
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 30 January 2024
Sec. Gynecological Oncology
Volume 14 - 2024 | https://doi.org/10.3389/fonc.2024.1331903
This article is part of the Research Topic Advances toward improved understanding and treatment of uncommon ovarian cancer types and subtypes View all 18 articles
 Christina H. Wei1Oluwole Fadare2*
Christina H. Wei1Oluwole Fadare2*Steroid cell tumors (SCT) of the ovary are rare, which has limited advances in the understanding of this enigmatic neoplasm. In this review, we summarize currently known clinicopathologic information on SCT. SCT are frequently hormonally active, leading to elevated serum and/or urine levels of androgenic hormones or their metabolites, and associated symptomatology, including virilization. The reported age at diagnosis is broad and has ranged from as young as 1 year old to 93 years old, although most patients were between ages 20 and 40 years. Most tumors are stage I and unilateral. The tumors are usually well circumscribed with a solid or solid to cystic cut surface. The tumors in one series reportedly ranged in size from 1.2 to 45 cm (average 8.4 cm). MRI is a useful imaging modality, typically showing a well delineated mass with contrast enhancement and lipid content on T2 and T1 weighted images, respectively. Microscopically, SCT display polygonal to epithelioid cells with abundant eosinophilic to vacuolated/clear cytoplasm and display an immunoprofile that is consistent with sex cord-stromal differentiation. Most cases are benign, without any recurrences after primary resection, but a subset – probably less than 20% of cases –are clinically malignant. Pathologic criteria that can specifically predict patient outcomes remain elusive, although features that correlate with adverse outcomes have been proposed based on retrospective studies. The molecular characteristics of SCTs are similarly under characterized, although there is some evidence of an enrichment for hypoxia-signaling gene mutations in SCT. In malignant SCT, the tumors generally show greater global genomic instability, copy number gains in oncogenes, and occasional BAP1 mutation. Future studies involving multi-institutional cohort and unbiased molecular profiling using whole exome/transcriptome sequencing are needed to help advance our molecular understanding of SCTs.
In the 5th edition of the World Health Organization (WHO) classification of female genital tumors, steroid cell tumor (SCT) is defined as “an ovarian parenchymal tumor comprised of steroid cells.” (1) This simple definition is a reflection of the current understanding of this rare and enigmatic neoplasm. Historically, it has long been recognized that a subset of ovarian tumors that are associated with virilization are exclusively comprised of cells that closely resemble steroid hormone secreting cells, including the adrenocortical cortical cells, Leydig cells, and lutein cells (2). For several decades, different authors applied a variety of terms to these lesions, including androblastoma diffusum, arrhenoblastoma, Leydig cell tumor, adrenal or adrenocortical tumor, adrenal rest tumor, adrenal-like tumor, stromal luteoma, lipoid or lipid cell tumor, virilizing or masculinizing lipoid/lipid cell tumor, ovoblastoma, masculinovoblastoma, sympatheticotropic tumor, hilus cell tumor, and hypernephroma/hypernephroid tumor (2–7). The 1st edition of the WHO classification of ovarian tumors (1973) included Leydig cell tumors and lipoid cell (or lipid cell) tumors as separate entities, with the latter defined as a tumor comprised of one of the aforementioned steroid hormone secreting cells, but which “cannot be identified specifically as any one of the three types.” (6) Given that many neoplasms of this class are comprised of tumor cells that contain no significant amounts of intracytoplasmic lipid, the term “lipoid or lipid cell tumor” was not ideal, and ultimately led to its replacement by “Steroid cell tumor”, a term that was initially proposed by Dr. Robert E Scully in 1979 (8) as a better descriptor for the group of tumors that included stromal luteoma (9), Leydig cell tumor (10) and tumors in this class that could not be classified as either of these 2 entities - steroid cell tumor not otherwise specified (SCT NOS) (11). These 3 entities were thought to comprise 20%, 20% and 60% of steroid cell tumors respectively. A Leydig cell tumor is a benign, typically androgen producing tumor that is usually confined to the ovarian hilum and which commonly shows cytoplasmic Reinke crystals (1, 6). Stromal luteomas were initially conceptualized as benign, small, ovarian cortex-confined neoplasms that were mostly seen in postmenopausal patients (11, 12). Patients most frequently presented with abnormal vaginal bleeding that was probably attributable to hyperestrogenism (11, 12). Although stromal luteomas were thought to display distinctive clinicopathologic features (13, 14), starting with the 4th edition of the WHO classification of ovarian tumors (2014), stromal luteoma ceased to be recognized as a distinct entity (15). Tumors that were previously classified as stroma luteoma and SCT NOS were both subsumed under the SCT (15), and the latter has remained the preferred terminology for this tumor (1). SCTs are rare, with fewer than a thousand cases reported in the literature to date. This rarity has limited advances in the understanding of this enigmatic neoplasm. In this review, we summarize currently known clinicopathologic information on SCT.
SCT are frequently hormonally active, leading to elevated serum and/or levels of androgenic hormones and their metabolites (11, 16, 17). In a subset of cases, ovarian SCT can induce ACTH secretion, leading to co-presentation of Cushing syndrome (18–21). Symptomatology is often related to androgenic excess, including virilization, hirsutism, balding, deepening of voice, acne, and clitoromegaly (11, 16). Overall, the most common initial manifestation in one series was virilization (41%), although 6.3% had estrogenic manifestations. In additional to symptoms related to androgen excess, there are age group-specific presentations. For example, in pediatric population, children may show isosexual precocious puberty (22). In child-bearing age group, women present with irregular menstrual cycles or infertility (23). In post-menopausal women, vaginal bleeding may occur (24, 25). In most cases, SCTs present as an unilateral ovarian tumor (11). However, it has been estimated that 6% of patients present with bilateral ovarian SCTs (11, 26). A subset of SCTs are malignant (11, 27)., and malignant SCTs has been reported in females as young as 4 years old (28). Malignant SCT presents with extra-ovarian disease, often involving the retroperitoneum, mesentery, omentum, and other intraabdominal organs such as colon (29). Distant metastasis includes the vertebral bone and brain (30). A rare case of malignant ascites from peritoneal dissemination has also been reported (31).
The age at diagnosis is broad, ranging from as young as 1 year old to 93 years old, but generally between 20s-40s. In one series (11), the average age was 43 years (range 2.5-80 years), and in one review of the literature, the median age was 33.5 years (range 3-93) (16). Accordingly, a significant number of ovarian SCT occurs in the pediatric population, wherein the tumors may initially be misdiagnosed with congenital adrenal hyperplasia, which may exhibit similar clinical symptomatology (32, 33). Along the same vein, women of reproductive age with ovarian SCT may be misdiagnosed with polycystic ovarian syndrome (PCOS) - a much more common hormonal disorder in this age group (34). Another critical point to underscore is that while the majority of the cases present with a unilateral ovarian mass (size ranging from 1.2-45 cm), smaller lesions may be missed by modern imaging techniques such as MRI, leading to underdiagnosis of ovarian SCT (35). Indeed, an integrative clinical, radiologic, and biochemical workup is necessary to achieve optimal screening. On rare occasion, for diagnostically occult cases, therapeutic oophorectomies has been performed to exclude the possibility of ovarian SCT (36). In general, MRI has the most specificity for a SCT, which typically demonstrates a well-defined solid mass. Key characteristics include contrast enhancement on T2-weighted image (37), and demonstration of lipid content on T1-weighted image with signal drop between pre-contrast T1-weighted opposed phase and T- weighted in phase images (38). On balance, clinical presentation of virilization, increased serum testosterone level, and presence of a lipid-containing ovarian mass on MRI should raise the differential diagnosis of an ovarian SCT.
Ovarian SCT can occur in patients with germline mutations in FH, VHL, and APC genes. The most frequently reported cancer predisposition syndrome associated with ovarian SCT is VHL. There are 5 reported cases of SCT arising in VHL patients in the literature, four are unilateral on presentation and one is bilateral (39, 40). The onset age ranged from 16 to 46 years old (39). There is only one case report of a patient with germline FH mutation. This patient presented with asynchronous bilateral ovarian SCT, initially at age of 22 (left ovary, 2 cm), and later at 31 years old (right ovary, 6.3 cm) (41). There is also one case report of a benign, unilateral ovarian SCT in a 47-year-old woman with familial adenomatous polyposis syndrome (42).
In one series of 63 cases, 51, 4,7 and 1 case(s) were stage I, II, III, and IV respectively (11). 94% were unilateral and 6% bilateral (11). The tumors reportedly ranged in size from 1.2 to 45 cm (average 8.4 cm); 65% were described as well circumscribed and a smaller subset as encapsulated (11). Most were described as having a solid cut surface, with smaller subsets being solid to cystic or entirely cystic (11). The tumoral cut surfaces were mostly yellow, or in a minority of cases, brown, tan or gray white (11). Calcifications, hemorrhage or necrosis may be grossly observed. Microscopically, SCT comprises a proliferation of polygonal to epithelioid cells with abundant eosinophilic to vacuolated/clear cytoplasm (Figure 1). The nuclear and nucleolar size may vary from case to case or within a given case, as may the level of nuclear pleomorphism. The cells are arranged in sheet-like to nested patterns, separated by a delicate vascular network. Most cases have a low mitotic index, but this may vary as well. Necrosis, lymphovascular invasion, zones of hypercellularity, stromal hyalinization, lipid droplets, vague spindling and/or hemorrhage may be seen. Significantly, no Reinke crystals are present (a defining feature of Ledyig cell tumor). The immunoprofile of SCT is consistent with sex cord-stromal differentiation, with >80% expressing inhibin-A, SF1 and calretinin (41,42). A subset of SCT variably (30-70%) demonstrate positivity for CD99, androgen receptor, Melan A, estrogen receptor, progesterone receptor, SMA, CD10 and pancytokeratins (41,42,43). SCT do not express WT1 or epithelial membrane antigen (43).
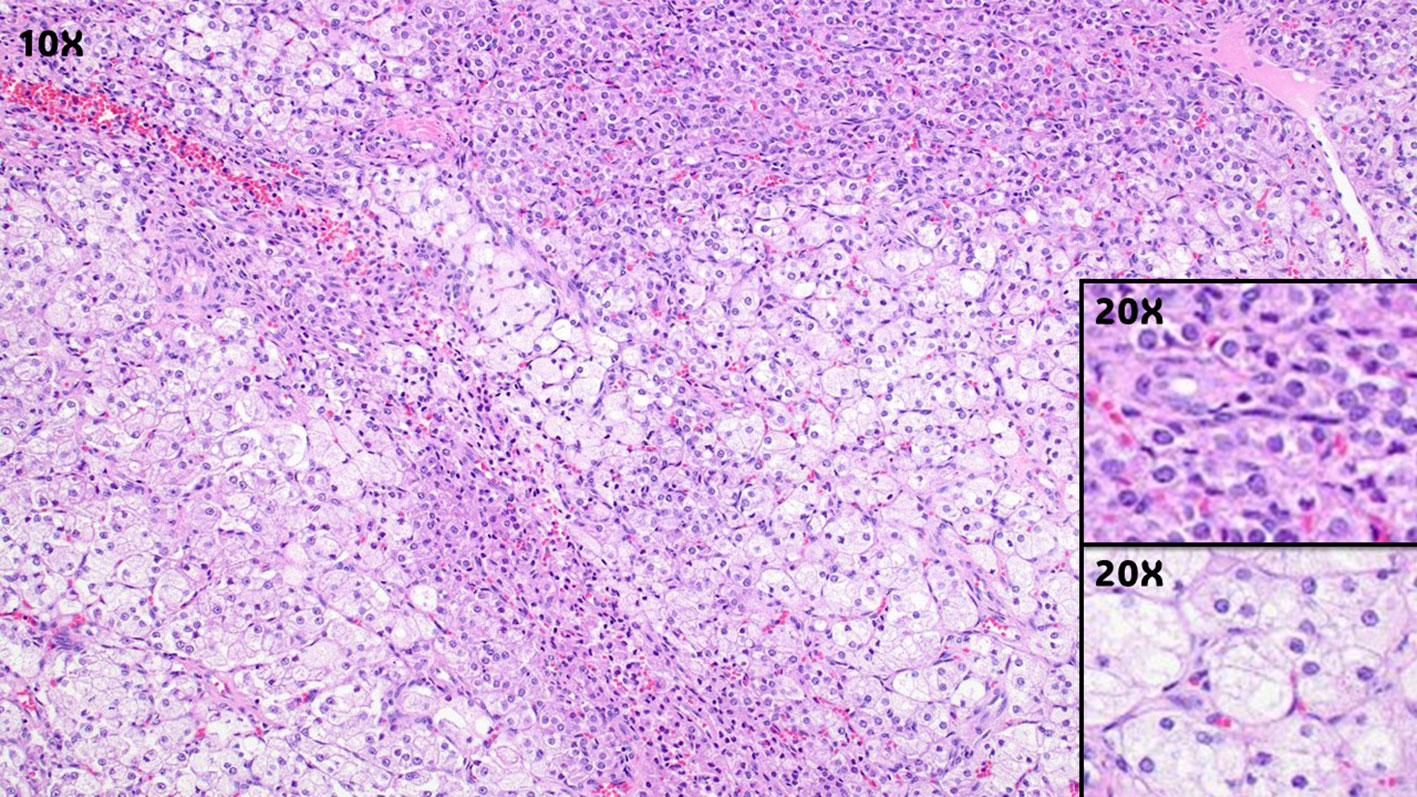
Figure 1 Ovarian steroid cell tumor, showing solid sheets of epithelioid to polygonal cell with eosinophilic to clear cytoplasm (Magnification, 10X). The insets show higher magnification of the tumor cells with eosinophilic cytoplasm (top inset, magnification 20X), or clear/vacuolated cytoplasm (lower inset, magnificent 20X).
Three molecular studies have been reported on SCT (27, 43, 44). One of aforementioned studies included a “metastatic” ovarian Leydig cell tumor, which likely present a steroid cell tumor (44). Overall, there appear to be few, if any, pathognomonic recurrent mutations for SCT. This contrasts with other types of ovarian sex cord stromal tumors, such as Sertoli-Leydig cell tumor, Sertoli cell tumor of pure-type, sex cord-stromal tumors with annular tubules (SCTAT), adult granulosa cell tumor (AGCT), and juvenile granulosa cell tumor (JGCT). In one series, 60% of the Sertoli-Leydig cell tumors was found to have DICER1 mutation, and some occurred in the setting of germline DICER1 mutation (45). A subset of SCTAT and pure-type Sertoli cell tumor cases arise in association with germline STK11 mutation that causes Peutz-Jegher syndrome (46). Interestingly, SCTAT occurring in context of syndromic germline STK11 mutation have improved outcomes compared to sporadic/non-syndromic patients (47). Over 95% of AGCT demonstrates recurrent somatic FOXL2 mutation (48). JGCT may occur in the setting of Ollier disease and Maffucci syndrome, or somatic mosaic mutations in IDH1 and IDH2, and somatic copy number changes in AKT (45).
In ovarian SCT, a more heterogeneous profile of genetic mutations has been reported, including BAP1, FH, TP53, CTNNB1, CASP10, HIF1A, SRC, FOXO4, HOXA13, LHCGR, VHL, IDH2, SDHB, and BRCA2 (27, 43, 44). Most are missense mutations, except for BAP1 and FOXO4, which are frameshift mutations (27, 43), and SRC, which is an in-frame deletion (43). In one of the studies, enrichment of hypoxia-associated gene mutation (HIF1A, VHL, SDHB, SRC, IDH2, and FOXO4) was observed in a retrospective case series of 5 benign and 2 malignant SCT patients (43). Interestingly, SCT has been reported in patients with germline mutation in VHL (39), suggesting a correlation between hypoxia signaling pathway in the tumorigenesis of SCT. Wnt signaling pathway is another implicated pathway dysregulated in SCT, since somatic CTNNB1 mutation and biallelic APC loss molecular events have been reported in SCT (27, 42).
For malignant SCTs, we found a total of six malignant SCT with molecular information, reported by three independent studies (27, 43, 44). The molecular findings are not entirely consistent between series. However, two general observations were seen. First, malignant SCTs exhibited more global genomic instability by copy number analysis. This is supported by the identification of copy number gain in MDM2 and CDK2 genes, ATRX rearrangement, and copy number amplification in NPM1, DCM1, and SS18 genes (27, 44). However, it is important to note that these genes are sporadically reported and are not consistently found in all malignant SCT cases. More likely, these identified amplification and structural rearrangement events are passenger events secondary to global genomic instability. Second, BAP1 mutation was found in two of the six malignant SCT cases sequenced to date, reported independently by two groups (27, 44). The mutation genotypes for BAP1 were p.K453fs and p.S126Rfs*61 (personal communications with Dr. Vranic and Dr. Bennett). Interestingly, BAP1 mutation has not been reported in benign SCTs to date. Other mutations found in malignant SCTs included HIF1A and SDHB (44).
Although the data is limited, other possibly negative molecular findings include: (1) The type of gene mutations does not appear to be correlated with the number of adverse histologic risk factors (27), and (2) Microsatellite instability was not identified in any tested sample, suggesting that SCTs are likely not hyper-mutated tumors (43, 44).
On balance, the malignant cases are genetically more unstable, characterized by global chromosomal number aberration, with occasional BAP1 mutation. However, readers are cautioned to avoid overgeneralizing these findings due to the small sample size. The genomic profile of benign and malignant SCTs is still relatively under-characterized, secondary to limited samples of this rare tumor type, and the selective use of cancer gene panel assays to profile their genomic makeup in the published studies (27, 43). Indeed, some noncancer-related genes, such as metabolic or hormonal-related genes, may be important for the development or prognostication of SCTs. Future studies with larger sample size, and the use of more advanced, unbiased molecular techniques, such as whole exome and transcriptome molecular profiling, will ultimately provide a more comprehensive molecular profile of SCT.
We found one functional molecular study of SCT in the literature (49). Using telomerase repeat amplification protocol (TRAP) assay, this study showed intact telomerase activity in a malignant SCT. In a retrospective series of sex cord-stomal ovarian tumors, Dowdy et al. demonstrated that telomerase activity has a 94% specificity for malignancy. In the same study, none of the benign sex cord-cord-stomal ovarian tumors showed telomerase activity. The prognostic significance of telomerase activity in SCT, particularly in distinguishing benignity from malignancy warrants further investigation (46).
Most reported cases of SCT have been clinically benign without recurrences or death from disease following the primary resection of the tumor (11,16). In a recent review of the literature, Lin et al. found post-resection disease recurrence or progression occurred in 17.86% of cases, with a median tumor-free interval of 23 months (16). The authors noted that recurrences seemed to be associated with patient age, with a recurrence rate of 11.43% for patients aged 40 years or younger, and 28.57% for those older than 40 years, and no patients younger than 20 years of age reported with recurrence or progression. In the series of Mendoza et al, approximately 14% of cases were malignant (27). In the series of Hayes and Scully, most of which were consultation or referral cases, approximately one third of cases were clinically malignant (11). Overall, our impression is that the malignancy rate is probably less than 20%. The authors noted that the best pathological correlates of malignant behavior were: the presence of two or more mitotic figures per 10 high power fields (92% malignant); necrosis (86% malignant); a diameter of 7 cm or greater (78% malignant); hemorrhage (77% malignant); and grade 2 or 3 nuclear atypia (64% malignant) (11). In one case series, although all malignant SCTs demonstrated at least 4 atypical features, at least one atypical feature was present in benign cases as well (27). Thus, pathologic features that are specifically predictive of behavior have not been conclusively defined, although the data suggests that there may be features that correlative with adverse outcomes. A combination of pathogenomic classification may improve our ability to classify the prognosis of SCTs with atypical features.
In malignant cases, patients may either present with advanced extra-ovarian disease or recur after surgery. The disease recurrence timeline is variable and can recur within months or as long as 17 years after initial diagnosis and surgery, even in stage IA cases (27, 43). Metastatic SCT typically presents with intra-abdominal and retroperitoneal metastases, and on rare occasions, ascites. The clinical course for malignant SCTs are generally guarded, and most succumb to the disease 6-44 months following the diagnosis (11, 16, 27, 29, 30). However, as previously noted, recurrences may occur many years after primary resection. SCTs are generally insensitive to chemotherapy (29, 50). Rare case reports of disease control with a GnRH agonist have been reported (51, 52). In benign cases, the serum testosterone level generally normalizes within days or weeks following surgical resection of SCT (16). Successful pregnancy is achievable following surgery, usually within 1 year of tumor removal (53, 54). Virilization and hirsutism are usually resolved within a year of surgical tumor removal. This underscores the importance of early detection and surgical management of SCT. However, to prevent overtreatment the readers are cautioned that increased use of prenatal ultrasound has led to increased detection of asymptomatic ovarian masses (55). Most adnexal masses detected during gestation are benign and functional (55). The most common sex cord stromal tumors detected during gestation are granulosa cell tumor (22%), thecoma (18.6%), and Sertoli-Leydig tumors (8.5%) (56). Fortunately, greater than 70% of sex cord stromal tumors found during pregnancy result in live births (56).
Ovarian SCT are rare, with fewer than a thousand cases reported in the literature to date. SCT patients frequently display evidence of androgenic excess, with elevation in plasma testosterone level. A subset of SCT occurs in patients with germline mutations in VHL, FH, and APC genes. While most SCT are benign, a small subset are malignant and recurrences may occur many years after primary resection of an apparently localized tumor. Pathologic criteria that can specifically predict patient outcomes remain elusive, although features that correlate with adverse outcomes have been proposed based on retrospective studies. The molecular characteristics of SCTs are still under characterized, due to rarity of this entity. However, a few key observations have been made, including an enrichment of hypoxia-signaling gene mutations. In malignant SCT, the tumors generally show greater global genomic instability, copy number gains in oncogenes, and occasional BAP1 mutation. Future studies involving multi-institutional cohort and unbiased molecular profiling using whole exome/transcriptome sequencing are needed to help advance our molecular understanding of SCTs.
CW: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. OF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. NCI-K12CA001727 (JM/CW); COH Circle1500 (CW).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. WHO Classification of Tumours Editorial Board. WHO Classification of Female genital tumors. 5th ed Vol. 4. . Lyon, France: World Health Organization (2020).
2. Brass P, King WB Jr., Krepp MW Jr. Lipoid-cell tumor of the ovary. Report of a case. Obstet Gynecol (1963) 21:201–5.
3. Taylor HB, Norris HJ. Lipid cell tumors of the ovary. Cancer (1967) 20(11):1953–62. doi: 10.1002/1097-0142(196711)20:11<1953::AID-CNCR2820201123>3.0.CO;2-2
5. Pedowitz P, Pomerance W. Adrenal-like tumors of the ovary. Review of the literature and report of two new cases. Obstet Gynecol (1962) 19:183–94.
6. Serov SF. S. R., in collaboration with L. H. Sobin and pathologists in ten countries, Histological typing of ovarian tumours. World Health Organ (1973).
7. Berger L. Tumeur des cellules sympathicotropes de l’ovaire avec virilisation. Un nouveau syndrome anatomo-clinique. Rev Canad Biol (1942) 1:539–66.
8. Scully RE. Tumors of the ovary and maldeveloped gonads. 16. ed. Washington DC: American registry of pathology. (1979) p. 215–20.
9. Scully RE. Stromal luteoma of the ovary. A distinctive type of lipoid-cell tumor. Cancer (1964) 17:769–78. doi: 10.1002/1097-0142(196406)17:6<769::AID-CNCR2820170612>3.0.CO;2-#
10. Paraskevas M, Scully RE. Hilus cell tumor of the ovary. A clinicopathological analysis of 12 Reinke crystal-positive and nine crystal-negative cases. Int J Gynecol Pathol (1989) 8(4):299–310. doi: 10.1097/00004347-198912000-00001
11. Hayes MC, Scully RE. Ovarian steroid cell tumors (not otherwise specified). A clinicopathological analysis of 63 cases. Am J Surg Pathol (1987) 11(11):835–45. doi: 10.1097/00000478-198711000-00002
12. Hayes MC, Scully RE. Stromal luteoma of the ovary: a clinicopathological analysis of 25 cases. Int J Gynecol Pathol (1987) 6(4):313–21. doi: 10.1097/00004347-198712000-00003
14. Tavassoli FA, Devilee P eds. Pathology and genetics of tumours of the breast and female genital organs, 3rd. ed Lyon: IARC. (2003).
15. Kurman RC, Carcangiu ML, Herrington CS, Young RH eds. WHO classification of tumours of the female reproductive organs, 4th ed Lyon: IARC. (2014).
16. Lin M, Bao K, Lu L, Xu S, Liang Y, Cheng X, et al. Ovarian steroid cell tumors, not otherwise specified: analysis of nine cases with a literature review. BMC Endocr Disord (2022) 22(1):265. doi: 10.1186/s12902-022-01170-9
17. Macut D, Ilic D, Mitrovic Jovanovic A, Bjekic-Macut J. Androgen-secreting ovarian tumors. Front Horm Res (2019) 53:100–7. doi: 10.1159/000494906
18. Young RH, Scully RE. Ovarian steroid cell tumors associated with Cushing’s syndrome: a report of three cases. Int J Gynecol Pathol (1987) 6(1):40–8. doi: 10.1097/00004347-198703000-00005
19. Chen S, Li R, Zhang X, Lu L, Li J, Pan H, et al. Combined ovarian and adrenal venous sampling in the localization of adrenocorticotropic hormone-independent ectopic cushing syndrome. J Clin Endocrinol Metab (2018) 103(3):803–8. doi: 10.1210/jc.2017-01977
20. Sawathiparnich P, Sitthinamsuwan P, Sanpakit K, Laohapensang M, Chuangsuwanich T. Cushing’s syndrome caused by an ACTH-producing ovarian steroid cell tumor, NOS, in a prepubertal girl. Endocrine (2009) 35(2):132–5. doi: 10.1007/s12020-009-9150-x
21. Sworczak K, Blaut K, Malecha M, Lewczuk A. Ectopic ACTH syndrome associated with ovarian steroid-cell tumor. J Endocrinol Invest (2002) 25(4):369–72. doi: 10.1007/BF03344020
22. Chu CH, Wang WD, Wang SY, Chao TK, Su RY, Lin CM. Ovarian steroid cell tumor causing isosexual pseudoprecocious puberty in a young girl: an instructive case and literature review. BMC Endocr Disord (2022) 22(1):41. doi: 10.1186/s12902-022-00956-1
23. Swain J, Sharma S, Prakash V, Agrawal NK, Singh SK. Steroid cell tumor: a rare cause of hirsutism in a female. Endocrinol Diabetes Metab Case Rep (2013) 2013:130030. doi: 10.1530/EDM-13-0030
24. Park YJ, Kim JH, Koh J. Hematometra due to cervical stenosis in a postmenopausal woman with incidental ovarian steroid cell tumor: A case report. J Menopausal Med (2022) 28(3):142–5. doi: 10.6118/jmm.22036
25. Wan J, Chen X, Li X. Ovarian steroid cell tumor, not otherwise specified: A rare case of postmenopausal vaginal bleeding. Oncol Lett (2014) 8(3):1187–9. doi: 10.3892/ol.2014.2251
26. Cooray SM, Bulugahapitiya UD, Samarasinghe K, Samarathunga P. Steroid cell tumor not otherwise specified of bilateral ovaries: A rare cause of post menopausal virilization. Indian J Endocrinol Metab (2013) 17(Suppl 1):S262–4. doi: 10.4103/2230-8210.119596
27. Mendoza RP, Wang P, Smith HL, Fitzpatrick CA, Haridas R, Wanjari P, et al. Clinicopathologic analysis and molecular profiling of ovarian steroid cell tumors. Am J Surg Pathol (2023) 47:1398–408. doi: 10.1097/PAS.0000000000002124
28. Yoshimatsu T, Nagai K, Miyawaki R, Moritani K, Ohkubo K, Kuwabara J, et al. Malignant ovarian steroid cell tumor, not otherwise specified, causes virilization in a 4-year-old girl: A case report and literature review. Case Rep Oncol (2020) 13(1):358–64. doi: 10.1159/000506044
29. Punneshetty S, Sebastian A, Thomas V, Daniel S, Briskala P, Singh A, et al. Malignant metastatic steroid cell tumor NOS: A rare presentation of a subtype of sex cord stromal tumor. Gynecol Oncol Rep (2023) 46:101169. doi: 10.1016/j.gore.2023.101169
30. Li K, Zhu F, Xiong J, Liu F. A rare occurrence of a Malignant ovarian steroid cell tumor not otherwise specified: A case report and literature review. Oncol Lett (2014) 8(2):770–4. doi: 10.3892/ol.2014.2233
31. Kosaka N, Hasegawa K, Kiuchi K, Ochiai S, Nagai T, Machida H, et al. Cytological findings of ascitic fluid with a Malignant ovarian steroid cell tumor: A case report and literature review. Acta Cytol (2017) 61(2):165–71. doi: 10.1159/000458750
32. Driano JE, Creo AL, Kumar S, Chattha AJ, Lteif AN. Ovarian steroid cell tumor masquerading as steroid-unresponsive congenital adrenal hyperplasia. AACE Clin Case Rep (2021) 7(4):261–3. doi: 10.1016/j.aace.2021.02.001
33. Yilmaz-Agladioglu S, Savas-Erdeve S, Boduroglu E, Onder A, Karaman I, Cetinkaya S, et al. A girl with steroid cell ovarian tumor misdiagnosed as non-classical congenital adrenal hyperplasia. Turk J Pediatr (2013) 55(4):443–6.
34. Wong FCK, Chan AZ, Wong WS, Kwan AHW, Law TSM, Chung JPW, et al. Hyperandrogenism, elevated 17-hydroxyprogesterone and its urinary metabolites in a young woman with ovarian steroid cell tumor, not otherwise specified: case report and review of the literature. Case Rep Endocrinol (2019) 2019:9237459. doi: 10.1155/2019/9237459
35. Sun M, Zhang B. Contrast-enhanced ultrasound of ovarian steroid cell tumor, not otherwise specified: A case report. Oncol Lett (2022) 24(4):370. doi: 10.3892/ol.2022.13490
36. Sood N, Desai K, Chindris AM, Lewis J, Dinh TA. Symptomatic ovarian steroid cell tumor not otherwise specified in a post-menopausal woman. Rare Tumors (2016) 8(2):6200. doi: 10.4081/rt.2016.6200
37. Wang PH, Chao HT, Lee RC, Lai CR, Lee WL, Kwok CF, et al. Steroid cell tumors of the ovary: clinical, ultrasonic, and MRI diagnosis–a case report. Eur J Radiol (1998) 26(3):269–73. doi: 10.1016/S0720-048X(96)01133-3
38. Morani AC, Mubarak AI, Bhosale HR, Ramani NS, Waguespack SG, Ying A. Steroid cell ovarian tumor in a case of von hippel-lindau disease: demonstrating lipid content of the mass with MR imaging. Magn Reson Med Sci (2019) 18(4):251–2. doi: 10.2463/mrms.ci.2018-0104
39. Marques A, Portugal R. Ovarian steroid cell tumor in an adolescent with von hippel-lindau syndrome: A case report and review of the literature. Int J Gynecol Pathol (2020) 39(5):473–7. doi: 10.1097/PGP.0000000000000628
40. Gong Y, Taraif S, Mazur I, Aneja A, Huang M, Somers DL, et al. Ovarian steroid cell tumor associated with von Hippel-Lindau syndrome: a report of two cases and literature review. Int J Clin Exp Pathol (2022) 15(8):332–7.
41. Arora R, Eble JN, Pierce HH, Crispen PL, DeSimone CP, Lee EY, et al. Bilateral ovarian steroid cell tumours and massive macronodular adrenocortical disease in a patient with hereditary leiomyomatosis and renal cell cancer syndrome. Pathology (2012) 44(4):360–3. doi: 10.1097/PAT.0b013e328353bf5a
42. Hu PJ, Knoepp SM, Wu R, Cho KR. Ovarian steroid cell tumor with biallelic adenomatous polyposis coli inactivation in a patient with familial adenomatous polyposis. Genes Chromosomes Cancer (2012) 51(3):283–9. doi: 10.1002/gcc.20953
43. Chao A, Huang HJ, Lin CY, Lee CH, Lin CH, Chao AS, et al. Hypoxia-associated genetic signature in ovarian steroid cell tumor NOS. Endocr Relat Cancer (2023) 30(11). doi: 10.1530/ERC-23-0179
44. Kruslin B, Gatalica Z, Hes O, Skenderi F, Miettinen M, Contreras E, et al. TERT gene fusions characterize a subset of metastatic leydig cell tumors. Clin Genitourin Cancer (2021) 19(4):333–8. doi: 10.1016/j.clgc.2021.02.002
45. Schultz KA, Harris AK, Schneider DT, Young RH, Brown J, Gershenson DM, et al. Ovarian sex cord-stromal tumors. J Oncol Pract (2016) 12(10):940–6. doi: 10.1200/JOP.2016.016261
46. Meserve EE, Nucci MR. Peutz-jeghers syndrome: pathobiology, pathologic manifestations, and suggestions for recommending genetic testing in pathology reports. Surg Pathol Clin (2016) 9(2):243–68. doi: 10.1016/j.path.2016.01.006
47. Young RH, Welch WR, Dickersin GR, Scully RE. Ovarian sex cord tumor with annular tubules: review of 74 cases including 27 with Peutz-Jeghers syndrome and four with adenoma Malignum of the cervix. Cancer (1982) 50(7):1384–402. doi: 10.1002/1097-0142(19821001)50:7<1384::AID-CNCR2820500726>3.0.CO;2-5
48. Shah SP, Kobel M, Senz J, Morin RD, Clarke BA, Wiegand KC, et al. Mutation of FOXL2 in granulosa-cell tumors of the ovary. N Engl J Med (2009) 360(26):2719–29. doi: 10.1056/NEJMoa0902542
49. Dowdy SC, O’Kane DJ, Keeney GL, Boyd J, Podratz KC. Telomerase activity in sex cord-stromal tumors of the ovary. Gynecol Oncol (2001) 82(2):257–60. doi: 10.1006/gyno.2001.6293
50. Vasilevska D, Rudaitis V, Vasilevska D, Mickys U, Wawrysiuk S, Semczuk A. Failure of multiple surgical procedures and adjuvant chemotherapy in early-stage steroid-cell ovarian tumor treatment: a case report and literature review. J Int Med Res (2021) 49(1):300060520983195. doi: 10.1177/0300060520983195
51. Wang PH, Chao HT, Lee WL. Use of a long-acting gonadotropin-releasing hormone agonist for treatment of steroid cell tumors of the ovary. Fertil Steril (1998) 69(2):353–5. doi: 10.1016/S0015-0282(97)00500-1
52. Nakasone T, Nakamoto T, Matsuzaki A, Nakagami H, Aoki Y. Direct evidence on the efficacy of GnRH agonist in recurrent steroid cell tumor-not otherwise specified. Gynecol Oncol Rep (2019) 29:73–5. doi: 10.1016/j.gore.2019.07.006
53. Matemanosak P, Peeyananjarassri K, Suwanrath C, Wattanakumtornkul S, Klangsin S, Thiangphak E, et al. Ovarian steroid cell tumor (not otherwise specified) with subsequent spontaneous pregnancy after tumor removal: a case report and literature review. Gynecol Endocrinol (2023) 39(1):2186138. doi: 10.1080/09513590.2023.2186138
54. Sielert L, Liu C, Nagarathinam R, Craig LB. Androgen-producing steroid cell ovarian tumor in a young woman and subsequent spontaneous pregnancy. J Assist Reprod Genet (2013) 30(9):1157–60. doi: 10.1007/s10815-013-0051-9
55. Boussios S, Moschetta M, Tatsi K, Tsiouris AK, Pavlidis N. A review on pregnancy complicated by ovarian epithelial and non-epithelial Malignant tumors: Diagnostic and therapeutic perspectives. J Adv Res (2018) 12:1–9. doi: 10.1016/j.jare.2018.02.006
Keywords: ovarian steroid cell tumor, hyperandrogenemia, ovarian neoplasm/diagnosis, sex cord stromal tumor, virilization, ovary
Citation: Wei CH and Fadare O (2024) Ovarian steroid cell tumors: what do we know so far? Front. Oncol. 14:1331903. doi: 10.3389/fonc.2024.1331903
Received: 01 November 2023; Accepted: 16 January 2024;
Published: 30 January 2024.
Edited by:
Mignon Van Gent, Amsterdam University Medical Center, NetherlandsReviewed by:
Pratibha Shukla, New York University, United StatesCopyright © 2024 Wei and Fadare. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oluwole Fadare, Oluwole.fadare@gmail.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.