
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 16 February 2024
Sec. Cancer Epidemiology and Prevention
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1335344
This article is part of the Research TopicRepurposed Drugs Targeting Cancer Signaling Pathways: Clinical Insights to Improve Oncologic Therapies Volume IIView all 10 articles
 Eulalia Villegas1
Eulalia Villegas1 María Arruñada2Miguel Ángel Casado2Sonia González3,4,5María Estela Moreno-Martínez6María Ángeles Peñuelas7Ana Maria Torres1Yanik Sierra8
María Arruñada2Miguel Ángel Casado2Sonia González3,4,5María Estela Moreno-Martínez6María Ángeles Peñuelas7Ana Maria Torres1Yanik Sierra8 Miguel Angel Seguí9,10*
Miguel Angel Seguí9,10*The diagnosis and treatment of cancer impose a significant emotional and psychological burden on patients, families, and caregivers. Patients undergo several interventions in a hospital setting, and the increasing number of patients requiring extended care and follow-up is driving the demand for additional clinical resources to address their needs. Hospital at Home (HaH) teams have introduced home-administered oncologic therapies that represent a new model of patient-centered cancer care. This approach can be integrated with traditional models and offers benefits to both patients and healthcare professionals (HCPs). Home-administered treatment programs have been successfully piloted globally, demonstrated as a preferred option for most patients and a safe alternative that could reduce costs and hospital burden. The document aims to establish the minimum recommendations for the home administration of oncologic therapies (ODAH) based on a national expert agreement. The expert panel comprised seven leading members from diverse Spanish societies and three working areas: clinical and healthcare issues, logistical and administrative issues, and economic, social, and legal issues. The recommendations outlined in this article were obtained after a comprehensive literature review and thorough discussions. This document may serve as a basis for the future development of home-administered oncologic therapy programs in Spain.
Cancer remains a major global health problem despite scientific efforts in the development of new therapies (1, 2). According to GLOBOCAN data, 19.3 million new cases and 10 million cancer deaths were reported in 2020 worldwide, and a 47% increase in new cases will occur in 2040 if the current rates remain constant (3). In Spain, 277,394 new cases were diagnosed in 2020, currently being the second cause of death and accounting for 22.2% of total deceases (109,706 cancer deaths). According to Spanish Network of Cancer Registries (REDECAN) data, 280,100 newly diagnosed patients are expected by the end of 2022 (4).
Patients with cancer undergo multiple interventions, typically performed within a hospital setting that provides the requisite logistical resources. The reliance on the hospital environment has been amplified by the necessity for a multidisciplinary team of healthcare professionals (HCPs) and the development and deployment of new technologies for diagnosis and treatment. Nevertheless, the COVID-19 pandemic has had adverse effects in various routine clinical procedures due to hospital saturation, insufficient resources, and recommended restrictions aimed at reducing the risk of infection (5–7). Consequently, the regular activity of the oncology units was affected (6, 7). A meta-analysis reported a reduction in general clinical activity in 58% of the centers worldwide during the first wave (6). Frequently, treatment delay or cancellation, change in treatment plans, and delay in outpatient visits (in 58%, 65%, and 75% of centers, respectively) were registered, and many centers (72%) implemented virtual visits (6).
Hospital at Home Service (HaH) is hospital-level substitutive care delivered at home for acute patients who required hospital admission. HaH has been associated with several advantages, including patient safety, reduction of nosocomial complications, similar or even better health outcomes compared to conventional hospitalization, high satisfaction levels from both patients and caregivers, and cost savings (8, 9).
HaH teams are trained to perform complex interventions at home, which would reduce the hospital burden preventing the negative consequences of this overload on cancer patients (10–13). Moreover, treating cancer patients at home can help to control high-risk situations such as the exposure to epidemics of multidrug-resistant pathogens or community viral infections with high morbidity and mortality (14).
Despite the growing interest, the available literature exploring the possibilities and benefits of oncologic drug administration at home (ODAH) and supportive care treatments in oncology patients is still limited and controversial, especially in Spain. The aim of the present document is to establish the minimum recommendations for an ODAH based on a national expert consensus. It should be noted that in the present document this setting refers to all healthcare-related procedures coordinated by a multidisciplinary group of HCPs that attend to the diagnostic and therapeutic needs of selected oncology patients at their homes. This home-based care is a complementary element of the protocol designed for those patients and, thus, it must be integrated as part of it. Due to their singularities, pediatric oncologic patients and those with haemato-oncologic diseases are not considered in the elaboration of this recommendations.
The panel of experts was multidisciplinary and included seven professionals from Madrid, Barcelona and Vigo involved in cancer treatment and who belong to diverse scientific societies: SEFH (Spanish Society of Hospital Pharmacy), SEHAD (Spanish Society of Home Hospitalization), SEEO (Spanish Oncology Nursing Society), and SEOM (Spanish Society of Medical Oncology). The panel included experts in the field of oncology, nursing, HaH, hospital pharmacy, and health economics. Three working areas were defined: 1) clinical and healthcare issues, 2) logistical and administrative issues, and 3) economic, social, and legal issues. Experts were assigned to a working group according to their knowledge and expertise (Supplementary Table 1).
A series of relevant questions for each section were prepared (see Supplementary Table 2). The experts reviewed the literature and provided individual responses, but a systematic review was not conducted. The working group then deliberated on the responses and arrived at a consensus on the recommendations. The decisions were primarily guided by expert opinions and were reinforced by the existing literature. In instances where evidence was lacking, only expert opinions were taken into account.
The consensus meeting took place on November 16th, 2022. The recommendations of each working group were presented to all experts and discussed in the meeting to reach a final agreement. The present recommendations are presented in question-answer format and have been endorsed by all participants. The role and functions of the main stakeholders involved in home administration of oncologic therapies were defined and summarized in Supplementary Table 3.
When considering the feasibility of a home-based oncology treatment program, it is important to take into account various factors related to the oncology drug, therapy, patient characteristics, and healthcare environment.
Question 1. Which drugs are potentially suitable for home administration?
When planning a home-based oncology treatment program, it is important to consider the pharmaceutical and clinical characteristics of the administered treatment, including its posology, stability, route and duration of administration, and safety profile. Most articles describing ODAH focus on parenterally administered treatments, with oral medications not typically considered as home-administered chemotherapy (12, 15). Oncologic therapies that have a non-complex administration protocol and a known and manageable safety profile are good candidates for home-base administration (15). The duration of chemotherapy treatment typically varies from two to eight months, and shorter administration times are generally preferable to longer ones (16). Prolonged home-administered therapy, especially if it requires the presence of a nurse throughout the entire procedure, can result in a waste of resources for hospitals and increase costs (15, 17, 18). According to published initiatives, the infusion duration of home-administered drugs usually took less than four hours (15). Moreover, guaranteeing drug stability for its administration at home is essential to ensure the best treatment for the patient (19).
An indicative list of oncologic drugs that can potentially be administered at home is presented in Table 1, although there is significant variability in the types of antineoplastic drugs used in home-based therapy programs (12, 15, 20–22).
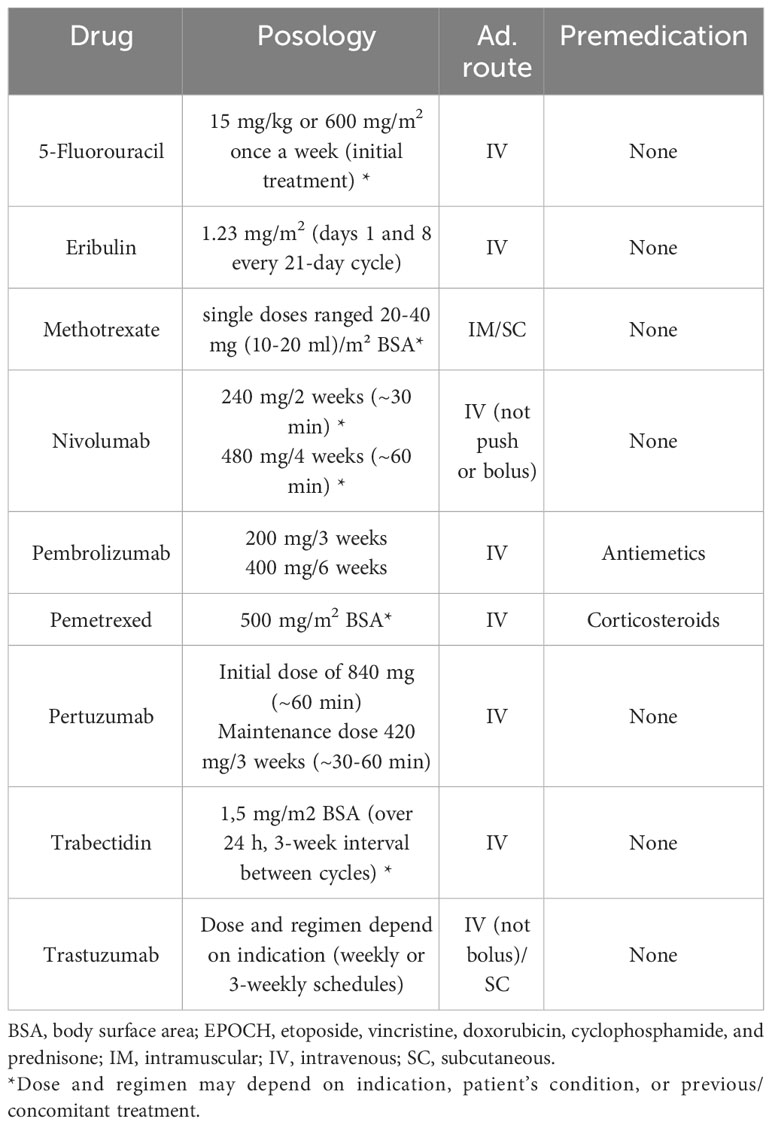
Table 1 Potential oncologic treatments for home administration.
Question 2. What profile of patients would benefit from oncology treatment administered at home?
Eligibility criteria for ODAH is crucial to maintain the safety and should be based on patient and caregiver readiness, diagnosis, characteristics and co-morbidities, treatment regimen, and hospital proximity and home environment (Table 2) (15, 16). Inclusion criteria should be related to the clinical and physical state, cancer type and grade, and type of treatment. External factors, such as the distance to the hospital, presence of a caregiver/relative and housing conditions should also be assessed by a multidisciplinary team of HCPs (16).
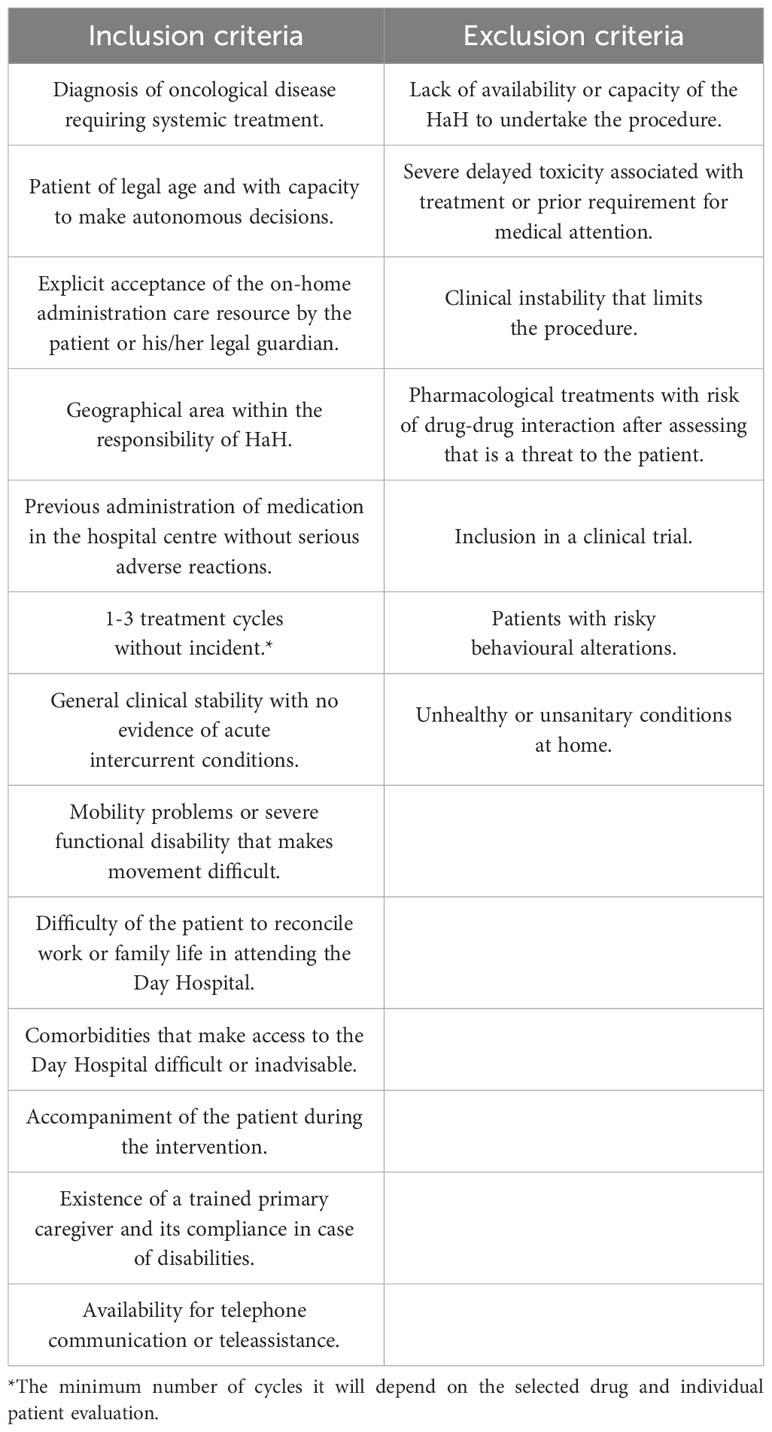
Table 2 Recommended inclusion and exclusion criteria to select the most adequate patients for home-administered chemotherapy.
Question 3. How would ODAH compromise the efficacy, safety, and quality of life of systemic treatments?
Research has shown that home-administered oncology treatment can be just as effective and safe as hospital-administered treatment and may lead to improvements in quality of life and patient satisfaction (12, 15, 16). Recently, a systematic review found that ODAH presented no statistically significant differences in quality of life compared to hospital administered setting (12, 23). Safety data showed that toxicities were expected regardless of the location of administration. In Spain, a randomized controlled trial comparing home-based chemotherapy to hospital treatment revealed higher satisfaction with home-based administration in terms of the perception of nursing availability and communication (24). Another systematic review, exploring the advantages of home chemotherapy pointed that the results obtained in several trials sustained that treatment administration at home was safe and feasible, and preferred by patients and caregivers (25).
However, some clinicians may still have concerns about patient safety (26), but the appropriate preparation and education can help ensure the safety of the procedure (16). Patients and caregivers should receive educational and supporting material that explains the program implications in simple and easy-to-understand vocabulary. Periodic satisfaction surveys can also help to monitor the patient experience and identify areas for improvement. Also, further research is needed to compare the efficacy, safety, and quality of home-administered therapy to hospital treatment.
Question 4. What kind of education, accreditation or training should receive the HCPs involved?
Oncology, HaH and Pharmacy Services must be coordinated for drug prescription, validation, evaluation of the clinical state before drug administration, detection of adverse events, and patient follow-up. Therefore, an interdisciplinary group of HCPs with defined responsibilities is required along with specialized education and training (15, 27).
Furthermore, antineoplastic drug administration is a complex procedure that must be performed by a qualified professional to avoid undesirable incidents (28–31). Specialized nurses are responsible for the chemotherapy and biotherapy administration, and they have specific education and training that ensure the safe care of the patient (28, 32).
Implementing this strategy will typically necessitate the establishment of specialized teams dedicated to administering antineoplastic treatments in patients’ homes. While it is feasible to utilize home hospitalization resources or hospital nursing to a certain extent, this approach generally entails a greater demand for human and material resources.
Question 5. What kind of controls should be performed?
Experts suggest and agree that certain minimum requirements must be met by the hospital when considering a ODAH program: 1) to have a Medical Oncology Service; 2) to have a territorial/regional HaH Service; 3) to have a Pharmacy Service that ensures the highest quality of care for patients; 4) to be provided with minimum healthcare resources in the units and available involved Services; and 5) to perform a demographic and geographic evaluation of the healthcare area.
An initial pilot program should be set up to evaluate the results and determine the compliance of requirements. Standardized approaches and procedures, along with interdisciplinary professional review, can help avoid medication mistakes (28–30). An indicative checklist is provided in Table 3 and a standardized nurse visit is shown in Supplementary Figure 1.
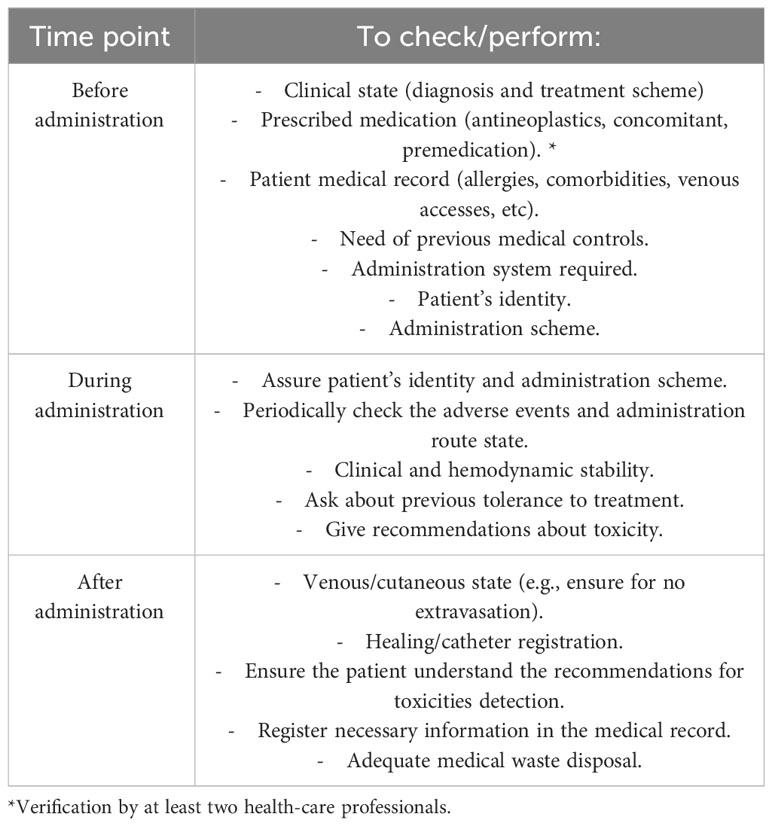
Table 3 Checklist of the optimal steps to perform the ODAH.
Question 6. What would be the minimum instruments, apparatus or equipment required?
Table 4 includes a list of materials to be considered for an ODAH program. The minimum required material will depend on the therapy and clinical state of the patient (18).
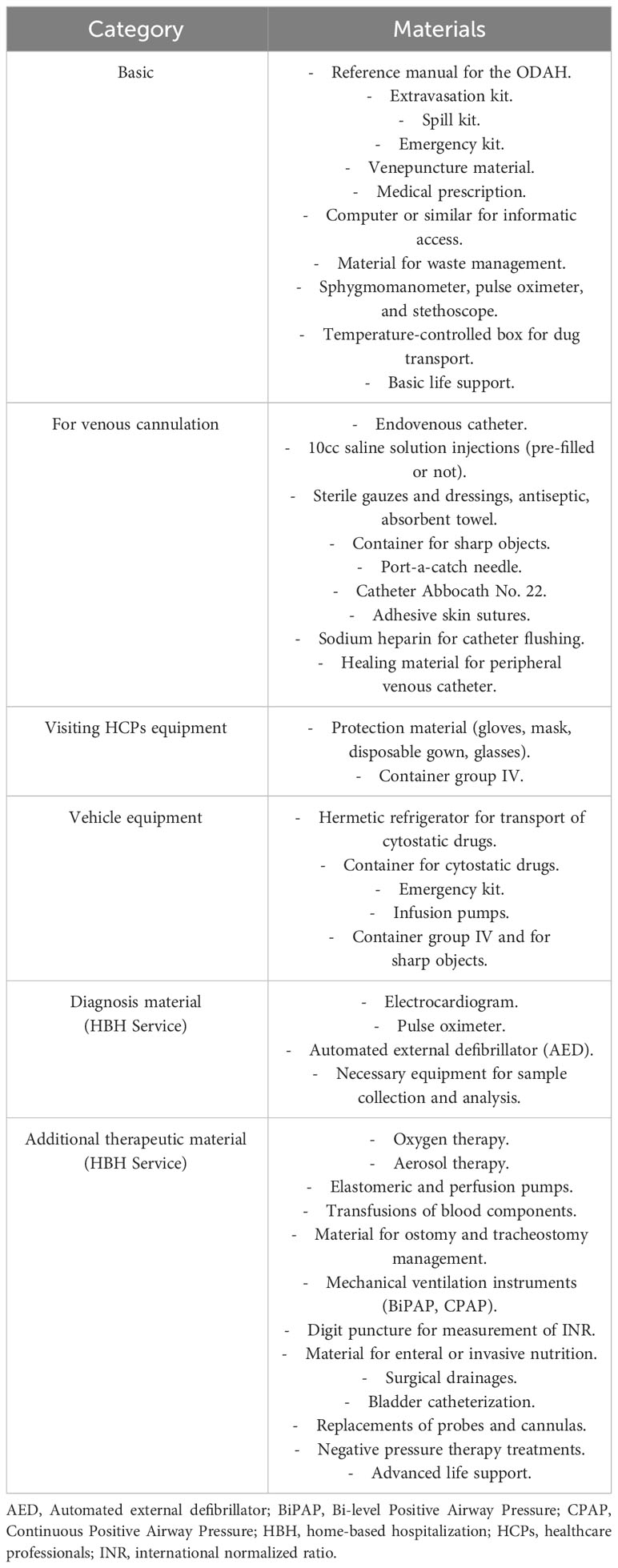
Table 4 Basic and additional materials needed for ODAH procedure.
Question 7. Which aspects should be considered for drug preparation?
To ensure the best treatment for the patient, it is crucial to maintain drug stability during home delivery. This requires a review of all factors involved in drug preparation and transport, and the implementation of protocols and controls to assess drug stability for optimal implementation of a home-based therapy program (19).
Table 5 contains the agreed recommendations made by the panel of experts regarding clinical and healthcare issues section.
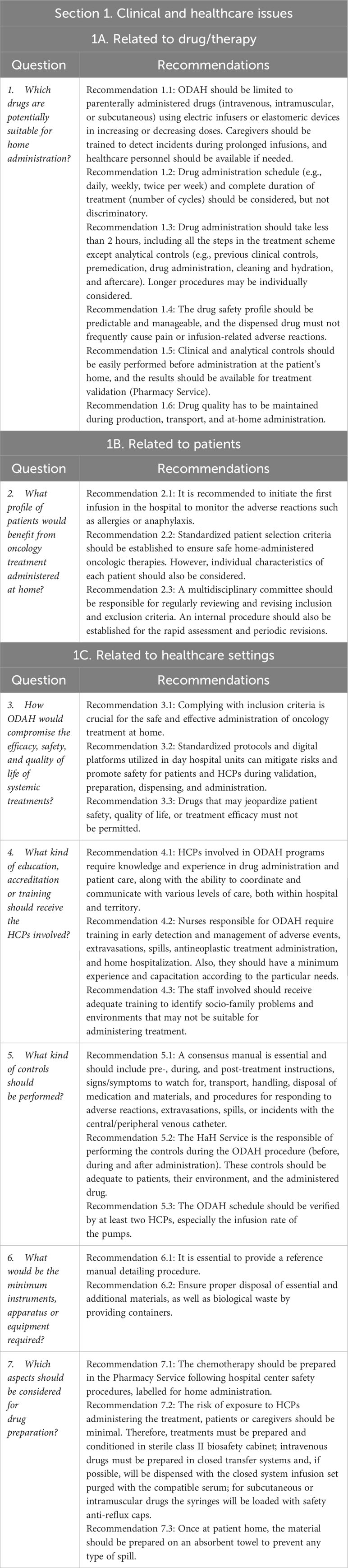
Table 5 Expert recommendations for clinical and healthcare issues.
Question 8. To consider the ODAH, what are the requirements that must be fulfilled by the oncology department/hospital?
Simplifying the patient’s journey and ensuring the availability of necessary resources and adherence to schedules and processes is crucial. This can be achieved by developing agreed protocols and plans that outline all the steps, stakeholders, and professionals involved. Therefore, it is essential to collaborate and coordinate among nursing, pharmacy, oncology and HaH Services, and all the other involved parties for the program’s success (16, 33, 34). Figure 1 depicts a recommended circuit model for ODAH.
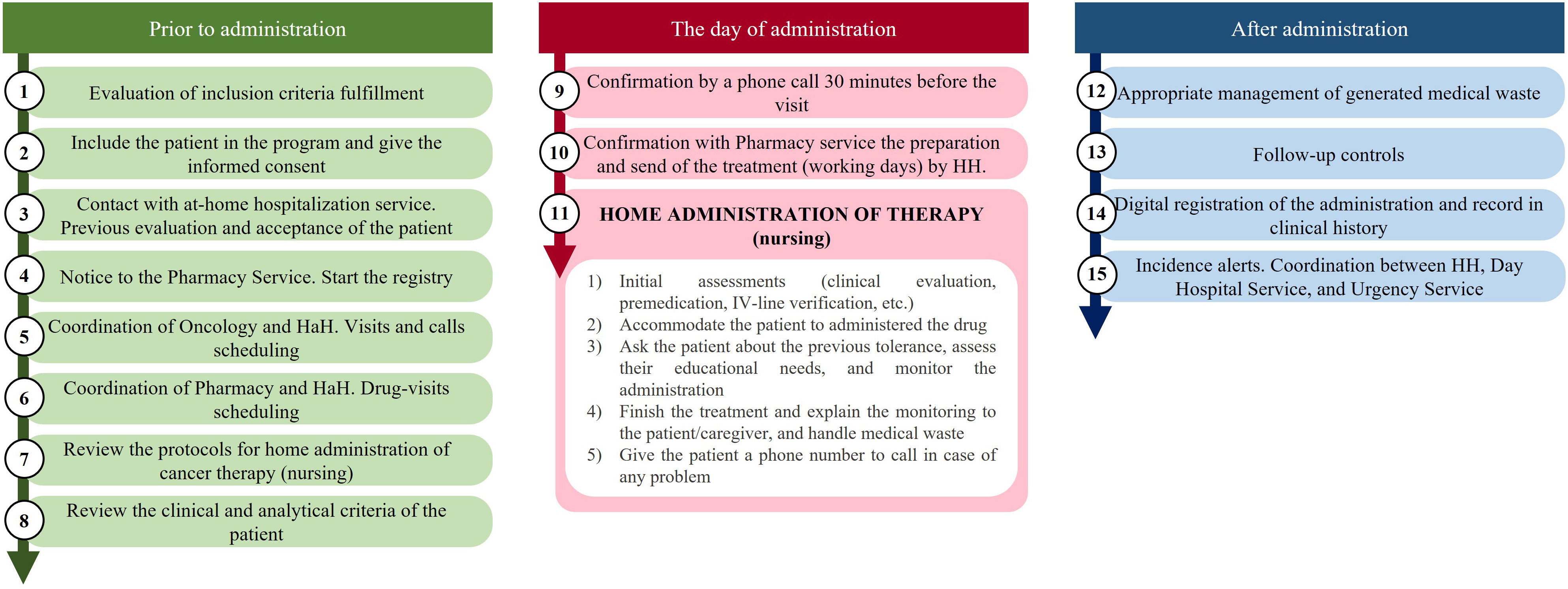
Figure 1 Diagram of the recommended logistic rout for home administration oncologic therapies.
Question 9. When should be considered ODAH and for what duration?
The inclusion of a cancer patient into ODAH will be based on compliance with the defined inclusion criteria. Once the oncologist has approved the treatment and the patient is considered a potential candidate, the Oncology Service is able to coordinate with the HaH Service to determine the patient’s eligibility.
Question 10. How should the telephone for medical support be implemented?
A dedicated telephone line for cancer patients has been shown to be effective in reducing unnecessary emergency evaluations and hospital admissions, leading to lower healthcare costs and improved patient quality of life. Oncologists and specialized nurses can detect potential adverse events early, reducing the need for hospital visits, while telephone support can enhance patient-centred care (33, 35).
Question 11. How could be defined the hospital logistic route?
Typically, oncology patients follow a pathway for treatment that includes: 1) access/referral to Oncology Service; 2) assessment and decision to treat; 3) patient consent for treatment. In home-based chemotherapy programs, eligibility for home-administered therapy is determined after the treatment decision has been made (16).
Table 6 contains the agreed recommendations regarding section 2.
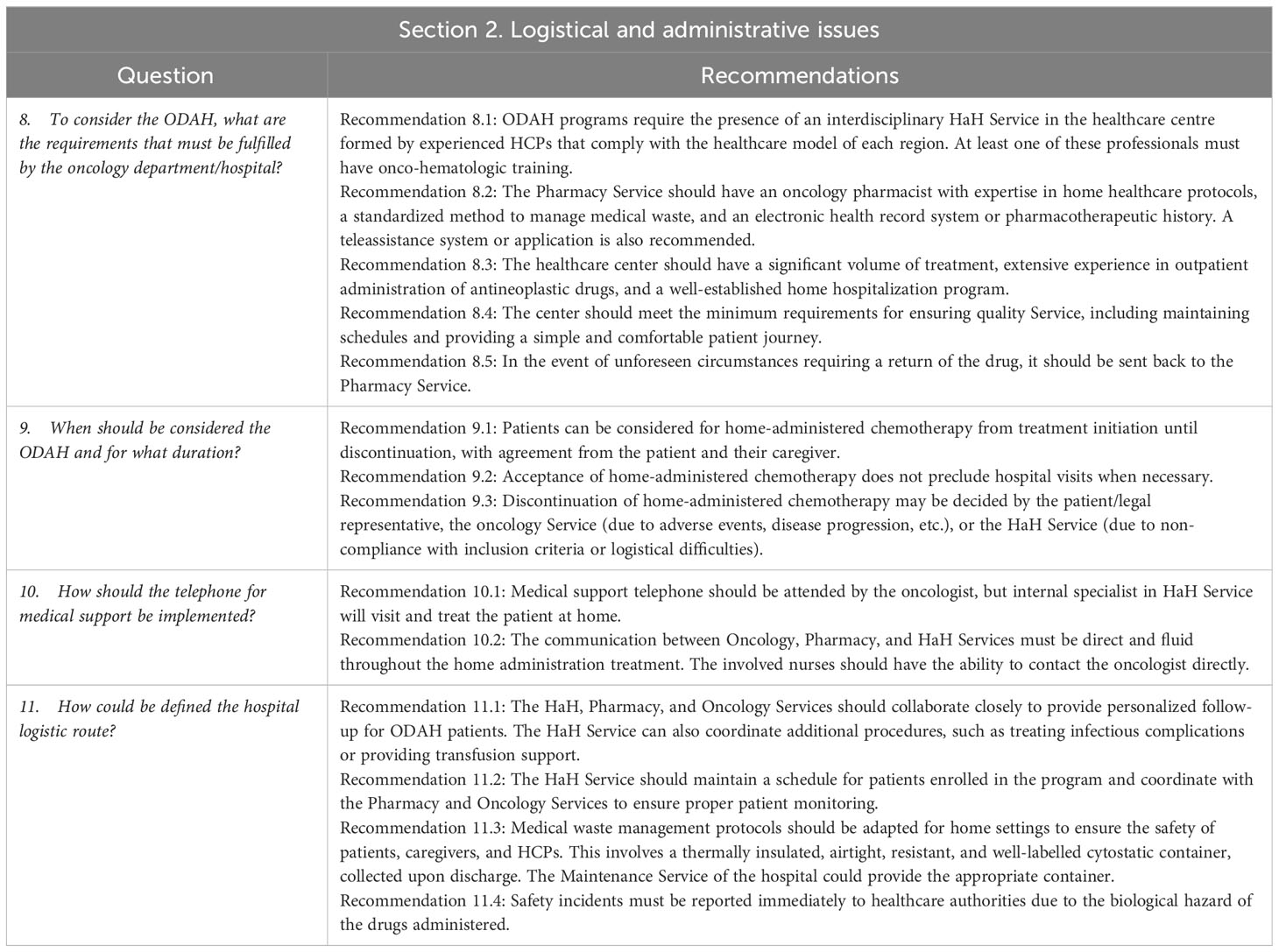
Table 6 Expert recommendations for logistical and administrative issues.
Question 12. How can the efficiency of ODAH be determined?
Health interventions must provide information on their socio-economic value, including the economic impact and whether the additional benefit justifies the cost. Healthcare policy and decision-making processes are recognizing the need to limit resources to finance available interventions while incorporating the concept of opportunity cost from a societal perspective. Therefore, healthcare programs should consider incorporating health outcomes and their incremental costs to provide necessary evidence for evaluating new interventions. A similar methodology should be employed to evaluate the efficiency of ODAH.
Firstly, to evaluate the efficiency of ODAH, the perspective of the analysis has to be established. As ODAH has potential benefits for both patients and the Spanish NHS, the analysis should be conducted from a societal perspective, which considers direct healthcare costs such as the cost of medication, premedication, hydration, and used materials, as well as possible adverse reactions. Direct non-healthcare costs, such as patient or family transportation expenses, the cost of time spent on these trips, and the cost of time spent waiting, should also be considered. Finally, indirect costs such as losses in productivity should be factored in as well.
To optimize ODAH efficiency, experts suggest conducting societal perspective evaluations, which can benefit patients and public healthcare administration by reducing hospital load. For oncological therapies, recommendations include implementing efficiency analysis and considering greater patient comfort and satisfaction, avoiding travel, and reduced Services saturation. If only the Spanish NHS perspective is considered, the cost of home administration may appear higher than hospital administration.
To fulfil the quality-of-life assessment, it is essential to measure outcomes related with patient perception (Patient-Reported Outcomes Measures-PROM/Patient-Reported Experience Measures-PREM) through validated questionnaires (e.g., from CatSalut in the case of Catalonia, or from the Patient Care Unit of the reference hospital). Ultimately, the results obtained in HaH can be compared to those obtained in cost-benefit analysis of the Day Care Hospital.
The implementation of an ODAH offers numerous benefits for patients, caregivers, and society as: (i) it eliminates the need for patients and caregivers to travel to the hospital for oncological therapies, thus saving time and effort; (ii) it prevents work productivity losses for the patient’s family or caregivers who would have otherwise accompanied them to the hospital; (iii) it reduces the care burden at the oncological day hospital, freeing up critical hospital resources; (iv) it potentially improves adherence and persistence to treatment since nursing staff regularly visit the patient’s home. Without home administration, there is a potential risk of non-attendance, which could result in medication non-receipt; (v) patients may experience greater satisfaction with treatment and improved humanization of care, as the home environment reduces the feeling of medicalization and increases comfort during administration, potentially leading to an improvement in health-related quality of life.
In turn, adequate organizational support, including sufficient budgetary and human resources, is necessary to meet the needs of patients in implementing an ODAH. This includes incorporating qualified technical staff and obtaining appropriate materials to carry out the project effectively. It is also recommended to carry out a pilot program in order to conduct an economic evaluation (Figure 2).

Figure 2 Factors to be considered for the implementation of a pilot study with the aim of assessing the efficiency of the ODAH.
Beyond this, other proposals could aid in implementing the ODAH setting, including the possibility of the laboratory covering the differential costs for home administration by sponsoring each patient attended or providing indirect resources, or by removing the VAT associated with drugs for home administration (as done in the United Kingdom) to utilize the potential savings to cover the additional expenses related (18).
In a systematic review by Cool et al. that evaluated the cost efficiency of Oncological Day Hospital at Home (ODAH), nine studies were reviewed (12). Of these, five studies estimate the difference in costs for one home-administered treatment versus hospital-administered from the perspective of the National Health Insurance. These studies reported reductions in costs (ranging from 9% to 53%) that favored home administration (12, 36, 37). Another study evaluated the cost per cycle and resulted in a 3.8% reduction of the costs from a societal perspective (12, 26). Additional systematic review, which included 13 heterogeneous articles, reported that home chemotherapy could result in savings ranging from $1,928 and $2,974 per treatment (38). Recent economic studies also suggest that ODAHs could lead to lower costs (39, 40). Nonetheless, current data do not fully confirm the potential cost reduction derived from home administration, but it is likely that better results of PROMs and PREMs would be obtained (12).
Question 13: How can the economic impact of ODAH be determined?
To conform with the guidelines presented in the CatSalut Guide for Economic Evaluations and Budgetary Impact Analyses, it is important to conduct separate assessments of an intervention’s efficiency and its economic impact in order to ensure proper evaluation (41).
As previously mentioned, the societal perspective is the most appropriate since it takes into account the benefits for the patient and their relatives and caregivers. Once the perspective has been defined, costs can be identified, quantified, and evaluated (42).
From a methodological perspective, it is necessary to conduct an economic impact assessment to estimate the difference in costs between ODAH and standard hospital administration (43, 44). To achieve this, two different scenarios should be developed for cancer patients who are suitable for home administration. In the current scenario, named as scenario 1, (S1; hospital administration) all patients received chemotherapy at the hospital, whereas in the potential scenario, named as scenario 2, (S2; home administration) all patients received the treatment at home. The economic impact of ODAH would be the difference between these two scenarios (Figure 3). Then, three possible results can be obtained after the estimation: 1) S1 costs higher than S2 costs; 2) S1 costs lower than S2; and 3) the same costs for S1 and S2.
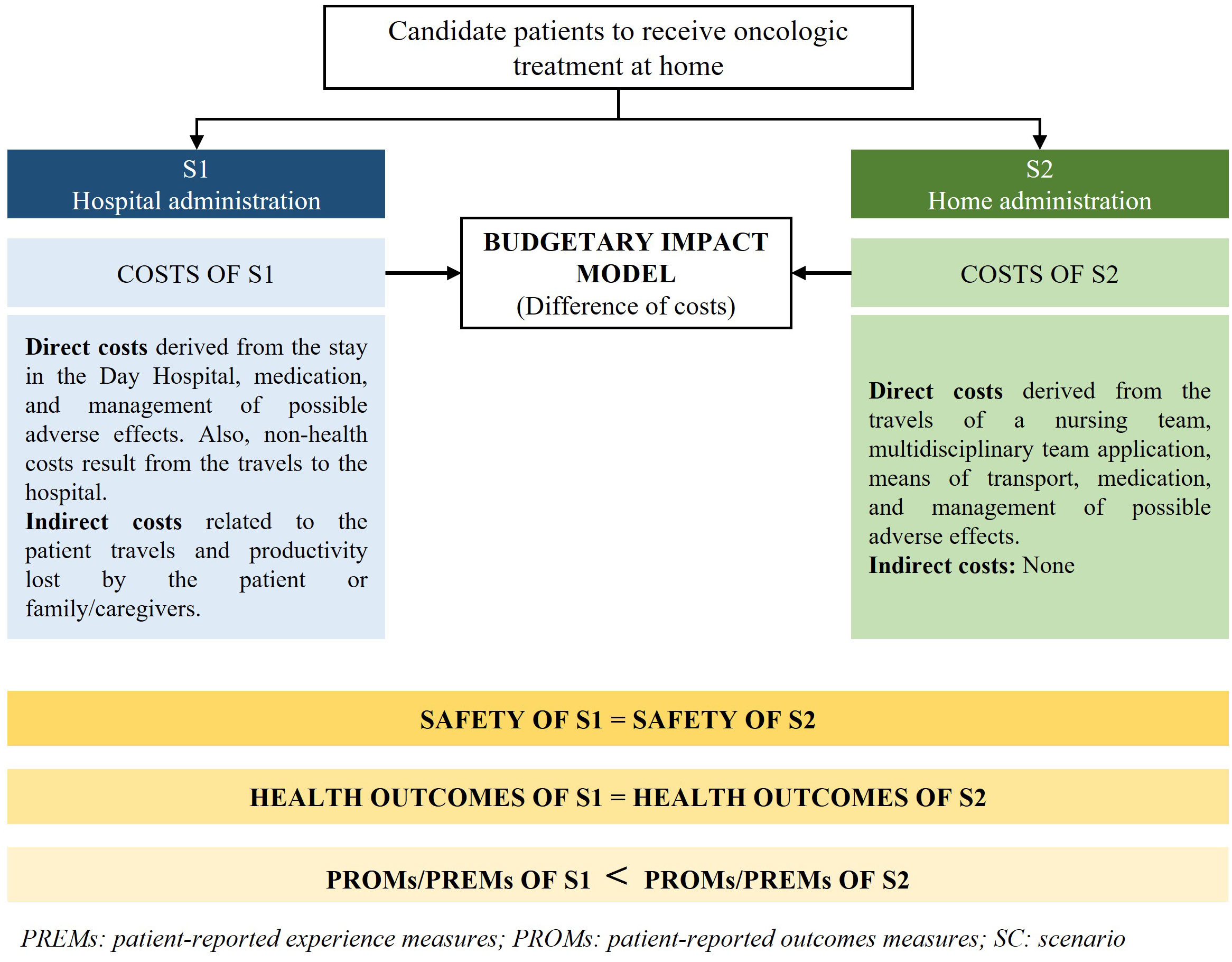
Figure 3 Scheme of the relevant aspects to consider during the economic evaluation of home-administered oncologic therapies.
While it would be reasonable to assume that the costs of scenario S1 would be comparable to those of scenario S2, if it is found that the costs of S1 are actually higher than those of S2, this could provide additional support for the adoption of ODAH programs from a healthcare administration perspective.
Question 14. Are there legal and ethical issues to be solved to implement the program?
Currently, there is no specific national legislation that regulates the ODAHs. Consequently, HCPs who provide home-administered treatments are legally covered as if they were delivering them at a hospital. Nevertheless, the administration of antineoplastic therapies must be carried out by qualified and experienced professionals to minimize potential risks for the patient and the handler. In case of accidental contamination such as breakage, spillage, or any other incident, the HCPs should be aware of the appropriate measures to manage it. Therefore, the administration of cytostatic agents should be restricted to HCPs who are trained and experienced in the safe handling of chemotherapeutic drugs (45).
Table 7 summarizes the agreed recommendations for the panel of experts regarding section 3.
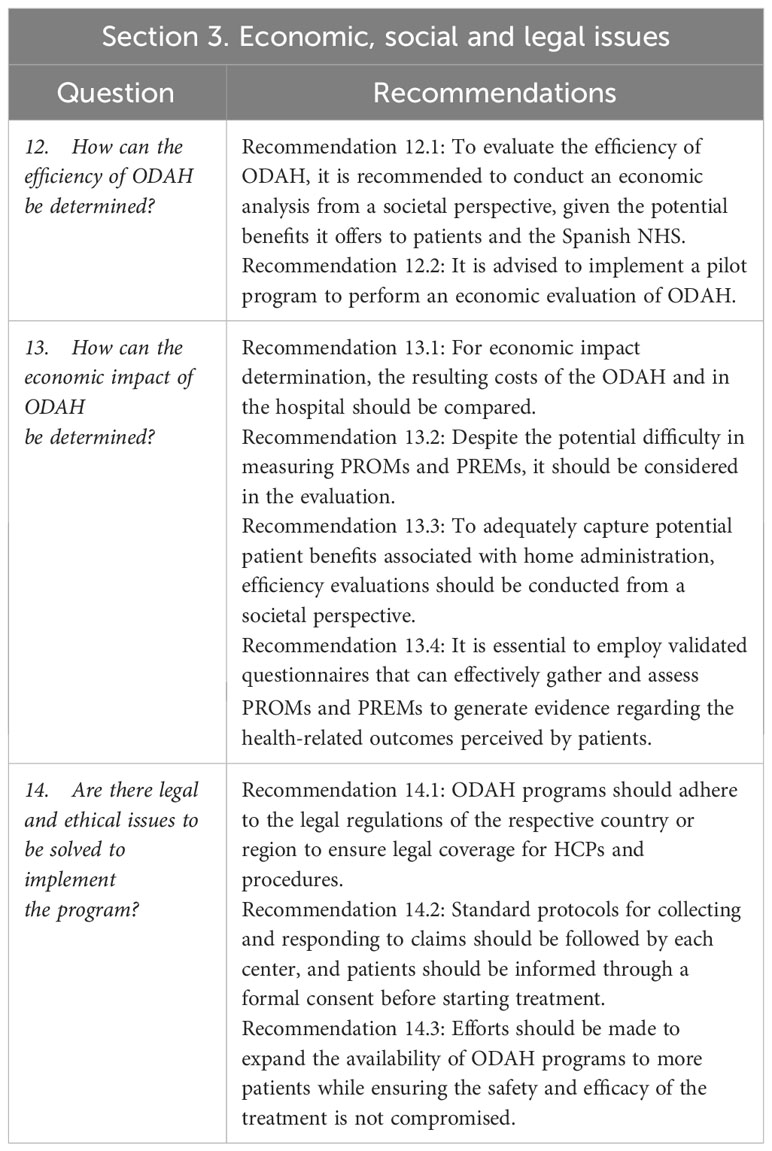
Table 7 Expert recommendations for economic, social and legal issues.
Home-based chemotherapy initiatives have emerged as a viable and safe alternative to traditional hospital treatment for oncology patients. These programs offer several advantages over traditional hospital-based treatment, including increased patient comfort and convenience, improved control of high-risk situations, and reduced costs and hospital overload. While most programs currently operate in urban environments where a high concentration of patients can be found, we believe that this strategy can also be successfully employed in areas with dispersed populations, as long as the travel time does not exceed 30-45 minutes. Furthermore, by providing patient-centered care and reducing the psychological and emotional burden of treatment, ODAH programs have the potential to significantly improve the quality of life of patients with cancer.
To support the development and implementation of these programs, a multidisciplinary group of experts have developed a list of recommendations based on the published literature and the collective expertise of the group aiming to serve as a foundation for the development of future initiatives.
Overall, ODAHs have the potential to revolutionize the way in which oncology patients receive treatment. By providing safe, effective, and patient-centered care, these programs can help to improve the overall experience of cancer treatment for patients and reduce the burden on healthcare systems. Also, an adequate financial investment and the training of specialized teams would be critical. It is therefore important that healthcare providers, policy makers, and other stakeholders work together to support the development and implementation of these programs to improve the quality of life for patients with cancer.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
EV: Conceptualization, Methodology, Validation, Writing – review & editing. MA: Conceptualization, Methodology, Validation, Writing – review & editing. MC: Conceptualization, Methodology, Validation, Writing – review & editing. SG: Conceptualization, Methodology, Validation, Writing – review & editing. MEM-M: Conceptualization, Methodology, Validation, Writing – review & editing. MP: Conceptualization, Methodology, Validation, Writing – review & editing. AT: Conceptualization, Methodology, Validation, Writing – review & editing. YS: Conceptualization, Methodology, Validation, Writing – review & editing. MS: Conceptualization, Methodology, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
Authors would like to thank Meisys for the assistance, whose service has been founded by Eisai Pharmaceuticals S.A.
Authors MA and MC were employed by the company Pharmacoeconomics & Outcomes Research Iberia (PORIB). Author YS was employed by the company Eisai Farmaceutica S.A. All authors have received honoraria from Eisai Pharmaceuticals S.A.
The authors declare that this study received funding from Eisai Farmaceutica, S.A. The funder had the following involvement in the study: responsible for contacting the project coordinator, setting the project goals, and developing the initial work plan. It was also in charge of gathering information from different sources about professional experts that could be invited to join in and, along with the project coordinator, invite them. Eisai provided the logistic support for the meetings (all via teleconference), selected the medical writing agency and the funding for the professional participants fees and external medical writer honorarium. Two members of the local Oncology Medical Affairs Department attended to the expert discussion meetings as observers, but they have not righted to review or modify the manuscript and the final consensus document.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1335344/full#supplementary-material
1. Sawada NO, Nicolussi AC, de Paula JM, Garcia-Caro MP, Marti-Garcia C, Cruz-Quintana F. Quality of life of Brazilian and Spanish cancer patients undergoing chemotherapy: an integrative literature review. Rev Lat Am Enfermagem (2016) 24:e2688. doi: 10.1590/1518-8345.0564.2688
2. Meneguin S, Matos TDS, Ferreira M. Perception of cancer patients in palliative care about quality of life. Rev Bras Enferm (2018) 71(4):1998–2004. doi: 10.1590/0034-7167-2017-0360
3. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
4. Red Española de Registros de Cáncer (REDECAN.Estimaciones de la incidencia del cáncer en España (2022). Available at: https://redecan.org/storage/documents/873877e1-af1b-43fe-8d97-0ee1434fe261.pdf (Accessed October 2022).
5. Alkatout I, Biebl M, Momenimovahed Z, Giovannucci E, Hadavandsiri F, Salehiniya H, et al. Has COVID-19 affected cancer screening programs? A systematic review. Front Oncol (2021) 11:675038 From NLM. doi: 10.3389/fonc.2021.675038
6. Di Cosimo S, Susca N, Apolone G, Silvestris N, Racanelli V. The worldwide impact of COVID-19 on cancer care: A meta-analysis of surveys published after the first wave of the pandemic. Front Oncol (2022) 12:961380 From NLM. doi: 10.3389/fonc.2022.961380
7. Riera R, Bagattini  M, Pacheco RL, Pachito DV, Roitberg F, Ilbawi A. Delays and disruptions in cancer health care due to COVID-19 pandemic: systematic review. JCO Glob Oncol (2021) 7:311–23. doi: 10.1200/go.20.00639
8. Leff B, Burton L, Mader SL, Naughton B, Burl J, Inouye SK, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med (2005) 143(11):798–808. doi: 10.7326/0003-4819-143-11-200512060-00008
9. Conley J, O'Brien CW, Leff BA, Bolen S, Zulman D. Alternative strategies to inpatient hospitalization for acute medical conditions: A systematic review. JAMA Intern Med (2016) 176(11):1693–702. doi: 10.1001/jamainternmed.2016.5974
10. Sanguinetti JM, Martinez D, Dimase F, Streich G, Castro P, Vega V, et al. Patient safety and satisfaction in home chemotherapy. Home Healthc Now (2021) 39(3):139–44. doi: 10.1097/NHH.0000000000000958
11. Murthy V, Wilson J, Suhr J, James L, Tombs H, Shereef E, et al. Moving cancer care closer to home: a single-centre experience of home chemotherapy administration for patients with myelodysplastic syndrome. ESMO Open (2019) 4(2):e000434. doi: 10.1136/esmoopen-2018-000434
12. Cool L, Vandijck D, Debruyne P, Desmedt M, Lefebvre T, Lycke M, et al. Organization, quality and cost of oncological home-hospitalization: A systematic review. Crit Rev Oncol Hematol (2018) 126:145–53. doi: 10.1016/j.critrevonc.2018.03.011
13. De Zen L, Del Rizzo I, Ronfani L, Barbieri F, Rabusin M, Dall'Amico R, et al. Safety and family satisfaction of a home-delivered chemotherapy program for children with cancer. Ital J Pediatr (2021) 47(1):43. doi: 10.1186/s13052-021-00993-x
14. Sandman KE, Bell TJ. Patient-Focused Benefits of at-Home Versus in-Clinic Administration of Cancer Therapy: New Considerations for the COVID-19 Era. Blood (2020) 136:35–6. doi: 10.1182/blood-2020-137560
15. Evans JM, Qiu M, MacKinnon M, Green E, Peterson K, Kaizer LA. multi-method review of home-based chemotherapy. Eur J Cancer Care (Engl) (2016) 25(5):883–902. doi: 10.1111/ecc.12408
16. Corbett M, Heirs M, Rose M, Smith A, Stirk L, Richardson G, et al. The delivery of chemotherapy at home: an evidence synthesis. Southampton (UK: NIHR Journals Library (2015). doi: 10.3310/hsdr03140
17. American society of clinical oncology (ASCO) position statement home infusion of anticancer therapy. (2020). Available at: https://old-prod.asco.org/sites/new-www.asco.org/files/content-files/advocacy-and-policy/documents/2020_Home-Infusion-Position-Statement.pdf (Accessed January 2023).
18. Burns V, Misra V, Paton N. Systemic anti-cancer therapy delivery in the home: a service model. Br J Nurs (2020) 29(10):S22–9. doi: 10.12968/bjon.2020.29.10.S22
19. Swinden J, Barton S, Peron JMR, Nabhani-Gebara S. Improving drug stability to promote home cancer therapy. (2014). Available at: https://hospitalpharmacyeurope.com/news/editors-pick/improving-drug-stability-to-promote-home-cancer-therapy/ (Accessed January 2023).
20. Vokes EE, Schilsky RL, Choi KE, Magid DM, Guarnieri CM, Whaling SM, et al. A randomized study of inpatient versus outpatient continuous infusion chemotherapy for patients with locally advanced head and neck cancer. Cancer (1989) 63(1):30–6. doi: 10.1002/1097-0142(19890101)63:1<30::aid-cncr2820630105>3.0.co;2-m
21. Cox K, Visintin L, Kovac S, Childs A, Kelleher H, Murray B, et al. Establishing a programme for continuous ambulatory infusion chemotherapy. Aust N Z J Med (1997) 27(6):680–4. doi: 10.1111/j.1445-5994.1997.tb00998.x
22. Rischin D, White MA, Matthews JP, Toner GC, Watty K, Sulkowski AJ, et al. A randomised crossover trial of chemotherapy in the home: patient preferences and cost analysis. Med J Aust (2000) 173(3):125–7. doi: 10.5694/j.1326-5377.2000.tb125563.x
23. Cool L, Missiaen J, Vandijck D, Lefebvre T, Lycke M, De Jonghe PJ, et al. An observational pilot study to evaluate the feasibility and quality of oncological home-hospitalization. Eur J Oncol Nurs (2019) 40:44–52. doi: 10.1016/j.ejon.2019.03.003
24. Borras JM, Sanchez-Hernandez A, Navarro M, Martinez M, Mendez E, Ponton JL, et al. Compliance, satisfaction, and quality of life of patients with colorectal cancer receiving home chemotherapy or outpatient treatment: a randomised controlled trial. BMJ (2001) 322(7290):826. doi: 10.1136/bmj.322.7290.826
25. Álvarez-Velásquez S, Sanz-Valero J. Home chemotherapy advantages in adult neoplasia sufferers: a systematic review. Hosp Domicilio (2020) 4(1):24–41. doi: 10.22585/hospdomic.v4i1.98
26. Corrie PG, Moody AM, Armstrong G, Nolasco S, Lao-Sirieix SH, Bavister L, et al. Is community treatment best? a randomised trial comparing delivery of cancer treatment in the hospital, home and GP surgery. Br J Cancer (2013) 109(6):1549–55. doi: 10.1038/bjc.2013.414
27. (ESMO), E. S. f. M. O. ESMO Standard Operating Procedures (SOPs) for Consensus Conference (CC) recommendations . Available at: https://www.esmo.org/content/download/77792/1426729/1/ESMO-ConsensusConference-SOPs.pdf (Accessed October 2022).
28. Neuss MN, Gilmore TR, Belderson KM, Billett AL, Conti-Kalchik T, Harvet BE, et al. 2016 Updated American society of clinical oncology/Oncology nursing society chemotherapy administration safety standards, including standards for pediatric oncology. Oncol Nurs Forum (2017) 44(1):31–43. doi: 10.1188/17.ONF.31-43
29. Jacobson JO, Polovich M, Gilmore TR, Schulmeister L, Esper P, Lefebvre KB, et al. Revisions to the 2009 american society of clinical oncology/oncology nursing society chemotherapy administration safety standards: expanding the scope to include inpatient settings. J Oncol Pract (2012) 8(1):2–6. doi: 10.1200/JOP.2011.000339
30. Ewen BM, Combs R, Popelas C, Faraone GM. Chemotherapy in home care: one team's performance improvement journey toward reducing medication errors. Home Healthc Nurse (2012) 30(1):28–37. doi: 10.1097/NHH.0b013e318233a75e
31. Nabhani-Gebara S, Salma D. Delivering chemotherapy at home: how much do we know? Br J Community Nurs (2019) 24(10):482–4. doi: 10.12968/bjcn.2019.24.10.482
32. Olsen M, LeFebvre K, Brassil K. Chemotherapy and immunotherapy guidelines and recommendations for practice. Oncol Nurs Soc (2019).
33. Tralongo P, Ferrau F, Borsellino N, Verderame F, Caruso M, Giuffrida D, et al. Cancer patient-centered home care: a new model for health care in oncology. Ther Clin Risk Manag (2011) 7:387–92. doi: 10.2147/TCRM.S22119
34. Casteli CPM, Mbemba GIC, Dumont S, Dallaire C, Juneau L, Martin E, et al. Indicators of home-based hospitalization model and strategies for its implementation: a systematic review of reviews. Syst Rev (2020) 9(1):172. doi: 10.1186/s13643-020-01423-5
35. Sweeney L, Halpert A, Waranoff J. Patient-centered management of complex patients can reduce costs without shortening life. Am J Manag Care (2007) 13(2):84–92.
36. Lassalle A, Thomare P, Fronteau C, Mahe B, Jube C, Blin N, et al. Home administration of bortezomib in multiple myeloma is cost-effective and is preferred by patients compared with hospital administration: results of a prospective single-center study. Ann Oncol (2016) 27(2):314–8. doi: 10.1093/annonc/mdv563
37. Touati M, Lamarsalle L, Moreau S, Vergnenegre F, Lefort S, Brillat C, et al. Cost savings of home bortezomib injection in patients with multiple myeloma treated by a combination care in Outpatient Hospital and Hospital care at Home. Support Care Cancer (2016) 24(12):5007–14. doi: 10.1007/s00520-016-3363-3
38. Polinski JM, Kowal MK, Gagnon M, Brennan TA, Shrank WH. Home infusion: Safe, clinically effective, patient preferred, and cost saving. Healthc (Amst) (2017) 5(1-2):68–80. doi: 10.1016/j.hjdsi.2016.04.004
39. Sharma D, Wojtynek J, Fox KM, Cooper C, Dokubo I. Cost of home vs clinic administration of paclitaxel in metastatic breast cancer. Am J Manag Care (2021) 27(2 Spec. No.):SP46–50. doi: 10.37765/ajmc.2021.88563
40. Kulthanachairojana N, Chansriwong P, Thokanit NS, Sirilerttrakul S, Wannakansophon N, Taychakhoonavudh S. Home-based chemotherapy for stage III colon cancer patients in Thailand: Cost-utility and budget impact analyses. Cancer Med (2021) 10(3):1027–33. doi: 10.1002/cam4.3690
41. Servei Català de la Salut [CatSalut]. Guía y recomendaciones para la realización y presentación de evaluaciones económicas y análisis de impacto presupuestario de medicamentos en el ámbito del CatSalut. Available at: https://catsalut.gencat.cat/web/.content/minisite/catsalut/proveidors_professionals/medicaments_farmacia/farmaeconomica/caeip/gaeip_publica_castellano_octubre2014_catsalut.pdf (Accessed March 2023).
42. Prieto L, Sacristán JA, Pinto JL, Badia X, Antoñanzas F, del Llano J. Análisis de costes y resultados en la evaluación económica de las intervenciones sanitarias. Evaluación económica para clínicos (2004) 122(11):423–9. doi: 10.1016/S0025-7753(04)74260-8
43. Brosa M, Gisbert R, Rodríguez JM, Soto J. Principios, métodos y aplicaciones del análisis del impacto presupuestario en el sector sanitario. Pharmacoecon. Span. Res Artic (2005) 2:65–78. doi: 10.1007/BF03320900
44. Sullivan SD, Mauskopf JA, Augustovski F, Jaime Caro J, Lee KM, Minchin M, et al. Budget impact analysis-principles of good practice: report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health (2014) 17(1):5–14. doi: 10.1016/j.jval.2013.08.2291
45. Comisión de Salud Pública (Consejo Interterritorial del Sistema Nacional de Salud). Protocolo de Vigilancia Sanitaria Específica para los trabajadores expuestos a Agentes Citostáticos (2003). Available at: https://www.sanidad.gob.es/ciudadanos/saludAmbLaboral/docs/Agentescitostaticos.pdf (Accessed 2023).
Keywords: oncology, home administration, expert recommendations, quality of life, oncology therapies
Citation: Villegas E, Arruñada M, Casado MÁ, González S, Moreno-Martínez ME, Peñuelas MÁ, Torres AM, Sierra Y and Seguí MA (2024) National expert consensus on home-administered oncologic therapies in Spain. Front. Oncol. 14:1335344. doi: 10.3389/fonc.2024.1335344
Received: 11 December 2023; Accepted: 12 January 2024;
Published: 16 February 2024.
Edited by:
Alma D. Campos-Parra, Universidad Veracruzana, MexicoReviewed by:
Giovanni Rosti, San Matteo Hospital Foundation (IRCCS), ItalyCopyright © 2024 Villegas, Arruñada, Casado, González, Moreno-Martínez, Peñuelas, Torres, Sierra and Seguí. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel Angel Seguí, bWFzZWd1aUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.