 Yahang Liang1,2†Hualin Liao1,2†Haoran Shi3
Yahang Liang1,2†Hualin Liao1,2†Haoran Shi3 Tao Li1,2
Tao Li1,2 Yaxiong Liu1,2Yuli Yuan1,2Mingming Li1,2Aidi Li1,2Yang Liu1,2Yao Yao1,2
Yaxiong Liu1,2Yuli Yuan1,2Mingming Li1,2Aidi Li1,2Yang Liu1,2Yao Yao1,2 Taiyuan Li1,2*
Taiyuan Li1,2*- 1Department of General Surgery, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi, China
- 2Gastrointestinal Surgical Institute, Nanchang University, Nanchang Jiangxi, China
- 3Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi, China
Background: The treatment strategy for stage II rectal mucinous adenocarcinoma (RMA) recommends neoadjuvant chemoradiotherapy (NCR) followed by total mesorectal excision (TME). However, the necessity of adjuvant chemotherapy (AC) remains controversial.
Materials and methods: Chi-square test was used to assess the relationship between pathological classification, AC and clinicopathological characteristics. Kaplan-Meier (KM) curves and the log-rank test were utilized to analyze differences in overall survival (OS) and cancer-specific survival (CSS) among different groups. Cox regression identified prognostic factors. Nomogram was established utilizing the independent prognostic factors. X-tile divided patients into three risk subgroups.
Results: Compared to RMA, rectal adenocarcinoma (RA) demonstrates longer OS and CSS in all and non-AC stage II patients, with no difference in OS and CSS for AC stage II patients. Propensity score matching analyses yielded similar results. Stratified analysis found that AC both improve OS of RA and RMA patients. Age, gender, pathologic T stage, regional nodes examined, and tumor size were identified as independent prognostic factors for RMA patients without AC. A nomogram was constructed to generate risk scores and categorize RMA patients into three subgroups based on these scores. KM curves revealed AC benefits for moderate and high-risk groups but not for the low-risk group. The external validation cohort yielded similar results.
Conclusions: In summary, our study suggests that, compared to stage II RA patients, stage II RMA patients benefit more from AC after NCR. AC is recommended for moderate and high-risk stage II RMA patients after NCR, whereas low-risk patients do not require AC.
Introduction
Colorectal cancer is an extremely aggressive and fatal disease (1), with rectal cancer accounting for 48.3% of cases (2). Rectal mucinous adenocarcinoma (RMA) is a distinct pathological subtype of rectal cancer, characterized by the presence of extracellular mucinous components comprising more than 50% of the tumor volume (3). Numerous studies have indicated that RMA is associated with poor prognosis (4, 5), which is closely associated with a higher proportion of lymph node infiltration, peritoneal implantation, and larger tumor volumes (6, 7). Nonetheless, the treatment strategies for RMA and rectal cancer are similar, advocating for neoadjuvant chemoradiation (NCR) before total mesorectal excision (TME) surgery, followed by standard adjuvant chemotherapy (AC) (8). However, there is still ongoing debate about whether AC treatment is necessary for stage II RMA after surgery (9).
Studies indicate that the high presence of acidic mucus in RMA can unevenly distribute drugs, reducing their effectiveness, making RMA less responsive to chemotherapy (10). However, clinical research from various centers debates whether AC benefits RMA patients. Das et al.’s study with 562 rectal cancer cases undergoing AC found no relationship between the histological subtype of mucinous adenocarcinoma and AC sensitivity (11). Zhang et al. conducted a meta-analysis on the prognosis of locally advanced rectal cancer patients after receiving first-line AC. They found that RMA patients are insensitive to AC and have a poorer prognosis (12). Our population-based retrospective cohort study suggests that, compared to stage II RA, stage II RMA benefits more from AC after NCR. However, the application of AC is likely to introduce toxicity implications for patients. So, selectively administering AC to patients at high risk of distant recurrence could maximize the avoidance of unnecessary toxicity for patients.
Therefore, based on the clinicopathological characteristics of stage II RMA patients obtained from the Surveillance, Epidemiology, and End Results (SEER) database, we constructed a nomogram. Using the risk scores obtained from this nomogram, we categorized patients into three subgroups: high, moderate, and low risk. This risk stratification system provides guidance on whether AC is necessary for stage II RMA patients.
Patients and methods
Data source and patient selection
All patient data in this study were extracted from the SEER database (https://seer.cancer.gov/). We conducted the subsequent analysis using the most recent database, which is the incidence - SEER Research Plus Data, 17 Registries, Nov 2021 Sub (2000-2019). A total of 5549 patients were enrolled to our study. The criteria for inclusion were as follows: (1) primary rectal cancer, (2) the pathological diagnosis was confirmed as rectal adenocarcinoma (RA) or RMA (ICD-O-3: 8140/2, 8140/3, 8480/3, 8481/3), (3) received curative resection, (4) patients with stage II pathology, (5) patients who received radiotherapy and systemic chemotherapy before surgery. The criteria for exclusion were as follows: (1) did not receive NCR, (2) clinicopathologic information or follow-up data is incomplete. Ultimately, we collected the following information from the enrolled patients: age, gender, race, marital status, household income, pathological T stage, RNE, and tumor size. In addition, a validation cohort comprising 143 RMA patients recruited from the First Affiliated Hospital of Nanchang University from January 2010 to October 2018 was selected. This study was approved by the Ethics Committee of First Affiliated Hospital of Nanchang University. Each participant was signed informed consent forms.
Subgroup and definition
Firstly, patients were divided into RA or RMA groups by the pathological classification. Then, based on whether they had received AC, each group was further divided into two groups, the AC group and the non-AC group. In addition, all RMA patients were divided into low (risk score: < 135, n = 132), moderate (risk score: 136-182, n = 107), and high-risk (risk score: > 182, n = 104) subgroups to evaluate the benefit of AC among different risk subgroups.
Statistical analysis
The chi-square test was used to assess the relationship between pathological classification, AC and clinicopathological characteristics. Kaplan-Meier (KM) curves and the log-rank test were utilized to analyze differences in OS and cancer-specific survival (CSS) among different groups. Univariate and multivariate Cox regression analysis were employed to identify independent prognostic factors. Nomogram was constructed utilizing the independent prognostic factors identified through multivariate Cox regression analysis. The effectiveness of the nomogram was assessed for its discriminative ability, which was quantified by the concordance index (C-index). A calibration curve was produced to demonstrate the concordance between predicted and actual survival rate. Using X-tile software, all RMA patients were divided into three risk subgroups based on their nomogram risk scores. The statistical analyses in this study were conducted using SPSS software (version 25, IBM, Armonk, NY, USA) and R software (version 4.1.1). P < 0.05 was considered to indicate a statistically significant difference.
Results
Clinicopathological characteristics
Between 2000 and 2019, according to our screening criteria, a total of 5549 patients were enrolled, with 5206 being RA and 343 being RMA. In the RA group, a total of 1589 patients received AC, while 3,617 did not receive AC. In the RMA group, 93 patients received AC, while 250 did not receive AC. Figure 1 displays the flowchart depicting the selection process. Patients with RMA tend to have an advanced T stage (P < 0.001), fewer RNE (P < 0.001), and larger tumor size (P = 0.001) compared to patients with RA (Table 1). There are no differences in terms of gender, race, marital status, household income, pathological T stage and RNE (Table 1).
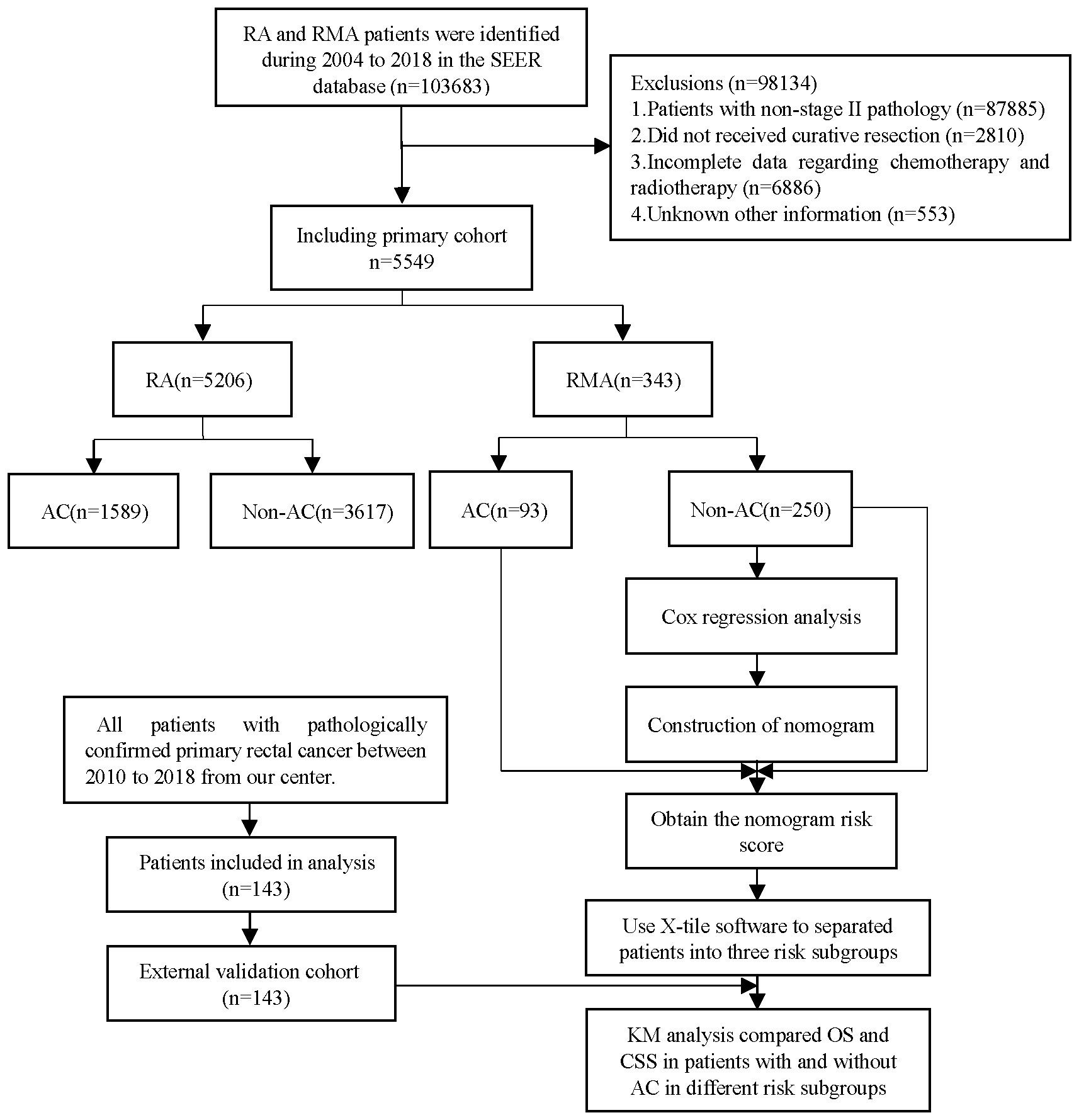
Figure 1 The workflow of the study cohort.
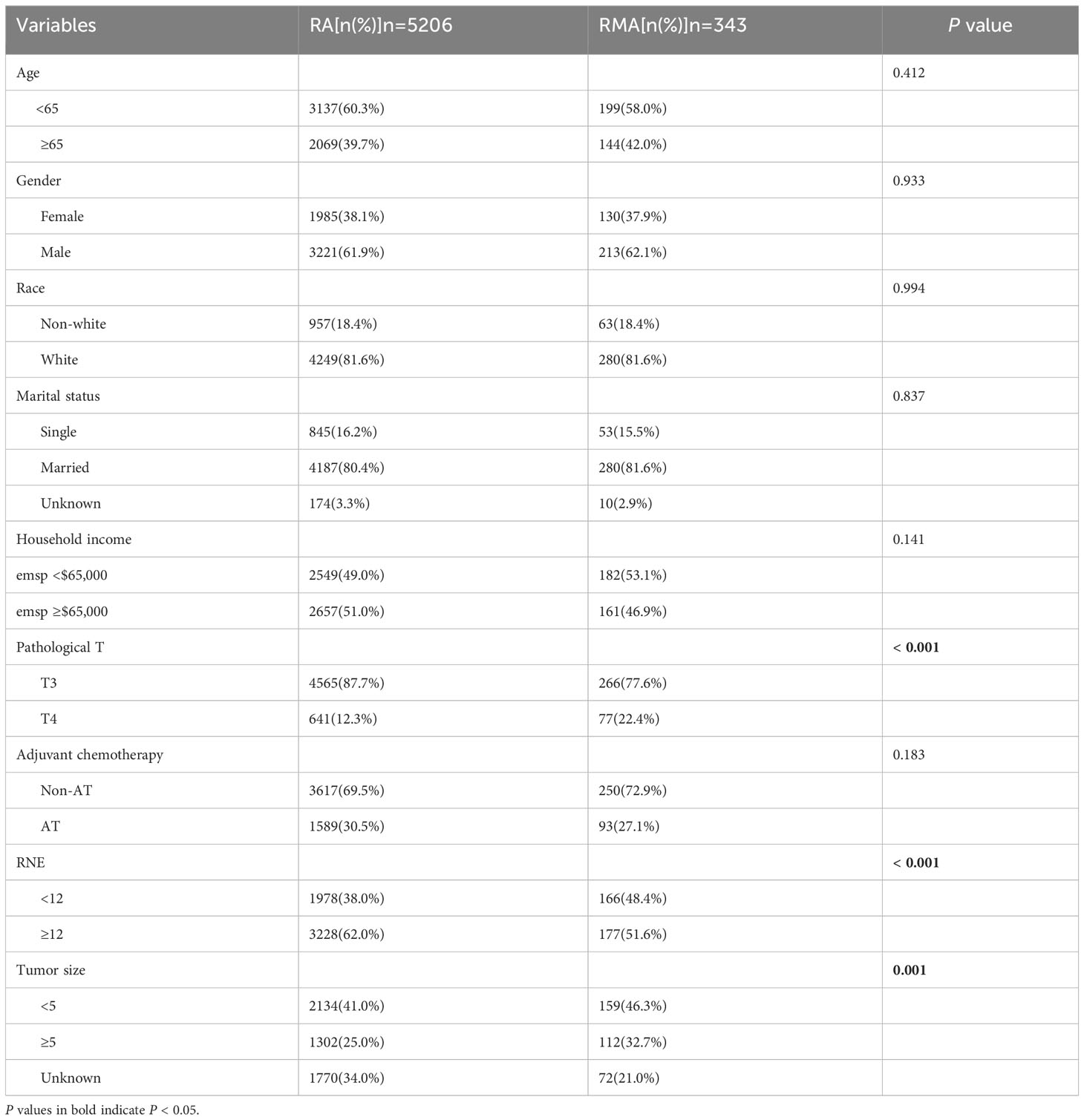
Table 1 Baseline characteristics of pathologic stage II patients with RA and RMA.
Survival prognostic factor
Then, we performed the survival analysis and found that OS (5-year OS 78.5% vs. 69.6%, P = 0.006, Figure 2A) and CSS (5-year CSS 84.7% vs. 77.1%, P = 0.002, Figure 2B) were superior in RA group compared to the RMA group. Further subgroup analysis showed that in the patients without AC, the OS (5-year OS 77.5% vs. 66.3%, P = 0.002, Figure 2C) and CSS (5-year CSS 84.7% vs. 75.2%, P < 0.001, Figure 2D) of the RA group were better than those of the RMA group, but in the patients that received AC, there was no difference in OS (5-year OS 80.8% vs. 78.9%, P = 0.95, Figure 2E) and CSS (5-year CSS 84.7% vs. 82.5%, P = 0.91, Figure 2F) between the RA group and the RMA group. The above results indicate that RMA patients have a poorer prognosis compared to RA patients. However, AC could bridge the gap in prognosis between the two groups.
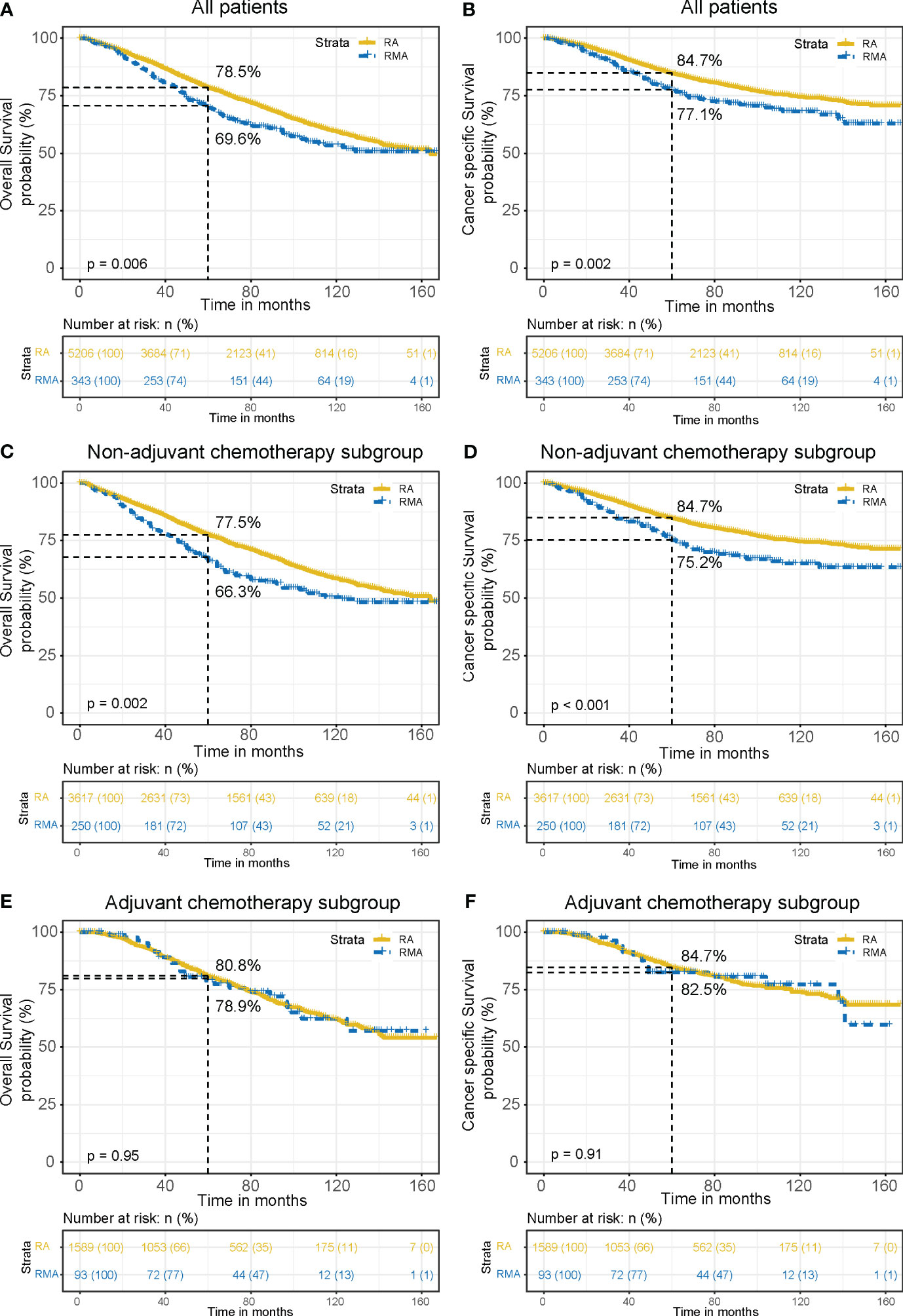
Figure 2 OS and CSS curves between the RA group and RMA group. OS (A) and CSS (B) for all patients. OS (C) and CSS (D) for non-AC patients. OS (E) and CSS (F) for AC patients.
Cox regression analysis showed that age (P < 0.001), gender (P < 0.001), household income (P < 0.001), RNE (P < 0.001) and pathological classification (P = 0.017) were independent prognostic factors of OS (Table 2). Age (P < 0.001), marital status (P = 0.002), household income (P = 0.004), RNE (P < 0.001), pathological classification (P = 0.004) were independent prognostic factors of CSS (Supplementary Table 1).
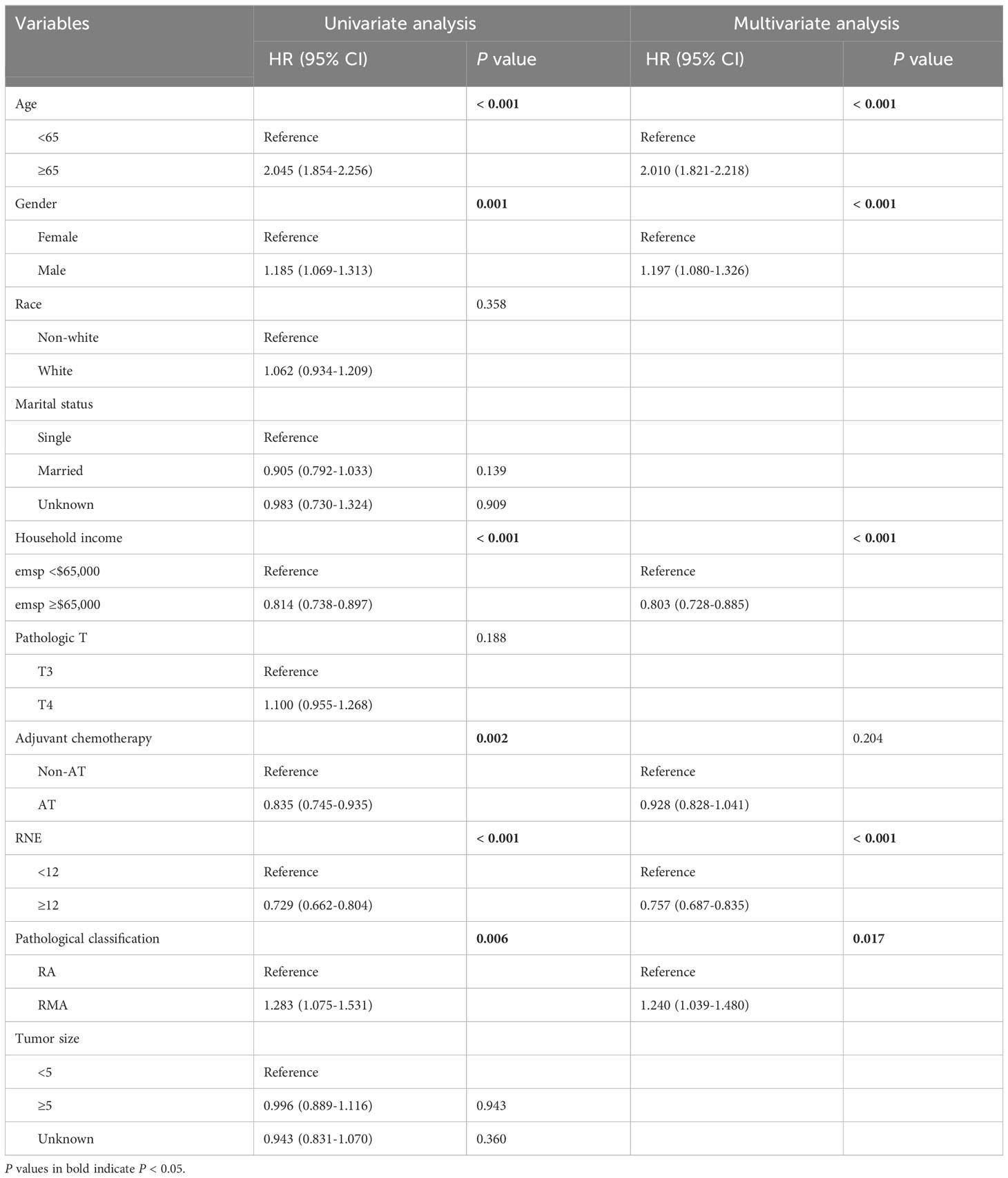
Table 2 Univariate and multivariate Cox regression analyses of OS for the stage II patients with RA and RMA.
Propensity score matching
In order to mitigate bias caused by confounding variables, we conducted a repeated analysis using propensity score matching (PSM). After adjustment with PSM, all variables were well balanced and no significant differences were found between the two groups (Supplementary Table 2). KM survival analysis showed that OS (5-year OS 83.1% vs. 69.6%, P < 0.001, Figure 3A) and CSS (5-year CSS 87.2% vs. 77.1%, P = 0.003, Figure 3B) were superior in RA group compared to the RMA group, consistent with the results before PSM. Subgroup analysis results also align with the pre-PSM findings. In the patients without AC, RA patients have better OS (5-year OS 83.0% vs. 66.3%, P < 0.001, Figure 3C) and CSS (5-year CSS 87.4% vs. 75.2%, P = 0.001, Figure 3D) than RMA patients. However, in the patients that received AC, there are no significant differences in OS (5-year OS 83.4% vs. 78.9%, P = 0.68, Figure 3E) and CSS (5-year CSS 86.7% vs. 82.5%, P = 0.85, Figure 3F) between two groups.
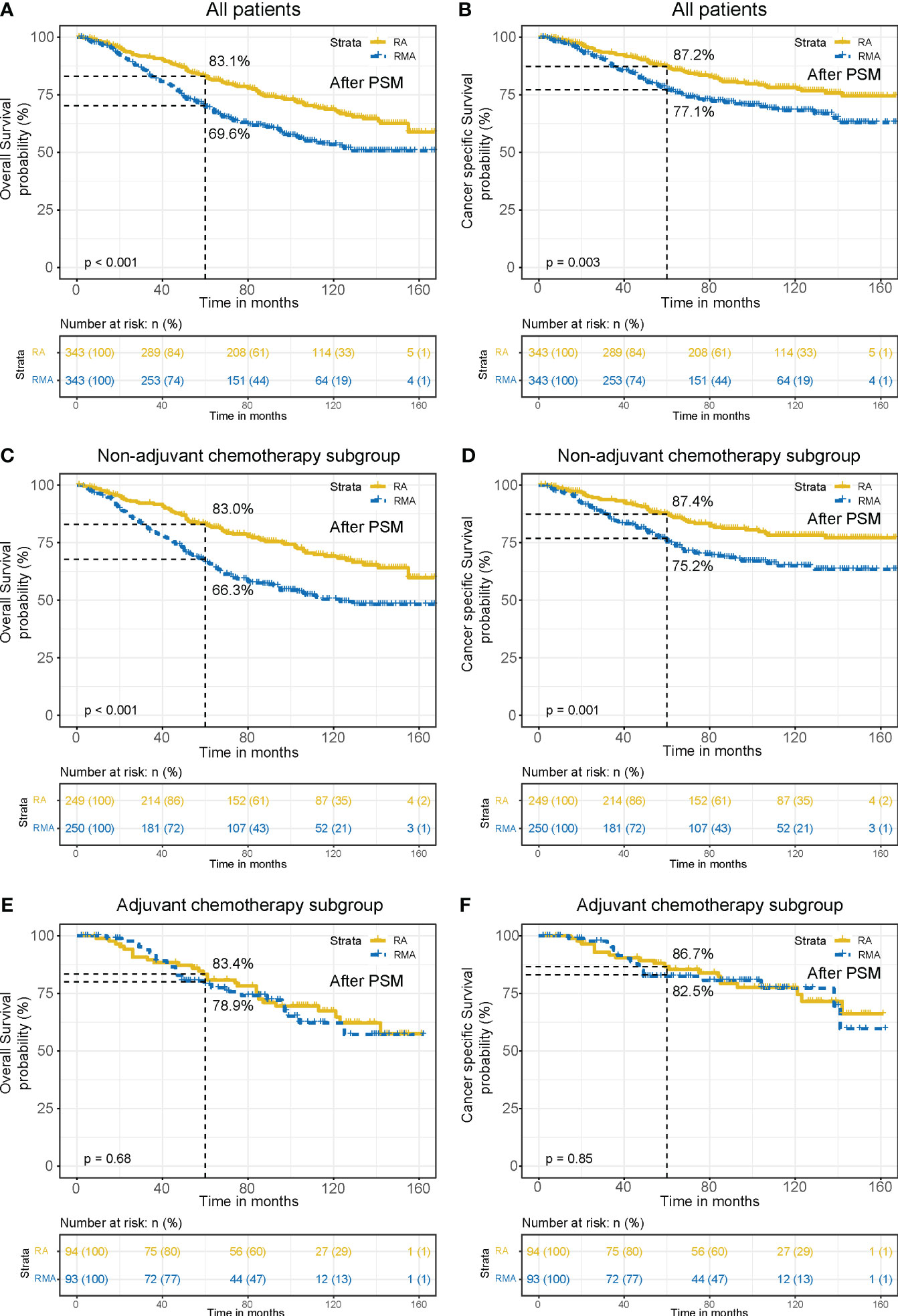
Figure 3 OS and CSS curves between the RA group and RMA group after PSM. OS (A) and CSS (B) for all patients. OS (C) and CSS (D) for non-AC patients. OS (E) and CSS (F) for AC patients.
After PSM, Cox regression analysis showed that age (P < 0.001), RNE (P < 0.001) and pathological classification (P < 0.001) were independent prognostic factors of OS (Table 3). RNE (P < 0.001), pathological classification (P = 0.003) were independent prognostic factors of CSS (Supplementary Table 3). This further corroborates the reliability of the conclusion that RMA patients have a worse prognosis than RA patients, but AC could bridge the gap in the prognoses of the two groups.
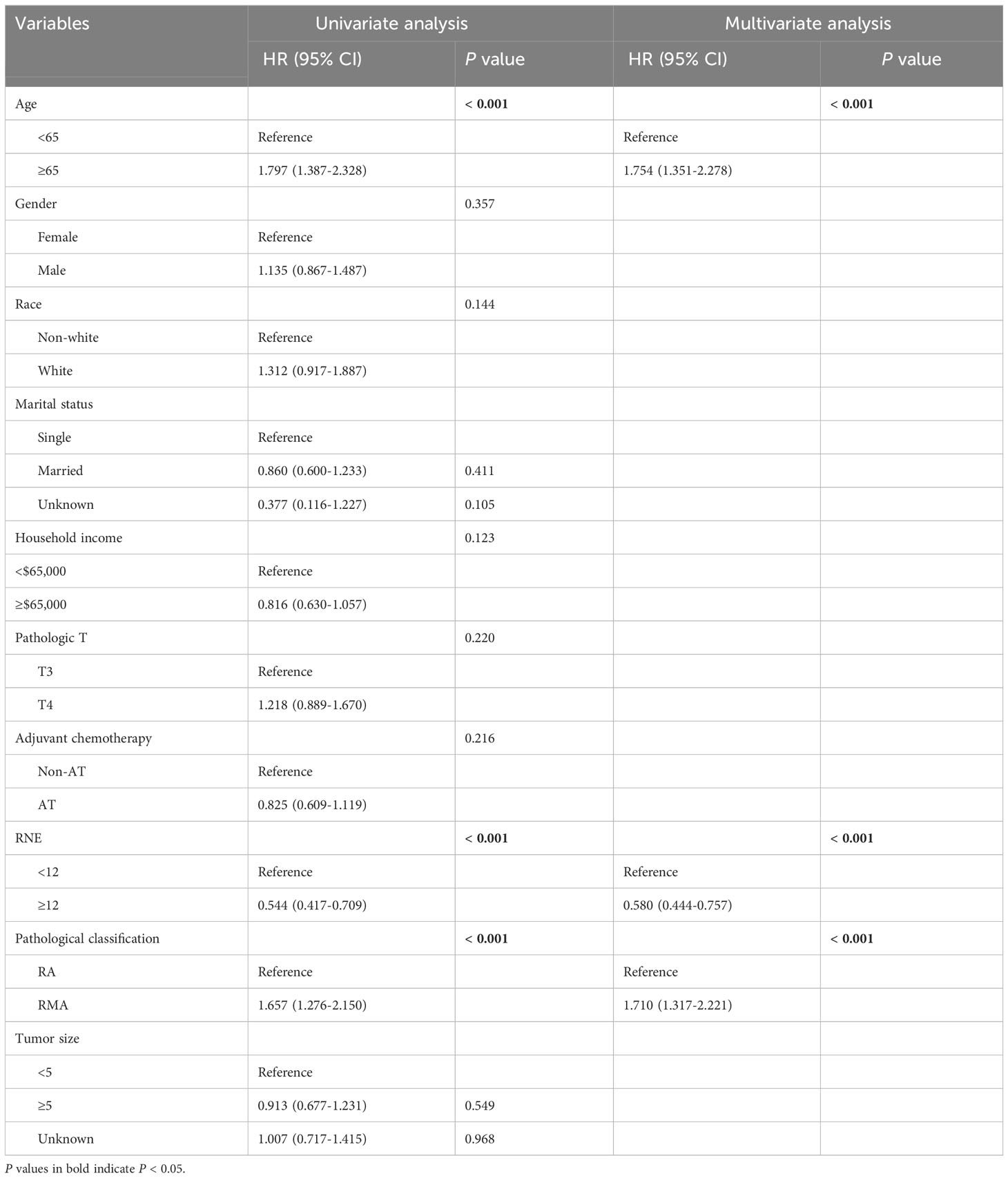
Table 3 Univariate and multivariate Cox regression analyses of OS for the stage II patients with RA and RMA after PSM.
Pathological classification-stratified analysis
Further stratified analysis revealed that AC could improve the OS of RA patients (5-year OS: 80.8% with AC vs. 77.5% non-AC, P = 0.009), with a 3.3% absolute survival benefit at 5 years (Figure 4A). In RMA patients, AC could also improve the OS (5-year OS: 78.9% with AC vs. 66.3% non-AC, P = 0.036). The 5-year absolute survival benefit is as high as 12.6% (Figure 4C). Consistent results were observed in RNE < 12 subgroup (P = 0.03, Figure 4E). However, AC does not improve the CSS for RA patients (P = 0.94, Figure 4B), RMA patients (P = 0.12, Figure 4D) and RMA patients with RNE < 12 (P = 0.23, Figure 4F). The above results indicate that AC could significantly improve the OS of stage II RMA patients. However, the application of AC is likely to introduce toxicity implications for patients. Therefore, selectively administering AC to patients at high risk of distant recurrence could maximize the avoidance of unnecessary toxicity for patients.
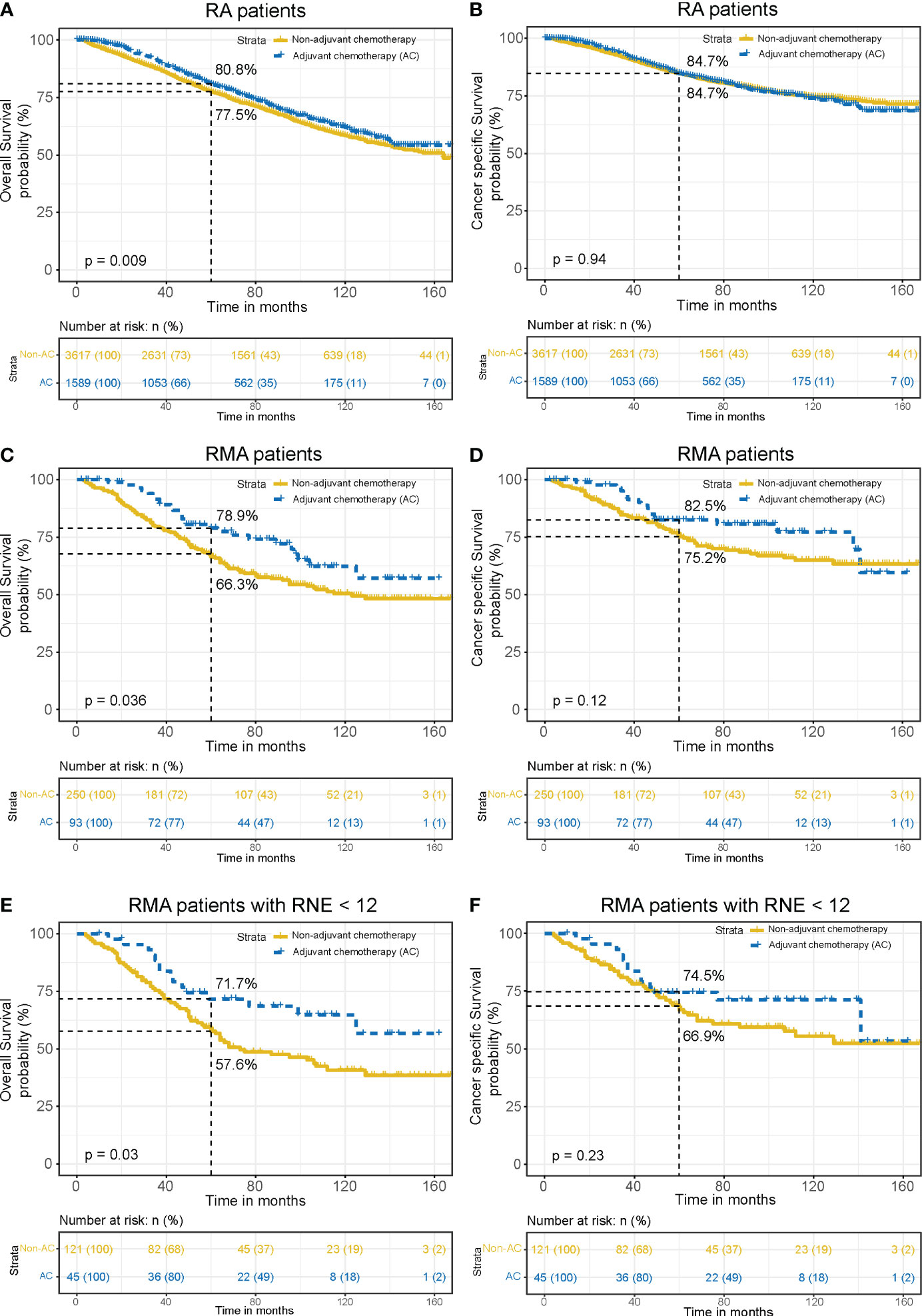
Figure 4 Pathological classification-stratified analysis. Comparison of OS (A) and CSS (B) between the AC group and non-AC group in RA patients. Comparison of OS (C) and CSS (D) between the AC group and non-AC group in RMA patients. Comparison of OS (E) and CSS (F) between the AC group and non-AC group in RMA patients with RNE < 12.
Among all stage II RMA patients, those receiving AC were younger (P = 0.048) and had larger tumor sizes (P = 0.042) compared to those without AC (Table 4). Subsequently, to eliminate the impact of AC on RMA patients’ OS, RMA patients without AC were incorporated into the Cox proportional hazard model. In the univariate analysis, age, gender, pathologic T stage, RNE, and tumor size exhibited associations with OS (all P < 0.05, Table 5). Meanwhile, in the multivariate analysis, age, gender, pathologic T stage, RNE, and tumor size were all identified as independent prognostic factors (all P < 0.05, Table 5).
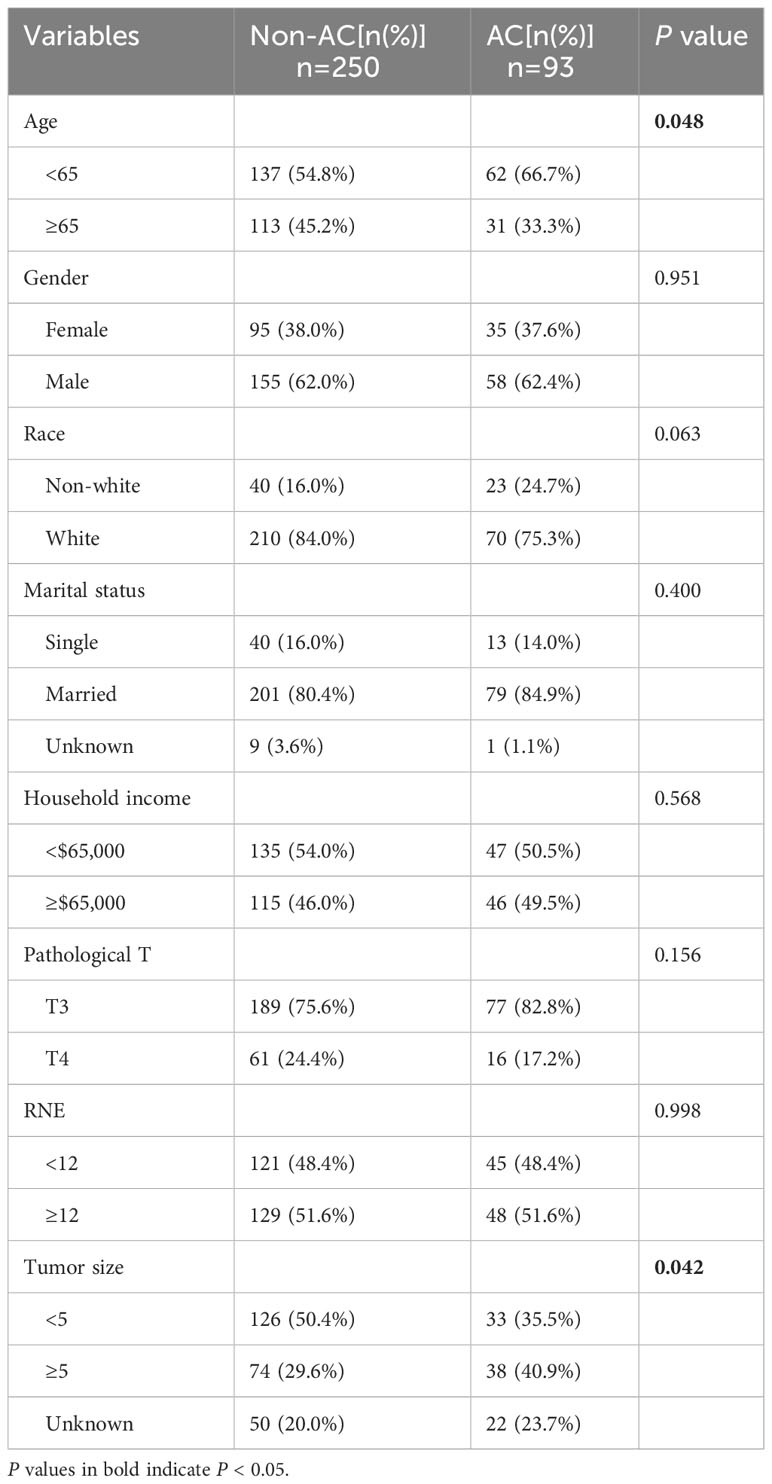
Table 4 Baseline characteristics of patients with pathologic stage II RMA.
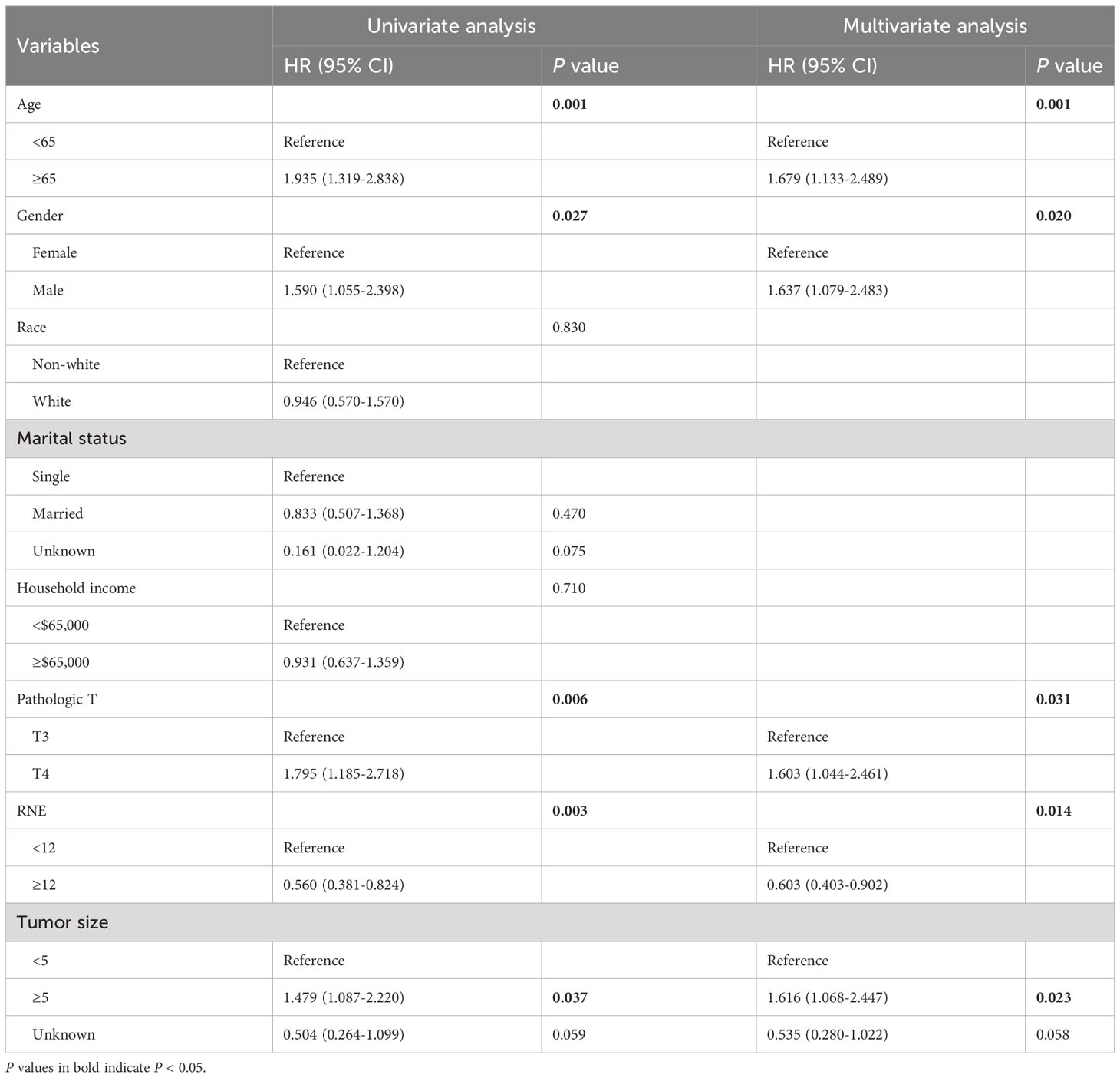
Table 5 Univariate and multivariate Cox regression analysis for OS in RMA patients who did not receive AC.
Constructing the nomogram and testing the effectiveness
A nomogram was constructed utilizing the independent prognostic factors identified through multivariate Cox regression analysis to predict 3- and 5-year OS rates, concurrently yielding a risk score for each RMA patient (Figure 5A). The C-index of the nomogram is 0.701 (95% CI: 0.652–0.750). The calibration curves of the nomogram for 3- and 5-year OS indicated that the predicted survival probabilities aligned closely with the actual survival probabilities (Figures 5B, C). The above results indicate that our nomogram possesses strong predictive potential and a high level of reliability.
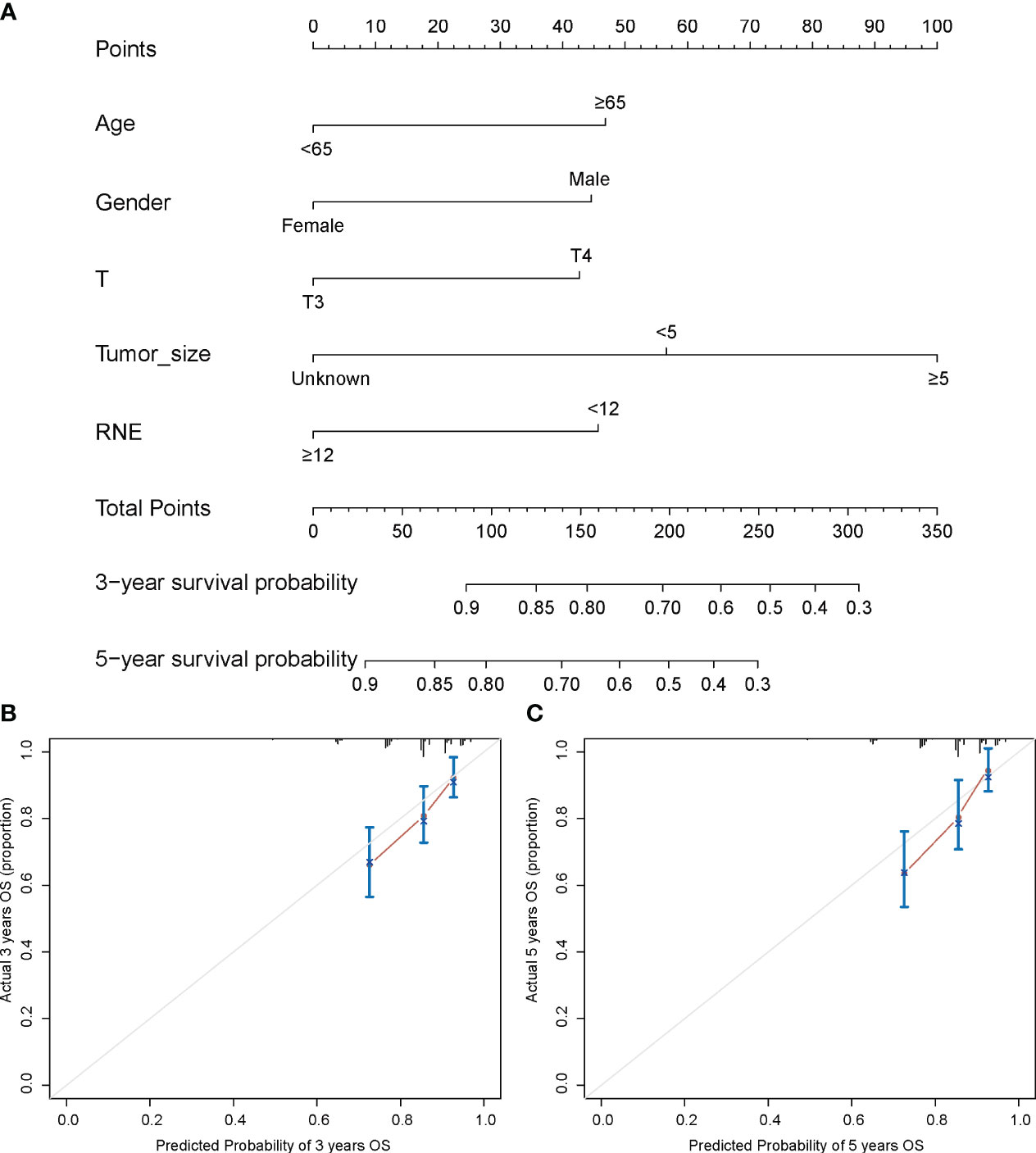
Figure 5 Nomogram for prediction of 3- and 5-year survival among stage II RMA patients (A). Calibration curves for 3- (B) and 5- (C) year OS prediction.
Overall cohort risk stratification system
Using X-tile software, all RMA patients were divided into three subgroups based on their risk scores: low-risk (risk score: < 135, n = 132), moderate-risk (risk score: 136-182, n = 107), and high-risk (risk score: > 182, n = 104) (Figures 6A, B). The 5-year OS rates for the low, moderate, and high-risk groups were 83.4%, 70.4%, and 55.2%, respectively, with significant differences (P < 0.001) (Figure 6C). Subgroup analysis showed that in the high-risk group, AC significantly improved 5-year OS (79.5% with AC vs. 48.0% without AC, P = 0.007), yielding a 31.5% absolute survival benefit at 5 years (Figure 6D). Similar results were observed in the moderate-risk group, where AC led to a significant improvement in 5-year OS (89.3% with AC vs. 63.6% without AC, P = 0.009), with a 25.7% absolute survival benefit at 5 years (Figure 6E). However, in the low-risk group, no notable difference in OS was observed between patients who received AC and those who did not (86.2% with AC vs. 75.4% without AC, P = 0.31) (Figure 6F). The above findings suggest that stage II RMA patients in the high and moderate-risk groups could benefit from AC, while those in the low-risk group do not derive a benefit from AC.
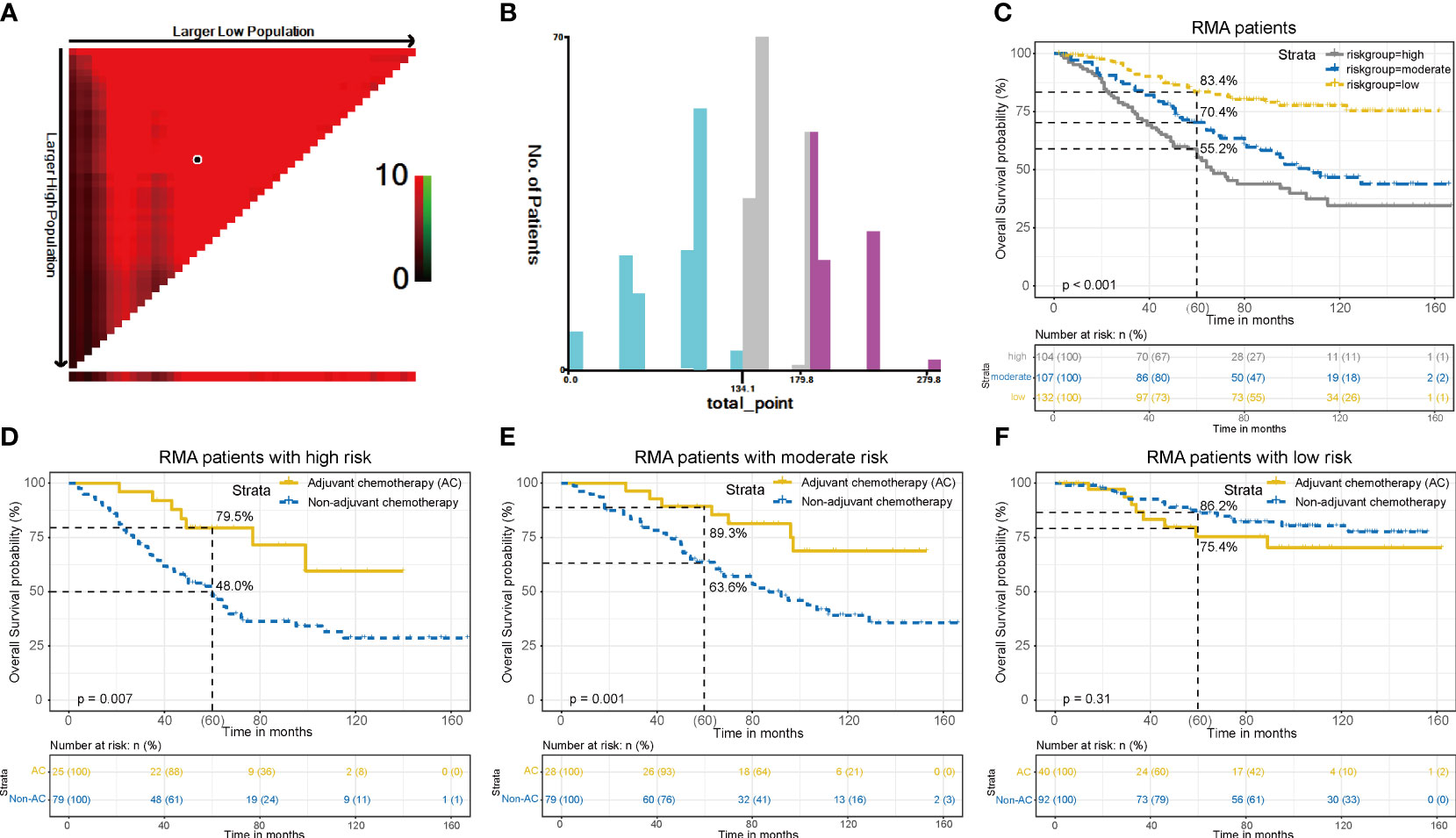
Figure 6 Overall RMA patients risk stratification system. (A). The ideal threshold values. (B). The number of patients in different risk subgroups. (C). OS curves in low, moderate and high-risk groups of all patients. Compare OS between the AC and non-AC patients in high-risk group (D), moderate-risk group (E), and low-risk group (F).
Validation of the risk stratification system
Subsequently, the risk stratification system was verified for predictive accuracy in the external validation cohort. Significant differences in 5-year OS rates were observed among the low (84.4%), moderate (71.1%), and high-risk (50.8%) groups (P = 0.001) (Figure 7A). In the high-risk subgroup, AC significantly improved 5-year OS (73.3% with AC vs. 39.3% without AC, P = 0.044), with an absolute survival benefit of 34.0% at 5 years (Figure 7B). Similarly, in the moderate-risk subgroup, AC led to a significant improvement in 5-year OS (84.7% with AC vs. 58.6% without AC, P = 0.036), with an absolute survival benefit of 26.1% at 5 years (Figure 7C). However, in the low-risk subgroup, no notable difference in OS was observed between patients who received AC and those who did not (82.3% with AC vs. 85.7% without AC, P = 0.87) (Figure 7D). The above results indicated that our risk stratification system was accurate.
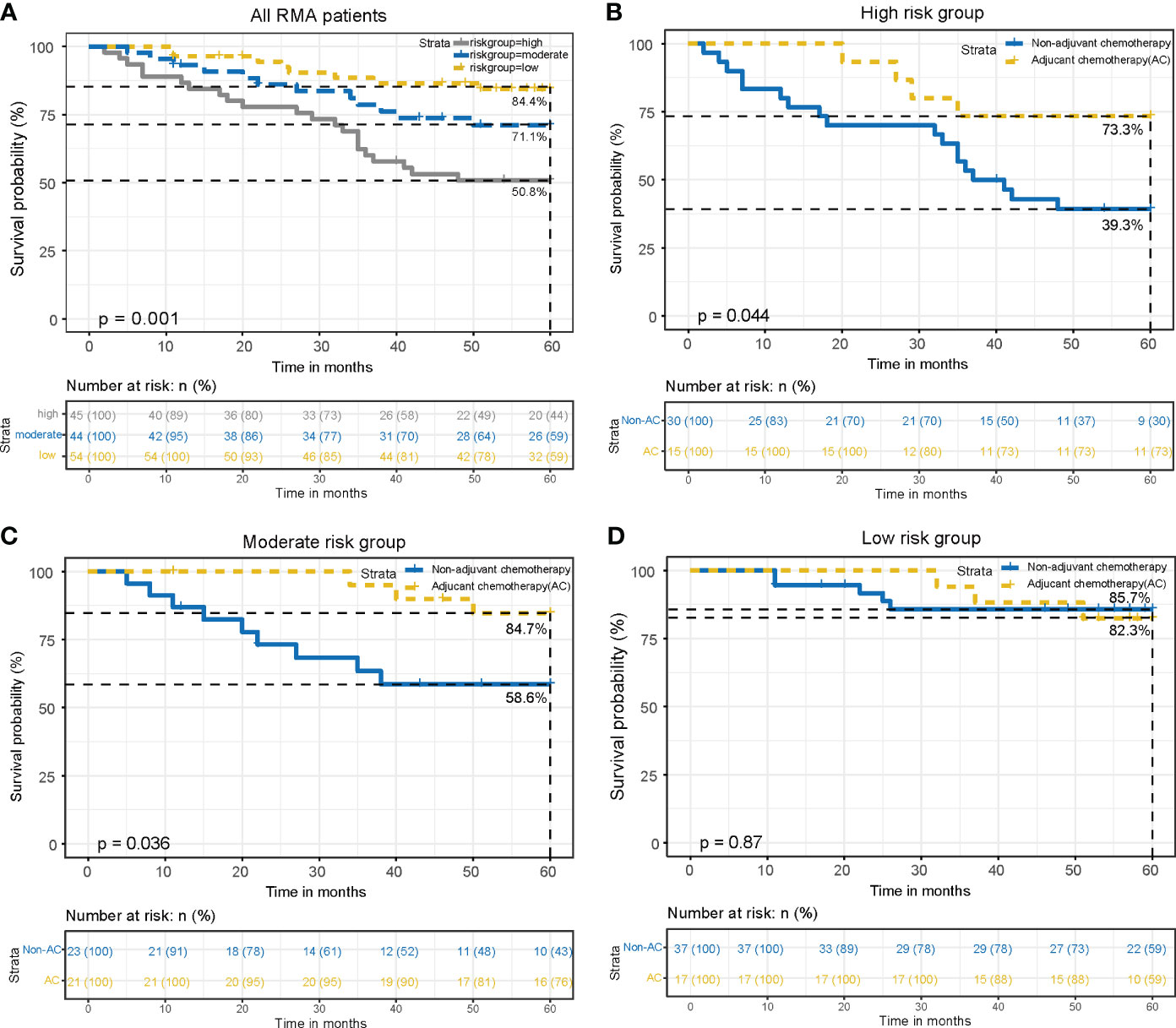
Figure 7 Validation of the risk stratification system. (A). OS curves in low, moderate and high-risk groups of all RMA patients. Compare OS between the AC and non-AC patients in high-risk group (B), moderate-risk group (C), and low-risk group (D).
Discussion
Although numerous guidelines currently recommend NCR followed by TME surgery for locally advanced rectal cancer patients (8, 13), the question of whether stage II RMA patients require additional AC after surgery remains a subject of debate. Some guidelines recommend routine AC for stage II rectal cancer patients after surgery (8), but the benefits of AC for stage II rectal cancer are primarily extrapolated from clinical trials conducted in colon cancer (14–16). The exact benefits of AC following NCR for rectal cancer remain unclear. Sainato A, and Breugom AJ, et al. (17, 18) found that NCR followed by AC after TME did not show significant benefits in OS, disease-free survival (DFS), and recurrence rate in patients with locally advanced rectal cancer. Glynne-Jones R, et al. ‘s study (19) found that in the AC group (n=54), there was no statistically significant improvement observed in the 3-year DFS (78% vs. 71%, p=0.56) and OS (89% vs. 88%, p=0.75) compared to the non-AC group (n=59). However, this study had a limited sample size and was prematurely terminated, so further clinical trials are needed to confirm the role of AC. Hence, it remains uncertain whether AC is warranted for all stage II rectal cancer patients who have received NCR and undergone TME.
RMA is a distinct pathological subtype of rectal cancer. While its treatment strategies resemble those of rectal cancer, its prognosis tends to be worse due to its lower sensitivity to chemotherapy (20). However, clinical research from various centers debates whether AC benefits RMA patients. In our study, we found that RA has longer OS and CSS than RMA in the all and non-AC stage II patients, but no significant difference in OS and CSS were observed between the RA and RMA groups for receiving AC treatment. PSM analyses yielded similar results. Stratified analysis found that AC could both improve the OS of RA patients and RMA patients (the absolute survival benefits were 3.3% and 12.6% at 5 years) patients. Therefore, AC is an essential measure for stage II RMA patients after NCR and TME (21). However, the application of postoperative AC has both a cytotoxic effect on residual tumor lesions and potential toxicity to patients (22, 23). Therefore, employing risk stratification to selectively treat patients at a high risk of distant recurrence can enhance clinical decision-making and prevent unnecessary toxicity in those unlikely to benefit.
In recent years, there have been rapid advancements in survival prediction models and risk stratification tools (24). Currently, numerous prediction models and risk stratification systems are being used for prognostic assessment or clinical treatment guidance in various cancers, including gastric cancer (25, 26), bladder cancer (27, 28), lung cancer (29, 30), nasopharyngeal carcinoma (31, 32), and more. Although prediction models cannot serve as a substitute for the evidence obtained from clinical trials, they hold significant value in supplying information for guiding clinical decisions in cancers with limited clinical trial data. Therefore, we established a nomogram based on independent prognostic factors identified through multivariate Cox regression analysis to predict 3- and 5-year OS rates, concurrently yielding a risk score for each patient. Using X-tile software, all RMA patients were divided into three subgroups based on their risk scores. KM curves and log-rank tests indicate that the high-risk group has the poorest prognosis, while the low-risk group has the best prognosis. This demonstrates the effectiveness of our risk stratification system. Further subgroup analysis results indicate that in the moderate and high-risk groups, receiving AC treatment significantly improves the 5-year OS of patients. However, in the low-risk group, there is no significant difference in OS between patients who received AC and those who did not. This result suggests that patients in the high and moderate-risk groups can benefit from AC, while those in the low-risk group do not derive a benefit from AC. And the external validation cohort yielded similar results, indicating the accuracy of our risk stratification system. Therefore, recommend AC for moderate and high-risk patients, while low-risk patients may forego it.
Finally, this study also has some limitations. First, the number of patients with stage II RMA who received NCR, underwent TME, and subsequently received AC is limited (n=93), which could potentially impact the assessment of the effectiveness of AC. Secondly, the specific regimens and completion rates of NCR and AC in patients were not clearly defined, which could introduce bias into our results. Thirdly, this study is retrospective, which may introduce bias as well. However, our study provides guidance on whether additional AC is necessary for stage II RMA following NCR and TME. Our model holds significant implications for personalized treatment of stage II RMA patients, highlighting the importance of our findings.
Conclusion
In summary, our population-based retrospective cohort study suggests that, compared to RA, stage II RMA benefits more from AC after NCR. Meanwhile, based on our prognostic predicted model and risk stratification system, it is advisable for moderate and high-risk RMA patients with pathological stage II after NCR undergo AC, while low-risk patients do not need AC.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://seer.cancer.gov/.
Ethics statement
The studies involving humans were approved by the ethics committee of First Affiliated Hospital of Nanchang University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YHL: Data curation, Funding acquisition, Methodology, Software, Validation, Writing – original draft. HL: Data curation, Methodology, Writing – original draft, Investigation. HS: Investigation, Methodology, Writing – original draft. TL: Investigation, Writing – original draft, Validation. YXL: Writing – original draft, Data curation, Software. YLY: Writing – original draft, Investigation, Methodology. ML: Methodology, Writing – original draft, Data curation. AL: Data curation, Writing – original draft, Investigation, Software. YL: Data curation, Writing – original draft, Methodology, Validation. YY: Data curation, Methodology, Validation, Writing – original draft. TYL: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by National Natural Science Foundation of China (grant no. 81860519, 82360524) and Jiangxi Province Graduate Innovation Special Fund Project (grant no. YC2022-B058).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1352660/full#supplementary-material
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Qu R, Ma Y, Tao L, Bao X, Zhou X, Wang B, et al. Features of colorectal cancer in China stratified by anatomic sites: a hospital-based study conducted in university-affiliated hospitals from 2014 to 2018. Chin J Cancer Res. (2021) 33:500–11. doi: 10.21147/j.issn.1000-9604.2021.04.07
3. Luo C, Cen S, Ding G, Wu W. Mucinous colorectal adenocarcinoma: clinical pathology and treatment options. Cancer Commun (Lond). (2019) 39:13. doi: 10.1186/s40880-019-0361-0
4. Wu P, Deng W, Yan L, Wang C, Lou Y, Wang C. Clinicopathologic and prognostic factors for colorectal cancer in children and adolescents: a population-based study. Int J Colorectal Dis. (2023) 38:35. doi: 10.1007/s00384-023-04343-7
5. Yan C, Yang H, Chen L, Liu R, Shang W, Yuan W, et al. Clinical significance of mucinous component in colorectal adenocarcinoma: a propensity score-matched study. BMC Cancer. (2021) 21:1286. doi: 10.1186/s12885-021-09031-9
6. Enblad M, Hammarström K, Folkesson J, Imam I, Golubovik M, Glimelius B. Mucinous rectal cancers: clinical features and prognosis in a population-based cohort. BJS Open. (2022) 6. doi: 10.1093/bjsopen/zrac039
7. Miyakawa T, Kawamura H, Honda M, Takano Y, Kinuta S, Kamiga T, et al. Impact of histological subtype on prognosis in stage iv colorectal cancer: a population-based cohort study. PloS One. (2022) 17:e264652. doi: 10.1371/journal.pone.0264652
8. Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, et al. Nccn guidelines insights: rectal cancer, version 6.2020. J Natl Compr Canc Netw. (2020) 18:806–15. doi: 10.6004/jnccn.2020.0032
9. Benson AB, Venook AP, Al-Hawary MM, Azad N, Chen YJ, Ciombor KK, et al. Rectal cancer, version 2.2022, nccn clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2022) 20:1139–67. doi: 10.6004/jnccn.2022.0051
10. Chand M, Yu S, Swift RI, Brown G. Mucinous carcinoma of the rectum: a distinct clinicopathological entity. Tech Coloproctol. (2014) 18:335–44. doi: 10.1007/s10151-013-1099-3
11. Das P, Skibber JM, Rodriguez-Bigas MA, Feig BW, Chang GJ, Hoff PM, et al. Clinical and pathologic predictors of locoregional recurrence, distant metastasis, and overall survival in patients treated with chemoradiation and mesorectal excision for rectal cancer. Am J Clin Oncol. (2006) 29:219–24. doi: 10.1097/01.coc.0000214930.78200.4a
12. Zhang Y, Chen Y, Huang J, Wu X, Tang R, Huang Q, et al. Mucinous histology is associated with poor prognosis in locally advanced colorectal adenocarcinoma treated with postoperative first-line adjuvant chemotherapy: a systematic review and meta-analysis. Eur J Surg Oncol. (2022) 48:2075–81. doi: 10.1016/j.ejso.2022.06.024
13. Glynne-Jones R, Wyrwicz L, Tiret E, Brown G, Rödel C, Cervantes A, et al. Rectal cancer: esmo clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2017) 28:v22–40. doi: 10.1093/annonc/mdx224
14. André T, Boni C, Navarro M, Tabernero J, Hickish T, Topham C, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage ii or iii colon cancer in the mosaic trial. J Clin Oncol. (2009) 27:3109–16. doi: 10.1200/JCO.2008.20.6771
15. Gray R, Barnwell J, McConkey C, Hills RK, Williams NS, Kerr DJ. Adjuvant chemotherapy versus observation in patients with colorectal cancer: a randomised study. Lancet. (2007) 370:2020–9. doi: 10.1016/S0140-6736(07)61866-2
16. Yothers G, O'Connell MJ, Allegra CJ, Kuebler JP, Colangelo LH, Petrelli NJ, et al. Oxaliplatin as adjuvant therapy for colon cancer: updated results of nsabp c-07 trial, including survival and subset analyses. J Clin Oncol. (2011) 29:3768–74. doi: 10.1200/JCO.2011.36.4539
17. Sainato A, Cernusco LNV, Valentini V, De Paoli A, Maurizi ER, Lupattelli M, et al. No benefit of adjuvant fluorouracil leucovorin chemotherapy after neoadjuvant chemoradiotherapy in locally advanced cancer of the rectum (larc): long term results of a randomized trial (i-cnr-rt). Radiother Oncol. (2014) 113:223–9. doi: 10.1016/j.radonc.2014.10.006
18. Breugom AJ, van Gijn W, Muller EW, Berglund Å, van den Broek C, Fokstuen T, et al. Adjuvant chemotherapy for rectal cancer patients treated with preoperative (chemo)radiotherapy and total mesorectal excision: a dutch colorectal cancer group (dccg) randomized phase iii trial. Ann Oncol. (2015) 26:696–701. doi: 10.1093/annonc/mdu560
19. Glynne-Jones R, Counsell N, Quirke P, Mortensen N, Maraveyas A, Meadows HM, et al. Chronicle: results of a randomised phase iii trial in locally advanced rectal cancer after neoadjuvant chemoradiation randomising postoperative adjuvant capecitabine plus oxaliplatin (xelox) versus control. Ann Oncol. (2014) 25:1356–62. doi: 10.1093/annonc/mdu147
20. McCawley N, Clancy C, O'Neill BD, Deasy J, McNamara DA, Burke JP. Mucinous rectal adenocarcinoma is associated with a poor response to neoadjuvant chemoradiotherapy: a systematic review and meta-analysis. Dis Colon Rectum. (2016) 59:1200–8. doi: 10.1097/DCR.0000000000000635
21. Gollins S, Moran B, Adams R, Cunningham C, Bach S, Myint AS, et al. Association of coloproctology of great britain & Ireland (acpgbi): guidelines for the management of cancer of the colon, rectum and anus (2017) - multidisciplinary management. Colorectal Dis. (2017) 19 Suppl 1:37–66. doi: 10.1111/codi.13705
22. Cartwright BM, Corso JN, Lightner J, Whitted C, Torrenegra RD, Krishnan K, et al. Achyrocline b (3,5 dihydroxy-6,7,8-trimethoxyflavone) synergizes with 5-fluorouracil allowing for dose reduction and reduced off-target toxicity in the treatment of colonic and pancreatic cancers. BioMed Pharmacother. (2023) 167:115546. doi: 10.1016/j.biopha.2023.115546
23. Zhao Y, Zhu D, Wu Z, Bai L, Wang D, Xu Y, et al. Effect of cinobufacini plus platinum-based chemotherapy regimen on the immune function of patients with non-small-cell lung cancer: a meta-analysis. Heliyon. (2023) 9:e20349. doi: 10.1016/j.heliyon.2023.e20349
24. Li T, Liang Y, Wang D, Zhou Z, Shi H, Li M, et al. Development and validation of a clinical survival model for young-onset colorectal cancer with synchronous liver-only metastases: a seer population-based study and external validation. Front Oncol. (2023) 13:1161742. doi: 10.3389/fonc.2023.1161742
25. Zhang C, Zhao S, Wang X. Prognostic nomogram for early gastric cancer after surgery to assist decision-making for treatment with adjuvant chemotherapy. Front Pharmacol. (2022) 13:845313. doi: 10.3389/fphar.2022.845313
26. Wang CY, Yang J, Zi H, Zheng ZL, Li BH, Wang Y, et al. Nomogram for predicting the survival of gastric adenocarcinoma patients who receive surgery and chemotherapy. BMC Cancer. (2020) 20:10. doi: 10.1186/s12885-019-6495-2
27. Patel KN, Salunke A, Sharma M, Puj K, Rathod P, Warikoo V, et al. Development and internal validation of a nomogram predicting overall survival based on log odds of positive lymph-nodes for post radical cystectomy patients in muscle invasive carcinoma of bladder. Clin Genitourin Cancer. (2023) 21:e153–65. doi: 10.1016/j.clgc.2022.11.018
28. Tian J, Sun J, Fu G, Xu Z, Chen X, Shi Y, et al. Population-based outcome of muscle-invasive bladder cancer following radical cystectomy: who can benefit from adjuvant chemotherapy? Transl Androl Urol. (2021) 10:356–73. doi: 10.21037/tau-20-960
29. Yang B, Liu C, Wu R, Zhong J, Li A, Ma L, et al. Development and validation of a deepsurv nomogram to predict survival outcomes and guide personalized adjuvant chemotherapy in non-small cell lung cancer. Front Oncol. (2022) 12:895014. doi: 10.3389/fonc.2022.895014
30. Wang W, Teng F, Bu S, Xu W, Cai QC, Jiang YQ, et al. A population-based study on the prognostic factors and efficacy of adjuvant chemotherapy in the postoperative stage for patients with stage iia non-small cell lung cancer. Risk Manag Healthc Policy. (2022) 15:1581–92. doi: 10.2147/RMHP.S373510
31. Yang K, Zhang Q, Zhang M, Xie W, Li M, Zeng L, et al. A nomogram for the determination of the necessity of concurrent chemotherapy in patients with stage ii-iva nasopharyngeal carcinoma. Front Oncol. (2021) 11:640077. doi: 10.3389/fonc.2021.640077
Keywords: neoadjuvant chemoradiation, stage II rectal mucinous adenocarcinoma, adjuvant chemotherapy, nomogram, survival
Citation: Liang Y, Liao H, Shi H, Li T, Liu Y, Yuan Y, Li M, Li A, Liu Y, Yao Y and Li T (2024) Risk stratification of stage II rectal mucinous adenocarcinoma to predict the benefit of adjuvant chemotherapy following neoadjuvant chemoradiation and surgery. Front. Oncol. 14:1352660. doi: 10.3389/fonc.2024.1352660
Received: 12 December 2023; Accepted: 20 February 2024;
Published: 05 March 2024.
Edited by:
Tadahiko Masaki, Kyorin University, JapanReviewed by:
Alfonso De Stefano, G. Pascale National Cancer Institute Foundation (IRCCS), ItalyEiji Sunami, Kyorin University, Japan
Copyright © 2024 Liang, Liao, Shi, Li, Liu, Yuan, Li, Li, Liu, Yao and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Taiyuan Li, anlsaXRhaXl1YW5AMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship