 Ana Varges Gomes1*
Ana Varges Gomes1* Gilberto Castro Jr.2
Gilberto Castro Jr.2 Thiago Bueno de Oliveira3
Thiago Bueno de Oliveira3 Ana Medina Colmenero4
Ana Medina Colmenero4 Leonor Ribeiro5
Leonor Ribeiro5 Amanda Psyrri6,7Nicolas Magné8,9
Amanda Psyrri6,7Nicolas Magné8,9 Maria Plana Serrahima10
Maria Plana Serrahima10 Joana Marinho11,12Raul Giglio13Leticia Iglesias Rey14
Joana Marinho11,12Raul Giglio13Leticia Iglesias Rey14 Martín Angel15Ana M. Macedo16,17
Martín Angel15Ana M. Macedo16,17- 1Medical Oncology Department, Centro Hospitalar Universitário do Algarve, Faro, Portugal
- 2Department of Medical Oncology, Instituto do Câncer do Estado de São Paulo, São Paulo, Brazil
- 3Medical Oncology Department, AC Camargo Cancer Center, São Paulo, Brazil
- 4Department of Medical Oncology, Fundación Centro Oncológico de Galicia, A Coruña, Spain
- 5Medical Oncology Department, Centro Hospitalar Universitário Lisboa Norte – Hospital Santa Maria, Lisbon, Portugal
- 6Medical Oncology Department, Attikon General University Hospital of Athens, Athens, Greece
- 7Department of Internal Medicine, National and Kapodistrian University of Athens, Athens, Greece
- 8Institut Bergonié, Department of Radiation Oncology, Bordeaux, France
- 9Institut Lucien Neuwirth, Department of Radiotherapy, Saint Priest en Jarez, France
- 10Oncología Médica, Institut Català d’Oncologia-Hospitalet, Instituto de Investigación Biomédica de Bellvitge (IDIBELL), Barcelona, Spain
- 11Medical Oncology Department, Centro Hospitalar Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal
- 12Associação de Investigação de Cuidados de Suporte em Oncologia (AICSO), Vila Nova de Gaia, Portugal
- 13Instituto de Oncología Ángel H. (AH) Roffo, Universidad de Buenos Aires, Buenos Aires, Argentina
- 14Department of Medical Oncology, Complejo Hospitalario Universitario de Ourense, Ourense, Spain
- 15Department of Genitourinary Cancer, Instituto Alexander Fleming, Buenos Aires, Argentina
- 16Department of Biomedical Sciences and Medicine Evidenze, Lisbon, Portugal
- 17Faculdade de Medicina e Ciências Biomédicas, Universidade do Algarve, Faro, Portugal
Introduction: Squamous cell carcinoma of the head and neck (SCCHN) is a multifactorial disease involving genetic and environmental factors representing one of the most frequent cancer-related deaths worldwide. Tobacco and alcohol use account for most SCCHN, while a growing subset of oropharyngeal cancers is causally associated with human papillomavirus (HPV) infection. Despite improvements in overall survival, patients with HPV-negative locally advanced (LA) SCCHN continue to have a poor prognosis. For these patients, the standard of care is radiotherapy with concurrent chemotherapy (RCT).
Methods: This retrospective, multicenter, and observational study analyzed the treatment compliance of 326 patients with LA-SCCHN who underwent RCT between January 1st, 2014, and June 30th, 2017. This study also evaluated the potential factors associated with treatment compliance, the compliance impact on clinical response, and the main toxicities experienced by patients.
Results: A total of 274 (84%) patients were compliant and received the planned dose of cisplatin. Overall, 957 adverse events were reported in 98.2% of patients during the study. The overall response rate was 80.2%, with 60.4% of patients achieving a complete response.
Discussion: Despite the high treatment compliance, 62.6% of adverse events reported were related to cisplatin. Identifying risk factors associated with non-compliance could enable physicians to identify ineligible patients for cisplatin-based RCT and prevent patients from receiving inadequate treatment leading to severe adverse events..
1 Introduction
Squamous cell carcinoma of the head and neck (SCCHN) is one of the most frequent causes of cancer-related deaths, with more than 500,000 cases diagnosed annually (1). SCCHN is typically observed in the oropharynx, oral cavity, hypopharynx, or larynx, being a complex disease influenced by genetic and environmental factors (2). Although alcohol and smoking represent the major etiological risk factors, human papillomavirus (HPV) and poor oral hygiene also play a relevant role (3, 4).
Patients with locally advanced (LA) SCCHN (stage III or IVA/B) represent approximately 60% of the SCCHN cases at diagnosis (5). Despite improvements in overall survival due to therapy innovation, patients with HPV-negative LA-SCCHN continue to have poor prognoses (6). Thus, concurrent cisplatin-based chemotherapy (CRT) has been used with improved outcomes (7–9).
CRT with high-dose cisplatin is the standard of care for LA-SCCHN. Bolus cisplatin 100 mg/m2 x 3 cycles Q21 days concomitant with radiotherapy (RT) represents the standard of care for LA-SCCHN. The efficacy of cisplatin-based radiochemotherapy (RCT) seems to be correlated with the cumulative dose received (10, 11). Still, compliance with platinum-based RCT treatment might be lower due to the significant toxicity caused by this regimen (12, 13).
HPV-positive cancers are typically associated with better outcomes compared to HPV-negative tumors (14). Hence, the clinical benefit of cisplatin-based RCT has been shown to decrease with lower total dosage in patients with HPV-negative LA-SCCHN. Notably, a cumulative cisplatin dose of <200 mg/m2 has been associated with lower overall survival than a cumulative dose of ≥200 mg/m2 (15).
This retrospective observational study assessed compliance with cisplatin-based RCT in real-world patients with LA-SCCHN. This study also evaluated the potential factors associated with treatment compliance, the compliance impact on clinical response, and the main toxicities.
2 Methodology
2.1 Study design
This retrospective, multicenter, and observational study analyzed the treatment compliance in patients with LA-SCCHN treated with cisplatin-based RCT, administered between January 1st, 2014, and June 30th, 2017. All RCT regimens were allowed if the planned cumulative dose of cisplatin was defined before treatment as ≥200 mg/m2 body surface area (BSA). The study was conducted in 11 centers, including Portugal, France, Spain, Greece, Brazil, and Argentina.
2.2 Patients
Adults with histologically confirmed LA-SCCHN (stage III, IVA, or IVB according to the American Joint Committee on Cancer (AJCC) staging 7th edition) of the oral cavity, oro- or hypopharynx, and larynx were enrolled in the study. Patients who had undergone surgery before cisplatin-based RCT, or were included in any clinical trial within 30 days before the RCT, were excluded.
2.3 Assessment
Medical history, prescriptions, and laboratory reports were collected from the patient’s medical records. The compliance was assessed based on the cumulative total dose of cisplatin ≥200 mg/m2 BSA. Patients receiving a cumulative dose of cisplatin <200 mg/m2 BSA were considered non-compliant.
The identification of a prognostic/predictive score for therapy compliance included the analysis of demographic characteristics (age, gender, body mass index, BSA, smoking/drinking status), disease characteristics (Tumor Nodes Metastases (TNM) classification, according to AJCC staging 7th edition, disease stage, HPV/p16 status), medical history (previous malignant disease, Eastern Cooperative Oncology Group performance status (ECOG PS) at baseline, time since initial diagnosis until the start of cisplatin/RT, creatinine clearance [(140 – age) x mass (kg) x [0.85 if female]/72 x [serum creatinine (mg/dL)], and involuntary weight loss ≥20%).
Treatment objective responses were evaluated according to RECIST 1.1 (16). Adverse events (AEs) were also described according to National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE; version 4.0).
2.4 Statistical analysis
Continuous variables are described as means, standard deviations (SD), or medians (interquartile range (IQR) and minimum and maximum) for variables with skewed distributions. Categorical and ordinal variables are described as absolute and relative frequencies. Compliance with cisplatin is presented as the number and percentage of patients who received a dosage of ≥200 mg/m2 cisplatin. A 95% confidence interval (CI) was calculated. A multiple logistic regression analysis was conducted to investigate the impact of explanatory variables on cisplatin compliance and to obtain a predictive score. The factors considered for the model included: demographic characteristics (age, gender, body mass index, BSA), disease characteristics (TNM classification, disease stage, HPV/p16 status), medical history (smoking/drinking status, ECOG PS at baseline, time since initial diagnosis until the start of cisplatin/RT, previous malignant disease, creatinine clearance, and involuntary weight loss ≥20%). A p-value of 0.05 significance level was considered. The Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA) software (version 22.0) was used to conduct the study analyses.
3 Results
3.1 Patients characterization
A total of 346 patients were enrolled in the study (Figure 1). Twenty patients were excluded for not fulfilling the screening criteria: tumor location other than the oral cavity, oro- or hypopharynx, and larynx; treatment with cisplatin and RCT initiated after June 30th, 2017; targeted cumulative cisplatin dose <200 mg/m2 or missing; TNM – M1; or patients whose cisplatin dose was not available. Therefore, the final eligible population comprised 326 patients.
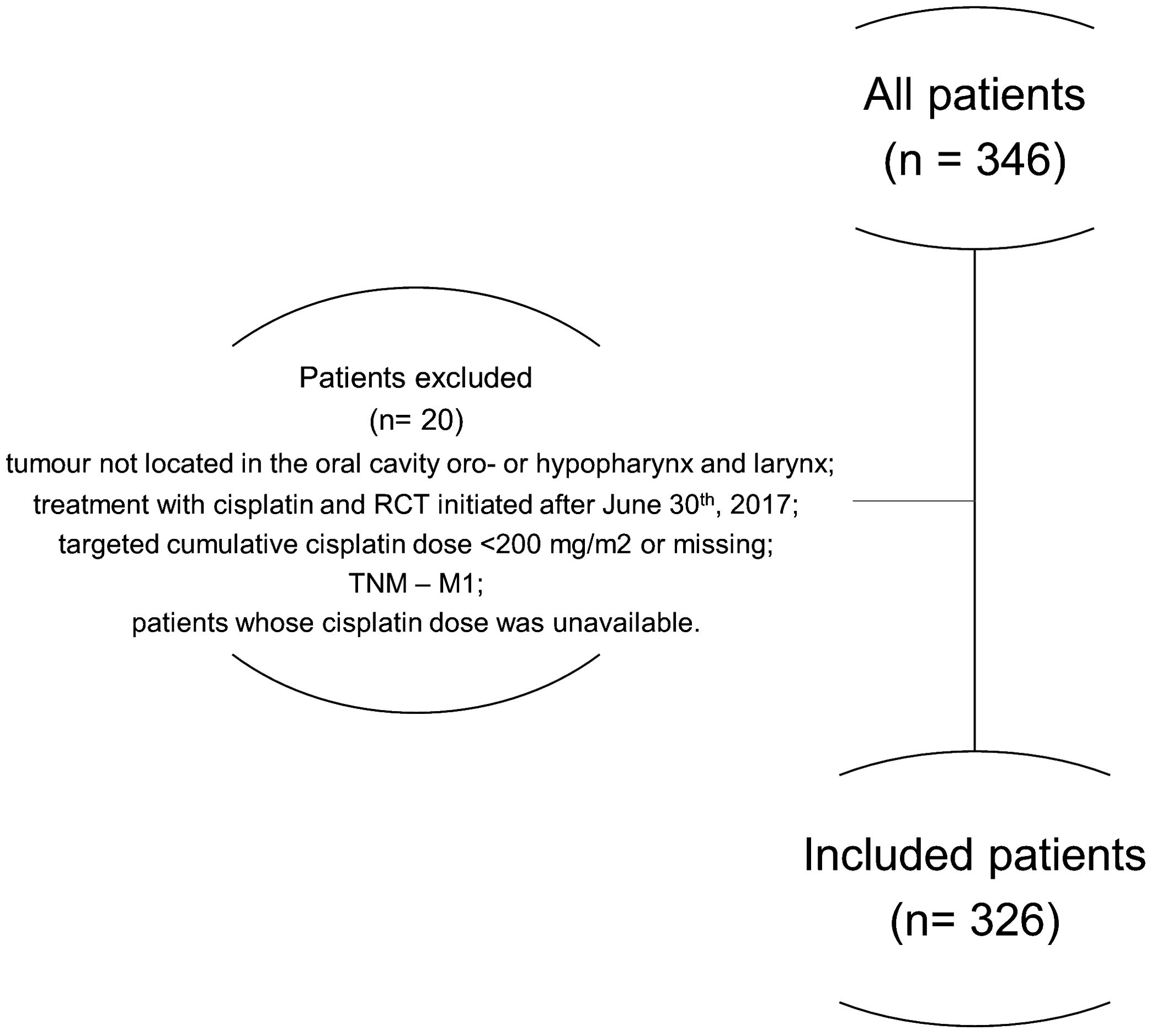
Figure 1. Description of the patient selection process.
The demographic and clinical characteristics of the patients are summarized in Table 1. The median age was 63.0 years (SD± 8.9) and 86.2% were male. Overall, 5.2% of patients had prior malignancies, and less than 1.8% had previous renal dysfunction. Nearly half of the patients were smokers (48.5%), and 55.8% of patients consumed alcohol at least five times per week. Among patients who performed HPV testing (16.3%) and whose data were available (92.5%), 63.3% tested positive. Of the 24.5% of patients tested for p16, 48.8% were positive (Supplementary Table 1). The most common tumor location was the oropharynx (44.8%), followed by the larynx (21.8%) and hypopharynx (20.2%). Globally, 30.4% of the patients enrolled were LA-SCCHN stage III, 56.4% stage IVA, and the remaining were IVB (13.2%). The mean time from the initial diagnosis to the initiation of cisplatin-based RCT was 11.9 weeks. Most patients (92.3%) had an ECOG PS of 0 or 1 at the time of RCT initiation. Regarding renal function, the mean serum creatinine was 0.8 mg/dL, and the mean creatinine clearance was 90.1%. Hearing function status was not evaluated in most patients (87%).
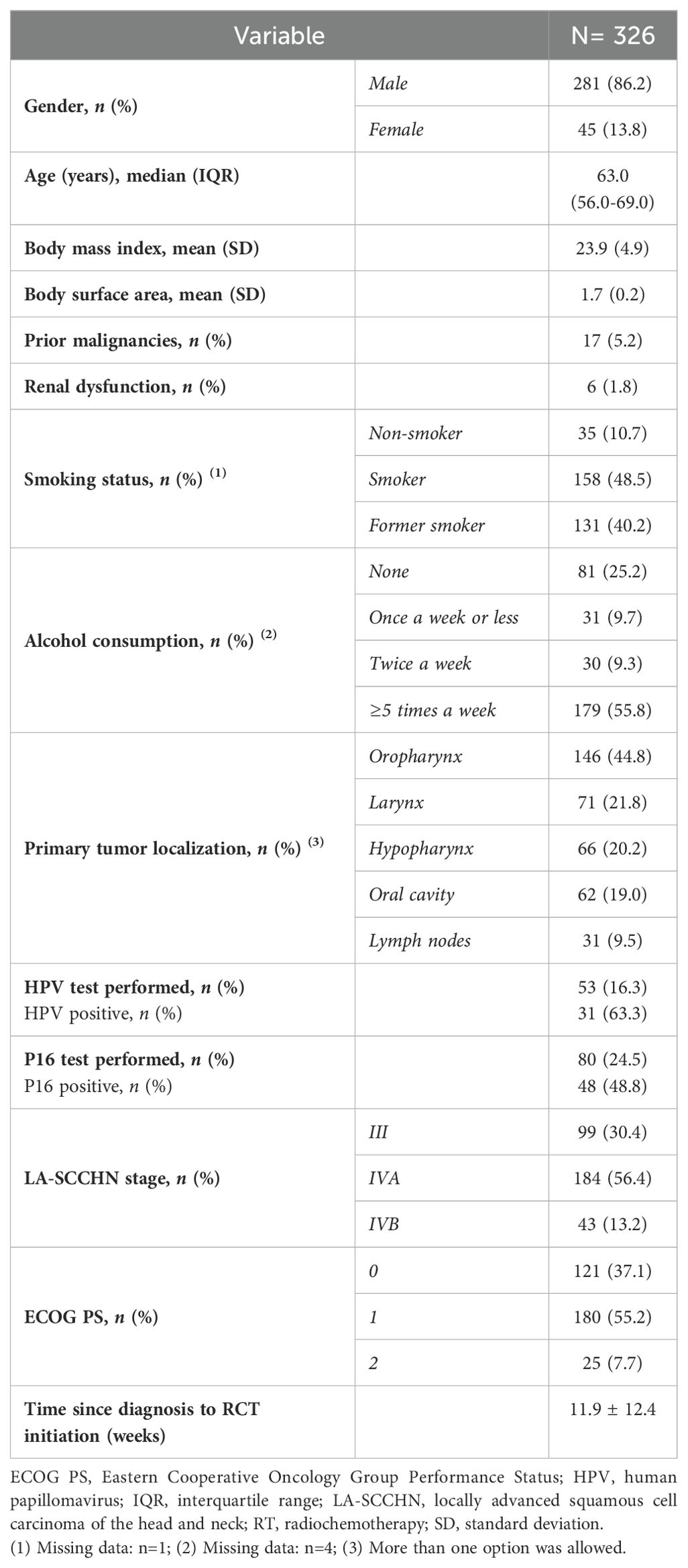
Table 1. Baseline and clinical characteristics of the patients.
3.2 Treatment compliance
The cisplatin regimens used were cisplatin 100 mg/m² q3w in 198 patients (60.7%), cisplatin 40 mg/m² q1w in 103 patients (31.6%) and cisplatin 4 mg/m² days 1-4 q1w in 25 patients (7.7%). The mean cumulative cisplatin dose received during RCT was 251 ± 98.3 mg/m2 (Table 2).
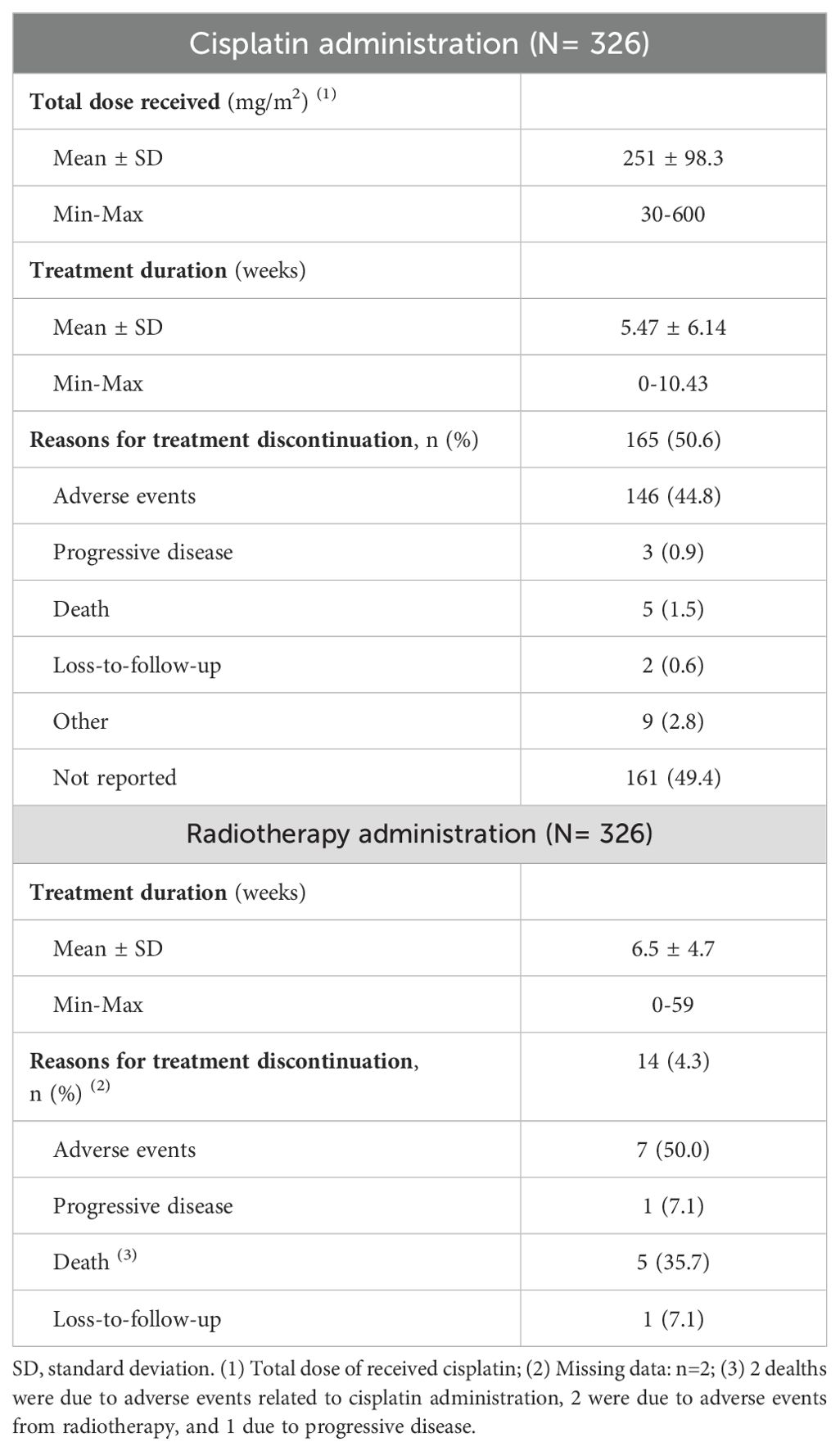
Table 2. Cisplatin and radiotherapy administration.
Overall, 274 (84.0%, 95% CI: 79.7% - 87.6%) patients were compliant and received the planned dose of ≥200 mg/m² BSA. The mean treatment duration was 5.47 weeks. Cisplatin treatment was prematurely discontinued in 50.6% of patients, mainly due to AEs, in 146 (88.5%) patients. Regarding RT administration, the median duration was 6.5 weeks. Overall, 4.3% of patients discontinued RT because of AEs (Table 2).
The multivariate regression analysis showed that ECOG PS was the only factor independently associated with cisplatin treatment compliance during RCT (ECOG PS 2 HR: 0.135 [95% CI: 0.35 - 0.528]; p = 0.004), underlining that patients who had an ECOG PS of 2 were less likely to be compliant with cisplatin-based RCT (Supplementary Table 2).
When analyzing the radiological response to cisplatin-based RCT, the overall response rate (ORR) was 80.2%, with 60.4% achieving a complete response (Figure 2A). While an ORR of 82.0% was achieved in compliant patients who received a total dose of cisplatin ≥200 mg/m², in non-compliant patients (who received a total dose of cisplatin <200 mg/m²), the ORR was 69.8%. This difference was not statistically significant between groups (p-value = 0.063, Figure 2B), with an estimated odds ratio of 1.97 [95% CI: 0.9547 - 4.0817].
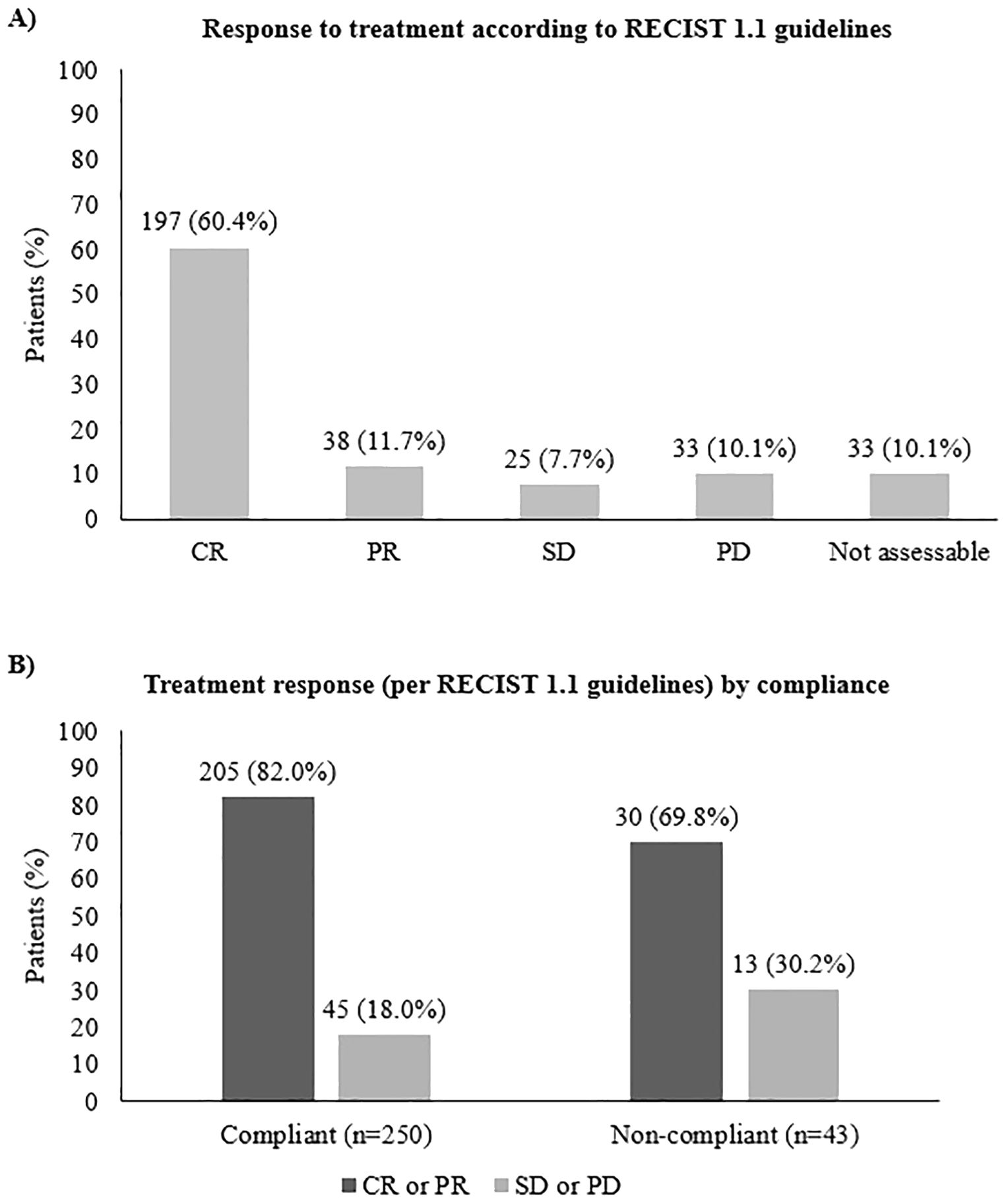
Figure 2. Response to cisplatin-based RCT (A) in the overall population and (B) according to compliance with treatment. CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
3.3 Safety analysis
A total of 957 AEs were reported in 98.2% (n= 320) patients during the study. Overall, 62.6% (n= 599) of AEs reported were related to cisplatin. Of the total AEs reported, 74.1% (n= 709) were mild to moderate (grade 1-2), 23.2% (n= 222) were grade 3, and 2.3% (n= 22) were grade 4. Severe adverse events (SAEs) were registered in 8.4% (n= 80), and 75.0% (n= 60) were related to cisplatin. The most common AEs related to cisplatin during RT were oral mucositis (26.6%, n= 159), nausea and vomiting (16.1%, n= 97), and neutropenia (7.7%, n= 46). Additionally, 43 (7.2%) AEs were related to impaired renal function. Table 3 summarizes the AEs that registered more than 20 occurrences.
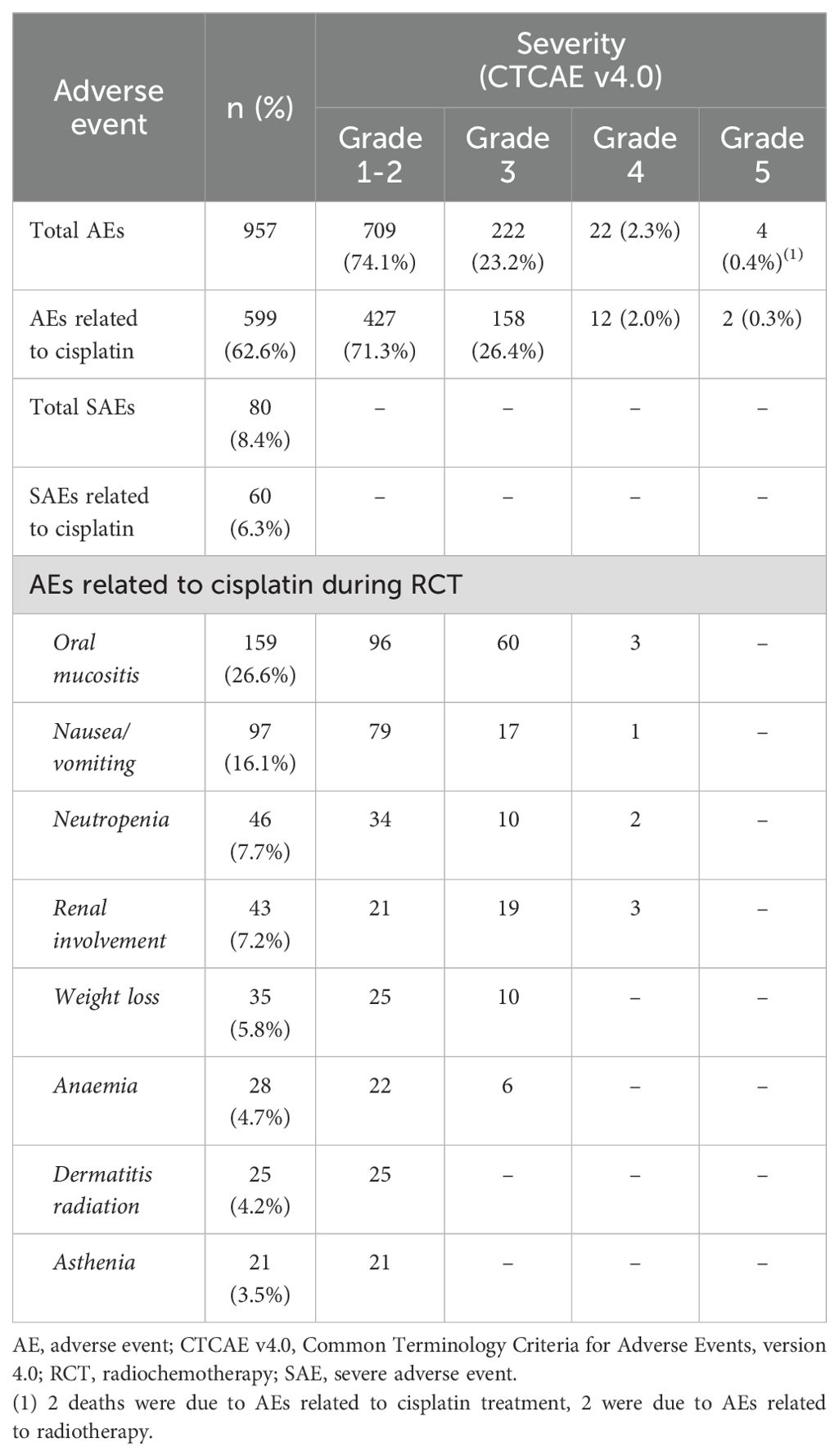
Table 3. Adverse events.
4 Discussion
This study revealed that patients with LA-SCCHN achieved a high compliance rate with cisplatin concomitantly administered with RT, which is adversely affected by poor ECOG PS. This study also disclosed that non-compliance might be associated with lower tumor response.
Though the clinical characteristics of these patients are heterogeneous, as they were collected in a real-world scenario, they are similar to populations studied in previous clinical trials. Regarding the TNM stage at diagnosis, most patients had T3 to T4 (78.2%) and were N2 (52.5%), respectively, similar to that of the GORTEC 2007-02 trial (14). Only 53 (16.3%) patients were tested for HPV and 80 (24.5%) for p16, values slightly lower than those previously published (17). The lower level of testing might be explained by the inclusion dates of the study, as HPV testing has only in recent years been recommended and implemented. Notably, it should be highlighted that performing HPV testing in oropharyngeal cancer patients is critical since HPV-positive cancers are commonly associated with better outcomes compared with HPV-negative tumors (14).
This international multicentered study disclosed a high treatment compliance rate (84%) among patients with LA-SCCHN. This compliance rate is notably higher than the one reported in a previous retrospective study (37%, COMPLY) conducted in patients with LA-SCCHN (stage III or IVA/B) who received a cumulative dose of ≥200 mg/m², based on their age, ECOG, and renal function (17). While the most common regimen used in our study was 100 mg/m² q3w, in the COMPLY study, the most common regimen was 40 mg/m² q1w, aiming to prevent toxicity (17). Of note, in the COMPLY study, the compliance rates were higher for lower-dose weekly schedules (77.8% for 40 mg/m2 and 65% for 30 mg/m2) than those obtained with a high-dose schedule (54.8% for 100 mg/m2). Still, in another retrospective study, nearly half of all patients completed three cycles of high-dose cisplatin (18).
The high-dose cisplatin regimen used in this study is considered the most adequate, as it promotes better locoregional and overall survival relative to RT following international clinical guidelines (19, 20). Still, it was associated with a higher incidence of AEs, as most toxicities are dose and schedule-dependent (17), which, in turn, might potentiate dose reductions and treatment delays with this intensive regime (12).
Identifying risk factors in patients who do not tolerate high cisplatin doses could enable physicians to identify ineligible patients for cisplatin-based RCT and prevent excessive toxicities and severe AEs (21). Accordingly, this study assessed the factors potentially affecting treatment compliance with cisplatin, such as demographic and clinical features and other SCCHN-related characteristics. The ECOG PS was the only factor identified by the multivariate model as an independent factor associated with compliance with cisplatin during RCT. Patients with an ECOG PS of 2 were less likely to comply with cisplatin-based RCT, suggesting that it should be considered a risk factor for compliance, and, thus, alternative treatments might be considered. These results are consistent with the international guidelines recommending that patients older than 70 years with an ECOG PS of ≥2 should not be treated with cisplatin (22, 23). Accordingly, most studies on CRT excluded patients older than 70 years. Nonetheless, in this model, age was considered a continuous variable; perhaps stratification of this variable could have revealed certain significant age ranges as predictors of compliance with cisplatin-based RCT. Another possible explanation is that as biological age per se is currently not recognized as a good predictor of benefit and/or toxicity in elderly patients, it should not guide treatment decisions and the functional age should be adopted instead (24). Decision-making in older patients requires a multidisciplinary evaluation and risk assessment provided by a comprehensive geriatric assessment.
The association between compliance and objective response to cisplatin-based RCT was also assessed. Suboptimal compliance with the cisplatin regimen might negatively impact patient outcomes. Regardless of the treatment regimen, it has been suggested that a cumulative dose of 200 mg/m² has to be achieved to allow a therapeutic benefit (12). A higher objective response was obtained in compliant patients (82.0%) who received a total dose of cisplatin ≥200 mg/m² compared with non-compliant patients (69.8%) who received a total dose of cisplatin <200 mg/m², with an estimated odds ratio of 1.974. These results suggest that the cumulative cisplatin dose might correlate with clinical response to cisplatin-based RCT.
The compliance to cisplatin plus RT is frequently lowered due to toxicity (17). Despite the high treatment compliance in this study, 62.6% (n= 599) of reported AEs were cisplatin-related. Most were low grade (grade 1 or 2) and aligned with those previously reported, including oral mucositis, neutropenia, and renal impairment (14). Strategies such as more frequent lower RT doses could potentially circumvent high-dose related toxicities, thereby improving compliance. A recent Japanese study found that weekly RCT was not inferior to 3-weekly RCT for post-operative high-risk patients with LA-SCCHN and had a favorable toxicity profile, leading the authors to conclude that this could be a new strategy in these patients (25, 26). Although there is lack of robust scientific evidence, weekly lower dose RCT may also benefit elderly patients who are frail (27). Other strategies such as accelerated fractionation with concomitant boost and RCT with concurrent split-dose cisplatin are also being explored as alternatives for patients who cannot safely tolerate high-dose RCT (28, 29). The main limitation of this study is its retrospective nature, as all the available data depends on the information already registered on the medical records. Still, this population represents the real-world setting, with a high prevalence of comorbidities and risk factors. Furthermore, this study was performed during the COVID pandemic, which impacted the recruitment period as the workload of clinicians/researchers increased considerably. Lastly, as HPV testing was not the diagnostic standard of SCCHN during the period the patients were diagnosed, we were unable to do subgroup analysis by HPV status due to the low number of patients with data available.
To our knowledge, this is the most extensive study that has provided up-to-date real-world data on compliance with cisplatin during RCT in patients with LA-SCCHN. The cisplatin regimen was administered according to each country’s site and local practices without being biased by screening criteria. Thus, the results from our retrospective study might be extrapolated to the general population of patients with LA-SCCHN receiving cisplatin.
This study shows a high cisplatin compliance rate (median cumulative dose ≥200 mg/m2) in patients with LA-SCCHN receiving cisplatin-based RCT, which is negatively influenced by ECOG PS. The absence of cisplatin compliance during RCT adversely affects tumor response.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Ethics Committee of each participating institution, which waived the requirement for informed consent to collect data from patients’ medical charts retrospectively. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
AVG: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. GC: Resources, Visualization, Writing – original draft, Writing – review & editing. TBdO: Resources, Writing – review & editing. AMC: Resources, Writing – review & editing. LR: Resources, Writing – review & editing. AP: Resources, Writing – review & editing. NM: Resources, Writing – review & editing. MPS: Resources, Writing – review & editing. JM: Resources, Writing – review & editing. RG: Resources, Writing – review & editing. LIR: Resources, Writing – review & editing. MA: Resources, Writing – review & editing. AMM: Data curation, Formal analysis, Software, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was financially supported by Merck, S.A., Alges, Portugal, an affiliate of Merck KGaA (CrossRef Funder ID: 10.13039/100009945).
Acknowledgments
The authors want to acknowledge the collaboration of Ana Joaquim and Ema Neto (Medical Oncologists from Centro Hospitalar Vila Nova de Gaia/Espinho), Gabriel Triana, Carolina Pena, Begoña Uriarte, María Dolores Pérez, Concepción Victoria, Jesús García Gómez, Cecília Melo Alvim (Medical Oncologist) and the group of coordinators from the Clinical Investigation Center of the Centro Hospitalar Universitário Lisboa Norte, E.P.E - Hospital Santa Maria, Lisboa, Portugal.
Conflict of interest
Merck KGaA, Darmstadt, Germany, reviewed the manuscript for medical accuracy only before the journal submission. The authors are fully responsible for the content of this manuscript, and the views and opinions described in the publication reflect solely those of the authors. AV: received a grant from Merck for the execution of this study. GC: received grants as a speaker from AstraZeneca, Bristol-Myers-Squibb, Merck Serono, Merck Sharp Dohme; participation in Advisory Boards from AstraZeneca, Bristol-Myers-Squibb, Merck Serono, Merck Sharp Dohme; principal investigator in sponsored trials: AstraZeneca, Bristol-Myers-Squibb, Merck Serono, Merck Sharp Dohme, GlaxoSmithKline; travel and/or accommodations: AstraZeneca, Merck Serono, Merck Sharp Dohme. TdO: received grants as a speaker from Merck, MSD, and Astra Zeneca advisory boards and travel grants from MSD, Sanofi, and Roche. AC: received travel grants from Merck and MSD. LR: received travel grants and participated in advisory boards and oncology education programs from MSD, Merck, BMS, Roche, and Novartis. AP: served as an advisor for MSD, Nanobiotics, BMS, AstraZeneca, and Merck Serono and received institutional research funding from BMS, Merck Serono, Roche, and Sanofi. NM: participated on Merck and MSD advisory boards. MS: participated on BMS advisory board and received travel grants from MSD. RG: participated on MSD and Merck advisory boards, received honoraria as a speaker for Merck and MSD, and travel grants from MSD, BMS, and Merck. LR: received travel grants from Merck and MSD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1220640/full#supplementary-material
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
2. Jefferies S, Eeles R, Goldgar D, A'Hern R, Henk JM, Gore M, et al. The role of genetic factors in predisposition to squamous cell cancer of the head and neck. Br J Cancer. (1999) 9:865–7. doi: 10.1038/sj.bjc.6690138
3. Goldenberg D, Lee J, Koch WM, Kim MM, Trink B, Sidransky D, et al. Habitual risk factors for head and neck cancer. Otolaryngology–Head Neck Surgery. (2004) 131:986–93. doi: 10.1016/j.otohns.2004.02.035
4. Galbiatti ALS, Padovani-Junior JA, Maníglia JV, Rodrigues CDS, Pavarino ÉC, Goloni-Bertollo EM. Head and neck cancer: causes, prevention and treatment. Braz J Otorhinolaryngol. (2013) 79:239–47. doi: 10.5935/1808-8694.20130041
5. Howlder N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, et al. SEER cancer statistics review (CSR) 1975-2018. SEER cancer statistics review, 1975-2018. Bethesda, MD: National Cancer Institute. (2021). Available at: https://seer.cancer.gov/csr/1975_2018/.
6. Bugter O, Iwaarden DLP, Dronkers EAC, de Herdt MJ, Wieringa MH, Verduijn GM, et al. Survival of patients with head and neck cancer with metachronous multiple primary tumors is surprisingly favorable. Head Neck. (2019) 41:1648–55. doi: 10.1002/hed.25595
7. Lacas B, Carmel A, Landais C, Wong SJ, Licitra L, Tobias JS, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 107 randomized trials and 19,805 patients, on behalf of MACH-NC Group. Radiother Oncol. (2021) 156:281–93. doi: 10.1016/j.radonc.2021.01.013
8. Adelstein DJ, Li Y, Adams GL, Wagner H Jr, Kish JA, Ensley JF, et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol. (2003) 21:92–8. doi: 10.1200/JCO.2003.01.008
9. Al-Sarraf M. Treatment of locally advanced head and neck cancer: historical and critical review. Cancer Control. (2002) 9:387–99. doi: 10.1177/107327480200900504
10. Le X, Hanna EY. Optimal regimen of cisplatin in squamous cell carcinoma of head and neck yet to be determined. Ann Transl Med. (2018) 6:229–9. doi: 10.21037/atm.2018.05.10
11. Al-Mamgani A, de Ridder M, Navran A, Klop WM, de Boer JP, Tesselaar ME. The impact of cumulative dose of cisplatin on outcome of patients with head and neck squamous cell carcinoma. Eur Arch Oto-Rhino-Laryngol. (2017) 274:3757–65. doi: 10.1007/s00405-017-4687-4
12. Helfenstein S, Riesterer O, Meier UR, Papachristofilou A, Kasenda B, Pless M, et al. 3-weekly or weekly cisplatin concurrently with radiotherapy for patients with squamous cell carcinoma of the head and neck – a multicentre, retrospective analysis. Radiat Oncol. (2019) 14:32. doi: 10.1186/s13014-019-1235-y
13. Wolff HA, Overbeck T, Roedel RM, Hermann RM, Herrmann MK, Kertesz T, et al. Toxicity of daily low dose cisplatin in radiochemotherapy for locally advanced head and neck cancer. J Cancer Res Clin Oncol. (2009) 135:961–7. doi: 10.1007/s00432-008-0532-x
14. Geoffrois L, Martin L, de Raucourt D, Sun XS, Tao Y, Maingon P, et al. Induction chemotherapy followed by cetuximab radiotherapy is not superior to concurrent chemoradiotherapy for head and neck carcinomas: results of the GORTEC 2007-02 phase III randomized trial. J Clin Oncol. (2018) 36:3077–83. doi: 10.1200/JCO.2017.76.2591
15. Spreafico A, Huang SH, Xu W, Granata R, Liu CS, Waldron JN, et al. Impact of cisplatin dose intensity on human papillomavirus-related and unrelated locally advanced head and neck squamous cell carcinoma. Eur J Cancer. (2016) 67:174–82. doi: 10.1016/j.ejca.2016.08.013
16. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargente D, Ford R, et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer. (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
17. Dunst J, Hildebrandt G, Becker-Schiebe M, Kuhnt T, Weykamp F, Richetti A, et al. Assessment of therapeutic COMpliance of patients treated with cisPLatin plus radiotherapY in locally advanced squamous cell carcinoma of the head and neck—first results of the retrospective, anonymized, observational, European, multicenter COMPLY trial. Poster presented at 6th Trends in Head and Neck Oncology (THNO), Nice., France (2017). Abstract P15.
18. Espeli V, Zucca E, Ghielmini M, Giannini O, Salatino A, Martucci F, et al. Weekly and 3-weekly cisplatin concurrent with intensity-modulated radiotherapy in locally advanced head and neck squamous cell cancer. Oral Oncol. (2012) 48:266–71. doi: 10.1016/j.oraloncology.2011.10.005
19. Jacobs C, Lyman G, Velez-García E, Sridhar KS, Knight W, Hochster H, et al. A phase III randomized study comparing cisplatin and fluorouracil as single agents and in combination for advanced squamous cell carcinoma of the head and neck. J Clin Oncol. (1992) 10:257–63. doi: 10.1200/JCO.1992.10.2.257
20. Machiels JP, Rene Leemans C, Golusinski W, Grau C, Licitra L, Gregoire V, et al. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2020) 31:1462–75. doi: 10.1016/j.annonc.2020.07.011
21. Porceddu SV, Scotte F, Aapro M, Salmio S, Castro A, Launay-Vacher V, et al. Treating patients with locally advanced squamous cell carcinoma of the head and neck unsuitable to receive cisplatin-based therapy. Front Oncol. (2020) 9:1522. doi: 10.3389/fonc.2019.01522
22. Su C, Zhou F, Shen J, Zhao J, O’Brien M. Treatment of elderly patients or patients who are performance status 2 (PS2) with advanced Non-Small Cell Lung Cancer without epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) translocations – Still a daily challenge. Eur J Cancer. (2017) 83:266–78. doi: 10.1016/j.ejca.2017.07.002
23. Ahn MJ, D’Cruz A, Vermorken JB, Chen JP, Chitapanarux I, Dang HQ, et al. Clinical recommendations for defining platinum unsuitable head and neck cancer patient populations on chemoradiotherapy: A literature review. Oral Oncol. (2016) 53:10–6. doi: 10.1016/j.oraloncology.2015.11.019
24. Fasano M, D’Onofrio I, Belfiore MP, Angrisani A, Caliendo V, Della Corte CM, et al. Head and neck squamous cell carcinoma in elderly patients: role of radiotherapy and chemotherapy. Cancers (Basel). (2022) 14:472. doi: 10.3390/cancers14030472
25. Kiyota N, Tahara M, Fuji H, Yamazaki T, Hiroki Mitani H, Iwae S, et al. Phase II/III trial of post-operative chemoradiotherapy comparing 3-weekly cisplatin with weekly cisplatin in high-risk patients with squamous cell carcinoma of head and neck (JCOG1008). J Clin Oncol. (2020) 38:6502. doi: 10.1200/JCO.2020.38.15_suppl.6502
26. Kiyota N, Tahara M, Mizusawa J, Kodaira T, Fujii H, Yamazaki T, et al. Weekly cisplatin plus radiation for postoperative head and neck cancer (JCOG1008): A multicenter, noninferiority, Phase II/III randomized controlled trial. J Clin Oncol. (2022) 40:1980–90. doi: 10.1200/JCO.21.01293
27. Szturz P, Vermorken JB. High-Dose Three-Weekly or Low-Dose Weekly Cisplatin during Radiation, What to Prefer? In: Vermorken JB, Budach V, René Leemans C, et al, editors. Critical Issues in Head and Neck Oncology. Cham, Switzerland: Springer (2021). p. 139–54. doi: 10.1007/978-3-030-63234-2_10
28. Narvaez CA, Schild SE, Janssen S, Schroeder U, Bruchhage KL, Hakim SG, et al. Accelerated fractionation with concomitant boost vs. conventional radio-chemotherapy for definitive treatment of locally advanced squamous cell carcinoma of the head-and-neck (SCCHN). Anticancer Res. (2021) 41:477–84. doi: 10.21873/anticanres.14798
29. Yokota T, Shibata M, Hamauchi S, Shirasu H, Onozawa Y, Ogawa H, et al. Feasibility and efficacy of chemoradiotherapy with concurrent split-dose cisplatin after induction chemotherapy with docetaxel/cisplatin/5-fluorouracil for locally advanced head and neck cancer. Mol Clin Oncol. (2020) 13:35. doi: 10.3892/mco.2020.2105
Keywords: SCCHN, concurrent chemotherapy, cisplatin, compliance, radiotherapy
Citation: Varges Gomes A, Castro G Jr., de Oliveira TB, Colmenero AM, Ribeiro L, Psyrri A, Magné N, Plana Serrahima M, Marinho J, Giglio R, Iglesias Rey L, Angel M and Macedo AM (2024) Retrospective study of cisplatin plus radiotherapy toxicities in locally advanced squamous cell carcinoma of the head and neck – ReCisTT study. Front. Oncol. 14:1220640. doi: 10.3389/fonc.2024.1220640
Received: 16 May 2023; Accepted: 13 September 2024;
Published: 14 October 2024.
Edited by:
Zhiyu Zhang, Fourth Affiliated Hospital of China Medical University, ChinaReviewed by:
Jozsef Dudas, Innsbruck Medical University, AustriaNerina Denaro, IRCCS Ca ‘Granda Foundation Maggiore Policlinico Hospital, Italy
Copyright © 2024 Varges Gomes, Castro, de Oliveira, Colmenero, Ribeiro, Psyrri, Magné, Plana Serrahima, Marinho, Giglio, Iglesias Rey, Angel and Macedo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Varges Gomes, YW5hZm1mZXJyZWlyYUB5YWhvby5jb20=