 Qiuhua Zhang
Qiuhua Zhang Yanan Gao
Yanan Gao Wenjun Wang3
Wenjun Wang3 Xiaoguang Zhao
Xiaoguang Zhao Jiabin Yu
Jiabin Yu Huiming Huang
Huiming Huang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol., 19 July 2024
Sec. Cancer Epidemiology and Prevention
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1393902
This article is part of the Research TopicMechanistic Roles of Exercise on Cancer Progression, Recurrence and Survival OutcomesView all articles
Objective: The purpose of this study is to conduct a systematic review to assess the effects of different forms of resistance exercises (resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises) on physical fitness, quality of life (QOL), and fatigue of patients with cancer.
Methods: We conducted a systematic review using the Cochrane Handbook for Systematic Reviews of Interventions guidelines. We searched PubMed, Web of Science, and Scopus databases for the studies from the establishment of the database to September 2023, including randomized controlled trials and clinical trials that evaluated the effects of different resistance exercise on physical fitness, QOL, and fatigue in all patients with cancer. Two reviewers independently assessed the quality of all the included studies using the Cochrane Handbook for Systematic Reviews of Interventions and MINORS scale. We divided the intervention into three types: resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises.
Results: In total, 48 studies (3,843 participants) met the inclusion criteria. The three exercise intervention forms have significant effects on physical fitness and QOL, but the improvement effect on fatigue is not clear. A total of 34 studies reported significant and beneficial effects of resistance exercise on physical fitness across all types of cancer. There were 28 studies that reported significant or borderline improvement effects of resistance on QOL, and only 10 studies reported significant effects of resistance exercise interventions on fatigue improvement in patients with cancer.
Conclusions: Resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises all have a positive effect on improving fitness and QOL in patients with cancer. Resistance exercise has an advantage in improving muscle strength, while combined resistance exercise has an advantage in improving QOL; however, there are no consistent findings in improving fatigue, although low-intensity resistance exercise is effective.
Systematic review registration: www.inplasy.com, identifier INPLASY2023110034.
Cancer is the second leading cause of death worldwide (1). As the number of cancer survivors and their longevity increase, long-term health issues related to cancer and its treatment are becoming more critical (2). However, patients with cancer receiving treatment often suffer from nausea, insomnia, diarrhea, and other treatment-related symptoms and side effects (3). Regardless of their cancer type, patients report decreased physical fitness (4, 5), fatigue, and reduced quality of life (QOL) (6). Consequently, there is growing interest in the impact of exercise interventions on patients with cancer. Increasing evidence shows that exercise interventions can significantly improve the physical and psychological functioning of patients with cancer, including their QOL (7, 8). Although the American College of Sports Medicine (ACSM) recommends exercise during cancer treatment, it does not provide specific guidelines on which type and intensity of physical exercise are most effective during chemotherapy or treatment (9).
Evidence suggests that moderate weekly physical activity improves cancer survivors’ QOL, physical activity levels, physical fitness, body mass index (BMI), and hormone levels (10–12), However, research on the effects of resistance exercise on cancer is still limited. Most systematic reviews to date have focused on breast cancer research. One study showed that guideline-compliant aerobic exercise can reduce breast cancer mortality and all-cause mortality compared with patients who do not meet physical activity guidelines (13). A 2013 meta-analysis assessed the effect of exercise training on the QOL of breast cancer survivors (14), but this analysis only included randomized controlled trials (RCTs) up to 2013. Zhang et al. conducted a comprehensive review of the impact of exercise on the QOL of patients with breast cancer, including various exercise interventions, but limited to breast cancer and a single QOL indicator (15). Although there was a study on the effect of exercise intervention on all types of cancer, it did not specify the effects on specific cancers and included fewer indicators in the results (16). Neo- and adjuvant therapies have increased the survival rate among patients with cancer (17, 18). However, as life expectancy increases, the side effects of long-term treatment persist and significantly impact the health and QOL of patients with cancer. Consequently, adverse effects on physical health indicators, including cardiorespiratory fitness and strength, are often observed clinically (19). Chemotherapy or radiation therapy often leads to dysfunction and reduced QOL in patients with cancer. Exercise has been shown to improve factors such as functional capacity and QOL in patients undergoing chemotherapy, therapy, or combination therapy (20). Increasing evidence suggests that regular physical activity, such as 3–5 h of moderate-intensity walking per week, reduces the risk of cancer-specific and all-cause mortality by 30%–50% compared with inactive patients with cancer (21). However, many studies on the effects of exercise programs on patients with cancer during radiation therapy have focused primarily on breast cancer cases (22). Fewer studies have investigated structured exercise-based rehabilitation programs to improve fitness and QOL in patients with various types of cancer, as well as programs combining resistance training with aerobic and other exercises. Recently, there has been a gradual increase in experimental studies of exercise interventions for patients with cancer. The effects of aerobic exercise on cancer are well established, and resistance training is the only known non-drug intervention that can improve skeletal muscle quality, strength, and prevent muscle loss (23). Therefore, combining resistance exercise with aerobic exercise has been proposed as a multidimensional intervention for patients with cancer to explore new methods of exercise-based therapy (24). However, evidence from experimental studies on resistance exercise interventions in patients with cancer is still limited, and some results are controversial. For example, some studies have found significant improvements in the QOL of patients with cancer after resistance exercise interventions (25–28), while others have reached different or even opposite conclusions (29–31). Although exercise has been proven to be effective in the treatment and rehabilitation of patients with cancer, comparison between different types of exercise and cancer is still relatively lacking.
Therefore, we conducted a systematic review of all experimental studies to date with the aim of exploring the effects of resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises on physical fitness, QOL, and fatigue in patients with cancer. Our goal is to provide a new reference value for non-drug intervention in the treatment of clinical patients with cancer.
We registered the review protocol in INPLASY (registration number INPLASY2023110034) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines and synthesis without meta-analysis guidelines.
We conducted comprehensive searches in PubMed, Web of Science, Scopus, and other databases comprehensively, and retrieved other potentially relevant studies from the included references. We included all published English literature from the inception of each database to 1 September 2023.
Our search strategy included Medical Subject Headings (Mesh) related to cancer and resistance training, along with free text terms (Supplementary Table 1).
Two authors independently conducted the retrieval. All potentially relevant studies meeting the predetermined inclusion criteria were included in the review. The third author resolved any disagreement arising in the retrieval process.
The included studies comprised RCTs and clinical intervention trials (non-RCT), including self-control and other quasi-experimental studies, with the language limited to English. Animal experiments and observational studies were excluded.
Participants were adults diagnosed with cancer, either undergoing treatment or having completed treatment, and older than 18 years old. Patients with severe cardiovascular disease, sports system disease, or weakness that prevented participation in the exercise program were excluded.
The inclusion criteria were as follows: (1) the intervention group received resistance exercise intervention, resistance exercise combined with aerobic exercise, or resistance exercise combined with other forms of exercise. (2) The control group did not receive any form of exercise intervention, including blank control and diet control. (3) Studies with a single-group pre- and post-control design, where exercise training is part of multiple interventions (e.g., combined with protein supplementation), were not excluded. Studies in which exercise was part of the control group were excluded.
The results of these included studies require reporting physical fitness, fatigue, QOL, or one of the outcome indicators. Studies that did not report any of these outcomes were excluded.
Two authors searched the aforementioned electronic database using the developed retrieval strategy. The titles and abstracts of all retrieved articles were independently screened by the two authors, and duplicates were removed. Then, according to the inclusion criteria, two authors independently reviewed the full text of articles that might be included in the study. All disputes arising in this process were settled by the third author through consultation. Finally, we extracted data from the selected studies using a predefined table. The extracted data mainly included the following: author, year, country, study name, study design, study population, sample size, mean age, proportion of female patients, type of exercise, frequency of exercise, duration of exercise, intensity of exercise, measurement instruments, comparative results, and description of results.
Two authors independently completed the quality assessment of the included studies. The quality assessment of RCTs followed the Cochrane Handbook for Systematic Reviews of Interventions (32). The quality evaluation criteria included seven parts: random sequence generation, distribution hiding, blinding of participants, blinding of researchers, blinding of result evaluation, incomplete result data, and selective report of results and other biases. According to the Cochrane Handbook, each evaluation item was classified into three levels: low risk, unclear risk, and high risk. The purpose was to evaluate selection, performance loss, and detection deviation through the possible bias risk of RCT design, trial, and outcome evaluation, and to understand the internal authenticity of the experimental study. The quality of non-RCTs was evaluated according to the MINORS criteria (33), which include 12 evaluation items, each scored from 0 to 2 points. The highest score of the first eight items for the study without the control group was 16 points; The last four items and the first eight items are for the study with the control group, and the maximum score is 24 points in total. 0 indicates no report; 1 point means that the report is reported but the information is not sufficient; 2 points means that the report has been reported and sufficient information has been provided.
Because of the heterogeneity of measurement tools in the included studies, the expression of the outcome indicators was inconsistent; thus, a meta-analysis was not performed. Therefore, in accordance with the Cochrane Handbook for Systematic Reviews of Interventions, a systematic evaluation and qualitative analysis were conducted on the included studies.
We categorized studies according to three outcomes—physical fitness, QOL, and fatigue. Figure 1 described changes in relevant indicators after resistance training intervention. The research under each outcome was categorized into three types of exercise: resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises.
Figure 1 A conceptual framework for the impact of resistance training on patients with cancer.
Figure 2 shows the complete process of literature screening. A total of 7,064 articles were retrieved from the database. Following the removal of duplicate literature and the screening of article titles and abstracts, two authors independently assessed the full texts of the remaining 202 potential articles that might meet the inclusion criteria. Following the exclusion of studies that did not meet the inclusion criteria, 48 articles were included in the final study (25–31, 34–72) (see Supplementary Table 2)
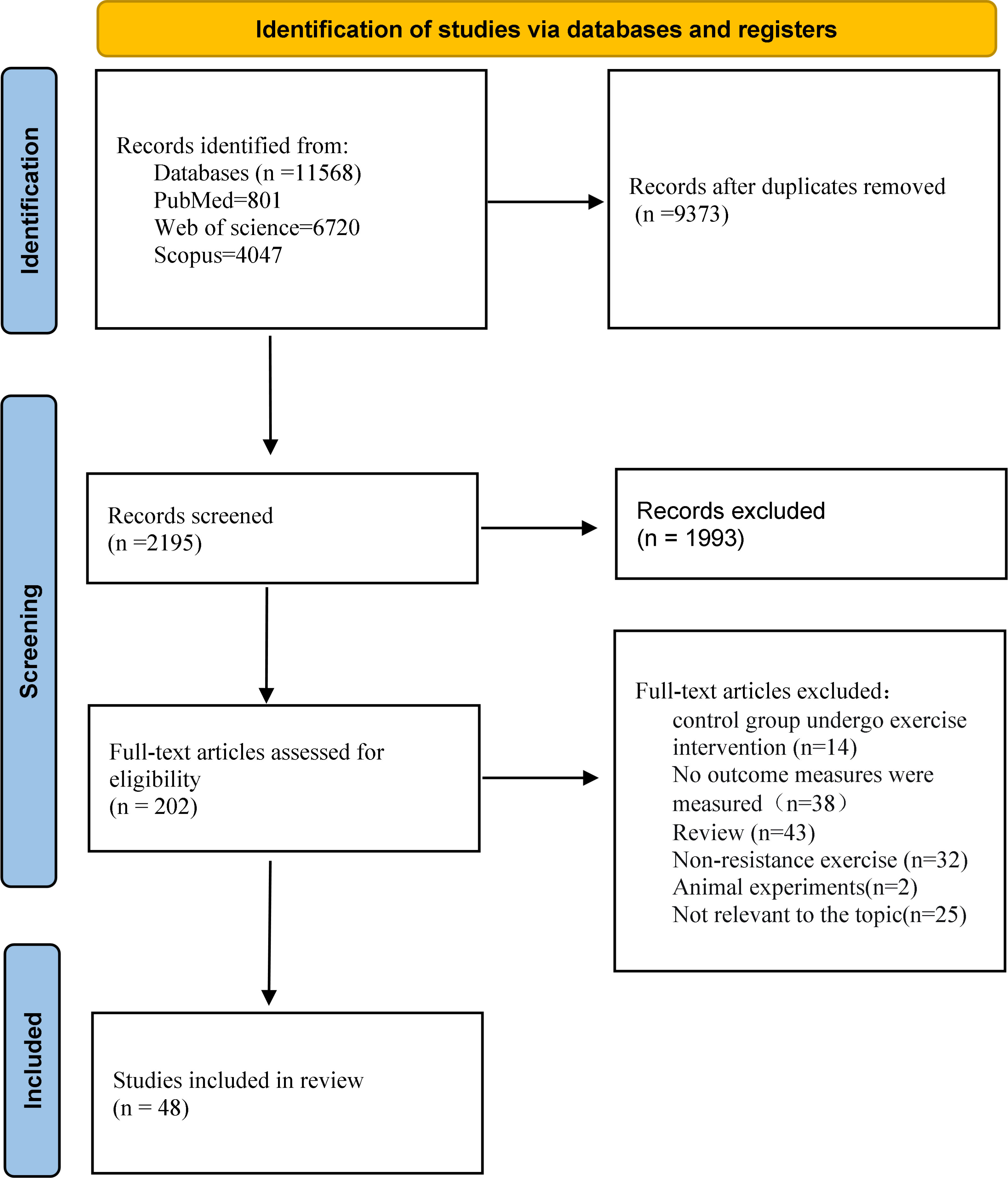
Figure 2 Flowchart of the selection of trials.
A total of 48 studies were conducted, involving 3,843 subjects from different countries and regions. Of the 48 studies, 13 were from the United States (25, 31, 34–36, 39, 54, 57–60, 62, 66), 9 were from Denmark (42, 47, 64, 65, 69, 70, 72–74), 5 were from China (26, 28, 48, 50, 63), 3 were from Australia (27, 29, 56), 3 were from Canada (44, 45, 71), 3 were from Germany (37, 40, 55), 2 were from Belgium (30, 43), 2 were from the Netherlands (51, 61), 2 were from Norway (46, 53), 2 were from Spain (38, 52), 1 was from Greece (68), 1 was from Korea (49), 1 was from Turkey (67), and 1 was from Brazil (41).
The studies included in this review encompass a wide range of cancer types, including breast, rectal, head and neck, prostate, lung, nasopharyngeal, and other cancers. A total of 21 studies were conducted on breast cancer (25, 31, 35–41, 57, 60, 66–68), followed by 6 studies on prostate cancer (27, 30, 46, 51, 56, 62), 4 studies on head and neck cancer (34, 47, 55, 59), 4 studies on gastrointestinal cancer (26, 29, 43, 63), 2 studies on lung cancer (44, 48), and 1 study on nasopharyngeal carcinoma (50). The remaining 10 studies were not limited to specific cancers (28, 45, 53, 58, 61, 69, 71–74).
The frequency, form, intensity, and duration of exercise interventions varied across the studies included in the systematic review. In most trials, two to three times per week was the usual frequency of exercise. Three main forms of exercise interventions were included, with 25 studies including resistance exercise interventions (26–28, 31, 35, 37, 39–41, 43, 49, 51, 55, 62, 66) and 11 studies combining resistance and aerobic interventions (25, 29, 34, 48, 52, 53, 56, 60, 67, 69, 71); the remaining 12 studies intervened with resistance exercise combined with other forms of exercise (including interval exercise, flexibility, relaxation, and massage) (36, 38, 42, 45, 57–59, 61, 68, 72–74). One study adopted high-intensity intermittent exercise combined with resistance as part of exercise intervention (61), two studies combined resistance, aerobic, and flexibility as part of exercise intervention (57, 68), and two studies included stretching and massage relaxation exercises (45, 73).
With regard to the report on the main results, 36 studies reported on physical fitness-related indicators, 40 studies reported on QOL-related indicators, and only 19 studies reported on fatigue-related outcomes. While the majority of studies included a common resistance exercise program, comprising chest press, leg press, chest extension, leg extension, knee extension, and leg curl, five studies did not mention a specific intervention exercise program (37, 43, 57, 68, 69). The duration of the studies ranged from 5 weeks to 52 weeks, but the majority of the studies had a duration of 12 weeks.
Upper and lower extremity muscle strength is the primary indicator of physical fitness when it comes to the measurement of research outcomes. The main testing instruments were the 1-repetition maximum test, the 8-repetition maximum test, and the 10-repetition maximum test. The results are expressed as the maximum weight that can be lifted in one repetition. Other metrics include VO2max, 6MWD, and others. The majority of the studies employed the EORTC QLQ-C30 as the QOL test tool, while others used the Functional Assessment of Cancer Therapy-General (FACT-G) and the 36-Item Short Form Survey (SF-36); the results were assessed by questionnaire scores. Tests of fatigue in patients with cancer include Functional Assessment of Cancer Therapy-Fatigue (FACT-F), Brief Fatigue Inventory (BFI), Multidimensional Fatigue Inventory (MFI), and Piper Fatigue Scale (PFS), and the results are also expressed in the form of questionnaire scores.
The characteristics of the included literature are shown in Table 1.
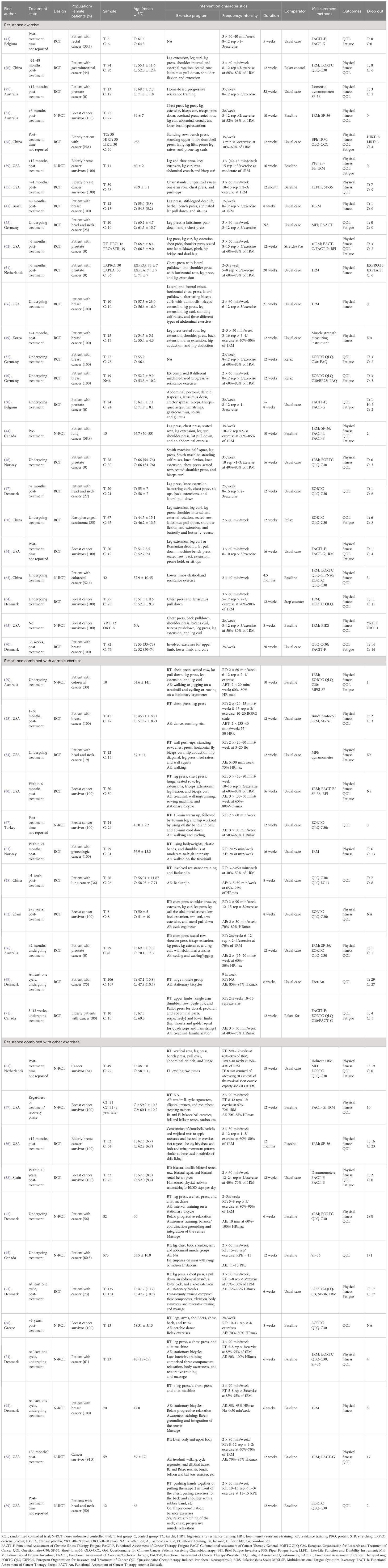
Table 1 Characteristics of studies included in the systematic review.
A total of 48 studies were included in the analysis, comprising 32 RCTs and 16 non-randomized controlled intervention trials (N-RCTs). The results of the assessment of the quality of the RCT literature are presented in Figure 3. In summary, the risk of bias for the included studies was low. The majority of the risk of bias was attributable to issues related to blinding of study subjects or investigators, blinding of outcome measures, and incomplete outcome follow-up. Moreover, the majority of researchers provided comprehensive descriptions of the methods employed for the generation and distribution of random sequences. Because of the nature of the intervention and the subjectivity of outcome assessment instruments, the implementation and execution of blind methods become more challenging. The results of the quality assessment of the 16 experimental studies of N-RCTs are presented in Table 2. Only one of the studies had a control group, and the rest were self-controlled. Most of the studies scored above 12 points, except for two studies that scored low (below 11 points).

Figure 3 (A) Quality assessment of selected studies. (B) Risk of bias graph and summary.
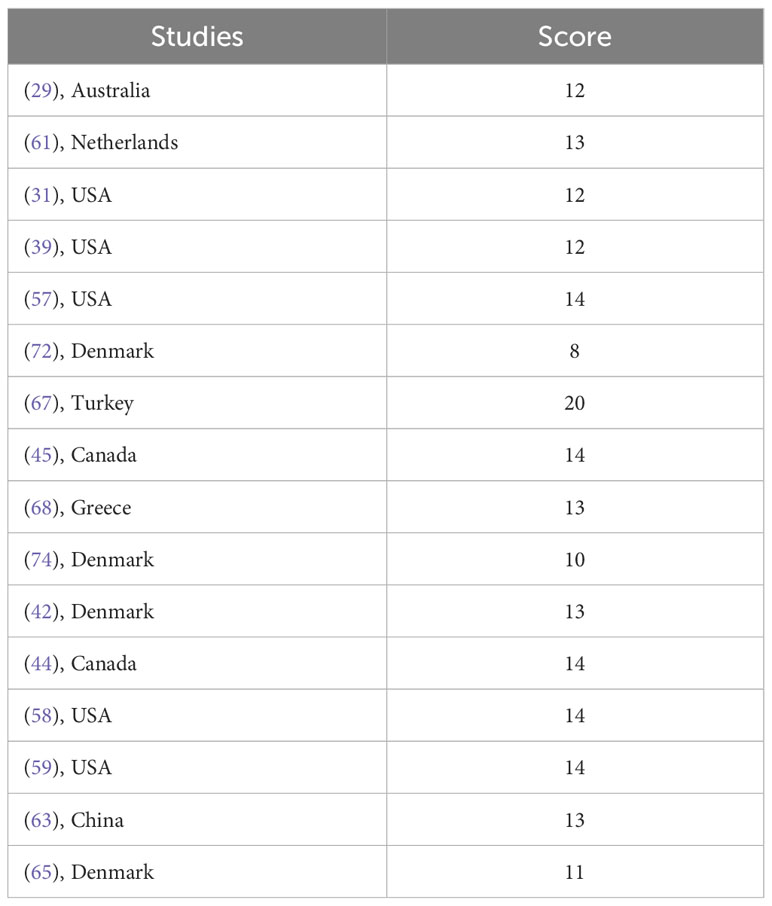
Table 2 MINORS score for non-RCTs.
Table 3 shows the changes in physical fitness after exercise interventions in patients with cancer in various research experiments, and 36 studies have investigated the effect of resistance on physical fitness in patients with cancer. There are many evaluation indexes of physical fitness, including but not limited to muscle strength, VO2max, and 6MWD, among others. Muscle strength, such as leg pressure and chest pressure, is the primary evaluation indicator of physical fitness.
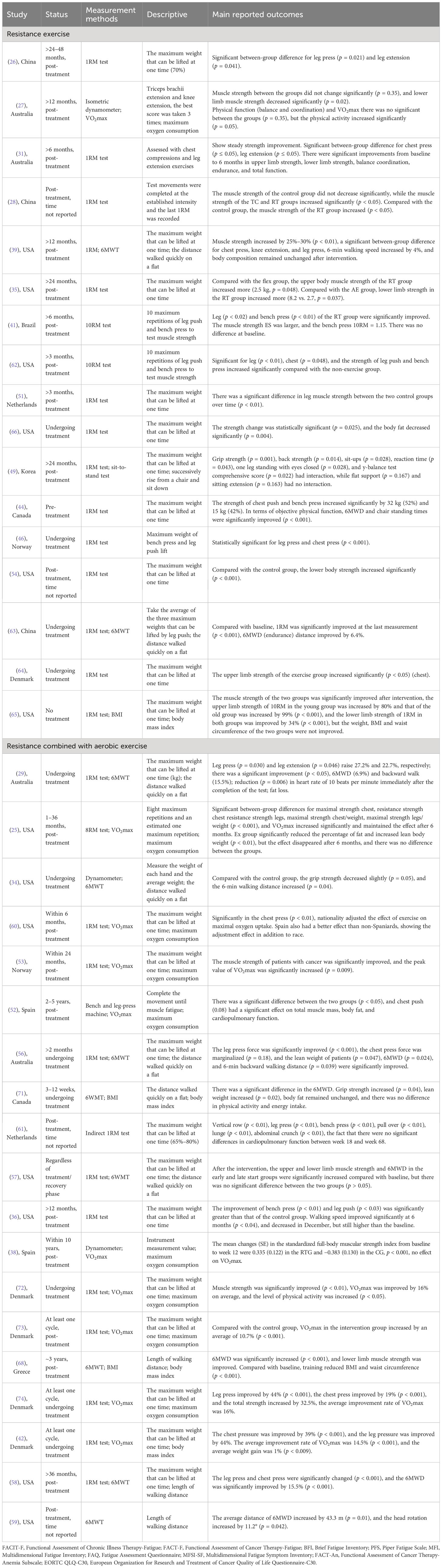
Table 3 Effect of resistance exercise on physical fitness of patients with cancer.
Seventeen studies reported the effect of resistance exercise intervention on physical fitness in patients with cancer, 16 studies demonstrated positive intervention effects of resistance exercise in patients with cancer, while 1 study reported reduced muscle strength but increased physical activity levels (27). Of these 16 studies, 8 reported significant improvements in leg press and chest press in patients with cancer compared to controls after exercise interventions (26, 31, 39, 41, 44, 46, 62, 64). Simonavice et al. (31) evaluated the effect of 6-month resistance training on physical fitness and QOL of patients with breast cancer. The results demonstrated a consistent and progressive enhancement in patient strength. Furthermore, significant improvements in balance, coordination, endurance, and overall function were observed in the study participants from baseline to month 6. Serra et al. (39) investigated the effects of 16 weeks of progressive resistance training on inflammation, fatigue, and physical functioning in patients with breast cancer under the supervision of an exercise physiologist. The results showed that resistance training not only improved muscle strength, but also resulted in a 4% increase in 6-min walking speed. The study found no significant changes in body composition compared to the control group. Peddle-McIntyre et al. (44) reported the feasibility and preliminary efficacy of progressive resistance exercise training (PRET) intervention for lung cancer survivors. The results showed significant therapeutic effects in objective physical, 6MWD, and chair standing. The results of the remaining eight studies (28, 35, 49, 51, 54, 63, 65, 66) not only included significant improvements in physical fitness, but Cheng et al. (28) also explored the effects of different intensities of tai chi (TC) and resistance exercise on fatigue and QOL in middle-aged and elderly Chinese patients with cancer. The results demonstrated that resistance exercise was more effective than TC in enhancing muscle strength, but TC was more efficacious than resistance exercise in improving sleep quality and mental health. In a study by Winters et al. (35), resistance was compared to the relaxation and aerobic exercise groups, respectively. There was a greater increase in upper limb muscle strength compared to the relaxation group, and a greater increase in limb muscle strength compared to the aerobic group; the lower limb strength increased more. Lee et al. (49) compared the effects of improvements in various aspects of physical fitness, with significant results being achieved in grip strength, back strength, sit-ups, reaction time, one-legged closed-eye stand, and Y-balance. Benton et al. (65) found that the younger group (40–59 years old) showed better improvement in upper limb strength than the older group (60–80 years old) and that resistance had no effect on body weight, BMI, or waist circumference. Moreover, of all the studies that have investigated the effects of resistance exercise on physical fitness in patients with cancer, a total of 11 studies have been conducted in which patients have participated in exercise tests following the completion of chemotherapy or radiotherapy; of these studies, 4 studies focused on breast cancer, 3 focused on prostate cancer, 1 focused on gastrointestinal cancer, and 4 focused on early-stage cancer. The results demonstrated that the resistance exercise intervention led to a favorable improvement in the study participants who had completed their cancer treatment. Most physical fitness indicators in patients with all types of cancer who completed treatment, including chest press and leg extension, exhibited statistically significant results. In addition, five studies had subjects who were still undergoing cancer treatment at the time of the exercise intervention: two studies on lung cancer, one on prostate cancer, one on lung cancer, and one on colorectal cancer. The findings of the study indicate that resistance exercise is an efficacious intervention for enhancing physical fitness in individuals undergoing cancer treatment. Nevertheless, a study was conducted on patients with breast cancer who underwent the exercise intervention without any additional treatment (65). However, it was demonstrated that, despite the absence of any therapeutic intervention, the implementation of an exercise regimen would yield comparable statistical benefits in terms of enhanced physical fitness.
Eight studies reported the effect of resistance exercise combined with aerobic exercise on physical fitness in patients with cancer. In comparison to the control group, most studies reported that resistance exercise combined with aerobic exercise had a positive effect on the physical fitness of patients with cancer (29, 52, 53, 56). In addition to the improvement of muscle strength, the studies also demonstrated significant effects, including the improvement of VO2max and 6MWD, the increase of muscle mass, the increase of lean weight, and the decrease of body fat rate. In the other four studies, Xiao et al. (34) reported the effect of resistance exercise combined with aerobic exercise intervention on patients with head and neck cancer undergoing radiotherapy. After the intervention, there was a slight decrease in grip strength but an increase in 6-min walk distance compared to the control group. Casla et al. (25) assessed the effect of aerobic and resistance exercise intervention on cardiorespiratory fitness in patients with early-stage breast cancer. The results showed significant increases in maximal oxygen capacity and muscle strength, which were also evident after 6 months of follow-up. Although there was an increase in lean body mass and a decrease in percent fat at the end of the intervention, the effects disappeared after follow-up. Dieli-Conwright et al. (60) showed that Hispanics had increased muscle strength and better VO2max improvement and reported the race-modifying role of exercise interventions in cancer treatment. Adeline et al. (71) explored the feasibility of combination of aerobic exercise and resistance exercise on the physical ability of elderly patients with cancer. The results showed that resistance exercise and aerobic exercise had significant effects on grip strength, 6-min walking distance, and lean weight of elderly patients with cancer, but had no effect on physical activity and energy intake. In these studies, subjects in four studies completed treatment related to cancer, and subjects in the other four studies were undergoing treatment for cancer. The studies that completed treatment included three on breast cancer and one on gynecologic cancer. Those undergoing treatment included one study on head and neck cancer, one on prostate cancer, one on rectal cancer, and one on early-stage cancer. The results demonstrated a significant impact on the enhancement of physical fitness through the integration of resistance exercise with aerobic training, both during the course of cancer treatment and across various types of patients with cancer. Statistically significant differences were observed between groups.
Eleven studies reported the effects of resistance exercise combined with other exercises on the physical fitness in patients with cancer. Four studies reported the significant effect of an exercise intervention on muscle strength and walking distance in patients with cancer (36, 57, 58, 68); Winters-Stone et al. (36) reported that although there was a decrease in 6MWD at 12 months, it was still higher than baseline values. Andrioti et al. (68) explored the effect of home-based tele-exercise training intervention on physical and mental health indicators in breast cancer survivors. In addition to the increase in lower limb muscle strength and 6MWD, they also found that exercise could reduce the BMI and waist circumference of patients. Six studies reported the effect of resistance exercise combined with other exercises interventions on muscle strength and VO2max of patients with cancer, with only two studies reporting no effect on VO2max (38, 61) and the other four studies reporting significant improvements in muscle strength and VO2max (42, 72–74). Felser et al. (59) explored the feasibility and impact of low and moderate-intensity exercise intervention on physical fitness and QOL in patients with head and neck cancer. They used 6MWD and head rotation as primary outcome indicators of physical function. The results showed significant changes in both. During the cancer treatment phase, subjects in seven studies participated in exercise interventions after completing the relevant treatment, and subjects in three studies were enrolled in an exercise testing program during cancer treatment and had completed at least one treatment cycle. Three studies were focused on breast cancer, one focused on head and neck cancer, and the remaining six studies did not target a specific cancer. The results of the 10 studies on the effects of resistance training combined with other exercise interventions on the physical functioning of patients with cancer demonstrated that the majority of the indices related to muscle fitness exhibited a significant improvement following the exercise interventions in comparison to the control group. However, only one study indicated that there was no significant change in VO2max following the exercise interventions. Soriano−Maldonado et al. (38) assessed the effects of 12-week supervised resistance training combined with home-based physical activity on physical fitness, cancer-related fatigue, depressive symptoms, QOL, and life satisfaction in female breast cancer survivors. The results of the study indicated that the exercise intervention significantly enhanced muscle strength in the upper and lower extremities, as well as the entire body, in patients with cancer. However, the patients reported no significant improvement in other health indicators, such as VO2max. Nevertheless, a study on breast cancer included subjects who had completed cancer treatment as well as those in the treatment stage. In 2018, Foley et al. (57). conducted a study investigating the effects of a 12-week community-based multimodal exercise program on physical function in breast cancer survivors. The results show that regardless of start delay, meaningful improvements in physical fitness were found after completing the community-based multimodal exercise program, but there was no significant difference between the two groups.
Table 4 shows the changes in QOL of patients with cancer after resistance exercise interventions across studies. A total of 40 studies reported the effect of resistance exercise interventions on the QOL of patients with various types of cancer.
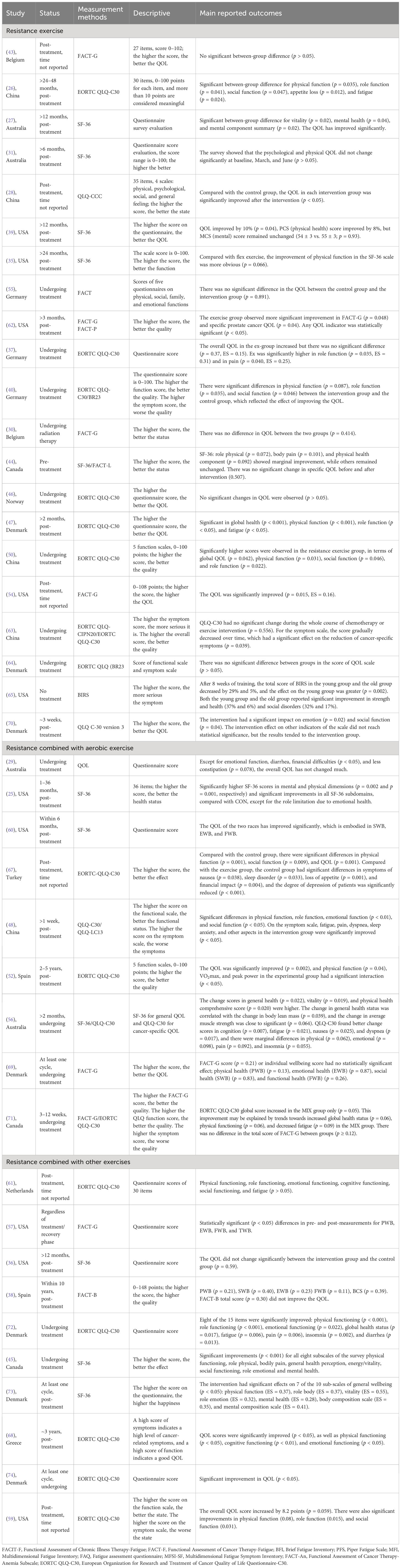
Table 4 Effect of resistance exercise intervention on the QOL of patients with cancer.
A total of 21 studies reported the effect of resistance exercise interventions on the QOL of patients with cancer. The results of seven studies (30, 31, 37, 43, 46, 55, 64) indicated that there was no significant change in the QOL of patients with cancer after exercise interventions compared to the control group. In their study, Simonavice et al. (31) assessed the QOL and psychological wellbeing of patients with breast cancer using the SF-36. The results demonstrated no significant change at baseline, in March, or in June. The best study conducted by Steindorf et al. (37) revealed that following the intervention, the overall QOL in the exercise group exhibited an increase solely in terms of role functioning and pain, with no discernible between the control and excise intervention groups. Ten studies have reported the effect of resistance exercise interventions on participants’ QOL (26–28, 39, 40, 47, 50, 54, 62, 65). Dawson et al. (62) explored the effects of 12 weeks of resistance training and protein supplementation on the body composition in patients with prostate cancer treated with ADT. The results showed improvements in FACT-G and FACT-P scores as well as significant improvements in outcome measures related to QOL. A study by Benton et al. (65) showed that resistance exercise had an effect on improving QOL in both young and old patients with breast cancer. However, the improvement in QOL was relatively more pronounced in young patients with breast cancer, reflecting the differential impact of age on QOL improvement. The other four studies (35, 44, 63, 70) did not directly conclude that resistance exercise improves QOL, but they all showed a marginal improvement in QOL with resistance exercise. Peddle-McIntyre et al. (44) evaluated the effect of progressive resistance exercise on physical function and QOL in 17 patients with lung cancer. The results of SF-36 showed that multiple QOL outcomes had marginal improvement, but the specific cancer QOL (FACT-L) had no change after intervention. Chen et al. (63), in a 4.5-month quasi-experimental study using a single-group longitudinal design, when exploring the effect of elastic band resistance exercise intervention on patients with rectal cancer, found no significant changes in the general QOL assessment scale after the intervention, but a significant decrease in the cancer-specific symptom scale scores. Ammitzboll et al. (70) also demonstrated that the intervention only had favorable effects on emotion and social function. Although other indicators did not reach statistical significance, the results favored the intervention group. 21 studies examined the effects of resistance exercise on QOL in patients with cancer. Of these, 11 studies included patients who had completed cancer treatment at baseline, and 8 studies included patients who were undergoing cancer treatment. Those that completed treatment included three studies on breast cancer, two studies on colorectal cancer, two studies on prostate cancer, one study on head and neck cancer, and three studies on early-stage cancer. Those in treatment included three studies on breast cancer, two studies on prostate cancer, and one study each on head and neck, nasopharyngeal, and colorectal cancer. The remaining two studies included one on pre-treatment intervention for lung cancer and one on breast cancer without any treatment. In the four studies that had completed cancer treatment at the time of the intervention, the majority of findings demonstrated relatively favorable improvements in QOL for patients with cancer who engaged in resistance exercise following the intervention. However, two studies indicated that there were no significant or statistically significant improvements in QOL after the exercise intervention (31, 43). In studies where patients were undergoing cancer treatment at the time of the exercise intervention, the results demonstrated that the majority of studies did not find significant improvements in QOL for patients with cancer following resistance exercise interventions (30, 37, 46, 55, 64). The remaining two studies, Peddle-McIntyre et al. (44) evaluated the feasibility and preliminary efficacy of a PRET intervention for survivors of lung cancer treatment. No significant changes in QOL metrics were observed, with the exception of role fitness, physical pain, and physical health components, which demonstrated significant improvements. Benton et al. (65) sought to assess the impact of age on the QOL of patients with breast cancer following resistance training. Their findings indicated a notable enhancement in the QOL of patients with breast cancer following an exercise intervention, with the younger group exhibiting superior outcomes compared to the older group.
Nine studies have reported the effect of resistance exercise combined with aerobic exercise intervention on the QOL of patients with cancer. The results of two studies indicated that there was no significant difference in overall QOL after the exercise intervention (29, 69). Seven studies reported a significant effect of resistance exercise combined with aerobic exercise on QOL of various types of patients with cancer (25, 48, 52, 56, 60, 67, 71). Dieli-Conwright et al. (60) found that resistance exercise had a significant improvement for both Hispanic and non-Hispanic individuals, especially in social wellbeing, emotional wellbeing, and functional wellbeing. Lei et al. (48) explored the effects of traditional Chinese mind–body medicine exercise on QOL, depression, and anxiety in patients with cancer. On the functional scale, the intervention group showed significant improvement in physical functioning, role functioning, emotional functioning, and social functioning. On the symptom scale, the intervention group showed significant improvement in fatigue, pain, dyspnea, and sleep anxiety. Galvao et al. (56) found significant improvements in the assessment of the general QOL, while there were marginal improvements in the assessment of the cancer-specific QOL, such as physical, emotional, sleep, and pain. Adeline et al. (71), while exploring the effects of a 12-week exercise program on QOL in early-stage elderly patients with cancer, found that the improvement in QOL came primarily from an improvement in the overall state of health, improved physical functioning, and reduced fatigue, whereas the FACT-G assessment showed no significant change. Of these nine studies, five studies involved patients who had completed cancer-related treatment at baseline, while the remaining four studies focused on patients who were currently undergoing cancer treatment. The studies that had completed treatment included four on breast cancer and one on lung cancer. The studies that were in treatment included one on colorectal cancer, one on prostate cancer, and two studies that were not cancer-specific. Nevertheless, it was revealed that only two studies of patients with colorectal and early-stage cancers who were undergoing treatment did not find significant improvements in QOL following resistance exercise combined with aerobic exercise interventions (29, 69).
Ten studies have reported the effect of resistance exercise combined with other exercise interventions on the QOL of patients with various types of cancer. Of these studies, three studies showed little improvement in QOL after exercise intervention (36, 38, 61). Soriano−Maldonado et al. (38) conducted an intervention combining resistance and home exercise in patients with breast cancer. Guided resistance exercise was added twice a week to a home exercise prescription. The results showed that the improvement in patients’ QOL was not ideal. The other seven studies reported significant effects of resistance exercise combined with other exercise interventions on improving QOL (45, 57, 59, 68, 72–74). In these studies, at the start of the exercise intervention, patients with cancer in six studies had completed treatment, patients in three studies were in treatment, and patients in one study contained both. Of the six trials in which cancer-related treatment was completed, three trials in patients with breast cancer and unspecified cancers did not show an improvement in QOL after resistance training combined with other exercise interventions (36, 38, 61). One trial involving patients undergoing treatment, regardless of treatment/recovery stage, had a significant and statistically significant improvement in QOL after the intervention.
Table 5 shows the changes in the fatigue status of patients with cancer following an exercise intervention in each study experiment. A total of 20 studies examined the effects of resistance exercise intervention on fatigue in patients with cancer.
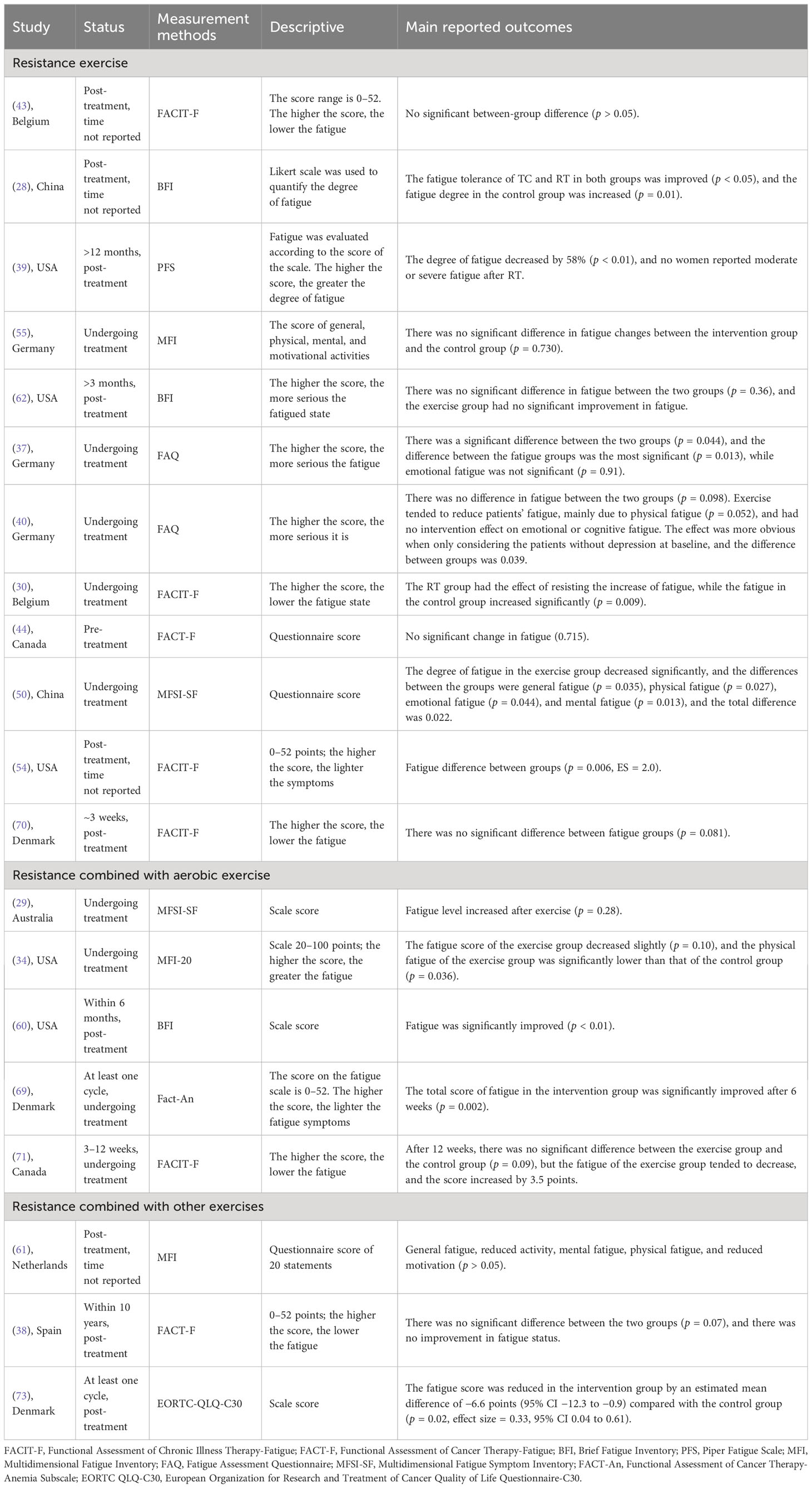
Table 5 Effect of resistance training on fatigue of patients with cancer.
Twelve studies were conducted to examine the effects of resistance exercise interventions on cancer fatigue. Six studies’ results indicated that there was no change or a decrease in fatigue status after the exercise intervention (40, 43, 44, 55, 62, 70), Schmidt et al. (40) conducted a resistance exercise intervention twice a week for 12 weeks in 101 patients with breast cancer. The results showed an increase in total fatigue and physical fatigue during chemotherapy in the control group. Although resistance exercise was found to reduce physical fatigue and improve QOL in patients with cancer to some extent, the observed effects were not statistically significant. The primary factor contributing to the decline in patients’ physical fatigue was a reduction in exercise intensity and frequency, whereas physical fatigue was not associated with emotional and cognitive fatigue and was influenced by the baseline condition of depressed patients. Six studies have reported the positive effects of resistance exercise on reducing fatigue in patients with cancer (28, 30, 37, 39, 50, 54), Cheng et al. (28) explored the effects of TC and resistance training of varying intensities on fatigue and QOL associated with elderly patients with cancer. Following the intervention, fatigue increased in the control group, while fatigue tolerance improved in the TC and resistance training groups, reaching statistically significant levels. Serra et al. (39), while exploring whether resistance training reduces fatigue and decreases systemic and tissue-specific inflammation in patients with breast cancer, found that resistance training reduced cancer-related fatigue by 58%. Steindorf et al. (37) found significant reductions in cancer-related fatigue, but not emotional fatigue, in the exercise group. Hu et al. (50) investigated the benefits of resistance exercise during chemotherapy in patients with nasopharyngeal carcinoma and found that patients in the exercise group had significantly less fatigue, with significant differences in general fatigue (p = 0.035), somatic fatigue (p = 0.027), emotional fatigue (p = 0.044), and mental fatigue (p = 0.013). Patients with cancer in six studies had completed cancer treatment, including two studies in breast cancer, one in prostate cancer, one in rectal cancer, and two studies in patients with early-stage cancer that did not differentiate between specific cancers. Patients in five trials are undergoing cancer treatment, including two breast cancer trials, one prostate cancer trial, one head and neck cancer trial, and one gastrointestinal cancer trial. Patients in one other lung cancer study have not yet been treated. The results showed that three studies of patients with cancer who had completed cancer-related treatments showed improvement in fatigue, while three other studies of rectal, breast, and prostate cancer showed no significant improvement in fatigue in patients with cancer with resistance exercise (43, 62, 70). For trials in which subjects were undergoing treatment, the results of two trials showed that resistance exercise did not improve fatigue in patients with cancer (40, 55). Schmidt et al. (40) conducted a resistance exercise intervention in patients with breast cancer; study results showed an increase in total fatigue and physical fatigue during chemotherapy. Exercise tended to reduce patients’ fatigue, mainly due to physical fatigue, and had no intervention effect on emotional or cognitive fatigue. The effect was more obvious when only considering the patients without depression at baseline. In another study of patients with lung cancer who were untreated before the test, the results demonstrated a similar, non-statistically significant improvement in fatigue in patients with cancer following the exercise intervention. Peddle-McIntyre et al. (44) reported the feasibility and preliminary efficacy of a PRET intervention in pre-treatment lung cancer survivors. There were borderline significant improvements in role-physical, bodily pain, and physical health component score. No other fatigue outcomes approached statistical significance, but most changed in a favorable direction.
Five studies reported the effects of resistance exercise combined with aerobic exercise on cancer-related fatigue. Of these five studies, the results of two studies showed little change or even a reduction in cancer-related fatigue after resistance exercise combined with aerobic exercise interventions (29, 71). Singh et al. (29) reported an increase in fatigue associated with the intervention. They explored the feasibility and efficacy of aerobic and resistance training twice a week for 10 weeks during neoadjuvant chemoradiotherapy (CRT) for rectal cancer. Adeline et al. (71) found a trend towards a significant reduction in fatigue and a 3.5-point increase in total fatigue score, although there was no significant change from the control group. Three studies reported significant reductions in fatigue following the intervention (34, 60, 69). The subjects of one study regarding breast cancer had completed cancer treatment. In four other studies, including one with rectal cancer, one with head and neck cancer, and two with unspecified cancers, the subjects were in the cancer treatment phase. The study demonstrated that patients who completed breast cancer-related treatment exhibited statistically significant improvements in fatigue following resistance training combined with aerobic exercise interventions. In studies of undergoing cancer treatment, two studies of patients with head and neck cancer and early-stage cancers did not achieve statistically significant results for improvements in fatigue levels (34, 71). However, three studies did demonstrate some effect on improvements or reductions in cancer-related fatigue. Singh et al. (29) examined the feasibility and preliminary efficacy of a 10-week exercise program in patients with rectal cancer; the results showed an increase in fatigue after intervention.
Three studies have reported the effects of resistance exercise combined with other exercises on fatigue in patients with cancer. Two studies have demonstrated that resistance exercise does not affect fatigue (38, 61). Adamsen et al. (73) evaluated the effects of a multimodal exercise intervention as an adjunct to usual care on fatigue, physical fitness, overall health, physical activity, and QOL in patients with cancer receiving adjuvant chemotherapy or treatment for advanced disease. After 6 weeks of intervention, patients exhibited a significant reduction in fatigue, with a 6.6-point decrease in fatigue scores. The studies included one on breast cancer and two on patients with non-specific cancers. All patients enrolled in the study had completed their cancer treatment prior to the commencement of the exercise intervention. The results of two studies indicated that resistance exercise combined with other exercise interventions did not result in improved fatigue status in patients with cancer.
It is well documented that incorporating exercise into one’s daily routine can promote numerous health benefits, and this also applies to patients with cancer. In addition to enhancing physical health, exercise can assist in the treatment of the side effects of cancer, including physical and psychological changes that can significantly impact muscle strength, QOL, and feelings of fatigue in patients with cancer. This review systematically assessed the effects of resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises on physical fitness, QOL, and fatigue in all patients with cancer. Meanwhile, the experimental protocols, types of interventions, frequency of exercise, intensity, duration of exercise, duration of the program, and measures of each outcome indicator varied considerably and were highly heterogeneous across all 48 included studies. Consequently, it is very important to analyze the optimal prescription of resistance exercise interventions that can have a greater positive beneficial effect on the majority of patients with cancer.
We discuss the efficacy of resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercise interventions for patients with various types of cancer. The primary outcomes of interest are physical fitness, QOL, and fatigue.
In terms of physical fitness, 34 out of 36 studies reported significant effects of resistance exercise on the physical fitness of patients with cancer compared with the control group. Whether the exercise involved resistance exercise training alone, resistance exercise combined with aerobic exercise, or some other form of exercise, all of them significantly improved physical fitness, especially muscle strength, in patients with cancer. Therefore, the adverse effect of reduced muscle mass in patients with cancer undergoing treatment can be effectively addressed through the implementation of these forms of exercise intervention. The impact of resistance exercise on QOL was not particularly prominent; rather, it was found to be most effective when combined with aerobic and other exercises. In the context of clinical cancer treatment, for patients with severely reduced QOL or mental health problems, the development of relevant non-drug intervention program may include a form of intervention that combines resistance exercise with other exercises, with the potential for improved outcomes. In studies of cancer-related fatigue, no significant effect of exercise on fatigue levels has been found. However, the majority of the studies employed a more rigorous intervention protocol, which may have exacerbated the patients’ perception of physical fatigue. This could be a contributing factor to the lack of significant improvement in fatigue levels. Therefore, in the actual treatment process, it is crucial to consider not only the impact on the physical fitness of patients with cancer, but also the potential for other adverse effects of exercise, such as the possibility that higher-intensity exercise may exacerbate the fatigue experienced by patients with cancer.
Owing to symptomatic limitations, the lack of adequate physical activity, and the associated vicious cycle, patients are adversely affected in terms of muscle mass during anticancer treatment. Unless the cancer is eradicated, this can result in a persistent deterioration in physical fitness (75, 76). A series of previous studies have demonstrated that exercise improves physical fitness and QOL in patients with cancer (77, 78), but these studies were small, family-based, and had little control over the intensity and amount of exercise, making it difficult to compare findings. In most sports studies, central location is a significant predictor of increased subject adherence (79). Home-based intervention programs have the potential to enhance patient acceptability while simultaneously reducing the overall cost of program supervision (80). Lam et al. (27) examined whether a 12-month exercise program developed at the start of ADT, which was based on home-based progressive resistance training, reduced adverse effects on body composition, metabolic health, physical functioning, and health-related QOL in patients with prostate cancer. A systematic review concludes that aerobic and resistance exercise improve upper and lower body muscle strength better than traditional care. The study also demonstrated that resistance exercise improved patients’ muscle strength more effectively than aerobic exercise (81). Thus, the impact of enhanced muscular strength may be discernible in interventions for patients with cancer, whether through resistance training alone or in combination with aerobic exercise. A recent meta-analysis also indicates the efficacy of resistance training in alleviating muscle dysfunction in patients with cancer. Based on patient data from 28 trials, it was concluded that exercise significantly improved muscle strength and function (82). Meanwhile, we also found that two of all included studies utilized an intervention model combining anti-resistance with nutritional supplements (51, 62). The result was a significant improvement in physical functioning as well. The principle of optimizing physical function and nutritional supplements in patients with cancer represents a broader concept of rehabilitation that is applicable to all patients with cancer. In patients with incurable cancer, the high prevalence of cachexia means that any intervention measures for this group should take nutritional support and supplementation as an important part of the means (83). Better nutrition is associated with higher baseline nutritional levels and a lower level of systemic inflammation. The effects of interventions to build muscle strength were more pronounced, particularly in terms of muscular endurance and reduced depression. Exercise interventions for patients with cancer during cancer treatment may better maintain or improve physical fitness and mental health outcomes (84), improve cardiorespiratory fitness (85), reduce anxiety and depression (86), improve health-related QOL (16), and reduce cancer-related fatigue (87). In the analysis of the QOL, resistance exercise interventions appear to have a weaker impact on patients with cancer than resistance exercise combined with aerobic and other exercise interventions. Nearly half of the 20 studies on resistance exercise intervention reported no significant effect or even a decrease in QOL, and 4 studies reported only marginal improvements in QOL, with no significant improvement in patients’ QOL (36, 44, 63, 70). However, the effect of resistance exercise intervention alone was not significant compared to resistance exercise combined with aerobic and other exercises. For example, studies by Bloomquist et al. and Nilsen et al. conducted high-intensity heavy resistance exercise interventions in patients with breast and prostate cancer, respectively, but did not elicit positive changes in patients’ QOL (46, 64). Most studies of resistance exercise combined with aerobic and other forms of exercise have demonstrated an improvement in QOL. It is evident that aerobic and other exercises, such as flexibility, stretching, and massage, play a significant role in enhancing QOL. Evidence suggests that patients with cancer suffer from severe psychological burdens, such as anxiety and depression, in addition to degradation of physical functioning from diagnosis to treatment (88), and the relationship between anxiety and depression and cancer prognosis has been well documented (89). The exercise intensity of the aerobic exercise intervention study in this review was approximately 75% HRmax. Resistance combined with stretching, flexibility, balance, and other sports can improve physical fitness. These elements also help to improve body composition and reduce excess adipose tissue and risk factors associated with lack of muscle strength. Additionally, they can reduce chemotherapy-induced neuropathic pain and improve physical and mental QOL (90–92). Resistance exercise, in combination with aerobic and other exercise interventions, represents an effective means of improving QOL and facilitating positive lifestyle changes in patients with cancer.
Fatigue is one of the most common adverse effects of cancer, can be present for years after the end of cancer treatment, and can undermine all aspects of QOL, which is an important factor in reducing survival.
Cancer-related fatigue represents one of the most significant symptoms associated with cancer and its treatment and can have a profound impact on a patient’s QOL. This effect is particularly pronounced during cancer radiotherapy and chemotherapy. From the studies of the effects of resistance exercise on cancer fatigue included in this systematic evaluation, it can be seen that resistance, resistance exercise combined with aerobic, and resistance exercise combined with other exercises did not improve fatigue as much, and that most of the positive effects were concentrated in studies of combined exercise interventions. Furthermore, it is pertinent to highlight that the study by Adamsen et al. employed exercise interventions, including resistance exercise combined with aerobic exercise and relaxation massage. This approach yielded notable outcomes in alleviating fatigue in patients with cancer, in which the role of relaxation massage should not be ignored (73). Reviewing all the included studies, we can see that most of the resistance exercise intensities used were above 75% 1RM, which might be a greater stress load for the participants and dilution of the fatigue-relieving effects. A recent indirect comparative meta-analysis evaluated the effects of diverse types of exercise and other non-pharmacological interventions on cancer-related fatigue during and after cancer treatment. The results showed that relaxation exercises during cancer treatment were the best measure to relieve cancer fatigue, followed by massage, cognitive behavioral therapy combined with physical activity, aerobic and resistance training, resistance training, aerobics, and yoga. At the end of treatment, yoga is the most effective in relieving fatigue, followed by aerobics combined with resistance training, aerobics, and resistance training (93). While most patients prefer low- to moderate-intensity exercise interventions, one study found that moderate- to vigorous-intensity exercise was beneficial for patients with cancer with fatigue compared with low-intensity exercise (94). This is inconsistent with the results of some of the studies included in the review, but there was no control for the amount of exercise, the treatment of patients with cancer involves different methods and phases, and the importance of exercise intensity itself cannot be determined. Therefore, more research comparing the relationship between different exercise intensities and cancer fatigue is needed. Combining the results of the systematic review, it is easy to see that combined exercise interventions for patients with cancer do not result in significant fatigue relief. It is crucial to consider the specific stage and the most appropriate interventions in light of this evidence.
Exercise can enhance motivation to change lifestyle behaviors, improve aerobic fitness and physical function, control fatigue, and enhance QOL. As a non-pharmacological and interventional measure, exercise has been demonstrated to reduce the risk of cancer. Moreover, physical activity plays a beneficial role in numerous cancers during cancer treatment. For instance, the adverse effects associated with cancer treatment can be mitigated, and the efficacy of other treatments can be enhanced, through physical activity. Consequently, in addition to an understanding of the impact of physical activity on various aspects of cancer, it is also necessary to identify the type, amount, and intensity of exercise that has an impact. Currently, cancer treatment employs a combination of therapeutic approaches, tailored to the specific characteristics of the disease, including the type, stage, and progression. These approaches may include targeted therapy, hormonal therapy, radiotherapy, and surgery. Radiotherapy and chemotherapy may induce physiological alterations and adverse effects (95, 96). Common side effects include fatigue, insomnia, nausea, and vomiting. Fatigue is one of the most common side effects of cancer. The utilization of different types and combinations of exercise can be employed for patients with cancer at various stages of treatment. For patients undergoing treatment, resistance training can effectively reduce the side effects of radiotherapy and chemotherapy. For cancer survivors who have completed their treatment, it can strengthen their physical health, enhance their immunity, and reduce the chances of cancer recurrence. The analysis of QOL revealed that resistance training, resistance training combined with aerobic exercise, or other exercises had a significant effect on improving the QOL of patients with cancer, regardless of whether the patients were in the treatment or recovery stage. This indicates that resistance training has a beneficial effect on patients in all stages of cancer treatment. These findings align with previous research indicating that resistance exercise during cancer chemotherapy is safe and may mitigate some of the treatment’s side effects (97). As can be seen from the inclusion in this study of results regarding the QOL of exercise interventions for cancer, the improvement in QOL was mainly due to resistance exercise combined with aerobic exercise as well as other exercises such as home-based exercise intervention models mainly for the treatment or recovery phase of cancer, and the improvement in QOL is more in favor of the population during treatment. Concurrently, the combination of resistance exercise with aerobic or other exercise was found to enhance the quality of life for the majority of cancer patients. There were no comparisons between resistance training and aerobic exercise in the included trials, but a previous randomized trial found no difference in QOL between the two groups by comparing the difference in QOL improvement between resistance and aerobic exercise in patients with cancer, including moderate to high intensity and home training (98). When resistance training is combined with aerobic exercise in interventions for patients with cancer undergoing treatment, the improvements in QOL may be greater than if the interventions were performed alone. As mentioned earlier, there was no consistent improvement in fatigue in patients with cancer regardless of the type of exercise intervention or stage of cancer treatment. Singh et al. (29), while exploring the effect of resistance exercise combined with aerobic exercise on the QOL of patients with breast cancer undergoing treatment, found that the patients showed increased fatigue. This may be related to the prevalence of fatigue in patients with most types of cancer. Patients often experience both psychological and physical stress during cancer treatment, and the increase in cancer-related fatigue is more severe, more painful, and less likely to be relieved by rest than fatigue in the healthy population. Although the exact etiology of cancer-related fatigue is not fully understood, it is thought to be based on the physical and psychological effects of cancer treatment. There are many theories about the factors that contribute to cancer-related fatigue. For example, one study suggests that the reduction in blood cells caused by chemotherapy may lead to anemia, which may lead to fatigue (99, 100). Meanwhile, treatment-induced activation of pro-inflammatory cytokines may be one trigger (101). Other factors include medications, psychological distress, altered immune function, excessive inactivity, neuromuscular dysfunction, and cognitive factors. It has already been mentioned that relaxation and massage are effective interventions during cancer treatment (73), but the role of relaxation after cancer treatment is less significant, suggesting that strategies to effectively manage fatigue during cancer treatment should include relaxation sessions in addition to individualized exercise and other non-pharmacological interventions. However, the effectiveness of relaxation massage declines after cancer treatment. More time should be spent on interventions to increase physical activity. Yoga is beneficial during and after cancer treatment, as are aerobic exercise, resistance training, and combined aerobic and resistance training. Only the magnitude of the effect is slightly lower.
Although there is sufficient evidence to support physical activity and exercise in adult patients with cancer, it is safe and acceptable for patients with all cancer types to engage in physical activity and exercise before, during, and after cancer treatment (102, 103). Designing a rational and scientific exercise intervention program for patients with cancer can better counteract the many side effects of the treatment process, better serve the rehabilitation program, improve the physical function of patients with cancer, reduce the feeling of fatigue, and, at the same time, improve the overall QOL. The majority of current studies have been conducted during and immediately after the treatment of patients with breast cancer. In contrast, relatively few studies on lung, digestive, and prostate cancers have been conducted. However, the evidence-based research literature in this area is rapidly accumulating. This study has several notable strengths. Primarily, it does not focus on a particular type of cancer, but rather examines all eligible cancer types, which makes it more broadly applicable. Second, a multilevel distinction was made in the form of exercise to facilitate the observation of the specific interventions in the future. Finally, the latest research evidence was included in the collection of research data for qualitative analysis. It should be noted that the study does have some limitations. Firstly, the literature collection is somewhat limited. A smaller number of studies have been conducted for specific cancers, and the findings may be biased. Second, owing to the heterogeneity of the measurement of the study results, a data-supported meta-analysis could not be performed, which could only provide a relatively limited reference value for the prognosis of clinical cancer treatment.
This systematic review shows that resistance exercise, resistance exercise combined with aerobic exercise, and resistance exercise combined with other exercises have a favorable intervention effect on the physical fitness (muscle strength, cardiorespiratory fitness, etc.) and QOL in patients with cancer. As far as physical fitness is concerned, all kinds of exercise interventions are effective in improving it, regardless of the patient’s stage of cancer treatment, but resistance is the best. QOL improvements, on the other hand, tend to favor a relative combination of resistance and aerobic and other exercises. The effects of the three resistance methods on alleviating cancer fatigue are inconsistent and controversial. Our conclusions may provide some valuable references for clinical cancer non-pharmacological intervention treatment and rehabilitation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
QZ: Methodology, Software, Writing – original draft. YG: Methodology, Software, Writing – original draft. WW: Project administration, Software, Writing – review & editing. XZ: Writing – review & editing. JY: Writing – review & editing. HH: Formal analysis, Methodology, Software, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We thank all the participants for participating in this study.
Author WW was employed by the company Ningbo New Fitness Health Technology Co., Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1393902/full#supplementary-material
1. Zhu J, Zhao L, Luo B, Sheng W. Shikonin regulates invasion and autophagy of cultured colon cancer cells by inhibiting yes−Associated protein. Oncol Lett. (2019) 18(6):6117–25. doi: 10.3892/ol.2019.10980
2. Demark-Wahnefried W, Aziz NM, Rowland JH, Pinto BM. Riding the crest of the teachable moment: promoting long-term health after the diagnosis of cancer. J Clin Oncol Off J Am Soc Clin Oncol. (2005) 23:5814–30. doi: 10.1200/JCO.2005.01.230
3. Greene D, Nail LM, Fieler VK, Dudgeon D, Jones LS. A comparison of patient-reported side effects among three chemotherapy regimens for breast cancer. Cancer Pract. (1994) 2:57–62.
4. Irvine D, Vincent L, Graydon JE, Bubela N, Thompson L. The prevalence and correlates of fatigue in patients receiving treatment with chemotherapy and radiotherapy. A comparison with the fatigue experienced by healthy individuals. Cancer Nurs. (1994) 17:367–78. doi: 10.1097/00002820-199410000-00001
5. Lucía A, Earnest C, Pérez M. Cancer-related fatigue: can exercise physiology assist oncologists? Lancet Oncol. (2003) 4:616–25. doi: 10.1016/s1470-2045(03)01221-x
6. Curt GA. Impact of fatigue on quality of life in oncology patients. Semin Hematol. (2000) 37:14–7. doi: 10.1016/S0037-1963(00)90063-5
7. Daley AJ, Crank H, Saxton JM, Mutrie N, Coleman R, Roalfe A. Randomized trial of exercise therapy in women treated for breast cancer. J Clin Oncol. (2007) 25:1713–21. doi: 10.1200/JCO.2006.09.5083
8. Courneya KS, Friedenreich CM. Physical activity and cancer control. Semin Oncol Nurs. (2007) 23:242–52. doi: 10.1016/j.soncn.2007.08.002
9. McGovern A, Mahony N, Mockler D, Fleming N. Efficacy of resistance training during adjuvant chemotherapy and radiation therapy in cancer care: A systematic review and meta-analysis. Supportive Care Cancer. (2022) 30:3701–19. doi: 10.1007/s00520-021-06708-6
10. Rogers LQ, Courneya KS, Anton PM, Hopkins-Price P, Verhulst S, Vicari SK, et al. Effects of the beat cancer physical activity behavior change intervention on physical activity, aerobic fitness, and quality of life in breast cancer survivors: A multicenter randomized controlled trial. Breast Cancer Res Treat. (2015) 149:109–19. doi: 10.1007/s10549-014-3216-z
11. Soares Falcetta F, de Araújo Vianna Träsel H, de Almeida FK, Rangel Ribeiro Falcetta M, Falavigna M, Dornelles Rosa D. Effects of physical exercise after treatment of early breast cancer: systematic review and meta-analysis. Breast Cancer Res Treat. (2018) 170:455–76. doi: 10.1007/s10549-018-4786-y
12. Speck RM, Courneya KS, Mâsse LC, Duval S, Schmitz KH. An update of controlled physical activity trials in cancer survivors: A systematic review and meta-analysis. J Cancer survivorship Res Pract. (2010) 4:87–100. doi: 10.1007/s11764-009-0110-5
13. Beasley JM, Kwan ML, Chen WY, Weltzien EK, Kroenke CH, Lu W, et al. Meeting the Physical Activity Guidelines and Survival after Breast Cancer: Findings from the after Breast Cancer Pooling Project. Breast Cancer Res Treat. (2012) 131:637–43. doi: 10.1007/s10549-011-1770-1
14. Zeng Y, Huang M, Cheng AS, Zhou Y, So WK. Meta-analysis of the effects of exercise intervention on quality of life in breast cancer survivors. Breast Cancer (Tokyo Japan). (2014) 21:262–74. doi: 10.1007/s12282-014-0521-7
15. Zhang X, Li Y, Liu D. Effects of exercise on the quality of life in breast cancer patients: A systematic review of randomized controlled trials. Supportive Care Cancer. (2019) 27:9–21. doi: 10.1007/s00520-018-4363-2
16. Mishra SI, Scherer RW, Geigle PM, Berlanstein DR, Topaloglu O, Gotay CC, et al. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Systematic Rev. (2012) 2012:Cd007566. doi: 10.1002/14651858.CD007566.pub2
17. Siegel RL, Miller KD, Jemal A. Cancer statistic. CA: Cancer J Clin. (2020) 70:7–30. doi: 10.3322/caac.21590
18. Malvezzi M, Carioli G, Bertuccio P, Boffetta P, Levi F, La Vecchia C, et al. European cancer mortality predictions for the year 2019 with focus on breast cancer. Ann Oncol Off J Eur Soc Med Oncol. (2019) 30:781–7. doi: 10.1093/annonc/mdz051
19. Neil-Sztramko SE, Kirkham AA, Hung SH, Niksirat N, Nishikawa K, Campbell KL. Aerobic capacity and upper limb strength are reduced in women diagnosed with breast cancer: A systematic review. J physiotherapy. (2014) 60:189–200. doi: 10.1016/j.jphys.2014.09.005
20. Holmes MD, Chen WY, Feskanich D, Kroenke CH, Colditz GA. Physical activity and survival after breast cancer diagnosis. Jama. (2005) 293:2479–86. doi: 10.1001/jama.293.20.2479
21. Van Blarigan EL, Meyerhardt JA. Role of physical activity and diet after colorectal cancer diagnosis. J Clin Oncol Off J Am Soc Clin Oncol. (2015) 33:1825–34. doi: 10.1200/JCO.2014.59.7799
22. Tomlinson D, Diorio C, Beyene J, Sung L. Effect of exercise on cancer-related fatigue: A meta-analysis. Am J Phys Med Rehabil. (2014) 93:675–86. doi: 10.1097/PHM.0000000000000083
23. Fyfe JJ, Hamilton DL, Daly RM. Minimal-dose resistance training for improving muscle mass, strength, and function: A narrative review of current evidence and practical considerations. Sports Med (Auckland NZ). (2022) 52:463–79. doi: 10.1007/s40279-021-01605-8
24. Pan B, Ge L, Xun YQ, Chen YJ, Gao CY, Han X, et al. Exercise training modalities in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Int J Behav Nutr Phys activity. (2018) 15:72. doi: 10.1186/s12966-018-0703-3
25. Casla S, Lopez-Tarruella S, Jerez Y, Marquez-Rodas I, Galvao DA, Newton RU, et al. Supervised physical exercise improves Vo2max, quality of life, and health in early stage breast cancer patients: A randomized controlled trial. Breast Cancer Res Treat. (2015) 153:371–82. doi: 10.1007/s10549-015-3541-x
26. Hong Y, Wu C, Wu B. Effects of resistance exercise on symptoms, physical function, and quality of life in gastrointestinal cancer patients undergoing chemotherapy. Integr Cancer therapies. (2020) 19:1534735420954912. doi: 10.1177/1534735420954912
27. Lam T, Cheema B, Hayden A, Lord SR, Gurney H, Gounden S, et al. Androgen deprivation in prostate cancer: Benefits of home-based resistance training. Sports Medicine-Open. (2020) 6(1):59. doi: 10.1186/s40798-020-00288-1
28. Cheng D, Wang X, Hu J, L-l D, Lv Y, Feng H, et al. Effect of tai chi and resistance training on cancer-related fatigue and quality of life in middle-aged and elderly cancer patients. Chin J Integr Med. (2021) 27:265–72. doi: 10.1007/s11655-021-3278-9
29. Singh F, Galvão DA, Newton RU, Spry NA, Baker MK, Taaffe DR. Feasibility and preliminary efficacy of a 10-week resistance and aerobic exercise intervention during neoadjuvant chemoradiation treatment in rectal cancer patients. Integr Cancer therapies. (2018) 17:952–9. doi: 10.1177/1534735418781736
30. Piraux E, Caty G, Renard L, Vancraeynest D, Tombal B, Geets X, et al. Effects of high-intensity interval training compared with resistance training in prostate cancer patients undergoing radiotherapy: A randomized controlled trial. Prostate Cancer prostatic Dis. (2021) 24:156–65. doi: 10.1038/s41391-020-0259-6
31. Simonavice E, Liu P-Y, Ilich JZ, Kim J-S, Arjmandi BH, Panton LB. The effects of resistance training on physical function and quality of life in breast cancer survivors. Healthcare (Basel Switzerland). (2015) 3:695–709. doi: 10.3390/healthcare3030695
32. Cumpston MS, McKenzie JE, Welch VA, Brennan SE. Strengthening systematic reviews in public health: Guidance in the cochrane handbook for systematic reviews of interventions, 2nd edition. J Public Health (Oxford England). (2022) 44:e588–e92. doi: 10.1093/pubmed/fdac036
33. Dent O. Methodological index for non-randomized studies. ANZ J Surg. (2003) 73:675–6. doi: 10.1046/j.1445-2197.2003.02762.x
34. Xiao C, Beitler JJ, Higgins KA, Chico CE, Withycombe JS, Zhu Y, et al. Pilot study of combined aerobic and resistance exercise on fatigue for patients with head and neck cancer: Inflammatory and epigenetic changes. Brain behavior Immun. (2020) 88:184–92. doi: 10.1016/j.bbi.2020.04.044
35. Winters-Stone KM, Torgrimson-Ojerio B, Dieckmann NF, Stoyles S, Mitri Z, Luoh S-W. A randomized-controlled trial comparing supervised aerobic training to resistance training followed by unsupervised exercise on physical functioning in older breast cancer survivors. J geriatric Oncol. (2022) 13:152–60. doi: 10.1016/j.jgo.2021.08.003
36. Winters-Stone KM, Dobek J, Bennett JA, Nail LM, Leo MC, Schwartz A. The effect of resistance training on muscle strength and physical function in older, postmenopausal breast cancer survivors: A randomized controlled trial. J Cancer survivorship Res Pract. (2012) 6:189–99. doi: 10.1007/s11764-011-0210-x
37. Steindorf K, Schmidt ME, Klassen O, Ulrich CM, Oelmann J, Habermann N, et al. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: Results on cancer-related fatigue and quality of life. Ann Oncol Off J Eur Soc Med Oncol. (2014) 25:2237–43. doi: 10.1093/annonc/mdu374
38. Soriano-Maldonado A, Diez-Fernandez DM, Esteban-Simon A, Rodriguez-Perez MA, Artes-Rodriguez E, Casimiro-Artes MA, et al. Effects of a 12-week supervised resistance training program, combined with home-based physical activity, on physical fitness and quality of life in female breast cancer survivors: The efican randomized controlled trial. J Cancer Survivorship. (2022) 17(5):1371–85. doi: 10.1007/s11764-022-01192-1
39. Serra MC, Ryan AS, Ortmeyer HK, Addison O, Goldberg AP. Resistance training reduces inflammation and fatigue and improves physical function in older breast cancer survivors. Menopause (New York NY). (2018) 25:211–6. doi: 10.1097/GME.0000000000000969
40. Schmidt ME, Wiskemann J, Armbrust P, Schneeweiss A, Ulrich CM, Steindorf K. Effects of resistance exercise on fatigue and quality of life in breast cancer patients undergoing adjuvant chemotherapy: A randomized controlled trial. Int J Cancer. (2015) 137:471–80. doi: 10.1002/ijc.29383
41. Santos W, Vieira A, de Lira CAB, Mota JF, Gentil P, de Freitas Junior R, et al. Once a week resistance training improves muscular strength in breast cancer survivors: A randomized controlled trial. Integr Cancer therapies. (2019) 18:1534735419879748. doi: 10.1177/1534735419879748
42. Quist M, Rorth M, Zacho M, Andersen C, Moeller T, Midtgaard J, et al. High-intensity resistance and cardiovascular training improve physical capacity in cancer patients undergoing chemotherapy. Scandinavian J Med Sci sports. (2006) 16:349–57. doi: 10.1111/j.1600-0838.2005.00503.x
43. Piraux E, Reychler G, Vancraeynest D, Geets X, Leonard D, Caty G. High-intensity aerobic interval training and resistance training are feasible in rectal cancer patients undergoing chemoradiotherapy: A feasibility randomized controlled study. Rep Pract Oncol radiotherapy J GreatPoland Cancer Center Poznan Polish Soc Radiat Oncol. (2022) 27:198–208. doi: 10.5603/RPOR.a2022.0036
44. Peddle-McIntyre CJ, Bell G, Fenton D, McCargar L, Courneya KS. Feasibility and preliminary efficacy of progressive resistance exercise training in lung cancer survivors. Lung Cancer (Amsterdam Netherlands). (2012) 75:126–32. doi: 10.1016/j.lungcan.2011.05.026
45. Noble M, Russell C, Kraemer L, Sharratt M. Uw well-fit: the impact of supervised exercise programs on physical capacity and quality of life in individuals receiving treatment for cancer. Supportive Care Cancer Off J Multinational Assoc Supportive Care Cancer. (2012) 20:865–73. doi: 10.1007/s00520-011-1175-z
46. Nilsen TS, Raastad T, Skovlund E, Courneya KS, Langberg CW, Lilleby W, et al. Effects of strength training on body composition, physical functioning, and quality of life in prostate cancer patients during androgen deprivation therapy. Acta Oncol. (2015) 54:1805–13. doi: 10.3109/0284186X.2015.1037008
47. Lonbro S, Dalgas U, Primdahl H, Johansen J, Nielsen JL, Aagaard P, et al. Progressive resistance training rebuilds lean body mass in head and neck cancer patients after radiotherapy - results from the randomized dahanca 25b trial. Radiotherapy Oncol. (2013) 108:314–9. doi: 10.1016/j.radonc.2013.07.002
48. Lei J, Yang J, Dong L, Xu J, Chen J, Hou X, et al. An exercise prescription for patients with lung cancer improves the quality of life, depression, and anxiety. Front Public Health. (2022) 10:1050471. doi: 10.3389/fpubh.2022.1050471
49. Lee K-J, An K-O. Impact of high-intensity circuit resistance exercise on physical fitness, inflammation, and immune cells in female breast cancer survivors: A randomized control trial. Int J Environ Res Public Health. (2022) 19(9):5463. doi: 10.3390/ijerph19095463
50. Hu Q, Zhao D. Effects of resistance exercise on complications, cancer-related fatigue and quality of life in nasopharyngeal carcinoma patients undergoing chemoradiotherapy: A randomised controlled trial. Eur J Cancer Care. (2021) 30:e13355. doi: 10.1111/ecc.13355
51. Houben LHP, Overkamp M, Kraaij PV, Trommelen J, Roermund JGHV, Vries PDE, et al. Resistance exercise training increases muscle mass and strength in prostate cancer patients on androgen deprivation therapy. Med Sci sports Exercise. (2023) 55:614–24. doi: 10.1249/MSS.0000000000003095
52. Herrero F, San Juan AF, Fleck SJ, Balmer J, Perez M, Canete S, et al. Combined aerobic and resistance training in breast cancer survivors: A randomized, controlled pilot trial. Int J sports Med. (2006) 27:573–80. doi: 10.1055/s-2005-865848
53. Hausmann F, Iversen VV, Kristoffersen M, Gundersen H, Johannsson E, Vika M. Combined aerobic and resistance training improves physical capacity in women treated for gynecological cancer. Supportive Care Cancer Off J Multinational Assoc Supportive Care Cancer. (2018) 26:3389–96. doi: 10.1007/s00520-018-4185-2
54. Hagstrom AD, Marshall PW, Lonsdale C, Cheema BS, Fiatarone Singh MA, Green S. Resistance training improves fatigue and quality of life in previously sedentary breast cancer survivors: A randomised controlled trial. Eur J Cancer Care. (2016) 25:784–94. doi: 10.1111/ecc.2016.25.issue-5
55. Grote M, Maihoefer C, Weigl M, Davies-Knorr P, Belka C. Progressive resistance training in cachectic head and neck cancer patients undergoing radiotherapy: A randomized controlled pilot feasibility trial. Radiat Oncol. (2018) 13(1):215. doi: 10.1186/s13014-018-1157-0
56. Galvão DA, Taaffe DR, Spry N, Joseph D, Newton RU. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: A randomized controlled trial. J Clin Oncol Off J Am Soc Clin Oncol. (2010) 28:340–7. doi: 10.1200/JCO.2009.23.2488
57. Foley MP, Hasson SM, Kendall E. Effects of a translational community-based multimodal exercise program on quality of life and the influence of start delay on physical function and quality of life in breast cancer survivors: A pilot study. Integr Cancer therapies. (2018) 17:337–49. doi: 10.1177/1534735417731514
58. Foley MP, Barnes VA, Hasson SM. Effects of a community-based multimodal exercise program on physical function and quality of life in cancer survivors: A pilot study. Physiotherapy Theory Pract. (2015) 31:303–12. doi: 10.3109/09593985.2015.1004390
59. Felser S, Behrens M, Liese J, Strueder DF, Rhode K, Junghanss C, et al. Feasibility and effects of a supervised exercise program suitable for independent training at home on physical function and quality of life in head and neck cancer patients: A pilot study. Integr Cancer therapies. (2020) 19:1534735420918935. doi: 10.1177/1534735420918935
60. Dieli-Conwright CM, Fox FS, Tripathy D, Sami N, Van Fleet J, Buchanan TA, et al. Hispanic ethnicity as a moderator of the effects of aerobic and resistance exercise on physical fitness and quality-of-life in breast cancer survivors. J Cancer survivorship Res Pract. (2021) 15:127–39. doi: 10.1007/s11764-020-00918-3
61. De Backer IC, Vreugdenhil G, Nijziel MR, Kester AD, van Breda E, Schep G. Long-term follow-up after cancer rehabilitation using high-intensity resistance training: persistent improvement of physical performance and quality of life. Br J Cancer. (2008) 99:30–6. doi: 10.1038/sj.bjc.6604433
62. Dawson JK, Dorff TB, Schroeder ET, Lane CJ, Gross ME, Dieli-Conwright CM. Impact of resistance training on body composition and metabolic syndrome variables during androgen deprivation therapy for prostate cancer: A pilot randomized controlled trial. BMC Cancer. (2018) 18(1):368. doi: 10.1186/s12885-018-4306-9
63. Chen SC, Huang HP, Huang WS, Lin YC, Chu TP, Beaton RD, et al. Non-randomized preliminary study of an education and elastic-band resistance exercise program on severity of neuropathy, physical function, muscle strength and endurance & Quality of life in colorectal cancer patients experiencing oxaliplatin-induced peripheral neuropathy. Eur J Oncol Nurs Off J Eur Oncol Nurs Soc. (2020) 49:101834. doi: 10.1016/j.ejon.2020.101834
64. Bloomquist K, Adamsen L, Hayes SC, Lillelund C, Andersen C, Christensen KB, et al. Heavy-load resistance exercise during chemotherapy in physically inactive breast cancer survivors at risk for lymphedema: A randomized trial. Acta Oncol. (2019) 58:1667–75. doi: 10.1080/0284186X.2019.1643916
65. Benton MJ, Schlairet MC, Gibson DR. Change in Quality of Life among Breast Cancer Survivors after Resistance Training: Is There an Effect of Age? J Aging Phys activity. (2014) 22:178–85. doi: 10.1123/japa.2012-0227
66. Battaglini C, Bottaro M, Dennehy C, Rae L, Shields E, Kirk D, et al. The effects of an individualized exercise intervention on body composition in breast cancer patients undergoing treatment. Sao Paulo Med J. (2007) 125:22–8. doi: 10.1590/S1516-31802007000100005
67. Aydin M, Kose E, Odabas I, Meric Bingul B, Demirci D, Aydin Z. The effect of exercise on life quality and depression levels of breast cancer patients. Asian Pacific J Cancer Prev APJCP. (2021) 22:725–32. doi: 10.31557/APJCP.2021.22.3.725
68. Andrioti A, Papadopetraki A, Maridaki M, Philippou A. The effect of a home-based tele-exercise training program on the quality of life and physical performance in breast cancer survivors. Sports (Basel Switzerland). (2023) 11(5):102. doi: 10.3390/sports11050102
69. Andersen C, Rorth M, Ejlertsen B, Stage M, Moller T, Midtgaard J, et al. The effects of a six-week supervised multimodal exercise intervention during chemotherapy on cancer-related fatigue. Eur J Oncol Nurs. (2013) 17:331–9. doi: 10.1016/j.ejon.2012.09.003
70. Ammitzboll G, Kjaer TK, Johansen C, Lanng C, Andersen EW, Kroman N, et al. Effect of progressive resistance training on health-related quality of life in the first year after breast cancer surgery - results from a randomized controlled trial. Acta Oncol. (2019) 58:665–72. doi: 10.1080/0284186x.2018.1563718
71. Adeline F, Hugo P-R, Rene M, Tamas F, Eleonor R, Michel P. Effects of a mixed exercise program on cancer related-fatigue and health-related quality of life in oncogeriatric patients: A feasibility study. J geriatric Oncol. (2021) 12:915–21. doi: 10.1016/j.jgo.2021.02.025
72. Adamsen L, Quist M, Midtgaard J, Andersen C, Moller T, Knutsen L, et al. The effect of a multidimensional exercise intervention on physical capacity, well-being and quality of life in cancer patients undergoing chemotherapy. Supportive Care Cancer. (2006) 14:116–27. doi: 10.1007/s00520-005-0864-x
73. Adamsen L, Quist M, Andersen C, Moller T, Herrstedt J, Kronborg D, et al. Effect of a multimodal high intensity exercise intervention in cancer patients undergoing chemotherapy: Randomised controlled trial. Bmj-British Med J. (2009) 339:b3410. doi: 10.1136/bmj.b3410
74. Adamsen L, Midtgaard J, Rorth M, Borregaard N, Andersen C, Quist M, et al. Feasibility, physical capacity, and health benefits of a multidimensional exercise program for cancer patients undergoing chemotherapy. Supportive Care Cancer. (2003) 11:707–16. doi: 10.1007/s00520-003-0504-2
75. Awad S, Tan BH, Cui H, Bhalla A, Fearon KCH, Parsons SL, et al. Marked changes in body composition following neoadjuvant chemotherapy for oesophagogastric cancer. Clin Nutr. (2012) 31:74–7. doi: 10.1016/j.clnu.2011.08.008
76. Antoun S, Birdsell L, Sawyer MB, Venner P, Escudier B, Baracos VE. Association of skeletal muscle wasting with treatment with sorafenib in patients with advanced renal cell carcinoma: results from a placebo-controlled study. J Clin Oncol Off J Am Soc Clin Oncol. (2010) 28:1054–60. doi: 10.1200/JCO.2009.24.9730
77. Segal R, Evans W, Johnson D, Smith J, Colletta S, Gayton J, et al. Structured exercise improves physical functioning in women with stages I and ii breast cancer: results of a randomized controlled trial. J Clin Oncol Off J Am Soc Clin Oncol. (2001) 19:657–65. doi: 10.1200/JCO.2001.19.3.657
78. Schwartz AL. Fatigue mediates the effects of exercise on quality of life. Qual Life Res an Int J Qual Life aspects treatment Care Rehabil. (1999) 8:529–38. doi: 10.1023/A:1008978611274
79. Ormel HL, van der Schoot GGF, Sluiter WJ, Jalving M, Gietema JA, Walenkamp AME. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psycho-oncology. (2018) 27:713–24. doi: 10.1002/pon.4612
80. Cheville AL, Dose AM, Basford JR, Rhudy LM. Insights into the reluctance of patients with late-stage cancer to adopt exercise as a means to reduce their symptoms and improve their function. J Pain symptom Manage. (2012) 44:84–94. doi: 10.1016/j.jpainsymman.2011.08.009
81. Stene GB, Helbostad JL, Balstad TR, Riphagen II, Kaasa S, Oldervoll LM. Effect of physical exercise on muscle mass and strength in cancer patients during treatment–a systematic review. Crit Rev oncology/hematology. (2013) 88:573–93. doi: 10.1016/j.critrevonc.2013.07.001
82. Sweegers MG, Altenburg TM, Brug J, May AM, van Vulpen JK, Aaronson NK, et al. Effects and moderators of exercise on muscle strength, muscle function and aerobic fitness in patients with cancer: A meta-analysis of individual patient data. Br J sports Med. (2019) 53:812. doi: 10.1136/bjsports-2018-099191
83. Maddocks M. Physical activity and exercise training in cancer patients. Clin Nutr ESPEN. (2020) 40:1–6. doi: 10.1016/j.clnesp.2020.09.027
84. Fong DY, Ho JW, Hui BP, Lee AM, Macfarlane DJ, Leung SS, et al. Physical activity for cancer survivors: Meta-analysis of randomised controlled trials. BMJ (Clinical Res ed). (2012) 344:e70. doi: 10.1136/bmj.e70
85. Scott JM, Zabor EC, Schwitzer E, Koelwyn GJ, Adams SC, Nilsen TS, et al. Efficacy of exercise therapy on cardiorespiratory fitness in patients with cancer: A systematic review and meta-analysis. J Clin Oncol Off J Am Soc Clin Oncol. (2018) 36:2297–305. doi: 10.1200/JCO.2017.77.5809
86. Craft LL, Vaniterson EH, Helenowski IB, Rademaker AW, Courneya KS. Exercise effects on depressive symptoms in cancer survivors: A systematic review and meta-analysis. Cancer epidemiology Biomarkers Prev Publ Am Assoc Cancer Research cosponsored by Am Soc Prev Oncol. (2012) 21:3–19. doi: 10.1158/1055-9965.EPI-11-0634
87. Kelley GA, Kelley KS. Exercise and cancer-related fatigue in adults: A systematic review of previous systematic reviews with meta-analyses. BMC Cancer. (2017) 17:693. doi: 10.1186/s12885-017-3687-5
88. Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. BMJ (Clinical Res ed). (2018) 361:k1415. doi: 10.1136/bmj.k1415
89. Wang YH, Li JQ, Shi JF, Que JY, Liu JJ, Lappin JM, et al. Depression and anxiety in relation to cancer incidence and mortality: A systematic review and meta-analysis of cohort studies. Mol Psychiatry. (2020) 25:1487–99. doi: 10.1038/s41380-019-0595-x
90. Socha M, Frączak P, Jonak W, Sobiech KA. Effect of resistance training with elements of stretching on body composition and quality of life in postmenopausal women. Przeglad menopauzalny = Menopause Rev. (2016) 15:26–31. doi: 10.5114/pm.2016.58770
91. Metz VR, Scapini KB, Dias Gomes AL, Andrade RM, Brech GC, Alonso AC. Effects of pilates on physical-functional performance, quality of life and mood in older adults: systematic review and meta-analysis of randomized clinical trials. J Bodyw Mov Ther. (2021) 28:502–12. doi: 10.1016/j.jbmt.2021.06.005
92. Dhawan S, Andrews R, Kumar L, Wadhwa S, Shukla G. A randomized controlled trial to assess the effectiveness of muscle strengthening and balancing exercises on chemotherapy-induced peripheral neuropathic pain and quality of life among cancer patients. Cancer Nurs. (2020) 43:269–80. doi: 10.1097/NCC.0000000000000693
93. Hilfiker R, Meichtry A, Eicher M, Nilsson Balfe L, Knols RH, Verra ML, et al. Exercise and other non-pharmaceutical interventions for cancer-related fatigue in patients during or after cancer treatment: A systematic review incorporating an indirect-comparisons meta-analysis. Br J sports Med. (2018) 52:651–8. doi: 10.1136/bjsports-2016-096422
94. van Waart H, Stuiver MM, van Harten WH, Geleijn E, Kieffer JM, Buffart LM, et al. Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: results of the paces randomized clinical trial. J Clin Oncol Off J Am Soc Clin Oncol. (2015) 33:1918–27. doi: 10.1200/JCO.2014.59.1081
95. Akram M, Iqbal M, Daniyal M, Khan AU. Awareness and current knowledge of breast cancer. Biol Res. (2017) 50:33. doi: 10.1186/s40659-017-0140-9
96. Parker PA, Youssef A, Walker S, Basen-Engquist K, Cohen L, Gritz ER, et al. Short-term and long-term psychosocial adjustment and quality of life in women undergoing different surgical procedures for breast cancer. Ann Surg Oncol. (2007) 14:3078–89. doi: 10.1245/s10434-007-9413-9
97. Battaglini CL, Mihalik JP, Bottaro M, Dennehy C, Petschauer MA, Hairston LS, et al. Effect of exercise on the caloric intake of breast cancer patients undergoing treatment. Braz J Med Biol Res = Rev Bras pesquisas medicas e biologicas. (2008) 41:709–15. doi: 10.1590/S0100-879X2008000800012
98. Santa Mina D, Alibhai SM, Matthew AG, Guglietti CL, Pirbaglou M, Trachtenberg J, et al. A randomized trial of aerobic versus resistance exercise in prostate cancer survivors. J Aging Phys activity. (2013) 21:455–78. doi: 10.1123/japa.21.4.455
99. Yang S, Chu S, Gao Y, Ai Q, Liu Y, Li X, et al. A narrative review of cancer-related fatigue (Crf) and its possible pathogenesis. Cells. (2019) 8(7):738. doi: 10.3390/cells8070738
100. Cartenì G, Giannetta L, Ucci G, De Signoribus G, Vecchione A, Pinotti G, et al. Correlation between variation in quality of life and change in hemoglobin level after treatment with epoetin alfa 40,000 iu administered once-weekly. Supportive Care Cancer Off J Multinational Assoc Supportive Care Cancer. (2007) 15:1057–66. doi: 10.1007/s00520-007-0220-4
101. Bower JE. Cancer-related fatigue–mechanisms, risk factors, and treatments. Nat Rev Clin Oncol. (2014) 11:597–609. doi: 10.1038/nrclinonc.2014.127
102. Segal R, Zwaal C, Green E, Tomasone JR, Loblaw A, Petrella T. Exercise for people with cancer: A systematic review. Curr Oncol (Toronto Ont). (2017) 24:e290–315. doi: 10.3747/co.24.3619
Keywords: resistance exercise, cancer, physical fitness, QOL, fatigue, systematic review
Citation: Zhang Q, Gao Y, Wang W, Zhao X, Yu J and Huang H (2024) Effect of resistance exercise on physical fitness, quality of life, and fatigue in patients with cancer: a systematic review. Front. Oncol. 14:1393902. doi: 10.3389/fonc.2024.1393902
Received: 28 March 2024; Accepted: 20 June 2024;
Published: 19 July 2024.
Edited by:
Melanie Keats, Dalhousie University, CanadaReviewed by:
Francesca Maffei, University of Bologna, ItalyCopyright © 2024 Zhang, Gao, Wang, Zhao, Yu and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huiming Huang, aHVhbmdodWltaW5nQG5idS5lZHUuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.