 Fengqin Liu1
Fengqin Liu1 Xiao Song
Xiao Song
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 28 May 2024
Sec. Cancer Molecular Targets and Therapeutics
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1390006
Lung cancer remains one of the leading causes of cancer-related mortality worldwide necessitating the development of innovative therapeutic strategies. Chimeric antigen receptor (CAR) natural killer (NK) cell therapy represents a promising advancement in the field of oncology offering a novel approach to target and eliminate tumor cells with high specificity and reduced risk of immune-related adverse effects. This paper reviews the mechanism, potential targets, and recent advances in CAR-NK cell therapy for lung cancer, including the design and engineering of CAR-NK cells, preclinical studies, and the outcomes of early-phase clinical trials. We highlight the unique advantages of using NK cells, such as their innate ability to recognize and kill cancer cells and their reduced potential for inducing graft-versus-host disease (GvHD) and cytokine release syndrome (CRS) compared to CAR T-cell therapies. Results from recent studies demonstrate significant antitumor activity in lung cancer models with improved targeting and persistence of CAR-NK cells observed in vitro and in vivo. Finally, we discuss the challenges in optimizing CAR-NK cell therapies, including the potential resistance mechanisms. The paper concludes with an outlook on the future directions of CAR-NK cell research and its implications for lung cancer treatment emphasizing the importance of continued innovation and collaboration in the field.
Lung cancer remains a major global health challenge accounting for a significant portion of cancer deaths worldwide. As of 2023, there occurred approximately 238,340 new cases of lung cancer (117,550 in men and 120,790 in women), and it was estimated to cause 127,070 deaths from lung cancer (67,160 in men and 59,910 in women) (1). From a global perspective, as of 2020, it was estimated to cause about 1.8 million deaths representing 18% of all cancer deaths (2). Lung cancer is the second most common cancer in both men and women in the U.S. after prostate and breast cancer, respectively (1). At diagnosis, lung cancer is classified based on the type of cells the tumor is derived from. There are two major types of lung cancer categorized by the pathological description of the malignant cells as follows: small-cell lung cancer (SCLC; 15% of cases) and non-small-cell lung cancer (NSCLC; 85% of cases) (3). The primary risk factor for lung cancer is smoking tobacco, which is responsible for approximately 85% of all cases. This includes cigarettes, cigars, and pipes. Other risk factors include exposure to secondhand smoke, occupational hazards (such as asbestos, radon, and certain chemicals), air pollution, hereditary cancer syndromes, and previous chronic lung diseases (3).
Physical examinations, imaging (chest X-rays, CT scans, MRI), bronchoscopy, biopsies, and molecular testing are often used to diagnose lung cancer and determine the specific subtype (NSCLC vs. SCLC). In addition to the classification of lung cancer, the staging of lung cancer is also particularly important for the selection of treatment options. Common treatments include surgery, radiation therapy, chemotherapy, targeted drug therapy, and immunotherapy (3). Common immunotherapies include adoptive cell therapy, checkpoint blockade immunotherapies (like drugs targeting the PD-1/PD-L1 pathway), and cancer vaccines (4). Adoptive cell therapies are quite popular in the field of lung cancer treatment, including chimeric antigen receptor T-cell (CAR T) therapy, T-cell receptor (TCR) therapy, and tumor-infiltrating lymphocyte (TIL) therapy (5). These approaches involve using a patient’s own immune cells, modified and expanded in the laboratory, to target and destroy cancer cells. However, due to the limitations of T cells themselves, such as limited sources and easy triggering of inflammatory factor storms, researchers have turned their attention to other immune cells that can be modified, such as NK (natural killer) cells (6). As a new star in cell therapy, CAR-NK therapy has attracted much attention in recent years. This study intends to discuss the possibility, advantages, and challenges of using CAR-NK in the treatment of lung cancer from multiple dimensions.
NK cells are a type of lymphocyte in the immune system that play a crucial role in the body’s defense against tumors and viral infections. NK cells are functionally similar to CD8+ cytotoxic T cells and kill target cells through similar cytotoxic mechanisms, but lack a somatically rearranged and antigen-specific TCR. Tumor cells with lower expression of human leukocyte antigen (HLA) may be more susceptible to NK cell killing due to a reduced KIR-mediated inhibition (7). NK cells used in therapy can be derived from various sources like peripheral blood mononuclear cells, cord blood, immortalized cell lines, hematopoietic stem and progenitor cells (HSPCs), and induced pluripotent stem cells (iPSCs) (6, 7). Allogeneic NK cells are often preferred over autologous cells due to the dysfunctional phenotype of autologous NK cells in cancer patients. NK cell lines like NK-92MI have also been approved to load the CAR structure to create a CAR-NK therapeutic system and apply it clinically. This further increases the source and availability of NK cells (8). NK-92 cells, in contrast to NK cells from other sources, have predictable expansion kinetics and can be grown in bioreactors that produce billions of cells within a couple of weeks. In addition, NK cell lines can easily be transduced by physical methods with high efficiency. CAR-expressing NK-92 has been generated to target several cancer surface receptors, such as CD19 (a type of B-cell receptor) (9), human epidermal growth factor receptor 2 (HER2/ErbB2) (10), and epidermal growth factor receptor (EGFR, aka HER1) (11), and many of these engineered NK-92 cells are currently in clinical trials for the treatment of cancer. CAR-NK cells are engineered to recognize and attack specific antigens present in cancer cells. Figure 1 shows the CAR-NK cell therapy process using PBMC as an example.
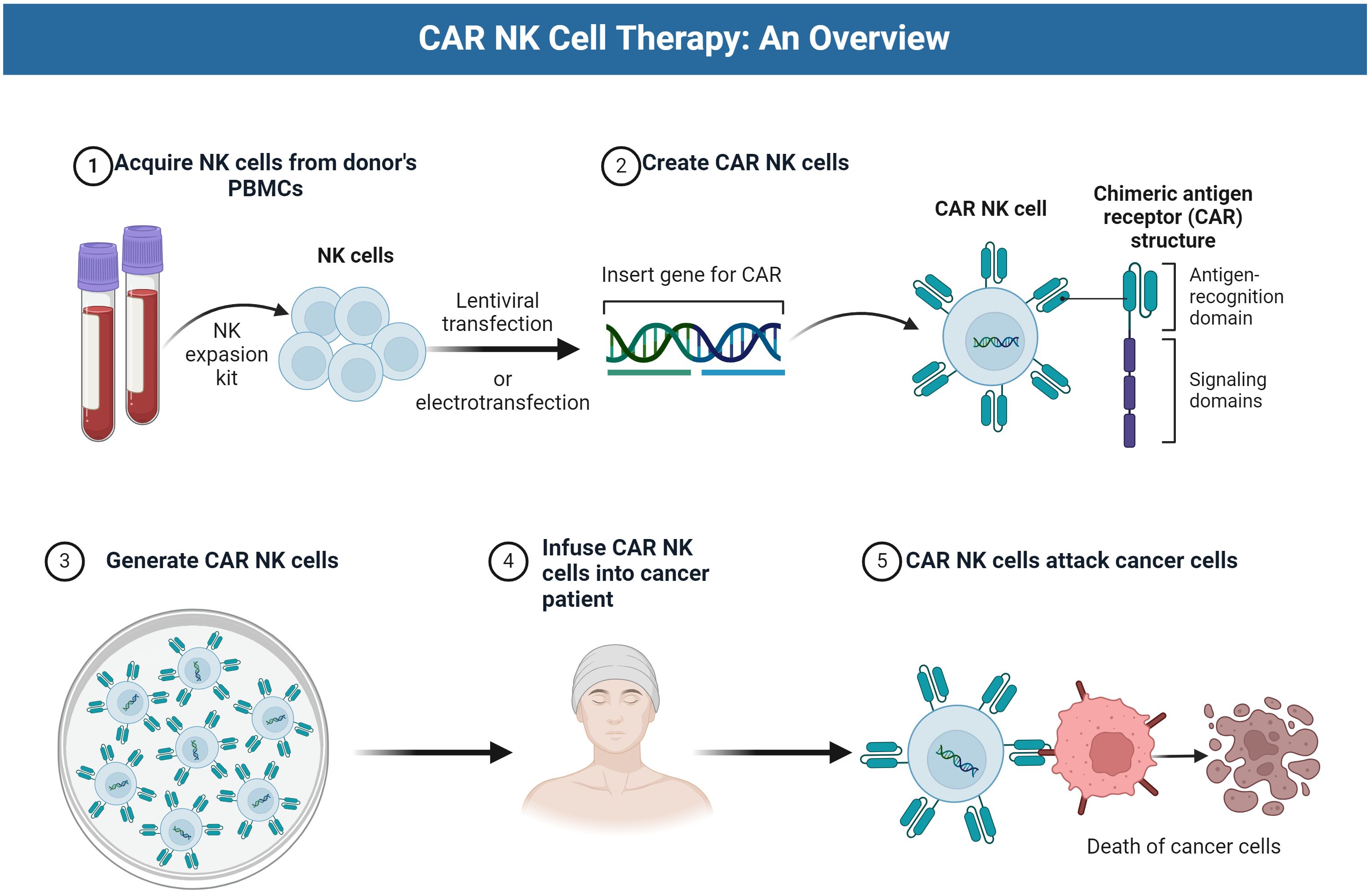
Figure 1 The CAR NK cell therapy process.
Immunotherapy for lung cancer is very popular and has achieved great success. Population-level mortality from NSCLC in the United States fell sharply from 2013 to 2016, and survival after diagnosis improved substantially (12). Several different genetic mutations may arise in lung tumors, and some may be more likely to cause the cancer cells to spread to other parts of the body. As an example, mutations of epidermal growth factor receptor (EGFR) have been identified as key drivers of metastasis, and safe, efficacious therapies have been developed to target EGFR mutations and inhibit cancer spread (13). These targets can also be used as a basis to design the antigen-recognition region of CAR-NK therapy.
Figure 2 shows some lung cancer targets that CAR-NK therapy can potentially target.
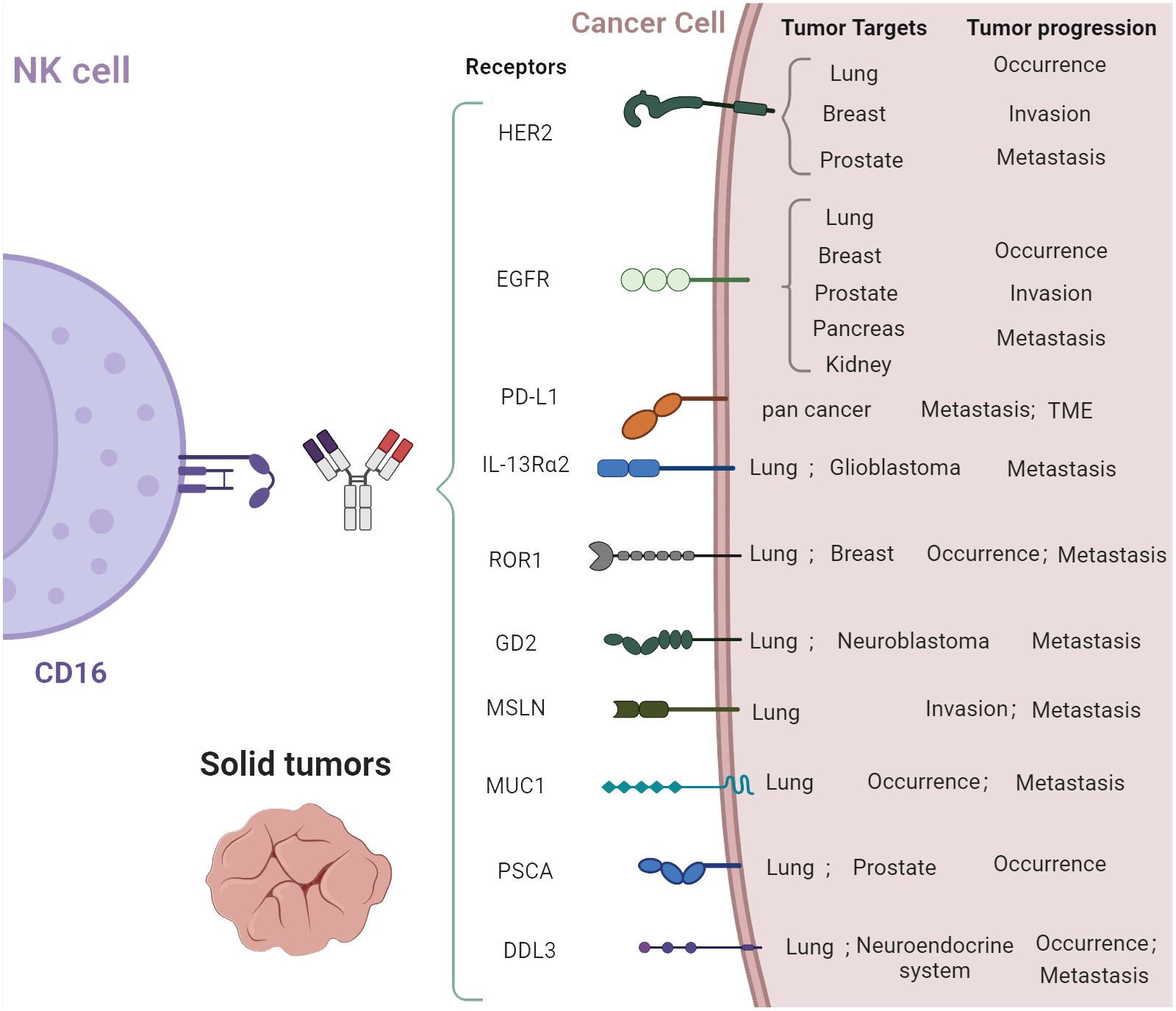
Figure 2 Potential lung cancer targets.
We have compiled published lung cancer-related targets in CAR-NK engineering therapies and corresponding preclinical research results:
1. HER2 (human epidermal growth factor receptor 2): HER2 is a well-known target in various cancers, including breast and ovarian cancers. It has also been targeted in lung cancer. Trastuzumab deruxtecan (a HER2 antibody–drug conjugate) showed durable anticancer activity in patients with previously treated HER2-mutant NSCLC (14).
2. EGFR (epidermal growth factor receptor): EGFR plays a significant role in the development and progression of non-small cell lung carcinoma and other types of cancer. Approximately 15% of NSCLCs express EGFR. CAR T-cell therapies targeting EGFR are being explored and could be adapted for CAR-NK cell therapies in lung cancer (13).
3. Programmed death ligand 1 (PD-L1) is one of the most successful targets since targeted cancer therapy became popular. Immunotherapies targeted PD-L1, and its receptor (PD-1) have improved survival in a subset of patients with advanced lung cancer (15). Membrane-bound programmed death ligand 1 (PD-L1) level was elevated on a tumor cell surface, which serves as an attractive target for natural killer (NK) cell-mediated therapy (16).
4. IL-13Rα2 (Interleukin-13 receptor alpha 2): This receptor is highly expressed in glioblastoma but has potential as a target in lung cancer due to its limited expression in normal tissues. It is a negative prognostic factor in human lung cancer and stimulates lung cancer growth in mice (17). IL-13Rα2-targeted therapies have been studied in glioblastoma and could be a novel avenue for lung cancer treatment.
5. ROR1 (receptor tyrosine kinase-like orphan receptor 1): ROR1 is expressed in many lymphatic and epithelial malignancies and involved in tumor cell survival. It is being examined as a target for CAR T-cell therapies in lung and breast cancers, suggesting potential for CAR-NK cell therapy (18).
6. GD2 (disialoganglioside GD2): GD2 is highly expressed in neuroblastoma and melanoma but could be considered for SCLC treatment due to its expression on certain small lung cancer cell lines (19). GD2 is one of the few SCLC-specific therapeutic targets. The anti-GD2 antibody dinutuximab was used to treat patients with relapsed/refractory SCLC (20).
7. 7.Mesothelin (MSLN) overexpression is a marker of tumor aggressiveness and associated with reduced recurrence-free and overall survival in early-stage lung cancer (21). Combined with chemokine receptor CCR2b, CAR T treatment targeting MSLN showed good results in the NSCLC mouse model (22).
8. Mucin 1 (MUC1) is an emerging therapeutic target for solid tumors in recent years. Artificial MUC1-positive animal tumor models show that CAR T therapy targeting MUC1 has a good effect on reducing tumor size and metastasis (23). As shown in a Phase I clinical trial, PD-1 disrupting anti-MUC1-CAR cells achieved a greater response rate and acceptable tolerability results in the NSCLC patients (24).
9. Prostate stem cell antigen (PSCA) is associated with prostate cancer metastasis. Using aCGH and protein expression analysis, researchers found that PSCA may play an important role in the development of NSCLC brain metastasis and it can be a good therapeutic target for advanced lung tumors (25). Similar with MUC1, PSCA, as a target, performed well in CAR T therapy for NSCLC (26).
10. Delta-like ligand 3 (DLL3) is an inhibitory Notch ligand that is highly expressed in SCLC and other neuroendocrine tumors but minimally expressed in normal tissues. It is therefore being explored as a potential therapeutic target in SCLC (27).
Additionally, new targets, such as erythropoietin-producing hepatocellular carcinoma A2 (EphA2) (28), tissue factor (TF) (29), and protein tyrosine kinase 7 (PTK7) (30) are currently under clinical investigation. The development of next-generation personalized CAR T cells against solid tumors like NSCLC remains a critical frontier in cancer immunotherapy, given the unique challenges posed by the strong immunosuppressive tumor microenvironment in solid tumors.
The principle of selecting cell therapy targets is the target’s high expression on lung cancer cells and the lack of expression on normal cells to minimize off-target effects. The expression of cell-surface molecules changes in malignantly transformed cells, and CAR-NK cells can target these altered expressions.
Immunotherapy has revolutionized cancer treatment by harnessing the body’s immune system to target and destroy cancer cells. Among various immunotherapy modalities, CAR-NK therapy and other approaches offer distinct advantages, paving the way for novel and effective cancer treatments. One of the most significant advantages of CAR-NK therapy over other forms of immunotherapy, such as CAR T-cell therapy, is its inherent ability to target cancer cells with high specificity while minimizing off-target effects. Table 1 shows comparison of CAR-T and CAR-NK technology. NK cells have a natural ability to distinguish between healthy and malignant cells, reducing the risk of autoimmune responses and collateral damage (31). In particular, CAR-NK therapy has demonstrated promising efficacy in treating solid tumors, including lung cancer, which has been a significant challenge for other forms of immunotherapy. The natural ability of NK cells to infiltrate solid tumors, combined with the specificity of CAR targeting, offers a potent therapeutic approach for lung cancer patients (32).
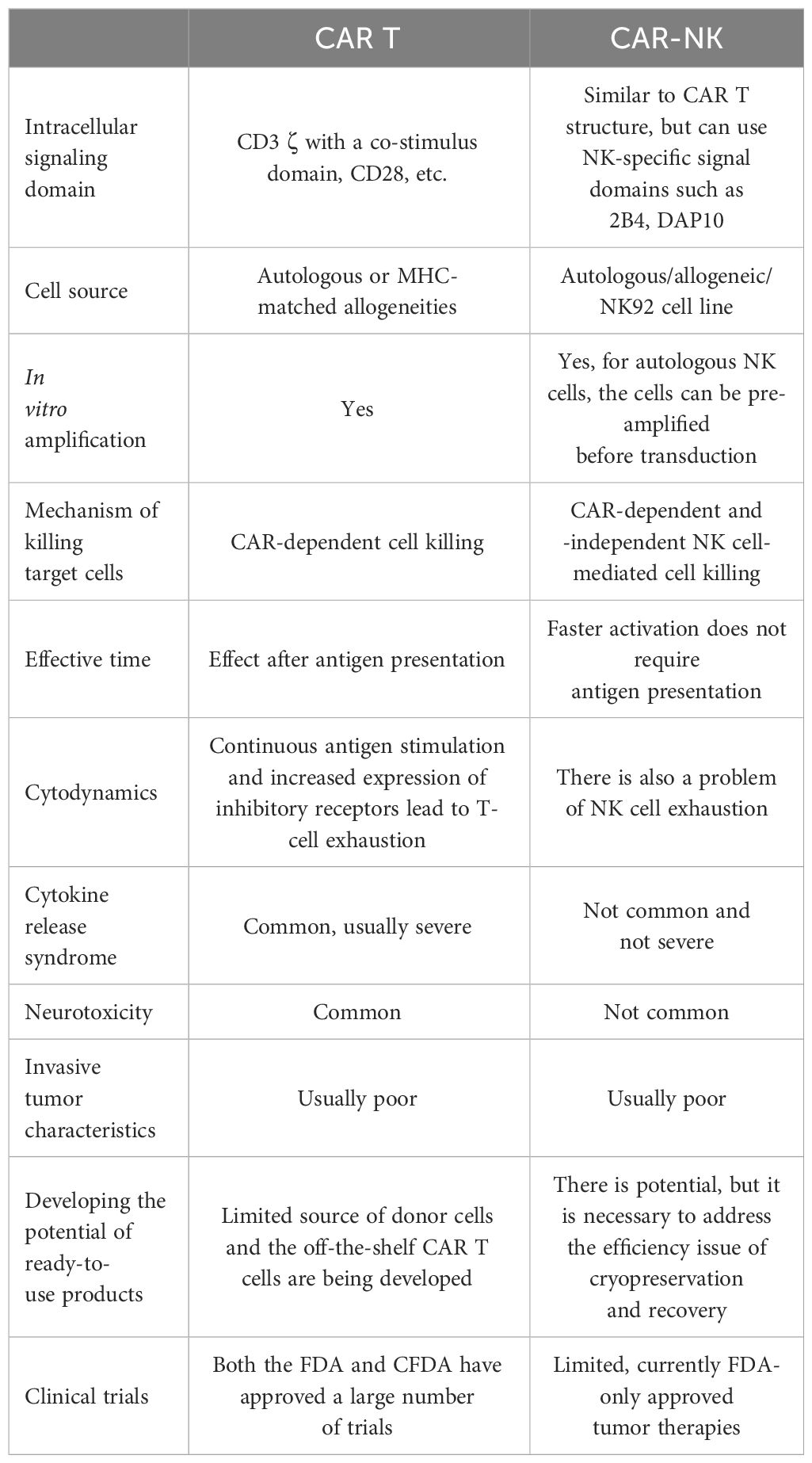
Table 1 The comparison of CAR-NK and CAR T technology.
Unlike CAR T therapy, CAR-NK therapy demonstrated superior treatment safety. CAR T-cell therapies have been associated with cytokine release syndrome (CRS), a potentially fatal immune response. CAR-NK cells have shown a lower propensity to induce CRS, making CAR-NK therapy a safer alternative (33). This reduced risk enhances patient safety and could lead to broader applicability in clinical settings.
The source of cells in cell therapy often becomes a constraint limiting the clinical application of the treatment. CAR T cells are typically autologous (derived from the patient), which limits its promotion. Currently, many attempts to manufacture off-the-shelf CAR T cells, such as using induced pluripotent stem cells (iPSCs) differentiate T cells (8, 34, 35), are being developed. Hopefully, the source and practicality of CAR T cells can be solved. Unlike T cells, NK cells can be derived from allogeneic sources (donors), making them readily available for “off-the-shelf” use (10, 31). This allogeneic capability significantly reduces the time and cost associated with CAR–NK cell therapy, making it more accessible to a broader patient population. The main sources of NK cells include peripheral blood, umbilical cord blood, NK cell lines, and induced pluripotent stem cells (iPSCs). Peripheral blood is the most traditional source of NK cells for therapeutic purposes. NK cells derived from peripheral blood are readily available and can be collected from the patient (autologous) or a donor (allogeneic). The peripheral blood collection is relatively straightforward, and autologous use minimizes the risk of immune rejection (36). Beyond peripheral blood, umbilical cord blood (UCB) is an alternative source of NK cells that has been explored due to its unique properties. UCB-derived NK cells display a higher degree of immaturity, which might result in better expansion and longevity after infusion. They also carry a lower risk of causing graft-versus-host disease (GvHD) when used allogeneically (37).
In addition to the abovementioned naturally derived NK cells, NK cells obtained through cell-engineering methods have also been proven to be able to load CAR structures to build CAR-NK therapy. The iPSCs represent a cutting-edge source of NK cells, capable of differentiating into any cell type, including NK cells. The iPSCs provide an inexhaustible source of NK cells that can be genetically engineered to enhance their anticancer properties. While the differentiation process is complex and costly, the long-term safety of iPSC-derived NK cells remains to be fully established (38). What is more, several human NK cell lines, such as NK-92, have been genetically modified to express CARs for therapeutic applications–10. NK cell lines offer a consistent and unlimited source of NK cells that can be readily engineered and expanded in vitro. The use of cell line sources makes the expansion and packaging process easy. At the same time, it can also reduce the batch effect and instability of engineered cells. The use of NK cell lines poses a risk of tumorigenicity, and regulatory authorities require irradiation before infusion, which can affect the longevity and potency of these cells in vivo (39).
As of January 2024, researchers have tried many different types of CAR-NK therapies for lung cancer, including two approved clinical trials. A chimeric co-stimulatory transition receptor, (CCCR) consisting of PD1 extracellular domain, NKG2D transmembrane and cytoplasmic domain, and NKG2D cytoplasmic domain 4–1BB, was applied to CAR-NK cell engineering. This receptor can convert negative PD1 signals into activation signals, effectively reversing the immunosuppressive effect of PD1. In a lung cancer xenograft model, CCCR-NK92 cells demonstrated significant inhibition of tumor growth (40). NCT03656705 has been conducted in the First Affiliated Hospital of Xinxiang Medical University, which uses the CCCR-NK92 cells to treat NSCLC patients from 18 to 75 years. For SCLC, Liu et al. engineered DLL3-specific NK-92 cells and explored their potential in treating SCLC. DLL3-CAR NK-92 cells induce tumor regression in an H446-derived lung metastatic tumor model at a favorable safety threshold (41). The DLL3-CAR approach also started a clinical trial in Tianjin Medical University Cancer Institute and Hospital to treat SCLC patients from 18 to 75 years old (NCT05507593). In addition to the abovementioned two studies that have carried out clinical trials, NK-92MI cells carrying an anti-B7-H3 CAR (second-generation CAR) effectively restricted the growth of transplanted non-small cell lung cancer in mice, significantly prolonging the survival time compared to unmodified NK-92MI cells (42). Mesenchymal–epithelial transition factor (C-Met) has been acknowledged as a significant therapeutic target for treating lung adenocarcinoma (LUAD). Anti-c-Met scFv, transmembrane domain of NKG2D, and cytoplasmic signaling domain of CD137, 2B4, DAP10, and CD3ζ were employed to construct four c-Met-CAR structures with different combinations (CC1, CC2, CC3, CC4). The tumor-inhibitory role of c-Met-CAR-NK cells was finally evaluated in vitro and in vivo (43).
While these therapies offer promising avenues for improving patient outcomes, they also face significant challenges that must be addressed to fully realize their potential. One of the primary challenges in CAR-NK cell therapy is the immunosuppressive nature of the tumor microenvironment (TME) in lung cancer. The TME can inhibit NK cell activation and function through various mechanisms, including the expression of inhibitory molecules [e.g., PD-L1 (44)] and the presence of immunosuppressive cells [e.g., Tregs (45), myeloid-derived suppressor cells (46)]. Overcoming the immunosuppressive barriers of the TME is crucial for enhancing the efficacy of CAR-NK cell therapies. Besides TME, the persistence and effective trafficking of CAR-NK cells to tumor sites are crucial for their antitumor activity. However, current CAR-NK cell therapies often face challenges with limited in vivo persistence and inefficient migration to the tumor site, which can significantly reduce their therapeutic efficacy (32). Tumor heterogeneity and the emergence of antigen escape variants pose significant challenges to CAR-related cell therapies. Similar to the dilemma faced by CAR T therapy, the loss or downregulation of target antigens on tumor cells can lead to the evasion of CAR-NK cell-mediated recognition and destruction, contributing to relapse and treatment resistance (47).
To overcome these difficulties, future CAR-NK cell therapies for lung cancer should be carried out in these following directions: 1. Overcoming TME suppression: future strategies could focus on combining CAR-NK cell therapy with agents that modulate the TME, such as checkpoint inhibitors [e.g., anti-PD-1, anti-PD-L1 antibodies (48)] or agents targeting the suppressive cells within the TME. These combinations could enhance the efficacy of CAR-NK cells by reducing immunosuppression and promoting a more favorable tumor microenvironment for NK cell activity. 2. Enhancing CAR NK cell persistence and trafficking: advancements in genetic engineering could lead to the development of CAR-NK cells with enhanced persistence and trafficking capabilities. For example, incorporating genes that encode for chemokine receptors matching the chemokines secreted by tumor cells can improve the homing of CAR-NK cells to the tumor site. Additionally, genetic modifications that promote the survival and proliferation of NK cells in vivo could improve their persistence and antitumor activity. 3. Targeting multiple antigens: to counteract antigen escape, developing CAR-NK cells that target multiple tumor-associated antigens could be a promising approach. Designing multi-target CAR structures (third-generation CAR structure) could reduce the likelihood of tumor cells evading CAR-NK cell-mediated detection and destruction potentially leading to more durable responses (32, 40, 48). 4. Advancements in manufacturing technologies: innovations in bioprocessing and genetic engineering could streamline the production of CAR-NK cells, making it more efficient and cost effective. The development of “off-the-shelf” CAR-NK cell products from universal donor cells or induced pluripotent stem cells (iPSCs) could also address scalability issues and improve accessibility to CAR-NK cell therapies (38).
Lung cancer’s high mortality rate and global prevalence underscore the importance of continued research and development in its detection, treatment, and prevention. Primary prevention, like smoking cessation and reducing exposure to environmental risk factors, remains crucial. Advances in medical treatments and early detection strategies offer hope for improved outcomes in lung cancer patients. CAR- NK cell therapy represents a promising avenue for the treatment of lung cancer offering potential advantages over traditional therapies, including reduced risk of CRS and GvHD, and the ability to target and kill cancer cells through innate immune mechanisms. However, addressing the challenges of TME suppression, CAR-NK cell persistence, antigen escape, and scalability is essential for the successful development and clinical implementation of these therapies. Future research and technological advancements will play a critical role in overcoming these obstacles and unlocking the full therapeutic potential of CAR-NK cell therapy for patients with lung cancer.
This review highlights the importance of continued research and collaboration across disciplines to address the complex challenges facing CAR-NK cell therapy in lung cancer. By leveraging advances in genetic engineering, immunology, and manufacturing technologies, there is significant potential to improve the efficacy, safety, and accessibility of CAR-NK cell therapies, offering new hope to patients with lung cancer.
XS: Investigation, Supervision, Writing – original draft, Writing – review & editing. FL: Writing – original draft, Writing – review & editing. XM: Data curation, Methodology, Writing – review & editing. LH: Investigation, Methodology, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
3. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet Lond Engl. (2021) 398:535–54. doi: 10.1016/S0140–6736(21)00312–3
4. Mamdani H, Matosevic S, Khalid AB, Durm G, Jalal SI. Immunotherapy in lung cancer: current landscape and future directions. Front Immunol. (2022) 13:823618. doi: 10.3389/fimmu.2022.823618
5. Bonini C, Mondino A. Adoptive T-cell therapy for cancer: The era of engineered T cells. Eur J Immunol. (2015) 45:2457–69. doi: 10.1002/eji.201545552
6. Gong Y, Klein Wolterink RGJ, Wang J, Bos GMJ, Germeraad WTV. Chimeric antigen receptor natural killer (CAR-NK) cell design and engineering for cancer therapy. J Hematol OncolJ Hematol Oncol. (2021) 14:73. doi: 10.1186/s13045–021-01083–5
7. Xie G, Dong H, Liang Y, Ham JD, Rizwan R, Chen J. CAR-NK cells: A promising cellular immunotherapy for cancer. eBioMedicine. (2020) 59:102975. doi: 10.1016/j.ebiom.2020.102975
8. Zhang C, Oberoi P, Oelsner S, Waldmann A, Lindner A, Tonn T, et al. Chimeric antigen receptor-engineered NK-92 cells: an off-the-shelf cellular therapeutic for targeted elimination of cancer cells and induction of protective antitumor immunity. Front Immunol. (2017) 8:533. doi: 10.3389/fimmu.2017.00533
9. Romanski A, Uherek C, Bug G, Seifried E, Klingemann H, Wels WS, et al. CD19-CAR engineered NK-92 cells are sufficient to overcome NK cell resistance in B-cell Malignancies. J Cell Mol Med. (2016) 20:1287–94. doi: 10.1111/jcmm.12810
10. Heim C, Moser LM, Kreyenberg H, Bonig HB, Tonn T, Wels WS, et al. ErbB2 (HER2)-CAR-NK-92 cells for enhanced immunotherapy of metastatic fusion-driven alveolar rhabdomyosarcoma. Front Immunol. (2023) 14:1228894. doi: 10.3389/fimmu.2023.1228894
11. Ma R, Lu T, Li Z, Teng KY, Mansour AG, Yu M, et al. An oncolytic virus expressing IL15/IL15Rα Combined with off-the-shelf EGFR-CAR NK cells targets glioblastoma. Cancer Res. (2021) 81:3635–48. doi: 10.1158/0008–5472.CAN-21–0035
12. Howlader N, Forjaz G, Mooradian MJ, Meza R, Kong CY, Cronin KA, et al. The effect of advances in lung-cancer treatment on population mortality. N Engl J Med. (2020) 383:640–9. doi: 10.1056/NEJMoa1916623
13. Da Cunha Santos G, Shepherd FA, Tsao MS. EGFR mutations and lung cancer. Annu Rev Pathol Mech Dis. (2011) 6:49–69. doi: 10.1146/annurev-pathol-011110–130206
14. Li BT, Smit EF, Goto Y, Nakagawa K, Udagawa H, Mazières J, et al. Trastuzumab deruxtecan in HER2 -mutant non–small-cell lung cancer. N Engl J Med. (2022) 386:241–51. doi: 10.1056/NEJMoa2112431
15. Hayashi H, Nakagawa K. Combination therapy with PD-1 or PD-L1 inhibitors for cancer. Int J Clin Oncol. (2020) 25:818–30. doi: 10.1007/s10147–019-01548–1
16. Liu WN, So WY, Harden SL, Fong SY, Wong MXY, Tan WWS, et al. Successful targeting of PD-1/PD-L1 with chimeric antigen receptor-natural killer cells and nivolumab in a humanized mouse cancer model. Sci Adv. (2022) 8:eadd1187. doi: 10.1126/sciadv.add1187
17. Xie M, Wu XJ, Zhang JJ, He CS. IL-13 receptor α2 is a negative prognostic factor in human lung cancer and stimulates lung cancer growth in mice. Oncotarget. (2015) 6:32902–13. doi: 10.18632/oncotarget.5361
18. Wallstabe L, Göttlich C, Nelke LC, Kühnemundt J, Schwarz T, Nerreter T, et al. ROR1-CAR T cells are effective against lung and breast cancer in advanced microphysiologic 3D tumor models. JCI Insight. (2019) 4:e126345, 126345. doi: 10.1172/jci.insight.126345
19. Esaki N, Ohkawa Y, Hashimoto N, Tsuda Y, Ohmi Y, Bhuiyan RH, et al. ASC amino acid transporter 2, defined by enzyme-mediated activation of radical sources, enhances Malignancy of GD2-positive small-cell lung cancer. Cancer Sci. (2018) 109:141–53. doi: 10.1111/cas.13448
20. Edelman M, Dvorkin M, Laktionov KK, Navarro A, Juan-Vidal O, Kozlov V, et al. The anti-disialoganglioside (GD2) antibody dinutuximab (D) for second-line treatment (2LT) of patients (pts) with relapsed/refractory small cell lung cancer (RR SCLC): Results from part II of the open-label, randomized, phase II/III distinct study. J Clin Oncol. (2020) 38:9017–7. doi: 10.1200/JCO.2020.38.15_suppl.9017
21. Kachala SS, Bograd AJ, Villena-Vargas J, Suzuki K, Servais EL, Kadota K, et al. Mesothelin overexpression is a marker of tumor aggressiveness and is associated with reduced recurrence-free and overall survival in early-stage lung adenocarcinoma. Clin Cancer Res. (2014) 20:1020–8. doi: 10.1158/1078–0432.CCR-13–1862
22. Wang Y, Wang J, Yang X, Yang J, Lu P, Zhao L, et al. Chemokine receptor CCR2b enhanced anti-tumor function of chimeric antigen receptor T cells targeting mesothelin in a non-small-cell lung carcinoma model. Front Immunol. (2021) 12:628906. doi: 10.3389/fimmu.2021.628906
23. Zhou R, Yazdanifar M, Roy LD, Whilding LM, Gavrill A, Maher J, et al. CAR T cells targeting the tumor MUC1 glycoprotein reduce triple-negative breast cancer growth. Front Immunol. (2019) 10:1149. doi: 10.3389/fimmu.2019.01149
24. Lin Y, Chen S, Zhong S, An H, Yin H, McGowan E. Phase I clinical trial of PD-1 knockout anti-MUC1 CAR-T cells in the treatment of patients with non-small cell lung cancer. Ann Oncol. (2019) 30:xi12. doi: 10.1093/annonc/mdz448
25. Galindo HG, Suraokar M, Behrens C, Woods DM, Kalhor N, Aldape KD, et al. Abstract 5166: Identification of prostate stem cell antigen (PSCA) as a potential marker for lung cancer brain metastasis. Cancer Res. (2011) 71:5166–6. doi: 10.1158/1538–7445.AM2011–5166
26. Wei X, Lai Y, Li J, Qin L, Xu Y, Zhao R, et al. PSCA and MUC1 in non-small-cell lung cancer as targets of chimeric antigen receptor T cells. OncoImmunology. (2017) 6:e1284722. doi: 10.1080/2162402X.2017.1284722
27. Owen DH, Giffin MJ, Bailis JM, Smit MAD, Carbone DP, He K. DLL3: an emerging target in small cell lung cancer. J Hematol OncolJ Hematol Oncol. (2019) 12:61. doi: 10.1186/s13045–019-0745–2
28. Amato KR, Wang S, Tan L, Hastings AK, Song W, Lovly CM, et al. EPHA2 blockade overcomes acquired resistance to EGFR kinase inhibitors in lung cancer. Cancer Res. (2016) 76:305–18. doi: 10.1158/0008–5472.CAN-15–0717
29. Regina S, Rollin J, Bléchet C, Iochmann S, Reverdiau P, Gruel Y. Tissue factor expression in non-small cell lung cancer: relationship with vascular endothelial growth factor expression, microvascular density, and K-ras mutation. J Thorac Oncol. (2008) 3:689–97. doi: 10.1097/JTO.0b013e31817c1b21
30. Jie Y, Liu G, Feng L, Li Y, E M, Wu L, et al. PTK7-targeting CAR T-cells for the treatment of lung cancer and other Malignancies. Front Immunol. (2021) 12:665970. doi: 10.3389/fimmu.2021.665970
31. Mehta RS, Rezvani K. Chimeric antigen receptor expressing natural killer cells for the immunotherapy of cancer. Front Immunol. (2018) 9:283. doi: 10.3389/fimmu.2018.00283
32. Wang W, Liu Y, He Z, Li L, Liu S, Jiang M, et al. Breakthrough of solid tumor treatment: CAR-NK immunotherapy. Cell Death Discovery. (2024) 10:40. doi: 10.1038/s41420–024-01815–9
33. Liu E, Marin D, Banerjee P, Macapinlac HA, Thompson P, Basar R, et al. Use of CAR-transduced natural killer cells in CD19-positive lymphoid tumors. N Engl J Med. (2020) 382:545–53. doi: 10.1056/NEJMoa1910607
34. Aparicio C, Acebal C, González-Vallinas M. Current approaches to develop “off-the-shelf” chimeric antigen receptor (CAR)-T cells for cancer treatment: a systematic review. Exp Hematol Oncol. (2023) 12:73. doi: 10.1186/s40164-023-00435-w
35. Castelli S, Young RM, June CH. Off-the-shelf CAR T cells to treat cancer. Cell Res. (2022) 32:1036–7. doi: 10.1038/s41422–022-00745–4
36. Childs RW, Carlsten M. Therapeutic approaches to enhance natural killer cell cytotoxicity against cancer: the force awakens. Nat Rev Drug Discovery. (2015) 14:487–98. doi: 10.1038/nrd4506
37. Herrera L, Santos S, Vesga MA, Anguita J, Martin-Ruiz I, Carrascosa T, et al. Adult peripheral blood and umbilical cord blood NK cells are good sources for effective CAR therapy against CD19 positive leukemic cells. Sci Rep. (2019) 9:18729. doi: 10.1038/s41598-019-55239-y
38. Goldenson BH, Zhu H, Wang YM, Heragu N, Bernareggi D, Ruiz-Cisneros A, et al. Umbilical cord blood and iPSC-derived natural killer cells demonstrate key differences in cytotoxic activity and KIR profiles. Front Immunol. (2020) 11:561553. doi: 10.3389/fimmu.2020.561553
39. Klingemann H, Boissel L, Toneguzzo F. Natural killer cells for immunotherapy – advantages of the NK-92 cell line over blood NK cells. Front Immunol. (2016) 7:91. doi: 10.3389/fimmu.2016.00091
40. Lu C, Guo C, Chen H, Zhang H, Zhi L, Lv T, et al. A novel chimeric PD1-NKG2D-41BB receptor enhances antitumor activity of NK92 cells against human lung cancer H1299 cells by triggering pyroptosis. Mol Immunol. (2020) 122:200–6. doi: 10.1016/j.molimm.2020.04.016
41. Liu M, Huang W, Guo Y, Zhou Y, Zhi C, Chen J, et al. CAR NK-92 cells targeting DLL3 kill effectively small cell lung cancer cells in vitro and in vivo. J Leukoc Biol. (2022) 112:901–11. doi: 10.1002/JLB.5MA0122-467R
42. Yang S, Cao B, Zhou G, Zhu L, Wang L, Zhang L, et al. Targeting B7-H3 immune checkpoint with chimeric antigen receptor-engineered natural killer cells exhibits potent cytotoxicity against non-small cell lung cancer. Front Pharmacol. (2020) 11:1089. doi: 10.3389/fphar.2020.01089
43. Peng Y, Zhang W, Chen Y, Zhang L, Shen H, Wang Z, et al. Engineering c-Met-CAR NK-92 cells as a promising therapeutic candidate for lung adenocarcinoma. Pharmacol Res. (2023) 188:106656. doi: 10.1016/j.phrs.2023.106656
44. Wang M, Zhu L, Yang X, Li J, Liu Y, Tang Y. Targeting immune cell types of tumor microenvironment to overcome resistance to PD-1/PD-L1 blockade in lung cancer. Front Pharmacol. (2023) 14:1132158. doi: 10.3389/fphar.2023.1132158
45. Dykema AG, Zhang J, Cheung LS, Connor S, Zhang B, Zeng Z, et al. Lung tumor–infiltrating T reg have divergent transcriptional profiles and function linked to checkpoint blockade response. Sci Immunol. (2023) 8:eadg1487. doi: 10.1126/sciimmunol.adg1487
46. Bronte G, Calabrò L, Olivieri F, Procopio AD, Crinò L. The prognostic effects of circulating myeloid-derived suppressor cells in non-small cell lung cancer: systematic review and meta-analysis. Clin Exp Med. (2022) 23:1551–61. doi: 10.1007/s10238–022-00946–6
47. Furqan F, Shah NN. Multispecific CAR T cells deprive lymphomas of escape via antigen loss. Annu Rev Med. (2023) 74:279–91. doi: 10.1146/annurev-med-042921–024719
Keywords: lung cancer, CAR-NK, immunotherapy, therapy, target
Citation: Liu F, Miao X, Han L and Song X (2024) Advances in CAR-NK cell therapy for lung cancer: is it a better choice in the future? Front. Oncol. 14:1390006. doi: 10.3389/fonc.2024.1390006
Received: 22 February 2024; Accepted: 22 April 2024;
Published: 28 May 2024.
Edited by:
Massimo Fantini, Precision Biologics, Inc., United StatesReviewed by:
Dorine De Jong, RefleXion Medical, United StatesCopyright © 2024 Liu, Miao, Han and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiao Song, MTM5NjQ2NTM3ODNAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.