 Reed Popp1*
Reed Popp1* Shivam Bansal2
Shivam Bansal2 Seema Sharan2
Seema Sharan2 Syeda Hoorulain Ahmed3
Syeda Hoorulain Ahmed3 Kulkaew Belle Sukniam4Swathi Raikot5Kyle Popp6
Kulkaew Belle Sukniam4Swathi Raikot5Kyle Popp6 Paola Berríos Jiménez7Harsheen Kaur Manaise2Gabrielle Kowkabany8Kristopher Attwood9
Paola Berríos Jiménez7Harsheen Kaur Manaise2Gabrielle Kowkabany8Kristopher Attwood9 Emmanuel M. Gabriel10
Emmanuel M. Gabriel10- 1Department of Surgery, University of Florida College of Medicine, Gainesville, FL, United States
- 2Department of Surgery, Government Medical College and Hospital, Chandigarh, India
- 3Department of Surgery, Dow University of Health Sciences, Karachi, Pakistan
- 4Department of Surgery, Duke University Medical Center, Durham, NC, United States
- 5Department of Surgery, Mayo Clinic, Rochester, MN, United States
- 6Department of Surgery, Florida State University, Tallahassee, FL, United States
- 7Department of Surgery, University of Puerto Rico School of Medicine, San Juan, Puerto Rico
- 8Department of Surgery, The University of Alabama, Tuscaloosa, AL, United States
- 9Department of Surgery, Roswell Park Comprehensive Cancer Center, Buffalo, NY, United States
- 10Department of Surgery, Mayo Clinic, Jacksonville, FL, United States
Background: This study investigated demographic and socioeconomic factors contributing to disparities in the time to treatment for rectal cancer. Subgroup analysis based on age < 50 and ≥ 50 was performed to identify differences in time to treatment among young adults (age < 50) compared to older adults with rectal cancer.
Methods: An analysis was performed using data from the National Cancer Database, spanning from 2004 to 2019. The study encompassed 281,849 patients diagnosed with rectal cancer. We compared time intervals from diagnosis to surgery, radiation, and chemotherapy, considering age, sex, race, and socioeconomic variables. Analyses were performed for the entire cohort and for two subgroups based on age (< 50 and ≥ 50).
Results: Overall, Hispanic patients experienced longer times to surgery, radiation, and chemotherapy compared to non-Hispanic patients (surgery: 94.2 vs. 79.1 days, radiation: 65.0 vs. 55.6 days, chemotherapy: 56.4 vs. 47.8 days, all p < 0.001). Patients with private insurance had shorter times to any treatment (32.5 days) compared to those with government insurance or no insurance (30.6 and 32.5 days, respectively, p < 0.001). Black patients experienced longer wait times for both radiation (63.4 days) and chemotherapy (55.2 days) compared to White patients (54.9 days for radiation and 47.3 days for chemotherapy, both p < 0.001). Interestingly, patients treated at academic facilities had longer times to treatment in surgery, radiation, and chemotherapy compared to those treated at comprehensive and community facilities. When analyzed by age, many of the overall differences persisted despite the age stratification, suggesting that these disparities were driven more by demographic and socioeconomic variables rather than by age.
Conclusion: Significant differences in the time to treatment for rectal cancer have been identified. Hispanic patients, individuals lacking private insurance, Black patients, and patients receiving care at academic facilities had the longest times to treatment. However, these differences were largely unaffected by the age (< 50 and ≥ 50) subgroup analysis. Further investigation into the causes of these disparities is warranted to develop effective strategies for reducing treatment gaps and enhancing overall care for rectal cancer patients.
Introduction
Colorectal cancer, ranking as the third most prevalent cancer among both men and women in the United States (excluding skin cancers), continues to be a major public health concern and is occurring at increasing frequency among young adults (1–6). In addressing the management of colorectal cancer, the National Comprehensive Cancer Network (NCCN) advocates for an individualized approach. For early-stage cases, the NCCN advocates a personalized approach that incorporates surgery, radiation therapy, and chemotherapy to address the unique needs of each patient, taking into account comorbidities, functionality, and frailty to determine how well the patient may tolerate any or all of these therapies. In locally advanced stages, the NCCN recommends a combination strategy, utilizing preoperative chemoradiotherapy followed by surgery to enhance the likelihood of a successful surgical resection with clear margins and minimized morbidity. In the context of advanced or metastatic stages, the NCCN emphasizes systemic chemotherapy as the primary treatment option. Additionally, considerations for targeted therapies and immune checkpoint inhibitors are advised in specific cases (5). In 2023, the American Cancer Society predicts that the United States will witness around 106,970 new cases of colon cancer and 46,050 new cases of rectal cancer. Colorectal cancer remains the third leading cause of cancer-related deaths among both genders in the United States. Over the past few decades, mortality rates associated with colorectal cancer have shown a consistent decline in both men and women (1–4). However, with the increasing incidence of rectal cancer among young adults, timely diagnosis and treatment are essential to achieving good outcomes for rectal cancer (7).
While there has been a decline in colorectal cancer mortality, disparities in cancer treatment and prognosis persist (5, 6, 8). Historically, overall survival among cancer patients has shown disparities across various racial and ethnic groups, with Black individuals experiencing the shortest overall survival compared to Asians and Whites (9). Black patients diagnosed with colorectal cancer at a younger age tend to receive delayed and suboptimal care compared to their White counterparts (10). Several factors, including patients’ insurance coverage, financial status, and demographic characteristics, contribute to longer time intervals to treatment (11). Furthermore, demographic factors and comorbidities explain only a small portion of this disparity, whereas the type of health insurance coverage accounts for a significant portion (28.6% for colon cancer and 19.4% for rectal cancer). This suggests that enhancing access to healthcare could potentially help reduce the disparities in cancer outcomes between racial groups. Examining the socioeconomic and demographic factors linked to longer times in initiating rectal cancer treatment, this study aimed to identify disparities related to the time (in days) to comprehensive cancer care (including surgery, radiation, and chemotherapy), with particular emphasis on age-based disparities (age < 50 and ≥ 50). To our knowledge, this study represents the largest cohort examining differences in time to treatment for rectal cancer, particularly with respect to assessing disparities among younger patients (age < 50). Shorter time to treatment of rectal cancer has been shown by prior to studies to be associated with improved survival outcomes (12, 13). Recognizing the importance of addressing these disparities, efforts should be directed towards narrowing the accessibility gap and ensuring timely access to appropriate medical care for rectal cancer patients.
Patients and methods
We conducted a retrospective study using the National Cancer Database (NCDB) between 2004 and 2019. Because the NCDB is a nationally available, deidentified dataset, Institutional Review Board approval was not required for our study, which focused on individuals aged 18 and older who were eligible for inclusion. Patients with rectal cancer, as defined as cancer located within 12 cm of the anal verge by rigid proctoscopy (5), coded by the following ICD-O-3 codes (8140–8148, 8200, 8260–8263, and 8480–8496), and staged according to the American Joint Committee on Cancer (AJCC 6th and 7th edition) guidelines, were included. Participants with missing information were excluded from the analysis.
Variables in the analysis included age (< 40, 40-50, 50-60, 60-70, > 70), sex (male, female), race (White, Black, Native American, Asian, other), Hispanic origin, insurance status (uninsured, private, government), income (< $63,000 and > $63,000, as predetermined by the NCDB based on neighborhood or zip code analysis), treatment facility type (community, comprehensive, academic, other also using predefined definitions from the NCDB), and geographic location (rural, metropolitan, urban). Times to actual treatment (surgery, chemotherapy, and/or radiation) were computed and summarized. The NCDB records whether a patient received these treatments, but does not indicate eligibility for treatment in the cases where no treatment (i.e., surgery, chemotherapy, and/or radiation) was received. The time to a specific treatment (in days) was defined as when that treatment was first received (e.g., receipt of chemotherapy as neoadjuvant, adjuvant, or peri-operative).
Overall, the NCDB is thought to capture approximately 70% of the cancer patients treated within the US for several cancer malignancies (5, 14). Each site specific dataset contains over 200 variables, ranging widely from demographic, socioeconomic, pathologic, and treatment related variables, including times to treatment for first initial therapy as well as second and third line therapies utilized commonly in the multidisciplinary approach to rectal cancer. The NCDB has been utilized extensively by many investigators, including our group, to analyze disparities in cancer care across many different cancers (15–19).
Statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The clinical and demographic characteristics among each treatment variable (time to any treatment, time to surgery, time to radiation, and time to chemotherapy) were summarized. The means and standard deviations were provided for continuous variables and analyzed using ANOVA. Analyses were performed for the entire cohort and for the two subgroups based on age (age < 50 and ≥ 50). The threshold for statistical significance was set at a p-value of 0.05.
Results
Time to first treatment
The study sample for time to first treatment comprised 281,849 patients. Younger patients (under 40) experienced the shortest time, averaging 25.3 days (Table 1). Wait times increased with age. White patients had the shortest average waiting period (28.8 days), followed by Asians (30.0 days), Black patients (31.5 days), and Native Americans (32.9 days). Hispanic patients generally waited longer (35.6 days) than non-Hispanic patients (28.8 days). Academic institutions had the longest average wait times (33.5 days), while community facilities had a shorter average wait time of 26.6 days. Patients with private insurance waited an average of 26.5 days. When analyzed by age, many of these disparities persisted regardless of the age subgroup (< 50 and ≥ 50), as shown in Table 2. Differences in time to first treatment among patients in urban or rural locations did not reach statistical significance among the age < 50 group (p = 0.08).
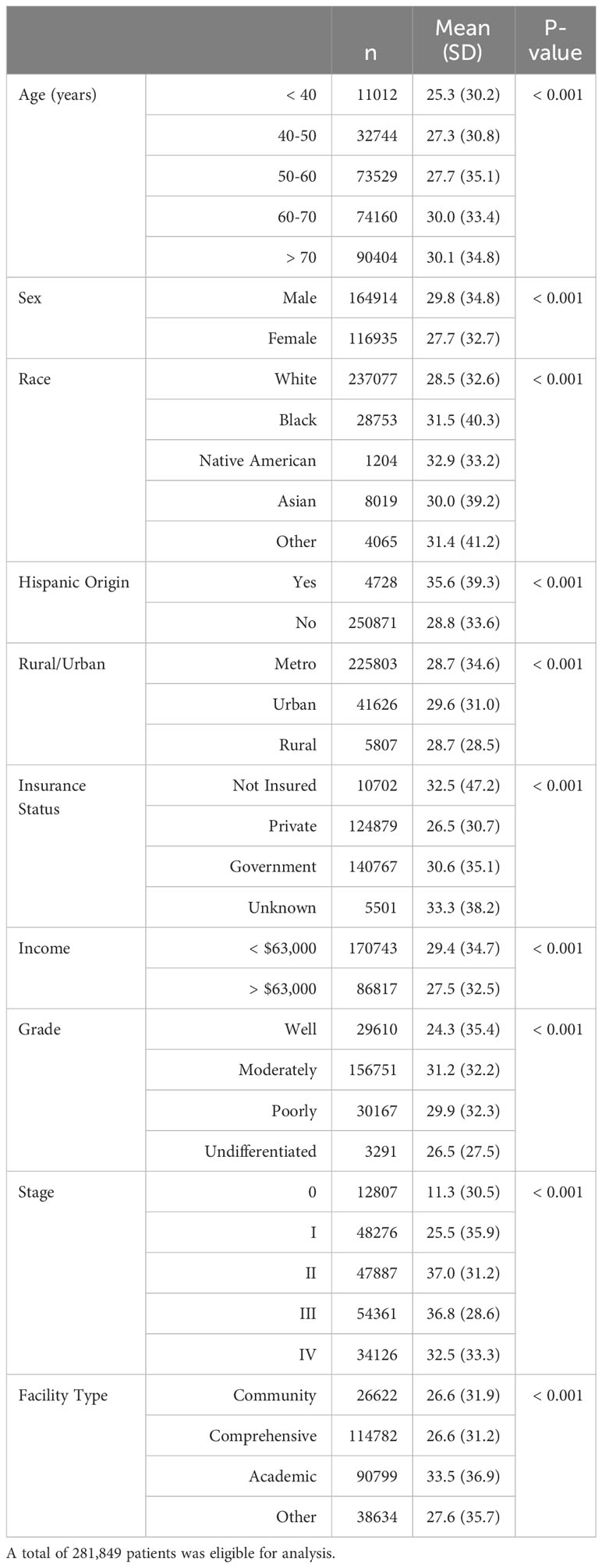
Table 1 Time (in days) to first treatment (including surgery, chemotherapy, and/or radiation).

Table 2 Time (in days) to first treatment (including surgery, chemotherapy, and/or radiation), analyzed by age < 50 years and age ≥ 50 years.
Time to surgery
The study sample for time to surgery included 233,332 patients. Males waited longer for definitive surgery (83.2 days), while females waited an average of 73.1 days (Table 3). Patients of Native American origin had the longest waiting period (96.5 days), followed by White patients (79.4 days), Asians (79.0 days), and Black patients (74.9 days). Urban residents had longer intervals (83.7 days) compared to metropolitan (77.8 days) and rural residents (81.9 days). Uninsured patients faced the longest waiting time (99.1 days), while those with private insurance waited 81.1 days. Academic facilities had the lengthiest waiting period (90.5 days), compared to community facilities (67.6 days) and comprehensive facilities (72.1 days). With regard to age-based disparities (Table 4), no new differences were identified from the overall cohort, and disparities within each variable all achieved statistical significance.
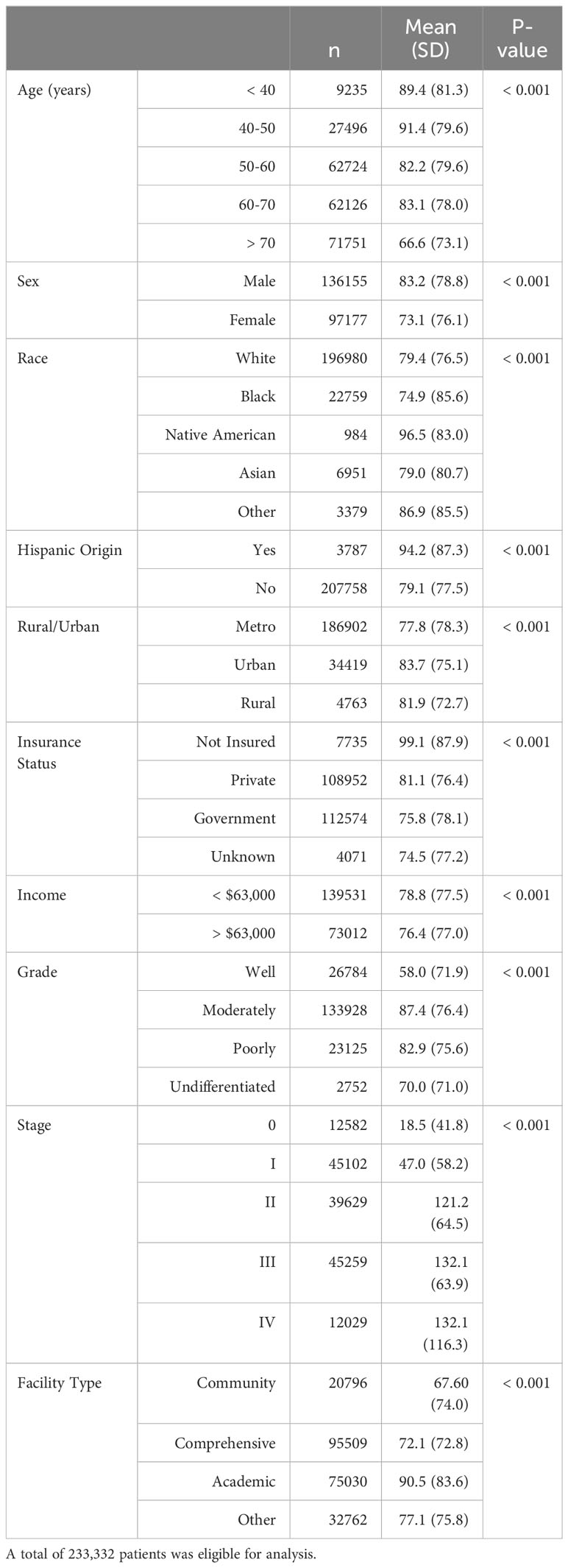
Table 3 Time (in days) to surgery.

Table 4 Time (in days) to surgery, analyzed by age < 50 years and age ≥ 50 years.
Time to radiation
The study sample for time to radiation included 118,969 patients. Black patients had the longest waiting period (63.4 days), followed by Asians (59.7 days), White patients (54.9 days), and Native Americans (50.2 days) (Table 5). Hispanic patients generally waited longer (65.0 days) than non-Hispanic patients (55.6 days). Patients with government insurance waited longer (57.4 days) than uninsured patients (56.3 days). Income levels did not significantly affect the time to receive radiation treatment. These findings were replicated with the subgroup age analysis as listed in Table 6.
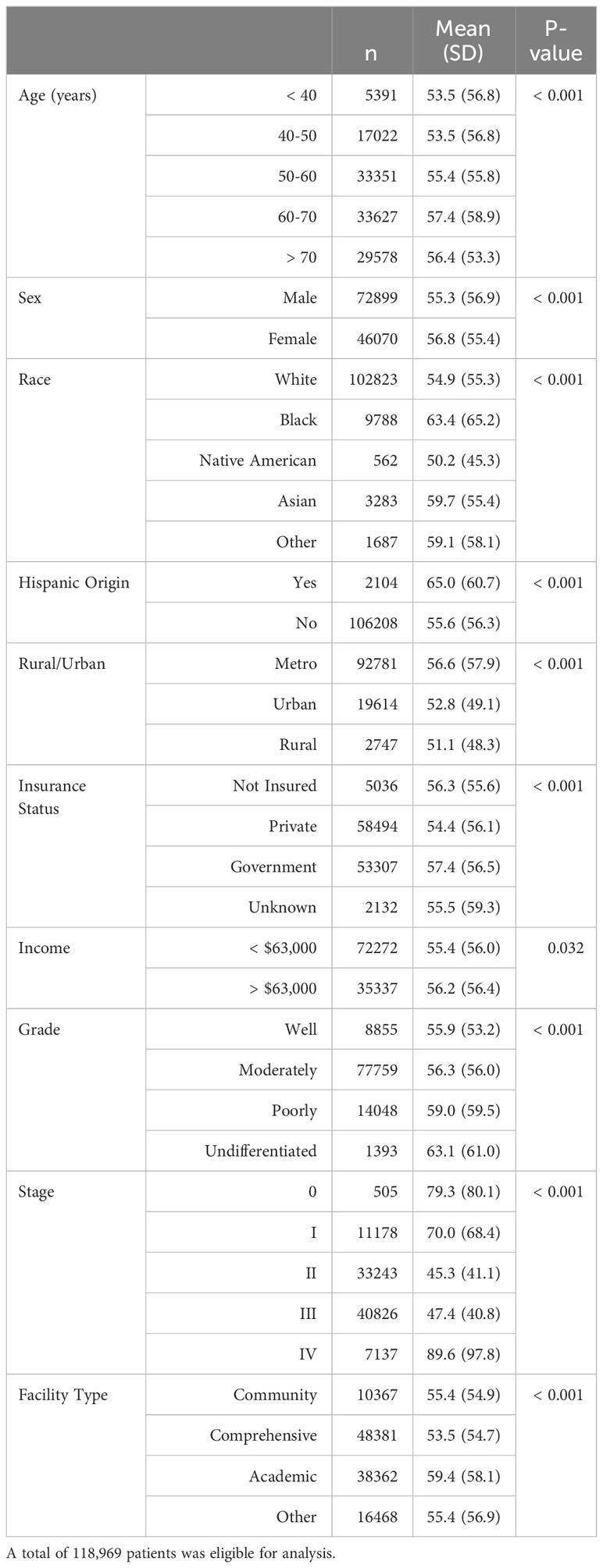
Table 5 Time (in days) to radiation.

Table 6 Time (in days) to radiation, analyzed by age < 50 years and age ≥ 50 years.
Time to chemotherapy
Lastly, the study sample for time to chemotherapy included 169,618 patients. Black patients had the longest time to chemotherapy treatment (55.2 days), while Asians, Whites, and Native Americans had shorter average waiting periods (49.7 days, 47.3 days, and 46.8 days, respectively) (Table 7). Patients of Hispanic origin experienced longer times (56.4 days) compared to their non-Hispanic counterparts (47.8 days). When analyzed by age, these racial and ethnic differences persisted regardless of the age subgroup (Table 8).
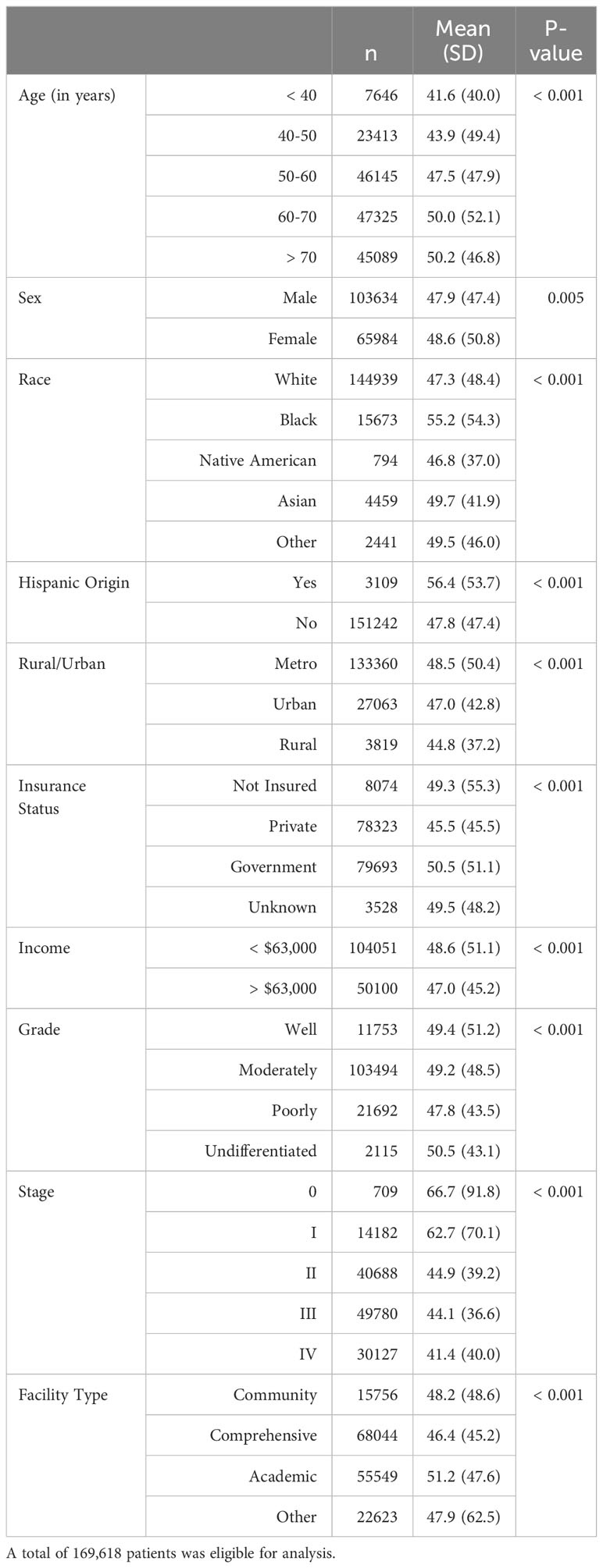
Table 7 Time (in days) to chemotherapy.

Table 8 Time (in days) to chemotherapy, analyzed by age < 50 years and age ≥ 50 years.
Discussion
Through our analysis, we have identified several socioeconomic and demographic factors that were associated with longer time intervals between the diagnosis and treatment of rectal cancer. The time to first treatment for rectal cancer may be an important interval when determining how the time interval of treatment may impact patient outcomes. Some studies have reported that longer diagnostic time intervals might not necessarily be associated with a worse prognosis (20). One meta-analysis found that, in their analysis of 40 studies involving over 20,000 patients, most studies showed no link between time to the treatment of colorectal cancer and survival rates (21). While survival rates may not be affected, however, early diagnosis and treatment remain critical as longer times to treatment can have psychological ramifications for patients. The uncertainty and anxiety linked to a postponed diagnosis can cause distress for both patients and their families. Survivors who perceive a diagnostic delay have been found to experience higher levels of cancer-related distress (22). They may also face challenges in terms of social support, as the prolonged duration of the treatment process can strain relationships and create a sense of isolation. These hurdles can have a profound effect on the patient’s mental health and their ability to cope with the demands associated with cancer diagnosis and treatment.
Notably, the ethnicity of the patients was associated with the timing of when therapeutic interventions like radiation, chemotherapy, and surgery were initiated. We found that Hispanic patients had longer time intervals before receiving these treatments compared to non-Hispanic patients, highlighting a potential disparity in treatment timing across various treatment modalities. Among young patients < 50, this finding persisted with approximately the same length of time compared to those ≥ 50. Overall this may raise concern, especially in the context of the substantial rise in colorectal cancer incidence among Hispanics aged 50-59, while the incidence in other racial and ethnic groups has remained stable (20). Language barriers, which can impede effective communication between healthcare providers and Hispanic patients, may be a key element exacerbating this disparity (23). The quality of physician-patient communication has been closely linked to language, with one study showing that Spanish-speaking patients expressed lower levels of satisfaction with the communication they received (23). Factors such as diverse cultural beliefs, immigration status, and limited access to healthcare due to lack of insurance further may hinder Hispanic patients’ ability to seek and receive proper healthcare (24).
The time to initiate treatment for rectal cancer also was associated with the patient’s racial background. Across all treatment modalities, except for surgery, Black patients experienced significantly longer intervals before receiving their first treatment compared to White patients, which was found regardless of the age subgroup analysis. Our results align with Robbins et al.’s findings, which showed that even after controlling for colorectal cancer screening and diagnosis rates, longer time intervals in receiving adjuvant therapy could still be observed among Black patients (21). This may imply that factors beyond screening and diagnosis could be associated with longer times to administration of necessary adjuvant therapies in Black patients. This could be attributed in part to a potential disparity in specialist consultations between Black and White patients. Black patients have been shown to have lower rates of consultation with medical oncologists and surgical oncologists compared to Whites (25). Disparities in cancer consultations carry consequences, particularly with respect to timely access to essential treatments such as surgery and chemotherapy. The absence of adequate referrals to specialists may lead to insufficient consideration of multimodality therapy (26). Many cancer cases require a combination of treatments, including surgery, chemotherapy, and radiation therapy. When Black patients experience lower rates of consultation, the opportunity to discuss and implement comprehensive multimodality therapy plans may be missed. This can affect the overall quality of care and the chances of achieving the best possible treatment outcomes. Moreover, it is important to note that the underlying mechanisms responsible for this disparity are complex and warrant further investigation. Efforts should be focused on understanding and addressing the barriers that contribute to the delayed initiation of treatment among Black patients. This may involve interventions to improve access to healthcare services, increase awareness and education about the importance of early treatment, and promote culturally sensitive care to ensure equitable and timely delivery of adjuvant therapies.
We also identified an association between the patient’s income level and the time intervals in rectal cancer treatment. Across all treatment modalities, except for radiation, individuals with an annual income below $63,000 experienced longer time intervals before receiving their initial rectal cancer treatment compared to their counterparts with incomes surpassing this threshold. The proportions of patients making < $63,000 and > $63,000 were very similar between the age < 50 and ≥ 50 subgroups, and both age groups < $63,000 experienced similar time intervals. This observation may be influenced by various factors, such as affordability challenges in paying health insurance premiums, difficulties in applying for Medicaid, postponing physician visits due to high co-pays, declining diagnostic testing due to cost, and concerns about work interference, all of which may be disproportionately more burdensome on younger patients (26). While our study does not provide causal association between income and time to treatment, these findings may underscore a need for interventions aimed at rectifying potential imbalances and ensuring equitable healthcare outcomes for all patients, regardless of their socioeconomic status.
It is vital that healthcare providers and policymakers collaborate to institute reforms that address the socioeconomic barriers faced by patients with lower incomes. This may include implementing policies that expand access to affordable healthcare coverage, subsidizing treatment costs for economically disadvantaged individuals, and fostering partnerships with community organizations to bridge the financial gap. By proactively addressing the link between income and longer times to treatment, we can work towards a healthcare landscape that prioritizes accessibility and equity, ensuring that individuals of all income levels have equitable opportunities to receive timely and life-saving rectal cancer treatment.
Beyond factors like race/ethnicity and socioeconomic status, the type of healthcare facility where patients receive treatment may also contribute to treatment disparities. When considering all types of treatment, individuals undergoing rectal cancer treatment at academic institutions had longer time intervals before their initial treatment compared to those treated at comprehensive and community facilities. Similar findings were yielded by Schmerhorn et al. in their study conducted on breast cancer patients. The research revealed that longer time intervals to treatment in breast cancer treatment were primarily linked to the decision to receive care at academic institutions (11). Factors such as educational level, comorbidity burden, and insurance status accounted for 11%, 8%, and 13% of the variation in treatment timing among Black, Hispanic, and other non-White patients, respectively (11).
Additionally, the timing of a patient’s initial rectal cancer treatment was associated with their insurance status. In every treatment type, our results showed that individuals with private insurance experienced shorter waiting times for treatment compared to those without insurance or relying on government insurance. This aspect of our research highlights the influence of diverse insurance coverage on healthcare results, revealing that patients with private insurance experience expedited access to treatments for rectal cancer, while individuals lacking insurance or reliant on government insurance encounter prolonged time intervals. Younger patients would not be expected to have of Medicare, which is most often based on age > 65 years old. Indeed, in our analysis, most patients under 50 had private insurance. But there were still a few thousand patients < 50 who were uninsured, and those patients also experienced longer wait times similar to the cohort as a whole.
Within the differences we have identified in the mean times to treatment for rectal cancer, it is also interesting to note that similar differences were identified in the variances (standard deviations) of many comparisons. For example, minority patients, including Black and Hispanic patients, had wider treatment time distributions than White and non-Hispanic patients. It may be the case that underrepresented patients are more likely to experience greater variability in their time to treatment. In addition, treatment at academic facilities overall had the high variance in time to treatment. However, it may have been the case that patients who received care at academic centers tended to have more advanced disease and required additional workup, which would have prolonged the timing of initial treatment. Thus, it important to note that limitations in the NCDB and our analysis preclude forming any causal associations among the differences that we observed.
Indeed, it is crucial to bear in mind that the data available in the NCDB has specific limitations, necessitating further in-depth analysis. Our study, being retrospective and based on a comprehensive examination of a large database, was subject several constraints, including error in data input. The reliability and generalizability of our findings may also be compromised by missing data, which was excluded. In addition, while many of the results were found to be statistically significant, likely because of the large cohort of patients, not all of the differences in time intervals would be expected to be clinically significant. We have highlighted the largest differences in time intervals, but many other differences were identified that were under 10 days. These differences would be less likely to be associated with suboptimal care than potentially longer time to treatment differences. The NCDB is also limited in distinguishing time intervals between multimodal treatment. Times to treatment overall represent time to the first treatment, but are not organized based on the steps in multidisciplinary care.
In conclusion, our study brings attention to differences in the time to rectal cancer treatment among different demographic and socioeconomic variables. While exploratory, the results of our study provides some insight into a large number of factors that are associated with the timely initiation of treatment for rectal cancer. When assessed by age, younger patients with rectal cancer overall were found to have similar differences to the older subgroup, suggesting that these disparities were driven more by demographic and socioeconomic variables rather than by age. Additional obstacles, such as affordability challenges in paying health insurance premiums, applying for Medicaid, high co-pays, and concerns about work interference, may also exist and were not specifically captured by our analysis. Nonetheless, healthcare and policy professionals should prioritize awareness of these factors and actively support rectal cancer patients, ensuring they receive adequate care and treatment.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
RP: Conceptualization, Investigation, Supervision, Writing – original draft, Writing – review & editing. EG: Conceptualization, Data curation, Project administration, Writing – original draft, Writing – review & editing. SB: Conceptualization, Writing – original draft, Writing – review & editing. SS: Conceptualization, Writing – original draft, Writing – review & editing. SA: Conceptualization, Writing – original draft, Writing – review & editing. KS: Conceptualization, Writing – original draft, Writing – review & editing. SR: Conceptualization, Writing – original draft, Writing – review & editing. KP: Conceptualization, Writing – original draft, Writing – review & editing. PJ: Conceptualization, Writing – original draft, Writing – review & editing. HM: Conceptualization, Writing – original draft, Writing – review & editing. GK: Conceptualization, Writing – original draft, Writing – review & editing. KA: Formal analysis, Methodology.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We wish to acknowledge that this study was conducted independently and without financial assistance from any organizations, agencies, or institutions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Society, A.C. Cancer facts & Figures 2023(2023). Available at: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2023-cancer-facts-figures.html.
2. Society, A.C. Colorectal cancer facts & Figures 2020-2022(2020). Available at: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/colorectal-cancer-facts-and-figures/colorectal-cancer-facts-and-figures-2020-2022.pdf.
3. Surveillance Epidemiology and End Results (SEER) Program. SEER cancer statistics review (CSR) 1975-2018(2021). Available at: https://seer.cancer.gov/csr/1975_2018/.
4. Miller KD, Nogueira L, Devasia T, Mariotto AB, Yabroff KR, Jemal A, et al. Cancer treatment and survivorship statistics, 2022. CA: A Cancer J Clin. (2022) 72:409–36. doi: 10.3322/caac.21731
5. Gabriel E, Attwood K, Al-Sukhni E, Erwin D, Boland P, Nurkin S, et al. Age-related rates of colorectal cancer and the factors associated with overall survival. J Gastrointest Oncol. (2018) 9:96–110. doi: 10.21037/jgo
6. Gabriel E, Attwood K, Al-Sukhni E, Erwin D, Boland P, Nurkin S, et al. Disparities in the age-related rates of colorectal cancer in the United States. Am Surg. (2017) 83:640–7. doi: 10.1177/000313481708300631
7. Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. (2023) 73:233–54. doi: 10.3322/caac.21772
8. Turab Mohammed RG, Navpreet R, Lemini R, Wang K, Agha A, Neupane A, et al. geographic and demographic disparities in colorectal cancer: A population-based study using national cancer database. Hematology/Oncology Stem Cell Ther. (2022) 16. doi: 10.56875/2589-0646.1061
9. Zyczynski TM, Shrestha R, Cook NM. Analysis of racial disparities in time to treatment initiation and survival among patients with advanced cancers. J Clin Oncol. (2021) 39:127–7. doi: 10.1200/JCO.2020.39.28_suppl.127
10. Nogueira LM, Gupta S. Racial disparities in receipt of guideline-concordant care for early-onset colorectal cancer in the U.S. J Clin Oncol. (2022) 40:6544–4. doi: 10.1200/JCO.2022.40.16_suppl.6544
11. Schermerhorn MC, Grunvald MW, O'Donoghue CM, Rao RD, Becerra AZ. Factors mediating racial/ethnic disparities in delayed treatment of breast cancer. Ann Surg Oncol. (2022) 29:7652–8. doi: 10.1245/s10434-022-12001-5
12. Tobin EC, Dobbs E, Deslich S, Richmond BK. Race/ethnicity and social determinants of health and their impact on the timely receipt of appropriate operative treatment of colon cancer. Am Surg. (2024), 31348241241697. doi: 10.1177/00031348241241697
13. Franssen RFW, trous MTA, Bongers BC, Vogelaar FJ, Janssen-Heijnen MLG. The association between treatment interval and survival in patients with colon or rectal cancer: A systematic review. World J Surg. (2021) 45:2924–37. doi: 10.1007/s00268-021-06188-z
14. Mohammed T, Gosain R, Rana N, Lemini R, Wang K, Agha A, et al. Geographic and demographic disparities in colorectal cancer: A national cancer database analysis. Hematol Oncol Stem Cell Ther. (2023) 16:262–71.
15. Gabriel E, Thirunavukarasu P, Attwood K, Nurkin SJ. National disparities in minimally invasive surgery for pancreatic tumors. Surg Endosc. (2017) 31:398–409. doi: 10.1007/s00464-016-4987-6
16. Bagaria SP, Neville M, Gray RJ, Gabriel E, Ashman JB, Attia S, et al. The volume-outcome relationship in retroperitoneal soft tissue sarcoma: evidence of improved short- and long-term outcomes at high-volume institutions. Sarcoma. (2018) 2018:3056562. doi: 10.1155/2018/3056562
17. Emmanuel Gabriel SN, Attwood K, Hochwald S, Kukar M, Nurkin S. Disparities in major surgery for esophagogastric cancer among hospitals by case volume. Am Surgeon. (2018) 9(3):503–16. doi: 10.21037/jgo.2018.01.18
18. Rana N, Gosain R, Lemini R, Wang C, Gabriel E, Mohammed T, et al. Socio-demographic disparities in gastric adenocarcinoma: A population-based study. Cancers (Basel). (2020) 12. doi: 10.3390/cancers12010157
19. Abbaszadeh Kasbi A, Ashary MA, Baksh M, Nussbaum S, Attwood K, Gabriel E. Age-related survival outcomes for pancreatic cancer by age. Cancer Diagn Progn. (2022) 2:71–7. doi: 10.21873/cdp.
20. Pita-Fernández S, González-Sáez L, López-Calviño B, Seoane-Pillado T, Rodríguez-Camacho E, Pazos-Sierra A, et al. Effect of diagnostic delay on survival in patients with colorectal cancer: a retrospective cohort study. BMC Cancer. (2016) 16:664. doi: 10.1186/s12885-016-2717-z
21. Robbins AS, Siegel RL, Jemal A. Racial disparities in stage-specific colorectal cancer mortality rates from 1985 to 2008. J Clin Oncol. (2012) 30:401–5. doi: 10.1200/JCO.2011.37.5527
22. Miles A, McClements PL, Steele RJ, Redeker C, Sevdalis N, Wardle J. Perceived diagnostic delay and cancer-related distress: a cross-sectional study of patients with colorectal cancer. Psycho-Oncology. (2017) 26:29–36. doi: 10.1002/pon.v26.1
23. Seijo R, Gomez H, Freidenberg J. Language as a communication barrier in medical care for Hispanic patients. Hispanic J Behav Sci. (1991) 13:363–76. doi: 10.1177/07399863910134001
25. Simpson DR, Martínez ME, Gupta S, Hattangadi-Gluth J, Mell LK, Heestand G, et al. Racial disparity in consultation, treatment, and the impact on survival in metastatic colorectal cancer. J Natl Cancer Inst. (2013) 105:1814–20. doi: 10.1093/jnci/djt318
Keywords: rectal cancer, treatment, disparity, socioeconomic factors, cancer care
Citation: Popp R, Bansal S, Sharan S, Ahmed SH, Sukniam KB, Raikot S, Popp K, Jiménez PB, Manaise HK, Kowkabany G, Attwood K and Gabriel EM (2024) Disparities in time to treatment initiation for rectal cancer patients: an analysis of demographic and socioeconomic factors. Front. Oncol. 14:1327400. doi: 10.3389/fonc.2024.1327400
Received: 07 November 2023; Accepted: 22 April 2024;
Published: 10 May 2024.
Edited by:
Jennifer Weiss, University of Wisconsin-Madison, United StatesReviewed by:
Thomas Lawler, University of Wisconsin-Madison, United StatesHamideh Salimzadeh, Tehran University of Medical Sciences, Iran
Jessica Schumacher, University of North Carolina at Chapel Hill, United States
Copyright © 2024 Popp, Bansal, Sharan, Ahmed, Sukniam, Raikot, Popp, Jiménez, Manaise, Kowkabany, Attwood and Gabriel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Reed Popp, cmVlZHBvcHBAdWZsLmVkdQ==