 Cindy A. Nájera-Muñoz1
Cindy A. Nájera-Muñoz1 Raúl Hernández-Romero
Raúl Hernández-Romero Rosa A. Salcedo-Hernández
Rosa A. Salcedo-Hernández- 1Gynecology Oncology Division, High Speciality Hospital Christus Muguerza, Monterrey, Nuevo Leon, Mexico
- 2Gynecology Oncology Division, National Cancer Institute (INCan) of Mexico, Mexico City, Mexico
Introduction: Cervical cancer is a public health problem in our country and worldwide. Less than 25% of cases are diagnosed in the early stages, where survival is more remarkable than 90% at five years. Here, we review surgical treatment in the early stages of cervical cancer.
Methodology: A literature review was carried out in the MEDLINE database. The search was mainly limited to the English language, with priority given to systematic reviews with or without meta-analysis and randomized studies. However, only retrospective or observational evidence was found for some topics.
Results: The standard treatment for early-stage cervical cancer is hysterectomy, and its radical nature will depend on the tumor size, lymphovascular permeation, and tumor-specific prognostic factors. Furthermore, the type of surgery (hysterectomy or trachelectomy) will rely on the patient’s desire to preserve fertility. Nodal evaluation is indicated as part of the treatment from stage IAI with PLV. However, the sentinel lymph node is more relevant in the treatment. The incidental finding of cervical cancer after a hysterectomy requires a multidisciplinary evaluation to determine the therapeutic approach. Less radical surgery has been described as oncologically safe in low-risk groups.
Conclusion: Surgical treatment in its early stages has evolved in recent decades, making it more individualized and seeking less morbidity in patients without compromising their survival.
Introduction
Cervical cancer (CC) represents a significant public health issue, ranking as the fourth most common neoplasm in women worldwide in terms of both incidence and mortality. Eighty-five percent of patients with this diagnosis reside in low-income countries, and despite the existence of effective primary and secondary prevention measures, diagnosis often occurs at advanced stages (1).
In the early stages, the standard treatment involves hysterectomy and node evaluation (bilateral pelvic lymphadenectomy). The extent of hysterectomy varies depending on the disease’s conditions and the patient’s desires regarding fertility preservation. However, in recent years, there has been a shift towards less radical surgery in low-risk patients and the incorporation of sentinel lymph node procedures. However, it is important to mention the necessity of conducting an appropriate diagnostic approach and staging the patient to determine the treatment. In 2018, FIGO updated this staging, where clinical, radiological, and pathological findings (if available) will be part of the criteria to determine the clinical stage of the disease. Imaging studies (ultrasound, computed tomography imaging, magnetic resonance imaging, and PET-CT) used will depend on their availability and access; however, it is important to utilize all available tools to determine the clinical stage of the patient (2).
A thorough review of the literature and critical evaluation of it was conducted concerning the surgical treatment of early-stage cervical cancer. The search was restricted to evidence in English and the MEDLINE database, with priority given to controlled, randomized studies and systematic reviews with meta-analyses. However, all available evidence was examined in cases where such studies were lacking on certain topics.
Methods
A literature review was conducted by 4 individuals in the MEDLINE database using PUBMED and OVID search engines. The search was primarily limited to English, Spanish, and Italian language literature, with priority given to systematic reviews with or without meta-analysis and randomized studies. The identified studies were screened by the authors based on the abstract, and the chosen articles were retrieved for full reading and analysis. The quality of articles included in this review was assessed using GRADE and risk of bias tools. In the initial search including the mesh terms “Uterine cervical neoplasms” and “surgical procedures, operative”, the search retrieved 28,263 articles, those in other languages different to English, Spanish and Italian were excluding, remaining 23,864 cases. From this, the articles corresponding to randomized clinical trials and systematic reviews were considered, remaining 380; then, after reviewing the abstracts of the articles, manuscripts about advanced stages and rare subtypes were excluded, remaining 62 references. Finally, after reading the full papers, 14 were excluded because they were from the same group of investigators (duplicated information or follow-up in different times of the same cohort, etc.), the authors included patients with advanced disease, or the title and abstract were misleading about the treatment or the stage. In total, 48 articles were included.
Surgical treatment
Hysterectomy
Surgery is the cornerstone of treatment for patients with cervical cancer (CC) in the early clinical stage (for this paper the FIGO staging 2018 is used). The radical nature of the surgery, as per the Querleu-Morrow classification, is determined based on tumor size and the presence of lymphvascular permeation (LVP) in tumors with microinvasion. The choice between hysterectomy or trachelectomy is influenced by the patient’s desire to preserve fertility. In cases where surgery is contraindicated, radiotherapy becomes the treatment of choice, yielding similar oncological outcomes but with a different toxicity profile (3).
Historically, the Piver classification was utilized to describe the radicality of hysterectomy. However, it had limitations regarding anatomical description. Therefore, Querleu-Morrow introduced a new classification in 2008 based on anatomical references and avascular spaces, leading to improved standardization of procedures globally (4).
Clinical Stage IA1
Cervical cancer in clinical stage IA1 is classified as microinvasive (stromal invasion < 3 mm). The radical nature of hysterectomy is determined by the presence or absence of LVP, as it correlates with lymph node involvement and recurrence (5). Patients without LVP have a lymph node involvement probability of less than 1%, thus indicating a simple hysterectomy (type A) without lymph node evaluation (6). For patients with LVP, the risk of lymph node involvement increases to 3 to 5%. Therefore, a type B hysterectomy with lymph node evaluation is recommended (5).
Clinical Stage IA2
In the IA2 clinical stage, the probability of lymph node involvement ranges from 5% to 13% (7). It is recommended to perform a type B hysterectomy with lymph node evaluation (8).
Stages IB1, IB2, and IIA1
For patients with stages IB1, IB2, or selected IIA1 clinical stages, the recommended treatment is a type C1 hysterectomy with lymph node evaluation (bilateral pelvic lymphadenectomy BLP, or node sentinel GC) (8). The likelihood of ovarian metastasis is 0.9% in squamous cell carcinoma, permitting consideration for ovarian preservation in premenopausal patients. However, in adenocarcinoma, the probability of ovarian metastasis increases to 5%, warranting bilateral salpingo-oophorectomy (BSO) in some cases (9).
Highlights:
1. Standard treatment for stage IA1 CC without LVP is a type A or cone hysterectomy, primarily due to fertility preservation, without lymph node evaluation.
2. Treatment for stage IA1 with PLV and IA2 involves a type B radical hysterectomy and bilateral pelvic lymphadenectomy (BPL) + pelvic para-aortic lymphadenectomy (PPAL).
3. For stages IB1, IB2, and selected IIA1 CC, radical hysterectomy type C1 and BPL + PPAL are recommended.
4. Ovarian preservation may be considered in premenopausal patients with cervical cancer and squamous cell histology.
Fertility preservation
In patients with stage IA1 CC without PLV who wish to preserve fertility, performing a cone with negative margins without lymph node evaluation is recommended (10). For patients with stages IA2 and IB1, less than 2 cm without LVP, stromal involvement of less than 10 mm, squamous cell carcinoma histology, and adenocarcinoma, a simple cone or trachelectomy with lymph node evaluation could be considered, with a recurrence risk of less than 4% (10). However, if there is PLV, radical trachelectomy with lymph node evaluation is necessary (11). The use of neoadjuvant chemotherapy for patients with early-stage CC with tumors >2 cm who wish to preserve fertility and seek to reduce tumor size is under investigation. Currently, only retrospective studies have shown promising results, both oncologically and obstetrically (12). Currently, the CONTESSA study is ongoing, which is a prospective study with a primary objective of evaluate the feasibility of fertility preservation after neoadjuvant chemotherapy (platinum/paclitaxel) in patients with stage IB2 (2–4cm) CC, however; this is far from an efficacy study. Because there are no randomized studies that demonstrate the oncological safety of neoadjuvant chemotherapy in this setting, this type of treatment cannot be considered standard of care (13).
Highlights:
- Cone is indicated in stage IA1 without LVP.
- Cone or simple trachelectomy may be considered in stages IA2 and IB1 with low-risk factors.
- Radical trachelectomy is indicated in stages IA2 and IB1 with LVP.
- Neoadjuvant chemotherapy for tumor size reduction in patients wishing to preserve fertility is not recommended as a standard treatment.
Surgical approach
Since the first description of laparoscopic radical hysterectomy by Nezhat et al. in 1992, this approach has demonstrated feasibility and safety (14). Retrospective studies on laparoscopic approaches in cervical cancer treatment consistently showed benefits of minimally invasive surgery with similar oncological outcomes to open surgery (15–17).
In 2018, the multicenter randomized phase III LACC trial (18) was published, demonstrating that minimally invasive radical hysterectomy was associated with lower rates of disease-free survival and overall survival compared to open abdominal radical hysterectomy in early-stage FIGO 2018 stage IA1 cervical cancer with LVP to IB2. Following this study, treatment guidelines revised their recommendations, favoring open surgery as the approach of choice for early cervical cancer treatment, with minimally invasive approaches reserved for IA1 cervical cancer without LVP and research protocols for others early stages (19–21).
After this change in clinical practice, researchers have explored if there is a subset of patients who could benefit from minimally invasive approaches or if specific maneuvers to avoid tumor manipulation could mitigate the increased risk of recurrence and mortality associated with minimally invasive surgery. However, all published studies are large retrospective cohorts with inherent selection biases, necessitating caution in interpreting their recommendations (22, 23).
Highlights:
1. Standard surgical management in early-stage cervical cancer FIGO 2018: 1A1 with lymphovascular invasion to IB2 is open surgery.
2. Minimally invasive surgery (laparoscopy and robotics) is not recommended for early-stage invasive cervical cancer.
3. Minimally invasive procedures should only be performed within research protocols for cervical cancer.
Sentinel lymph node
In patients with apparent early-stage CC, nodal status stands as the most crucial prognostic factor (24, 25). The standard treatment involves hysterectomy or radical trachelectomy with pelvic lymphadenectomy. However, lymph node metastases are detectable in only approximately 15–20% of cases treated with surgery (26), this implies that 80–85% of patients could undergo unnecessary surgical overtreatment, exposing them to procedural morbidity such as lymphoceles and lymphedema (27, 28). The sentinel lymph node (SLN) serves as the initial nodal basin receiving tumor lymphatic drainage, indicating the status of other lymph nodes in the region. This concept allows for avoiding complete lymphadenectomy (29) and this technique (SLN) has been regularly and safely employed in gynecological malignancies like vulvar and endometrial cancer. Presently, active prospective protocols (SENTIX, SENTICOL III, PHENIX) aim to establish the oncological safety of SLN use without pelvic lymphadenectomies and we wait the results in coming years (30–32).
International guidelines, such as ESGO/ESTRO/ESP, recommend SLN as the initial step in surgery, subjecting it to intraoperative evaluation to determine further surgical management, including completing pelvic lymphadenectomy or referral for chemoradiotherapy (33). NCCN recommends SLN in selected stage I cases (<2 cm) and remove the suspicious or enlarged lymph nodes; also, advises lymphadenectomy if SLN mapping fail. FIGO suggests SLN only for stages IA1 and IA2, awaiting further evidence for routine use (2).
Evaluation and size of metastases in the sentinel lymph node
Nodal involvement encompasses macrometastasis (MM; tumor deposit >2 mm), micrometastasis (MIM; tumor deposit >0.2 mm up to 2 mm), and isolated tumor cells (ITC tumor deposit up to 0.2 mm). According to TNM 8, MM is considered pN1, MIM pN1(mi), and ITC pN0 (34, 35). Studies have yet to define the prognostic impact of these distinctions.
SLN evaluation is more precise than pelvic lymphadenectomy due to ultrastaging, which increases the likelihood of detecting MIM. Multiple studies, both retrospective and prospective, demonstrate high sensitivity of SLN for detecting lymph node involvement. For instance, the prospective French SENTICOL study reported a sensitivity of 92% and a negative predictive value of 98.2% (36). Similarly, a significant retrospective study analyzing SLN sensitivity in CC reported 91% sensitivity in the entire cohort and 97% in the bilateral migration subgroup (37).
Debate surrounds the intraoperative evaluation of SLN due to its low sensitivity (53–89%) and increased tissue management complexity, potentially resulting in undetected MIM, ITC and even MM (38, 39). Nevertheless, intraoperative evaluation can detect most MM (82.1%), potentially avoiding combined treatment if surgery is abandoned, and the patient is referred for primary chemoradiation (40). Therefore, patients should be informed before surgery that despite negative intraoperative SLN evaluation, metastases may be identified later in 30–50% of cases with ultrastaging (41).
Technical recommendations
ESGO/ESTRO/ESP guidelines endorse performing SLN with indocyanine green (ICG) as the preferred technique, another technique is combined blue dye and radiocolloid. A non-inferiority study, “FILM,” comparing ICG and isosulfan blue, demonstrated better ICG detection rates (42). ICG offers advantages over patent blue, reducing the risk of anaphylaxis, and over radiotracer, as it avoids handling radioactive materials.
For radioisotope use, specifically Technetium-99, two injection protocols exist: a long one with 120 MBq injected one day preoperatively and a short one with 60 MBq injected on the morning of the operation. It is advisable to combine lymphoscintigraphy with patent blue. For colorimetric methods, blue dye or ICG is used, with injections performed superficially and deeply once surgery has commenced, as dye migration occurs within 10 to 15 minutes (42, 43).
The initial step involves verifying lymphatic channel migration with the peritoneum closed, followed by exploration of external iliac territories, iliac bifurcation, and obturator region, ensuring complete exposure of relevant structures. Lymph nodes should not be removed without visualizing their afferent channel to avoid resecting non-sentinel nodes. Systematic searching for routes and SLN in atypical territories should be conducted (43).
No specific CC study provides information regarding the number of cases constituting the learning curve. However, some retrospective studies on endometrial cancer suggest around 30 to 40 cases (44, 45).
Highlights: In the Table 1 we show the main articles about this topic.
1. Standard lymph node evaluation in early-stage CC involves bilateral pelvic lymphadenectomy.
2. SLN can be considered in patients with stage IAI CC with PLV and IA2, IB1, IB2, and IIA1.
3. Intraoperative SLN study may be considered for patients at higher risk of lymph node involvement, balancing the risk of tissue loss for detecting micrometastases and isolated tumor cells.
4. Any suspicious lymph node should undergo intraoperative evaluation.
5. Preferred techniques include ICG, with patent blue + radiocolloid considered an acceptable alternative.
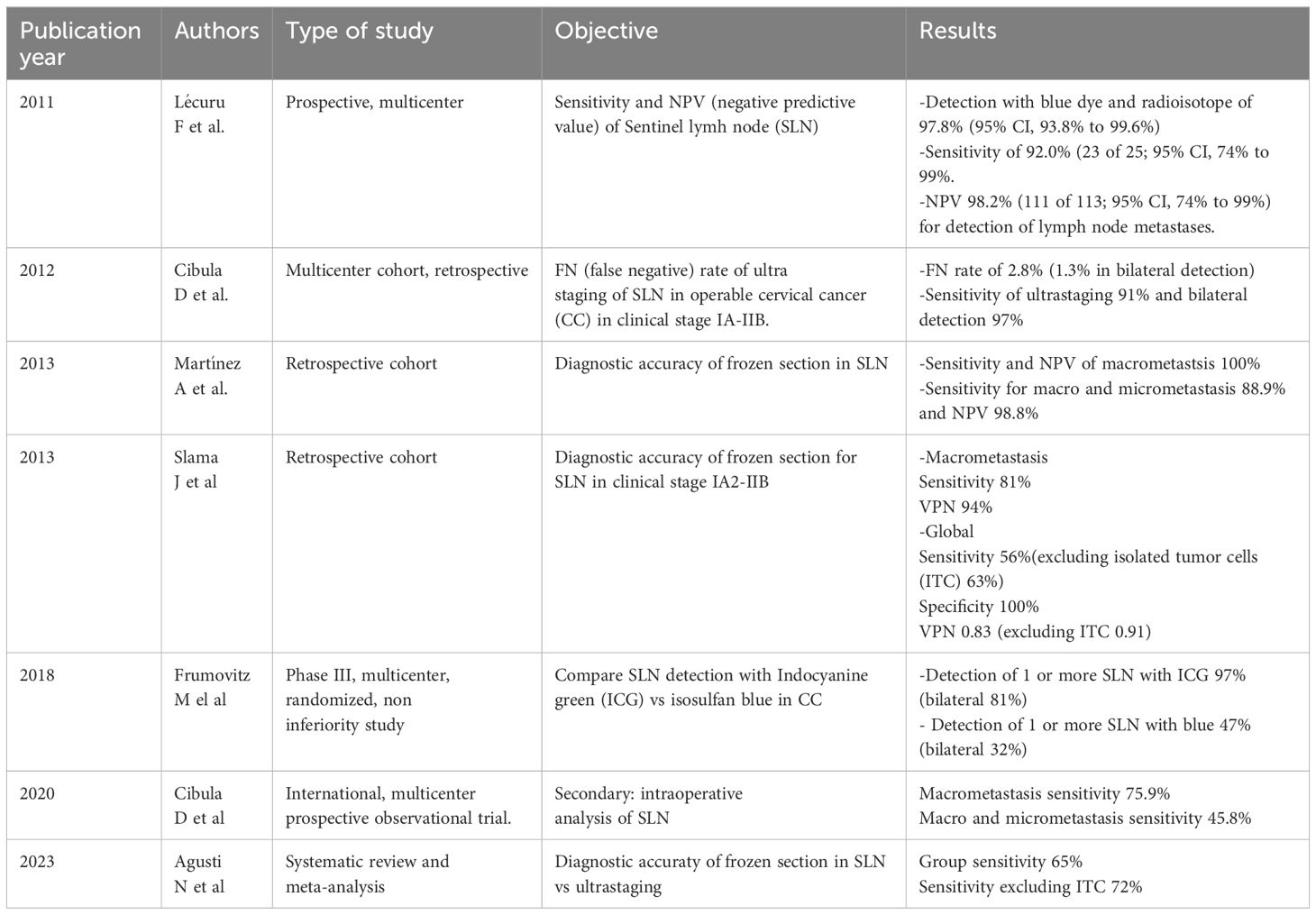
Table 1 Sentinel node articles reviewed.
Less than radical surgery
While radical hysterectomy/trachelectomy and bilateral pelvic lymphadenectomy constitute the standard treatment for cervical cancer, these procedures carry complications affecting quality of life (e.g., sexual and bladder dysfunction). Recent theories propose that low-risk patients, defined by specific tumor characteristics, could safely undergo less radical surgery, such as cone or extrafascial hysterectomy with lymph node evaluation. The ConCerv study demonstrated the feasibility of such less radical surgery in low-risk patients, with a 2-year recurrence pattern of 3.5% (9). The SHAPE study, a prospective phase III non-inferiority study comparing extrafascial hysterectomy against radical hysterectomy in low-risk patients (stage IA2 – IB1, squamous-cell carcinoma, adenocarcinoma or adenosquamous histology, tumors <2cm, with limited depth of cervical stromal invasion (less 10 mm) obtained by diagnostic loop electrosurgical excision procedure or conization or by preoperative pelvic magnetic resonance showing < 50% stromal invasion, w/not PLV); evidencing non- inferiority with a recurrence rate at 4.5 years (46), with less adverse events in extrafascial hysterectomy group however is necessary take these results with caution and know how to carefully select the patients who will benefit from this treatment.
Highlights
1. Low-risk cervical cancer patients may benefit from less radical surgery, such as type A/cone hysterectomy, with lymph node evaluation. However, awaiting SHAPE study publication for oncological safety confirmation is advised.
Incidental cervical cancer diagnosis after hysterectomy
The incidence of cervical cancer discovery after hysterectomy ranges from 3.5% to 1.9%, attributable to factors like inadequate preoperative evaluation or errors in clinical or pathology evaluation, leading to suboptimal treatment. Patients without residual disease by imaging studies post-hysterectomy may benefit from complementary surgery + adjuvant treatment, demonstrating improved survival compared to those without complementary surgery, nevertheless is necessary to evaluate each case and evaluated the patient (functional status, presence of comorbidities, etc.), histology subtype and tumor characteristics to choose the best treatment. Subgroup analyses suggest observation may suffice for select patients, but this warrants further study (47, 48).
Highlights
1. Pathology review by an expert is essential post-hysterectomy.
2. Imaging studies should assess residual disease presence.
3. Multidisciplinary team evaluation is crucial.
4. Patients with residual disease or adverse prognostic factors should receive standard treatment.
5. Complementary surgery consideration should align with disease prognostic factors and treatment necessity.
Conclusion
Cervical cancer treatment has evolved to become increasingly individualized, necessitating a multidisciplinary team approach considering tumor characteristics and patient preferences to determine the optimal therapeutic strategy.
Author contributions
CN-M: Writing – original draft, Writing – review & editing. RH-R: Writing – original draft, Writing – review & editing. DI-O: Writing – original draft, Writing – review & editing. RS-H: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. GLOBOCAN Estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2021 update. Int J Gynecol Obstet. (2021) 155(Suppl 1):28–44. doi: 10.1002/ijgo.13865
3. Bansal N, Herzog TJ, Shaw RE, Burke WM, Deutsch I, Wright JD. Primary therapy for early-stage cervical cancer: radical hysterectomy vs radiation. Am J Obstet Gynecol. (2009) 201(5):485.e1–9. doi: 10.1016/j.ajog.2009.06.015
4. Querleu D, Cibula D, Abu-Rustum NR. "2017 update on the Querleu–Morrow classification of radical hysterectomy. Ann Surg Oncol. (2017) 24:3406–12. doi: 10.1245/s10434-017-6031-z
5. Webb JC, Key CR, Qualls CR, Smith HO. Population-based study of microinvasive adenocarcinoma of the uterine cervix. Obstet Gynecol. (2001) 97(5):701–6. doi: 10.1016/s0029-7844(01)01330-8
6. Cormier B, Diaz JP, Shih K, Sampson RM, Sonoda Y, Park KJ, et al. Establishing a sentinel lymph node mapping algorithm for the treatment of early cervical cancer. Gynecologic Oncol. (2011) 122.2:275–80. doi: 10.1016/j.ygyno.2011.04.023
7. Buckley SL, Tritz DM, Van Le L, Higgins R, Sevin BU, Ueland FR, et al. Lymph node metastases and prognosis in patients with stage IA2Cervical cancer. Gynecologic Oncol. (1996) 63.1:4–9. doi: 10.1006/gyno.1996.0268
8. Covens A, Rosen B, Murphy J, Laframboise S, DePetrillo AD, Lickrish G, et al. How important is removal of the parametrium at surgery for carcinoma of the cervix? Gynecologic Oncol. (2002) 84.1:145–9. doi: 10.1006/gyno.2001.6493
9. Landoni F, Zanagnolo V, Lovato-Diaz L, Maneo A, Rossi R, Gadducci A, et al. Ovarian metastases in early-stage cervical cancer (IA2–IIA): a multicenter retrospective study of 1965 patients (a Cooperative Task Force study). " Int J Gynecological Cancer. (2007) 17.3:623–8. doi: 10.1111/j.1525-1438.2006.00854.x
10. Schmeler KM, Pareja R, Lopez Blanco A, Humberto Fregnani J, Lopes A, Perrotta M, et al. ConCerv: a prospective trial of conservative surgery for low-risk early-stage cervical cancer. Int J Gynecol Cancer. (2021) 31:1317–25. doi: 10.1136/ijgc-2021-002921
11. Abu-Rustum NR, Neubauer N, Sonoda Y, Park KJ, Gemignani M, Alektiar KM, et al. Surgical and pathologic outcomes of fertility-sparing radical abdominal trachelectomy for FIGO stage IBI cervical cancer. Gynecol Oncol. (2008) 111:261–4. doi: 10.1016/j.ygyno.2008.07.002
12. Gwacham NI, McKenzie ND, Fitzgerald ER, Ahmad S, Holloway RW. Neoadjuvant chemotherapy followed by fertility sparing surgery in cervical cancers size 2–4 cm; emerging data and future perspectives. Gynecol Oncol. (2021) 2021:809–815. doi: 10.1016/j.ygyno.2021.06.006
13. Plante M, van Trommel N, Lheureux S, Oza AM, Wang L, Sikorska K, et al. FIGO 2018 stage (2 – 4 cm). Cervical cancer treated with Neo-adjuvant chemotherapy followed by fertility sparing surgery (CONTESSA); Neo-adjuvant chemotherapy and conservative surgery in cervical cancer to preserve fertility (NEOCON-F). A PMHC, DGOG, GCIG/CCRN and multicenter study. Int J Gynecol Cancer. (2019) 29:969–75. doi: 10.1136/ijgc-2019-000398
14. Nezhat CR, Burrell MO, Nezhat FR, Benigno BB, Welander CE. Laparoscopic radical hysterectomy with paraaortic and pelvic node dissection. Am J Obstet Gynecol. (1992) 166:864–5. doi: 10.1016/0002-9378(92)91351-a
15. Li G, Yan X, Shang H, Wang G, Chen L, Han Y. A comparison of laparoscopic radical hysterectomy and pelvic lymphadenectomy and laparotomy in the treatment of Ib-IIa cervical cancer. Gynecologic Oncol. (2007) 105:176–80. doi: 10.1016/j.ygyno.2006.11.011
16. Garabedian C, Merlot B, Bresson L, Tresch E, Narducci F, Leblanc E. Minimally invasive surgical management of early-stage cervical cancer: an analysis of the risk factors of surgical complications and of oncologic outcomes. Int J Gynecol Cancer. (2015) 25:714–21. doi: 10.1097/IGC.0000000000000390
17. Wang YZ, Deng L, Xu HC, Zhang Y, Liang ZQ. Laparoscopy versus laparotomy for the management of early stage cervical cancer. BMC Cancer. (2015) 15:928. doi: 10.1186/s12885-015-1818-4
18. Ramirez PT, Frumovitz M, Pareja R, Lopez A, Vieira M, Ribeiro R, et al. Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N Engl J Med. (2018) 379:1895–904. doi: 10.1056/NEJMoa1806395
19. NCCN clinical practice guidelines in oncology (NCCN guidelines®) cervical cancer version 1 (2023). Available online at: https://www.nccn.orgguidelines.
20. Marth C, Landoni F, Mahner S, McCormack M, Gonzalez-Martin A, Colombo N. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2017) 28:iv72–83. doi: 10.1093/annonc/mdx220
21. NICE National Institute for Health and Care Excellence. Minimally invasive radical hysterectomy for early stage cervical câncer Interventional procedures guidance (2022). Available online at: www.nice.org.uk/guidance/ipg686.
22. Chiva L, Zanagnolo V, Querleu D, Martin-Calvo N, Arévalo-Serrano J, Căpîlna ME, et al. SUCCOR study: an international European cohort observational study comparing minimally invasive surgery versus open abdominal radical hysterectomy in patients with stage IB1 cervical cancer. Int J Gynecol Cancer. (2020) 30:1269–77. doi: 10.1136/ijgc-2020-001506
23. Leitao MM Jr, Zhou QC, Brandt B, Iasonos A, Sioulas V, Lavigne Mager K, et al. The MEMORY study: Multicenter study of minimally invasive surgery versus open radical hysterectomy in the management of early-stage cervical cancer: survival outcomes. Gynecol Oncol. (2022) 166:417–24. doi: 10.1016/j.ygyno.2022.07.002
24. Noguchi H, Shiozawa I, Sakai Y, Yamazaki T, Fukuta T. Pelvic lymph node metastasis of uterine cervical cancer. Gynecol Oncol. (1987) 27:150–8. doi: 10.1016/0090–8258(87)90287–3
25. Fuller AF, Elliott N, Kosloff C, Hoskins WJ, Lewis JL. Determinants of increased risk for recurrence in patients undergoing radical hysterectomy for stage IB and IIA carcinoma of the cervix. Gynecol Oncol. (1989) 33:34–9. doi: 10.1016/0090–8258(89)90598–2
26. Diaz JP, Sonoda Y, Leitao MM, Zivanovic O, Brown CL, Chi DS, et al. Oncologic outcome of fertility-sparing radical trachelectomy versus radical hysterectomy for stage IB1 cervical carcinoma. Gynecol Oncol. (2008) 111:255–60. doi: 10.1016/j.ygyno.2008.07.014
27. Levenback C, Coleman RL, Burke TW, Lin WM, Erdman W, Deavers M, et al. Lymphatic mapping and sentinel node identification in patients with cervix cancer undergoing radical hysterectomy and pelvic lymphadenectomy. J Clin Oncol. (2002) 20:688–93. doi: 10.1200/JCO.2002.20.3.688
28. Mathevet P, Lécuru F, Uzan C, Boutitie F, Magaud L, Guyon F, et al. Sentinel lymph node biopsy and morbidity outcomes in early cervical cancer: Results of a multicentre randomised trial (SENTICOL-2). Eur J Cancer. (2021) 148:307–15. doi: 10.1016/j.ejca.2021.02.009
29. Berveiller P, Mir O, Veyrie N, Barranger E. The sentinel-node concept: a dramatic improvement in breast-cancer surgery. Lancet Oncol. (2010) 11:906. doi: 10.1016/S1470-2045(09)70237-2
30. Tu H, Huang H, Xian B, Li J, Wang P, Zhao W, et al. Sentinel lymph node biopsy versus pelvic lymphadenectomy in early-stage cervical cancer: a multi-center randomized trial (PHENIX/CSEM 010). Int J Gynecol Cancer. (2020) 30:1829–33. doi: 10.1136/ijgc-2020-001857
31. Lecuru FR, McCormack M, Hillemanns P, Anota A, Leitao M, Mathevet P, et al. SENTICOL III: an international validation study of sentinel node biopsy in early cervical cancer. A GINECO, ENGOT, GCIG and multicenter study. Int J Gynecol Cancer. (2019) 29:829–34. doi: 10.1136/ijgc-2019-000332
32. Cibula D, Dusek J, Jarkovsky J, Dundr P, Querleu D, van der Zee A, et al. A prospective multicenter trial on sentinel lymph node biopsy in patients with early-stage cervical cancer (SENTIX). Int J Gynecol Cancer. (2019) 29:212–5. doi: 10.1136/ijgc-2018-000010
33. Cibula D, Raspollini MR, Planchamp F, Centeno C, Chargari C, Felix A, et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer – Update 2023*. Int J Gynecol Cancer. (2023) 33(5):649–66. doi: 10.1136/ijgc-2023-004429
34. Cibula D, McCluggage WG. Sentinel lymph node (SLN) concept in cervical cancer: Current limitations and unanswered questions. Gynecol Oncol. (2019) 152:202–7. doi: 10.1016/j.ygyno.2018.10.007
35. O'Sullivan B, Brierley J, Byrd D, Bosman F, Kehoe S, Kossary C, et al. The TNM classification of Malignant tumours—towards common understanding and reasonable expectations. Lancet Oncol. (2017) 18:849. doi: 10.1016/S1470–2045(17)30438–2
36. Lécuru F, Mathevet P, Querleu D, Leblanc E, Morice P, Daraï E, et al. Bilateral negative sentinel nodes accurately predict absence of lymph node metastasis in early cervical cancer: results of the SENTICOL study. J Clin Oncol. (2011) 29:1686–91. doi: 10.1200/JCO.2010.32.0432
37. Cibula D, Abu-Rustum NR, Dusek L, Slama J, Zikán M, Zaal A, et al. Bilateral ultrastaging of sentinel lymph node in cervical cancer: Lowering the false-negative rate and improving the detection of micrometastasis. Gynecol Oncol. (2012) 127:462–6. doi: 10.1016/j.ygyno.2012.08.035
38. Martínez A, Mery E, Filleron T, Boileau L, Ferron G, Querleu D. Accuracy of intraoperative pathological examination of SLN in cervical cancer. Gynecol Oncol. (2013) 130:525–9. doi: 10.1016/J.YGYNO.2013.01.023
39. Slama J, Dundr P, Dusek L, Cibula D. High false negative rate of frozen section examination of sentinel lymph nodes in patients with cervical cancer. Gynecol Oncol. (2013) 129:384–8. doi: 10.1016/J.YGYNO.2013.02.001
40. Agustí N, Viveros-Carreño D, Mora-Soto N, Ramírez PT, Rauh-Hain A, Wu C, et al. Diagnostic accuracy of sentinel lymph node frozen section analysis in patients with early-stage cervical cancer: A systematic review and meta-analysis. Gynecol Oncol. (2023) 177:157–64. doi: 10.1016/j.ygyno.2023.08.019
41. Lang-Avérous G, Croce S, Mery E, Devouassoux-Shisheboran M, et al. Sentinel lymph node processing in gynecological cancer histopathology and molecular biology. Chin Clin Oncol. (2021) 10:17. doi: 10.21037/cco-20-192
42. Frumovitz M, Plante M, Lee PS, Sandadi S, Lilja JF, Escobar PF. A randomized phase III multicenter study assessing near infrared fluorescence in the detection of sentinel lymph nodes in women with cervical and uterine cancers: the FILM Trial. Lancet Oncol. (2018) 19(10):1394–403.
43. Balaya V, Guani B, Bonsang-Kitzis H, Deloménie M, Ngô C, Montero Macias R, et al. Place du ganglion sentinelle dans les cancers du col utérin débutants. Bull Cancer. (2020) 107:696–706. doi: 10.1016/j.bulcan.2019.06.011
44. Kim S, Ryu KJ, Min KJ, Lee S, Jung US, Hong JH, et al. Learning curve for sentinel lymph node mapping in gynecologic Malignancies. J Surg Oncol. (2020) 121:599–604. doi: 10.1002/jso.25853
45. Tucker K, Staley SA, Gehrig PA, Soper JT, Boggess JF, Ivanova A, et al. Defining the learning curve for successful staging with sentinel lymph node biopsy for endometrial cancer among surgeons at an academic institution. Int J Gynecol Cancer. (2020) 30:346–51. doi: 10.1136/ijgc-2019-000942
46. Plante M, Kwon JS, Ferguson S, Samouëlian V, Ferron G, Maulard A, et al. Simple versus Radical Hysterectomy in Women with low-Risk Cervical Cancer. N Engl J Med. (2024) 390:819–29. doi: 10.1056/NEJMoa2308900
47. Bai H, Cao D, Yuan F, Wang H, Chen J, Wang Y, et al. Occult invasive cervical cancer after simple hysterectomy: a multi-center retrospective study of 89 cases. BMC Cancer. (2016) 16:507. doi: 10.1186/s12885-016-2480-1
48. Narducci F, Merlot B, Bresson L, Katdare N, Le Tinier F, Cordoba A, et al. Occult invasive cervical cancer found after inadvertent simple hysterectomy: Is the ideal management: Systematic parametrectomy with or without Radiotherapy o radiotherapy only? Ann Surg Oncol. (2015) 22:1349–52. doi: 10.1245/s10434-014-4140-5
Keywords: cervical cancer, surgical treatment, cervicouterine cancer, hysterectomy, sentinel lymph node
Citation: Nájera-Muñoz CA, Hernández-Romero R, Isla-Ortiz D and Salcedo-Hernández RA (2024) Mexican consensus about surgical treatment in early-stage cervicouterine cancer. Front. Oncol. 14:1385887. doi: 10.3389/fonc.2024.1385887
Received: 14 February 2024; Accepted: 28 May 2024;
Published: 19 June 2024.
Edited by:
Oscar Medina-Contreras, Mexico Children’s Hospital, MexicoReviewed by:
Nicolae Bacalbasa, Carol Davila University of Medicine and Pharmacy, RomaniaKemin Li, Sichuan University, China
Copyright © 2024 Nájera-Muñoz, Hernández-Romero, Isla-Ortiz and Salcedo-Hernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosa A. Salcedo-Hernández, cm9zYXNhbGhlckBnbWFpbC5jb20=
†ORCID: Raúl Hernández-Romero, orcid.org/0000-0002-6385-5503
David Isla-Ortiz, orcid.org/0000-0001-8987-8669
Rosa A. Salcedo-Hernández, orcid.org/0000-0003-4537-8034