 Claudia Robles1*
Claudia Robles1* Laura Monfil1
Laura Monfil1 Raquel Ibáñez1,2
Raquel Ibáñez1,2 Esther Roura1,2Rebeca Font3
Esther Roura1,2Rebeca Font3 Paula Peremiquel-Trillas1,2,4
Paula Peremiquel-Trillas1,2,4 Maria Brotons1,2
Maria Brotons1,2 Cristina Martínez-Bueno4,5,6
Cristina Martínez-Bueno4,5,6 Silvia de Sanjosé7,8Josep Alfons Espinàs3
Silvia de Sanjosé7,8Josep Alfons Espinàs3 Laia Bruni1,2
Laia Bruni1,2- 1Unit of Infections and Cancer – Information and Interventions, Cancer Epidemiology Research Programme, Institut Català d’Oncologia (ICO), Infections and Cancer Group, Epidemiology, Public Health, Cancer Prevention and Palliative Care Program, Institut d’Investigació Biomèdica de Bellvitge (IDIBELL), L’Hospitalet de Llobregat, Barcelona, Spain
- 2Centro de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP - CB06/02/0073), Madrid, Spain
- 3Catalan Cancer Strategy, Department of Health, Catalonia, Spain
- 4University of Barcelona, Barcelona, Spain
- 5Atenció a la Salut Sexual i Reproductiva (ASSIR) Catalunya, Institut Català de la Salut, Barcelona, Spain
- 6Grup de Recerca en Salut Sexual i Reproductiva (GRASSIR), Barcelona, Spain
- 7Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, MD, United States
- 8Institut de Salut Global (ISGlobal), Barcelona, Spain
Background: The COVID-19 pandemic led to a national lockdown and the interruption of all cancer preventive services, including cervical cancer screening. We aimed to assess the COVID-19 pandemic impact on opportunistic screening participation, abnormal cytology (ASCUS+) prevalence and screening interval in 2020 and 2021 within the Public Health System of Catalonia, Spain.
Methods: Individual data on cytology and HPV testing of women aged 25–65 from 2014 to 2021 were retrieved from the Information System for Primary Care Services (SISAP). Time-series regression models were used to estimate expected screening participation and abnormal cytology prevalence in 2020 and 2021. The impact was determined by comparing observed and expected values (ratios). Additionally, changes in screening interval trends between 2014 and 2021 were assessed by fitting a Piecewise linear regression model.
Results: Cervical cancer screening participation decreased by 38.8% and 2.2% in 2020 and 2021, respectively, with the most significant impact on participation (-96.1%) occurring in April 2020. Among older women, participation was lower, and it took longer to recover. Abnormal cytology prevalence was 1.4 times higher than expected in 2020 and 2021, with variations by age (range=1.1–1.5). From June 2020 onwards, the screening interval trend significantly changed from an increase of 0.59 to 3.57 months per year, resulting in a median time of 48 months by December 2021.
Conclusions: During the pandemic, fewer women have participated in cervical cancer screening, abnormal cytology prevalence has increased, and the screening interval is more prolonged than before. The potential cervical cancer lifetime risk implications highlight the need for organized HPV-based screening.
Introduction
The COVID-19 pandemic has had a significant impact on cancer screening programs around the world. Numerous countries worldwide have reported varying degrees of reductions in participation (1–5). For example, in comparison to 2019, Slovenia saw a 92% decline in cytology volume between March and May 2020 (6), while Belgium experienced a 43% reduction in volume between January and April 2020 (7). Meanwhile, the United States reported a 92% decrease in participation compared to 2019 during March and April 2020 (8). In Peru, a 76% reduction in cytology volume was observed for 2020 compared to the expected volume based on modeled data (9)
In Spain, a nationwide lockdown was imposed on March 14th 2020. All cancer preventive services, including cervical cancer screening, were suspended, and only follow-up appointments for previous abnormal results were maintained (10). The lockdown was gradually lifted between May 11th and June 2020 (11), and primary screening in Catalonia was partially resumed in July 2020. In the two years since the pandemic began, six COVID-19 waves have occurred. Containment measures for these waves have varied across and within Spanish regions, including social distancing or mobility restriction within residential areas, although exceptions were made for medical visits.
The medium- and long-term impact of these disruptions on cervical cancer is still uncertain although Mexico has observed an increasing trend in the proportion of advanced stage and metastatic cancer cases (12). In Catalonia, the COVID-19 pandemic and related control measures have resulted in cancer underdiagnosis (13–15). In the two years since the lockdown, 11% fewer cervical cancers have been diagnosed, and as of February 2022, cervical cancer detection in Catalonia had not yet returned to pre-pandemic levels (15). The potential impact on the cancer stage is unknown. However, no differences have been observed in the prevalence of cancer diagnoses in pathology records from 2019 and 2020 in two hospitals in Girona (16).
When the pandemic began, Catalonia was offering opportunistic cytology-based cervical cancer screening to women aged 25 to 65 through the public primary care system. The first pandemic wave hit when the transition from cytology-based to HPV-based screening on clinician-collected samples had just begun through a pre-scale-up pilot in an area of Barcelona city on October 2019 (17). Therefore, a significant consequence of the pandemic in Catalonia was the interruption and delay in the transition to primary HPV testing that was underway. To date, HPV testing has not yet been extended to the entire territory due to the pandemic, which prompted the development of a newly organized cervical cancer screening program based on self-sampling. This new strategy aimed to counteract the reduced number of scheduled visits to facilitate social distancing and the lower willingness of potential participants to visit a health center after the lockdown period. Accordingly, a pilot program for HPV testing of self-collected samples was launched in July 2021 in Metropolitana Sud, a metropolitan area in the south of Barcelona city (18).
A better understanding of the post-lockdown screening landscape can help inform decisions on the best catch-up strategies for under screened women. However, only some studies have explored the impact of the pandemic beyond the lockdown period. Germany reported a lower average number of women screened per clinic in 2021 than in 2020 (19). In the United States, despite a rebound in the third quarter of 2020, a slow decline in screening rates has been observed up to the last quarter of 2021 (20).
The pandemic has likely led to longer screening intervals between cervical cancer screenings, as observed for breast and colorectal cancer screening in Belgium (21). However, the same study also found that there were either no differences or shorter screening intervals in cervical cancer screening during the pandemic compared to before, probably due to the opportunistic screening and follow-up tests done during the lockdown. Women with longer screening intervals have a higher risk of disease and therefore higher prevalences of abnormal cytology or biopsy results are expected. In Brazil, the prevalence of abnormal cytology findings remained unchanged overtime; however, in 2020 and 2021, the CIN3 prevalence doubled compared to the 1.9% observed in 2019 (22). Other studies have only explored changes in the number of cases, and as observed with cancer diagnoses, underdiagnosis of high-grade cytologies and CIN2+ cases have been described in Slovenia and Canada, respectively (6, 23).
We evaluated the impact of the COVID-19 pandemic on opportunistic screening participation, abnormal cytology prevalence, and screening intervals within the Catalan public health system throughout the first two years after the pandemic started (period 2020–2021) using primary care electronic health records data.
Materials and methods
We performed a time-series analysis of 2020 and 2021 on the participation, abnormal cytology prevalence and screening interval in the opportunistic cervical cancer screening program of Catalonia.
Study population
Catalonia is a northeastern region of Spain with a total population of almost 8 million, including about 2.2 million women aged between 25–65 years who are targeted for cervical cancer screening.
In Catalonia, screening is opportunistic and free of charge within the public health system, which is administratively divided into seven health regions. Women are screened based on their age and previous screening history, either when they request it or when they visit the sexual and reproductive health centers for other reasons. At the time of this analysis, screening is still mainly cytology-based, with repeat testing every three years, except in two piloting areas where cytology is offered only to women aged 25–29 years, and HPV testing is being implemented every five years to those aged 30–65 years. The scale-up to a full organized HPV-based program is being planned for the coming years.
Data source
Anonymized individual data were retrieved from the Primary Care Services Information System (SISAP). This is an electronic healthcare database containing structured primary care data from the Catalan Health Institute (ICS), the leading primary care provider of public health services in Catalonia. This provider manages about 75% of all Catalan primary care practices and covers around 80% of the Catalan population, which has proven to be highly representative of the population of Catalonia in terms of geographical area, age distribution and gender (24).
Historical screening self-reported or systematically registered data from 2008 onwards were retrieved from all women aged 25–65 who were assigned to primary care centers under the ICS between 2014 and 2021 regardless of their cervical cancer or hysterectomy history. Data included demographics (age and administrative health region) and all recorded cervical cancer screening related data, including the sampling date, type of screening test (cytology, HPV testing or both) and test results.
Statistical analysis
The impact of the pandemic was explored on screening participation (defined as the proportion of screened women among the number of age-eligible women), abnormal cytology prevalence (defined as the proportion of cytologies with a result of atypical squamous cells of undetermined significance or worse (ASC-US+) among the total number of cytologies performed with a valid result), and screening interval (defined as the median number of months between the current screening event and the last screening cytology among women with no history of abnormal results).
Time-series regression was used to estimate the monthly expected screening participation and the abnormal cytology prevalence for 2020 and 2021.
Data from 2014 to 2018 (training set) were used to initially forecast the expected estimates for 2019 (test set) to validate the model. Data decomposition by moving averages showed a trend and seasonality pattern. Therefore, potentially suitable predictive models included a i) time series linear model potentially adjusted for trend and seasonality, ii) an autoregressive integrated moving average (ARIMA) model and iii) a Holt-winters additive model (25–27). Among these, the best-fit model was selected based on performance metrics (lower errors), residual examination and forecast values in the overall population. Further details on the model validation and selection are provided in Supplementary Material 1.
Once the best model was defined, 2019 data was incorporated into the regression models to project a 24-month forecast of the screening participation and abnormal cytology prevalence along with their 95% prediction interval (95%PI) over 2020 and 2021. The administrative health region of Girona (only 3.3% of the analysis population) had to be excluded from the forecast models for the overall Catalonia and age-stratified estimates because it behaved as an outlier and produced biased results. It is a region where the COVID-19 containment measures and the resumption of screening activity differed significantly from the rest of the regions (early 2022 instead of summer 2020 elsewhere in Catalonia).
Best-fit models were a time-series regression model adjusted for trend and seasonality for the screening participation analysis, whereas the expected abnormal cytology prevalence was estimated by adjusting a Holt-winters model.
The monthly impacts of COVID-19 on screening participation and abnormal cytology prevalence were estimated as ratios of observed values to expected ones. Ratio ranges included the ratios obtained when observed estimates are compared to the lower and the upper bounds of the 95%PI expected values. Expected values for time periods were estimated as the sum of monthly expected values except for those months in which expected values were not statistically different from observed ones, in which case, the latter were used.
Changes in abnormal cytology prevalence may result from increased screening intervals due to lower participation in screening. Therefore, the median number of months since the last screening cytology (not follow-up) with a normal result was estimated for all women with no history of previous abnormal results, screened between 2014 and 2021 and irrespective of the screening test used. The screening intervals’ median trend over time was assessed by fitting a piecewise linear regression model to identify potential breakpoints (changes in trend) and to quantify the increases in the median time for each identified period. Differences by abnormal cytology status were assessed using a non-parametric equality-of-medians test.
Analyses were conducted using statistical R version 4.2.1 (http://www.R-project.org) and Stata version 16.1.
Ethical aspects
This research has been approved by the Ethics Committee from the Hospital Universitari de Bellvitge (code PR271/11). It complies with the national and international regulations on ethics and data protection.
Results
Screening participation
Overall, 1,598,069 women aged 25–65 years were assigned to an ICS primary care and ICS gynecology service between 2014 and 2021. Out of these, 706,432 women participated in cervical cancer screening at least once during this period. The average monthly screening participation between 2014 and 2019 was 0.88%, with lower participation in August and December (summer and Christmas holidays).
Time-regression analyses showed that in 2020 there was a reduction in participation of 38.8% (ratio=0.61; range=0.56,0.68) in women aged 25–65 years (Table 1). The predicted monthly screening participation in 2020 based on previous years would have ranged between 0.53 and 1.05% of eligible women aged 25–65. However, observed participation dropped to 0.04% of eligible women screened in April 2020 (ratio=0.04; range=0.03,0.05) (Supplementary Table 1). Over the full year 2021, screening participation was reduced by 2.2% (ratio=0.98; range=0.97,0.99) due to the 24% lower participation observed in January 2021 (ratio=0.76; range=0.66,0.89).
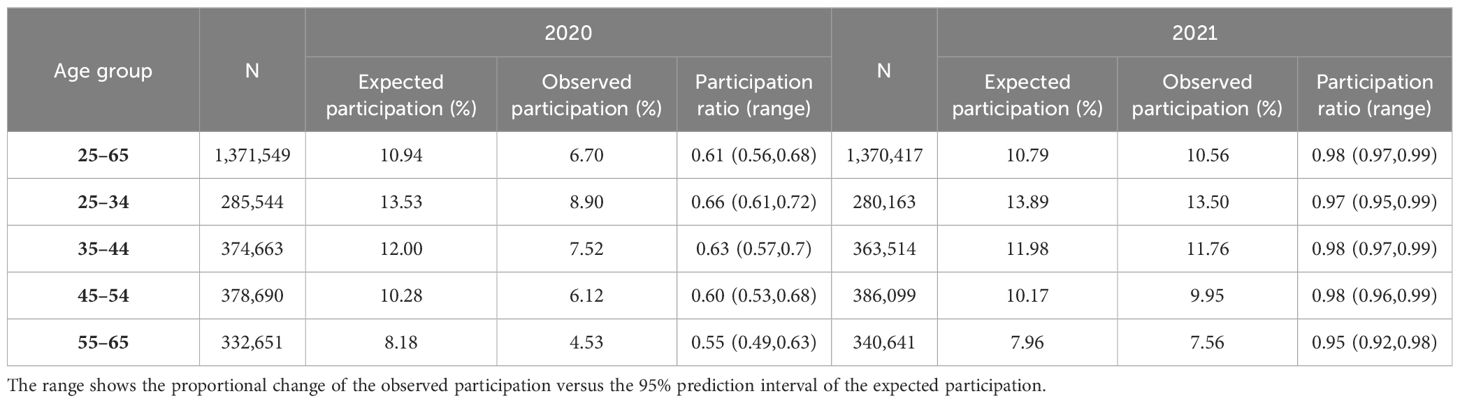
Table 1 Participation ratio between observed and expected participation by age group in 2020–2021.
Stratified results by age groups (Table 1 and Figure 1) showed higher reductions in observed versus expected participation at increasing age groups (in 2020, 34.3% fewer women aged 25–34 were screened compared to 44.7% fewer women aged 55–65). Expected screening participation estimates were achieved at a different pace depending on the age group (Supplementary Table 2); in women aged 25–34, participation recovery was achieved in October 2020; in women aged 35–44 and 45–54 years, it was achieved in November 2020 whereas, in women aged 55–65 years, it was definitively achieved in March 2021.
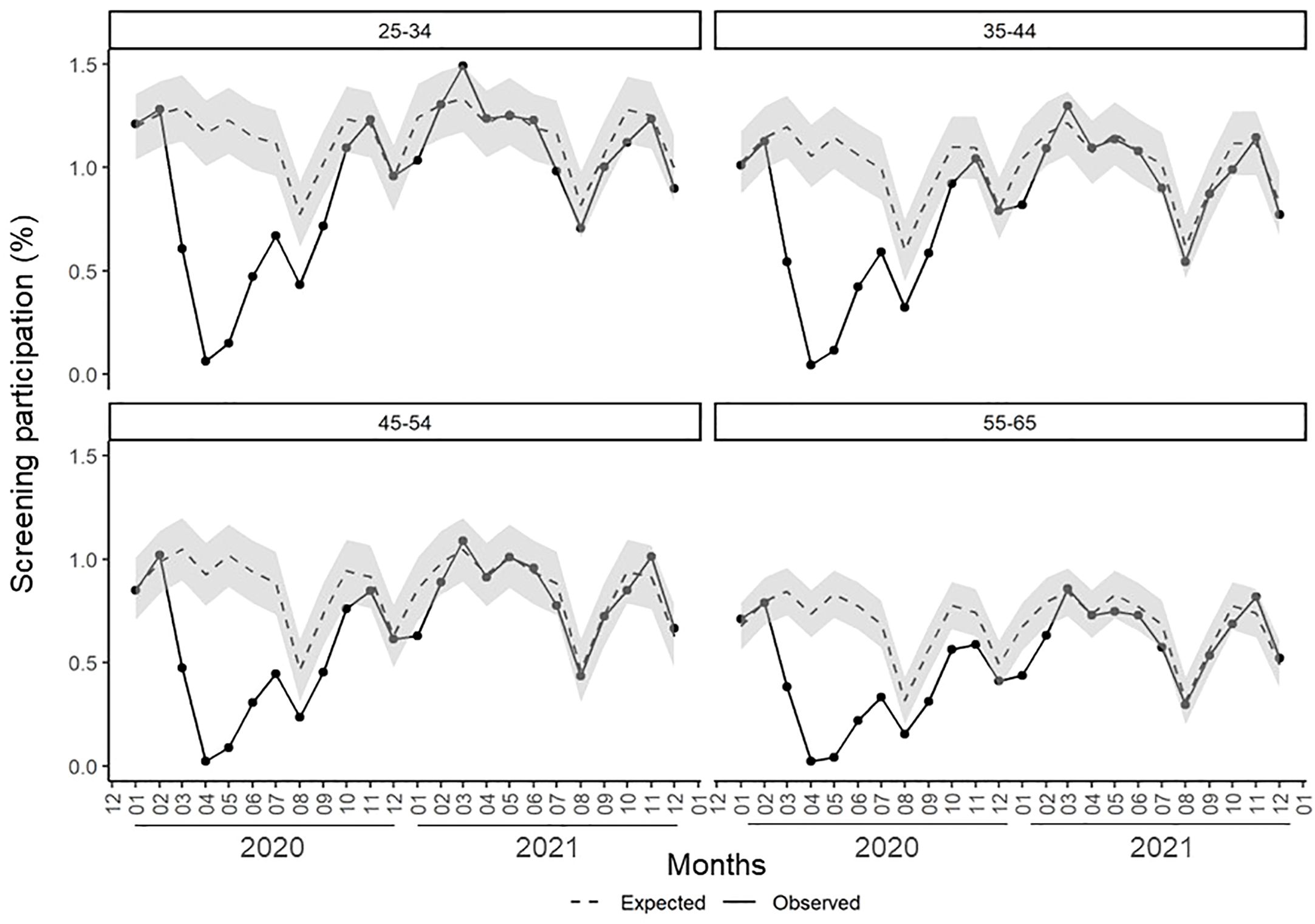
Figure 1 Monthly screening participation (expected and observed) in 2020 and 2021 in Catalonia by age group. Grey area depicts the 95% prediction interval of the expected monthly participation based on observed data from 2014-2019.
Differences in participation were also observed by health region (Supplementary Table 3). In 2020, screening activity decreased by 24% to 52% depending on the region. In 2021, some regions showed no statistically significant decrease in expected activity while others only experienced a minor reduction (<5%). However, in Girona, where the resumption of activity occurred on January 2022, 44% fewer women got screened.
Abnormal cytology prevalence
The expected abnormal cytology prevalence in women aged 25–65 for 2020 was 4.40%, but the observed prevalence was 5.92% (ratio=1.35; range=1.22,1.50) (Table 2). In 2021, abnormal cytology prevalence was slightly higher than in 2020 (ratio=1.38; range=1.16,1.71).
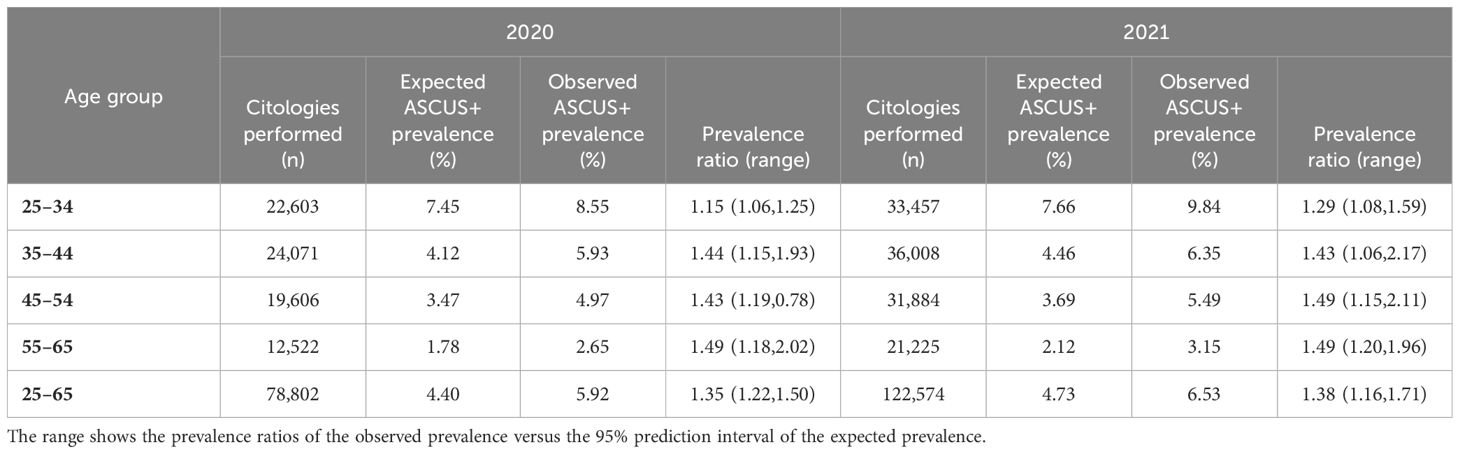
Table 2 Prevalence ratio between observed and expected abnormal cytology (ASCUS+) prevalences by age group in 2020–2021.
By age group, abnormal cytology prevalence ranged between 8.6% in women aged 25–34 to 2.7% in those aged 55–65 in 2020 and between 9.8 and 3.1% in 2021, respectively (Table 2). These observed annual abnormal cytology prevalences were between 1.1 and 1.5 times higher than expected. Lower increases in those prevalences were observed in women aged 25–34.
Time since last normal screening cytology (screening interval)
Analysis of the trend in the median time since the last normal screening cytology identified an inflection point in June 2020 (Figure 2). Between January 2014 and May 2020, the median time increased from 38.1 to 40.6 months, respectively (0.59 months per year; 95%CI=0.46,0.71). From June 2020 onwards, the median time increased by 3.57 months per year (95%CI=2.42,4.71). This resulted in an increase in the median time from 41.6 months in June 2020 to 48.0 months in December 2021 (Supplementary Table 4).
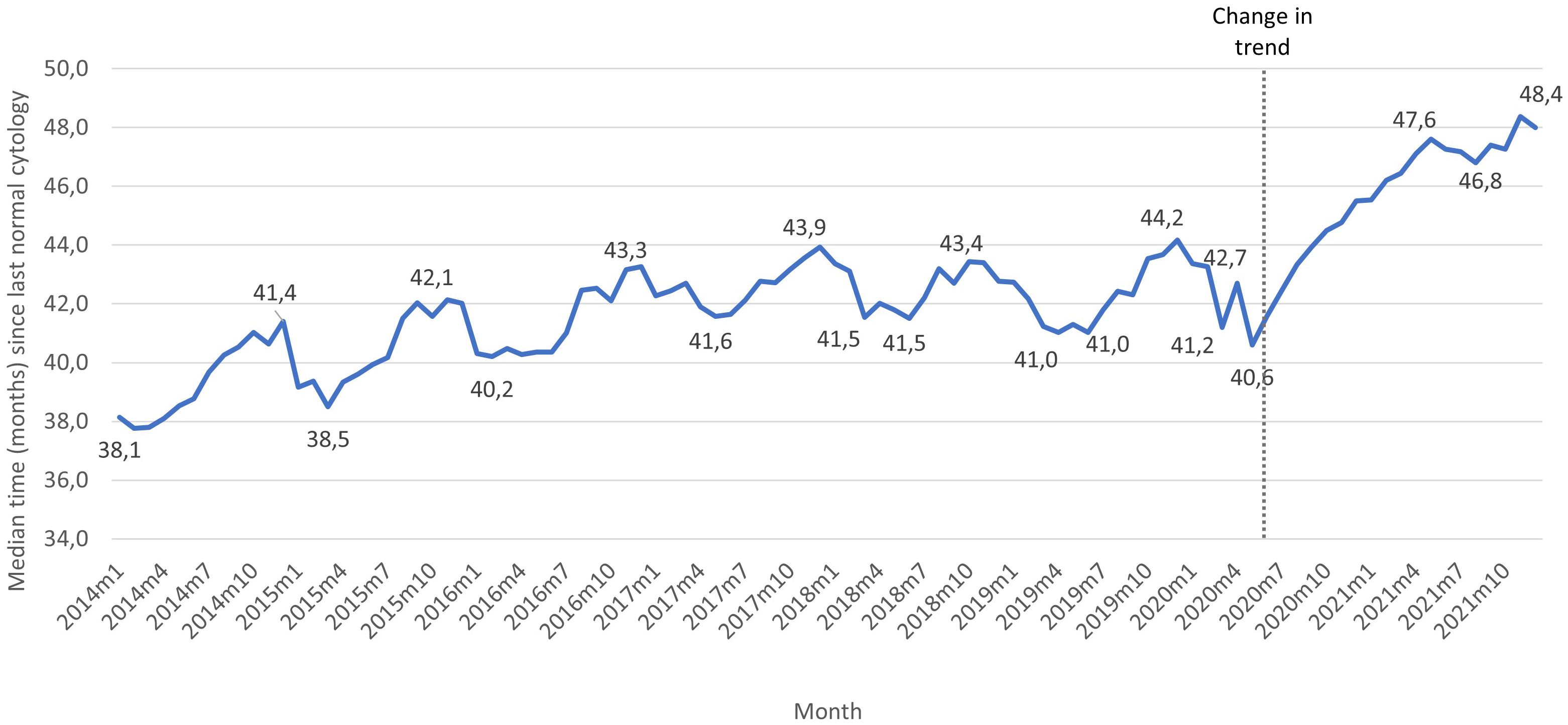
Figure 2 Median time (months) since the last normal screening cytology among women aged 25-65 years with no previous history of abnormal results screened between 2014 and 2021. The figure shows the highest and lower values in median time over the years 2014 and 2021. All monthly values can be found in Supplementary Table 3.
Women with an abnormal cytology result showed statistically significant higher screening intervals than those with a normal cytology (45 versus 43.8 months in 2020 and 48.8 versus 46.6 months in 2021).
Discussion
In Catalonia, after the lockdown period due to the COVID-19 pandemic, lower participation in cervical cancer opportunistic screening was observed in 2020 and 2021, although it highly improved in 2021. Participation was lower at increasing ages. Since the pandemic, a higher abnormal cytology prevalence and a larger screening interval have also been observed.
During the lockdown period in Catalonia, there was up to a 96% reduction in participation to cervical cancer screening in April 2020. Similarly, others have reported the highest impact in April 2020 with similar estimates (7, 8, 28). However, pooled data from other studies worldwide show the most significant reduced cervical cancer screening participation in March 2020 (5), whereas in Slovenia and Japan, it took place in May 2020 (6, 29). The start and end of lockdown periods had likely played a role when the highest reduction was observed.
In 2020, 39% fewer women (47% if the first two months without contentious measures implemented are excluded from the analysis) participated in cervical cancer screening in Catalonia. Different countries have described lower participation or screening test volumes (2–5). However, the impact estimate highly depends on the reported period, which hampers a straight comparison with others. The impact of COVID-19 in Catalonia over the 12 months period of 2020 was higher than the 23% lower cytology volume reported in Slovenia over a 7-month period in the same year (6) and the 36% lower screening estimated for the United States over a 9-month period, also in 2020 (8). However, it was less severe than the 76% reduction in cytology volume observed in Peru over the same 12-month period (9). Overall, in 2021, 2% fewer women participated in cervical cancer screening because of the reduced participation in January (24% reduction) as the third epidemic wave took place and mobility restrictions were again implemented. However, these mobility restrictions did not prohibit attendance to cancer screening visits. Therefore, this lower participation might be related to changes in women’s attitude towards self-care behavior, such as the self-reported lower willingness to attend cervical cancer screening and the perception that screening tests were not urgent in the United Kingdom (30, 31) or the observed longer time to help-seeking for cancer symptoms in Spain (32) after the first COVID-19 pandemic wave. Except for January, observed participation in 2021 was not different than expected, as opposed to the lower estimates observed in Germany and the United States (19, 20).
At an increasing age, Catalonia observed a more considerable impact in screening participation and a slower recovery in regular participation. Lower participation at increasing age was also observed in Slovenia (6), whereas a larger impact was observed in England at young ages (33). The higher impact in women aged 55–65 years than those younger might be related to a higher self-perceived risk of getting severe COVID-19 if infected by the SARS-CoV2 virus at older ages and willingness to avoid contact with the health system unless symptomatic.
The COVID-19 pandemic in Catalonia has not only affected the still opportunistic cervical cancer screening activities. Lower participation in organized cancer screening programs in the region has also been observed for breast (34) and colorectal (35) cancer screening programs. A lower number of diagnoses have also been observed in other chronic diseases managed at primary care services, such as asthma or ischemic heart disease (36).
A higher prevalence of abnormal cytology was observed after the lockdown period (up to 1.5 times higher than expected). The validation of the predictive models with 2014 - 2018 data showed an increasing trend in abnormal cytologies prevalence before the pandemic, yet it was used to adjust the expected prevalences for 2020 and 2021. It follows that the previously observed trend does not explain the observed higher prevalence of abnormal cytology during the pandemic. In Brazil, the prevalence of abnormal cytology findings remained unchanged in the years 2020 and 2021 but, in São Paulo city, the CIN3 prevalence increased (4.5% in 2020 and 3.8% in 2021) in comparison with the 1.9% CIN3 prevalence in 2019 (22). The authors argue that the increase in CIN3 might be related to the follow-up of 2019 abnormal cytology results. Ours is the first study to measure an increase in cytology abnormal prevalence since the pandemic started although we cannot assess whether this increase in cytology abnormality has resulted in an increase in CIN2+ prevalence.
Another potential explanation for the higher prevalence could be related to a larger screening interval. The longer the period after a normal screening result, the lower assurance that the patient remains disease-free and, therefore, a greater prevalence of abnormal cytology results. In our study, we have observed an increasing median time since the last normal cytology from June 2020 onwards among all women and a longer interval in those with an abnormal cytology result compared to those with a normal one. To our knowledge, only one study has explored the cervical cancer screening interval with contrasting findings to our study. In Belgium, no differences in the screening interval were observed between the pre-pandemic and pandemic periods (21). The authors attribute this to the opportunistic screening activity and the follow-up tests done during the lockdown period. In contrast, we excluded follow-up tests from the analyses to accurately estimate the median time since the last screening test, which was 48 months by December 2021.
According to modeling studies, COVID-19-related screening delays have a lower impact on the lifetime cervical cancer risk than the screening test used and the screening frequency (37). Another study estimated that the risk of cervical cancer is higher in women missing the screening round, i.e., those being screened, although with a longer screening interval. Therefore, catch-up campaigns using HPV testing have been suggested to address this issue (38). However, due to a potentially limited capacity in screening organizations, others have estimated that the best balance between screening capacity and health impact is to ensure that women are screened, even if it is done at a longer interval (39). This is consistent with the increased risk observed in women that missed their round (i.e., a delay in screening participation equal to the screening interval) than those that were screened at a longer screening interval (40). However, in Catalonia, cervical cancer screening is still opportunistic and, as a result, women at higher risk (longer time since their last screening) are not identified and offered to screen. Therefore, we are currently piloting the implementation of self-sampling methods in an organized cervical cancer screening program aiming to increase screening capacity and to offer screening to those under screened. However, its scale-up has been slowed down.
In this study, we highlight using predictive models to estimate the expected participation in 2020 after validating our model with expected versus observed data in 2019 instead of assuming constant participation as in previous years. It is also noteworthy to mention that using the SISAP database facilitates the reporting of objective data (others have reported data facilitated by questionnaires to health managers) known to be highly representative of the whole Catalan population. Despite the strengths, our study has some limitations that need to be mentioned. Although changes in participation, abnormal cytology prevalence and screening interval coincide with the COVID-19 pandemic, we cannot rule out other reasons for such changes due to the use of ecological data to study the potential association between our findings and the COVID pandemic. One of these reasons could be that more women use private health services during the pandemic, so participation has been maintained in the overall population but decreased in the public health sector. However, our analysis database only contains data from the latter. On the other hand, the lack of access to structured histology data has prevented us from exploring whether the increase in abnormal cytology prevalence has been translated in an increase in CIN2+ prevalence.
The COVID-19 pandemic has significantly impacted cervical cancer screening in Catalonia, resulting in decreased screening participation, longer screening intervals and a potentially related increase in abnormal cytology prevalence. Therefore, close monitoring of the potential increases in cervical cancer diagnosis or the changes in cancer stage at diagnosis is warranted. Furthermore, to prevent a further increase in advanced cervical cancer diagnosis, it is crucial to expedite the implementation of the organized HPV-based screening program in Catalonia.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: It contains health records. Requests to access these datasets should be directed to Y3JvYmxlc0BpY29uY29sb2dpYS5uZXQ=.
Ethics statement
The studies involving humans were approved by Ethics Committee from the Hospital Universitari de Bellvitge. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
CR: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. LM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RI: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing. ER: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. RF: Data curation, Resources, Writing – review & editing. PP-T: Methodology, Writing – review & editing. MB: Methodology, Writing – review & editing. CM-B: Resources, Writing – review & editing. SS: Methodology, Writing – review & editing. JE: Data curation, Resources, Writing – review & editing. LB: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by a grant from the Instituto de Salud Carlos III (Spanish Government) through the project PI21/00982 (co-funded by European Regional Development Fund, a way to build Europe) and CIBERESP CB06/02/0073, and the Secretariat for Universities and Research of the Department of Business and Knowledge of the Government of Catalonia grants to support the activities of research groups (grant number 2017SGR1718 and 2021SGR01029). The project has also received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement number 847845 (RISCC project). We thank CERCA Programme/Generalitat de Catalunya for institutional support. The funders had no role in study design, data collection and analysis, manuscript preparation or decision to publish.
Acknowledgments
We would like to thank Mireia Fabregas, Mencia Benítez and Encarnacion López for clarifications on electronic health data collection.
Conflict of interest
The Cancer Epidemiology Research Programme has received unrestricted grants from Merck Sharp & Dohme, and HPV test kits at no cost from Roche for research purposes. PP-T has received speakers’ honorarium from Werfen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1338859/full#supplementary-material
References
1. Elemes S, Stachteas P, Haidich A-B, Mamopoulos A, Smyrnakis E. The impact of the COVID-19 pandemic on breast and cervical cancer screening: A systematic review. Vivo Athens Greece. (2023) 37:1455–76. doi: 10.21873/invivo.13230
2. Ferrara P, Dallagiacoma G, Alberti F, Gentile L, Bertuccio P, Odone A. Prevention, diagnosis and treatment of cervical cancer: A systematic review of the impact of COVID-19 on patient care. Prev Med. (2022) 164:107264. doi: 10.1016/j.ypmed.2022.107264
3. Mayo M, Potugari B, Bzeih R, Scheidel C, Carrera C, Shellenberger RA. Cancer screening during the COVID-19 pandemic: A systematic review and meta-analysis. Mayo Clin Proc Innov Qual Outcomes. (2021) 5:1109–17. doi: 10.1016/j.mayocpiqo.2021.10.003
4. Sasidharanpillai S, Ravishankar N. The short-term impact of COVID-19 pandemic on cervical cancer screening: A systematic review and meta-analysis. Asian Pac J Cancer Prev APJCP. (2022) 23:1497–504. doi: 10.31557/APJCP.2022.23.5.1497
5. Teglia F, Angelini M, Astolfi L, Casolari G, Boffetta P. Global association of COVID-19 pandemic measures with cancer screening: A systematic review and meta-analysis. JAMA Oncol. (2022) 8:1287–93. doi: 10.1001/jamaoncol.2022.2617
6. Ivanuš U, Jerman T, Gašper Oblak U, Meglič L, Florjančič M, Strojan Fležar M, et al. The impact of the COVID-19 pandemic on organised cervical cancer screening: The first results of the Slovenian cervical screening programme and registry. Lancet Reg Health Eur. (2021) 5:100101. doi: 10.1016/j.lanepe.2021.100101
7. de Pelsemaeker M-C, Guiot Y, Vanderveken J, Galant C, Van Bockstal MR. The impact of the COVID-19 pandemic and the associated belgian governmental measures on cancer screening, surgical pathology and cytopathology. Pathobiol J Immunopathol Mol Cell Biol. (2021) 88:46–55. doi: 10.1159/000509546
8. Miller MJ, Xu L, Qin J, Hahn EE, Ngo-Metzger Q, Mittman B, et al. Impact of COVID-19 on cervical cancer screening rates among women aged 21–65 years in a large integrated health care system - southern california, january 1-september 30, 2019, and january 1-september 30, 2020. MMWR Morb Mortal Wkly Rep. (2021) 70:109–13. doi: 10.15585/mmwr.mm7004a1
9. Rojas-Zumaran V, Walttuoni-Picón E, Campos-Siccha G, Cruz-Gonzales G, Huiza-Espinoza L, Moya-Salazar J. Decline of cytology-based cervical cancer screening for COVID-19: a single-center Peruvian experience. Medwave. (2022) 22:e2589. doi: 10.5867/medwave.2022.S3.2589
10. Puricelli Perin DM, Elfström KM, Bulliard J-L, Burón A, Campbell C, Flugelman AA, et al. Early assessment of the first wave of the COVID-19 pandemic on cancer screening services: The International Cancer Screening Network COVID-19 survey. Prev Med. (2021) 151:106642. doi: 10.1016/j.ypmed.2021.106642
11. Alfonso Viguria U, Casamitjana N. Early interventions and impact of COVID-19 in Spain. Int J Environ Res Public Health. (2021) 18:4026. doi: 10.3390/ijerph18084026
12. Cruz-Valdez A, Palacio-Mejía LS, Quezada-Sánchez AD, Hernández-Ávila JE, Galicia-Carmona T, Cetina-Pérez LDC, et al. Cervical cancer prevention program in Mexico disrupted due to COVID-19 pandemic: Challenges and opportunities. Front Oncol. (2023) 13:1008560. doi: 10.3389/fonc.2023.1008560
13. Coma E, Guiriguet C, Mora N, Marzo-Castillejo M, Benítez M, Méndez-Boo L, et al. Impact of the COVID-19 pandemic and related control measures on cancer diagnosis in Catalonia: a time-series analysis of primary care electronic health records covering about five million people. BMJ Open. (2021) 11:e047567. doi: 10.1136/bmjopen-2020–047567
14. Mora N, Guiriguet C, Cantenys R, Méndez-Boo L, Marzo-Castillejo M, Benítez M, et al. Cancer diagnosis in primary care after second pandemic year in Catalonia: a time-series analysis of primary care electronic health records covering about 5 million people. Fam Pract. (2023) 40:183–7. doi: 10.1093/fampra/cmac083
15. Ribes J, Pareja L, Sanz X, Mosteiro S, Escribà JM, Esteban L, et al. Cancer diagnosis in Catalonia (Spain) after two years of COVID-19 pandemic: an incomplete recovery. ESMO Open. (2022) 7:100486. doi: 10.1016/j.esmoop.2022.100486
16. Sanvisens A, Puigdemont M, Rubió-Casadevall J, Vidal-Vila A, López-Bonet E, Martín-Romero F, et al. Differences in the impact of COVID-19 on pathology laboratories and cancer diagnosis in Girona. Int J Environ Res Public Health. (2021) 18:13269. doi: 10.3390/ijerph182413269
17. Robles C, Monfil L, Ibáñez R, Roura E, Peremiquel-Trillas P, Font R, et al. [Evaluation of the HPV-based cervical cancer screening implementation in Catalonia]. San Sebastian. (2022).
18. Peremiquel-Trillas P, Roura E, Ibáñez R, Robles C, Monfil L, Carvajal M, et al. [Implementation of cervical cancer screening with self-sampling in Catalonia]. San Sebastian. (2022).
19. Gremke N, Griewing S, Felgentreff M, Kostev K, Kalder M. Impact of the coronavirus disease 2019 (COVID-19) pandemic on cervical cancer screening in gynecological practices in Germany. Cancers. (2022) 14:4820. doi: 10.3390/cancers14194820
20. Oakes AH, Boyce K, Patton C, Jain S. Rates of routine cancer screening and diagnosis before vs after the COVID-19 pandemic. JAMA Oncol. (2022) 9:145–6. doi: 10.1001/jamaoncol.2022.5481
21. Jidkova S, Hoeck S, Kellen E, le Cessie S, Goossens MC. Flemish population-based cancer screening programs: impact of COVID-19 related shutdown on short-term key performance indicators. BMC Cancer. (2022) 22:183. doi: 10.1186/s12885-022-09292-y
22. Martins TR, Witkin SS, Mendes-Corrêa MC, de GAS, Cury L, Balancin ML, et al. Impact of the COVID-19 pandemic on cervical cancer screening in São Paulo State, Brazil. Acta Cytol. (2023) 67:388–94. doi: 10.1159/000529249
23. Meggetto O, Jembere N, Gao J, Walker MJ, Rey M, Rabeneck L, et al. The impact of the COVID-19 pandemic on the Ontario Cervical Screening Program, colposcopy and treatment services in Ontario, Canada: a population-based study. BJOG Int J Obstet Gynaecol. (2021) 128:1503–10. doi: 10.1111/1471–0528.16741
24. Bolíbar B, Fina Avilés F, Morros R, Garcia-Gil M del M, Hermosilla E, Ramos R, et al. [SIDIAP database: electronic clinical records in primary care as a source of information for epidemiologic research]. Med Clin (Barc). (2012) 138:617–21. doi: 10.1016/j.medcli.2012.01.020
25. Hyndman RJ, Athanasopoulos G. Forecasting: principles and practice (2021). OTexts. Available online at: https://otexts.com/fpp3/ (Accessed December 28, 2022). 442 p.
26. Holt CC. Forecasting seasonals and trends by exponentially weighted moving averages. Int J Forecast. (2004) 20:5–10. doi: 10.1016/j.ijforecast.2003.09.015
27. Winters PR. Forecasting sales by exponentially weighted moving averages. Manag Sci. (1960) 6:324–42. doi: 10.1287/mnsc.6.3.324
28. DeGroff A, Miller J, Sharma K, Sun J, Helsel W, Kammerer W, et al. COVID-19 impact on screening test volume through the National Breast and Cervical Cancer early detection program, January-June 2020, in the United States. Prev Med. (2021) 151:106559. doi: 10.1016/j.ypmed.2021.106559
29. Nogami Y, Makabe T, Komatsu H, Kawana K, Okamoto A, Mikami M, et al. Impact of COVID-19 on cervical cancer screening in Japan: A survey of population-based screening in urban Japan by the Japan Society of Gynecologic Oncology. J Obstet Gynaecol Res. (2022) 48:757–65. doi: 10.1111/jog.15130
30. Gunn CM, Berrian K, Weiss JE, Tosteson AAN, Hasson R, Di Florio-Alexander R, et al. A population-based survey of self-reported delays in breast, cervical, colorectal and lung cancer screening. Prev Med. (2023) 175:107649. doi: 10.1016/j.ypmed.2023.107649
31. Sanger K. Impact of COVID-19 on cervical screening(2020). Available online at: https://www.jostrust.org.uk/about-us/news-and-blog/blog/impact-covid-19-cervical-screening (Accessed December 28, 2022).
32. Petrova D, Pollán M, Rodriguez-Barranco M, Garrido D, Borrás JM, Sánchez M-J. Anticipated help-seeking for cancer symptoms before and after the coronavirus pandemic: results from the Onco-barometer population survey in Spain. Br J Cancer. (2021) 124:2017–25. doi: 10.1038/s41416–021-01382–1
33. Armitage R. Cervical screening coverage in England before and during COVID-19. Public Health. (2021) 198:e11. doi: 10.1016/j.puhe.2021.04.025
34. Bosch G, Posso M, Louro J, Roman M, Porta M, Castells X, et al. Impact of the COVID-19 pandemic on breast cancer screening indicators in a Spanish population-based program: a cohort study. eLife. (2022) 11:e77434. doi: 10.7554/eLife.77434
35. Vives N, Binefa G, Vidal C, Milà N, Muñoz R, Guardiola V, et al. Short-term impact of the COVID-19 pandemic on a population-based screening program for colorectal cancer in Catalonia (Spain). Prev Med. (2022) 155:106929. doi: 10.1016/j.ypmed.2021.106929
36. Mora N, Fina F, Méndez-Boo L, Cantenys R, Benítez M, Moreno N, et al. Decline and uneven recovery from 7 common long-term conditions managed in the Catalan primary care after two pandemic years: an observational retrospective population-based study using primary care electronic health records. BMC Prim Care. (2022) 24:9. doi: 10.21203/rs.3.rs-2056867/v1
37. Burger EA, de Kok IMCM, O’Mahony JF, Rebolj M, Jansen EEL, de Bondt DD, et al. A model-based analysis of the health impacts of COVID-19 disruptions to primary cervical screening by time since last screen for current and future disruptions. eLife. (2022) 11:e81711. doi: 10.7554/eLife.81711
38. Smith MA, Burger EA, Castanon A, de Kok IMCM, Hanley SJB, Rebolj M, et al. Impact of disruptions and recovery for established cervical screening programs across a range of high-income country program designs, using COVID-19 as an example: A modelled analysis. Prev Med. (2021) 151:106623. doi: 10.1016/j.ypmed.2021.106623
39. Kregting LM, Kaljouw S, de Jonge L, Jansen EEL, Peterse EFP, Heijnsdijk EAM, et al. Effects of cancer screening restart strategies after COVID-19 disruption. Br J Cancer. (2021) 124:1516–23. doi: 10.1038/s41416–021-01261–9
Keywords: cervical cancer, cancer screening program, Catalonia (NE Spain), COVID-19, impact, participation, abnormal cytology prevalence, screening interval
Citation: Robles C, Monfil L, Ibáñez R, Roura E, Font R, Peremiquel-Trillas P, Brotons M, Martínez-Bueno C, de Sanjosé S, Espinàs JA and Bruni L (2024) Impact of the COVID-19 pandemic on cervical cancer screening participation, abnormal cytology prevalence and screening interval in Catalonia. Front. Oncol. 14:1338859. doi: 10.3389/fonc.2024.1338859
Received: 15 November 2023; Accepted: 15 May 2024;
Published: 29 May 2024.
Edited by:
Paul Licciardi, Royal Children’s Hospital, AustraliaReviewed by:
Boya Guo, Fred Hutchinson Cancer Center, United StatesGrant McGeechan, Teesside University, United Kingdom
Jeel Moya-Salazar, Hospital Nacional Docente San Bartolome, Peru
Copyright © 2024 Robles, Monfil, Ibáñez, Roura, Font, Peremiquel-Trillas, Brotons, Martínez-Bueno, de Sanjosé, Espinàs and Bruni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claudia Robles, Y3JvYmxlc0BpY29uY29sb2dpYS5uZXQ=