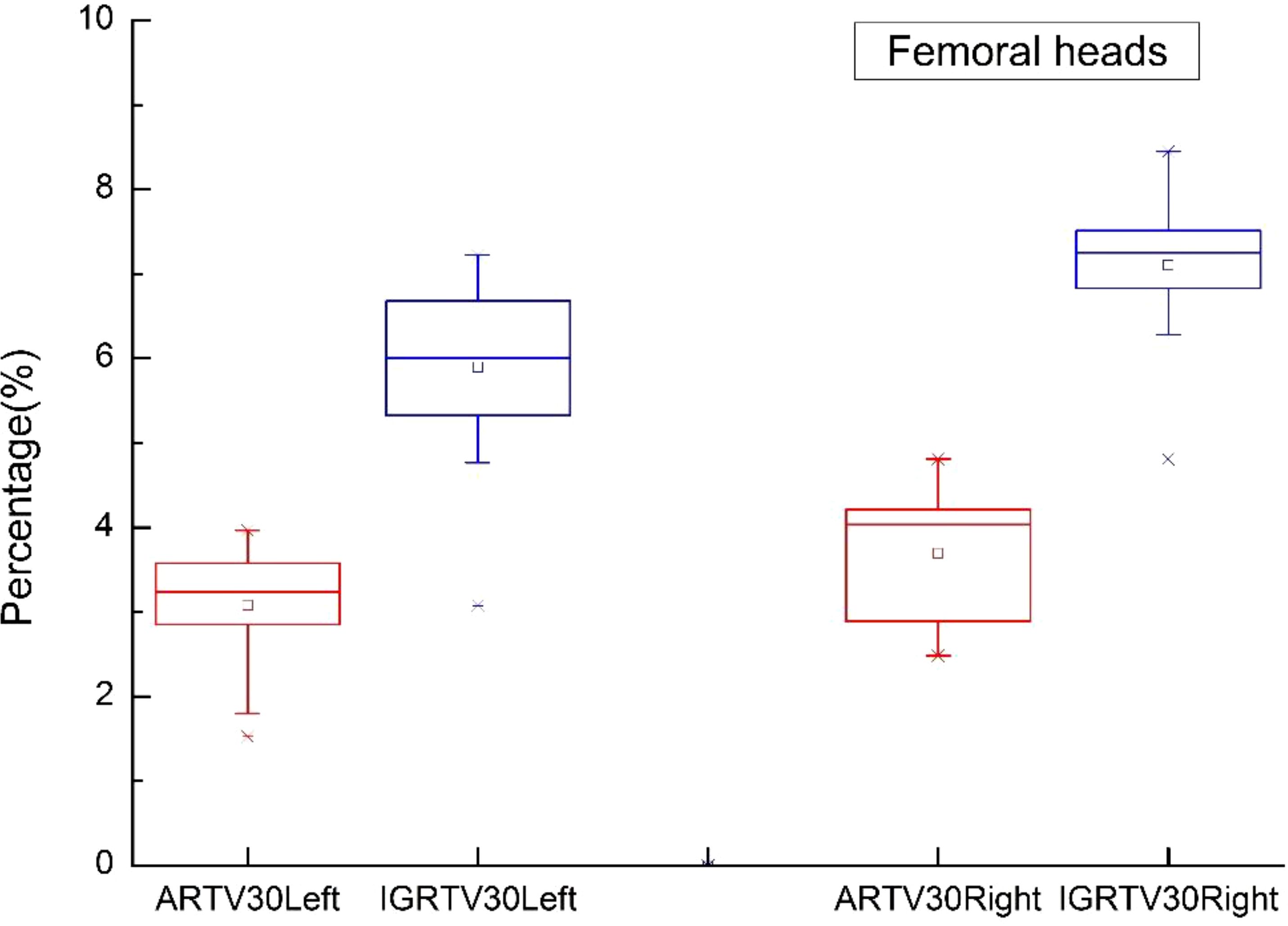
Figure 8. Boxplot showed the values of femoral heads different DVH parameters for both IGRT selection and online ART.
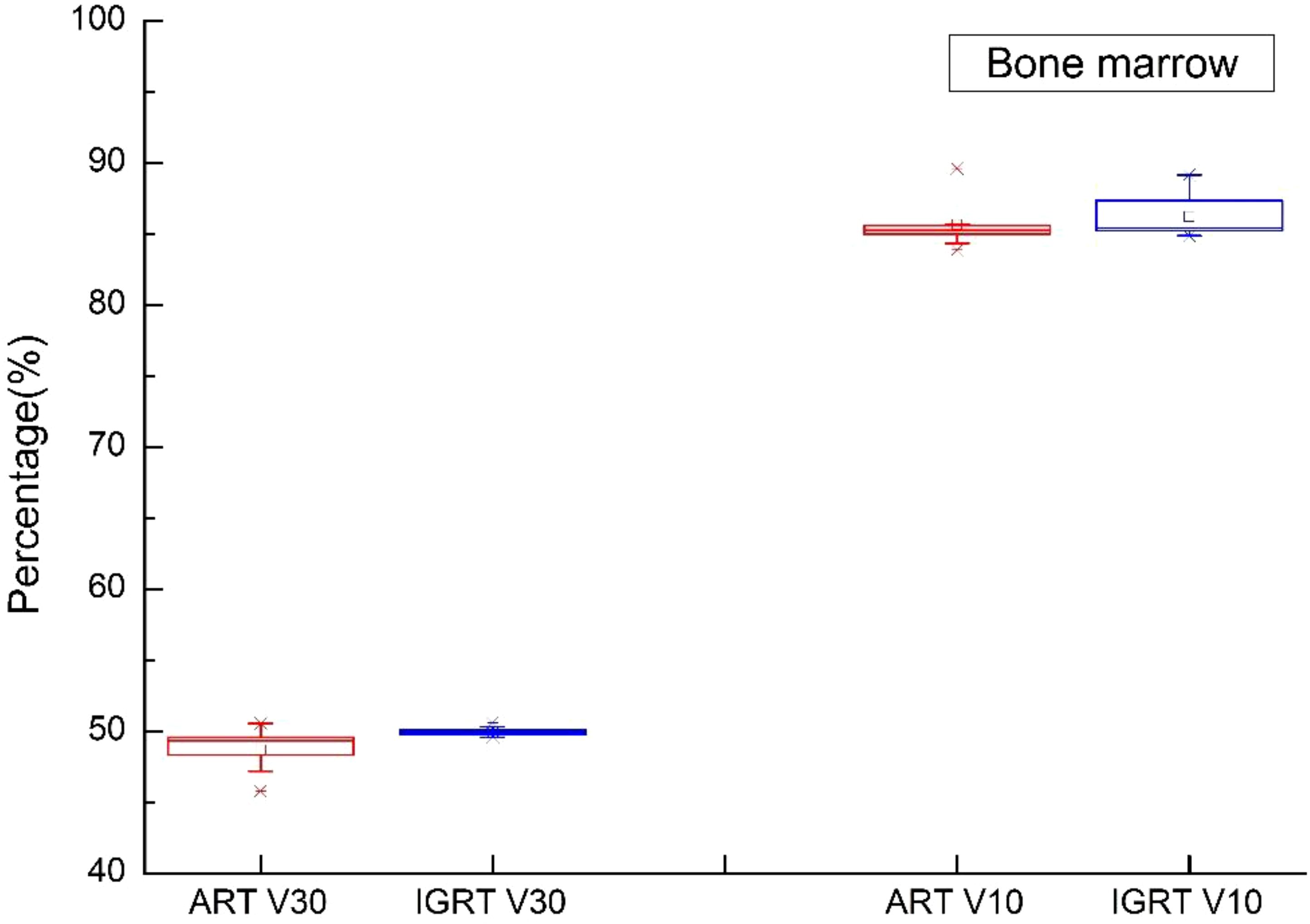
Figure 9. Boxplot showed the values of bone marrow different DVH parameters for both IGRT selection and online ART.
In this study, the average time from positioning to the end of beam exit was 21.22 minutes (SD 2.057 minutes), with an average positioning time of 107 seconds (SD 26.60 seconds), target modification time of 257 seconds (SD 59.21 seconds), rescheduling time of 294 seconds (SD 57.32), and beam exit time of 368 seconds (SD 64.01).
The objective response rate was 91.7% for 12 patients with gross tumor in which 11 patients reached complete response at the first or second tumor evaluation. The median follow-up time is 28.0 months. 3 patients experienced tumor recurrence and none of recurrent lesion was in the radiation field. Event-free survival rate and overall survival rate at 3 years were 79.4% (Figure 10) and 92.9% (Figure 11). Median event-free survival and overall survival were not reached.
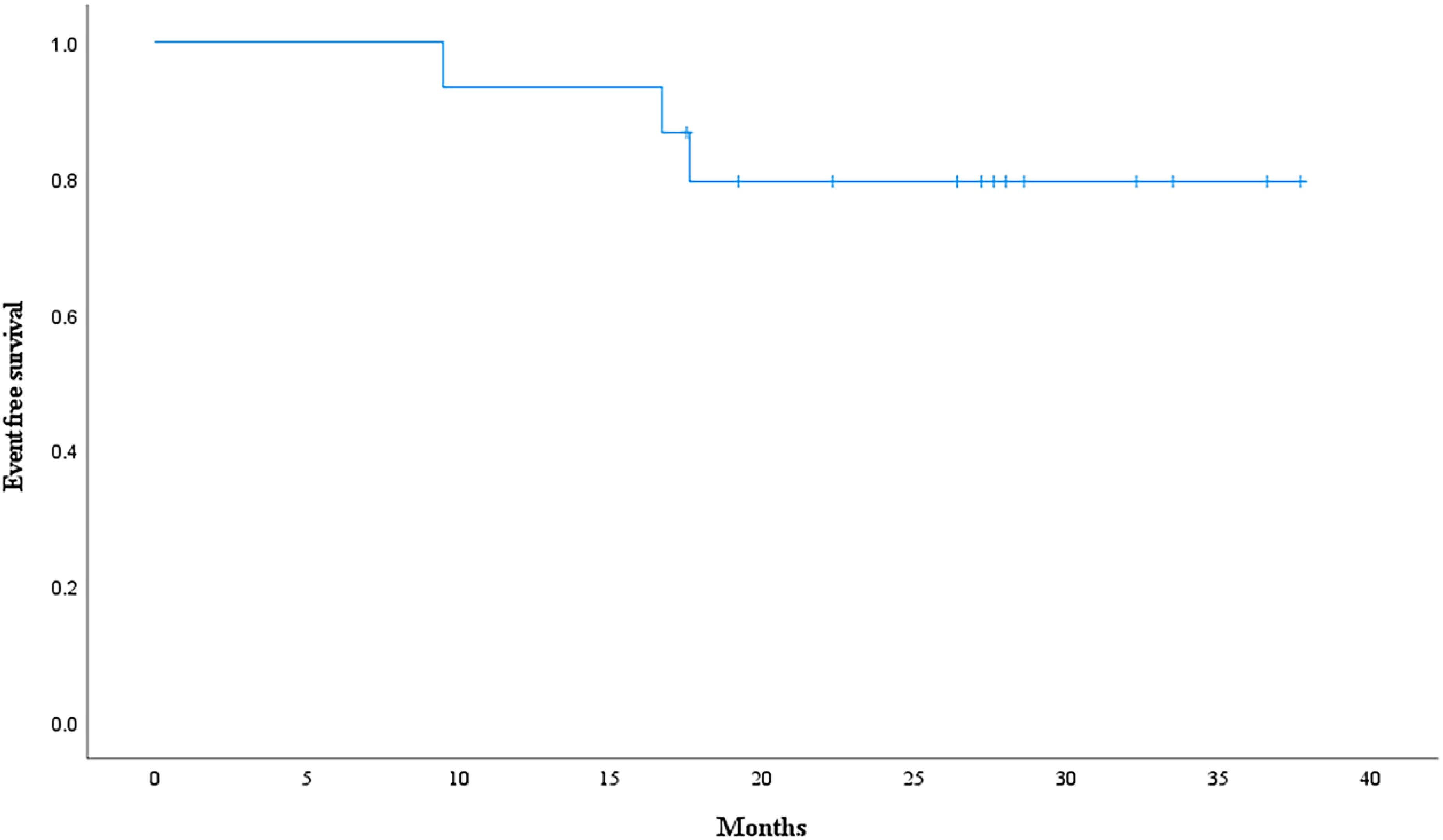
Figure 10. Event-free survival curve calculated with Kaplan-Meier methods.
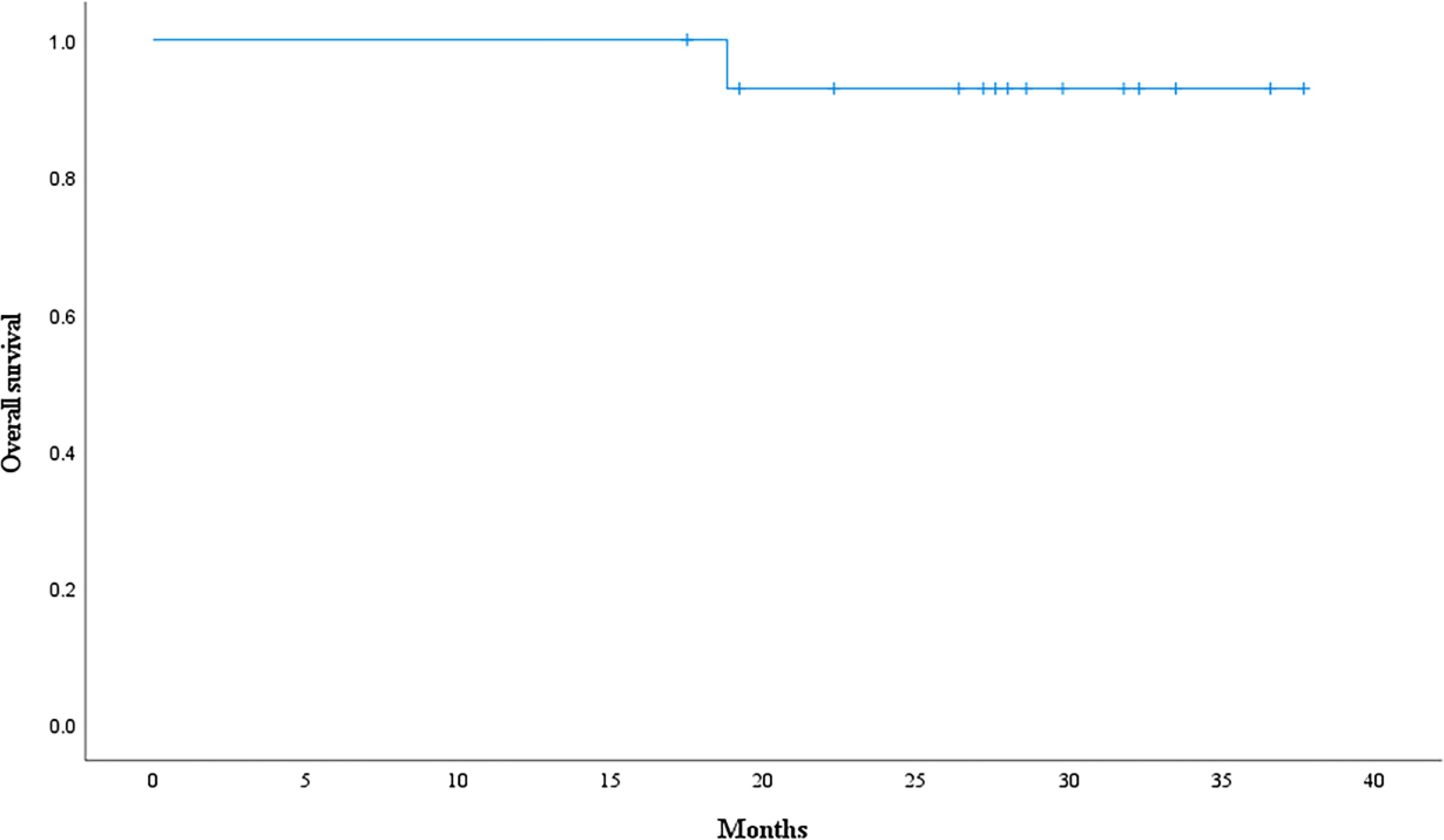
Figure 11. Overall survival curve calculated with Kaplan-Meier methods.
Discussion
This trial revealed the dosimetric benefits of daily ART for cervical cancer over IGRT. Except for bone marrow, oART technology considerably increases target coverage and dramatically lowers OAR doses. oART techniques necessitate workflows and roles to be reorganized along with precise and quick contouring and treatment planning. Because of these requirements, a radiation oncologist, medical physicist, and/or dosimetrist need to be present while using the treatment machines. Because adaption is time-consuming, timeslots could also need to be changed (20, 21).
In patients with rectal cancer and cervical cancer, most simulated adaptive therapies may have been completed in 30- and 15-min treatment windows, respectively (19). The mean duration in this study was 21.22 min. The simulated ART workflow for cervical cancer was completed in 24.4 min to determine the OARs structure and target contours (19). Henke et al. and Lamb et al. reported ART processes of 23 and 24 min, respectively, for abdominal SBRT by using an MRI-guided system (ViewRay, Oakwood Village, OH) (22). In another study, the median total treatment durations for abdominal SBRT were 46 and 62 min for adapt-to-shape–based and adapt-to-position–based workflows (23).
By preserving target coverage and lowering doses to OARs, online ART has the benefit of providing dosimetric gains. To confirm the disease control and fewer complications of online ART in customized treatment, more research is necessary. Four fundamental technologies are needed for ART: quality assurance, replanning, assessment, and imaging (24). Patients are chosen for adaptation based on alterations in the volume of the tumor or physiological changes to OARs, which are frequently difficult to identify without excellent imaging. To calculate the dosage for the existing AR workflows that incorporate kV CBCT (25) or MRI (26), a pseudo CT has to be created. The pseudo CT is produced by deforming the daily CBCT or MRI from the CT simulation. An assignment of the water-air-bone density may then be necessary for the MRI-based ART workflow. Consequently, the accuracy of the dose calculation depends on the uncertainty of the deformable image registration, which needs to be carefully quantified. The viability of CBCT-only or MRI-only treatment planning is still being investigated, despite the fact that deep learning can be used to create a synthetic CT that is required for dose calculation from CBCT or MRI images (27, 28). Because of its superior CT-to-density accuracy, diagnostic-quality FBCT is currently a better image modality for adaptive radiotherapy.
Yoon et al. used the Varian Ethos system to simulate adaptive therapy for head and neck cancer patients. They presented the closest direct comparison of the metrics reported in the present study (29). The average time required for identifying the influencer structure and target contours and for creating an adaptive replan (11.8 and 6.1 min, respectively) was comparable with those reported here for patients with rectal and cervical cancer, although the process was replicated for a completely different treatment site (19).
Numerous studies have examined how different adaptive processes affect the target coverage and dosage of OARs. Oh et al. simulated numerous ART approaches for cervical cancer patients, while doing so they combined offline adaptive replanning once or once a week with or without bone or soft tissue MRI guidance (30). In this study, we used FBCT, which is a modality of considerably higher quality than CBCT and traditional MVCT (31, 32). ART can be completed more rapidly with diagnostic-grade FBCT than with CBCT-based ART, according to the planned CT used in the present study. ART in which MVCT and CBCT are used can reduce several problems, including the deformation correction and HU value correction of CT images (31–33). The typical changes in the D2cc of the rectum, bladder, bowel, and sigmoid colon, as determined from the dose accumulated by using ART approaches, varied from −0.96 to 0.10 Gy compared with the nominal plan. Furthermore, the average V45Gy discrepancies of these organs varied from −3.9% to 6.4%.
In this study, the PTV Dmax of the ART plan decreased by 1.23 Gy, PTV D95 increased by 1.34 Gy, PTV coverage V50 increased by 4.86%, and CTV coverage increased by 3.02%. On comparing oART replanning with daily IGRT alignment by using CBCT images, Qin et al. discovered that oART reduces doses to multiple OARs, including the bladder (D1% decreased 1.6 Gy) and the rectal wall (D5% decreased 0.9 Gy) and increased the average dose to 99% of the CTV (D99% increased by 1.8 Gy) (34). In our study, the D2cc in the colon, rectum, and small intestine decreased by 1.12, 1.29, and 1.24 Gy, respectively. While V10 and V30 in the pelvis increased by 1.27% and 0.56%, respectively. V30 in the left and right femoral heads decreased by 2.82% and 3.41%. Using an MRI linear accelerator, Dunlop et al. evaluated the dosimetric impact of oART on the prostate (35). Additionally, a 0.5% drop in dosages to OARs, such as the V95% to the rectum, was observed in their study. The benefits of replanning may not always yield dosimetric improvement for all OARs, as evidenced by the 3.5% and 0.8% increases in the bladder V95% and bowel D0.01cc, respectively (36). These benefits also depend on several interrelated factors associated with plan reoptimization. However, the results of the present study are consistent with those of previous studies in showing that oART approaches can augment OAR sparing by several centigrays to several grays per fraction, and target coverage by several percent. After physicians gain more clinical experience with these devices, the exact values of the dosimetric effects of ART approaches will become clearer.
Furthermore, factors unique to each patient may substantially affect the quality of CBCT images, which must be high to achieve accurate contour propagation and deformable image registration. Even when the underlying anatomical alteration presents no significant issue, physicians may have to modify outlines because of artifacts in the image.
Most oART is based on transforming CBCT and MRI images into pseudo-CT images for radiotherapy planning design, which increases the time of oART and introduces certain errors. This study is based on the FBCT-linac accelerator, a fan-beam CT that can be directly used in radiotherapy planning design. The use of the FBCT-linac accelerator prominently shortens the time required for oART and improves the dose accuracy. ART plan was accurately implemented and provided dosimetric results with significant advantages in this study. To ensure the accuracy of dose accumulation in fading tumors, understand the principles of target volume adjustment, determine the trigger conditions for online ART, and determine the potential risks of increasing the radiation dose of each KV-FBCT, among other detailed investigations that are still necessary (37, 38).
This study analyzes the usage time of various stages of FBCT-based oART in detail. The target area, OAR modification time, and radiotherapy planning optimization time occupy a considerable proportion. Therefore, to improve clinical efficiency, we collaborated with a third party to develop an artificial intelligence-based system to delineate target areas and OARs automatically for cervical cancer. To improve the treatment time, the conventional 9-field treatment is replaced with the VMAT plan, thereby reducing the treatment time. However, the optimization time of the VMAT plan also increased accordingly. According to the preliminary research results, employing the VMAT program can reduce a certain amount of ART time, and specific research results will be published in the future.
Online ART presents a lot of difficulties. One is the method of calculating dose accumulation, which takes into consideration changes in dosimetry and anatomy and may be reflected with in vivo dose monitoring, to determine the actual total dose delivered. Furthermore, the completion of other tasks is delayed and resource costs rise as a result of the critical processes requiring full human interventions and the presence of dedicated staff, such as medical physicists and radiation oncologists (39, 40). Third, as ART spreads outside of high-volume centers, it will become increasingly important to decide how and when to adapt with more quantitative, automated, or assisted approaches in order to reduce variability and ensure that ART is administered correctly and consistently. Lastly, data demonstrating the effectiveness of online ART is essential to justify the additional resources and help direct its wider implementation. Lastly, data demonstrating the effectiveness of online ART is essential for directing its wider implementation and providing justification for the extra resources and equipment needed for the method.
Conclusions
To sum up, the oART system improved target coverage and significantly decreased the maximum dose to nearby OARs. Session planning duties must be completed throughout each session, which necessitates additional planning for manpower and workflow. During the process, most time was spent on analyzing and changing target contours. Better contour determination has the most substantial potential to reduce the demand on the resource pool of online ART.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
This study was approved by the medical ethics committee of Zhongnan Hospital of Wuhan University [2022144k]. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
DJ: Data curation, Methodology, Writing – original draft, Writing – review & editing. CY: Methodology, Writing – review & editing. SS: Writing – review & editing, Formal analysis, Investigation. DW: Writing – review & editing, Software. ZX: Formal analysis, Writing – review & editing, Data curation. JH: Formal analysis, Supervision, Writing – review & editing. ZM: Conceptualization, Project administration, Writing – review & editing. CX: Project administration, Resources, Supervision, Writing – review & editing. HL: Conceptualization, Investigation, Resources, Supervision, Validation, Writing – review & editing. HQ: Data curation, Formal analysis, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. XW: Data curation, Investigation, Software, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work is supported by National Key R&D Program of China, Ministry of Science and Technology of the People’s Republic of China. (Grant No. 2022YFC2407100, 2022YFC2407104), Hubei Provincial Natural Science Foundation (Grant No. 2023AFB204) and the Science, Technology and Innovation Seed Fund of Zhongnan Hospital, Wuhan University (project number znpy2019022), Technology and Innovation Seed Fund of Zhongnan Hospital, Wuhan University (project number CXPY2023102).
Acknowledgments
The authors thank the Department of Radiation and Medical Oncology, Zhongnan Hospital of Wuhan University. Thanks for all colleagues’ help and guidance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394e424. doi: 10.3322/caac.21492
2. Otter S, Coates A, Franklin A, Cunningham M, Stewart A. Improving dose delivery by adding interstitial catheters to fixed geometry applicators in high-dose-rate brachytherapy for cervical cancer. Brachytherapy. (2018) 17:580e586. doi: 10.1016/j.brachy.2018.01.003
3. Rangarajan R. Interfraction variations in organ filling and their impact on dosimetry in CT image based HDR intracavitary brachytherapy. J Med Phys. (2018) 43:23e27. doi: 10.4103/jmp.JMP_90_17
4. Thiruthaneeswaran N, Groom N, Lowe G, Bryant L, Hoskin PJ. Focal boost to residual gross tumor volume in brachytherapy for cervical cancer e a feasibility study. Brachytherapy. (2018) 17:181e186. doi: 10.1016/j.brachy.2017.09.012
5. Rijkmans EC, Nout RA, Rutten IH, Ketelaars M, Neelis KJ, Laman MS, et al. Improved survival of patients with cervical cancer treated with image-guided brachytherapy compared with conventional brachytherapy. Gynecol Oncol. (2014) 135:231e238. doi: 10.1016/j.ygyno.2014.08.027
6. Forrest J, Presutti J, Davidson M, Hamilton P, Kiss A, Thomas G. A dosimetric planning study comparing intensitymodulated radiotherapy with four-field conformal pelvic radiotherapy for the definitive treatment of cervical carcinoma. Clin Oncol. (2012) 24:e63ee70. doi: 10.1016/j.clon.2011.06.008
7. Naik A, Gurjar OP, Gupta KL, Singh K, Nag P, Bhandari V. Comparison of dosimetric parameters and acute toxicity of intensity-modulated and three-dimensional radiotherapy in patients with cervix carcinoma: a randomized prospective study. Cancer Radiother. (2016) 20:370e376. doi: 10.1016/j.canrad.2016.05.011
8. Gandhi AK, Sharma DN, Rath GK, Julka PK, Subramani V, Sharma S, et al. Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma: a prospective randomized study. Int J Radiat Oncol Biol Phys. (2013) 87:542e548. doi: 10.1016/j.ijrobp.2013.06.2059
9. Chan P, Dinniwell R, Haider MA, Cho YB, Jaffray D, Lockwood G, et al. Inter- and intrafractional tumor and organ movement in patients with cervical cancer undergoing radiotherapy: a cinematic-MRI point-of-interest study. Int J Radiat Oncol Biol Phys. (2008) 70:1507e1515. doi: 10.1016/j.ijrobp.2007.08.055
10. Beadle BM, Jhingran A, Salehpour M, Sam M, Iyer RB, Eifel PJ. Cervix regression and motion during the course of external beam chemoradiation for cervical cancer. Int J Radiat Oncol Biol Phys. (2009) 73:235e241. doi: 10.1016/j.ijrobp.2008.03.064
11. Jadon R, Pembroke CA, Hanna CL, Palaniappan N, Evans M, Cleves AE, et al. A systematic review of organ motion and image-guided strategies in external beam radiotherapy for cervical cancer. Clin Oncol. (2014) 26:185e196. doi: 10.1016/j.clon.2013.11.031
12. Tyagi N, Lewis JH, Yashar CM, Vo D, Jiang SB, Mundt AJ, et al. Daily online cone beam computed tomography to assess interfractional motion in patients with intact cervical cancer. Int J Radiat Oncol Biol Phys. (2011) 80:273e280. doi: 10.1016/j.ijrobp.2010.06.003
13. Yang D, Kim H, Green O, Henke L, Gu B, Cai B, et al. Co-60 MR guided adaptive radiation treatment improves target coverage and organs-at-risk sparing: dosimetric analysis of 1185 adaptive fractions and 5 years’ experience (Conference Abstract). Int J Radiat Oncol Biol Phys. (2020) 108:e300. doi: 10.1016/j.ijrobp.2020.07.718
14. Lim-Reinders S, Keller BM, Al-Ward S, Sahgal A, Kim A. Online adaptive radiation therapy. Int J Radiat Oncol Biol Phys. (2017) 99:994–1003. doi: 10.1016/j.ijrobp.2017.04.023
15. Hunt A, Hansen VN, Oelfke U, Nill S, Hafeez S. Adaptive radiotherapy enabled by MRI guidance. Clin Oncol. (2018) 30:711e719. doi: 10.1016/j.clon.2018.08.001
16. White IM, Mcquaid D, Goodwin E, Lalondrelle S. Image guided adaptive external beam radiotherapy (EBRT) planning for cervical cancer - a comparison of offline, online and MRI-guided techniques to reduce organ at risk (OAR) dose using a dose accumulation model (Abstract). Int J Radiat Oncol Biol Phys. (2019) 105:S250eS251. doi: 10.1016/j.ijrobp.2019.06.373
17. Belhadj H, Berek J, Bermudez A, Bhatla N, Cain J, Denny L, et al. FIGO staging for carcinoma of the vulva, cervix, and corpus uteri. Int J Gynaecol Obstet. (2014) 125:97–8. doi: 10.1016/j.ijgo.2014.02.003
18. William JS, Loren KM, Penny A, Carien C, Jennifer D, David G, et al. Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy in postoperative treatment of endometrial and cervical cancer. Int J Radiat Oncol Biol Phys. (2007) 71. doi: 10.1016/j.ijrobp.2007.09.042
19. Yock AD, Ahmed M, Ayala-Peacock D, Chakravarthy AB, Price M. Initial analysis of the dosimetric benefit and clinical resource cost of CBCT-based online adaptive radiotherapy for patients with cancers of the cervix or rectum. J Appl Clin Med Phys. (2021) 22:210–21. doi: 10.1002/acm2.13425
20. Alongi F, Rigo M, Figlia V, Cuccia F, Giaj-Levra N, Nicosia L, et al. 1.5 T MR-guided and daily adapted SBRT for prostate cancer: feasibility, preliminary clinical tolerability, quality of life and patient-reported outcomes during treatment. Radiat Oncol. (2020) 15:69. doi: 10.1186/s13014-020-01510-w
21. Raaymakers BW, Jurgenliemk-Schulz IM, Bol GH, Glitzner M, Kotte ANTJ, van Asselen B, et al. First patients treated with a 1.5 T MRI-Linac: clinical proof of concept of a high-precision, highfield MRI guided radiotherapy treatment. Phys Med Biol. (2017) 62:L41–50. doi: 10.1088/1361-6560/aa9517
22. Henke L, Kashani R, Robinson C, Curcuru A, DeWees T, Bradley J, et al. Phase I trial of stereotactic MR-guided online adaptive radiation therapy (SMART) for the treatment of oligometastatic or unresectable primary Malignancies of the abdomen. Radiother Oncol. (2018) 126:519–26. doi: 10.1016/j.radonc.2017.11.032
23. Paulson ES, Ahunbay E, Chen X, Mickevicius NJ, Chen GP, Schultz C, et al. 4D-MRI driven MR-guided online adaptive radiotherapy for abdominal stereotactic body radiation therapy on a high field MR-Linac: Implementation and initial clinical experience. Clin Transl Radiat Oncol. (2020) 23:72–9. doi: 10.1016/j.ctro.2020.05.002
24. Green OL, Henke LE, Hugo GD. Practical clinical workflows for online and offline adaptive radiation therapy. Semin Radiat Oncol. (2019) 29:219–27. doi: 10.1016/j.semradonc.2019.02.004
25. Liugang G, Kai X, Xiaojin W, Zhengda L, Chunying L, Jiawei S, et al. Generating synthetic CT from low-dose cone-beam CT by using generative adversarial networks for adaptive radiotherapy. Radiat Oncol (London England). (2022) 16:1, 202. doi: 10.1186/s13014-021-01928-w
26. Boulanger M, Nunes J, Chourak H, Largent A, Tahri S, Acosta O, et al. Deep learning methods to generate synthetic ct from mri in radiotherapy: a literature review. Physica medica: PM: an Int J devoted to Appl Phys to Med biology: Off J Ital Assoc Biomed Phys (AIFB). (2021) 89:265–81. doi: 10.1016/j.ejmp.2021.07.027
27. Tyagi N, Fontenla S, Zelefsky M, Chong-Ton M, Hunt M. Clinical workflow for mr-only simulation and planning in prostate. Radiat Oncol. (2017) 12(1). doi: 10.1186/s13014-017-0854-4
28. Lei Y, Harms J, Wang T, Liu Y, Shu HK, Jani AB, et al. MRI-only based synthetic ct generation using dense cycle consistent generative adversarial networks. Med Phys. (2019) 46:3565–81. doi: 10.1002/mp.13617
29. Yoon SW, Lin H, Alonso-Basanta M, Anderson N, Apinorasethkul O, Cooper K, et al. Initial evaluation of a novel cone-beam CT-based semi-automated online adaptive radiotherapy system for head and neck cancer treatment - A timing and automation quality study. Cureus. (2020) 12:e9660. doi: 10.7759/cureus.9660
30. Oh S, Stewart J, Moseley J, Kelly V, Lim K, Xie J, et al. Hybrid adaptive radiotherapy with on-line MRI in cervix cancer IMRT. Radiother Oncol. (2014) 110:323–8. doi: 10.1016/j.radonc.2013.11.006
31. Huang Y, Wang H, Li C, Hu Q, Liu H, Deng J, et al. A preliminary simulation study of dose-guided adaptive radiotherapy based on halcyon MV cone-beam CT images with retrospective data from a phase II clinical trial. Front Oncol. (2020) 10:574889. doi: 10.3389/fonc.2020.574889
32. Jong RD, Visser J, Wieringen NV, Wiersma J, Bel A. Feasibility of conebeam ct-based online adaptive radiotherapy for neoadjuvant treatment of rectal cancer. Radiat Oncol. (2021) 16(1). doi: 10.1186/s13014-021-01866-7
33. Jong RD, Crama KF, Visser J, Wieringen NV, Wiersma J, Geijsen ED, et al. Online adaptive radiotherapy compared to plan selection for rectal cancer: quantifying the benefit. Radiat Oncol. (2020) 15:1–9. doi: 10.1186/s13014-020-01597-1
34. Qin A, Sun Y, Liang J, Yan D. Evaluation of online/offline image guidance/adaptation approaches for prostate cancer radiation therapy. Int J Radiat Oncol Biol Phys. (2015) 91:1026–33. doi: 10.1016/j.ijrobp.2014.12.043
35. Dunlop A, Mitchell A, Tree A, Barnes H, Bower L, Chick J, et al. Daily adaptive radiotherapy for patients with prostate cancer using a high field MR-linac: Initial clinical experiences and assessment of delivered doses compared to a C-arm linac. Clin Transl Radiat Oncol. (2020) 23:35–42. doi: 10.1016/j.ctro.2020.04.011
36. O’Reilly FH, Shaw W. A dosimetric evaluation of IGART strategies for cervix cancer treatment. Phys Med. (2016) 32:1360e1367. doi: 10.1016/j.ejmp.2016.06.003
37. Murphy MJ, Balter J, Balter S, BenComo JJ, Das IJ, Jiang SB, et al. The management of imaging dose during image-guided radiotherapy: report of the aapm task group 75. Med Phys. (2007) 34(1). doi: 10.1118/1.2775667
38. Steiner E, Stock M, Kostresevic B, Ableitinger A, Jelen U, Prokesch H, et al. Imaging dose assessment for IGRT in particle beam therapy. Radiother Oncol. (2013) 109:409–13. doi: 10.1016/j.radonc.2013.09.007
39. McComas KN, Yock A, Darrow K, et al. Online adaptive radiation therapy and opportunity cost. Adv Radiat Oncol. (2022) 8:101034. doi: 10.1016/j.adro.2022.101034
Keywords: online adaptive radiation therapy, cervical cancer, FBCT-Linac, image-guide radiation therapy, dosimetry, survival follow-up
Citation: Jiang D, Yang C, Sun S, Wang D, Xiao Z, Hu J, Mei Z, Xie C, Liu H, Qiu H and Wang X (2024) First implementation and results of online adaptive radiotherapy for cervical cancer based on CT-Linac combination. Front. Oncol. 14:1399468. doi: 10.3389/fonc.2024.1399468
Received: 12 March 2024; Accepted: 25 October 2024;
Published: 14 November 2024.
Edited by:
Li-Sheng Geng, Beihang University, ChinaReviewed by:
Thomas Samuel Ram, Christian Medical College and Hospital, IndiaRuijie Yang, Peking University Third Hospital, China
Copyright © 2024 Jiang, Yang, Sun, Wang, Xiao, Hu, Mei, Xie, Liu, Qiu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyong Wang, d2FuZ3hpYW95b25nQHpuaG9zcGl0YWwuY24=; Hui Qiu, cWl1aHVpem55eUB3aHUuZWR1LmNu
†These authors have contributed equally to this work