
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 19 March 2024
Sec. Radiation Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1347727
 Abel Cordoba1*
Abel Cordoba1* Estelle Gesta1
Estelle Gesta1 Alexandre Escande2
Alexandre Escande2 Alexandra Noeuveglise1Romain Cayez3Adrien Halty3Mohamed Tahar Ladjimi3Fabrice Narducci4Delphine Hudry4Carlos Martinez Gomez4Sofia Cordoba5Marie-Cécile Le Deley6
Alexandra Noeuveglise1Romain Cayez3Adrien Halty3Mohamed Tahar Ladjimi3Fabrice Narducci4Delphine Hudry4Carlos Martinez Gomez4Sofia Cordoba5Marie-Cécile Le Deley6 Maël Barthoulot6Eric F. Lartigau1
Maël Barthoulot6Eric F. Lartigau1Background and purpose: Image-guided adapted brachytherapy (IGABT) is superior to other radiotherapy techniques in the treatment of locally advanced cervical cancer (LACC). We aimed to investigate the benefit of interstitial needles (IN) for a combined intracavitary/interstitial (IC/IS) approach using IGABT over the intracavitary approach (IC) alone in patients with LACC after concomitant external beam radiotherapy (EBRT) and chemotherapy.
Materials and methods: We included consecutive patients with LACC who were treated with IC/IS IGABT after radiochemotherapy (RCT) in our retrospective, observational study. Dosimetric gain and sparing of organs at risk (OAR) were investigated by comparing the IC/IS IGABT plan with a simulated plan without needle use (IC IGABT plan) and the impact of other clinical factors on the benefit of IC/IS IGABT.
Results: Ninety-nine patients were analyzed, with a mean EBRT dose of 45.5 ± 1.7 Gy; 97 patients received concurrent chemotherapy. A significant increase in median D90% High Risk Clinical target volume (HR-CTV) was found for IC/IS (82.8 Gy) vs IC (76.2 Gy) (p < 10-4). A significant decrease of the delivered dose for all OAR was found for IC/IS vs IC for median D2cc to the bladder (77.2 Gy), rectum (68 Gy), sigmoid (53.2 Gy), and small bowel (47 Gy) (all p < 10-4).
Conclusion: HR-CTV coverage was higher with IC/IS IGABT than with IC IGABT, with lower doses to the OAR in patients managed for LACC after RCT. Interstitial brachytherapy in the management of LACC after radiotherapy provides better coverage of the target volumes, this could contribute to better local control and improved survival of patients.
Cervical cancer accounted for more than 500,000 new cancer cases worldwide in 2018, and remains the third leading cause of cancer-related deaths among women in developing countries (1). Over 66,000 women are diagnosed with cervical cancer every year within the World Health Organization European region, and over 30,000 die from this preventable disease (2). Over the last 30 years, a decrease in the incidence and mortality of cervical cancer has been observed in developed countries (North America and Western Europe) owing to the democratization of screening and the development of vaccination of young women between the ages of 12 and 26 years against Human Papilloma Virus, particularly against HPV-16 and HPV-18 (3).
Concomitant radiochemotherapy (RCT) and image-guided adapted brachytherapy (IGABT) are the main treatment for locally advanced cervical cancer (LACC) (4). IGABT is superior to other radiotherapy techniques for the treatment of LACC (5). IGABT comprises both the implantation of MRI/CT in contouring tools to delineate residual tumor accuracy (6) and the use of intracavitary interstitial applicators and interstitial needles (IC/IS) to adapt brachytherapy material to each patient (7), which has allowed the delivery of higher doses to residual tumors while sparing the organs at risk (OAR).
The clinical benefits of IGABT, mostly in terms of local control, have been published in large retrospective series (8–12) and recently in the EMBRACE prospective protocol (13). The use of interstitial needles has been democratized and is now established as a quality indicator according to the GEC-ESTRO group in teams performing brachytherapy in LACC (14). The main dosimetric prognostic factor for local control is the dose delivered to the residual tumor and the whole cervical tissue, called the high-risk clinical target volume (HR-CTV) (8, 10, 12, 13). We aimed to investigate the benefit of interstitial needles for combined IC/IS IGABT versus IC IGABT alone for patients with LACC.
We conducted a single-center, retrospective, observational study in which all patients were consecutively included as follows: LACC patients, > 18 years of age, treated with intracavitary/interstitial (IC/IS) brachytherapy after external beam radiotherapy treatment (EBRT); between January 2017 and December 2020; with a diagnostic pelvic MRI and an MRI at first IGABT application. The exclusion criteria were incomplete RCT and IGABT treatment, noncervical primitive tumors, absence of MRI during IGABT, and refusal of consent. Patient, tumor, treatment, dosimetric, and outcome characteristics were collected from patient medical records. All patients were clinically staged according to International of FIGO criteria (15). Clinical tumor size was defined as the maximum size on clinical examination or MRI in centimeters.
The included patients did not object to the use of their clinical data for research purposes, and the study complied with the Reference Methodology MR004 adopted by the Commission Nationale de l’Informatique et des Libertés (CNIL).
All patients were treated for LACC using radiotherapy (RT) or RCT and IC/IS IGABT. EBRT consisted of 25 or 28 fractions (1.8 Gy to deliver 45 or 50.4 Gy to the pelvis and/or para-aortic lymph nodes, if indicated and 2.2 or 2.4 Gy to deliver 55 or 60 Gy positive lymph node involvement suspected either from positron emission tomography or MRI or after lymph node staging). Concomitant platinum chemotherapy was prescribed to all patients either by weekly cisplatin 40 mg/m2 or carboplatin AUC 2. IGABT was performed immediately after the completion of RT or RCT.
Before brachytherapy, an MRI with contrast was performed at the end of RCT to determine early tumor response to primary treatment. IGABT (four high dose rate fractions of 6.5-7Gy) consisted of one or two applications under general anesthesia; a Utrecht applicator (Nucletron®, Veenendaal, The Netherlands) with vaginal ovoids was used. After visualization of MRI at the end of RT/RCT and clinical examination, we proceeded to placement of the adapted applicators in the surgical room (14). After cervix dilatation, the intracavitary and ovoid applicators were adapted to the patient and tumor, and ultrasound control-guided interstitial implants were placed for each ovoid (3 laterals, 1 anterior, 1 posterior) depending on the residual tumor seen by MRI and clinical examination. Only needles parallel to the endo-uterine catheter were implanted, and there were no possibility to implant obliques needles due to the use of the Utrecht applicator. Finally, the vagina and packed to fix the applicator.
All patients underwent an MRI with the applicator in place to delineate the gross tumor volume (GTV), HR-CTV, IR-CTV, rectum, sigmoid, bladder, and small bowel. The prescription dose for high resolution CT (HRCT) was 6.5–7 Gy per fraction, for a total of four fractions. We aimed to deliver at least an equivalent dose of 2 Gy per fraction (EQD2) of 85 Gy to the D90 HR-CTV. Using the Raystation treatment planning system, HR-CTV and OAR were contoured from MRI brachytherapy images on the day of the first implantation using information from both the clinical examination and MRI-image, according to the GYN-GEC-ESTRO recommendations (6).
We used the EMBRACE protocol dosimetric requirements (16) based on GEC-ESTRO-ABS recommendations for CTVs and OARs in EQD2: D90 HR-CTV had to be more than 85 Gy, without compromising OAR (D2cc of bladder, rectum, and sigmoid less than 90 Gy, 75 Gy, and 75 Gy, respectively). The linear-quadratic model with α/β = 10 Gy for tumor and α/β = 3 Gy for OAR was used to evaluate total dose reported during EBRT and IGABT. We considered that the OAR received all prescribed doses during EBRT. Intermediate-risk CTV (IR_CTV), GTV, and ICRU reference points (rectovaginal point, bladder point, vaginal point, PIBS, PIBS-2, and Point A) were reported.
According to the initial plan, we created a simulated treatment, deactivated interstitial positions, and re-optimized with IC only to deliver the highest possible dose to the HR-CTV according to the OAR dose limitation.
The characteristics of the population are described in terms of median and range for quantitative data, and in terms of frequency and percentage for qualitative data. Different dosimetric parameters were estimated for each approach (median, range) and compared between the two treatment plans using Student’s t-test for paired samples or Wilcoxon’s signed rank test for paired samples when the hypotheses of Student’s t-test were not valid (normal distribution of the quantitative variable, equality of the variances in the two groups). The dosimetric data have also been treated as qualitative variables and compared using the McNemar’s test for paired sample. The relationship between the benefit of IN and FIGO 2018 stage, initial tumor size, laterality of affected parameters, number of IN placements, and period of IN placement were explored using univariate logistic regression models.
A total of 194 patients were treated for LACC with IGABT after RCT between 2017 and 2020. A total of 76 patients were excluded because they were treated with IC brachytherapy alone. Thirteen patients were excluded because brachytherapy MRI was not performed due to contraindications to MRI (seven patients) or unavailability (six patients); three patients received incomplete brachytherapy treatment; and three patients opposed the re-use of their data, leaving 99 patients for analysis (Figure 1).
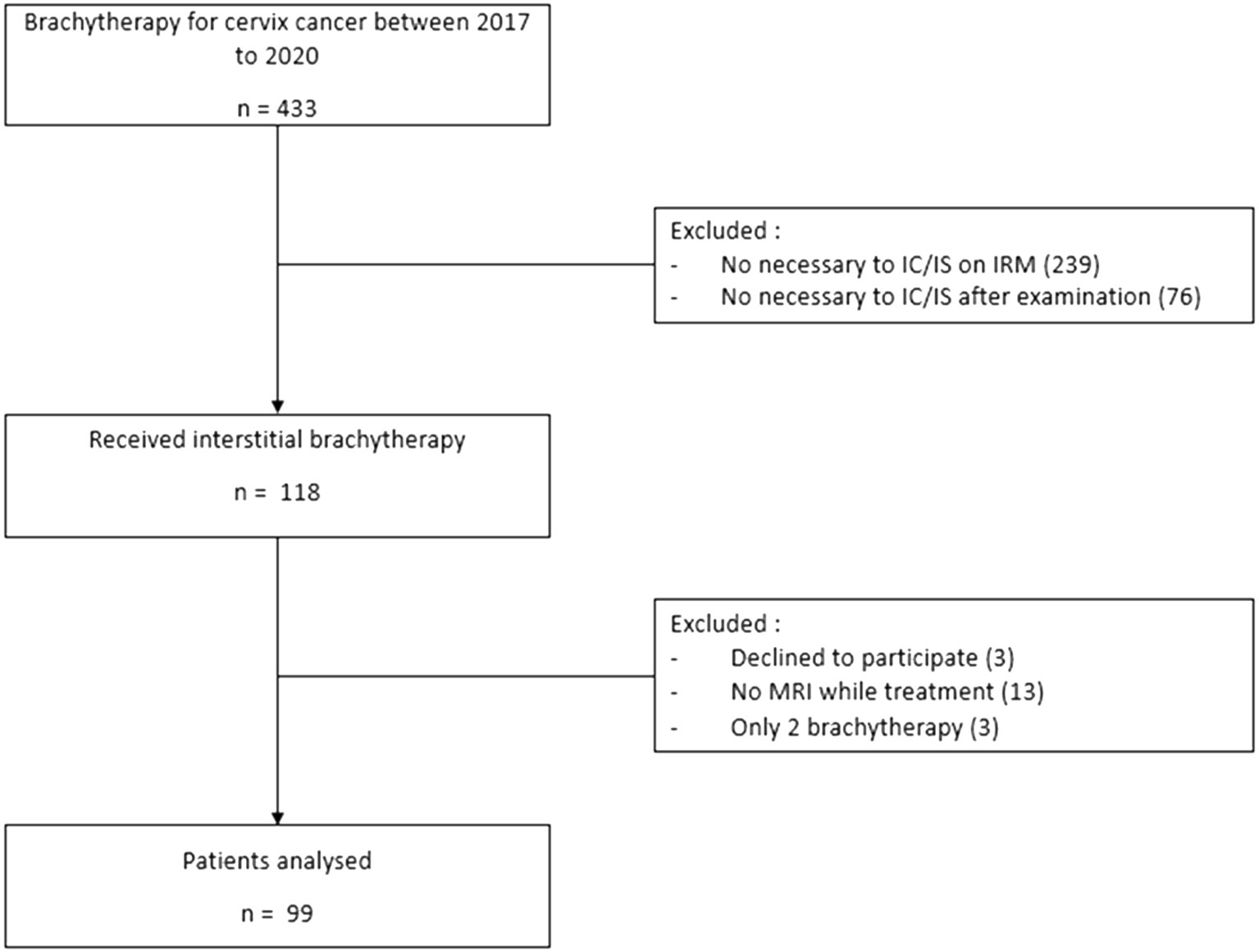
Figure 1 Flow chart of the study.
The median age at diagnosis was 51 years (range, 23–86). Five patients had been treated for cervical cancer relapse, with three patients treated after total hysterectomy. Eighty-two (82.8%) patients had squamous cell carcinoma. Mean EBRT dose was 45.5 ± 1.7 Gy; 97% received concurrent chemotherapy. Mean HR-CTV was 40 ± 19.1 cm3; 63 (68.5%) patients had an HR-CTV ≥30 cm3. At diagnosis, parametrial invasion was observed in 92 (92.9%) patients, bilateral parametrial invasion in 66 (66.7%), and distal parametrial invasion in 41 (41.4%). Seven patients with FIGO stage IVB tumors were treated with RCT and IGABT after first-line chemotherapy. Seventy-seven (77.7%) patients underwent MRI at the end of the RCT before brachytherapy. The clinical characteristics of the patients are shown in Table 1.
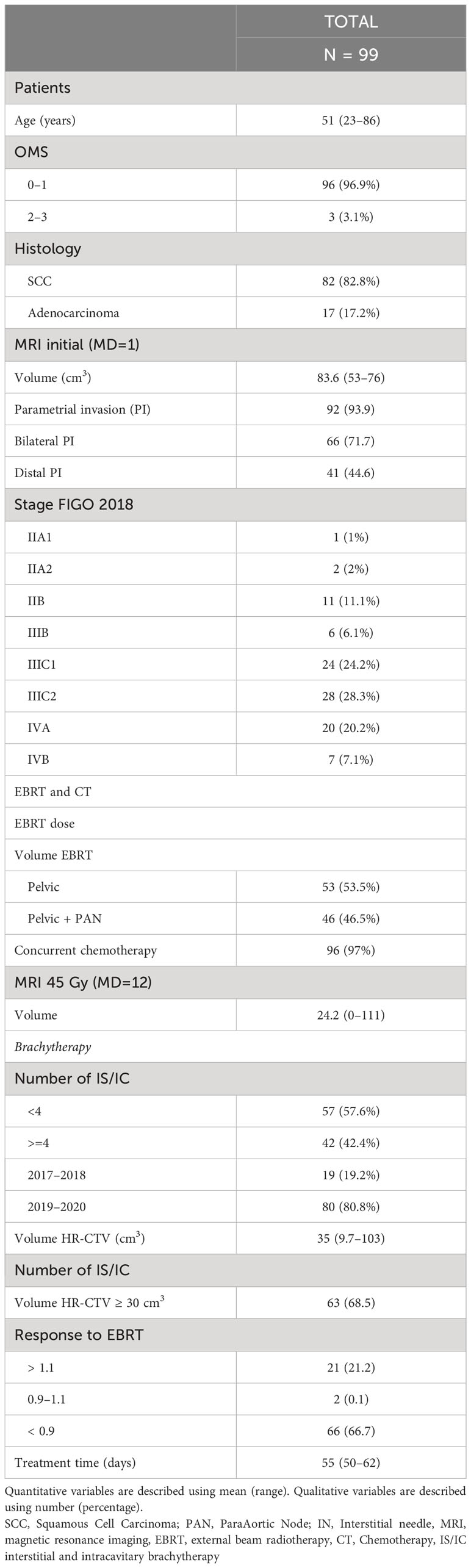
Table 1 Quantitative variables are described using median (range). Qualitative variables are described using number (percentage).
Different dosimetric parameters were compared between the IC/IS IGABT plan and the simulated plan without needle use (IC IGABT plan) (Table 2). A significant increase in median D90% HR-CTV was found (IC/IS vs IC: 82.8 Gy [56.4–92.3 Gy] vs 76.2 Gy [54.4–97.8 Gy], p<10-4). A significant decrease of the delivered dose for all OAR was found (IC/IS vs IC): median D2cc for the bladder was 77.2 (53.2–90.4 Gy) vs 85.2 Gy (60.2–91.7 Gy), p<10-4; median D2cc for the rectum was 68 Gy (48.1–96.2 Gy) vs 72.7 Gy (49.5–80.4 Gy), p<10-4; median D2cc for the sigmoid was 53.2 Gy (44.9–70.5) vs 53.5 Gy (45.1–80.3 Gy), p<10-4; and median D2cc for the small bowel was 47 Gy (43.9–68.2 Gy) vs 47.5 Gy (44–74.6 Gy), p<10-4.
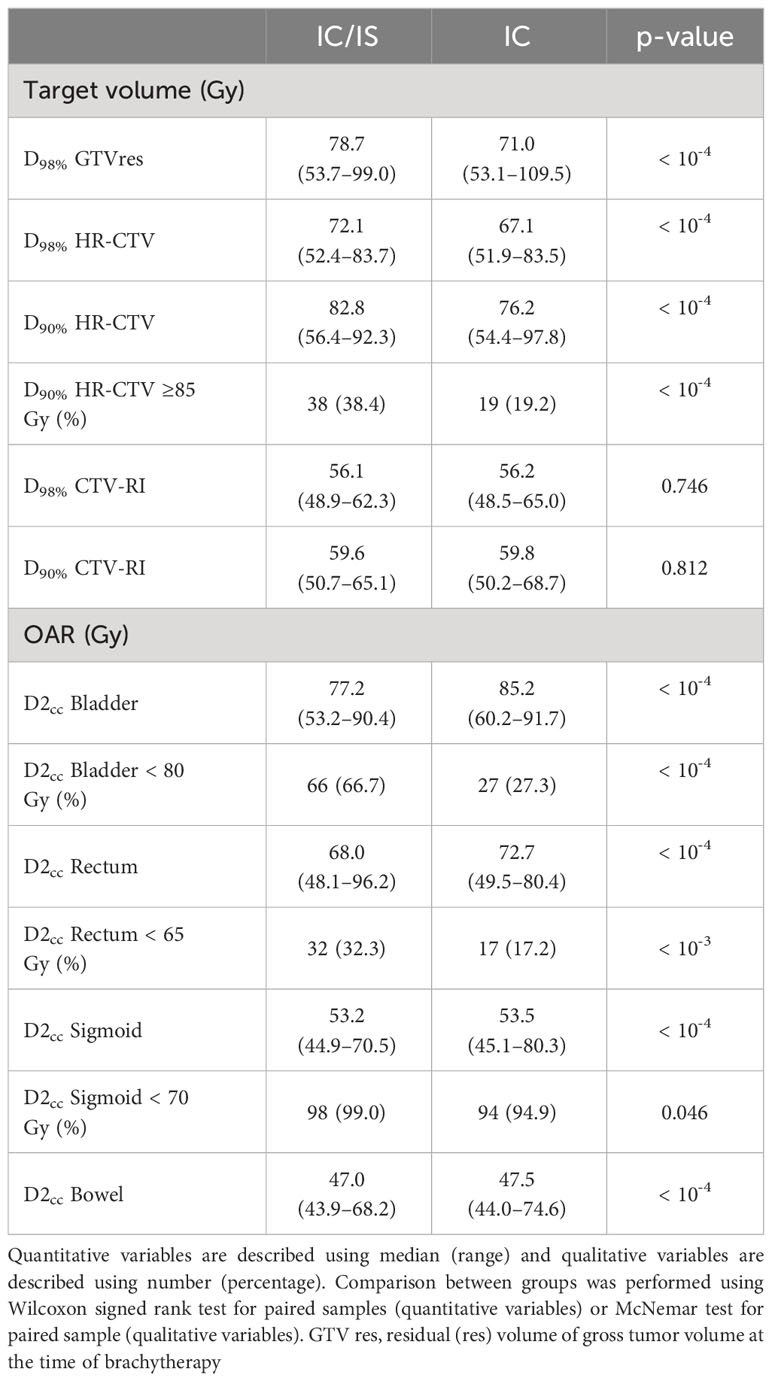
Table 2 Dosimetric analysis.
Figure 2 shows a scatterplot of D90% HR-CTV with IC/IS (ordinate) versus D90% HR-CTV with IC (abscissa). This graph shows the patients whose D90% HR-CTV with IC/IS was better than that with IC; these patients were above the bisector. Moreover, if we define good coverage as a D90% HR-CTV > 85 Gy, this graph shows that 21 (21.2%) patients benefited from needle insertion (green rectangle), while two (2.0%) patients were penalized (red rectangle). For the remaining 66 (66.7%) patients, there was no impact and coverage was good with or without the IC plan using a needle. Table 3 describes the different situations observed from Figure 3: the percentage of HR-CTV couverture depending on IC or IC/IS implantation.
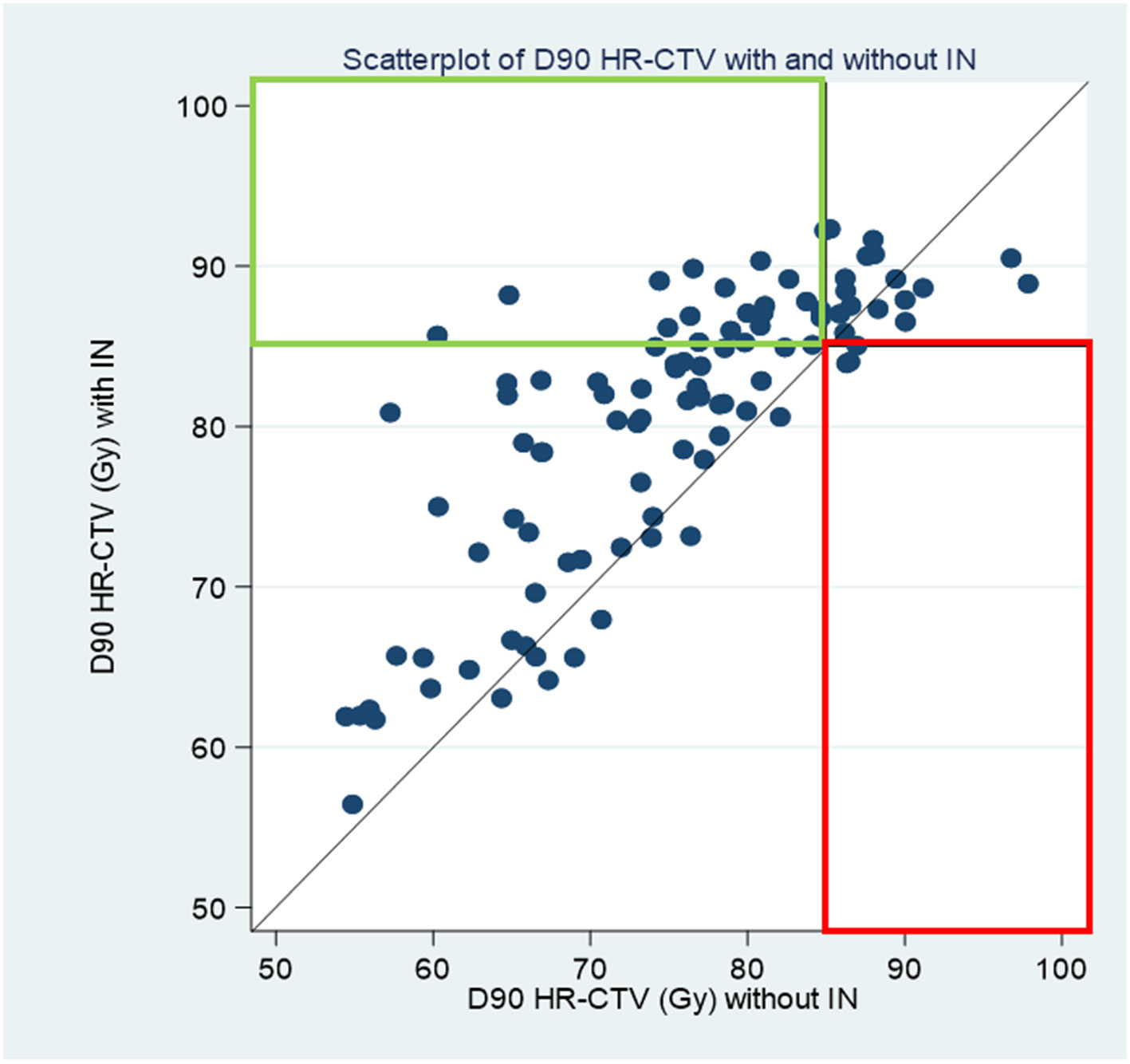
Figure 2 scatterplot of D90 HRCTV with IC IS versus D90 HRCTV with IC.
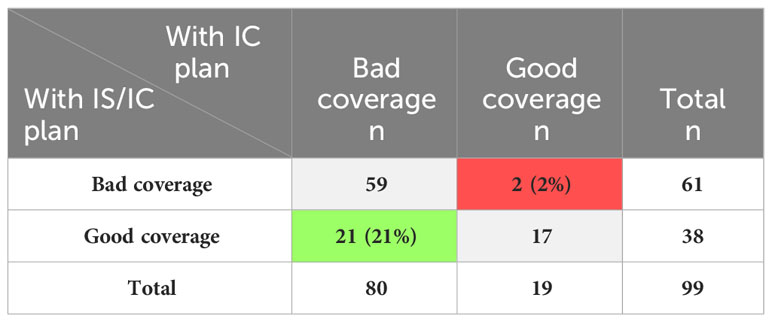
Table 3 Percentage of couverture depending on IC or IC/IS implantation.
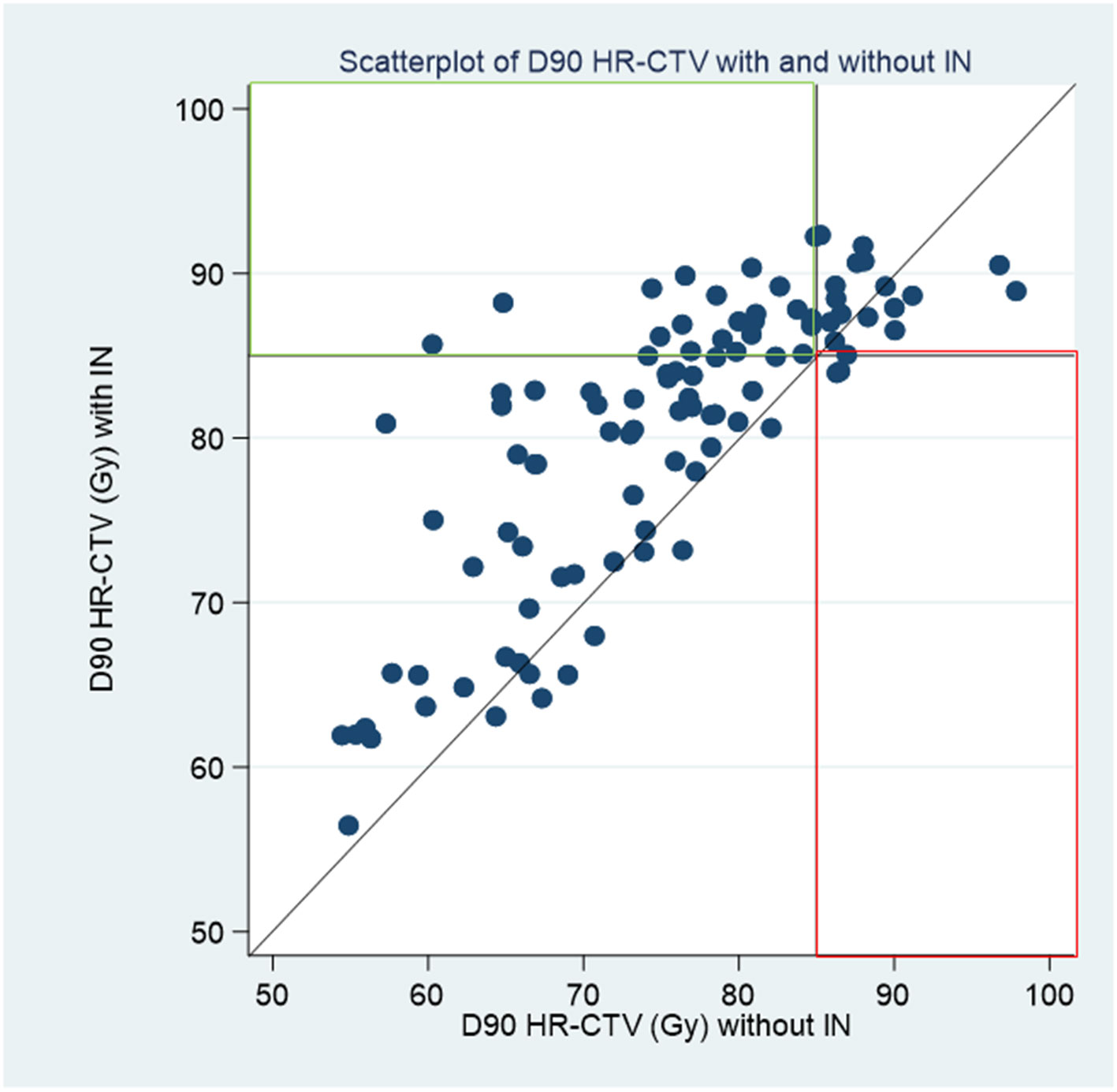
Figure 3 IC/IS HR-CTV D90 versus IC HR-CTV D90.
Using simple logistic regression models, we investigated whether there was a relationship between the benefit of IC/IS and FIGO 2018 stage, initial tumor size, laterality of affected parameters, number of needles placed, and period of needle placement, respectively (Table 4). There was a statistically significant relationship between the benefit of IC/IS versus IC alone and the laterality of the affected parameters (p = 0.05); however, this result should be interpreted with caution as the numbers are very small.
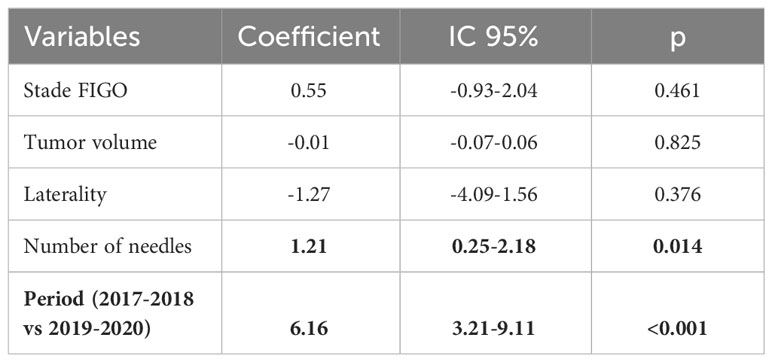
Table 4 Factors explaining the difference in HR-CTV D90 (IC/IS vs IC).
We performed this retrospective analysis of the first 99 patients treated at our institution using IGABT with IC/IS after RT or RCT for LACC. Our results showed a benefit of using interstitial needles during uterovaginal brachytherapy on target volume coverage, particularly in high-risk CTV (HR-CTV), in the management of LACC after RT or RCT. Indeed, the application of interstitial needles during uterine brachytherapy delivered 85 Gy on the D90 HR-CTV in 38.4% of patients, compared to only 19.2% if we had performed endo-uterine brachytherapy with IC plan interstitial needles. To interpret these results from the point of view of a new technique developed in our Brachytherapy Unit, we started performing interstitial implants in January 2017 and, at that time, our only applicator was the Utrecht. Therefore, we only had the possibility of implanting interstitial needles parallel to the endo-uterine probe, with no possibility of performing implants with oblique needles.
Mazeron et al. (10) showed in their series of 225 consecutively treated patients that the goal of administering > 85 Gy to the HR-CTV was only possible in 30.7% of the cases; in their series, there were no data on the percentage of patients treated with IGABT IC/IS. In our series, we identified only 21% of patients who benefited from IC/IS IGABT and, for 77% of patients, there was no benefit of adding IC/IS to IC alone, which can be explained by the learning process of the medical team, poor patient selection, and the inability to perform only IGABT implants with oblique needles to cover the disease in the distal parametria. Indeed, the interest in performing simulated treatment with IC/IS before starting brachytherapy was studied in 58 patients (17). The application of IC plan interstitial needles followed by dosimetric MRI was performed before brachytherapy. Finally, only 41% of patients received treatment with interstitial needles. Tumors eccentric to the endo-uterine probe and OAR close to the target volumes were good indications for brachytherapy with IC/IS. Furthermore, the D90 for HR-CTV was higher than 85 Gy EQD2 in all patients with the IC/IS preplan and only in 50% of the patients using the optimized IC preplan. The dose volume histogram constraints for OAR were respected in 79% of the IC/IS plans compared with 46% for the optimized IC preplan.
The first series of interstitial needles improved the dose in the HR-CTV. The RETRO EMBRACE series (18) retrospectively analyzed 610 patients treated by RCT and IGABT for LACC; the team investigated the evolution of IC brachytherapy towards IC/IS over time and proved that D90 HR-CTV EQD2 is superior when using IGABT with IC/IS (92 Gy ± 13 Gy) compared to IC alone. Similarly, the role of interstitial brachytherapy and the use of interstitial oblique and parallel needles were reported in 2019 (19). In 69 patients with longer residual tumor after RCT (HR-CTV volume: 69 ± 32 cm3), they showed that the D90 HR-CTV of 86 ± 7 Gy with cumulative mean EQD2 for the bladder, rectum, and sigmoid D2 cm3 was 86 ± 12 Gy, 68 ± 7 Gy, and 68 ± 9 Gy, respectively. In their series, they implanted a median of seven [3–15] needles with four oblique needles [1–7].
Rogowski et al. (20) published their series of 44 patients treated consecutively for LACC by RCT and IC/IS IGABT with the Venezia applicator. They showed that the D90 HR-CTV of 92.3 Gy EQD2 (72.2–100.8) with D2cc EQD2 for the bladder, rectum, sigmoid, and bowel were 74.8 Gy (58.6–89.7), 57.9 Gy (49.6–72.4), 60.0 Gy (47.2–75.0), and 52.4 Gy (44.1–72.1), respectively. This series illustrates how the use of oblique interstitial needles allows coverage of the target volume by decreasing the dose to organs such as the bladder, rectum, and sigmoid colon.
Our study proposes a design with a direct comparison of two treatment plans with and without IC interstitial needles during uterovaginal brachytherapy in a large population, which allows an adapted evaluation for each patient. We showed a correlation between the HR-CTV volume and the probability of needle implantation. It is important to note that, during the study period, we used an Utrecht applicator with the possibility of inserting only interstitial needles parallel to the endo-uterine probe, without the possibility of inserting oblique needles for more distal parametrial infiltrations.
There is also a factor linked to the period in which the implants were placed and HR-CTV coverage. Our results in terms of HR-CTV coverage were better in the period of 2019–2020 than in 2017–2018. This effect can be explained by several factors, but is probably due to a better selection of patients and better acknowledgement of the IC/IS technique.
We chose to conduct the analyses on the target volumes, with the only limit being the maximum acceptable dose received in nearby OAR. The D2cc EQD2 delivered to the bladder (75.5 vs 81.1 Gy), rectum (67.2 vs 70.2 Gy), and sigmoid (53.8 Gy vs 55 Gy) are, therefore, higher than for brachytherapy with interstitial needles, and the analyses performed are, therefore, not interpretable in view of the study design.
Our study had some limitations. We observed poorer coverage of HR-CTV, explained by several reasons. It is our experience that, in the treatment of patients with larger tumors using the IC/IS IGABT technique and learning time from initiation of a new technique, obtaining expected results is important, and eligibility of patients to IC/IS may be difficult. We also initiated this technique with an Utrecht applicator that gives you the opportunity to place interstitial needles only in the same axis of the intrauterine tandem; we did not place oblique needles for patients who presented with more distal parametrial infiltration.
The use of interstitial brachytherapy in the management of LACC after radiotherapy provides better coverage of the target volumes, this could contribute to better local control and improved survival of treated patients. This study reflects the real-life treatment of patients with initial tumors and a poor prognosis. The recent use of brachytherapy with interstitial needles in these patients has resulted in better tumor coverage, and the experience developed by the interventional team could also be a factor in better local tumor control.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Centre Oscar Lambret CEC, Lille, France. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because The included patients did not object to the use of their clinical data for research purposes, and the study complied with the Reference Methodology MR004 adopted by the Commission Nationale de l’Informatique et des Libertés (CNIL).
AC: Conceptualization, Methodology, Project administration, Resources, Validation, Writing – original draft, Writing – review & editing. EG: Methodology, Writing – original draft, Writing – review & editing. AE: Conceptualization, Methodology, Validation, Writing – review & editing. AN: Validation, Writing – review & editing. RC: Formal analysis, Writing – review & editing. AH: Formal analysis, Writing – review & editing. ML: Formal analysis, Writing – review & editing. FN: Writing – review & editing. DH: Writing – review & editing. CMG: Writing – review & editing. SC: Validation, Writing – original draft, Writing – review & editing. M-CLD: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. MB: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. EL: Conceptualization, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. (2019) 393:169–82. doi: 10.1016/S0140-6736(18)32470-X
2. Compaoré ZC, Monnet E, Gérazime A, Molinié F, Guizard AV, Delafosse P, et al. To what extent do age, stage and treatment influence survival after invasive cervical cancer: A French population-based study. Cancer Causes Control. (2022) 33:403–15. doi: 10.1007/s10552-021-01536-9
3. Schuind AE, Rees H, Schiller J, Mugo N, Dull P, Barnabas R, et al. State-of-the-Science of human papillomavirus vaccination in women with human immunodeficiency virus: Summary of a scientific workshop. Prev Med Rep. (2023) 35:102331. doi: 10.1016/j.pmedr.2023.102331
4. Cibula D, Pötter R, Planchamp F, Avall-Lundqvist E, Fischerova D, Haie Meder C, et al. The European society of gynaecological oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines for the management of patients with cervical cancer. Radiother Oncol. (2018) 127:404–16. doi: 10.1016/j.radonc.2018.03.003
5. Han K, Milosevic M, Fyles A, Pintilie M, Viswanathan AN. Trends in the utilization of brachytherapy in cervical cancer in the United States. Int J Radiat Oncol Biol Phys. (2013) 87:111–9. doi: 10.1016/j.ijrobp.2013.05.033
6. Dimopoulos JCA, Petrow P, Tanderup K, Petric P, Berger D, Kirisits C, et al. Recommendations from gynaecological (GYN) GEC-ESTRO working group (IV): Basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother Oncol. (2012) 103:113–22. doi: 10.1016/j.radonc.2011.12.024
7. Serban M, Kirisits C, de Leeuw A, ötter R, Jürgenliemk-Schulz I, Nesvacil N, et al. Ring versus ovoids and intracavitary versus intracavitary-interstitial applicators in cervical cancer brachytherapy: Results from the EMBRACE I Study. Int J Radiat Oncol Biol Phys. (2020) 106:1052–62. doi: 10.1016/j.ijrobp.2019.12.019
8. Dimopoulos JCA, Pötter R, Lang S, Fidarova E, Georg P, Dörr W, et al. Dose–effect relationship for local control of cervical cancer by magnetic resonance image-guided brachytherapy. Radiother Oncol. (2009) 93:311–5. doi: 10.1016/j.radonc.2009.07.001
9. Dimopoulos JCA, Schirl G, Baldinger A, Helbich TH, Pötter R. MRI assessment of cervical cancer for adaptive radiotherapy. Strahlenther Onkol. (2009) 185:282–7. doi: 10.1007/s00066-009-1918-7
10. Mazeron R, Castelnau-Marchand P, Dumas I, del Campo ER, Kom LK, Martinetti F, et al. Impact of treatment time and dose escalation on local control in locally advanced cervical cancer treated by chemoradiation and image-guided pulsed-dose rate adaptive brachytherapy. Radiother Oncol. (2015) 114:257–63. doi: 10.1016/j.radonc.2014.11.045
11. Petric P, Lindegaard JC, Sturdza A, Fokdal L, Kirchheiner K, Tan LT, et al. Results of image guided brachytherapy for stage IB cervical cancer in the RetroEMBRACE study. Radiother Oncol. (2021) 157:24–31. doi: 10.1016/j.radonc.2021.01.005
12. Sturdza A, Pötter R, Fokdal LU, Haie-Meder C, Tan LT, Mazeron R, et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother Oncol. (2016) 120:428–33. doi: 10.1016/j.radonc.2016.03.011
13. Pötter R, Tanderup K, Schmid MP, Jürgenliemk-Schulz I, Haie-Meder C, Fokdal LU, et al. MRI-guided adaptive brachytherapy in locally advanced cervical cancer (EMBRACE-I): A multicentre prospective cohort study. Lancet Oncol. (2021) 22:538–47. doi: 10.1016/S1470-2045(20)30753-1
14. Chargari C, Tanderup K, Planchamp F, Chiva L, Humphrey P, Sturdza A, et al. ESGO/ESTRO quality indicators for radiation therapy of cervical cancer. Radiother Oncol. (2023) 183:109589. doi: 10.1016/j.radonc.2023.109589
15. Bhatla N, Berek JS, Cuello Fredes M, Denny LA, Grenman S, Karunaratne K, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet. (2019) 145:129–35. doi: 10.1002/ijgo.12749
16. Pötter R, Tanderup K, Kirisits C, de Leeuw A, Kirchheiner K, Nout R, et al. The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. Clin Transl Radiat Oncol. (2018) 9:48–60. doi: 10.1016/j.ctro.2018.01.001
17. Fokdal L, Tanderup K, Hokland SB, Røhl L, Pedersen EM, Nielsen SK, et al. Clinical feasibility of combined intracavitary/interstitial brachytherapy in locally advanced cervical cancer employing MRI with a tandem/ring applicator in situ and virtual preplanning of the interstitial component. Radiother Oncol. (2013) 107:63–8. doi: 10.1016/j.radonc.2013.01.010
18. Fokdal L, Sturdza A, Mazeron R, Haie-Meder C, Tan LT, Gillham C, et al. Image guided adaptive brachytherapy with combined intracavitary and interstitial technique improves the therapeutic ratio in locally advanced cervical cancer: Analysis from the retroEMBRACE study. Radiother Oncol. (2016) 120:434–40. doi: 10.1016/j.radonc.2016.03.020
19. Mahantshetty U, Sturdza A, Naga Ch P, Berger D, Fortin I, Motisi L, et al. Vienna-II ring applicator for distal parametrial/pelvic wall disease in cervical cancer brachytherapy: An experience from two institutions: Clinical feasibility and outcome. Radiother Oncol. (2019) 141:123–9. doi: 10.1016/j.radonc.2019.08.004
Keywords: cervical cancer, brachytherapy, radiotherapy, interstitial needles, chemotherapy
Citation: Cordoba A, Gesta E, Escande A, Noeuveglise A, Cayez R, Halty A, Ladjimi MT, Narducci F, Hudry D, Martinez Gomez C, Cordoba S, Le Deley M-C, Barthoulot M and Lartigau EF (2024) Interstitial needles versus intracavitary applicators only for locally advanced cervical cancer: results from real-life dosimetric comparisons. Front. Oncol. 14:1347727. doi: 10.3389/fonc.2024.1347727
Received: 01 December 2023; Accepted: 09 February 2024;
Published: 19 March 2024.
Edited by:
Timothy James Kinsella, Brown University, United StatesReviewed by:
Valentina Lancellotta, Agostino Gemelli University Polyclinic (IRCCS), ItalyCopyright © 2024 Cordoba, Gesta, Escande, Noeuveglise, Cayez, Halty, Ladjimi, Narducci, Hudry, Martinez Gomez, Cordoba, Le Deley, Barthoulot and Lartigau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abel Cordoba, YS1jb3Jkb2JhQG8tbGFtYnJldC5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.