
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 17 September 2024
Sec. Surgical Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1360936
This article is part of the Research TopicAdvancing Patient-Centric Oncology: Non-Operative Management and Surgical De-Escalation in Cancer CareView all 10 articles
 Emrullah Birgin1*
Emrullah Birgin1* Heiner Nebelung2
Heiner Nebelung2 Schaima Abdelhadi3
Schaima Abdelhadi3 Johann S. Rink4
Johann S. Rink4 Matthias F. Froelich4Svetlana Hetjens5
Matthias F. Froelich4Svetlana Hetjens5 Mohammad Rahbari3
Mohammad Rahbari3 Patrick Téoule3Erik Rasbach3
Patrick Téoule3Erik Rasbach3 Christoph Reissfelder3,6Jürgen Weitz7Stefan O. Schoenberg4Carina Riediger7Verena Plodeck2†Nuh N. Rahbari1†
Christoph Reissfelder3,6Jürgen Weitz7Stefan O. Schoenberg4Carina Riediger7Verena Plodeck2†Nuh N. Rahbari1†Background: Microvascular invasion is a major histopathological risk factor of postoperative recurrence in patients with hepatocellular carcinoma. This study aimed to develop and validate a digital biopsy model using imaging features to predict microvascular invasion before hepatectomy.
Methods: A total of 217 consecutive patients who underwent hepatectomy for resectable hepatocellular carcinoma were enrolled at two tertiary-care reference centers. An imaging-based digital biopsy model was developed and internally validated using logistic regression analysis with adjustments for age, sex, etiology of disease, size and number of lesions.
Results: Three imaging features, i.e., non-smoothness of lesion margin (OR = 16.40), ill-defined pseudocapsula (OR = 4.93), and persistence of intratumoral internal artery (OR = 10.50), were independently associated with microvascular invasion and incorporated into a prediction model. A scoring system with 0 - 3 points was established for the prediction model. Internal validation confirmed an excellent calibration of the model. A cutoff of 2 points indicates a high risk of microvascular invasion (area under the curve 0.87). The overall survival and recurrence-free survival stratified by the risk model was significantly shorter in patients with high risk features of microvascular invasion compared to those patients with low risk of microvascular invasion (overall survival: median 35 vs. 75 months, P = 0.027; recurrence-free survival: median 17 vs. 38 months, P < 0.001)).
Conclusion: A preoperative assessment of microvascular invasion by digital biopsy is reliable, easily applicable, and might facilitate personalized treatment strategies.
Hepatocellular carcinoma (HCC) is a major global health challenge with a rising incidence worldwide (1). HCC development is closely related to chronic liver disease with viral hepatitis, alcoholic and non-alcoholic steatohepatitis as leading etiologies (1). Due to the reliance on tumor burden and the functional hepatic reserve for determining patient treatment and outcomes, managing HCC proves exceptionally challenging (2). The complexity of this heterogenous disease and its treatment is reflected in markedly variable outcomes following potentially curative therapy such as surgical resection, liver transplantation, or local ablation (3). Patients undergoing these treatments typically exhibit a 5-year survival rate of approximately 62-70% (4, 5). Moreover, HCC recurrence in patients after potentially curative treatment remains a major burden with rates up to 70% within 5 years after treatment (6). Microvascular invasion (MVI), characterized by the microscopic presence of tumor cells in hepatic vessels (arteries, hepatic vein, and portal vein) lined with endothelial cells, stands as the most crucial determinant of disease recurrence and long-term survival (7). Unfortunately, MVI can only be histopathologically diagnosed based on the resected surgical specimen and therefore its use to guide personalized treatment strategies remains limited. Recently, the prediction of MVI before surgery has gained increasing attention, with several promising noninvasive methods utilizing imaging features or tumor markers embedded into risk models (8–12). However, current evidence is primarily characterized by complex risk models involving multimodal biomarkers, or restriction of imaging modalities to either magnetic resonance imaging (MRI) or computed tomography (CT) (13, 14). Furthermore, the vast majority of risk models were developed in selective subsets of HCC patients (i.e., predominantly viral hepatitis) with significant imbalances of the number of predictor variables and high MVI rates in the cohorts hampering its transferability to the clinical routine (12, 15, 16).
In this study, we aimed to develop a noninvasive digital biopsy risk model to predict MVI using preoperative imaging features and assess its prognostic outcome in patients undergoing hepatectomy for HCC.
This retrospective cohort study was approved by the institutional review board (2023–831) and conducted in line with the Declaration of Helsinki and the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) guidelines (17). All consecutive patients who underwent hepatectomy for HCC between April 2008 and June 2023 at the Department of Surgery, University Hospital Mannheim and Department of Gastrointestinal, Thoracic and Vascular Surgery, University Hospital Carl Gustav Carus at the Technische Universität Dresden were identified from prospectively recorded databases and screened for eligibility. Informed consent was obtained from each patient to store data on prospective databases. The following inclusion criteria were used: a) adult patients (age 18 years or older) who underwent hepatectomy in curative-intent for resectable HCC; b) histopathologically documented status of MVI; c) preoperative imaging including computed tomography (CT) and/or magnetic resonance imaging (MRI) within 3 months of surgery. We excluded patients who had an inadequate quality of imaging for the evaluation of imaging features associated with MVI, and patients with mixed-type HCC-cholangiocarcinoma.
Patient records were reviewed for clinical variables such as age, gender, underlying liver disease, presence of liver cirrhosis, Child-Pugh classification, preoperative treatment, preoperative laboratory values such as alanine-aminotransferase, aspartate-aminotransferase, albumin, bilirubin, platelet count, and international normalized ratio. Pathological data included the number of resected lesions (classified as single, oligonodular (2-3 lesions) or multinodular (> 3 lesions)) (18), the diameter of lesions, resection margin, and the presence of microvascular invasion. Operative details, including the type and extent of hepatectomy, were also extracted. The Brisbane classification was used to categorize liver resections (19). Major hepatectomy was defined as resections of four or more Couinaud segments. HCC lesions were considered for resection irrespective of lesion size if patients had resectable lesions (single or multifocal) with an adequate future liver remnant, liver function, and performance status as well as the absence of distant metastasis or portal vein thrombosis. Postoperative surveillance included routine abdominal multiphasic computed tomography or magnetic resonance imaging and chest radiography every three months. Dates of last follow-up, recurrence, and death were recorded to calculate overall- and recurrence-free survival from the time of hepatectomy. Recurrence-free survival was defined as the time from hepatectomy to the first documented disease recurrence (radiologic or histologic evidence of local, regional, or distant metastasis) or death by any cause.
Preoperative CT and MRI images were independently evaluated by two radiologists at each center who were blinded to clinical, surgical, pathologic, and follow-up results. At each center, discordance between two radiologists was solved by a third senior radiologist until consensus was generated. The presence of the following radiologic markers was assessed for its potential association with MVI as previously described in the literature (8, 10, 16, 20, 21): 1. extrahepatic growth pattern, i.e., exophytic lesions; 2. intratumoral hemorrhage; 3. intratumoral necrosis; 4. intratumoral vascularity, i.e. hyper-arterial enhancement in the arterial phase within the tumor; 5. internal artery, i.e. persistence of intratumoral arterial enhancements in the portal phase; 6. ill-defined incomplete pseudocapsula, i.e., irregular peritumoral hyperenhancement on portal phase of a radiological tumor capsule; 7. nonsmooth margin, i.e., nodular lesions with extranodular growth, confluent multinodular lesions or focal infiltrative margins; 8. peritumoral halo, i.e., peritumoral hypodense or hypointense halo in the portal phase; 9. rim enhancement, i.e., irregular circumferential peritumoral enhancement in the arterial phase; 10. wedge-shaped lesion, i.e. peritumoral hypodense or hypointense lesion located outside of the tumor margin in the delayed or hepatobiliary phase.
Microvascular invasion was defined as nests of tumor cells lining vascular cavities of endothelial cells or portal and hepatic systems on hematoxylin and eosin staining (22). To determine the histopathological MVI status, all specimens were analyzed by two independent pathologists blinded to the clinical outcomes at each center.
Data between the study groups were evaluated using the Fisher’s exact test for categorical data and t- or Mann-Whitney-U tests for continuous data. In the training cohort, a logistic regression analysis with adjustments for age, sex, underlying liver disease, size, and number of lesions was conducted to identify significant predictors of preoperative imaging features to predict MVI. Significant variables (P < 0.05) on univariate analysis were applied to a multivariate analysis while controlling for age, sex, underlying liver disease, size, and number of lesions to develop the digital biopsy prediction model. A scoring system was derived from the β regression coefficient values divided by 2 to the nearest integer and an optimal threshold for patients at high risk of MVI was determined by the Youden’s index. Two risk categories were defined (low versus high risk) and internally validated by 1,000 bootstrap samples (23). The model performance, predictive strength, and model accuracy were evaluated by the area under the curve (AUC), the Nagelkerke’s R2 (a value of 1 indicates perfect fit), and the Brier scores (a value of 0 indicates total accuracy) (23). The calibration performance of the model was visualized by a calibration plot. The Kaplan-Meier method was used to calculate survival outcomes (log-rank test). To estimate the sample size for adequate modeling (24), the presence of MVI in the training cohort was anticipated to be 15% (25) and the number of candidate predictors to be included in the multivariate model was restricted to three variables. Assuming an estimated input C-statistic of 0.95, a shrinkage factor of 0.9, and an optimism of 0.05 in the apparent R2, a minimum sample size of 196 patients were calculated. A two-sided p-value < 0.05 was considered statistically significant. Statistical analyses were performed using R version 4.1.2.
A total of 217 patients underwent hepatectomy for hepatocellular carcinoma at both institutions during the study period (Figure 1). Of these, 37 patients (17%) had a histopathological positive MVI. The baseline characteristics of patients with and without MVI are detailed in Table 1. In the MVI-positive group, more patients showed lesions exceeding 5 cm (68% vs. 43%, P = 0.030) and required major hepatectomies (46% vs. 17%, P = 0.030) as compared to patients in the MVI-negative group. Other characteristics were well-balanced between the groups.
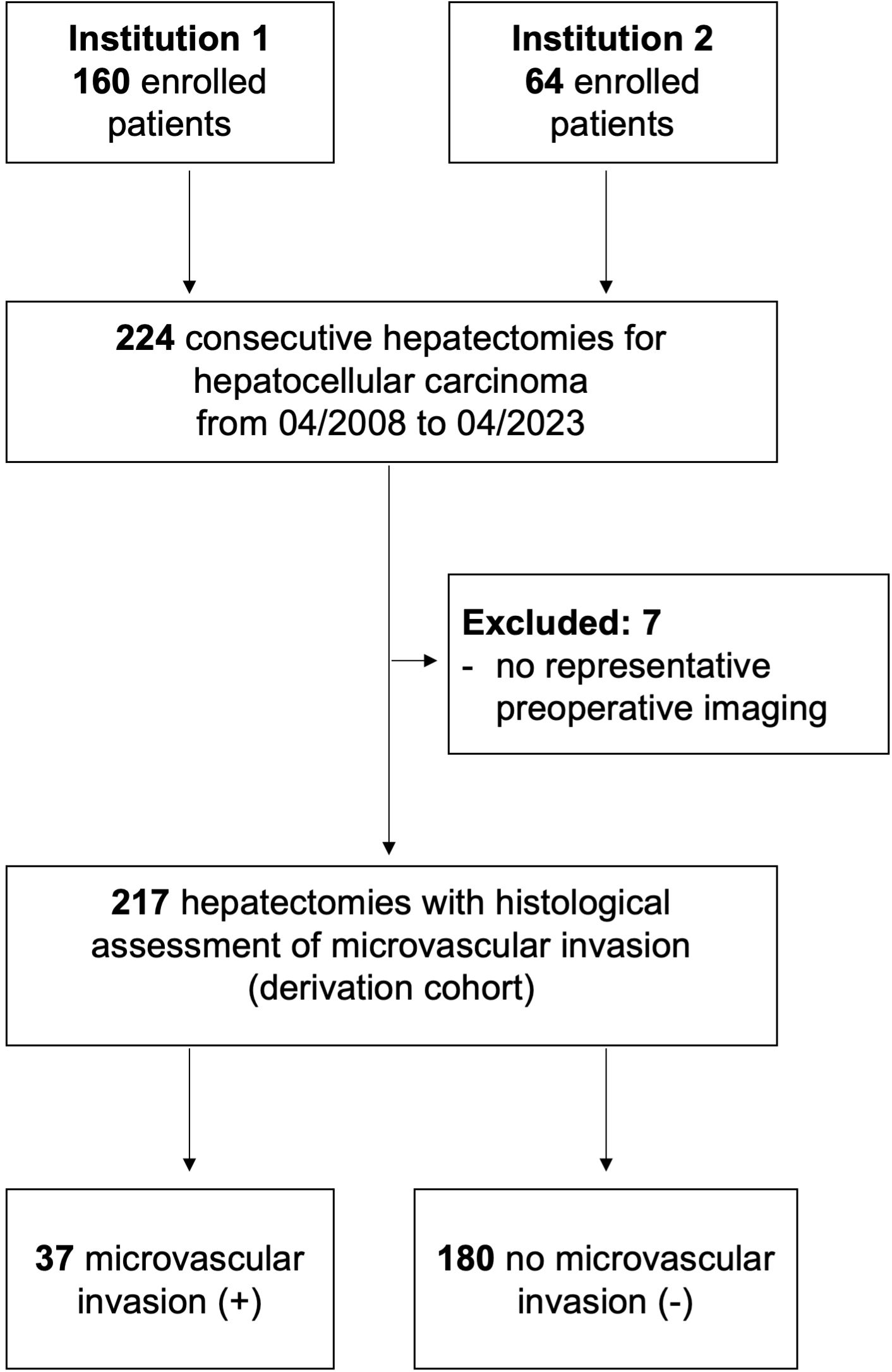
Figure 1. Patient flow chart.
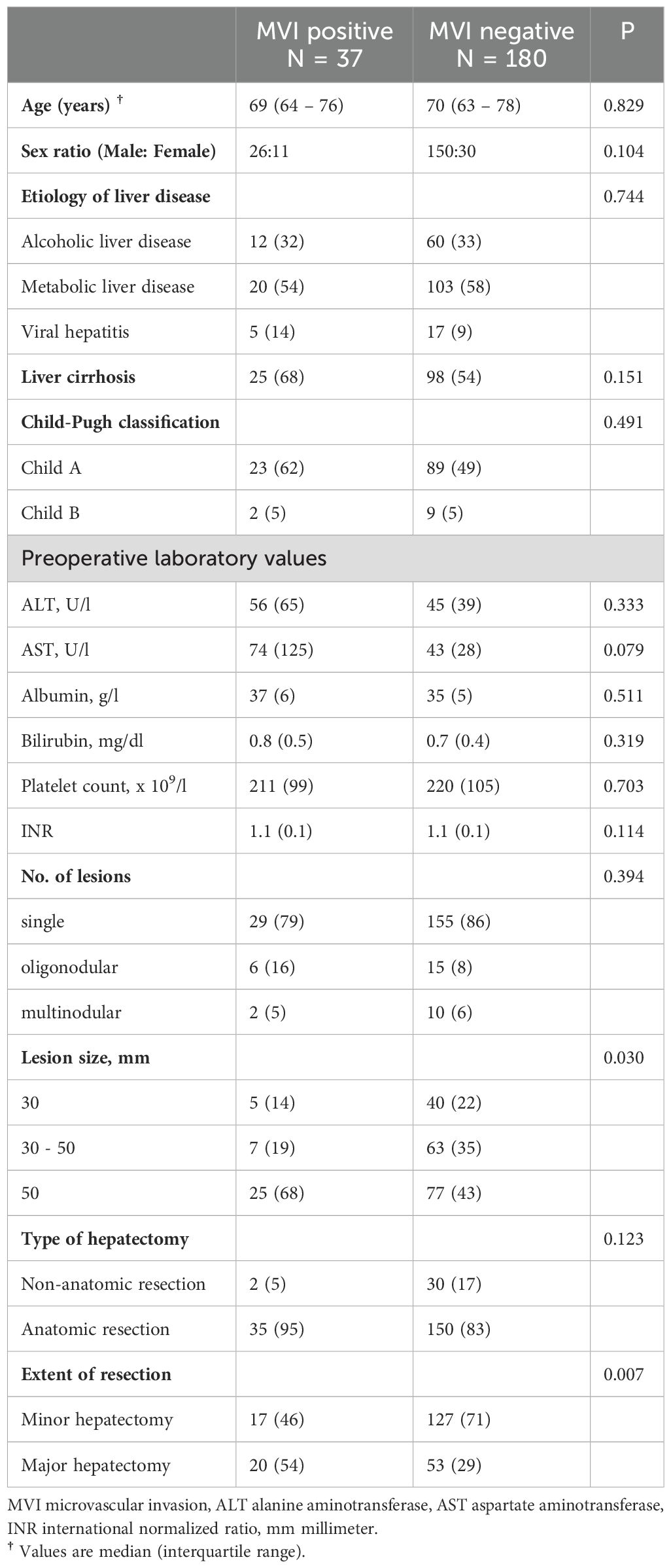
Table 1. Baseline characteristics of microvascular invasion positive and negative patients.
To develop a digital biopsy prediction model, we initially performed a logistic regression analysis (with adjustments for age, sex, etiology of disease, size, and number of lesions) on 10 potential predictive variables, which were previously shown to be associated with MVI (Table 2) (8, 10, 16, 20, 21). We identified three distinct imaging features, on univariate analyses to be associated with MVI i.e., 1) internal artery (OR 29.90, P < 0.001), 2) irregular pseudocapsula (OR 4.42, P < 0.001), and 3) non-smooth peritumoral margin (OR 12.40, P < 0.001). Multivariate analysis confirmed all three features as strong independent predictors of MVI. A non-smooth peritumoral margin predisposed a 16-fold increase, while an internal artery or an irregular pseudocapsula was associated with a 10-fold and 5-fold increase of the likelihood for the histopathological diagnosis of MVI, respectively. Figure 2 illustrates these distinct imaging features to predict MVI.
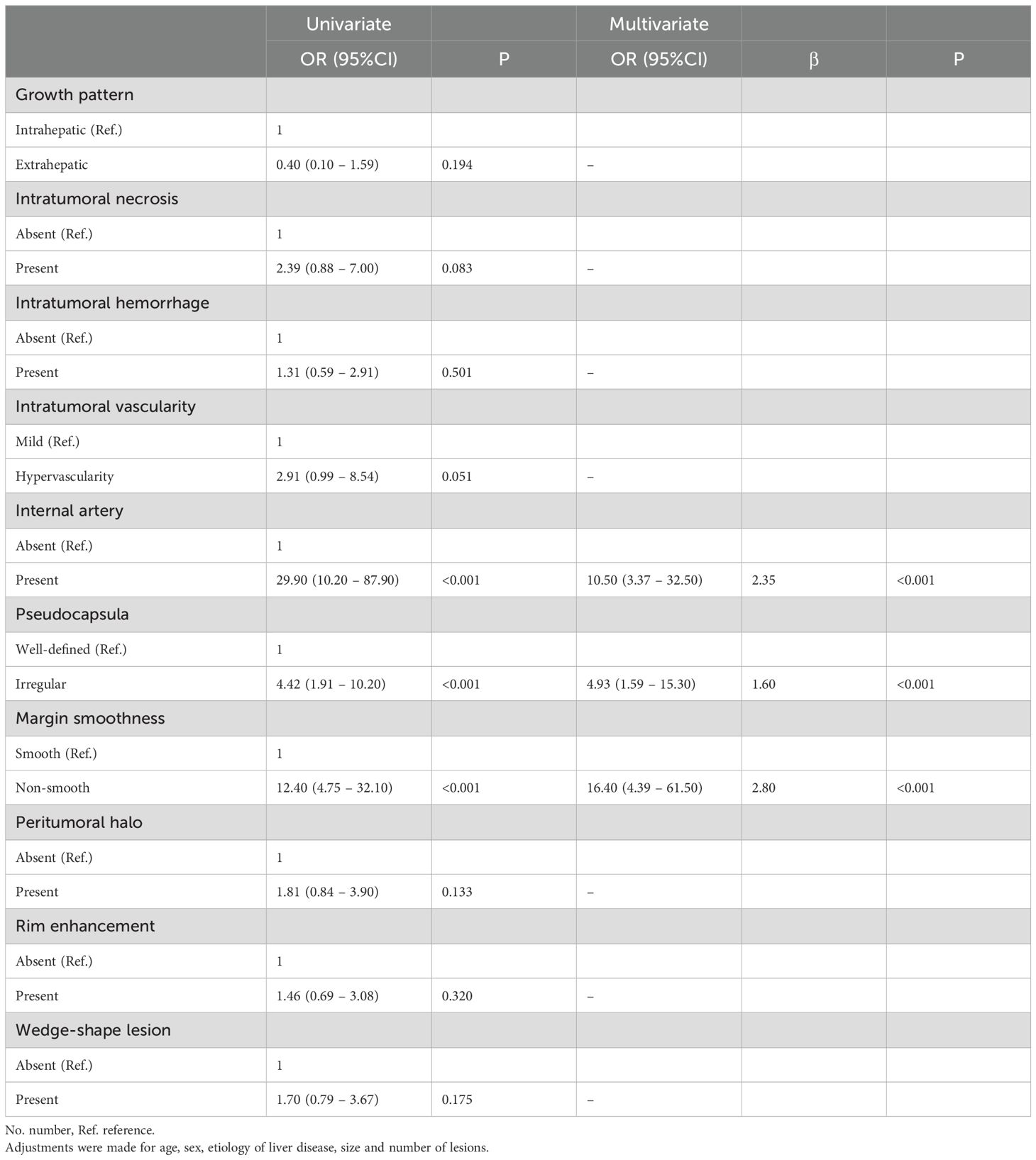
Table 2. Univariate und multivariate analysis of radiological factors associated with microvascular invasion.
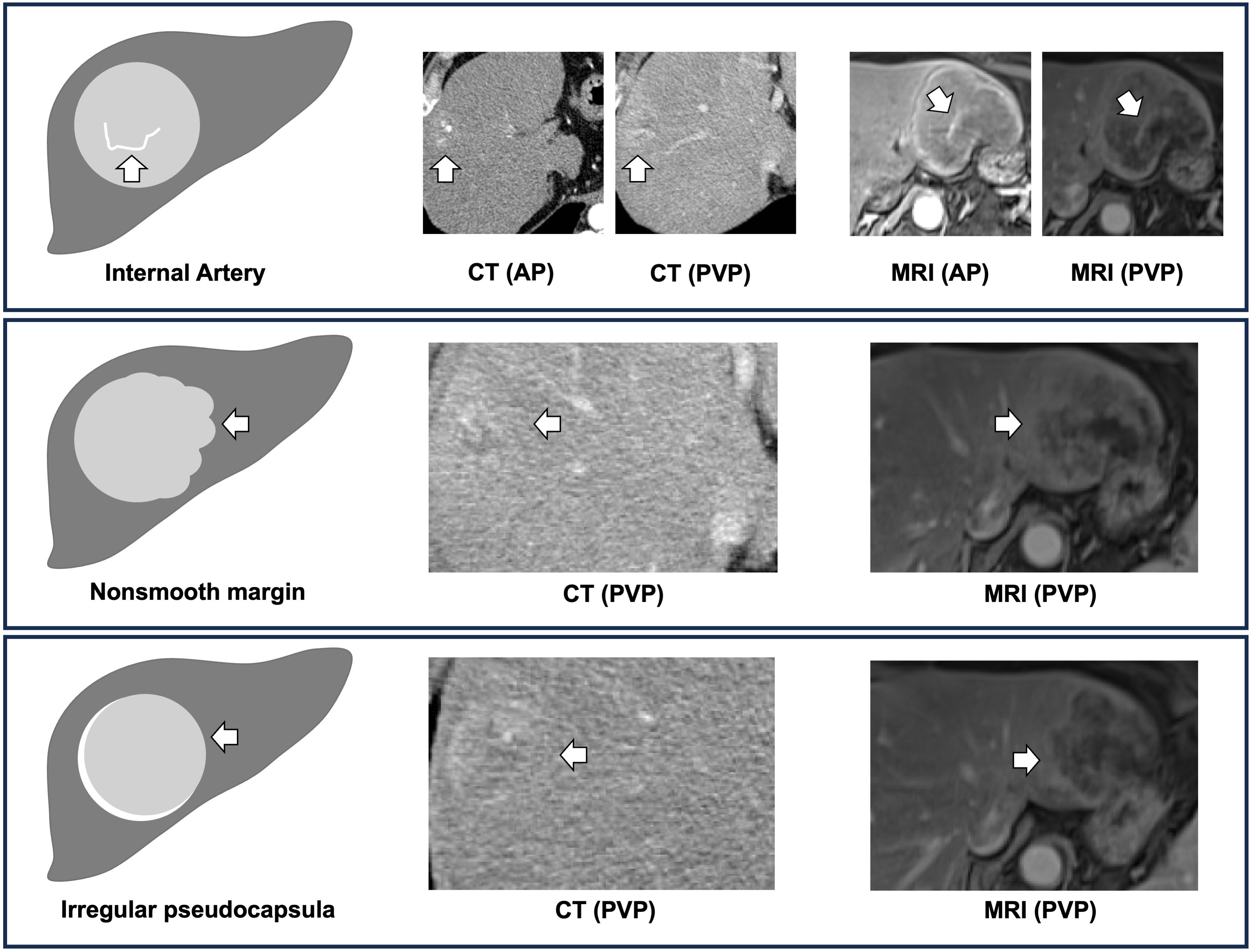
Figure 2. Digital biopsy features of microvascular invasion. The digital biopsy features (i.e. internal artery, nonsmooth margin, irregular pseudocapsula) are illustrated with white arrows (CT, computed tomography; MRI, magnetic resonance imaging; AP, arterial phase; PVP, portal venous phase).
In the next step, we assigned scores proportional to the β regression coefficient with a single point for each risk factor. The digital biopsy model resulted in a discrimination ability of an AUC of 0.91 (95%CI 0.85 – 0.96) to predict MVI (Figure 3A). Of 37 patients with histopathologically confirmed MVI, 36 (98%) had at least one point on the model. The overall MVI positivity rate was 2%, 4%, 47%, and 88% in patients with 0, 1, 2, and 3 points, respectively. Internal validation of the digital biopsy model using 1,000 bootstrap samples confirmed a high discrimination ability with a corrected AUC of 0.90. Supplementary Figure S1A displays the calibration plot with an excellent calibration between predicted and observed MVI frequencies. Further model metrics revealed high prediction value (Brier-Score of 0.08) and relationship between the predictors and MVI (Nagelkerke R2 of 0.56).
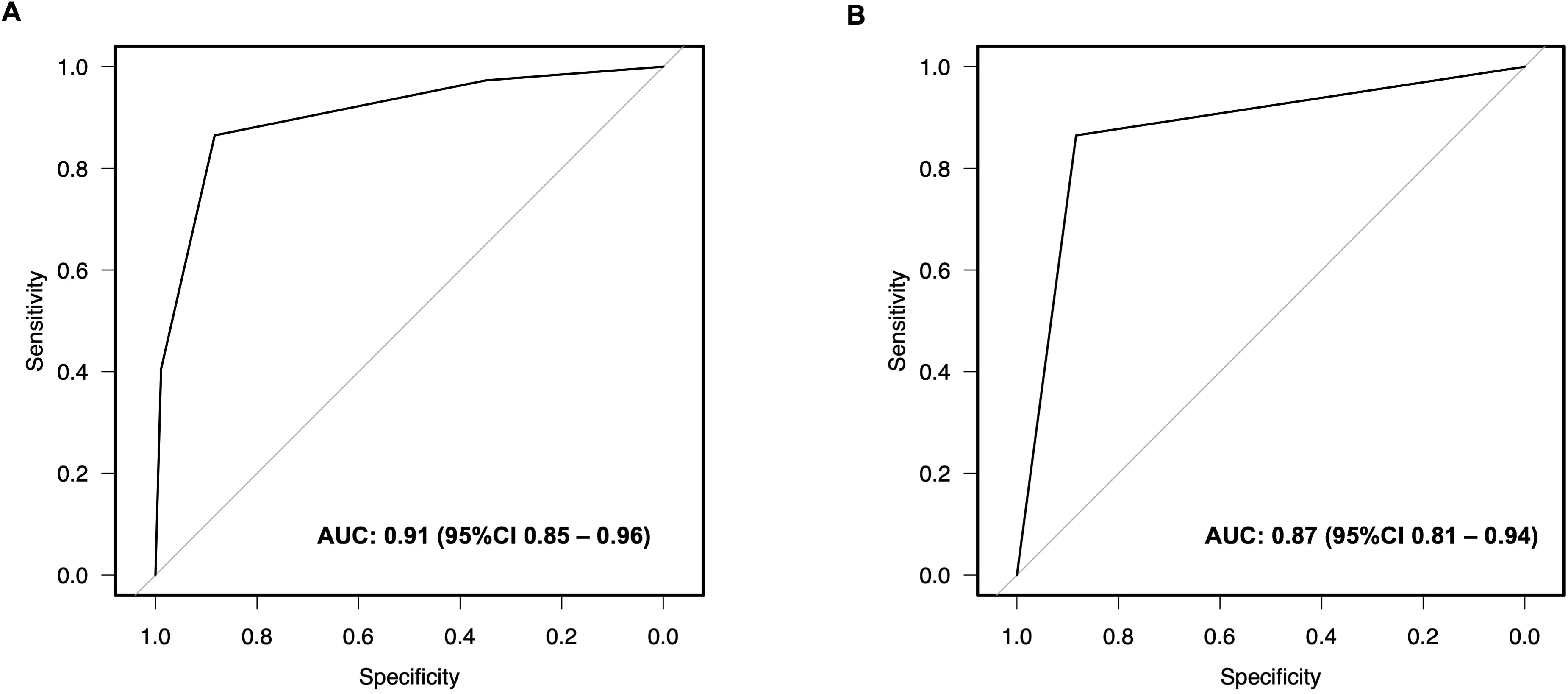
Figure 3. Receiver Operating Characteristics (ROC) curves of the digital biopsy microvascular invasion predictive system. The digital biopsy model with 0- to 3 points (yielded an area under the curve (AUC) of 0.91 (95% CI 0.93 - 0.99) (A). An AUC of 0.87 (95% CI 0.81 - 0.94) was calculated for the digital biopsy risk model with high vs. low risk of microvascular invasion (B).
To enhance the clinical utility of the digital biopsy model, we applied a threshold analysis to discriminate between high risk and low risk MVI patients. A threshold of 2 points was determined to predict a high risk for MVI with a sensitivity of 87% and specificity of 88%. Of 53 patients with 2 points on the digital biopsy risk model, 32 (60%) had confirmed MVI on histopathological analysis, compared to 5 (10%) out of 164 patients with < 2 points (Table 3). The discrimination analysis of this digital biopsy risk model yielded an AUC of 0.87 (95%CI 0.85 – 0.96) (Figure 3B). Bootstrap validation of the risk model resulted in a corrected AUC of 0.87, a Brier-Score of 0.08, and a Nagelkerke R2 of 0.52. The calibration plot of the risk model is shown in Supplementary Figure S1B.

Table 3. Risk classification system of digital biopsy proved microvascular invasion.
The median follow-up was 20 months (interquartile range: 4 - 40). Patients with histopathological confirmed MVI had a shorter recurrence-free survival (16 months, 95%CI: 7 - 23, vs. 34 months 95%CI: 26 - 52; P < 0.001), while there were no significant differences in overall survival compared to patients without MVI (35 months, 95%CI: 8 - NA, vs. 72 months 95%CI: 60 - NA, P < 0.102) (Figures 4A, B). Notably, patients with high risk of MVI according to our digital biopsy risk model had both a significantly shorter overall survival and recurrence-free survival as opposed to patients with low risk of MVI (overall survival: 35 months, 95%CI: 20 - NA, vs. 75 months 95%CI: 60 - NA, P < 0.027; recurrence-free survival: 17 months, 95%CI: 7 - 21, vs. 38 months 95%CI: 30 - 55; P < 0.001) (Figures 4C, D).
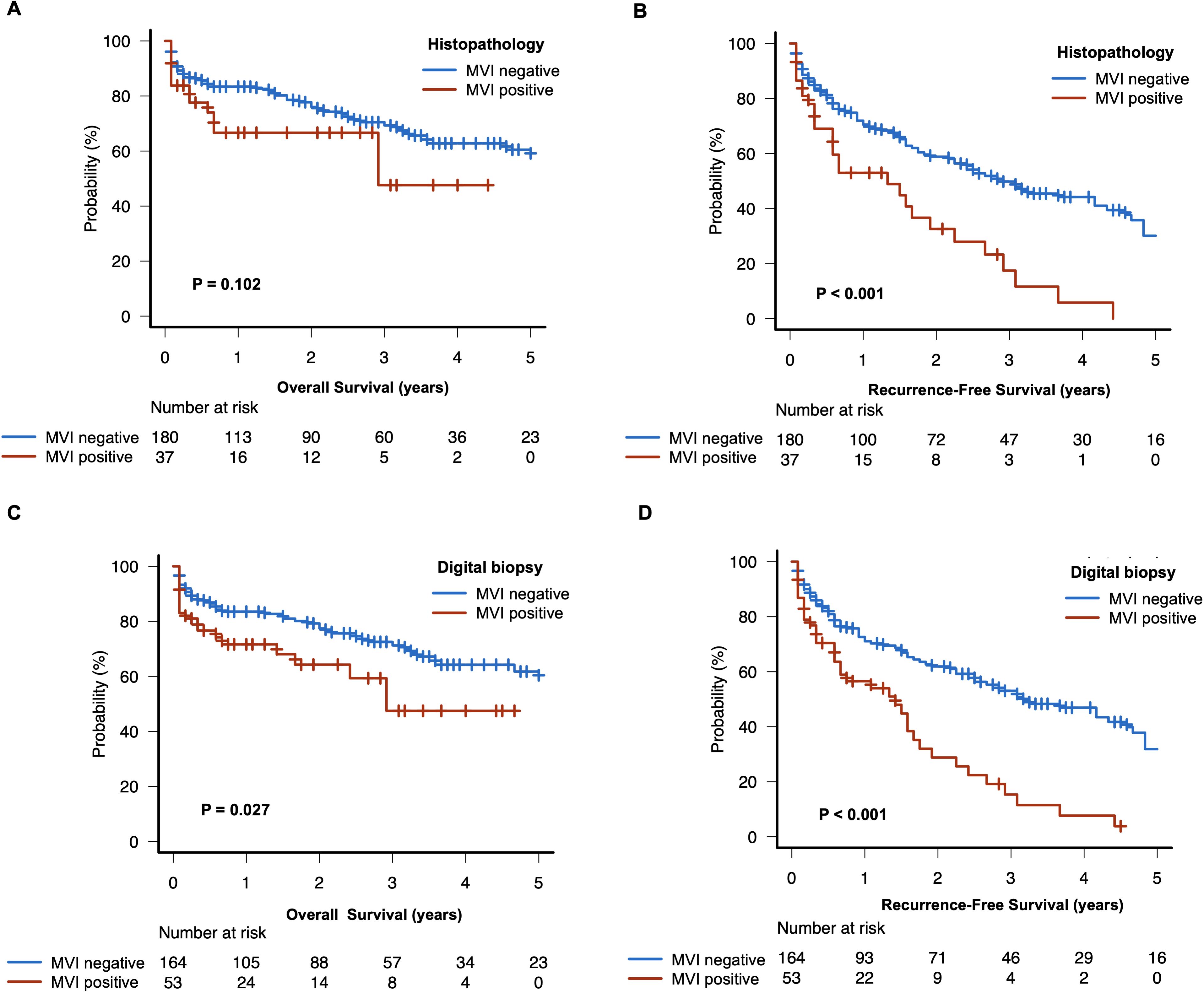
Figure 4. Survival plot stratified by pathologic and digital biopsy of microvascular invasion. The overall and recurrence-free survival plots of histopathological MVI (A, B) and digital biopsy proven MVI (C, D) are displayed.
In the present dual-center study, we developed a straightforward scoring system to predict MVI in patients with HCC using distinct preoperative radiologic features. Our digital biopsy model included the presence of a non-smooth peritumoral margin, intratumoral arterial enhancement, and irregular peritumoral hyperenhancement. The presence of at least two out of three radiologic features was associated with high sensitivity (87%) and specificity (88%) for predicting MVI before hepatectomy. Moreover, the survival outcomes stratified by our digital biopsy risk model achieved a significant difference of overall and recurrence-free survival in patients with predicted high risk versus low risk of MVI.
MVI is defined as the microscopic presence of cancer cells in hepatic vessels, indicating aggressive tumor biology (7). On preoperative imaging, a non-smooth peritumoral margin implies an upfront sign of tumor aggressiveness characterized by tumor protrusion into peritumoral areas (26). A meta-analysis on the predictive value of a nonsmooth peritumoral margin revealed that a non-smooth peritumoral margin is associated with a diagnostic odds ratio of >20 for MVI (27). Three other meta-analyses on the impact of different preoperative imaging features to predict MVI determined that a nonsmooth peritumoral margin is an important independent predictor of MVI (28–30). In the present study, we confirmed that this marker was the strongest predictor of MVI.
The presence of internal arteries in the portal phase is another substantial radiologic marker of MVI. Previous studies reported that internal arteries in HCC are correlated with angiogenesis and cellular proliferation which in turn results in tumor progression (31, 32). In 2007, a radiogenomic biomarker to predict MVI was developed in 28 patients with HCC and further validated in a cohort of 157 patients (29% with MVI) (20, 33). This radiogenomic biomarker was based on the correlation of two combined radiologic features (i.e., presence of internal arteries and peritumoral hypodense halo) with angiogenesis gene expression patterns and resulted in a sensitivity and specificity of 76% and 94% to predict MVI (20, 33). Some studies confirmed the predictive value of these two combined radiogenomic features (8, 34), while other studies including larger patient cohorts reported conflicting results (35, 36) and discovered an even higher predictive and prognostic value for internal arteries compared to peritumoral hypodense halo (12). Thus, in our study, we evaluated no combined imaging features and depicted a high predictive value of internal arteries for MVI, while peritumoral hypodense halo failed statistical significance to predict MVI.
Another characteristic imaging feature of advanced HCC is the presence of a radiologic tumor capsule (referred to pseudocapsula or peritumoral hyperenchancement), found in 70% of HCC cases (37). While the absence of a pseudocapsula might indicate an early HCC, an irregular or incomplete pseudocapsula is associated with MVI (diagnostic odds ratio of 1.85) according to a meta-analysis (38). In the present study, an irregular pseudocapsula was one of the three independent imaging features associated with MVI.
So far, a plethora of risk models exists in the literature, incorporating imaging features to predict MVI (11, 39, 40). However, the majority of available risk models were developed in patients with viral HCC having a high incidence of MVI. These models included multiple candidate variables in multivariate analyses based on the “rule of thumb”, without considering sample size considerations (8, 9, 12, 16). Renzulli et al. identified three “worrisome” features (i.e., nonsmooth tumor margin, the radiogenomic features (combination of internal arteries and hypodense peritumoral halo), and irregular pseudocapsula) to be associated with MVI in a total of 140 patients (64% with MVI and 6 candidate variables) with a c-index of 0.85 and 0.90 (8). However, these features were not tested in a multivariate analysis (8). Similarly, Min et al. described a diagnostic model in a total of 100 patients (39% with MVI) including four radiologic features (i.e., non-smooth margin, irregular pseudocapsula, peritumoral hyperenhancement, peritumoral hypointensity) with a c-index of 0.80, again without multivariate testing (9). Lee et al. developed a 6-point risk model including two radiologic features (i.e., peritumoral arterial enhancement, peritumoral hypointensity) and two serological biomarkers in a total of 276 patients (28% with MVI and 15 candidate variables) with a c-index of 0.87 (16). Recently, Jiang et al. presented a complex 10-point risk model that outperformed the models of Renzulli et al., Min et al., and Lee et al. in a comparative analysis. However, the risk model by Jiang et al. was developed in 319 patients (47% with MVI), evaluating 22 candidate variables in a multivariate analysis. Hence, the current risk models in literature are at high risk of statistical overfitting owing to the high number of candidate variables and the selection of MVI patients (MVI incidence ranging between 27% - 64%) (24). The major strength of our digital biopsy risk model is that we performed a formal sample size calculation and adjusted our analysis by controlling for several confounders (i.e., etiology of disease, lesion pattern, age, sex) which were not addressed in previous studies (8, 9, 16, 20, 33). Our digital biopsy risk model achieved a high discrimination value (c-index of 0.87) and yielded excellent calibration metrics. Notably, we included only three imaging features on CT or MRI, making it highly applicable in the daily routine compared to other models comprising more features with or without additional serum analyses as well as restrictions on the imaging modality (i.e., MRI or CT) (8–12). Additionally, the prognostic utility of our risk model was further proven by stratified survival analyses. Remarkably, patients with a high risk of MVI on the digital biopsy risk model reflected an even worse prognosis in terms of overall survival compared to patients with histopathologically proven MVI. This finding is in line with other reports in literature, indicating a higher prognostic performance of pretreatment radiologic features as compared to histopathological MVI (41, 42). Therefore, our risk model provides a “digital biopsy” and may represent an additional noninvasive armamentarium to facilitate personalized HCC treatment strategies and improve patient outcome. To this end, patients with high risk of MVI might benefit from neoadjuvant local (i.e., chemoembolization, radioembolization) or systemic treatment prior surgical resection. Given that patients with high risk of MVI recur more frequently, the digital biopsy model could also be helpful to stratify candidates for liver transplantation and, thus, impacting organ allocation policies.
There are some limitations to our study. This is a retrospective prognostic study with a potential selection bias. To increase the generalizability of our results, we performed a rigorous methodology with adjusted analyses, and imaging features were evaluated by local radiologists at each center. Still, our study lacks an external validation cohort, and the findings of our study need to be tested in a separate HCC population.
In conclusion, we developed and internally validated a robust and reliable prediction model of MVI.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethikkomission II, Heidelberg University, Medical Faculty Mannheim. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
EB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft. HN: Data curation, Formal analysis, Investigation, Writing – review & editing. SA: Data curation, Formal analysis, Investigation, Writing – review & editing. JR: Data curation, Formal analysis, Investigation, Writing – review & editing. MF: Data curation, Formal analysis, Investigation, Writing – review & editing. SH: Formal analysis, Investigation, Methodology, Writing – review & editing. MR: Data curation, Investigation, Writing – review & editing. PT: Data curation, Investigation, Writing – review & editing. ER: Data curation, Formal analysis, Investigation, Writing – review & editing. ChR: Writing – review & editing. JW: Project administration, Writing – review & editing. SS: Supervision, Writing – review & editing. CaR: Data curation, Supervision, Writing – review & editing. VP: Data curation, Formal analysis, Supervision, Writing – review & editing. NR: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1360936/full#supplementary-material
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Rahbari NN, Mehrabi A, Mollberg NM, Muller SA, Koch M, Buchler MW, et al. Hepatocellular carcinoma: current management and perspectives for the future. Ann Surg. (2011) 253:453–69. doi: 10.1097/SLA.0b013e31820d944f
3. Birgin E, Hetjens S, Tam M, Correa-Gallego C, Rahbari NN. Stereotactic body radiation therapy versus surgical resection for stage I/II hepatocellular carcinoma. Cancers (Basel). (2023) 15. doi: 10.3390/cancers15082330
4. Birgin E, Kaslow SR, Hetjens S, Correa-Gallego C, Rahbari NN. Minimally invasive versus open liver resection for stage I/II hepatocellular carcinoma. Cancers (Basel). (2021) 13. doi: 10.3390/cancers13194800
5. Zhou XD, Tang ZY, Yang BH, Lin ZY, Ma ZC, Ye SL, et al. Experience of 1000 patients who underwent hepatectomy for small hepatocellular carcinoma. Cancer. (2001) 91:1479–86. doi: 10.1002/(ISSN)1097-0142
6. Roayaie S, Obeidat K, Sposito C, Mariani L, Bhoori S, Pellegrinelli A, et al. Resection of hepatocellular cancer </=2 cm: results from two Western centers. Hepatology. (2013) 57:1426–35. doi: 10.1002/hep.25832
7. Rodríguez-Perálvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK. A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol. (2013) 20:325–39. doi: 10.1245/s10434-012-2513-1
8. Renzulli M, Brocchi S, Cucchetti A, Mazzotti F, Mosconi C, Sportoletti C, et al. Can current preoperative imaging be used to detect microvascular invasion of hepatocellular carcinoma? Radiology. (2016) 279:432–42. doi: 10.1148/radiol.2015150998
9. Min JH, Lee MW, Park HS, Lee DH, Park HJ, Lim S, et al. Interobserver variability and diagnostic performance of gadoxetic acid-enhanced MRI for predicting microvascular invasion in hepatocellular carcinoma. Radiology. (2020) 297:573–81. doi: 10.1148/radiol.2020201940
10. Lee S, Kim SH, Lee JE, Sinn DH, Park CK. Preoperative gadoxetic acid-enhanced MRI for predicting microvascular invasion in patients with single hepatocellular carcinoma. J Hepatol. (2017) 67:526–34. doi: 10.1016/j.jhep.2017.04.024
11. Zhou Q, Zhou C, Yin Y, Chen W, Liu C, Atyah M, et al. Development and validation of a nomogram combining hematological and imaging features for preoperative prediction of microvascular invasion in hepatocellular carcinoma patients. Ann Transl Med. (2021) 9:402. doi: 10.21037/atm
12. Jiang H, Wei J, Fu F, Wei H, Qin Y, Duan T, et al. Predicting microvascular invasion in hepatocellular carcinoma: A dual-institution study on gadoxetate disodium-enhanced MRI. Liver Int. (2022) 42:1158–72. doi: 10.1111/liv.15231
13. Tang M, Zhou Q, Huang M, Sun K, Wu T, Li X, et al. Nomogram development and validation to predict hepatocellular carcinoma tumor behavior by preoperative gadoxetic acid-enhanced MRI. Eur Radiol. (2021) 31:8615–27. doi: 10.1007/s00330-021-07941-7
14. Chong HH, Yang L, Sheng RF, Yu YL, Wu DJ, Rao SX, et al. Multi-scale and multi-parametric radiomics of gadoxetate disodium-enhanced MRI predicts microvascular invasion and outcome in patients with solitary hepatocellular carcinoma ≤ 5 cm. Eur Radiol. (2021) 31:4824–38. doi: 10.1007/s00330-020-07601-2
15. Eguchi S, Takatsuki M, Hidaka M, Soyama A, Tomonaga T, Muraoka I, et al. Predictor for histological microvascular invasion of hepatocellular carcinoma: a lesson from 229 consecutive cases of curative liver resection. World J Surg. (2010) 34:1034–8. doi: 10.1007/s00268-010-0424-5
16. Lee S, Kang TW, Song KD, Lee MW, Rhim H, Lim HK, et al. Effect of microvascular invasion risk on early recurrence of hepatocellular carcinoma after surgery and radiofrequency ablation. Ann Surg. (2021) 273:564–71. doi: 10.1097/SLA.0000000000003268
17. Moons KG, Altman DG, Reitsma JB, Ioannidis JP, Macaskill P, Steyerberg EW, et al. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): explanation and elaboration. Ann Intern Med. (2015) 162:W1–73. doi: 10.7326/M14-0698
18. Vitale A, Morales RR, Zanus G, Farinati F, Burra P, Angeli P, et al. Barcelona Clinic Liver Cancer staging and transplant survival benefit for patients with hepatocellular carcinoma: a multicenter, cohort study. Lancet Oncol. (2011) 12:654–62. doi: 10.1016/S1470-2045(11)70144-9
19. Wakabayashi G, Cherqui D, Geller DA, Abu Hilal M, Berardi G, Ciria R, et al. The tokyo 2020 terminology of liver anatomy and resections: updates of the brisbane 2000 system. J Hepatobiliary Pancreat Sci. (2021). doi: 10.1002/jhbp.1091
20. Banerjee S, Wang DS, Kim HJ, Sirlin CB, Chan MG, Korn RL, et al. A computed tomography radiogenomic biomarker predicts microvascular invasion and clinical outcomes in hepatocellular carcinoma. Hepatology. (2015) 62:792–800. doi: 10.1002/hep.27877
21. Xu X, Zhang HL, Liu QP, Sun SW, Zhang J, Zhu FP, et al. Radiomic analysis of contrast-enhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J Hepatol. (2019) 70:1133–44. doi: 10.1016/j.jhep.2019.02.023
22. Wang W, Guo Y, Zhong J, Wang Q, Wang X, Wei H, et al. The clinical significance of microvascular invasion in the surgical planning and postoperative sequential treatment in hepatocellular carcinoma. Sci Rep. (2021) 11:2415. doi: 10.1038/s41598-021-82058-x
23. Steyerberg EW, Harrell FE Jr., Borsboom GJ, Eijkemans MJ, Vergouwe Y, Habbema JD. Internal validation of predictive models: efficiency of some procedures for logistic regression analysis. J Clin Epidemiol. (2001) 54:774–81. doi: 10.1016/S0895-4356(01)00341-9
24. Riley RD, Ensor J, Snell KIE, Harrell FE Jr., Martin GP, Reitsma JB, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. (2020) 368:m441. doi: 10.1136/bmj.m441
25. Chen ZH, Zhang XP, Wang H, Chai ZT, Sun JX, Guo WX, et al. Effect of microvascular invasion on the postoperative long-term prognosis of solitary small HCC: a systematic review and meta-analysis. HPB (Oxford). (2019) 21:935–44. doi: 10.1016/j.hpb.2019.02.003
26. Kim H, Park MS, Choi JY, Park YN, Kim MJ, Kim KS, et al. Can microvessel invasion of hepatocellular carcinoma be predicted by pre-operative MRI? Eur Radiol. (2009) 19:1744–51. doi: 10.1007/s00330-009-1331-8
27. Hu H, Zheng Q, Huang Y, Huang XW, Lai ZC, Liu J, et al. A non-smooth tumor margin on preoperative imaging assesses microvascular invasion of hepatocellular carcinoma: A systematic review and meta-analysis. Sci Rep. (2017) 7:15375. doi: 10.1038/s41598-017-15491-6
28. Song L, Li J, Luo Y. The importance of a nonsmooth tumor margin and incomplete tumor capsule in predicting HCC microvascular invasion on preoperative imaging examination: a systematic review and meta-analysis. Clin Imaging. (2021) 76:77–82. doi: 10.1016/j.clinimag.2020.11.057
29. Wang L, Jia M, Wen X, Shen J, Yang H. Diagnostic value of magnetic resonance imaging features of microvascular invasion in hepatocellular carcinoma: a meta-analysis. Diagn Interv Radiol. (2022) 28:428–40. doi: 10.5152/dir
30. Hong SB, Choi SH, Kim SY, Shim JH, Lee SS, Byun JH, et al. MRI features for predicting microvascular invasion of hepatocellular carcinoma: A systematic review and meta-analysis. Liver Cancer. (2021) 10:94–106. doi: 10.1159/000513704
31. Kitao A, Matsui O, Yoneda N, Kozaka K, Shinmura R, Koda W, et al. The uptake transporter OATP8 expression decreases during multistep hepatocarcinogenesis: correlation with gadoxetic acid enhanced MR imaging. Eur Radiol. (2011) 21:2056–66. doi: 10.1007/s00330-011-2165-8
32. Asayama Y, Yoshimitsu K, Irie H, Nishihara Y, Aishima S, Tajima T, et al. Poorly versus moderately differentiated hepatocellular carcinoma: vascularity assessment by computed tomographic hepatic angiography in correlation with histologically counted number of unpaired arteries. J Comput Assist Tomogr. (2007) 31:188–92. doi: 10.1097/01.rct.0000236417.82395.57
33. Segal E, Sirlin CB, Ooi C, Adler AS, Gollub J, Chen X, et al. Decoding global gene expression programs in liver cancer by noninvasive imaging. Nat Biotechnol. (2007) 25:675–80. doi: 10.1038/nbt1306
34. Zhang T, Pandey G, Xu L, Chen W, Gu L, Wu Y, et al. The value of TTPVI in prediction of microvascular invasion in hepatocellular carcinoma. Cancer Manag Res. (2020) 12:4097–105. doi: 10.2147/CMAR.S245475
35. Liu P, Tan XZ, Zhang T, Gu QB, Mao XH, Li YC, et al. Prediction of microvascular invasion in solitary hepatocellular carcinoma ≤ 5 cm based on computed tomography radiomics. World J Gastroenterol. (2021) 27:2015–24. doi: 10.3748/wjg.v27.i17.2015
36. Wei M, Lin M, Zhong X, Dai Z, Shen S, Li S, et al. Role of preoperational imaging traits for guiding treatment in single ≤ 5 cm hepatocellular carcinoma. Ann Surg Oncol. (2022) 29:5144–53. doi: 10.1245/s10434-022-11344-3
37. Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology. (2014) 272:635–54. doi: 10.1148/radiol.14132361
38. Zhu F, Yang F, Li J, Chen W, Yang W. Incomplete tumor capsule on preoperative imaging reveals microvascular invasion in hepatocellular carcinoma: a systematic review and meta-analysis. Abdom Radiol (NY). (2019) 44:3049–57. doi: 10.1007/s00261-019-02126-9
39. Huang M, Liao B, Xu P, Cai H, Huang K, Dong Z, et al. Prediction of microvascular invasion in hepatocellular carcinoma: preoperative gd-EOB-DTPA-dynamic enhanced MRI and histopathological correlation. Contrast Media Mol Imaging. (2018) 2018:9674565. doi: 10.1155/2018/9674565
40. Ahn SY, Lee JM, Joo I, Lee ES, Lee SJ, Cheon GJ, et al. Prediction of microvascular invasion of hepatocellular carcinoma using gadoxetic acid-enhanced MR and (18)F-FDG PET/CT. Abdom Imaging. (2015) 40:843–51. doi: 10.1007/s00261-014-0256-0
41. An C, Kim DW, Park YN, Chung YE, Rhee H, Kim MJ. Single hepatocellular carcinoma: preoperative MR imaging to predict early recurrence after curative resection. Radiology. (2015) 276:433–43. doi: 10.1148/radiol.15142394
Keywords: biomarker, radiology, resection, perioperative oncology, hepatectomy
Citation: Birgin E, Nebelung H, Abdelhadi S, Rink JS, Froelich MF, Hetjens S, Rahbari M, Téoule P, Rasbach E, Reissfelder C, Weitz J, Schoenberg SO, Riediger C, Plodeck V and Rahbari NN (2024) Development and validation of a digital biopsy model to predict microvascular invasion in hepatocellular carcinoma. Front. Oncol. 14:1360936. doi: 10.3389/fonc.2024.1360936
Received: 24 December 2023; Accepted: 30 August 2024;
Published: 17 September 2024.
Edited by:
Marco Pellicciaro, University of Rome Tor Vergata, ItalyReviewed by:
Tongyi Huang, The First Affiliated Hospital of Sun Yat-sen University, ChinaCopyright © 2024 Birgin, Nebelung, Abdelhadi, Rink, Froelich, Hetjens, Rahbari, Téoule, Rasbach, Reissfelder, Weitz, Schoenberg, Riediger, Plodeck and Rahbari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emrullah Birgin, ZW1ydWxsYWguYmlyZ2luQHVuaWtsaW5pay11bG0uZGU=
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.