
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol. , 08 May 2024
Sec. Genitourinary Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1391825
This article is part of the Research Topic The Need for Pragmatic Trials in Genitourinary Oncology View all 3 articles
 Guillaume Grisay1Fabio Turco2
Guillaume Grisay1Fabio Turco2 Saskia Litiere3Béatrice Fournier4Anna Patrikidou5
Saskia Litiere3Béatrice Fournier4Anna Patrikidou5 Enrique Gallardo6Ray McDermott7Ahu Alanya8Silke Gillessen2,9Bertrand Tombal10*
Enrique Gallardo6Ray McDermott7Ahu Alanya8Silke Gillessen2,9Bertrand Tombal10*The landscape of treating metastatic prostate cancer has evolved with the addition of Androgen Receptor pathway inhibitor (ARPI) to Androgen Deprivation Therapy (ADT), significantly improving survival rates. However, prolonged use of these therapies introduces notable side effects, prompting a need to revisit intermittent treatment duration. The EORTC 2238 De-Escalate trial is a pragmatic trial seeking to reassess the role of intermittent therapy in patients undergoing maximal androgen blockade (MAB) for metastatic hormone naïve prostate cancer (mHNPC), i.e., the combination of ADT with an ARPI, with the aims of reducing side effects, enhancing Quality of Life (QoL) and optimizing resource usage, while maintaining oncological benefits.
Androgen deprivation therapy (ADT) through surgical castration or GnRH analogs has been the standard of care treatment for advanced prostate cancer (PCa) for six decades. Seven trials have now demonstrated that combining ADT with one of the androgen receptor pathway inhibitors (ARPI) - abiraterone, apalutamide, enzalutamide, and darolutamide - significantly prolongs progression-free (PFS) and overall survival (OS) (1–7). Called maximal androgen blockade (MAB), the combination of ADT and an ARPI also delays the progression to a further line of treatment and deterioration of quality of life (QoL) by delaying symptomatic progression. Consequently, MAB has become the new standard of care for men with metastatic hormone-naïve prostate cancer (mHNPC), regardless of the tumor burden (high vs. low volume/risk), timing (de novo vs. metachronous), or the co-administration of docetaxel and/or prostate radiotherapy.
There is, however, a price to pay. In landmark trials, the treatment was administered continuously until progression or unacceptable toxicity, sometimes up to several years. The patient is thus exposed for extended periods to the well-known toxicities of ADT and, furthermore, to the specific side effects of ARPI.
Interestingly, prior to the era of the ARPI trials, intermittent ADT (iADT) was often used to alleviate the side effects of androgen deprivation. Three prospective trials have tested an iADT regimen in patients with newly diagnosed mHNPC. None of these trials showed a clear difference in OS of iADT versus continuous dosing (8–10). A 10% difference in mortality appeared to favor the continuous arm, however, this did not reach statistical significance. Non-inferiority cannot therefore be proved or disproved, nor can the superiority of either strategy be ruled out.
EORTC 2238 (De-Escalate) investigates the risk/benefit of intermittent treatment in patients on MAB for 6 to 12 months who have achieved a significant prostate-specific antigen (PSA) decline to ≤0.2 ng/ml (Figure 1). First demonstrated by Hussain, deep PSA response is a robust prognostic survival factor. Patients who are good responders are, therefore, likely to be exposed for longer periods to toxicities and side effects while deriving few benefits (11).
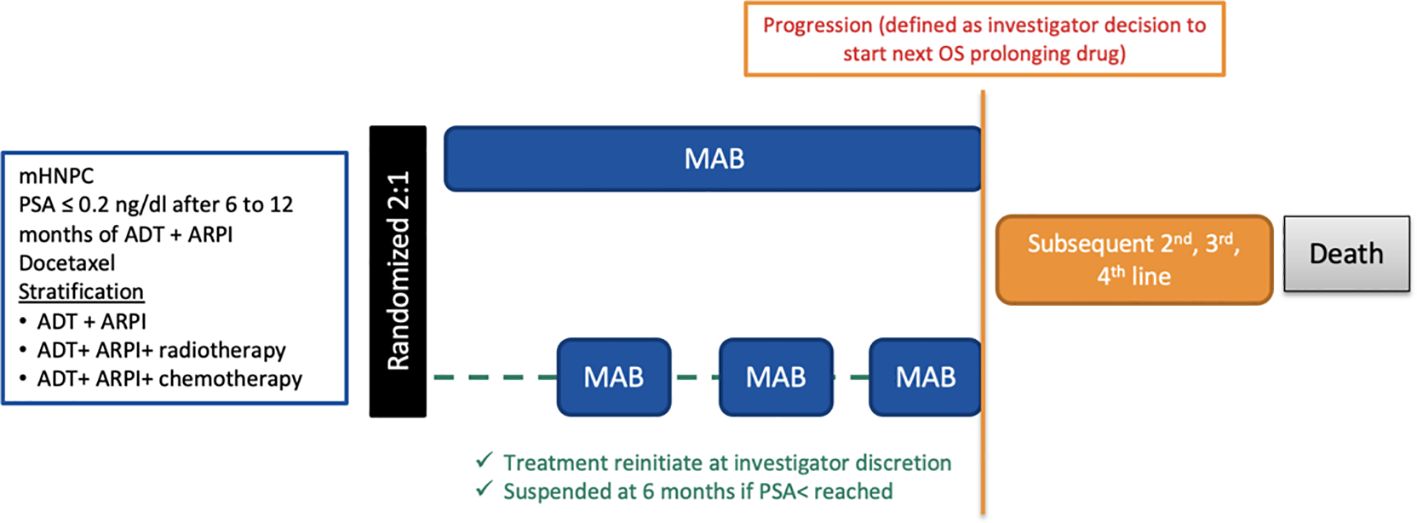
Figure 1 Trial scheme.
This trial is essential to reassess the benefit of intermittent treatment in patients receiving ADT and an ARPI as it could potentially reduce side-effects, improve QoL and reduce resource utilization.
The development of four ARPI has profoundly reshaped the management of mHNPC. They are the CYP17A inhibitor (abiraterone acetate) and the AR antagonists (apalutamide, darolutamide and enzalutamide). Seven trials have demonstrated that combining any of these drugs to ADT ± docetaxel consistently reduces the risk of death by 20 to 40%, delays progression to the next line of treatment and improves health related QoL (HRQoL) by delaying symptomatic progression. Apalutamide (TITAN trial) and enzalutamide (ARCHES and ENZAMET) have been evaluated in patients with either high or low-volume disease (4–6). Darolutamide has been tested only with docetaxel (ARASENS) (12). Abiraterone acetate has been evaluated in high-risk disease in the LATITUDE trial, but has also been tested in broader disease settings in the STAMPEDE and PEACE-1 trials (1, 3).
Hence, MAB with one of these agents is the new standard of care for mHNPC, notwithstanding the volume (high vs. low volume/risk) and timing of metastasis (de-novo vs metachronous) of the disease (EAU guidelines).
During the most recent Advanced Prostate Cancer Consensus Conference (APCCC), 77% of panelists recommended radical local treatment of the primary tumor and ADT plus one of the ARPIs for treating synchronous, low-volume HNPC (13). Eighty-nine percent of panelists recommended ADT and an ARPI (with 40% of them adding docetaxel) to treat synchronous, high-volume HNPC.
The addition of an ARPI to continuous ADT increases OS therefore resulting in a much longer treatment duration, thus increasing the toxicity associated. A recent meta-analysis of studies conducted in non-metastatic castration-resistant PCa (nmCRPC) concluded that the addition of an ARPI to ADT is associated with a significantly increased risk of cardiovascular events (RR = 1.71; 95% CI 1.29-2.27) and grade 3-4 hypertension (RR = 1.53; 95% CI 1.19-1.97) (14). In another recent review, the use of an ARPI was associated with an increased risk of falls and fractures: all-grade falls (RR, 1.8; 95% CI, 1.42-2.24; p < 0.001); grade ≥ 3 fall (RR, 1.6; 95% CI, 1.27-2.08; p < 0.001); all-grade fractures (RR, 1.59; 95% CI, 1.35-1.89; p < 0.001); and likely grade ≥3 fracture (RR, 1.71; 95% CI, 1.12-2.63; p = 0.01) (15). Furthermore, the recent systematic review and meta-analysis by Nowakowska et al. showed an increased risk of cognitive toxic effects (risk ratio (RR) 2.10; 95%CI 1.30-3.38; p = 0.002) and fatigue (RR 1.34; 95%CI 1.16-1.54; p <.001) with the use of ARPIs (16).
Intermittent ADT (iADT) consists of interrupting ADT in patients with a significant PSA response after 6 to 12 months of treatment. This allows the testosterone to return to normal, side effects to resolve, and HRQoL to improve. Regular measurements of testosterone and PSA are performed. ADT is restarted, usually upon PSA rise to a value at the investigator’s discretion, with each trial using its own individual criteria. Multiple cycles of on- and off-treatment can be performed in this way.
Nine randomized trials have assessed the feasibility of iADT as a strategy to preserve efficacy while decreasing side effects (17). All these trials used a conditional randomization scheme as the patients had to have achieved a predefined decrease in PSA levels from baseline. Three trials have included patients with mHNPC.
The FinnProstate Study VII randomized 852 locally advanced (50%) or metastatic (50%) PCa to receive ADT for 24 weeks (18). Five hundred fifty-four patients in whom PSA decreased to less than 10 ng/ml, or by 50% or more if less than 20 ng/ml at baseline, were randomized to intermittent (iADT) or continuous ADT (cADT). There were 248 prostate cancer-related deaths: 117 (43%) in the iADT and 131 (47%) in the cADT arms (p = 0.29). This study also investigated HR-Qol with a validated and self-administered 30-item questionnaire addressing ten domains (18). In metastatic patients, ADT improved the pain, activity limitation, and social functioning domain, with iADT further improving activity limitation, social functioning, and recovery of sexual functioning domains.
The South European Urooncological Group (SEUG) trial included 766 patients with locally advanced (67%) or metastatic PCa (30%) who have received a 3-month induction treatment (9). The 626 patients whose PSA level decreased to <4 ng/ml or 80% below the initial value were randomized between iADT and cADT. There was no difference in survival, with an HR of 0.99 (95% CI 0.80-1.23) and 170 deaths in the iADT arm and 169 deaths in cADT arm. Side effects were more pronounced in the continuous arm, and men treated with intermittent therapy reported better sexual function (p < 0.01). The median time off treatment for the patients on iADT was 52 (95% CI 39.4-65.7) weeks.
The intergroup trial SWOG-9346 (EORTC 30985) enrolled 3040 patients with newly diagnosed mHNPC to receive ADT for seven months (8). Of these, 1535 patients achieved a PSA decrease to ≤ 4 ng/mL and were randomized to iADT or cADT. The median follow-up period was 9.8 years. Median survival was 5.8 years in the cADT and 5.1 years in the iADT, resulting in a HR for death with iADT of 1.10 (90% CI 0.99-1.23). The 10% difference in mortality appears to favor the continuous arm, but this did not reach significance. Furthermore, the confidence limits crossed both unity and the pre-determined non-inferiority margin so that non-inferiority was neither proved nor disproved, and the superiority of either arm could not be ruled out. For patients receiving iADT, the median percentage of time on therapy was 47% (IQ range, 23-69). Intermittent treatment was associated with better erectile function and mental health (p<0.001 and p=0.003, respectively) at month three but not after that.
Niraula and Tannock systematically reviewed all the randomized trials comparing iADT to cADT (17). They identified nine studies totaling 5,508 patients treated with either approach. The pooled HR for OS was 1.02 (95% CI 0.94-1.11) for iADT compared with cADT, and the HR for progression-free survival was 0.96 (95% CI 0.76-1.20). Given that neither strategy showed superiority for time-to-event outcomes and iADT was associated with reduced cost, better convenience, and less potential toxicity, they recommended that men with relapsing locally advanced, or metastatic prostate cancer who achieved a good initial response to ADT be treated intermittently rather than continuously. Becker et al. recently performed a meta-analysis of 12 randomized clinical trials using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines (19). There was no statistically significant difference in prostate cancer specific mortality between intermittent androgen deprivation therapy and continuous androgen deprivation therapy (RR=1.10 [0.85-1.42]) in this mixed population, comprising patients with failure after local treatment and locally advanced or metastatic prostate cancer. The analysis of non-prostate cancer mortality favored intermittent androgen deprivation therapy over continuous androgen deprivation therapy, but the difference was not statistically significant (RR=0.94 [0.76-1.17]).
The registration trials of MAB were designed using continuous administration of both drugs until progression, which is currently the standard of care. However, the continuous use of both drugs results in increased toxicity. In daily practice, physicians, must regularly assess the risk/benefit balance between continuous use or drug holidays. An urgent medical need is to redefine this risk/benefit balance with modern combinations.
Registration trials have certain essential limitations.
First, patients are carefully selected to avoid comorbidities and optimize treatment duration. Hence, patients with cardiovascular disease and cognitive changes are often underrepresented. Real-world data collections have shown a significant increase in hospitalization due to cardiovascular complications in patients with pre-existing cardiovascular comorbidities treated with ARPI (20).
Second, pragmatic clinical trials (PrCTs) differ from classical randomized controlled trials (RCTs) as they answer the critical question of the “effectiveness” of a treatment in the real-world population rather than its “efficacy” in a pre-specified highly selected patient population. PrCTs involve four key design elements: 1) enrolling a real-world population, 2) being conducted in a real-world setting, 3) capturing relevant outcomes important to inform optimal healthcare treatment decisions and 4) using an appropriate comparison arm, which may not always be a placebo treatment. One of the main advantages of PrCTs over real-world observational studies is the use of randomization (21).
Third, unlike explanatory RCTs, PrCTs seek to enroll a broader patient population, including those with comorbidities, adopt more flexible treatment dispensing instructions, and use existing data sources. This leads to more relevant and generalizable findings. Moreover, PrCTs are more likely to incorporate patient-centered outcomes, enabling assessing patient-centered outcomes that are not extensively collected in traditional RCTs. Patient-reported outcomes such as QoL, treatment adherence, and long-term survivorship are critical considerations for individuals living with cancer. By incorporating these outcomes into pragmatic trial designs, clinicians can gain a comprehensive understanding of the impact of interventions on patients’ lives, enabling shared decision-making and improving patient-centered care.
As PrCTs target real-world patients deemed eligible for a given treatment by their physicians, minimizing the inclusion and exclusion criteria is necessary. Reducing the bureaucracy associated with modern RCTs is crucial to increase pragmatic trial participation by physicians and patients (22). Attempts should be made to reduce the complexity of the study by limiting the number of study procedures and visits, the length of patient questionnaires, or any other deviation from standard of care, routine clinical practice procedures. The idea is to be as close as possible to a real-world setting. The investigator selection should also represent the heterogeneity in clinical practice involving a mix of academic and non-academic centers from different countries.
RCTs are usually conducted in double-blind conditions, with data collection obtained via a strict protocol that must be closely adhered to, to produce robust data. Blinding allows for better reporting of critical endpoints or patients’ outcomes. This does not mimic real-life practice. Because ensuring high-quality data collection in PrCTs is essential, investigators may rely on unified electronic medical records (EMR) to capture prespecified events of interest. Other advantages of EMR include long-term treatment efficacy and safety monitoring at a lower cost. It can also produce data regarding the cost-effectiveness of a given treatment. The De-Escalate trial will incorporate all these principles.
The most critical implementation challenge, not unique to PrCTs, will be patient acceptance of their randomization choice. Patients experiencing toxicity on treatment may refuse to stay on MAB or become silently non adherent. Anxious patients or physicians may find it challenging to adhere to a treatment pause. To mitigate this risk, novel informed consent strategies have been developed, such as the two-stage informed consent, recently introduced by A. Vickers (23, 24).
In the two-stage consent process, patients are first informed that they are invited to join a study and discuss data collection and research procedures, such as questionnaires. They are then informed that they might later be randomly selected to hear about an experimental treatment, and if so, they can decide whether to try it or continue with the standard of care. Once baseline data have been collected, randomization will be performed centrally. Patients who signed the first consent and are not randomized to the experimental arm will stay in the control arm, receiving standard-of-care treatment. In De-Escalate, patients with deep PSA response will first consent to the collection of data. Then, within a month of the randomization, patients randomly selected to the intermittent treatment arm will be informed about the investigational treatment (here iMAB) and are asked to sign a second informed consent. If they refuse, they will stay on the control arm (cMAB) and the only addition to their clinical routine will be to complete HR-QoL questionnaires at regular intervals. PSA, testosterone, further anticancer treatment, and grade 3 to 5 toxicity will be collected from routine follow-up. Following the intent-to-treat principle, patients are analyzed in the experimental arm irrespective of their decision at this second stage. Vickers et al. have reported that conducting consent in two stages reduces the decisional anxiety, confusion, and information overload commonly associated with informed consent (23, 24). Although this raised some concerns during an advisory ethical committee review, with further explanations and endorsement from patients’ organization Europa Uomo, it was found acceptable.
Finally, a last major hurdle we observed while developing the study design was its recognition as a low interventional clinical trial. This is defined by EU clinical trial regulation (CTR) when 1) the interventional medicine product (IMP) is authorized and considered as SOC, 2) the use of the IMP is evidence-based and supported by robust scientific evidence on its safety and efficacy and 3) the additional diagnostic or monitoring procedures do not pose more than minimal additional risk or burden to the safety of the subjects compared to normal clinical practice. De-Escalate trial will not mandate the use of any specific ADT or ARPI drug. But instead, all medications currently used as standard of care under their marketing authorization, depending on the participating countries, will be available as treatment options, addressing the first two point of the definition of a low interventional clinical trial. Since there are no extra tests or imaging required, and monitoring of PSA and testosterone level is routinely done, there is no extra burden for the patients. We faced however some issues regarding the intermittent use of both ADT and ARPI or “treatment holiday”, as in registration trials, regulators requested that patients would be treated continuously for methodological reasons.
Not every trial can be pragmatic. The PRECIS-2 criteria “PRagmatic-Explanatory Continuum Indicator Summary v2” have been developed to help investigators develop more pragmatic trials (25). It evaluates a trial’s design via several key dimensions: recruitment of participants (no exclusion criteria based on upper age limit, comorbidities, …) and investigators, the setting of the trial (multiple centers, academic and non-academic), the delivery and adherence to the protocol (flexibility in monitoring of compliance), follow-up (minimum number of FU visits), endpoints (relevant for patients such as OS or QoL) and analysis (all data are included in the analysis)?. Each dimension is scored between 0 to 5, with 5 being the most pragmatic.
We tested the PRECIS-2 tool with EORTC 2238 De-Escalate (Figure 2). It demonstrates the trials pragmatic approach, as it scores 5 points in eligibility, flexibility in treatment delivery, follow-up, primary outcome and primary analysis. It scores 4 in setting of the trial, adherence and organization. The only dimension to score 3 points is recruitment of patients. Figure 2 summarizes each dimension.
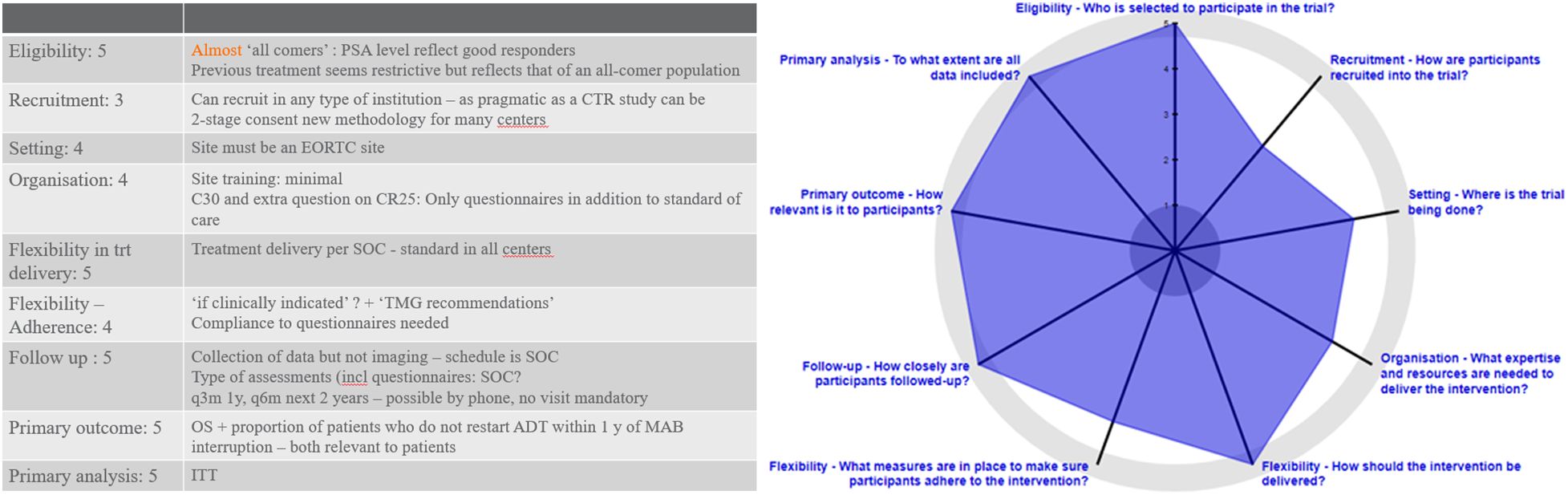
Figure 2 PRECIS-2 evaluation of EORTC-2238.
Revisiting the concept of intermittent treatment in the era of combined treatment for metastatic hormone-naïve prostate cancer is a critical challenge. Routinely combining AR pathway inhibitors with androgen deprivation therapy does indeed significantly prolong survival but at the price of more toxicity and resource utilization. Patients with a profound PSA response deserve that we investigate a better balance between treatment duration, toxicity, and survival. Such trials require many patients from many countries, hence large resources.
Pragmatic trials have emerged as a valuable tool for generating evidence that could guide clinical practice and health policy decisions. These trials can improve treatment outcomes, enhance patient care, and optimize resource allocation by including diverse patient populations, evaluating patient-centered outcomes, and assessing implementation strategies. However, challenges include methodology issues, data collection quality, and balancing protocol flexibility with scientific rigor.
The EORTC 2238 De-Escalate trial will revisit the concept of intermittent treatment in patients with a deep PSA response after 6 to 12 months of induction treatment, seeking to spare them from chronic toxicities while maintaining their overall survival and improving their quality of life.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
GG: Writing – review & editing, Writing – original draft. FT: Writing – review & editing, Writing – original draft. SL: Writing – review & editing, Writing – original draft. BF: Writing – review & editing, Writing – original draft. AP: Writing – review & editing, Writing – original draft. EG: Writing – review & editing, Writing – original draft. RM: Writing – review & editing, Writing – original draft. AA: Writing – review & editing, Writing – original draft. SG: Writing – review & editing, Writing – original draft. BT: Writing – review & editing, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This project has received funding from the European Union’s Horizon Europe under Grant Agreement number: 101104574. Views and opinions expressed are, however, those of the authors only and do not necessarily reflect those of the European Union. Neither the European Union nor the granting authority can be held responsible for them.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. (2017) 377:352–60. doi: 10.1056/NEJMoa1704174
2. James ND, de Bono JS, Spears MR, Clarke NW, Mason MD, Dearnaley DP, et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med. (2017) 377:338–51. doi: 10.1056/NEJMoa1702900
3. Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2× 2 factorial design. Lancet. (2022) 399:1695–707. doi: 10.1016/S0140-6736(22)00367-1
4. Chi KN, Chowdhury S, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: final survival analysis of the randomized, double-blind, phase III TITAN study. J Clin Oncol. (2021) 39:2294–303. doi: 10.1200/JCO.20.03488
5. Davis ID, Martin AJ, Stockler MR, Begbie S, Chi KN, Chowdhury S, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. (2019) 381:121–31. doi: 10.1056/NEJMoa1903835
6. Armstrong AJ, Szmulewitz RZ, Petrylak DP, Holzbeierlein J, Villers A, Azad A, et al. ARCHES: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. (2019) 37:2974–86. doi: 10.1200/JCO.19.00799
7. Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. (2022) 386:1132–42. doi: 10.1056/NEJMoa2119115
8. Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, et al. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. (2013) 368:1314–25. doi: 10.1056/NEJMoa1212299
9. Calais da Silva FE, Bono AV, Whelan P, Brausi M, Marques Queimadelos A, Martin JA, et al. Intermittent androgen deprivation for locally advanced and metastatic prostate cancer: results from a randomised phase 3 study of the South European Uroncological Group. Eur Urol. (2009) 55:1269–77. doi: 10.1016/j.eururo.2009.02.016
10. Crook JM, O'Callaghan CJ, Duncan G, Dearnaley DP, Higano CS, Horwitz EM, et al. Intermittent androgen suppression for rising PSA level after radiotherapy. N Engl J Med. (2012) 367:895–903. doi: 10.1056/NEJMoa1201546
11. Hussain M, Goldman B, Tangen C, Higano CS, Petrylak DP, Wilding G, et al. Prostate-specific antigen progression predicts overall survival in patients with metastatic prostate cancer: data from Southwest Oncology Group Trials 9346 (Intergroup Study 0162) and 9916. J Clin Oncol. (2009) 27:2450–6. doi: 10.1200/JCO.2008.19.9810
12. Saad F, Hussain M, Tombal B, Fizazi K, Sternberg C, Crawford D, et al. Association of prostate-specific antigen (PSA) response and overall survival (OS) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) from the phase 3 ARASENS trial. JCO. (2022) 40:5078–8. doi: 10.1200/JCO.2022.40.16_suppl.5078
13. Gillessen S, Bossi A, Davis ID, de Bono J, Fizazi K, James ND, et al. Management of patients with advanced prostate cancer—metastatic and/or castration-resistant prostate cancer: report of the Advanced Prostate Cancer Consensus Conference (APCCC) 2022. Eur J Cancer. (2023) 185:178–215. doi: 10.1016/j.ejca.2023.02.018
14. Rizzo A, Merler S, Sorgentoni G, Oderda M, Mollica V, Gadaleta-Caldarola G, et al. Risk of cardiovascular toxicities and hypertension in nonmetastatic castration-resistant prostate cancer patients treated with novel hormonal agents: a systematic review and meta-analysis. Expert Opin Drug Metab Toxicol. (2021) 17:1237–43. doi: 10.1080/17425255.2021
15. Myint ZW, Momo HD, Otto DE, Yan D, Wang P, Kolesar JM. Evaluation of fall and fracture risk among men with prostate cancer treated with androgen receptor inhibitors: a systematic review and meta-analysis. JAMA Netw Open. (2020) 3:e2025826. doi: 10.1001/jamanetworkopen.2020.25826
16. Nowakowska MK, Ortega RM, Wehner MR, Nead KT. Association of second-generation antiandrogens with cognitive and functional toxic effects in randomized clinical trials: A systematic review and meta-analysis. JAMA Oncol. (2023) 9:930–7. doi: 10.1001/jamaoncol.2023.0998
17. Niraula S, Le LW, Tannock IF. Treatment of prostate cancer with intermittent versus continuous androgen deprivation: a systematic review of randomized trials. J Clin Oncol. (2013) 31:2029–36. doi: 10.1200/JCO.2012.46.5492
18. Salonen AJ, Taari K, Ala-Opas M, Viitanen J, Lundstedt S, Tammela TL, et al. Advanced prostate cancer treated with intermittent or continuous androgen deprivation in the randomised FinnProstate Study VII: quality of life and adverse effects. Eur Urol. (2013) 63:111–20. doi: 10.1016/j.eururo.2012.07.040
19. Becker B, Stroever S, Reddy A, de Riese WTW. Comparison of intermittent and continuous androgen deprivation therapy in prostate cancer patients: an up-to-date meta-analysis for urologists and medical providers. Urol Pract. (2023) 10:424–34. doi: 10.1097/UPJ.0000000000000424
20. Lu-Yao G, Nikita N, Keith SW, Nightingale G, Gandhi K, Hegarty SE. Mortality and hospitalization risk following oral androgen signaling inhibitors among men with advanced prostate cancer by pre-existing cardiovascular comorbidities. Eur Urol. (2020) 77:158–66. doi: 10.1016/j.eururo.2019.07.031
21. Gamerman V, Cai T, Elsäßer A. Pragmatic randomized clinical trials: best practices and statistical guidance. Health Serv Outcomes Res Method. (2019) 19:23–35. doi: 10.1007/s10742-018-0192-5
22. Gribben J, Macintyre E, Sonneveld P, Doorduijn J, Gisselbrecht C, Jäger U, et al. Reducing bureaucracy in clinical research: a call for action. Hemasphere. (2020) 4:e352. doi: 10.1097/HS9.0000000000000352
23. Vickers AJ, Vertosick EA, Carlsson SV, Ehdaie B, Kim SYH. Patient accrual and understanding of informed consent in a two-stage consent design. Clin Trials. (2021) 18:377–82. doi: 10.1177/1740774520988500
24. Vickers AJ, Young-Afat DA, Ehdaie B, Kim SY. Just-in-time consent: the ethical case for an alternative to traditional informed consent in randomized trials comparing an experimental intervention with usual care. Clin Trials. (2018) 15:3–8. doi: 10.1177/1740774517746610
Keywords: mHNPC, de-escalation, maximal androgen blockade, AR pathway inhibitor, quality of life
Citation: Grisay G, Turco F, Litiere S, Fournier B, Patrikidou A, Gallardo E, McDermott R, Alanya A, Gillessen S and Tombal B (2024) EORTC 2238 “De-Escalate”: a pragmatic trial to revisit intermittent androgen deprivation therapy in the era of new androgen receptor pathway inhibitors. Front. Oncol. 14:1391825. doi: 10.3389/fonc.2024.1391825
Received: 26 February 2024; Accepted: 20 March 2024;
Published: 08 May 2024.
Edited by:
Piet Ost, Ghent University, BelgiumReviewed by:
Giulia Baciarello, San Camillo Forlanini Hospital, ItalyCopyright © 2024 Grisay, Turco, Litiere, Fournier, Patrikidou, Gallardo, McDermott, Alanya, Gillessen and Tombal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bertrand Tombal, YmVydHJhbmQudG9tYmFsQHNhaW50bHVjLnVjbG91dmFpbi5iZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.