 Sabrine Hasnaoui1
Sabrine Hasnaoui1 Aurélie Van Hoye1,2
Aurélie Van Hoye1,2 Marc Soudant3Christine Rotonda4,5Andréia Carvalho de Freitas3Didier Peiffert1,6Cécile Delattre7Julien Raft8,9Margaux Temperelli10
Marc Soudant3Christine Rotonda4,5Andréia Carvalho de Freitas3Didier Peiffert1,6Cécile Delattre7Julien Raft8,9Margaux Temperelli10 Edem Allado10,11Oriane Hily10
Edem Allado10,11Oriane Hily10 Bruno Chenuel10,11Dominique Hornus-Dragne12Abdou Y. Omorou1,3,13
Bruno Chenuel10,11Dominique Hornus-Dragne12Abdou Y. Omorou1,3,13 Mathias Poussel10,11*
Mathias Poussel10,11*- 1Université de Lorraine, INSERM, UMR 1319, INSPIIRE, Nancy, France
- 2University of Limerick, Physical Activity for Health Research Center, Limerick, Ireland
- 3Université de Lorraine, CHRU-Nancy, Inserm CIC-1433 Clinical Epidemiology, Nancy, France
- 4Université de Lorraine, INSERM, UMR 1319, INSPIIRE, Metz, France
- 5Université de Lorraine, Centre Pierre Janet, Metz, France
- 6Lorraine Institute of Oncology, Department of Radiation Oncology, Vandoeuvre-Lès-Nancy, France
- 7Lorraine Institute of Oncology, Supportive Care Unit, Vandoeuvre-Lès-Nancy, France
- 8Lorraine Institute of Oncology, Department of Anesthesiology, Vandoeuvre-Lès-Nancy, France
- 9Université de Lorraine, INSERM UMR-S 1116 Equipe 2, Nancy, France
- 10Université de Lorraine, CHRU-Nancy, University Centre of Sports Medicine and Adapted Physical Activity, Nancy, France
- 11Université de Lorraine, DevAH, Department of Physiology, Nancy, France
- 12Solution RIPOSTE, Balma, France
- 13The French National Platform Quality of Life and Cancer, Nancy, France
Background: Adapted physical activity programs have shown promising results in reducing the physical, social and psychological side effects associated with breast cancer, but the extent to which they can be effectively adopted, implemented and maintained is unclear. The aim of this study is to use the framework to guide the planning and evaluation of programs according to the 5 following keys: Reach, Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) framework to evaluate a fencing program under the French acronym RIPOSTE (Reconstruction, Image de soi, Posture, Oncologie, Santé, Thérapie, Escrime) literally in English (Reconstruction, Self-Image, Posture, Oncology, Health, Therapy, Fencing). This program is an innovative intervention focused on improving the quality of life (QoL) of breast cancer surgery patients through fencing.
Methods: A convergent mixed methods pilot study was conducted to preliminary evaluate the different RE-AIM dimension of the pilot program. Twenty-four participants who have just undergone surgery for invasive breast cancer were randomly allocated in two groups: one group started immediately after their inclusion (Early RIPOSTE group) and the other started 3 months following their inclusion (Delayed RIPOSTE group). Participants answered a questionnaire at inclusion and at the end of the program on QoL, shoulder functional capacity, fatigue, anxiety-depression and physical activity.
Results: RIPOSTE program was able to reach mainly young and dynamic participants, attracted by the originality of fencing and keen to improve their physical condition. Regarding effectiveness, our results suggest a trend to the improvement of QoL, shoulder functional capacity, fatigue and anxiety-depression state, even without any significant differences between the Early RIPOSTE group and the Delayed RIPOSTE group.
Discussions: The cooperation, exchanges and cohesion within the group greatly facilitated the adoption of the program, whereas interruptions during school vacations were the main barriers. The intervention was moderately well implemented and adherence to the protocol was suitable.
Conclusion: RIPOSTE is an acceptable and effective program for involving breast cancer survivors in physical activity, that needs to be tested at a larger scale to investigate its effectiveness, but has the potential to be transferred and scaled up worldwide.
1 Introduction
Breast cancer (BC) remains the most diagnosed cancer and the leading cause of cancer death among women in France (1). Treatment improvements have enhanced cancer survivorship, leading to a 5-year survival rate of 89% for people diagnosed with BC (1). These high cancer survival rates have led to increased exposure to physiological (e.g., fatigue, mobility problems) and psychological (e.g., anxiety, depression, low quality of life) adverse side effects associated with the disease and related common treatments (2).
One of the key non-pharmacological treatments showing promising results in managing these adverse effects are physical activity (PA) programs, implemented at each stage of the cancer progression. Indeed, PA interventions have been shown to enhance quality of life (QoL), reduce symptoms and simultaneously minimize the risk of recurrence and comorbidities among patients living with and beyond cancer (3–9). Based on these evidence-based benefits, a fencing program under the French acronym RIPOSTE (Reconstruction, Image de soi, Posture, Oncologie, Santé, Thérapie, Escrime) literally in English (Reconstruction, Self-Image, Posture, Oncology, Health, Therapy, Fencing) was created for BC surgery patients in 2014 (10). This adapted physical activity (APA) program has been considered by public health and medical stakeholders as an innovative intervention through fencing (10, 11). APA is defined as “a cross-disciplinary body of practical and theoretical knowledge directed toward impairments, activity limitations, and participation restrictions in physical activity” (12). The relevance of fencing as an APA program in the context of BC was suggested quite naturally, as it is well adapted to combating fatigue, pain and reduced arm mobility, as well as improving patients’ physical and psychological well-being (10, 13, 14). More specifically, the use of the saber (and not the foil or epee) allows maximum mobilization and opening of the shoulder, due to the particularity of this weapon. The RIPOSTE program will celebrate its 10th anniversary in 2024. Currently, over 100 fencing clubs offer this adapted fencing program in France and a few more abroad. The aim of the scientific committee is to further develop this program for as many clubs as possible, always with the same high-quality standards, and to spread more widely internationally. Contacts have already been established with the International Fencing Federation (IFF) and with some North American clubs, so that adapted fencing could be considered a valid non-pharmacological treatment worldwide. But more data on its benefits and implementation process is needed to anticipate this process (11, 15).
To date, despite large evidence on the benefits of PA for people with BC, the extent to which PA programs could be effectively adopted, implemented and sustained remains unclear (16–20). Previous literature has shown mixed results over the long-term impact of interventions on PA practice (16, 17). Indeed, several programs have achieved limited success in improving PA among adults, particularly due to a lack of maintenance and sustainability of practice once the intervention ends (18, 19). Also, the existing evidence has focused almost exclusively on the high internal validity – or the magnitude of effect as a key indicator for programs impact. However, issues related to external validity - how the results of a study can be generalized to other contexts (21) - received less attention (20). Assessing external validity when synthesizing the results of this type of program is important to support sustainably their translation into practice (22–24). An accurate and comprehensive evaluation of the system supporting the implementation process is needed in order to understand what works, for whom and how (25, 26).
While RIPOSTE program has provided some success on the field across France, its evaluation in terms of effectiveness and implementation process has remained at its infancy, with no proper evaluation so far. Determining the extent to which this program is effective, acceptable and implementable is a necessary preliminary step. These findings would help to enrich the literature on how to best intervene to enhance treatment and recovery among BC patients, considering both patient and professional preferences and adoption, to facilitate transfer from a research program to a field daily practice. The aim of this preliminary study was to evaluate the RIPOSTE program effectiveness and implementation process.
2 Method
2.1 Study design
A convergent mixed methods (QUAN+QUAL) pilot study was conducted using the framework to guide the planning and evaluation of programs according to the 5 following keys: Reach, Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) framework as a guide to evaluate RIPOSTE (27). Quantitative and qualitative data were collected at the same time and combined during data analysis in a convergent design, giving the same weight to each type of data. A commonly used framework to assess research implementation is the RE-AIM framework which conceptualizes the public health impact of interventions as a function of the 5 dimensions of RE-AIM (Table 1) (28). This framework extends beyond standard measures of efficacy, considering individual and organizational factors that can either facilitate or impede the successful implementation and dissemination of a program (29, 30). A full description of the design and methodological protocol of the program have been reported previously (10). This research complies with the Helsinki declaration and received ethical authorization by the French committee for individual protection (CPP Sud Méditerranée IV, N°ID-RCB: 2020-A01916-33). This research is registered on clinicaltrials.gov (NCT04627714).
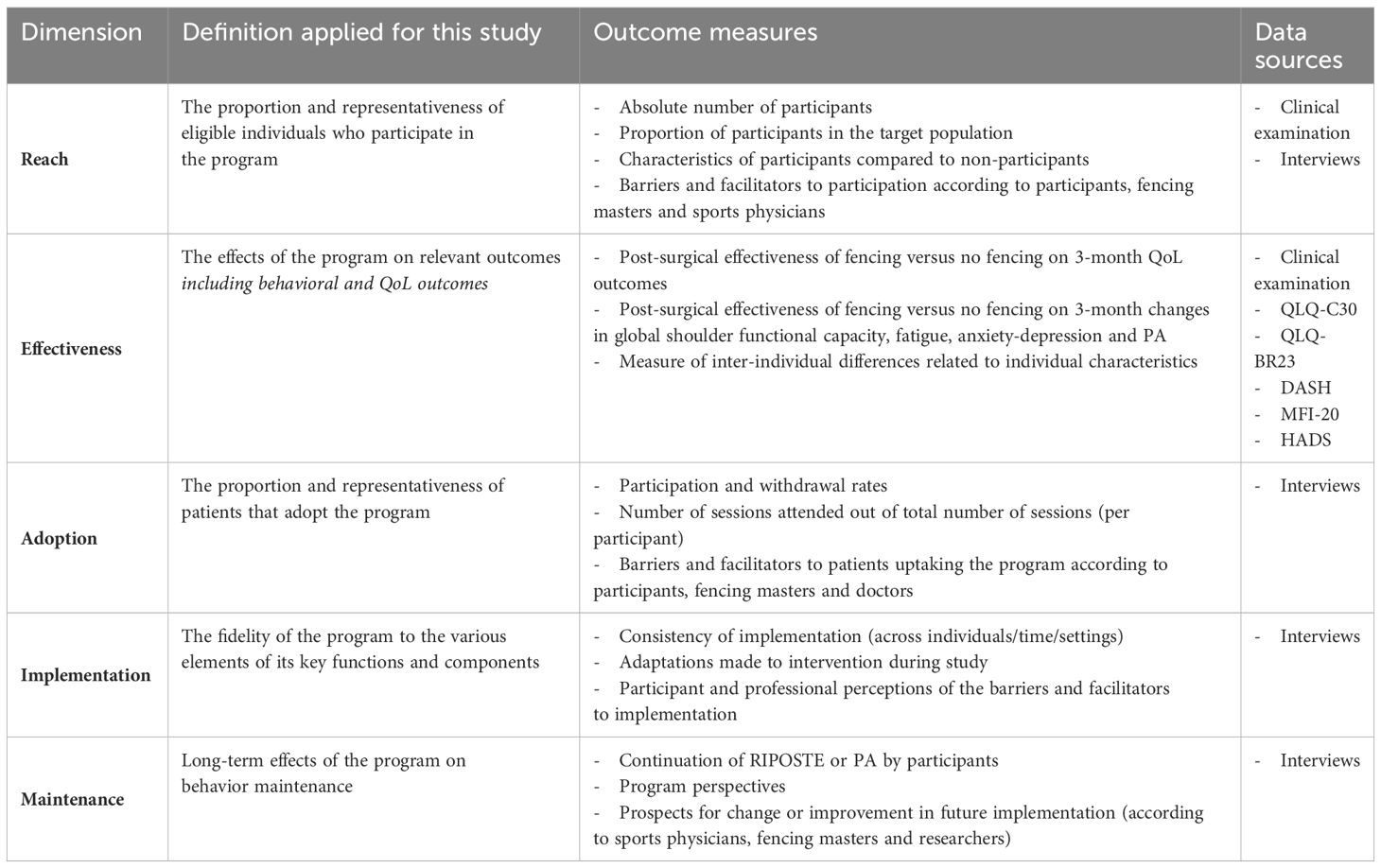
Table 1 RE-AIM components in the context of the RIPOSTE trial.
2.2 Participants and recruitment
From November 10th to January 19th 2021, patients diagnosed with invasive BC were screened from 3 centers in Northeastern France (University Hospital of Nancy CHRU, France), Institut de Cancérologie de Lorraine, Nancy, France and Hôpital d’Instruction des Armées Legouest, Metz, France). Among the 309 patients screened, 24 met the inclusion criteria (10) and were selected from those who had recently undergone breast surgery for invasive BC. The surgeon, anesthesiologist or oncologist referred them to a sports physician within 2 to 4 weeks after surgery for an inclusion visit. All participants were provided with an information letter outlining the research and completed written informed consent. Patients were then randomized, with centralized 1:1 computerized requested via the web interface (e-crf) by the investigator with a sequential minimization of factor 85%, to one of two groups. The Early RIPOSTE group received one fencing session (duration of 1–1.5 h/session) per week from inclusion and for 3 months in the program. The Delayed RIPOSTE group received a follow-up without fencing for the first 3 months after inclusion and then the program (i.e. one fencing session per week) for the last 3 months (see Figure 1 for sample allocation and intervention description). Recruitment occurred between November 2021 and January 2022. They followed fencing sessions that had a common structure in the fencing French halls in the cities of Vandoeuvre-lès-Nancy and Thionville. Participation in all sessions was not required to be considered a study participant, but the level of participation was analyzed as a reach indicator.
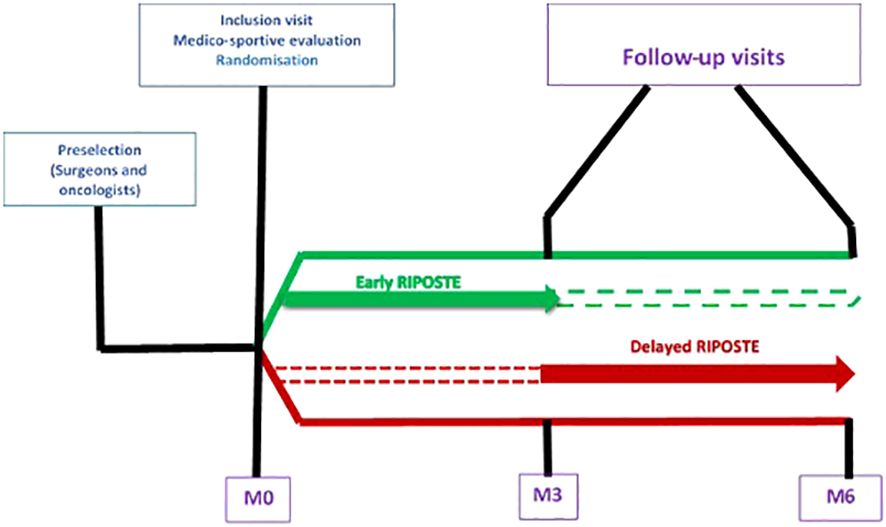
Figure 1 Study design and patient allocation.
2.3 Data collection
Included patients underwent a sports medical examination at inclusion, 3 months after randomization, and 6 months after randomization. Quantitative data regarding each RE-AIM dimension were collected, without blinding of the randomization arm, at each time. Qualitative interviews were also conducted with 10 patients (5 patients per group), 3 sports medicine physicians, and 1 fencing master at the end of follow-up. Methods of data collection included clinical examination, questionnaires and interviews.
2.3.1 Quantitative outcomes
2.3.1.1 Clinical examination
The sociodemographic and clinical factors of study patients at enrollment included age, marital and familial status, number and age of children, education level, current employment status, socio-professional category, social support, sleep habits and PA. At inclusion, data on disease stage, age of diagnosis, age and type of breast surgery were also collected. Medical data such as additional treatments, weight gain, presence of lymphedema and comorbidities were collected at the baseline, 3-month and 6-month follow-up by the sports physician or the clinical study technician. At each visit, the sports physician also collected the shoulder functional score from the Constant index as well as injuries or any other pathological symptoms related to fencing.
2.3.1.2 Questionnaires
At the end of each visit, a notebook was given to the patient to answer the different questionnaires. The evolution of QoL at 3 months was measured by the third version of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30 (QLQ-C30) (31) and BC specific Quality of Life Questionnaire module (QLQ-BR23) (32). The QLQ-BR23 is a supplementary 23-item questionnaire module that measures BC symptoms as well as treatment side effects.
Global functional capacity of both upper extremities was assessed using the Disabilities of the Arm, Shoulder and Hand (DASH) measurement, validated in French (33).
Fatigue over the previous days was measured by the Multidimensional Fatigue Inventory (MFI-20), validated in French (34).
The 14-item Hospital Anxiety and Depression Scale (HADS) was used to measure a standardized anxiety and depression score (35).
PA was assessed by the International Physical Activity Questionnaire (IPAQ), a validated international questionnaire that has been translated into several languages including French (36).
2.3.2 Qualitative interviews
Semi-structured retrospective narrative interviews were conducted with 10 participants (5 per group) within weeks of the 3-month follow-up data collection period. These interviews ranged from 40 to 60 minutes in duration and consisted of asking participants open-ended questions pertaining to their experiences with the program, identified difficulties and facilitators, and their perceptions of how the program could be improved. Semi-structured interviews were also conducted with 3 sports physicians (SP1, SP2, SP3) and 1 fencing master (FM) at the end of the follow-up to identify indicators of efficacy, including patient acceptability, from the professionals’ perspective. Interviews were recorded and transcribed verbatim.
2.4 Data analysis
2.4.1 Quantitative data
The change in QLQ C30 global health status score at 3 months was analyzed using Student’s t test, after checking normality and homoscedasticity assumptions, between the randomization arms according to intention to treat principle. This analysis was done on complete cases. Multivariate mixed modeling was also performed with patient random effect in order to take into account repeated measures correlations. For sensitivity analysis purposes, the same analysis was realized using multiple imputations. Patterns of missing data were studied and multiple imputations were used when observations with at least one missing data exceeded 5%, the von Hippel method was used to determine the number of imputation datasets. Other comparisons used the same non-adjusted statistical methods for the other measured variables replacing Student’s ‘t tests’ by Welch’s tests and Wilcoxon-Mann Whitney tests when homoscedasticity and normality, respectively, were not satisfied. Considering the second period (M6), without covariates adjustment, a two-stage crossover model using Grizzle model based on Student’s ‘t tests’ evaluating the carryover (residual of the intervention), direct of the intervention and period effects. Confounding effects were taken into account in the second time with a mixed model explaining each score progression since baseline with the same selection strategy as the mixed model restricted to the first 3 months. The data analysis was generated using SAS/STAT software, Version 9.4 of the SAS System for Microsoft Windows.
2.4.2 Qualitative data
Patient and professional discourse were fully transcribed and cross-referenced. A deductive thematic content analysis (37), based on each RE-AIM category, was conducted using Dedoose (Version 9.0.17, cloud application for managing, analyzing, and presenting qualitative and mixed method research data (2021). Los Angeles, CA, USA). The coded data were reviewed and compared within each dimension to identify common as well as contrasting ideas and experiences by the first author and cross-checked by a second author. Descriptive summaries for each category along with illustrative quotes were developed from these data and discussed within the team.
3 Results
In order to best reflect the aims of the study, the results are presented under the RE-AIM framework.
3.1 Reach
3.1.1 Number and proportion of participants
Among the 309 patients screened, 73 were eligible for enrollment. Among them, 49 were not included (refusal) so 24 patients were allocated either in the Early RIPOSTE group (n = 11) or the Delayed RIPOSTE group (n = 13).
3.1.2 Characteristics of participants
Sociodemographic and clinical characteristics of the study sample are presented in Table 2.
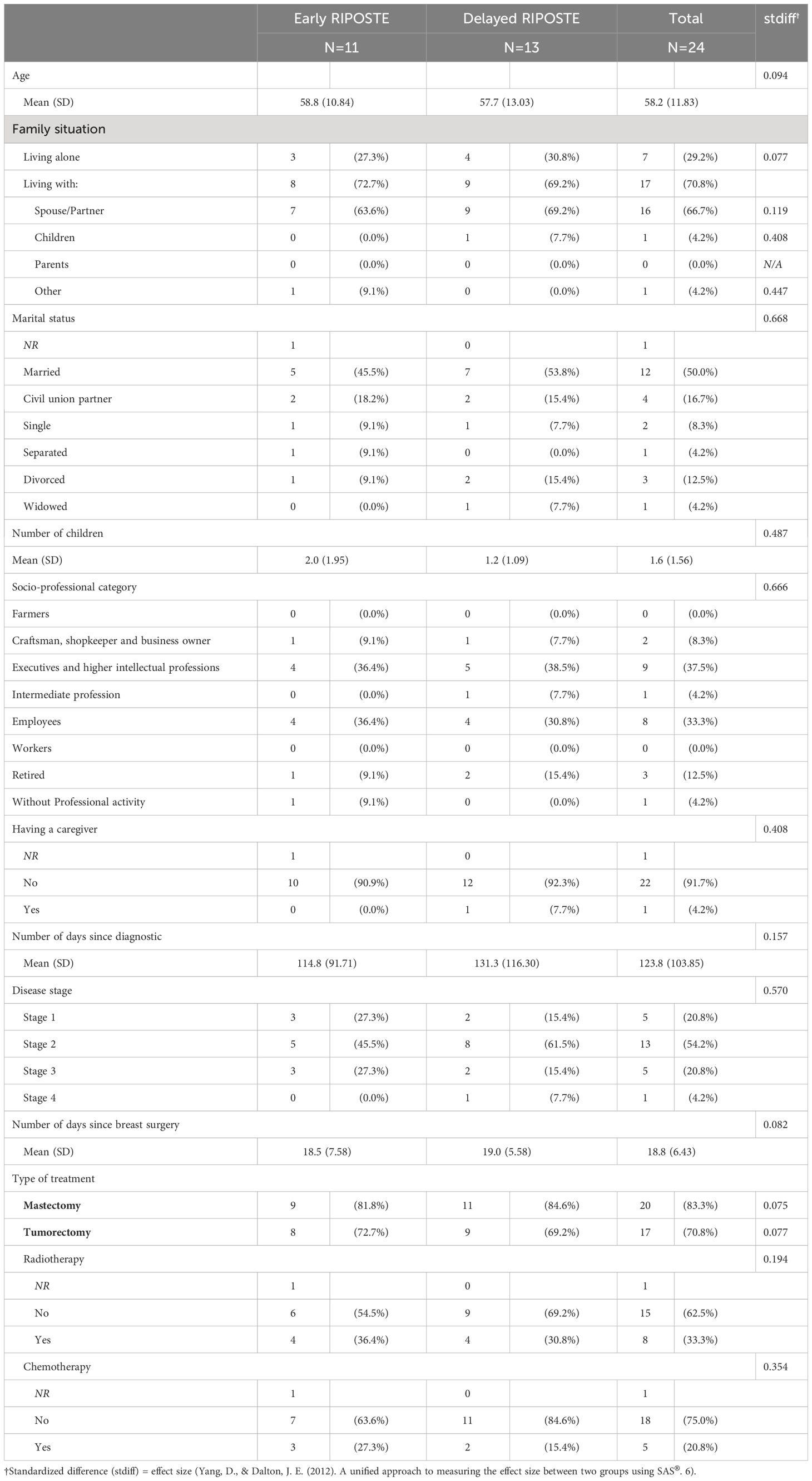
Table 2 Sociodemographic and clinical characteristics of the study sample.
3.1.3 Profile and reasons for participation
Participant’s quotations in regard to their participation and experience are described in Table 3. Elderly or sedentary patients were less likely to participate, or the sports medicine physician did not suggest the program to them. Most of the participants were dynamic and physically active prior to their cancer. The main reasons for participation were the originality of fencing, the symbolism of “combat”, and the fact that the program was free, as well as known to sports medicine physicians. Their participation was also motivated by a desire to take control over their lives and distance themselves from the cancer environment. At the same time, most patients saw the program as an opportunity to improve disease-related symptoms and manage the side effects of treatment. A few were more interested in taking part in a study and contributing to cancer research. While some participants expressed a desire to share an activity with other cancer survivors, the more introverted ones were held back by the collective dimension of fencing. From an organizational point of view, the distance between home and the fencing gym, the day and time suited most of the participants, principally because they were no longer working and therefore had few constraints. However, those with children regretted that the training sessions were not offered during school hours.
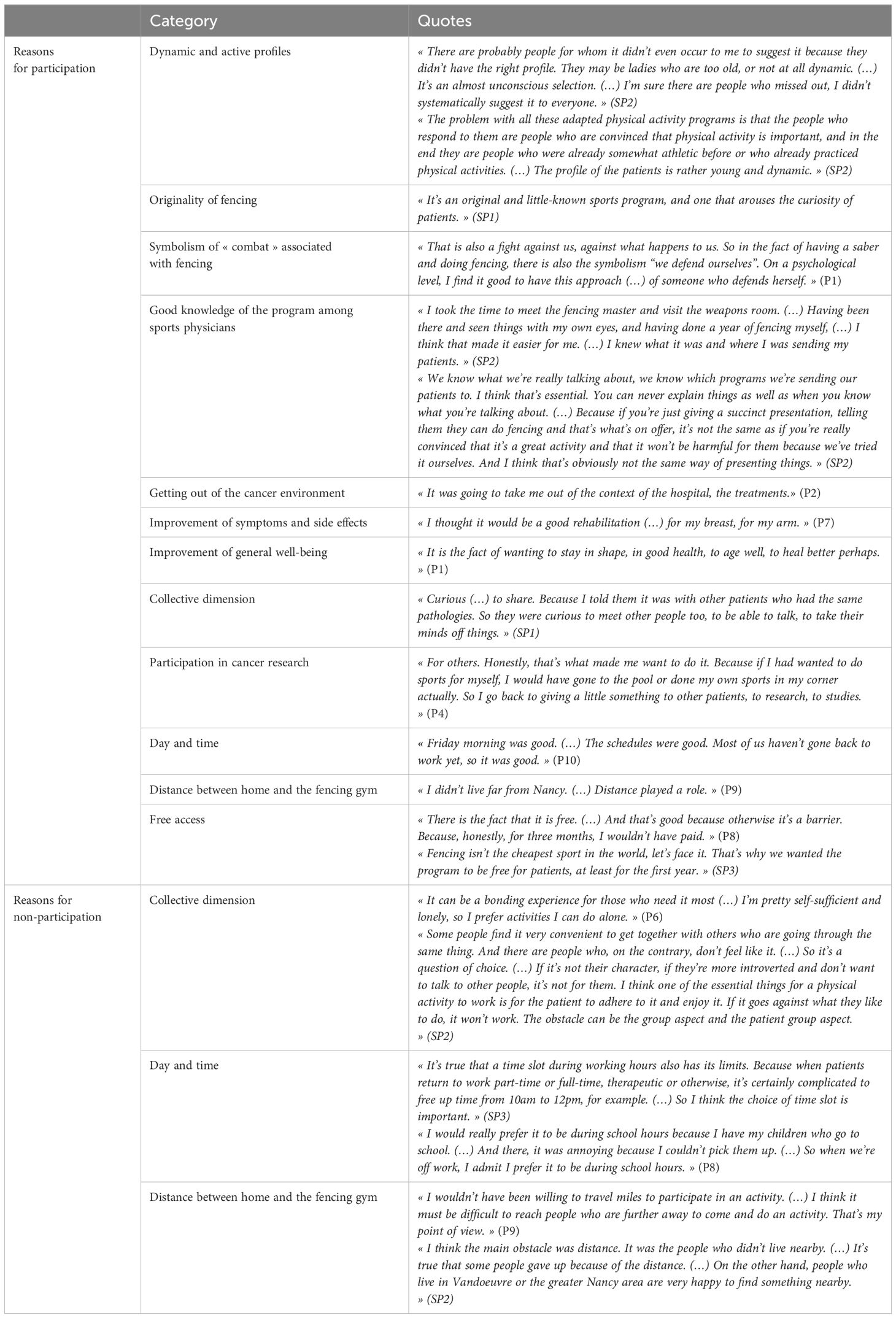
Table 3 Participant’s quotation in regard to their participation and experience to RIPOSTE.
3.2 Effectiveness
The effectiveness of the RIPOSTE pilot trial is presented in Tables 4 and 5.
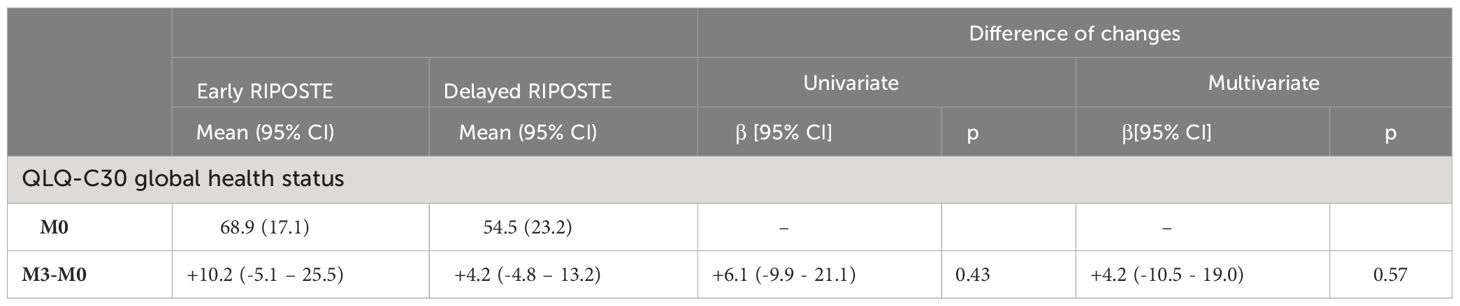
Table 4 Effectiveness of early RIPOSTE versus delayed RIPOSTE on global health status.
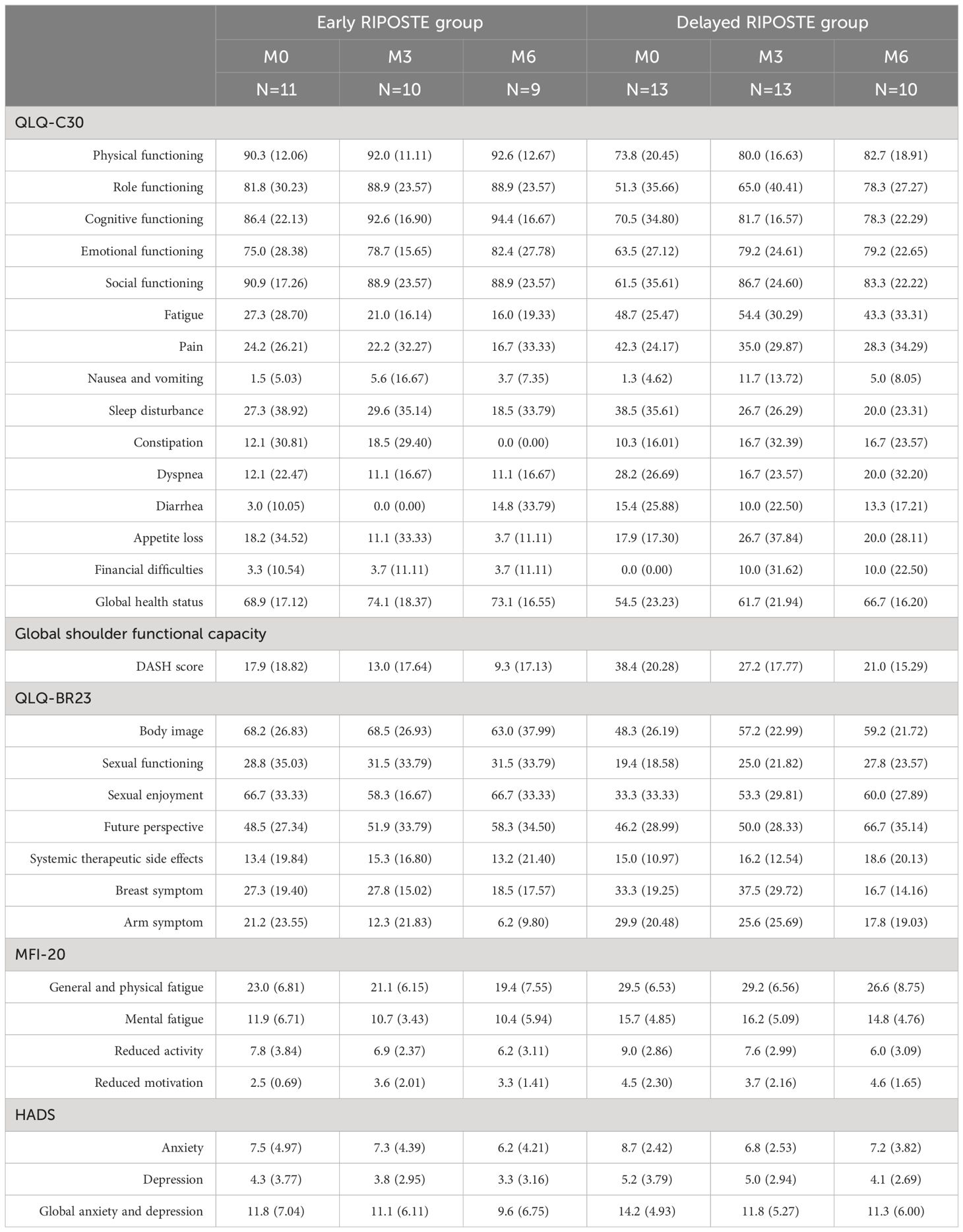
Table 5 Evolution of scores (QLQ-C30, Global Shoulder Functional Capacity, QLQ-BR23, MFI-20, HADS) at M0, M3 and M6 in each group.
3.2.1 Quality of Life
Global health status (GHS) score at inclusion (M0) was 68.9 (17.1) and 54.5 (23.2) respectively for the Early RIPOSTE and Delayed RIPOSTE groups (Table 4). At M3, GHS scores increased by +10.2 [-5.1; 25.5] and +4.2 [-4.8; +13.2] respectively in the Early RIPOSTE and Delayed RIPOSTE groups corresponding to a greater, but not statistically significant, increase of +6.0 [-9.9; +21.9] in favor of the Early RIPOSTE group. Multivariate analysis also highlights a trend for a larger increase of (+ 4.2 [-10.5 – 19.0], p = 0.57) of the quality of life score of the Early RIPOSTE group.
3.2.2 Global shoulder functional capacity
At inclusion, the standardized DASH score was better in the Early RIPOSTE group than in the Delayed RIPOSTE group (17.9 versus 38.4). This score improved in both groups at M3 (13.0 versus 27.2) and at M6 (9.3 versus 21.0), suggesting an improvement of functional capacity (Table 5). Change between M0 and M3 was not statistically significant (-0.7 [-15.0 – 13.6], p=0.91) (Supplementary Appendix 1).
3.2.3 Fatigue (MFI-20), anxiety and depression
At baseline, the general/physical fatigue score was 23.0 in the Early RIPOSTE group and 29.5 in the Delayed RIPOSTE group (Table 5). For the Early RIPOSTE group, this score decreased at M3 (21.1) and M6 (19.4), reflecting an improvement in fatigue status. Similarly, in the Delayed RIPOSTE group, there was a decrease at M3 (29.2) and M6 (26.6). In terms of mental fatigue, at inclusion, the score was better in the Early RIPOSTE group than in the Delayed RIPOSTE group (11.9 versus 15.7). At 3 months, this score improved in the Early RIPOSTE group but worsened in the Delayed RIPOSTE group (10.7 versus 16.2). At 6 months, this score improved in both groups (10.4 versus 14.8). Results were similar for anxiety and depression scales (Table 5).
3.2.4 Physical activity
No difference between groups was observed regarding the level of physical activity.
3.3 Adoption
3.3.1 Participation and withdrawal rates
The participation rate in the sessions was between 57% and 93%. One patient was lost to follow-up at 3 months and 4 at 6 months (refusal to continue). This corresponds to a withdrawal rate of 4.2% at 3 months and 16.6% at 6 months (Appendix 2 Supplementary Data).
3.3.2 Barriers and facilitators to adoption
Barriers and facilitators to adoption are described in Table 6. The facilitators were the discovery of a new activity, good supervision of sessions and the physical and moral benefits associated with the practice. In contrast, participants cited contrasted laterality, fatigue and pain as the main barriers. In terms of organization, the majority of participants were satisfied with the duration (2 hours) and frequency of the sessions, although some would not have minded a second session a week, or regretted that the sessions were interrupted during school vacations. The size of the group seemed to suit everyone when it was reduced to around ten participants, with an even number to be able to work in pairs. While most participants appreciated the diversity and richness of the sessions, which were judged to be adapted to everyone’s abilities, some complained of boredom due to the lack of intensity. The facilitators were also the heterogeneity of profiles, and the cooperation and mutual support between participants, whatever their individual talent. However, integrating new participants during the program and reteaching them the basics seemed to disrupt and slow down the group’s progress somewhat. The good atmosphere and cohesion of the group, as well as the exchange and sharing of cancer-related experiences, also contributed to the adhesion of some participants, fostering a strong sense of community and belonging. Conversely, some saw the program as an opportunity to get away from the context of their illness and treatment.
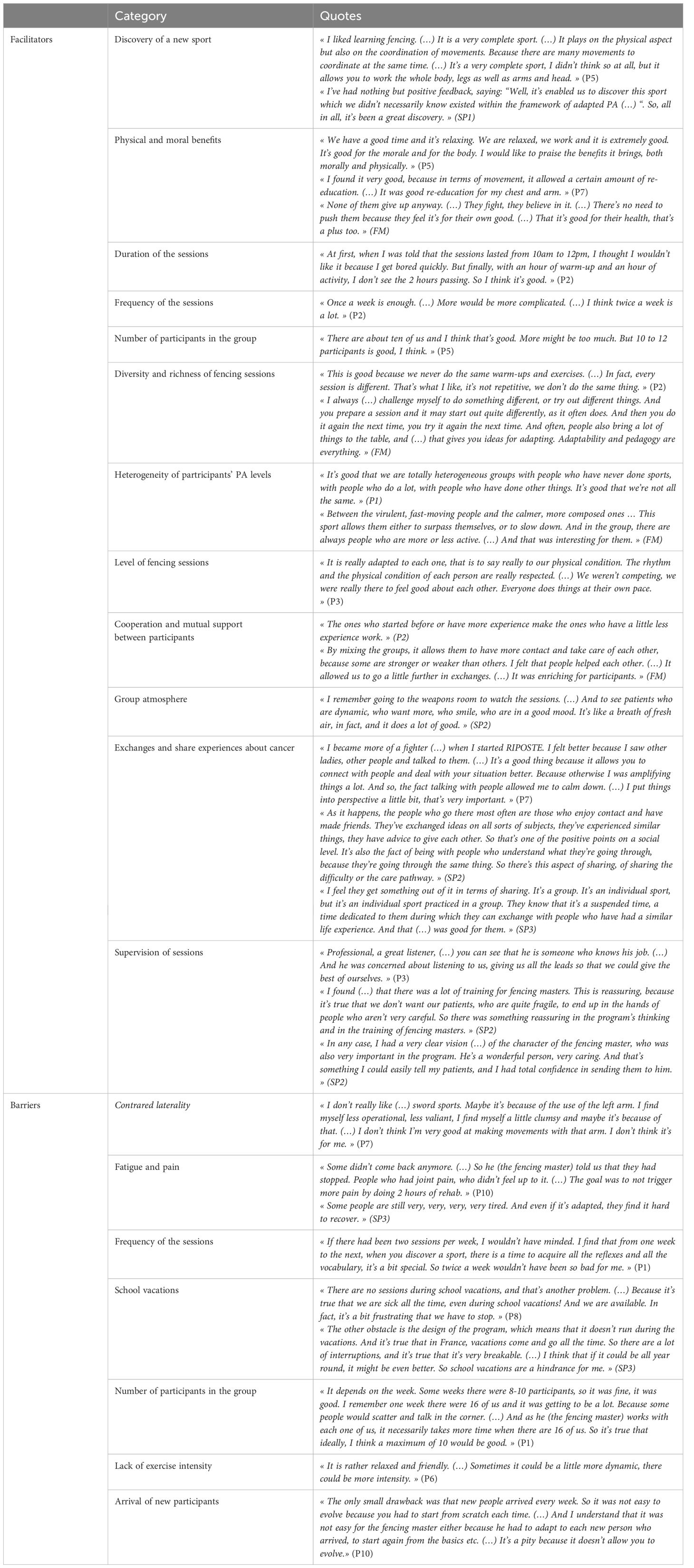
Table 6 Barriers and facilitators to the adoption of the RIPOSTE.
3.4 Implementation
3.4.1 Consistency of implementation and adaptations
3.4.1.1 Time and settings
The intervention was implemented according to the organizational context described in the protocol, with one fencing session per week for 3 months for each of the two groups. The Early RIPOSTE Group attended sessions on Monday at 4:00 p.m., while the Delayed RIPOSTE Group attended sessions on Friday at 10:00 a.m. The duration of 1-1.5h/session was deemed insufficient by participants and fencing masters, and was therefore extended to 2h. Sessions were sometimes interrupted due to school vacations or the absence of the fencing masters. These unforeseen events were well managed thanks to good communication within the group, especially via social networks. The number of participants fluctuated with each session and was not limited to 10-12 as planned. This was because some participants started the program later, were absent or dropped out.
3.4.1.2 Structure of sessions
The sessions were divided into two periods of one hour each: a warm-up time dedicated to muscle awakening and progressive cardiorespiratory solicitation, followed by varied and adapted fencing exercises. The participants trained during lessons with the fencing master and among themselves. There were also regular breaks and exchange times according to the needs of the participants. When the number of participants was odd, they could not work in pairs. And when the number of participants was too high, the fencing master did not have enough time to work individually with each participant.
3.4.1.3 Equipment and materials
The sessions included the use of sabers and dummies. In some sessions, fencing outfits with jackets and masks were loaned to participants. One participant complained that there were no outfits in her size, and another that the mask did not fit her hearing aids.
3.5 Maintenance
3.5.1 Continuation of RIPOSTE or physical activity
Almost half of the participants planned to continue fencing, either in the RIPOSTE program or outside of it. Some wanted to continue in an adapted PA program, while others wanted to continue in a normal setting. For the other participants, the program made them aware of and motivated them to start new activities or to resume their previous activities. They felt more able and willing to pursue PA because of RIPOSTE but they wanted to move on to other types of PA, especially individual ones. Finally, a small minority of participants did not plan to continue PA, being mainly constrained by their schedule or physical condition.
3.5.2 Prospects for change or improvement
According to sports physicians, it seems necessary to improve patient recruitment to optimize participation. Better communication about PA by all healthcare professionals involved in patient care could be a good solution in this respect. Sports physicians could also show fencing videos to their patients during consultations. Beforehand, healthcare professionals could be made more aware of and trained in the issue of PA and cancer, or even attend fencing sessions themselves, to help them get the message across to their patients. To improve patient follow-up and support, it may also be necessary to formalize exchanges between sports physicians and fencing masters. Other professionals involved in patient care, such as psychologists, could also be involved in this collaboration. Patient support could also be optimized at the end of the program, either through group discussion or individual follow-up consultations. The interviews also revealed prospects for change linked to the organizational context of the intervention. These changes concern the duration of the sessions, which could be set at 2 hours, and interruptions during school vacations. Participants also suggested that session times be better aligned with school and work schedules. The question also arose as to whether a second session per week, at different times, would be necessary to best accommodate participants. To overcome the obstacle of distance, we could consider having the fencing master travel to extend the program to the whole of the target area, or cover the participants’ transport costs. Regarding the size of the group, it seemed preferable to all that it be small (10–12) and stable, with an even number of participants. Finally, the interviews also highlighted the importance of considering participants’ particularities (e.g., vision or hearing problems) to ensure that the equipment is adapted.
4 Discussion
To achieve greater dissemination and generalization of PA programs, one of the current challenges is to address the lack of translation of evidence-based research protocols into practice (38, 39). A recent review by Klesges et al. highlighted the importance of considering dissemination when designing health promotion programs (40), but few behavioral intervention evaluations reported evidence of external validity of RE-AIM criteria (41). To our knowledge, our pilot study is the first to evaluate the RIPOSTE program effectiveness and implementation process using the RE-AIM framework. The RE-AIM model proved useful in highlighting the complexities of RIPOSTE implementation and evaluation, which could lead to a more complete program that addresses issues related to improving the external and internal validity of translating research into practical-generalizable practice.
Reach among all patients was good (24 patients, i.e. around a third of eligible patients). Most participants were young and dynamic and had expectations and beliefs about program outcomes. Similarly, BC survivors who exercise regularly report significantly more positive attitudes towards their physical condition, higher body esteem, better mood and higher vigor than sedentary (42). Psychological or physical, barriers to participation were mainly related to fatigue and pain. Difficulties in reaching older or sedentary patients could then be explained by differences in their existing abilities, but also in their motivation and beliefs. Previous studies have established that there are significant differences in perceived barriers to PA as a function of age and activity level (43). Older people’s motivation to engage in PA is particularly influenced by socio-cognitive variables such as their perceived physical frailty and poor health, perceived self-efficacy, perceived social support or perceived benefits/barriers to continued PA (44). It has been shown that older adults may have prevailing social beliefs that exercise is inappropriate, or even harmful, for them, or that they may be unaware of the importance of regular PA in preserving their health (45, 46). Participation may also be influenced by PA preferences, which are subjective constructs that prioritize choices, influenced by structural, interpersonal and intrapersonal factors (47, 48). The higher level of participation among young patients could be partly due to the match between the sports on offer - described as innovative and original - and their preferences (48, 49). Taking these preferences into account could make it possible to adapt the offer and support the involvement of all patients in PA. This highlights a further reach challenge in trying to recruit older, sedentary patients, as these are often the ones who need it most.
There is a high level of evidence supporting the benefits of PA programs in breast cancer. More precisely, PA interventions have been shown to enhance QoL, reduce symptoms and adverse effects of medical treatments and above all decrease the risk of recurrence and comorbidities (3–9). However, less information was available regarding the nature and the timing for such PA interventions in breast cancer. In a systematic review (50) aimed to assess the effects of Olympic combat sport on health QoL, only 6 studies were available and only one concerned fencing and breast cancer (51). Overall, it appears that interventions based on Olympic combat sports produce beneficial effects on health QoL. Another review also showed that Olympic combat sport improves older adults physiological and physical health (52). Our study (10) allows to more precisely explore the potential effects of adapted fencing after breast cancer surgery, considering a different timing among patients (i.e. “Early” vs “Delayed” RIPOSTE program). Therefore, we can’t conclude to a superiority (in terms of QoL) of starting RIPOSTE early (i.e. 4 weeks after surgery) vs starting later (i.e. 3 months after surgery). The lack of statistical significance of the results despite an overall trend towards a more favorable effect in the “Early RIPOSTE” group can however be explained by various reasons. First, the small size of our pilot study doesn’t allow to have enough statistical power to show a significant difference. This is consistent with the calculation of the minimum detectable difference when planning the study. Indeed, we had calculated a predicted minimum detectable difference of 12 points of QoL, but the observed difference is 6.1 points. This should be considered to adjust the hypotheses for calculating the number of subjects required when setting up a larger study in the future. In addition, we also observed differences in clinical characteristics and perceived health at baseline between our two groups (DASH and HADS scores). Indeed, almost all of the baseline clinical and perceived health criteria, were more favorable in the “Early RIPOSTE” group compared to the “Delayed RIPOSTE” group. Of course, probabilistic randomization was done, but it could not correct these initial differences. It would then be appropriate in a future study to increase the size of the included population also allowing to target or identify more particularly the patients according to diseases stages (subgroup analysis) to help highlight a difference.
On the other hand, and as a corollary to our results (i.e. only a trend for a better improvement of QoL in the “Early RIPOSTE” group), we can also suggest, because of the absence of significant difference between the 2 groups, that starting adapted fencing early is not more harmful than starting it later. This message is important, because it’s still regularly considered that a rapid/early resumption of physical activity can be harmful for the patient (risk of injury, risk for the surgical scar in particular). Offering an adapted fencing program, with trained fencing masters and under cover of medical examinations (performed by certified sports medical doctors) should therefore be considered as key elements of the RIPOSTE program, and also a guarantee of quality and patient’s safety. The qualitative analysis also provides interesting feedback on the RIPOSTE program, showing that it has been largely adopted and implemented.
Data demonstrate that participants adopted the program, largely because of the physical and moral benefits associated with the practice, regardless of the timing of the intervention. These beneficial effects were probably influenced by the diversity and richness of the exercises proposed, which were appreciated, as well as by the good group cohesion, support and exchanges that punctuated the sessions and facilitated the patients’ experience of the disease. In line with previous research, camaraderie and friendship within a small group are important reasons why BC survivors adopt PA (53, 54), helping them to feel accepted and supported by “similar others” (54). Some participants were motivated by sharing experiences around cancer, while others adopted the program because it enabled them to distance themselves from their illness. RIPOSTE offered women the opportunity to define and listen to their own specific needs and interests. The program thus seems to have fostered autonomy and behavioral control, key factors in behavior change according to the theoretical underpinnings of the self-determination theory (55) and theory of planned behavior (56). Financial barriers are one of the reasons why many BC survivors don’t make PA a priority after treatment (57). The free nature of the program has played a key role in its adoption by patients, offering them the opportunity to try an activity they hadn’t considered or didn’t think was aligned to their capabilities. We also feel it’s important to reconsider the organizational aspects that could act as a barrier to adoption, by adapting more closely to participants’ availability, particularly in terms of school or work schedules, and by remedying the interruption of sessions during school vacations. The lack of intensity mentioned by some participants as a barrier to adoption could be linked to the size of the group, which is sometimes too large, or to the arrival of new participants during the program, which slows down the group’s progress. Despite this, our results emphasize the success of the program, which depended in part on good supervision of the fencing masters. To ensure the sustainability of the intervention, it is essential to ensure that participants receive adequate supervision and support.
Implementation of the protocol elements was stable throughout the intervention. Assessing barriers to implementation while the program was ongoing enabled professionals to modify the organization and overcome the most common barriers, for example by setting the duration of sessions at 2 hours. Fencing masters also used social networks to communicate with participants and deal with unforeseen circumstances. In future, setting the number of participants at 10 or 12 would enable participants to train in pairs under optimum conditions, with the opportunity to work individually with the fencing master. Particular attention will need to be paid to the equipment, so that it is adapted to the patients’ physical particularities.
By creating a motivating and supportive environment, group PA programs are considered an effective way of encouraging BC survivors to maintain PA (54). As many participants started to notice positive changes in their health (e.g. arm and breast rehabilitation and reduced fatigue), it seems that their motivation to maintain PA after the program was enhanced, as indicated in the interviews. However, we have little follow-up data on this dimension, as participants’ continuation of PA has not been evaluated over the long term. The lack of reported long-term maintenance information is problematic, as it limits the estimation of the long-term impact of the program. We believe that additional strategies are needed to encourage and support the continuation of the intervention. Patient follow-up and support could be improved, for example by implementing collaboration and communication strategies between sports physicians and fencing masters, but also with other healthcare professionals such as psychologists. Another idea for doing so would be to add follow-up assessments, which would take place at least 6 months after the end of the intervention, and which would report on its degree of sustainability.
5 Conclusion
This randomized pilot trial mainly reached young and dynamic patients, and demonstrated strong effects in the dimensions of adoption and implementation. While organizational factors such as time, setting and equipment have a major influence on the successful adoption and implementation of this type of intervention, the implementation of follow-up and support strategies for patients seems essential to adapt the offer to their needs and preferences. Participants’ abilities, social support or any physical and/or psychological difficulties are all factors to be taken into account when offering APA in a context as specific as that of cancer. Intervention effectiveness and maintenance require further attention and innovation to confirm the overall positive trends. Increasing the size of the included population and the number of centers involved (i.e. multicentric study), and using more rigorous measures to assess PA maintenance are needed in future research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by French ethics committee: Comité de Protection des Personnes Sud Méditerranée IV, N°ID-RCB: 2020-A01916-33. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SH: Writing – review & editing, Formal analysis. AV: Writing – review & editing, Writing – original draft, Validation, Supervision, Methodology, Formal analysis. MS: Writing – review & editing, Software, Methodology. CR: Writing – review & editing, Methodology, Funding acquisition, Formal analysis, Conceptualization. AC: Writing – review & editing, Project administration, Data curation. DP: Writing – review & editing, Validation, Supervision, Conceptualization. CD: Writing – review & editing, Supervision, Investigation, Formal analysis, Conceptualization. JR: Writing – review & editing, Supervision, Formal analysis. MT: Writing – review & editing, Supervision, Investigation, Formal analysis. EA: Writing – review & editing, Validation, Formal analysis. OH: Validation, Formal analysis, Writing – review & editing. BC: Writing – review & editing, Validation, Formal analysis. DH: Writing – review & editing, Validation, Supervision, Formal analysis, Conceptualization. AO: Writing – review & editing, Writing – original draft, Validation, Supervision, Project administration, Methodology, Funding acquisition, Formal analysis, Conceptualization. MP: Writing – original draft, Validation, Supervision, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Conceptualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by la Ligue Interrégionale Grand Est contre le Cancer and the Région Grand Est and Pôle Biologie Médecine Santé de l'Université de Lorraine, through a doctoral grant.
Acknowledgments
Acknowledgements to the sponsor: CHRU de Nancy (Direction de la Recherche et de l’Innovation).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1335442/full#supplementary-material
References
1. Panorama des cancers en France - Edition 2022 - Ref : PANOKFR2022 (2023). Available online at: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Panorama-des-cancers-en-France-Edition-2022.
2. Browall M, Ahlberg K, Karlsson P, Danielson E, Persson LO, Gaston-Johansson F. Health-related quality of life during adjuvant treatment for breast cancer among postmenopausal women. Eur J Oncol Nurs Off J Eur Oncol Nurs Soc. (2008) 12:180−9. doi: 10.1016/j.ejon.2008.01.005
3. Manneville F, Rotonda C, Conroy T, Bonnetain F, Guillemin F, Omorou AY. The impact of physical activity on fatigue and quality of life during and after adjuvant treatment for breast cancer. Cancer. (2018) 124:797−806. doi: 10.1002/cncr.31108
4. Van Dijck S, Nelissen P, Verbelen H, Tjalma W, Gebruers N. The effects of physical self-management on quality of life in breast cancer patients: A systematic review. Breast Edinb Scotl. (2016) 28:20−8. doi: 10.1016/j.breast.2016.04.010
5. Foucaut AM, Berthouze-Aranda SE, Touillaud M, Kempf-Lépine AS, Baudinet C, Meyrand R, et al. Reduction of health risk factors through an adapted physical activity program in patients with breast cancer. Support Care Cancer Off J Multinatl Assoc Support Care Cancer. (2014) 22:1097−104. doi: 10.1007/s00520-013-2065-3
6. Canário ACG, Cabral PUL, de Paiva LC, Florencio GLD, Spyrides MH, Gonçalves AK da S. Physical activity, fatigue and quality of life in breast cancer patients. Rev Assoc Med Bras 1992. (2016) 62:38−44. doi: 10.1590/1806-9282.62.01.38
7. Mishra SI, Scherer RW, Snyder C, Geigle PM, Berlanstein DR, Topaloglu O. Exercise interventions on health-related quality of life for people with cancer during active treatment. Cochrane Database Syst Rev. (2012). 2012(8):CD008465. doi: 10.1002/14651858.CD008465.pub2
8. Lee J, Lee MG. Effects of exercise interventions on breast cancer patients during adjuvant therapy: A systematic review and meta-analysis of randomized controlled trials. Cancer Nurs. (2020) 43:115. doi: 10.1097/NCC.0000000000000682
9. Pan Y, Yang K, Wang Y, Zhang L, Liang H. Could yoga practice improve treatment-related side effects and quality of life for women with breast cancer? A systematic review and meta-analysis. Asia Pac J Clin Oncol. (2017) 13:e79−95. doi: 10.1111/ajco.12329
10. Omorou A, Peiffert D, Rotonda C, Van Hoye A, Allado E, Hily O, et al. STUDY PROTOCOL adapted fencing for patients with invasive breast cancer: the RIPOSTE pilot randomized controlled trial. Front Sports Act Living. (2022) 4:786852. doi: 10.3389/fspor.2022.786852
11. Meyer V, Rosnet E, Guérin V, Hornus-Dragne D, Dedieu P, Poussel M. Fencing:" en garde! Ready! Fence". Sci Sports. (2017) 32:169−78. doi: 10.1016/j.scispo.2017.04.001
12. IFAPA. Definition (2023). Available online at: https://ifapa.net.
13. Rosenbaum E, Gautier H, Fobair P, Neri E, Festa B, Hawn M, et al. Cancer supportive care, improving the quality of life for cancer patients. A program evaluation report. Support Care Cancer Off J Multinatl Assoc Support Care Cancer. (2004) 12:293−301. doi: 10.1007/s00520-004-0599-0
14. Leroy MF. [Fencing for promoting health after breast cancer]. Rev Infirm. (2017) 66:41−3. doi: 10.1016/j.revinf.2017.07.008
15. Berretta M, Facchini BA, Garozzo D, Necci V, Taibi R, Torrisi C, et al. Adapted physical activity for breast cancer patients: shared considerations with two Olympic and world Italian sports champions. Eur Rev Med Pharmacol Sci. (2022) 26:5393−8.
16. Dugdill L, Graham RC, McNair F. Exercise referral: the public health panacea for physical activity promotion? A critical perspective of exercise referral schemes; their development and evaluation. Ergonomics. (2005) 48:1390−410. doi: 10.1080/00140130500101544
17. Haverinen EH, Elonheimo HM, Tolonen HK, Jousilahti PJ, Wennman HJC. The effects of long-term physical activity interventions in communities: Scoping review in the Nordic countries. Scand J Public Health. (2022) 50:272−86. doi: 10.1177/14034948211020599
18. Sansano-Nadal O, Giné-Garriga M, Brach JS, Wert DM, Jerez-Roig J, Guerra-Balic M, et al. Exercise-based interventions to enhance long-term sustainability of physical activity in older adults: A systematic review and meta-analysis of randomized clinical trials. Int J Environ Res Public Health. (2019) 16:2527. doi: 10.3390/ijerph16142527
19. Williams NH, Hendry M, France B, Lewis R, Wilkinson C. Effectiveness of exercise-referral schemes to promote physical activity in adults: systematic review. Br J Gen Pract. (2007) 57:979−86. doi: 10.3399/096016407782604866
20. White SM, McAuley E, Estabrooks PA, Courneya KS. Translating physical activity interventions for breast cancer survivors into practice: an evaluation of randomized controlled trials. Ann Behav Med Publ Soc Behav Med. (2009) 37:10−9. doi: 10.1007/s12160-009-9084-9
21. Jüni P, Altman DG, Egger M. Assessing the quality of controlled clinical trials. BMJ. (2001) 323:42−6. doi: 10.1136/bmj.323.7303.42
22. Glasgow RE, Klesges LM, Dzewaltowski DA, Bull SS, Estabrooks P. The future of health behavior change research: what is needed to improve translation of research into health promotion practice? Ann Behav Med Publ Soc Behav Med. (2004) 27:3−12. doi: 10.1207/s15324796abm2701_2
23. Glasgow RE, Emmons KM. How can we increase translation of research into practice? Types of evidence needed. Annu Rev Public Health. (2007) 28:413−33. doi: 10.1146/annurev.publhealth.28.021406.144145
24. Green LW, Glasgow RE. Evaluating the relevance, generalization, and applicability of research: issues in external validation and translation methodology. Eval Health Prof. (2006) 29:126−53. doi: 10.1177/0163278705284445
25. Salter KL, Kothari A. Using realist evaluation to open the black box of knowledge translation: a state-of-the-art review. Implement Sci. (2014) 9:115. doi: 10.1186/s13012-014-0115-y
26. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance | The BMJ. Available online at: https://www.bmj.com/content/374/bmj.n2061.
27. Guével MR, Pommier J. Recherche par les méthodes mixtes en santé publique : enjeux et illustration. Santé Publique. (2012) 24:23−38.
28. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. (1999) 89:1322−7. doi: 10.2105/AJPH.89.9.1322
29. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. RE-AIM planning and evaluation framework: adapting to new science and practice with a 20-year review. Front Public Health. (2019) 7:64. doi: 10.3389/fpubh.2019.00064
30. Tabak RG, Khoong EC, Chambers D, Brownson RC. Bridging research and practice. Am J Prev Med. (2012) 43:337−50. doi: 10.1016/j.amepre.2012.05.024
31. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European organization for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. JNCI J Natl Cancer Inst. (1993) 85:365−76. doi: 10.1093/jnci/85.5.365
32. Sprangers MA, Groenvold M, Arraras JI, Franklin J, te Velde A, Muller M, et al. The European Organization for Research and Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: first results from a three-country field study. J Clin Oncol Off J Am Soc Clin Oncol. (1996) 14:2756−68. doi: 10.1200/JCO.1996.14.10.2756
33. Dubert T, Voche P, Dumontier C, Dinh A. [The DASH questionnaire. French translation of a trans-cultural adaptation]. Chir Main. (2001) 20:294−302. doi: 10.1016/S1297-3203(01)00049-X
34. Smets EM, Garssen B, Bonke B, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. (1995) 39:315−25. doi: 10.1016/0022-3999(94)00125-O
35. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361−70. doi: 10.1111/j.1600-0447.1983.tb09716.x
36. Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381−95. doi: 10.1249/01.MSS.0000078924.61453.FB
37. Huberman A, Miles M. The qualitative researcher’s companion. Thousand Oaks California: SAGE Publications, Inc (2002). Available at: https://methods.sagepub.com/book/the-qualitative-researchers-companion.
38. Glasgow RE, Lichtenstein E, Marcus AC. Why don’t we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am J Public Health. (2003) 93:1261−7. doi: 10.2105/AJPH.93.8.1261
39. Cohen DJ, Crabtree BF, Etz RS, Balasubramanian BA, Donahue KE, Leviton LC, et al. Fidelity versus flexibility: translating evidence-based research into practice. Am J Prev Med. (2008) 35:S381−9. doi: 10.1016/j.amepre.2008.08.005
40. Klesges LM, Estabrooks PA, Dzewaltowski DA, Bull SS, Glasgow RE. Beginning with the application in mind: Designing and planning health behavior change interventions to enhance dissemination. Ann Behav Med. (2005) 29:66−75. doi: 10.1207/s15324796abm2902s_10
41. Dzewaltowski DA, Estabrooks PA, Klesges LM, Bull S, Glasgow RE. (2004). Behavior change intervention research in community settings: how generalizable are the results? Health Promot Int. 19(2):235–45.
42. Pinto BM, Trunzo JJ. Body esteem and mood among sedentary and active breast cancer survivors. Mayo Clin Proc. (2004) 79:181−6. doi: 10.4065/79.2.181
43. O’Neill K, Reid G. Perceived barriers to physical activity by older adults. Can J Public Health Rev Can Sante Publique. (1991) 82:392−6.
44. Rhodes RE, Martin AD, Taunton JE, Rhodes EC, Donnelly M, Elliot J. Factors associated with exercise adherence among older adults. Sports Med. (1999) 28:397−411. doi: 10.2165/00007256-199928060-00003
45. Afonso C, Graça P, Kearney JM, Gibney MJ, de Almeida MD. Physical activity in European seniors: attitudes, beliefs and levels. J Nutr Health Aging. (2001) 5:226−9.
46. Hardcastle S, Taylor AH. Looking for More than Weight Loss and Fitness Gain: Psychosocial Dimensions among Older Women in a Primary-Care Exercise-Referral Program. J Aging Phys Act. (2001) 9:313−28. doi: 10.1123/japa.9.3.313
47. Dietrich F, List C. Where do preferences come from? Int J Game Theory. (2013) 42:613−37. doi: 10.1007/s00182-012-0333-y
48. Crane J, Temple V. A systematic review of dropout from organized sport among children and youth. Eur Phys Educ Rev. (2015) 21:114−31. doi: 10.1177/1356336X14555294
49. Hallmann K, Wicker P, Breuer C, Schönherr L. Understanding the importance of sport infrastructure for participation in different sports – findings from multi-level modeling. Eur Sport Manag Q. (2012) 12:525−44. doi: 10.1080/16184742.2012.687756
50. Valdés-Badilla P, Herrera-Valenzuela T, Guzmán-Muñoz E, Delgado-Floody P, Núñez-Espinosa C, Monsalves-Álvarez M, et al. Effects of olympic combat sports on health-related quality of life in middle-aged and older people: A systematic review. Front Psychol. (2022) 12:797537. doi: 10.3389/fpsyg.2021.797537
51. Lantheaume S, Fabre F, Fisch C, Motak L, Massol P, Lantheaume S, et al. Cancer du sein, activité physique adaptée et qualité de vie. Ann Méd-Psychol Rev Psychiatr. (2017) 175:841−8. doi: 10.1016/j.amp.2016.03.016
52. Valdés-Badilla P, Herrera-Valenzuela T, Ramirez-Campillo R, Aedo-Muñoz E, Báez-San Martín E, Ojeda-Aravena A, et al. Effects of olympic combat sports on older adults’ Health status: A systematic review. Int J Environ Res Public Health. (2021) 18:7381. doi: 10.3390/ijerph18147381
53. Wurz A, St-Aubin A, Brunet J. (2015). Breast cancer survivors’ barriers and motives for participating in a group-based physical activity program offered in the community. Support Care Cancer. 23:2407–16.
54. Emslie C, Whyte F, Campbell A, Mutrie N, Lee L, Ritchie D, et al. ‘I wouldn’t have been interested in just sitting round a table talking about cancer’; exploring the experiences of women with breast cancer in a group exercise trial. Health Educ Res. (2007) 22:827−38. doi: 10.1093/her/cyl159
55. Deci EL, Ryan RM. Intrinsic motivation and self-determination in human behavior. Springer Science & Business Media. (2013), 606. p.
56. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. (1991) 50:179−211. doi: 10.1016/0749-5978(91)90020-T
Keywords: breast cancer, adapted physical activity, fencing, quality of life, fatigue
Citation: Hasnaoui S, Van Hoye A, Soudant M, Rotonda C, Carvalho de Freitas A, Peiffert D, Delattre C, Raft J, Temperelli M, Allado E, Hily O, Chenuel B, Hornus-Dragne D, Omorou AY and Poussel M (2024) Evaluating the feasibility and acceptability of an adapted fencing intervention in breast cancer surgery post-operative care: the RIPOSTE pilot randomized trial. Front. Oncol. 14:1335442. doi: 10.3389/fonc.2024.1335442
Received: 11 January 2024; Accepted: 25 March 2024;
Published: 11 April 2024.
Edited by:
Valeria Sebri, European Institute of Oncology (IEO), ItalyReviewed by:
Xinfeng Wang, Shanxi Province Cancer Hospital, ChinaLiam Humphreys, Sheffield Hallam University, United Kingdom
Copyright © 2024 Hasnaoui, Van Hoye, Soudant, Rotonda, Carvalho de Freitas, Peiffert, Delattre, Raft, Temperelli, Allado, Hily, Chenuel, Hornus-Dragne, Omorou and Poussel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mathias Poussel, bS5wb3Vzc2VsQGNocnUtbmFuY3kuZnI=