 Valentina A. Zavala1
Valentina A. Zavala1 Sandro Casavilca-Zambrano2
Sandro Casavilca-Zambrano2 Jeannie Navarro-Vásquez3
Jeannie Navarro-Vásquez3 Lizeth I. Tamayo4
Lizeth I. Tamayo4 Carlos A. Castañeda5
Carlos A. Castañeda5 Guillermo Valencia5
Guillermo Valencia5 Zaida Morante5Mónica Calderón5Julio E. Abugattas6
Zaida Morante5Mónica Calderón5Julio E. Abugattas6 Henry L. Gómez5Hugo A. Fuentes5
Henry L. Gómez5Hugo A. Fuentes5 Ruddy Liendo-Picoaga7
Ruddy Liendo-Picoaga7 Jose M. Cotrina6
Jose M. Cotrina6 Silvia P. Neciosup5Katia Roque5Jule Vásquez5Luis Mas5
Silvia P. Neciosup5Katia Roque5Jule Vásquez5Luis Mas5 Marco Gálvez-Nino5
Marco Gálvez-Nino5 Laura Fejerman1,8*†
Laura Fejerman1,8*† Tatiana Vidaurre5†
Tatiana Vidaurre5†- 1Department of Public Health Sciences, University of California, Davis, Davis, CA, United States
- 2Instituto Nacional de Enfermedades Neoplásicas, Departamento de Patología, Lima, Peru
- 3Instituto Nacional de Enfermedades Neoplásicas, Departamento de Investigación, Lima, Peru
- 4Department of Public Health Sciences, The University of Chicago, Chicago, IL, United States
- 5Instituto Nacional de Enfermedades Neoplásicas, Departamento de Oncología Médica, Lima, Peru
- 6Instituto Nacional de Enfermedades Neoplásicas, Departamento de Cirugía de Mamas y tumores Blandos, Lima, Peru
- 7Instituto Nacional de Enfermedades Neoplásicas, Banco de Tumores, Lima, Peru
- 8University of California Davis Comprehensive Cancer Center, University of California, Davis, Davis, CA, United States
Introduction: Breast cancer is a heterogeneous disease, and the distribution of the different subtypes varies by race/ethnic category in the United States and by country. Established breast cancer-associated factors impact subtype-specific risk; however, these included limited or no representation of Latin American diversity. To address this gap in knowledge, we report a description of demographic, reproductive, and lifestyle breast cancer-associated factors by age at diagnosis and disease subtype for The Peruvian Genetics and Genomics of Breast Cancer (PEGEN-BC) study.
Methods: The PEGEN-BC study is a hospital-based breast cancer cohort that includes 1943 patients diagnosed at the Instituto Nacional de Enfermedades Neoplásicas in Lima, Peru. Demographic and reproductive information, as well as lifestyle exposures, were collected with a questionnaire. Clinical data, including tumor Hormone Receptor (HR) status and Human Epidermal Growth Factor Receptor 2 (HER2) status, were abstracted from electronic medical records. Differences in proportions and mean values were tested using Chi-squared and one-way ANOVA tests, respectively. Multinomial logistic regression models were used for multivariate association analyses.
Results: The distribution of subtypes was 52% HR+HER2-, 19% HR+HER2+, 16% HR-HER2-, and 13% HR-HER2+. Indigenous American (IA) genetic ancestry was higher, and height was lower among individuals with the HR-HER2+ subtype (80% IA vs. 76% overall, p=0.007; 152 cm vs. 153 cm overall, p=0.032, respectively). In multivariate models, IA ancestry was associated with HR-HER2+ subtype (OR=1.38,95%CI=1.06-1.79, p=0.017) and parous women showed increased risk for HR-HER2+ (OR=2.7,95%CI=1.5-4.8, p<0.001) and HR-HER2- tumors (OR=2.4,95%CI=1.5-4.0, p<0.001) compared to nulliparous women. Multiple patient and tumor characteristics differed by age at diagnosis (<50 vs. >=50), including ancestry, region of residence, family history, height, BMI, breastfeeding, parity, and stage at diagnosis (p<0.02 for all variables).
Discussion: The characteristics of the PEGEN-BC study participants do not suggest heterogeneity by tumor subtype except for IA genetic ancestry proportion, which has been previously reported. Differences by age at diagnosis were apparent and concordant with what is known about pre- and post-menopausal-specific disease risk factors. Additional studies in Peru should be developed to further understand the main contributors to the specific age of onset and molecular disease subtypes in this population and develop population-appropriate predictive models for prevention.
Introduction
Globally, breast cancer is the most commonly diagnosed cancer and the leading cause of cancer death in women (1, 2). Breast cancer risk and mortality vary based on several risk factors. Age, race/ethnicity category, family history, genetics, lifestyle, anthropometric, reproductive, and hormonal factors have been associated with the risk of developing breast cancer (3–5). In addition, tumor subtype, socioeconomic status, education level, and access to care have been shown to impact mortality after diagnosis (6, 7). Analyses stratified by race/ethnicity category have shown that despite sharing risk factors for developing breast cancer, disease risk, clinical characteristics, and risk of mortality differ between populations (6, 8–10). For example, U.S. Hispanics/Latinas (H/Ls) are less likely to develop breast cancer than non-Hispanic White (NHW) and African American women (11). However, after diagnosis, H/L women are at higher risk of mortality compared with NHW women (12).
The use of gene expression profiles for molecular classification of breast cancer tumors (i.e., PAM50) has identified three main intrinsic subtypes: Luminal (A and B), HER2-enriched, and Basal-like (13, 14). A combination of immunohistochemical markers for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor 2 (HER2) are routinely used in clinic to classify tumors into these subtypes and to provide relevant information for individualized therapeutic decision making. Hormone receptor (HR) positive tumors, defined by ER and/or PR expression, are classified as HR+HER2− and HR+HER2+, based on the HER2 expression status, and are overrepresented among luminal intrinsic subtypes. HR−HER2+ and HR−HER2− are overrepresented among HER2-enriched and basal-like subtypes, respectively. Besides chemotherapy, patients with an HR+ disease diagnosis can benefit from endocrine therapy, such as tamoxifen or aromatase inhibitors (15), whereas patients with HER2+ tumors can be treated with anti-HER2 therapy (mainly trastuzumab and pertuzumab) (16). For the HR−HER2− subtype, treatment options are limited. Currently, these patients receive systemic therapy, although targeted therapies, such as PARP and immune checkpoint inhibitors, are being evaluated in clinical trials and approved for BRCA1 and BRCA2 mutation carriers (17).
Multiple studies have suggested heterogeneity in the association between established breast cancer risk factors and tumor subtype. Family history of breast cancer in a first-degree relative is associated with increased breast cancer risk (3, 18, 19), and specific patterns of cancer family history increase the risk of particular tumor subtypes (20, 21). For example, having one first-degree relative with a history of breast cancer was shown to be associated with increased risk of HR+ subtypes, whereas having two or more was associated with increased risk of HR− disease. (20, 21). However, some studies have failed to confirm these findings (3, 22–24). Among reproductive factors, early menarche, and late menopause increase the risk of developing breast cancer (3, 20, 25–27) with no evidence of heterogeneity by tumor subtype (3, 20, 26, 27). Parity is associated with reduced risk of HR+ disease (3, 19, 20, 27–33) and increased odds for developing HR− subtypes (3, 24, 27, 31, 33–35) in populations of European and African origins. Some studies have reported that older age at first full-term pregnancy was associated with increased risk of HR+ disease (27, 28, 30). Longer breastfeeding history is associated with reduced breast cancer risk with lower odds of developing HR− tumors (19, 20, 25–28, 30–34, 36). Among African Americans, prolonged lactation is associated with reduced risk of HR−, but not HR+ disease, with an increased risk of HR− disease among parous women who have not breastfed (34, 37). This observation has also been described among NHW women (32). Reports on lifestyle factors, such as alcohol intake and smoking history, have shown heterogeneity by tumor subtype, with a stronger association with HR+HER2− subtypes (3, 38).
The effects of some of the abovementioned factors are different among pre- and post-menopausal women. Controversial evidence shows that high BMI (obesity) is protective against breast cancer in premenopausal women, and conversely, it suggests that obesity increases the risk in postmenopausal women (39, 40), especially for HR+ subtypes (41–43). Other factors known to affect breast cancer risk in both groups in the same direction can present different magnitudes of the effect by menopausal status, such as alcohol intake (44), physical activity (45, 46), and breastfeeding (47).
Previous studies have assessed the association of breast cancer risk with numerous structural, social, environmental, and genetic factors (4, 48–50); however, these studies are primarily composed of individuals of European origin. Few breast cancer studies describe patient characteristics in Latin America (26, 51–54), a region characterized by cultural and genetic heterogeneity (55–57). For example, Indigenous American genetic ancestry estimates vary across different Latin American countries, ranging between ~5% in Puerto Rico and ~80% in Peru and Bolivia (56–58). Previous studies have identified that the degree of Indigenous American genetic ancestry may modify the magnitude and direction of association with currently known breast cancer risk variants among H/L women (59) and is associated with differential lifestyle risk factors (60). Latin American cohorts with high proportions of Indigenous American ancestry are underrepresented in breast cancer research (61).
The Peruvian Genetics and Genomics of Breast Cancer Study (PEGEN-BC) is a hospital-based cohort including patients from the Instituto Nacional de Enfermedades Neoplásicas (INEN) in Lima, Peru. We have previously described the distribution of demographic, anthropometric, reproductive, lifestyle, and clinical factors for 1,312 breast cancer participants, with an emphasis on the distribution by breast tumor subtypes (62). Moreover, we reported that increasing Indigenous American ancestry is associated with higher odds of developing the HR−HER2+ subtype (62). The current report aims to provide a more complete and updated description of these variables by tumor subtype and age at diagnosis, including a total of 1,943 breast cancer patients, highlighting potential heterogeneity in the latter categories.
Methods
Study participants
The Peruvian Genetics and Genomics of Breast Cancer Study (PEGEN-BC) is a hospital-based cohort study. As of April 2022, we have recruited 1,943 participants from the INEN in Lima, Peru. Women were invited to participate if they had a diagnosis of invasive breast cancer in 2010 or later and were between 21 and 79 years of age when diagnosed. A blood sample was drawn by a certified phlebotomist at the INEN central laboratory. The present report includes analyses with a subset of 1,796 patients with available genetic ancestry estimates (63). This study was approved by the INEN and the University of California Davis Institutional Review Boards. All individuals provided written informed consent to participate.
Data collection
Each PEGEN-BC participant completed a standardized survey administered by a trained research coordinator at INEN. The survey includes questions regarding anthropometric (weight and height), demographic (place of birth and residence), lifestyle (alcohol intake and smoking history), and reproductive (menopause status, age at first pregnancy, number of full-term pregnancies, and breastfeeding history) variables, and family history of breast cancer. Weight and height were assessed by trained nurses/professionals at INEN at the time of diagnosis. Body mass index (BMI) was calculated as weight (kilograms) divided by height (meters) squared and categorized as underweight (BMI < 18.5 kg/m 2), normal (BMI ≥ 18.5 < 25 kg/m2), overweight (BMI ≥ 25 < 30 kg/m 2), and obese (BMI ≥ 30 kg/m2). Alcohol use was assessed as the self-reported frequency of glasses of alcohol consumed per day and categorized as < 1 glass/day, > 1 glass/day, and non-drinker (never). Smoking status was classified into “ever” (current and former) and “never.” If there was a history of familial breast cancer, the relative (i.e., mother, sister, and aunt) was indicated to determine cases with breast cancer family history in a first-degree relative. Clinical variables, including ER, PR, HER2, lymph node status, tumor grade, and clinical stage, were extracted from electronic records.
Genetic ancestry estimates for 1,796 PEGEN-BC participants were available from a previous study (63). Briefly, genome-wide genotype data obtained with the Affymetrix Precision Medicine Array were pruned using PLINK v.1.9 (64) [window size = 50, number of variants = 5, variance inflation factor threshold = 2] and merged with data from four reference populations from the 1000 Genomes project (65): Admixed Americans (Peru, Colombia, Mexico, Puerto Rico), Europeans (Americans with Northern and Western European Ancestry, Italy, Spain, Finland, Scotland), East Asians (China, Japan, Vietnam), and African populations (Nigeria, Kenya, Gambia, Sierra Leone). Individual continental, global genetic ancestry was estimated using ADMIXTURE (66) (unsupervised, k = 4), including 122,605 independent variants. The PEGEN-BC study includes a large proportion of patients with > 98% Indigenous American ancestry, as previously reported (62), and therefore provides a source of non-admixed reference samples for this component.
Tumoral tissues were obtained from core biopsy or freshly resected invasive breast cancers pre-treatment that were formalin-fixed and paraffin-embedded following standard protocols at INEN. Tumor subtypes were defined using immunohistochemistry (IHC) markers by a certified pathologist at INEN. HR positivity was defined at 1% or more cells showing ER and/or PR staining. HER2 positivity was defined as 3+ staining by IHC or by gene amplification detected by fluorescence in situ hybridization following a 2+ (borderline) IHC result. These markers were used to classify tumors as HR+HER2−, HR+HER2+, HR−HER2+, and HR−HER2−. Two independent pathologists from the University of California San Francisco reviewed the IHC slides at INEN for a subset of 52 patients. The concordance rate was 100% for ER, 87% for PR, and 85% for HER2. Most of the discordant calls for HER2 were scored as “negative” or 1+ at INEN and 2+ by the independent pathologists. Immunohistochemical subtype classification was not available for 141 samples (7%).
Statistical analysis
We performed descriptive analyses of available demographic, anthropometric, reproductive, and clinical characteristics by breast cancer subtype. Differences in characteristics between tumor subtypes were tested by means of one-way ANOVA for normally distributed continuous variables and Chi-squared tests for categorical variables. Age at first full-term pregnancy presented a non-normal distribution; therefore, it was log2 transformed. The correlation between genetic ancestry and continuous and categorical variables was performed using Pearson’s correlation coefficient test and Point-Biserial Correlation Coefficient, respectively. Multinomial logistic regression models were used to calculate odds ratios (ORs) and 95% confidence intervals (CI) for the association of multiple variables and subtype-specific breast cancer. East Asian and African ancestry proportions were not included in multivariable models due to the low contribution of these components and high correlation with the Indigenous American/European axis of ancestry variation. P-values (P) <= 0.05 were considered statistically significant. All analyses were conducted in R v.3.6.0 (67).
Results
Demographics, anthropometrics, and lifestyle factors in the PEGEN-BC study by tumor subtype
The most common breast cancer subtype among PEGEN-BC study participants was HR+HER2− (52.4%), followed by HR+HER2+ (18.7%), HR−HER2− (16.0%), and HR−HER2+ (12.9%) (Table 1). The average age at diagnosis was 49.8 years (SD = 11), and differences by tumor subtype were not statistically significant (p = 0.087). PEGEN-BC study patients included individuals born in the three main biogeographic regions of Peru (Figure 1): The Coastal (55.5%), Mountainous (36.4%), and Amazonian (7.5%) regions. Less than 1% of the patients were born in another country (mainly Venezuela). These groups did not show statistically significant differences in their distribution by tumor subtype (Table 1). Most patients resided in the Coastal region (7%), and differences in the proportion of patients who resided in each biogeographic area by tumor subtype category were not statistically significant (Table 1).
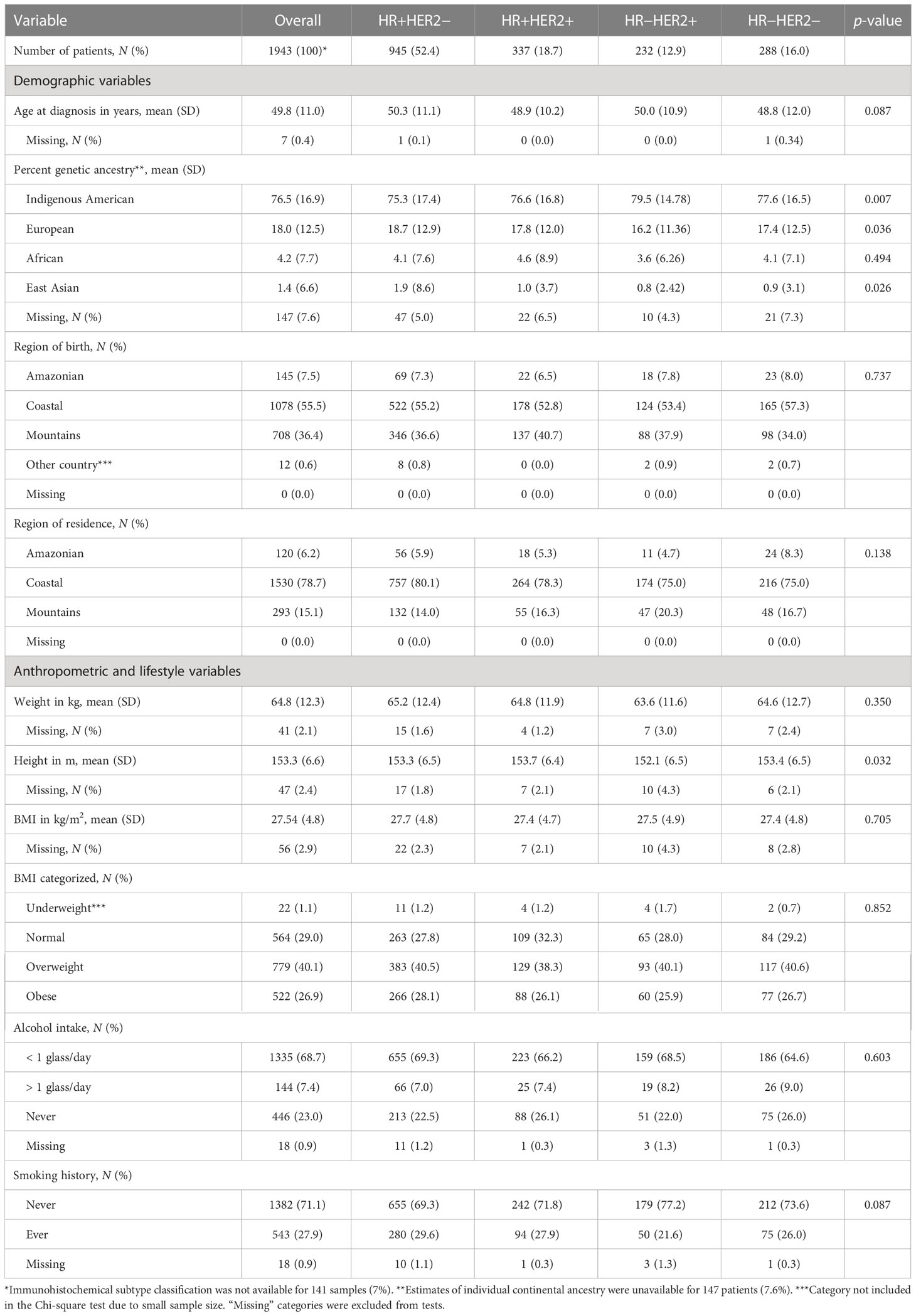
Table 1 Distribution of demographic, lifestyle, and anthropometric characteristics of PEGEN-BC patients overall and by tumor subtype.

Figure 1 Biogeographical regions of Peru. Red star shows the location of INEN. This figure was created using the ggmap, maps, and mapdata R packages.
Estimates of individual continental genetic ancestry were available for 1,796 patients. Average Indigenous American ancestry among patients was 76.5%, followed by 18.0% European, 4.2% African, and 1.4% East Asian (Table 1). Furthermore, 92% of PEGEN-BC study participants had > 50% of Indigenous American ancestry, 25% at least 90%, and 12% at least 95% of Indigenous American ancestry (Figure 2A). Seven patients (0.4%) had more than 50% of East Asian ancestry, and eight (0.4%) had more than 50% African ancestry. Principal components analysis showed that the PEGEN-BC patients defined the Indigenous American cluster along principal component (PC) 1 when compared against 1000 Genomes Project reference populations (Figures 2B, C), reflecting the high degree of Indigenous American genetic ancestry that characterizes this cohort.
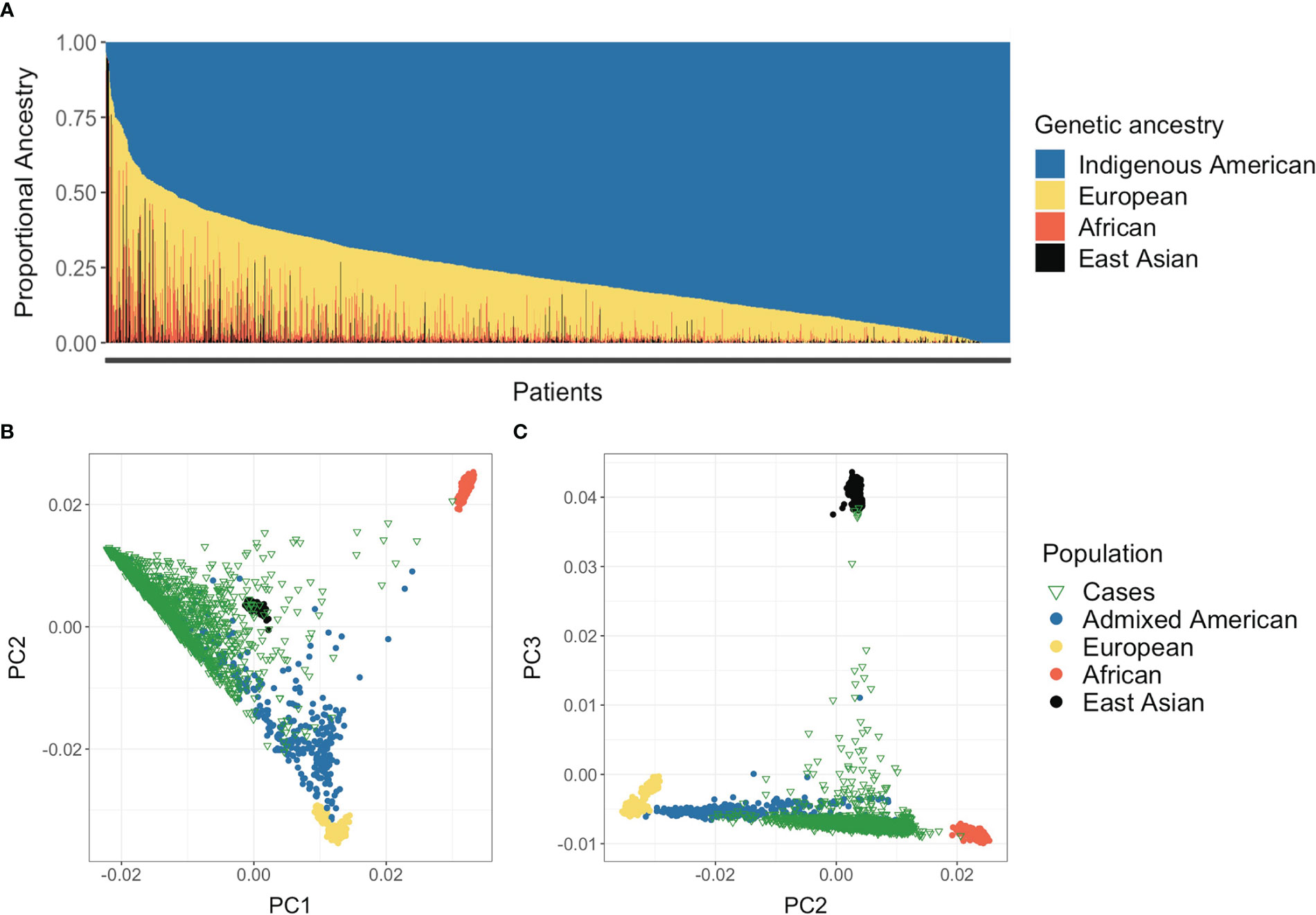
Figure 2 Population genetic structure of the PEGEN-BC study participants. (A) ADMIXTURE continental ancestry estimates obtained in unsupervised analysis, assuming K = 4. (B, C) Principal components analysis (PCA) including breast cancer patients and 1000 Genomes Project individuals. The first three principal components are shown.
We found that the average Indigenous American ancestry proportion of participants was different across tumor subtypes. Individuals diagnosed with HR−HER2+ tumors showed the highest average proportion of Indigenous American ancestry (79.5%, SD = 15) (Table 1).
The average height of patients was 153.3 cm (SD = 6.6), with lower average height among patients diagnosed with HR−HER2+ tumors compared with all other subtypes (152.1 vs. ~153.6 cm, p = 0.032). There were no statistically significant differences in weight or BMI by tumor subtype, with a large overall proportion of patients being overweight (40.1%) (Table 1).
Most PEGEN-BC patients (68.7%) reported low levels of alcohol consumption (< 1 glass/day), whereas 7.4% reported consuming more than one glass per day. Moreover, 27.9% of participants reported being a current or past smoker. There was no statistically significant association between alcohol consumption, smoking history, and tumor subtype (Table 1).
Demographic, anthropometric, and lifestyle variables that did not show statistically significant differences by tumor subtypes did not show significant differences by HR status either (Supplementary Table S1).
Reproductive variables by tumor subtype
The average age at menarche among PEGEN-BC patients was 12.9 years (SD = 1.7), the average age at first full-term pregnancy was 23.2 years (SD = 5.7), and the average number of full-term pregnancies was 2.42 (SD = 1.8). Most study participants reported having had at least one child (83.5%), and 80% of parous women had at least two children (Table 2). The frequency of parous women and number of births differed by tumor subtype, being higher among HR− tumors (p < 0.001) (Table 2).
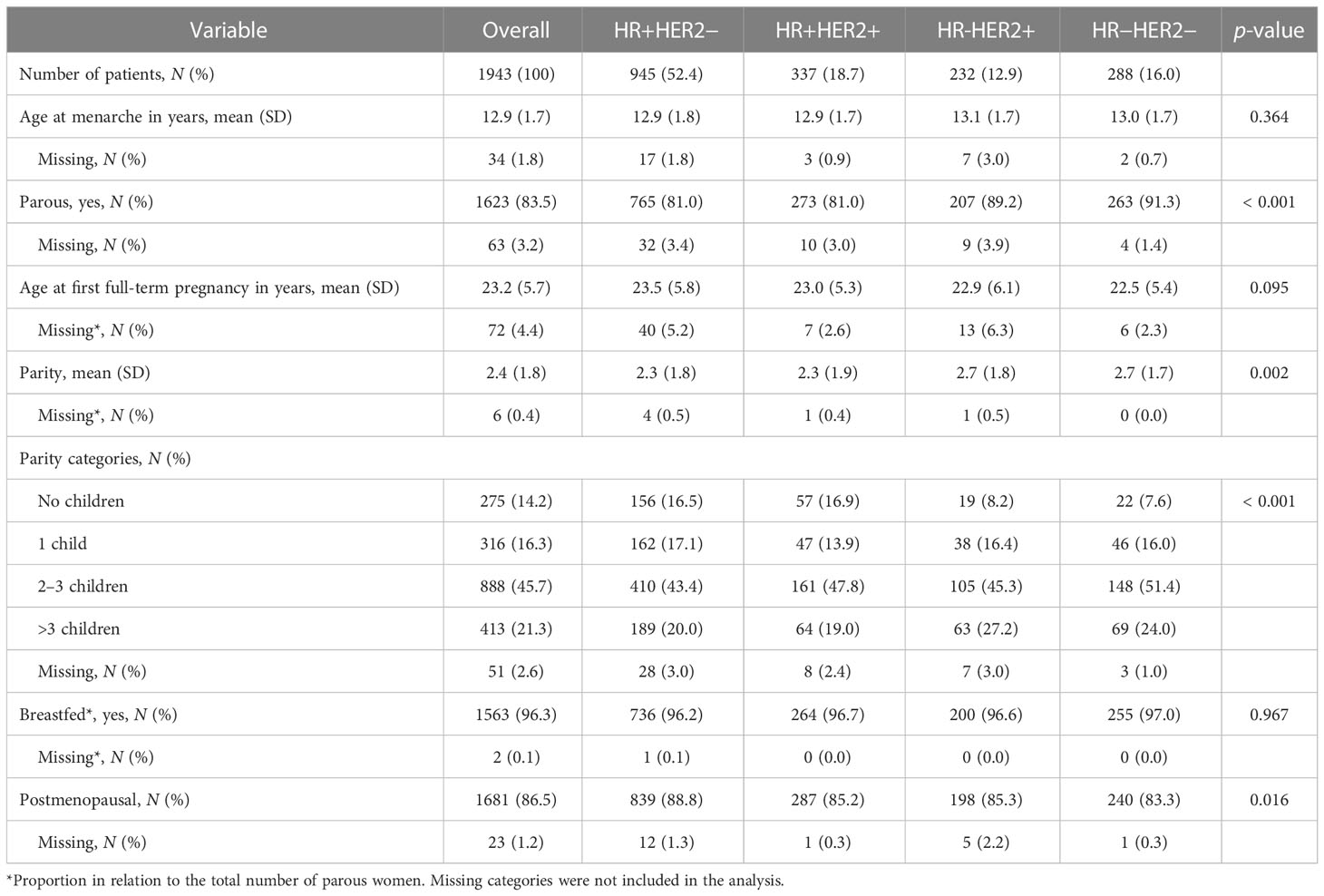
Table 2 Distribution of reproductive variables overall and by tumor subtype.
Breastfeeding was a common practice among parous women (96.3%), and we did not observe the differences in the proportion of women who breastfed their children by tumor subtype category (Table 2).
More than 85% of women reported being menopausal at recruitment. Patients with HR+HER2− tumors were more likely to report being menopausal than patients with other tumor subtypes (p = 0.016). However, since many of these patients had induced menopause due to treatment, we did not consider this variable in subsequent multivariate analyses and stratified by age at diagnosis instead.
All these variables remained significant in analyses stratified by HR status (Supplementary Table S2). In addition, age at first full-term pregnancy showed a higher average age among patients diagnosed with HR+ disease compared with HR− (23.4 vs. 22.7, p = 0.043, Supplementary Table S2).
Clinical characteristics by tumor subtype
Overall, approximately 8% of PEGEN-BC study patients reported a family history of breast cancer in a first-degree relative (Table 3). Differences in breast cancer family history by breast cancer subtype were not statistically significant.
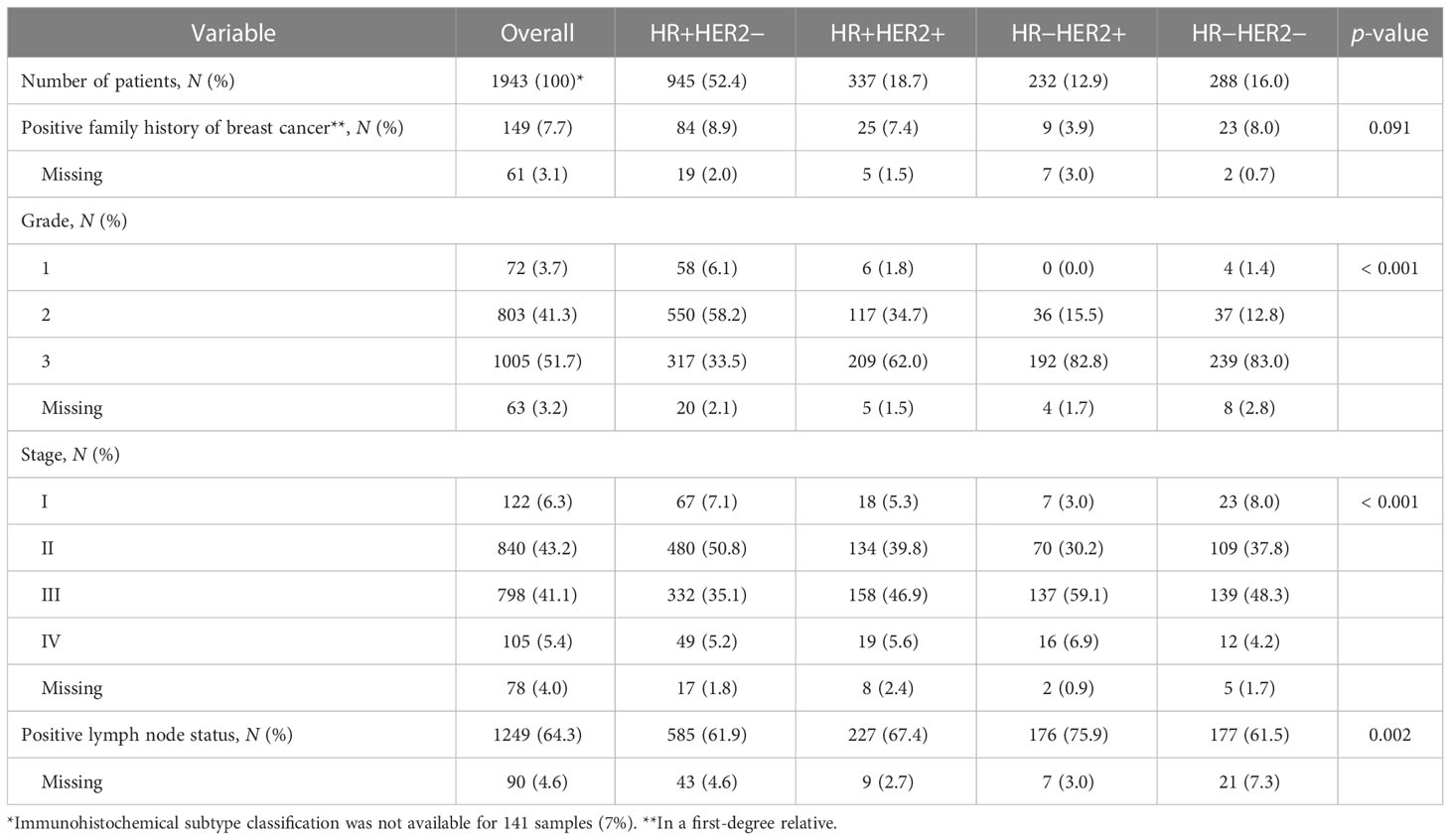
Table 3 Distribution of clinical characteristics of PEGEN-BC study participants overall and by tumor subtype.
More than 90% of patients were diagnosed with Grades 2 and 3 tumors (Table 3). Patients with HR+HER2− tumors were more likely to be diagnosed with Grades 1 and 2 disease, whereas those with HR−HER2+ and HR−HER2− tumors were more likely to be high grade (Table 3). Most PEGEN-BC participants were diagnosed with stage II or III disease, with a larger number of stage I and II diagnoses among HR+HER2− patients than those with other subtypes (Table 3). Concordant with the distribution of tumor stage, we observed a high proportion of positive lymph node status among patients overall (64.3%), with a statistically significantly higher proportion of lymph node positivity among patients with HR−HER2+ tumors compared with those with other disease subtypes (78.2% vs. ~67%) (Table 3). Distribution of these variables by HR status is shown in Supplementary Table S2.
Distribution of patient characteristics by age at diagnosis
We compared the distribution of anthropometric, demographic, reproductive, clinical, and lifestyle risk variables between patients diagnosed before the age of 50 years (N = 981) and at 50 years or older (N = 955). Compared with patients diagnosed at 50 years or older, younger patients had higher average Indigenous American ancestry (78.6 vs. 74.3, p < 0.001); they were more likely to reside in the Mountainous region (17.3% vs. 12.8%, p = 0.015), and they were 1.4 cm taller (p < 0.001) and had lower prevalence of obesity (25.4% vs. 30.0%, p = 0.036) (Table 4). Additionally, there was a higher proportion of older patients with more than three children compared with the younger group (31% vs. 13%, p < 0.001), and a larger proportion of younger patients reported breastfeeding their children (98% vs. 95%, p = 0.001) (Table 5). Regarding clinical characteristics, younger patients reported lower family history of breast cancer in a first-degree relative (6.5% vs. 9.5%, p = 0.02) and presented with more advanced disease (44% diagnosed at stage III compared with 42%, p = 0.017) (Table 5). We did not observe statistically significant differences in subtype distribution between both age categories.
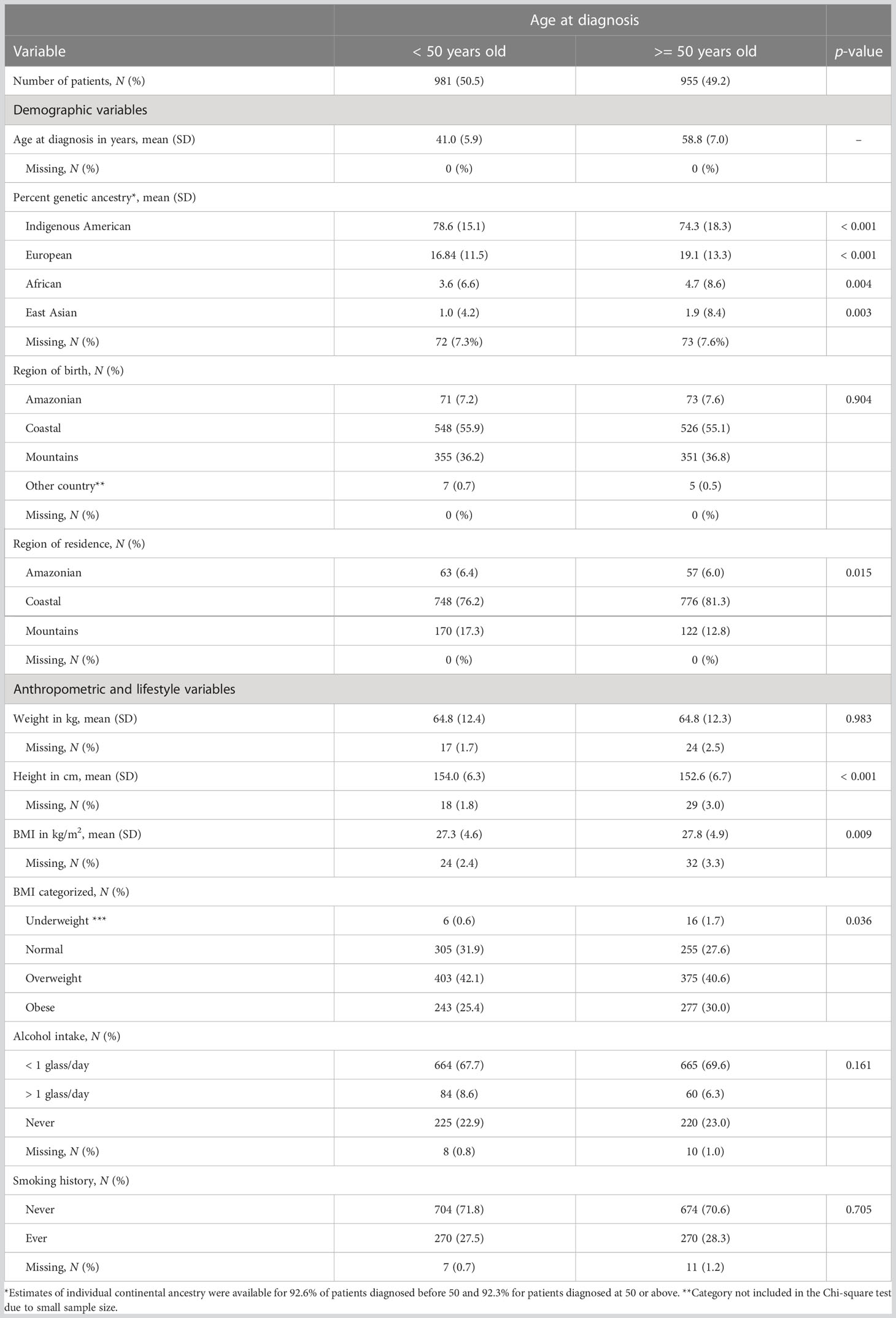
Table 4 Distribution of demographic and anthropometric variables by age at diagnosis categories.
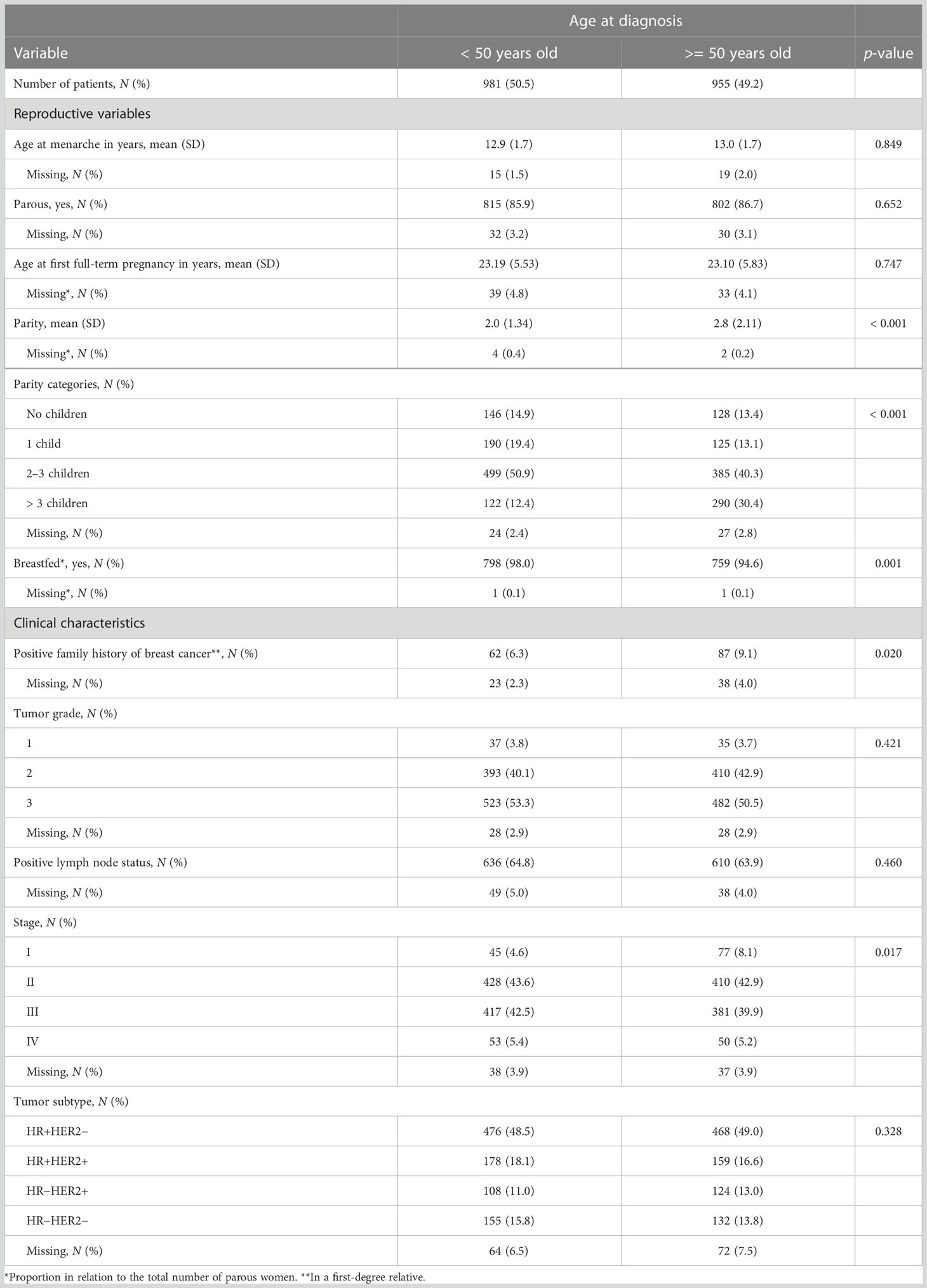
Table 5 Distribution of reproductive and clinical variables by age at diagnosis categories.
Additional stratified analyses comparing demographic, anthropometric, reproductive, and clinical factors by tumor subtype in the two different age groups are included as Supplementary Materials (Supplementary Tables S3 and S4). As additional stratification reduced the number of observations per category, we suggest taking these results with caution.
Correlation between Indigenous American genetic ancestry and other patient and tumor characteristics
We assessed the correlation between Indigenous American ancestry and patient and tumor characteristics to better understand the observed patterns in ancestry distribution and those factors by tumor subtype in the PEGEN-BC study. We observed an inverse correlation between Indigenous American ancestry and age at diagnosis (r = −0.15, p < 0.001), weight (r = −0.11, p < 0.001), height (r = −0.25, p < 0.001), age at first full-term pregnancy (r = −0.08, p = 0.002), family history of breast cancer in a first-degree relative (r = −0.12, p < 0.001), smoking history (r = −0.11, p < 0.001), HR+ status (r = −0.06, p = 0.012) and a positive correlation with age at menarche (r = 0.06, p = 0.017) and HER2+ status (r = 0.053, p = 0.029).
Multivariable analyses testing the association between demographic, lifestyle factors, and breast cancer subtype
Variables that showed statistically significant associations at the 10% level with tumor subtype in the univariate analyses (Tables 1–3) were included in a multivariate model, using HR+HER2− as reference (Table 6). Indigenous American ancestry remained associated with HR−HER2+ subtype (OR per 25% increment in ancestry = 1.38, 95% CI = 1.06–1.79, p = 0.02). Smoking history and height were no longer statistically significantly associated with subtype. Parous women were more likely to be diagnosed with HR−HER2+ (OR = 2.72, 95% CI = 1.53–4.83, p < 0.001) and HR-HER2- (OR = 2.47, 95% CI = 1.51–4.04, p < 0.001) disease compared with the HR+HER2− subtype. Family history of breast cancer in a first-degree relative was not included as a covariate in the multivariate model because the number of patients that reported family history of breast cancer in a first-degree relative was relatively small and rendered unstable estimates when included. We tested models excluding patients with a family history of breast cancer, and results were similar to those using the full dataset (Table 6).
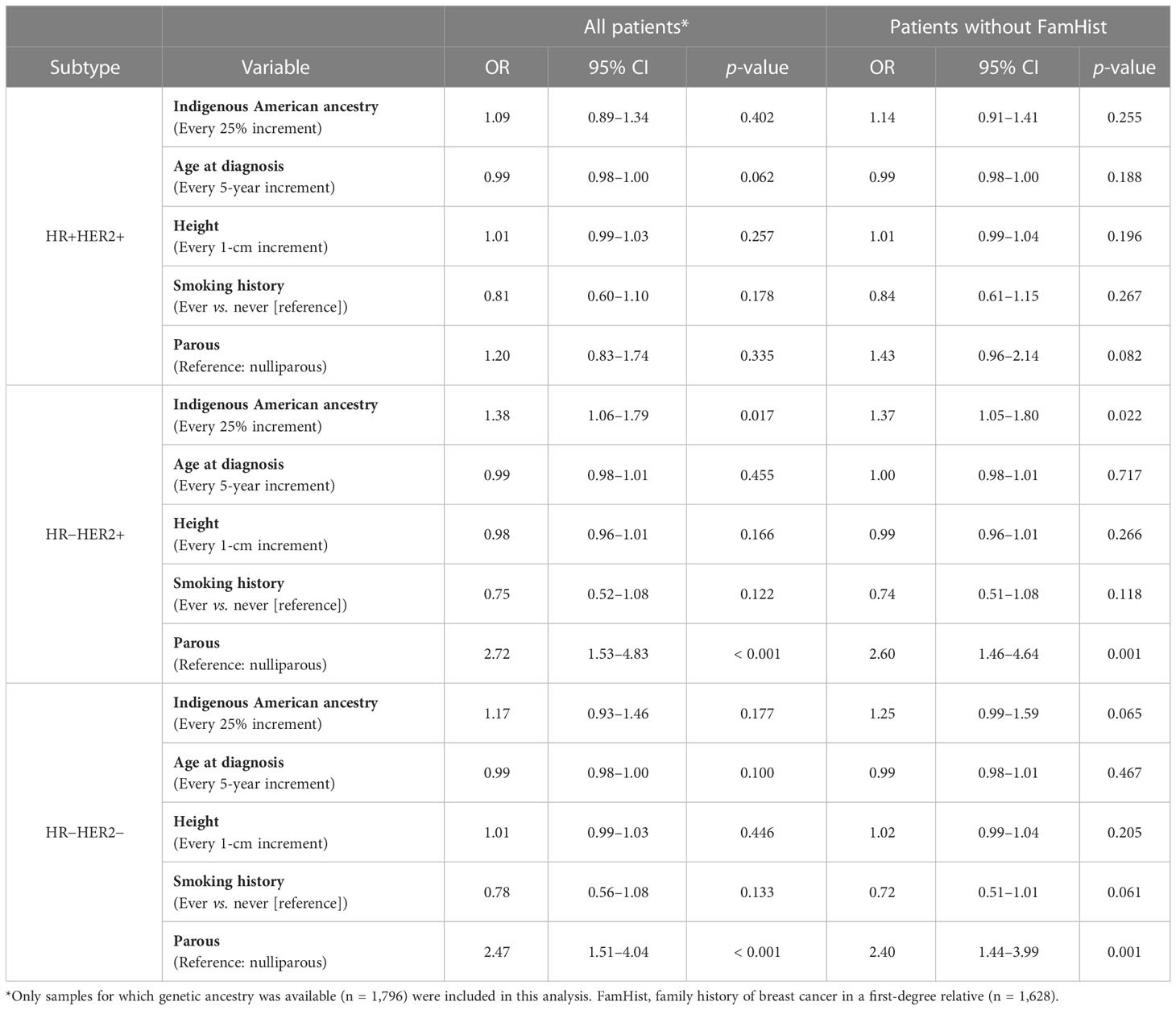
Table 6 Multivariate multinomial logistic regression models testing the association between demographic and lifestyle variables and breast cancer subtype (HR+HER2− as reference).
Indigenous American ancestry, region of residence, height, BMI, breastfeeding history, number of full-term pregnancies, and family history of breast cancer in a first-degree relative showed statistically significant associations at the 10% level with age at diagnosis categories. These variables were included in a multivariate model using age at diagnosis < 50 as reference (Table 7). We found that increasing Indigenous American ancestry and increasing height were associated with reduced odds of being diagnosed at 50 years or older (OR = 0.63, 95% CI = 0.53–0.75, p < 0.001 and OR = 0.96, 95% CI = 0.95–0.98, p < 0.001, respectively). Patients that resided in the Mountainous region had reduced odds of being diagnosed at 50 years of age or older compared with those in the Coastal region (OR = 0.63, 95% CI = 056–0.9, p = 0.004). Breastfeeding was associated with lower odds of being diagnosed at 50 years of age or older (OR = 0.35, 95% CI = 0.2–0.7, p = 0.001). Compared with nulliparous women, giving birth to at least one child increased the odds of being diagnosed at an older age (OR = 1.55, 95% CI = 0.2–0.7, p < 0.001). Increasing BMI was no longer associated with age at diagnosis (Table 7).
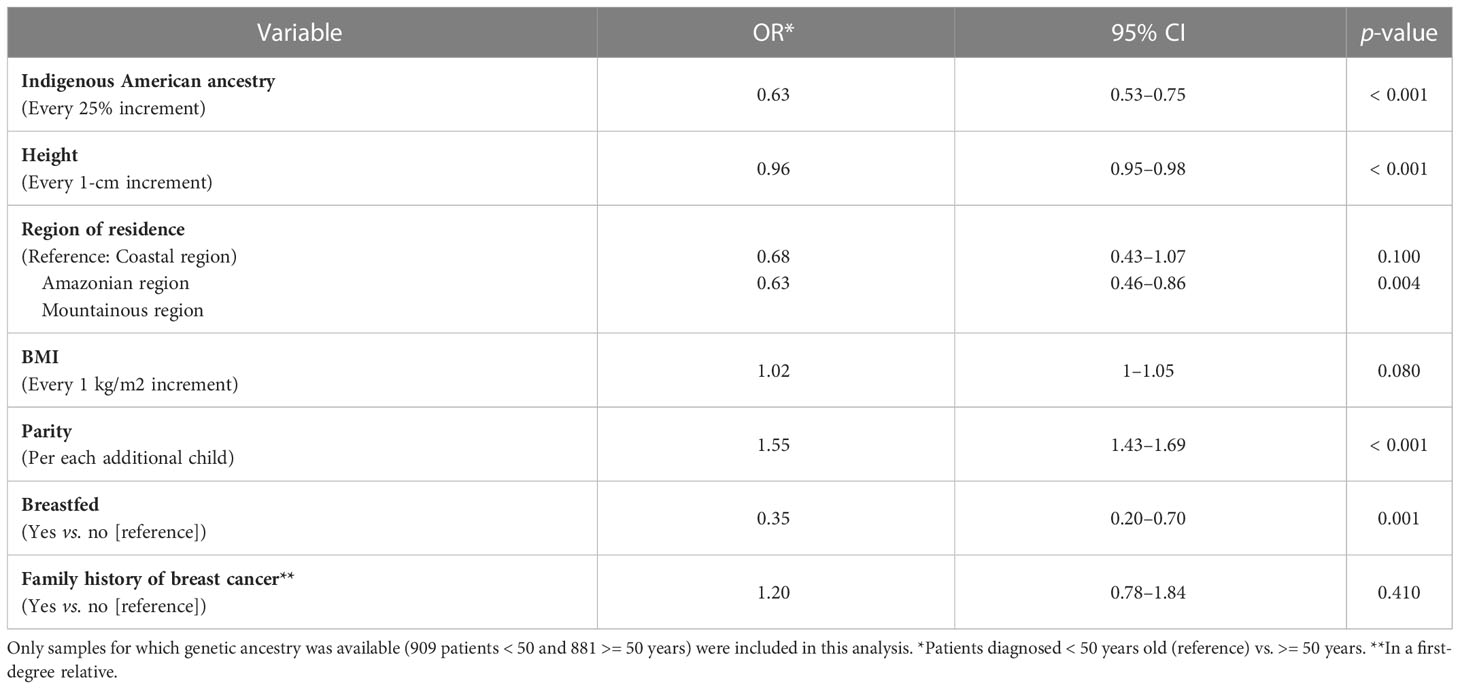
Table 7 Multivariate logistic regression model testing the association between demographic and lifestyle variables and age at diagnosis (< 50 [reference] vs. >= 50).
Discussion
In the present report, we aimed to provide a more complete description of the distribution of anthropometric, demographic, clinical, and known breast cancer–associated risk factors among Peruvian women that are part of The Peruvian Genetics and Genomics of Breast Cancer Study (PEGEN-BC). This work constitutes an update of a previously reported study, including a larger number of recruited patients and extending analyses to describe the distribution of patient characteristics not only by tumor subtype but also by age at diagnosis (62).
Being a hospital-based cohort, the PEGEN-BC study included a large proportion of women who resided in the Coastal region, where the INEN main hospital is located (Figure 1). Despite this bias in terms of residential representation, when looking at place of birth, the proportion of the cohort’s patients from the Coastal region followed closely that of the Peruvian population (58.0% Peru vs. 55.5% of cohort patients). The study has an overrepresentation of patients born in the Mountainous region (28.1% Peru vs. 36.4% of cohort patients) (68) and an underrepresentation of patients born in the Amazonian region (13.9% Peru vs. 7.5% of cohort patients) (68). The proportion of patients within each geographical region is consistent with what has been reported in two studies describing mortality of breast cancer (69) and incidence of triple-negative breast cancer tumors in Peruvian women (70).
A large proportion of patients were overweight/obese (67%), and the prevalence of exposure to alcohol and tobacco was higher than what has been previously reported for Peruvian women (71, 72). The average Indigenous American ancestry among the PEGEN-BC patients is 76.5%, which is higher than the average ancestry proportion of women in other breast cancer studies, including Latin America and U.S. Latinas (12, 51, 60, 73–89). In addition, the average height in our cohort was consistent with what has been reported in the literature for the Peruvian population (90) and with the known inverse correlation with Indigenous American ancestry (91). Overall, some reproductive variables showed a similar trend to what has been reported, including a similar age at menarche (92) and a high breastfeeding rate (93). The number of full-term pregnancies reported here (average of 2.8 children) was more closely related to what has been observed in rural areas of Peru (2.5) compared with urban areas (1.4) (94).
The distribution of tumor subtypes is similar to what has been previously described in other Latin American countries (95), with differences being partially explained by the inclusion of KI-67 expression and tumor grade for subtype classification (95), as indicated by the 2013 St. Gallen consensus (96). This classification criterion was not used in this report since KI-67 was not available for more than 20% of patients, and parameters for subtype determination based on this marker tend to be unstable across populations and studies (97). A study describing patient and tumor characteristics from Peruvian breast cancer patients at INEN diagnosed between 2000 and 2002 (80) (PEGEN-BC patients were recruited if diagnosed in 2010 or later) reported a lower proportion of HR+ tumors compared with PEGEN-BC (62.5% vs. 71.1%). This difference is likely to be explained by the higher positivity percentage cutoff value for HR+ status used in the previous report (10%, compared with 1% in PEGEN-BC), increasing the proportion of HR+ tumors in our cohort. Other characteristics, such as age at diagnosis and stage, presented similar distribution to the PEGEN-BC study cohort.
We found statistically significant differences by tumor subtype for Indigenous American genetic ancestry and height. In addition, we observed suggestive associations for age at diagnosis, family history of breast cancer in a first-degree relative and tobacco exposure. Differences were mostly driven by the HR−HER2+ subtype. Among patients with HR−HER2+ disease, we observed that the average height was lower compared with patients diagnosed with other tumor subtypes and was less likely to report smoking or a positive family history of breast cancer in a first-degree relative. Even though subtype-specific associations have been reported for these variables in other populations (38, 98–101), results in the Peruvian cohort showed that of all the above variables Indigenous American ancestry proportion was the only one that was differentially distributed by tumor subtype in multivariable models.
We did not find statistically significant differences for age at menarche by tumor subtype. Some studies have shown consistent associations between age at menarche and reduced risk of HR+HER2− breast cancer (3, 19, 20). One multicenter study did not find subtype-specific associations (27), consistent with our study. The PRECAMA Study, a Latin American population-based case-control study of premenopausal breast cancer, reported reduced odds for HR− tumors among women who were > 12 years old at menarche, compared with those younger at menarche (26, 51). In the current study, we did not find a statistically significant difference in average age at menarche by tumor subtype despite the observed correlation between the former and Indigenous American ancestry proportion.
We observed a higher frequency of parous women diagnosed with HR− subtypes compared with HR+. Parity (ever vs. never) has been associated with a higher risk of HR−HER2− subtypes, especially among women of African origin (33–35). Higher number of full-term pregnancies has been associated with reduced breast cancer risk (19, 31), with lower odds of developing HR+ tumors (3, 19, 20, 24–27, 29–35). We found significant differences in number of births by subtype, being higher among HR− subtypes compared with HR+ (2.7 compared with 2.3, respectively). Results suggested a larger proportion of women with > 3 children among those with HR− disease subtypes. This observation was consistent with studies in African American women reporting a higher number of reported full-term pregnancies among women with HR− disease (33). Studies that have tested the association between age at first full-term pregnancy and subtype-specific risk have shown a decreased risk of developing HR+HER2− tumors with unclear associations for other subtypes (25, 27, 31). In African American cohorts, limited breastfeeding among parous women is associated with an increased risk for HR−HER2− subtypes (34). The current study does not include detailed pregnancy and lactation history for the patients. As a result, we could not assess the association between time to breastfeeding cessation and cumulative time of breastfeeding and HR− subtypes.
There were statistically significant differences in the prevalence of demographic, anthropometric, and reproductive factors by age at diagnosis categories. The multivariate analysis showed that these variables are independently associated with age at diagnosis. Moreover, the differences in BMI by age at diagnosis were concordant with what is known about pre- and post-menopausal–specific disease risk factors (39–43). It must be considered that the observed differences in parity and height by age at diagnosis could be due to the correlation between age and the former (i.e., number of children and height are positively correlated with age) and not to an association between those variables and pre- versus post-menopausal disease.
The observed association between tumor subtype and Indigenous American ancestry could be due to a multiplicity of factors that we might not have collected information on in the PEGEN-BC study. For example, the study did not obtain information on the level of education or socioeconomic status of participants; both variables were previously shown to be associated with Indigenous American ancestry) among U.S. Latinas and Mexican women (76, 102, 103). Socioeconomic status can also impact screening, which in turn can affect tumor subtype distribution and mortality rates. Reports showed that less than 20% of Peruvian women 40–59 years of age have had a mammography, with vast differences according to socioeconomic status, educational level, health insurance, and region of residence (104, 105). Plan Esperanza, launched in 2012, has aimed to provide universal cancer screening and decentralize oncological health care across Peru, focusing on underserved commuties (106).
The PEGEN-BC study had some additional limitations. First, since menopause can be induced by treatment, most of the PEGEN-BC participants were postmenopausal at the time of the interview (86%). Therefore, we did not perform stratification by menopausal status and used age at diagnosis (< 50 vs. >= 50) instead to differentiate early onset versus late onset disease, as it has been widely used in epidemiological studies (107, 108). Even though menopausal status and age at diagnosis are highly correlated, studies have shown that age at diagnosis is a driver for breast cancer heterogeneity, acting as a confounder in analyses stratified by menopausal status (109). For this reason, the use of age as a proxy for menopausal status should be taken with caution. The second limitation concerns the relatively low variability of some of the assessed factors among PEGEN-BC study participants. For example, the assessment of the association between breastfeeding and the number of births and tumor subtype was hampered by the low prevalence of women without children and of women with children who did not breastfeed them. Additionally, we described the distribution of multiple factors across tumor subtypes, which provide evidence of heterogeneity; however, future case-control design studies should further explore subtype-specific breast cancer risk. Finally, average East Asian and African genetic ancestry components showed differences by subtypes in the univariate analyses. However, since ancestry estimates are correlated, and the proportions of East Asian and African genetic ancestries were relatively low as to provide reliable estimates, we focused the current description on the Indigenous American ancestry, which is the dominant component in Peruvians.
In summary, results confirmed the previously reported higher average Indigenous American ancestry among patients with HR−HER2+ breast cancer in this larger sample of PEGEN-BC study participants. Moreover, differences in tumor subtype by age at diagnosis were apparent and concordant with what is known about pre- and post-menopausal–specific disease associated risk factors. Larger studies are needed to understand the consistently observed association between ancestry, age of onset, and disease subtypes, considering the contribution of screening and treatment, to develop population-appropriate predictive models and targeted outreach and prevention campaigns.
Data availability statement
All data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by University of California Davis Institutional Review Boards and the Instituto Nacional de Enfermedades Neoplásicas (INEN). The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
LF= Conceptualization, Methodology, Investigation, Formal Analysis, Writing- Review and editing, Supervision, Project administration, and Funding acquisition. VZ: Methodology, Investigation, Formal Analysis, Writing- Original Draft, Software, Data curation, and Visualization. TV= Conceptualization, Resources, Project administration at INEN. SC-Z= Resources, Project administration at INEN. JN-V= Investigation, Data curation. CC, GV, MC, JA, HG, HF, RL-P, JC, SN, KR, JV, LM, MG-N= Conducted patient recruitment investigation process. All authors contributed to the article and approved the submitted version.
Funding
The PEGEN-BC Study was supported by the National Cancer Institute of the (NIH) under award number [R01CA204797] for LF.
Acknowledgments
We want to thank the biobank at the Instituto Nacional de Enfermedades Neoplásicas, Lima, Peru, for their assistance in managing and storing the material for the study. We also want to thank participants from the PEGEN-BC study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.938042/full#supplementary-material
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin (2020) 70(1):7–30. doi: 10.3322/caac.21590
3. Barnard ME, Boeke CE, Tamimi RM. Established breast cancer risk factors and risk of intrinsic tumor subtypes. Biochim Biophys Acta (2015) 1856(1):73–85. doi: 10.1016/J.BBCAN.2015.06.002
4. Holm J, Eriksson L, Ploner A, Eriksson M, Rantalainen M, Li J, et al. Assessment of breast cancer risk factors reveals subtype heterogeneity. Cancer Res (2017) 77(13):3708–17. doi: 10.1158/0008-5472.CAN-16-2574
5. Jones ME, Schoemaker MJ, Wright LB, Ashworth A, Swerdlow AJ. Smoking and risk of breast cancer in the generations study cohort. Breast Cancer Res (2017) 19(1). doi: 10.1186/S13058-017-0908-4
6. Daly B, Olopade OI. A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin (2015) 65(3):221–38. doi: 10.3322/caac.21271
7. Newman LA. Breast cancer disparities: Socioeconomic factors versus biology. Ann Surg Oncol (2017) 24(10):2869–75. doi: 10.1245/s10434-017-5977-1
8. National Cancer Institute. SEER cancer stat facts: Female breast cancer. Bethesda, MD: National Cancer Institute.
9. Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer health disparities in racial/ethnic minorities in the united states. Br J Cancer (2021) 124:315–32. doi: 10.1038/s41416-020-01038-6. Springer Nature.
10. Thompson B, Hohl SD, Molina Y, Paskett ED, Fisher JL, Baltic RD, et al. Breast cancer disparities among women in underserved communities in the USA. Curr Breast Cancer Rep (2018) 10(3):131–41. doi: 10.1007/s12609-018-0277-8
11. Miller KD, Goding Sauer A, Ortiz AP, Fedewa SA, Pinheiro PS, Tortolero-Luna G, et al. Cancer statistics for Hispanics/Latinos, 2018. CA Cancer J Clin (2018) 68(6):425–45. doi: 10.3322/caac.21494
12. Fejerman L, Hu D, Huntsman S, John EM, Stern MC, Haiman CA, et al. Genetic ancestry and risk of mortality among U.S. latinas with breast cancer. Cancer Res (2013) 73(24):7243–53. doi: 10.1158/0008-5472.CAN-13-2014
13. Sørlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci U.S.A. (2001) 98(19):10869–74. doi: 10.1073/pnas.191367098
14. Perou CM, Sørlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature. (2000) 406(6797):747–52. doi: 10.1038/35021093
15. Shien T, Iwata H. Adjuvant and neoadjuvant therapy for breast cancer. Jpn J Clin Oncol (2020) 50(3):225–9. doi: 10.1093/JJCO/HYZ213
16. Wang J, Xu B. Targeted therapeutic options and future perspectives for HER2-positive breast cancer. Signal Transduct Target Ther (2019) 4(1). doi: 10.1038/S41392-019-0069-2
17. Yin L, Duan JJ, Bian XW, Yu SC. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res (2020) 22(1). doi: 10.1186/S13058-020-01296-5
18. Liu L, Hao X, Song Z, Zhi X, Zhang S, Zhang J. Correlation between family history and characteristics of breast cancer. Sci Rep (2021) 11(1). doi: 10.1038/S41598-021-85899-8
19. Xing P, Li J, Jin F. A case-control study of reproductive factors associated with subtypes of breast cancer in northeast China. Med Oncol (2010) 27(3):926–31. doi: 10.1007/S12032-009-9308-7
20. Tamimi RM, Colditz GA, Hazra A, Baer HJ, Hankinson SE, Rosner B, et al. Traditional breast cancer risk factors in relation to molecular subtypes of breast cancer. Breast Cancer Res Treat (2012) 131(1):159–67. doi: 10.1007/S10549-011-1702-0
21. Zhou W, Ding Q, Pan H, Wu N, Liang M, Huang Y, et al. Risk of breast cancer and family history of other cancers in first-degree relatives in Chinese women: a case control study. BMC Cancer. (2014) 14(1):1–7. doi: 10.1186/1471-2407-14-662
22. Phipps AI, Buist DSM, Malone KE, Barlow WE, Porter PL, Kerlikowske K, et al. Family history of breast cancer in first-degree relatives and triple-negative breast cancer risk. Breast Cancer Res Treat (2011) 126(3):671–8. doi: 10.1007/S10549-010-1148-9
23. Mavaddat N, Pharoah PD, Blows F, Driver KE, Provenzano E, Thompson D, et al. Familial relative risks for breast cancer by pathological subtype: a population-based cohort study. Breast Cancer Res (2010) 12(1). doi: 10.1186/BCR2476
24. Yang XR, Chang-Claude J, Goode EL, Couch FJ, Nevanlinna H, Milne RL, et al. Associations of breast cancer risk factors with tumor subtypes: a pooled analysis from the breast cancer association consortium studies. J Natl Cancer Inst (2011) 103(3):250–63. doi: 10.1093/JNCI/DJQ526
25. Phipps AI, Malone KE, Porter PL, Daling JR, Li CI. Reproductive and hormonal risk factors for postmenopausal luminal, HER-2-overexpressing, and triple-negative breast cancer. Cancer. (2008) 113(7):1521–6. doi: 10.1002/CNCR.23786
26. Romieu I, Biessy C, Carayol M, His M, Torres-Mejía G, Ángeles-Llerenas A, et al. Reproductive factors and molecular subtypes of breast cancer among premenopausal women in Latin America: the PRECAMA study. Sci Rep (2018) 8(1). doi: 10.1038/S41598-018-31393-7
27. Brouckaert O, Rudolph A, Laenen A, Keeman R, Bolla MK, Wang Q, et al. Reproductive profiles and risk of breast cancer subtypes: a multi-center case-only study. Breast Cancer Res (2017) 19(1). doi: 10.1186/S13058-017-0909-3
28. Lambertini M, Santoro L, Del Mastro L, Nguyen B, Livraghi L, Ugolini D, et al. Reproductive behaviors and risk of developing breast cancer according to tumor subtype: A systematic review and meta-analysis of epidemiological studies. Cancer Treat Rev (2016) 49:65–76. doi: 10.1016/J.CTRV.2016.07.006
29. Ellingjord-Dale M, Vos L, Tretli S, Hofvind S, dos-Santos-Silva I, Ursin G. Parity, hormones and breast cancer subtypes - results from a large nested case-control study in a national screening program. Breast Cancer Res (2017) 19(1). doi: 10.1186/S13058-016-0798-X
30. Turkoz FP, Solak M, Petekkaya I, Keskin O, Kertmen N, Sarici F, et al. Association between common risk factors and molecular subtypes in breast cancer patients. Breast. (2013) 22(3):344–50. doi: 10.1016/J.BREAST.2012.08.005
31. Sanderson M, Pal T, Beeghly-Fadiel A, Fadden MK, Dujon SA, Clinton C, et al. A pooled case-only analysis of reproductive risk factors and breast cancer subtype among black women in the southeastern united states. Cancer Epidemiol Biomarkers Prev (2021) 30(7):1416–23. doi: 10.1158/1055-9965.EPI-20-1784
32. Fortner RT, Sisti J, Chai B, Collins LC, Rosner B, Hankinson SE, et al. Parity, breastfeeding, and breast cancer risk by hormone receptor status and molecular phenotype: results from the nurses’ health studies. Breast Cancer Res (2019) 21(1). doi: 10.1186/S13058-019-1119-Y
33. Ambrosone CB, Zirpoli G, Ruszczyk M, Shankar J, Hong CC, McIlwain D, et al. Parity and breastfeeding among African-American women: differential effects on breast cancer risk by estrogen receptor status in the women’s circle of health study. Cancer Causes Control. (2014) 25(2):259–65. doi: 10.1007/S10552-013-0323-9
34. Palmer JR, Viscidi E, Troester MA, Hong CC, Schedin P, Bethea TN, et al. Parity, lactation, and breast cancer subtypes in African American women: results from the AMBER consortium. J Natl Cancer Inst (2014) 106(10). doi: 10.1093/JNCI/DJU237
35. Millikan RC, Newman B, Tse CK, Moorman PG, Conway K, Smith LV, et al. Epidemiology of basal-like breast cancer. Breast Cancer Res Treat (2008) 109(1):123–39. doi: 10.1007/S10549-007-9632-6
36. Gaudet MM, Press MF, Haile RW, Lynch CF, Glaser SL, Schildkraut J, et al. Risk factors by molecular subtypes of breast cancer across a population-based study of women 56 years or younger. Breast Cancer Res Treat (2011) 130(2):587–97. doi: 10.1007/S10549-011-1616-X
37. Shinde SS, Forman MR, Kuerer HM, Yan K, Peintinger F, Hunt KK, et al. Higher parity and shorter breastfeeding duration: association with triple-negative phenotype of breast cancer. Cancer. (2010) 116(21):4933–43. doi: 10.1002/CNCR.25443
38. Ellingjord-Dale M, Vos L, Hjerkind KV, Hjartåker A, Russnes HG, Tretli S, et al. Alcohol, physical activity, smoking, and breast cancer subtypes in a Large, nested case-control study from the Norwegian breast cancer screening program. Cancer Epidemiol Biomarkers Prev (2017) 26(12):1736–44. doi: 10.1158/1055-9965.EPI-17-0611
39. García-Estévez L, Cortés J, Pérez S, Calvo I, Gallegos I, Moreno-Bueno G. Obesity and breast cancer: A paradoxical and controversial relationship influenced by menopausal status. Front Oncol (2021) 11:3114. doi: 10.3389/fonc.2021.705911
40. Schoemaker MJ, Nichols HB, Wright LB, Brook MN, Jones ME, O’Brien KM, et al. Association of body mass index and age with subsequent breast cancer risk in premenopausal women. JAMA Oncol (2018) 4(11). doi: 10.1001/JAMAONCOL.2018.1771
41. Bandera EV, Chandran U, Hong CC, Troester MA, Bethea TN, Adams-Campbell LL, et al. Obesity, body fat distribution, and risk of breast cancer subtypes in African American women participating in the AMBER consortium. Breast Cancer Res Treat (2015) 150(3):655–66. doi: 10.1007/S10549-015-3353-Z
42. Gravena AAF, Lopes TCR, Demitto M de O, Borghesan DHP, Dell’ Agnolo CM, Brischiliari SCR, et al. The obesity and the risk of breast cancer among pre and postmenopausal women. Asian Pac J Cancer Prev (2018) 19(9):2429–36. doi: 10.22034/APJCP.2018.19.9.2429
43. Gathirua-Mwangi WG, Palmer JR, Champion V, Castro-Webb N, Stokes AC, Adams-Campbell L, et al. Maximum and time-dependent body mass index and breast cancer incidence among postmenopausal women in the black women’s health study. Am J Epidemiol. (2022) 191(4):646–54. doi: 10.1093/AJE/KWAC004
44. Petri AL, Tjønneland A, Gamborg M, Johansen D, Høidrup S, Sørensen TIA, et al. Alcohol intake, type of beverage, and risk of breast cancer in pre- and postmenopausal women. Alcohol Clin Exp Res (2004) 28(7):1084–90. doi: 10.1097/01.ALC.0000130812.85638.E1
45. Ángeles-Llerenas A, Ortega-Olvera C, Pérez-Rodríguez E, Esparza-Cano JP, Lazcano-Ponce E, Romieu I, et al. Moderate physical activity and breast cancer risk: the effect of menopausal status. Cancer Causes Control. (2010) 21(4):577–86. doi: 10.1007/S10552-009-9487-8
46. Si S, Boyle T, Heyworth J, Glass DC, Saunders C, Fritschi L. Lifetime physical activity and risk of breast cancer in pre-and post-menopausal women. Breast Cancer Res Treat (2015) 152(2):449–62. doi: 10.1007/S10549-015-3489-X
47. Unar-Munguía M, Torres-Mejía G, Colchero MA, González De Cosío T. Breastfeeding mode and risk of breast cancer: A dose-response meta-analysis. J Hum Lact. (2017) 33(2):422–34. doi: 10.1177/0890334416683676
48. Nickels S, Truong T, Hein R, Stevens K, Buck K, Behrens S, et al. Evidence of gene-environment interactions between common breast cancer susceptibility loci and established environmental risk factors. PloS Genet (2013) 9(3). doi: 10.1371/JOURNAL.PGEN.1003284
49. Rudolph A, Chang-Claude J, Schmidt MK. Gene-environment interaction and risk of breast cancer. Br J Cancer. (2016) 114(2):125–33. doi: 10.1038/BJC.2015.439
50. Dierssen-Sotos T, Palazuelos-Calderón C, Jiménez-Moleón JJ, Aragonés N, Altzibar JM, Castaño-Vinyals G, et al. Reproductive risk factors in breast cancer and genetic hormonal pathways: a gene-environment interaction in the MCC-Spain project. BMC Cancer. (2018) 18(1). doi: 10.1186/S12885-018-4182-3
51. Olivier M, Bouaoun L, Villar S, Robitaille A, Cahais V, Heguy A, et al. Molecular features of premenopausal breast cancers in Latin American women: Pilot results from the PRECAMA study. PloS One (2019) 14(1). doi: 10.1371/JOURNAL.PONE.0210372
52. de Almeida LM, Cortés S, Vilensky M, Valenzuela O, Cortes-Sanabria L, de Souza M, et al. Socioeconomic, clinical, and molecular features of breast cancer influence overall survival of Latin American women. Front Oncol (2022) 0:556. doi: 10.3389/fonc.2022.845527
53. Carvalho FM, Bacchi LM, Pincerato KM, Van de Rijn M, Bacchi CE. Geographic differences in the distribution of molecular subtypes of breast cancer in Brazil. BMC Womens Health (2014) 14(1). doi: 10.1186/1472-6874-14-102
54. Cazap E, Buzaid AC, Garbino C, de la Garza J, Orlandi FJ, Schwartsmann G, et al. Breast cancer in Latin America: results of the Latin American and Caribbean society of medical Oncology/Breast cancer research foundation expert survey. Cancer. (2008) 113(8 Suppl):2359–65. doi: 10.1002/CNCR.23834
55. Homburger JR, Moreno-Estrada A, Gignoux CR, Nelson D, Sanchez E, Ortiz-Tello P, et al. Genomic insights into the ancestry and demographic history of south America. PloS Genet (2015) 11(12):e1005602. doi: 10.1371/journal.pgen.1005602
56. Adhikari K, Chacón-Duque JC, Mendoza-Revilla J, Fuentes-Guajardo M, Ruiz-Linares A. The genetic diversity of the americas. Annu Rev Genomics Hum Genet (2017) 18(1):277–96. doi: 10.1146/annurev-genom-083115-022331
57. Norris ET, Wang L, Conley AB, Rishishwar L, Mariño-Ramírez L, Valderrama-Aguirre A, et al. Genetic ancestry, admixture and health determinants in Latin America. BMC Genomics (2018) 19(S8):861. doi: 10.1186/s12864-018-5195-7
58. Heinz T, Álvarez-Iglesias V, Pardo-Seco J, Taboada-Echalar P, Gómez-Carballa A, Torres-Balanza A, et al. Ancestry analysis reveals a predominant native American component with moderate European admixture in bolivians. Forensic Sci Int Genet (2013) 7(5):537–42. doi: 10.1016/j.fsigen.2013.05.012
59. Fejerman L, Stern MC, Ziv E, John EM, Torres-Mejia G, Hines LM, et al. Genetic ancestry modifies the association between genetic risk variants and breast cancer risk among Hispanic and non-Hispanic white women. Carcinogenesis. (2013) 34(8):1787–93. doi: 10.1093/carcin/bgt110
60. Fejerman L, Stern MC, John EM, Torres-Mejía G, Hines LM, Wolff RK, et al. Interaction between common breast cancer susceptibility variants, genetic ancestry, and nongenetic risk factors in Hispanic women. Cancer Epidemiol Biomarkers Prev (2015) 24(11):1731–8. doi: 10.1158/1055-9965.EPI-15-0392
61. Fejerman L, Ramirez AG, Nápoles AM, Gomez SL, Stern MC. Cancer epidemiology in Hispanic populations: what have we learned and where do we need to make progress? Cancer Epidemiol Biomarkers Prev (2022) 31(5):932–41. doi: 10.1158/1055-9965.EPI-21-1303
62. Marker KM, Zavala VA, Vidaurre T, Lott PC, Vásquez JN, Casavilca-Zambrano S, et al. Human epidermal growth factor receptor 2–positive breast cancer is associated with indigenous American ancestry in Latin American women. Cancer Res (2020) 80(9):1893–901. doi: 10.1158/0008-5472.CAN-19-3659
63. Zavala VA, Casavilca-Zambrano S, Navarro-Vásquez J, Castañeda CA, Valencia G, Morante; Z, et al. Association between ancestry-specific 6q25 variants and breast cancer subtypes in Peruvian women. Cancer Epidemiol Biomarkers Prev (2022) 31(8):1602–9. doi: 10.1158/1055-9965.EPI-22-0069
64. Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MAR, Bender D, et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet (2007) 81(3):559–75. doi: 10.1086/519795
65. Consortium T 1000 GP, Campbell CL, Scheller C, Horn H, Kidd JM, Doddapaneni H, et al. A global reference for human genetic variation. Nature. (2015) 526(7571):68–74. doi: 10.1038/nature15393
66. Alexander DH, Novembre J, Lange K. Fast model-based estimation of ancestry in unrelated individuals. Genome Res (2009) 19:1655–64. doi: 10.1101/gr.094052.109.vidual
67. Team RC. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2018).
68. Instituto Nacional de Estadística e Informática. Censos nacionales 2017: XII de población, VII de vivienda y III de comunidades indígenas. (2018).
69. Torres-Roman JS, Martinez-Herrera JF, Carioli G, Ybaseta-Medina J, Valcarcel B, Pinto JA, et al. Breast cancer mortality trends in Peruvian women. BMC Cancer. (2020) 20(1):1–9. doi: 10.1186/S12885-020-07671-X/FIGURES/4
70. De-La-Cruz-Ku G, Luyo M, Morante Z, Enriquez D, Möller MG, Chambergo-Michilot D, et al. Triple-negative breast cancer in Peru: 2000 patients and 15 years of experience. PloS One (2020) 15(8). doi: 10.1371/JOURNAL.PONE.0237811
71. Machado MPA, Opaleye DC, Pereira TV, Padilla I, Noto AR, Prince M, et al. Alcohol and tobacco consumption concordance and its correlates in older couples in Latin America. Geriatr Gerontol Int (2017) 17(11):1849–57. doi: 10.1111/GGI.12974
72. Champagne BM, Sebrié EM, Schargrodsky H, Pramparo P, Boissonnet C, Wilson E. Tobacco smoking in seven Latin American cities: the CARMELA study. Tob Control. (2010) 19(6):457–62. doi: 10.1136/TC.2009.031666
73. Shieh Y, Fejerman L, Lott PC, Marker K, Sawyer SD, Hu D, et al. A polygenic risk score for breast cancer in U.S. latinas and Latin-American women. J Natl Cancer Inst (2019) 112(6):590–8. doi: 10.1093/jnci/djz174
74. Slattery ML, Lundgreen A, Hines L, Wolff RK, Torres-Mejia G, Baumgartner KN, et al. Energy homeostasis genes and breast cancer risk: The influence of ancestry, body size, and menopausal status, the breast cancer health disparities study. Cancer Epidemiol. (2015) 39(6):1113–22. doi: 10.1016/j.canep.2015.08.012
75. Fejerman L, John EM, Huntsman S, Beckman K, Choudhry S, Perez-Stable E, et al. Genetic ancestry and risk of breast cancer among U.S. latinas. Cancer Res (2008) 68(23):9723–8. doi: 10.1158/0008-5472.CAN-08-2039
76. Engmann NJ, Ergas IJ, Yao S, Kwan ML, Roh JM, Ambrosone CB, et al. Genetic ancestry is not associated with breast cancer recurrence or survival in U.S. latina women enrolled in the kaiser permanente pathways study. Cancer Epidemiol Biomarkers Prev (2017) 26(9):1466–9. doi: 10.1158/1055-9965.EPI-17-0148
77. Sanchez SS, Tachachartvanich P, Stanczyk FZ, Gomez SL, John EM, Smith MT, et al. Estrogenic activity, race/ethnicity, and indigenous American ancestry among San Francisco bay area women. PloS One (2019) 14(3). doi: 10.1371/JOURNAL.PONE.0213809
78. John EM, Sangaramoorthy M, Hines LM, Stern MC, Baumgartner KB, Giuliano AR, et al. Overall and abdominal adiposity and premenopausal breast cancer risk among hispanic women: the breast cancer health disparities study. Cancer Epidemiol Biomarkers Prev (2015) 24(1):138–47. doi: 10.1158/1055-9965.EPI-13-1007-T
79. Slattery ML, Lundgreen A, John EM, Torres-Mejia G, Hines L, Giuliano AR, et al. MAPK genes interact with diet and lifestyle factors to alter risk of breast cancer: the breast cancer health disparities study. Nutr Cancer. (2015) 67(2):292–304. doi: 10.1080/01635581.2015.990568
80. Vallejos C, Gómez H, Cruz W, Pinto J, Dyer R, Velarde R, et al. Breast cancer classification according to immunohistochemistry markers: Subtypes and association with clinicopathologic variables in a peruvian hospital database. Clin Breast Cancer. (2010) 10(4):294–300. doi: 10.3816/CBC.2010.n.038
81. Macari A, Soberanis-Pina P, Varela-Santoyo E, Valle-Sanchez MA, Leal-Hidalgo JL, Torres-Guillen VM, et al. Prevalence and molecular profile of breast carcinoma using immunohistochemistry markers in Mexican women. World J Oncol (2021) 12(4):119–23. doi: 10.14740/WJON1392
82. Gómez R, Ossa CA, Montoya ME, Echeverri C, Ángel G, Ascuntar J, et al. Impact of immunohistochemistry-based molecular subtype on chemosensitivity and survival in Hispanic breast cancer patients following neoadjuvant chemotherapy. Ecancermedicalscience. (2015) 9. doi: 10.3332/ECANCER.2015.562
83. Romero-Cordoba SL, Salido-Guadarrama I, Rebollar-Vega R, Bautista-Piña V, Dominguez-Reyes C, Tenorio-Torres A, et al. Comprehensive omic characterization of breast cancer in Mexican-Hispanic women. Nat Commun (2021) 12(1). doi: 10.1038/S41467-021-22478-5
84. Serrano-Gomez SJ, Sanabria-Salas MC, Hernández-Suarez G, García O, Silva C, Romero A, et al. High prevalence of luminal b breast cancer intrinsic subtype in Colombian women. Carcinogenesis. (2016) 37(7):669–76. doi: 10.1093/CARCIN/BGW043
85. Fernandes GC, Michelli RA, Galvão HC, Paula AE, Pereira R, Andrade CE, et al. Prevalence of BRCA1/BRCA2 mutations in a Brazilian population sample at-risk for hereditary breast cancer and characterization of its genetic ancestry. Oncotarget. (2016) 7(49):80465–81. doi: 10.18632/oncotarget.12610
86. Fejerman L, Chen GK, Eng C, Huntsman S, Hu D, Williams A, et al. Admixture mapping identifies a locus on 6q25 associated with breast cancer risk in US latinas. Hum Mol Genet (2012) 21(8):1907–17. doi: 10.1093/hmg/ddr617
87. Hoffman J, Fejerman L, Hu D, Huntsman S, Li M, John EM, et al. Identification of novel common breast cancer risk variants at the 6q25 locus among latinas. Breast Cancer Res (2019) 21(1):3. doi: 10.1186/s13058-018-1085-9
88. Fejerman L, Sanchez SS, Thomas R, Tachachartvanich P, Riby J, Gomez SL, et al. Association of lifestyle and demographic factors with estrogenic and glucocorticogenic activity in Mexican American women. Carcinogenesis. (2016) 37(9):904–11. doi: 10.1093/CARCIN/BGW074
89. Bonilla C, Bertoni B, Hidalgo PC, Artagaveytia N, Ackermann E, Barreto I, et al. Breast cancer risk and genetic ancestry: a case-control study in Uruguay. BMC Womens Health (2015) 15:11. doi: 10.1186/s12905-015-0171-8
91. Ruiz-Linares A, Adhikari K, Acuña-Alonzo V, Quinto-Sanchez M, Jaramillo C, Arias W, et al. Admixture in Latin America: Geographic structure, phenotypic diversity and self-perception of ancestry based on 7,342 individuals. PloS Genet (2014) 10(9):e1004572. doi: 10.1371/journal.pgen.1004572
92. Barrios YV, Sanchez SE, Nicolaidis C, Garcia PJ, Gelaye B, Zhong Q, et al. Childhood abuse and early menarche among Peruvian women. J Adolesc Health (2015) 56(2):197. doi: 10.1016/J.JADOHEALTH.2014.10.002
94. Huayanay-Espinoza CA, Quispe R, Poterico JA, Carrillo-Larco RM, Bazo-Alvarez JC, Miranda JJ. Parity and Overweight/Obesity in Peruvian women. Prev Chronic Dis (2017) 14. doi: 10.5888/PCD14.160282
95. Yábar A, Meléndez R, Muñoz S, Deneo H, Freire J, Domínguez V, et al. Effect of ki-67 assessment in the distribution of breast cancer subtypes: Evaluation in a cohort of Latin American patients. Mol Clin Oncol (2017) 6(4):503–9. doi: 10.3892/MCO.2017.1185
96. Goldhirsch A, Winer EP, Coates AS, Gelber RD, Piccart-Gebhart M, Thürlimann B, et al. Personalizing the treatment of women with early breast cancer: highlights of the St gallen international expert consensus on the primary therapy of early breast cancer 2013. Ann Oncol Off J Eur Soc Med Oncol (2013) 24(9):2206–23. doi: 10.1093/annonc/mdt303
97. Guth AA, Chun Kim J, Schwartz S, Montes J, Snyder RA, Axelrod D, et al. The relationship of race, oncotype DX, and Ki67 in a population highly screened for breast cancer. Breast J (2017) 23(2):177–81. doi: 10.1111/TBJ.12781
98. Cai S, Zuo W, Lu X, Gou Z, Zhou Y, Liu P, et al. The prognostic impact of age at diagnosis upon breast cancer of different immunohistochemical subtypes: A surveillance, epidemiology, and end results (SEER) population-based analysis. Front Oncol (2020) 10:1729. doi: 10.3389/FONC.2020.01729
99. Clarke CA, Keegan THM, Yang J, Press DJ, Kurian AW, Patel AH, et al. Age-specific incidence of breast cancer subtypes: understanding the black-white crossover. J Natl Cancer Inst (2012) 104(14):1094–101. doi: 10.1093/JNCI/DJS264
100. Butler EN, Tse CK, Bell ME, Conway K, Olshan AF, Troester MA. Active smoking and risk of luminal and basal-like breast cancer subtypes in the Carolina breast cancer study. Cancer Causes Control. (2016) 27(6):775. doi: 10.1007/S10552-016-0754-1
101. Kawai M, Malone KE, Tang MTC, Li CI. Active smoking and the risk of estrogen receptor-positive and triple-negative breast cancer among women ages 20 to 44 years. Cancer. (2014) 120(7):1026–34. doi: 10.1002/CNCR.28402
102. Santiago-Torres M, De Dieu Tapsoba J, Kratz M, Lampe JW, Breymeyer KL, Levy L, et al. Genetic ancestry in relation to the metabolic response to a US versus traditional Mexican diet: a randomized crossover feeding trial among women of Mexican descent. Eur J Clin Nutr (2017) 71(3):395–401. doi: 10.1038/EJCN.2016.211
103. Ziv E, John EM, Choudhry S, Kho J, Lorizio W, Perez-Stable EJ, et al. Genetic ancestry and risk factors for breast cancer among latinas in the San Francisco bay area. Cancer Epidemiol Biomarkers Prev (2006) 15(10):1878–85. doi: 10.1158/1055-9965.EPI-06-0092
104. Chang-Cabanillas S, Peñafiel-Sam J, Alarcón-Guevara S, Pereyra-Elías R. Social determinants of mammography screening among women aged 50 to 59, Peru 2015. Health Care Women Int (2021) 42(1):1–15. doi: 10.1080/07399332.2020.1786093
105. Hernández-Vásquez A, Chacón-Torrico H. Use of mammography in Peruvian women: An analysis of the 2018 demographic and health survey. Medwave. (2019) 19(9):e7701. doi: 10.5867/MEDWAVE.2019.09.7701
106. Vidaurre T, Santos C, Gómez H, Sarria G, Amorin E, López M, et al. The implementation of the plan esperanza and response to the imPACT review. Lancet Oncol (2017) 18(10):e595–606. doi: 10.1016/S1470-2045(17)30598-3
107. Research on the menopause in the 1990s. Report of a WHO Scientific Group. World Health Organ Tech Rep Ser. (1996) 886:1–107.
108. Phipps AI, Ichikawa L, Bowles EJA, Carney PA, Kerlikowske K, Miglioretti DL, et al. Defining menopausal status in epidemiologic studies: A comparison of multiple approaches and their effects on breast cancer rates. Maturitas. (2010) 67(1):60–6. doi: 10.1016/J.MATURITAS.2010.04.015
Keywords: breast cancer, genetic ancestry, Hispanics/Latinas, Indigenous American, tumor subtype
Citation: Zavala VA, Casavilca-Zambrano S, Navarro-Vásquez J, Tamayo LI, Castañeda CA, Valencia G, Morante Z, Calderón M, Abugattas JE, Gómez HL, Fuentes HA, Liendo-Picoaga R, Cotrina JM, Neciosup SP, Roque K, Vásquez J, Mas L, Gálvez-Nino M, Fejerman L and Vidaurre T (2023) Breast cancer subtype and clinical characteristics in women from Peru. Front. Oncol. 13:938042. doi: 10.3389/fonc.2023.938042
Received: 06 May 2022; Accepted: 30 January 2023;
Published: 16 February 2023.
Edited by:
Folakemi Odedina, Mayo Clinic Florida, United StatesReviewed by:
Sandhya Annamaneni, Osmania University, IndiaLucas Delmonico, Oncoclinicas Group, Brazil
Patricia Thompson, Cedars Sinai Medical Center, United States
Copyright © 2023 Zavala, Casavilca-Zambrano, Navarro-Vásquez, Tamayo, Castañeda, Valencia, Morante, Calderón, Abugattas, Gómez, Fuentes, Liendo-Picoaga, Cotrina, Neciosup, Roque, Vásquez, Mas, Gálvez-Nino, Fejerman and Vidaurre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Fejerman, bGZlamVybWFuQHVjZGF2aXMuZWR1
†These authors share senior authorship