
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 23 January 2024
Sec. Thoracic Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1330468
This article is part of the Research TopicAdvances in the use of EGFR TKIs in the Treatment of NSCLCView all 21 articles
 Myriam Mirza1*
Myriam Mirza1* Aseem Shrivastava1Cecile Matthews2
Aseem Shrivastava1Cecile Matthews2 Natasha Leighl3†
Natasha Leighl3† Calvin S. H. Ng4†
Calvin S. H. Ng4† David Planchard5,6†Sanjay Popat7,8,9†
David Planchard5,6†Sanjay Popat7,8,9† Julia Rotow10†
Julia Rotow10† Egbert F. Smit11†Ross Soo12†Masahiro Tsuboi13†
Egbert F. Smit11†Ross Soo12†Masahiro Tsuboi13† Fan Yang14†Brendon Stiles15‡Christian Grohe16‡
Fan Yang14†Brendon Stiles15‡Christian Grohe16‡ Yi-Long Wu17‡
Yi-Long Wu17‡Introduction: Osimertinib is recommended by major guidelines for use in the adjuvant setting in patients with EGFR mutation-positive NSCLC following the significant improvement in disease-free survival observed in the Phase III ADAURA trials. Due to limited real-world data in the adjuvant setting, little guidance exists on how to approach potential recurrences either during or after the completion of the treatment. This study aimed to reach a broad consensus on key treatment decision criteria in the events of recurrence.
Methods: To reach a broad consensus, a modified Delphi panel study was conducted consisting of two rounds of surveys, followed by two consensus meetings and a final offline review of key statements. An international panel of experts in the field of NSCLC (n=12) was used to provide clinical insights regarding patient management at various stages of NSCLC disease including patient monitoring, diagnostics, and treatment approach for specific recurrence scenarios. This study tested recurrences occurring 1) within or outside the central nervous system (CNS), 2) during or after the adjuvant-osimertinib regimen in NSCLC disease which is 3) amenable or not amenable to local consolidative therapy.
Results: Panellists agreed on various aspects of patient monitoring and diagnostics including the use of standard techniques (e.g., CT, MRI) and tumour biomarker assessment using tissue and liquid biopsies. Consensus was reached on 6 statements describing treatment considerations for the specific NSCLC recurrence scenarios. Panellists agreed on the value of osimertinib as a monotherapy or as part of the overall treatment strategy within the probed recurrence scenarios and acknowledged that more clinical evidence is required before precise recommendations for specific patient populations can be made.
Discussion: This study provides a qualitative expert opinion framework for clinicians to consider within their treatment decision-making when faced with recurrence during or after adjuvant-osimertinib treatment.
A significant number of NSCLC patients harbor EGFR driver mutations (EGFRm NSCLC) which activate EGFR tyrosine kinase to have a ligand-independent activity, resulting in tumorigenesis (1–3). In US plus Europe and Asia, EGFRm NSCLC patients account for ~10-15% and ~30-50% of all NSCLC cases, respectively (4). The two most common EGFR mutations are short in-frame deletions of exon 19 and a point mutation in exon 21 which result in the substitution of leucine by arginine at codon 858 (L858R), together, accounting for ∼85% of all EGFR mutations in NSCLC (4). EGFR tyrosine kinase inhibitors (EGFR-TKIs) have been shown to significantly improve disease-free survival (DFS) in patients with resected early-stage EGFRm NSCLC (5, 6). Osimertinib is a third-generation EGFR-TKI approved in many countries around the world for both EGFR-TKI sensitizing (exon 19 deletion & L858R point mutation in exon 21) and T790M resistance mutations in advanced stage NSCLC patients (7). In 2020, primary analysis of the pivotal phase 3 ADAURA trial demonstrated a substantial DFS benefit in patients with EGFR-mutated NSCLC who underwent complete tumor resection, with hazard ratios of 0.17 (99% CI 0.11 to 0.26; p < 0.001) for stage II to IIIA disease and 0.20 (99% CI 0.14 to 0.30; p < 0.001) for stage IB to IIIA disease compared to placebo. Due to the significant improvement in DFS, the independent data monitoring committee recommended reporting the trial results two years earlier than originally planned, allowing patients to continue in the trial (8). Updated data with an additional 2 years of follow-up continued to show a sustained DFS benefit (hazard ratios of 0.23 in stage II and IIIA disease and 0.27 in stage IB and IIIA disease, respectively), In addition, recurrences among all the patients with stage IB to IIIA disease were less frequent with osimertinib (93 patients [27%]) than with placebo (205 patients [60%]). Recurrences in the osimertinib group included distant metastases only (45 patients [13%]), local/regional only (42 patients [12%]), as well as both local/regional and distance (6 patients [2%]) (9).
Most recently, published data on overall survival (OS) in the overall population (patients with stage IB to IIIA disease) report an OS HR of 0.49 (95% CI 0.34 to 0.70; p < 0.0001) with a 5-year OS rate of 88% with osimertinib vs 78% with placebo. In stage II–IIIA disease, OS HR was reported to be 0.49 (95% CI 0.33 to 0.73; p=0.0001) and the 5-year OS rate was 85% with osimertinib vs 73% with placebo. The median OS was not reached in either population or treatment group (10).
While adjuvant-osimertinib demonstrated an unprecedented patient benefit in terms of OS improvements, there is a need to understand better the optimal management of patients who show tumor recurrence either during or after the completion of the adjuvant-osimertinib regimen. Given the anticipated emergence of a patient population with disease relapse following adjuvant osimertinib treatment, and the absence of real-world data or trial data, creating formal guidelines on how to approach and manage recurrent patients either during or after completion of adjuvant-osimertinib is not yet possible. The knowledge gap regarding the appropriate approach for patient monitoring, diagnostics, and treatment sequencing decisions in cases of various recurrence scenarios can be bridged via clinical consensus studies. Recent consensus studies echoed the need for further clinical trial data to create formal guidelines (11, 12) and outlined the appropriate treatment options (including osimertinib) for different recurrence scenarios (12). In this consensus paper, we discuss the key clinical factors that can be considered during treatment decision-making as well as clinical value of osimertinib for various recurrence scenarios.
The study utilized a modified Delphi method which included two rounds of surveys, followed by two consensus meetings and a final offline review by an expert panel. The key topics addressed in this study are listed in Table 1.

Table 1 Key topics addressed in this studyi.
In this study, an international panel of experts was recruited with significant expertise in NSCLC as well as patient management with EGFR-TKIs or other systemic therapies (n=12). Experts who fulfil the following criteria were selected as panelists in this study: a physician specializing in NSCLC (medical oncologist or thoracic surgeon); based in a specialist lung cancer treatment and research center; significant years of experience in practice since completing residence/fellowship; over 60% of combined professional time dedicated to clinical practice and research activities related to NSCLC; regularly treating and managing patients across all stages of NSCLC (stage I-III); active advisor/member of a national or international society for lung cancer with participation in guideline creation for NSCLC in the last 5 years; has published on the topic of stage I-III NSCLC in international peer-reviewed journals within the last 5 years.
The steering committee consisted of two medical oncologists and one thoracic surgeon from different geographies (Asia, Europe, and the USA) to ensure geographic as well as different clinical expertise were incorporated in the development of materials.
Both surveys were composed of a series of open and close ended question and shared via email. All materials tested in the study were co-developed and reviewed by the steering committee. In Survey 1, panelists were presented with six hypothetical patient case studies representing distinct real-world EFGRm NSCLC patients who recur during or after the treatment with adjuvant-osimertinib and were surveyed on their approach to patient monitoring, diagnostic workup, and treatment sequencing (see Supplementary Data 1 – Table 1 for hypothetical patient cases). Most questions were asked in an open-ended style to capture individual approach as well as clinical considerations. After analysis, topics that reached clinical consensus were reported back in Survey 2 as anonymized consolidated feedback and those that did not reach consensus were further probed using new clinical statements based on insights from Survey 1 (see Supplementary Data 2 for both survey 1 and 2). The insights gathered from Survey 2 were analyzed to find topics of clinical consensus. Statements or insights where clinical consensus was not achieved were brought forward to a series of consensus meetings (see Supplementary Data 1 – Table 2).
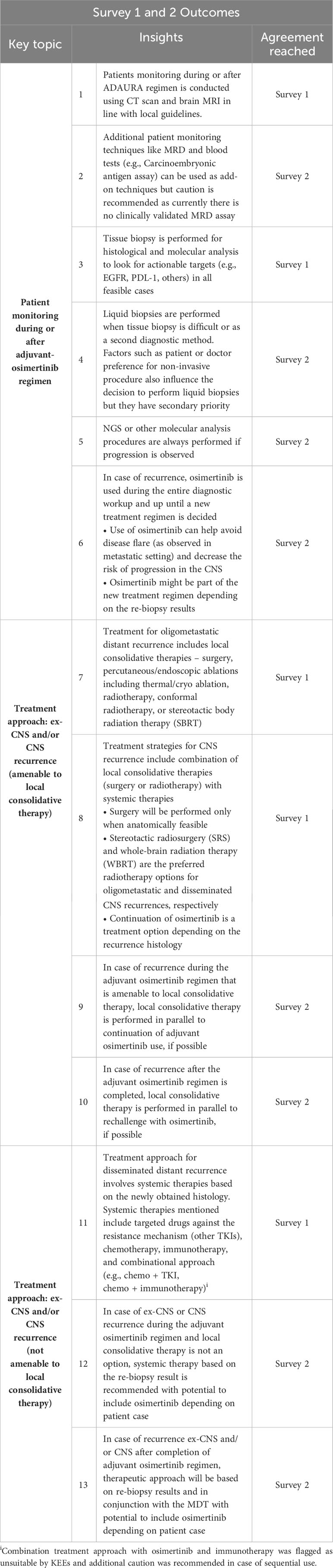
Table 2 Survey 1 and Survey 2 outcomes – Major insights with an overall panellists’ agreement.
Two virtual consensus meetings were held where a final set of statements were discussed and amended live during the meeting. The level of consensus on the amended statements was probed through anonymous polls. The statement modification process was iterated until an overall clinical consensus (≥80% panelist agreement) was achieved for all six statements (see Supplementary Data 1 – Table 3 for the evolution of the survey statements pre- and post-consensus meeting). The final set of consensus statements were shared with all panelists for offline review and to capture their final level of agreement.
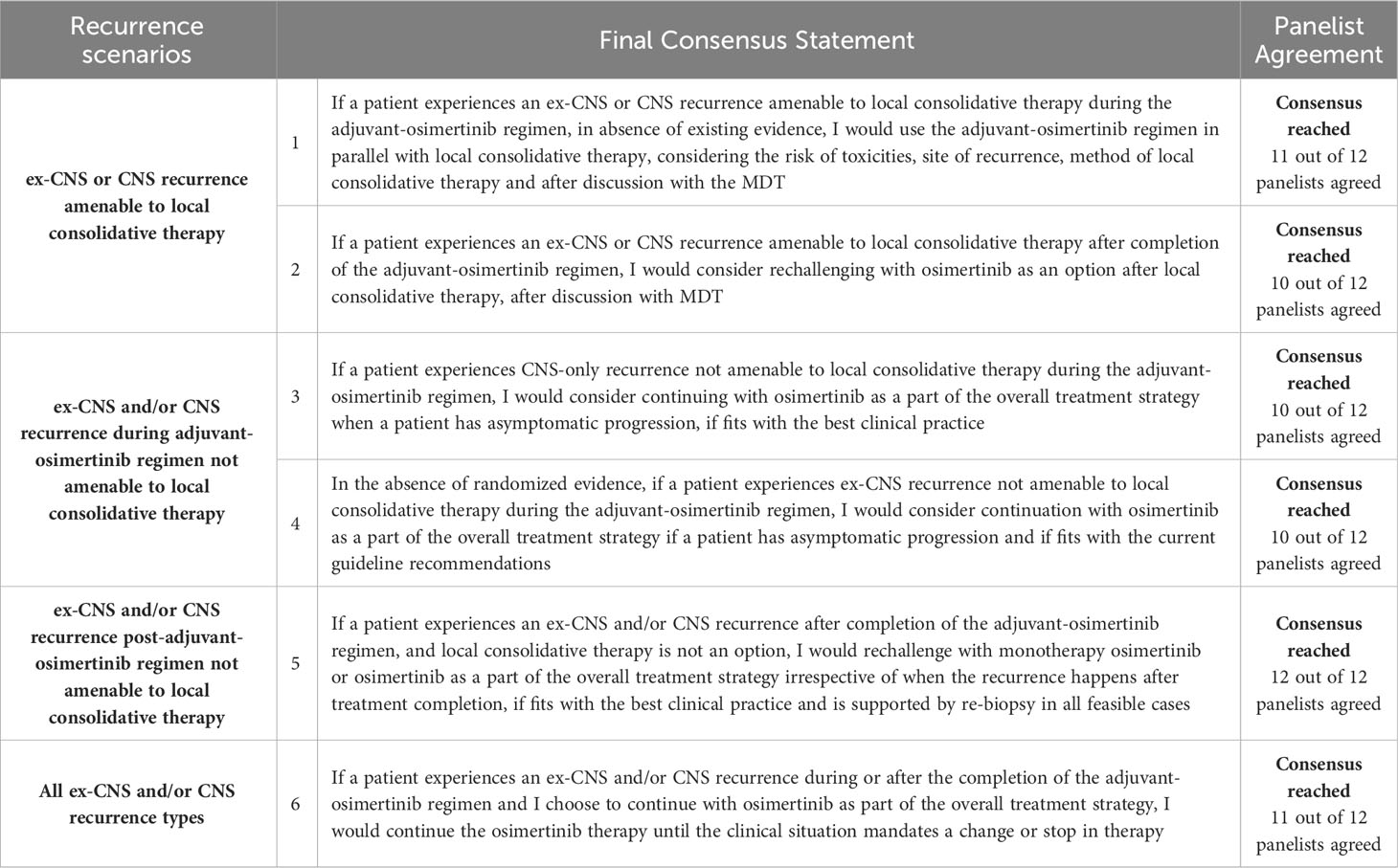
Table 3 Final consensus statements with an overall panelist agreement.
Closed statements were ranked on the Likert scale of 1 to 9, where 1 equals “strongly disagree with the statement,” and 9 equals “strongly agree with the statement,”. Likert scale rating of 7 or higher for a given statement from a minimum of 80% of panelists was defined as a threshold for a consensus on the statement. In contrast, a rating of 3 or lower for a given statement from a minimum of 80% of panelists indicated consensus had been reached of disagreement with the statement.
To limit bias, all surveys were conducted anonymously, and identity of experts was revealed only during the consensus meetings. Furthermore, results from rating exercises were provided as median scores and anonymous votes were held to finalize the consensus statements. In addition, offline review of the final statements was conducted individually without revealing the level of agreement from other panelists.
An independent third-party vendor, Charles River Associates (CRA) designed the survey, moderated the consensus meetings, analyzed the data and supported the manuscript development. The sponsor of the study (AstraZeneca Ltd.) did not participate in consensus meetings.
Surveys 1 and 2 were used to gather a greater understanding of the factors influencing treatment sequencing within the adjuvant-osimertinib setting, including recurrence type and timing. A summary of the key insights gathered from Surveys 1 and 2 is shown in Table 2.
In Survey 1, six distinct hypothetical NSCLC patient case studies were used to understand how panelists approach management of different patient types and understand the potential differences under varying recurrence scenarios. Patients within the case studies had varying EGFRm mutations, ethnicities (Asian/non-Asian), age groups (40-65 years old), smoking status, past experience with adjuvant chemotherapies, recurrence either during or after adjuvant-osimertinib and details of the recurrence. All patients within the case studies were given a performance status (PS) score of 1.
Overall, panelists agreed that all the hypothetical patient cases are representative of real-world profiles and the use of adjuvant-osimertinib in these hypothetical patient cases is approved under the ADAURA label. Panelists also agreed on the monitoring and diagnostic approaches laid out, albeit frequency of monitoring and how molecular analysis is conducted remained unclear. Moreover, although some panelists mentioned the use of monitoring techniques such as minimal residual disease (MRD) tests and blood tests (e.g., CEA - carcinoembryonic antigen), it was unclear if these techniques would be used for all patients or in specific circumstances. Finally, there was a lack of agreement on the value of liquid biopsy within the diagnostic process. Overall, despite no diagnostic procedural differences between oligometastatic and disseminated recurrences being reported there remained a lack of clarity as to whether adjuvant-osimertinib regimen should be continued during diagnostic workup and up until a new treatment strategy is confirmed.
Panelists agreed on treatment approaches for local and distant oligometastatic CNS/ex-CNS recurrence as well as disseminated CNS/ex-CNS recurrence. However, treatment sequencing decision for both ex-CNS and CNS recurrences and the associated driving factors were unclear. No consensus was observed on how patients treated with the preferred initial treatment (e.g., ablative therapy) are therapeutically followed up and to what extent osimertinib would be considered a therapeutic option.
Gaps identified in Survey 1 were explored in Survey 2, where agreement was reached on all outstanding aspects of diagnosis and monitoring. Panelists were presented with different scenarios to better understand the treatment sequencing drivers and how adjuvant-osimertinib would be considered in the overall treatment strategy. These scenarios focused on understanding the impact of recurrence location (CNS versus ex-CNS), amenability to local consolidative therapy, timing (during or after adjuvant-osimertinib regimen) as well as time points (3, 6, 18 months after initiation of adjuvant-osimertinib versus 3, 12 and 36 months after completion with adjuvant-osimertinib regimen).
While panelists agreed that continuing with adjuvant-osimertinib is clinically suitable during the diagnostic process and can be considered within treatment decision-making in the described CNS/ex-CNS recurrence scenarios, how its use would be decided remained unclear. Furthermore, there was no consensus on how long treatment with osimertinib would continue within recurrence scenarios and what considerations would influence this decision. Finally, some panelists suggested temporarily pausing the adjuvant-osimertinib regimen upon recurrence and resuming after ablative therapy, but the recommended pause duration and its applicability to all ablative therapy procedures are not clear. For recurrences after completing the adjuvant-osimertinib regimen, a combination of ablative therapy and osimertinib rechallenge was proposed, but it remains unclear whether the rechallenge would be performed alongside ablative therapy or after its completion.
Gaps in key treatment decision factors and the value of osimertinib across tested recurrence scenarios were addressed during 2 virtual consensus meetings, where experts amended wording of original proposed statements in line with best clinical practice and experience given limited randomized evidence. A summary of the statements that reached a consensus is shown in Table 3.
A lack of clinical guidance on how to treat recurrences during or after the completion of the adjuvant-osimertinib regimen has been raised in recent publications (11, 12). Our Delphi consensus study surveyed an international panel of experts on patient-specific as well as recurrence scenario-specific considerations when making treatment decisions in the absence of extensive clinical data and formalized guidelines.
Our study approach enables experts to share their own opinions based on clinical experience, and, where relevant, knowledge of the ADAURA phase 3 data, with the aim of fostering the integration of these viewpoints. Overall, our research shows a high consensus regarding patient considerations and approaches to various recurrence scenarios. Statements and considerations that garnered consensus can serve as valuable guidance in clinical practice when combined with a tailored patient approach and recommendations from multidisciplinary teams.
Our results show that the decision to use adjuvant-osimertinib is not driven by patient’s gender, ethnicity, age, smoking or alcohol use status, or previous treatment experience with adjuvant-chemotherapy. However, the decision to use adjuvant-osimertinib might change if a patient has poor PS score (PS >1), has high comorbidities or is likely to be less compliant with the dosing regimen.
Furthermore, patients receiving adjuvant-osimertinib should be monitored using local guidelines which broadly align with international guidelines such as ESMO (Table 2 – statement 1).
In our study, tissue biopsy is recommended in all feasible cases in case of progression to assess the suitability of different treatment options based on tumor biomarker/mutation profile. The diagnostic result from liquid biopsy was highlighted to be less sensitive and contingent on site and burden of the recurrence (Table 2 – statements 3-5). Therefore, only when tissue biopsy is not possible should liquid biopsy be used as it is unable to capture histologic transformation and has limited sensitivity from amplifications and fusions (12). Moreover, liquid biopsies may give false negative or positive results, especially in cases of low volume disease with lower than threshold circulating ctDNA (13). These recommendations are echoed in the ESMO expert consensus on the management of EGFRm NSCLC (12). The panel’s consensus is to continue use of adjuvant-osimertinib during the diagnostic workup and up until a new treatment regimen is decided for patients who present with recurrence during the adjuvant-osimertinib regimen. The continued use of osimertinib can help avoid disease flare, a well-established scenario for metastatic disease, and to additionally protect against CNS progression (Table 2 – statement 6) (9, 14, 15).
Across all tested scenarios, treatment decisions are taken on a patient-by-patient basis and taking input from the multi-disciplinary team (MDT), aligning with major guidelines (16–21). The following key clinical criteria should be considered during the treatment sequencing decision process (Table 2 – statements 7-13):
● Pattern and location – Number of lesions, size and location determine if the recurrence is oligometastatic and amenable to local consolidative therapy or disseminated and requires treatment with a systemic therapy. Furthermore, limited metastases which may include lesions in contralateral lung, lymph node, CNS or other organs could be managed with a combination of local consolidative therapy and a systemic therapy. Panelists did not rule out the treatment value of osimertinib in various recurrence scenarios solely based on pattern and location.
● Timing of recurrence – whether and when recurrence occurs during or after the adjuvant-osimertinib regimen can indicate if the recurrent lesion is sensitive or resistant to osimertinib in addition to genetic profiling. Recurrence during the adjuvant-osimertinib regimen (especially ex-CNS) might be a sign of acquired resistance to osimertinib, while recurrence after the completion of the regimen might indicate a disease flare post-treatment cessation.
● Molecular characterization of the recurrence – Confirming molecular histology or biomarker profile informs the presence of any actionable target and is necessary when considering further treatment with osimertinib.
It is important to note here that while panelists acknowledge osimertinib to be a valuable treatment option for patients with complex clinical presentations, including the emergence of distinct resistance mechanisms (e.g., MET amplification, PIK3CA mutation, BRAF mutation) and/or progression to acquire other genetic alterations (e.g., ALK mutation), these specific recurrence scenarios were not explored in this study.
For ex-CNS or CNS recurrences which occur during the adjuvant-osimertinib regimen and are amenable to local consolidative therapy (surgery, ablation, or radiotherapy), the panel recommended to continue adjuvant-osimertinib treatment along with local consolidative therapy if found clinically suitable (Table 3 – consensus statement 1). A consensus was achieved in pausing osimertinib regimen during radiotherapy due to severe toxicity risk in case of combined use, however, length of pause was not specified. Pausing the use of therapies such as osimertinib during radiotherapy was also recently highlighted in published consensus recommendations by the EORTC-ESTRO OligoCare consortium, where a consensus was reached to not perform SBRT within one week of the administration of anti-EGFR antibody (22).
However, in the absence of safety data in combining local consolidative therapy with osimertinib treatment, recommendations on pausing or continuing with osimertinib during ablative or surgical procedures could not be reached and instead in the absence of treatment guidelines, the decision to pause osimertinib should be based on treatment experience from the metastatic setting, i.e., considering the extent of recurrence including location, size and number of the lesions (note that the treatment guidelines for metastatic settings are also not yet established). Additionally, caution was recommended when patients are given other drugs (e.g., prophylactic antibiotics before local consolidative therapy) that could show drug-drug interactions with osimertinib.
While the place of osimertinib within the treatment strategy is dependent on multiple factors (see Section 4.2), the treatment value of rechallenging with osimertinib was thought to increase as duration between time to recurrence and completion of the adjuvant-osimertinib regimen increases. However, no consensus was achieved on the minimum recurrence free time (3, 12 or 36 months) to consider osimertinib for rechallenge.
In cases of post-adjuvant osimertinib regimen recurrence scenarios that are amenable to local consolidative therapy and rechallenging with osimertinib is suitable, the consensus is to rechallenge with osimertinib after the completion of the local consolidative therapy (Table 3 – consensus statement 2), especially in the case of radiotherapy where parallel use of osimertinib is not recommended due to the risk of toxicities. However, it is still to be determined whether stand-alone local consolidative therapy is sufficient and has curative potential in some patient cases or whether it should always be followed with osimertinib rechallenge to prevent potential distant metastasis.
In case of post-adjuvant osimertinib regimen recurrence scenarios that are not amenable to local consolidative therapy, rechallenge with osimertinib may be of high clinical value and should therefore be considered either as osimertinib monotherapy or as a part of treatment strategy involving other therapies (Table 3 – consensus statement 5).
Our study found that ex-CNS recurrence in the first 6 months is an indication of treatment failure of adjuvant-osimertinib, requiring change of treatment to either chemotherapy, other targeted therapies, or a combination of both. However, for later recurrences, continuation of osimertinib as a part of a broad treatment strategy could be potentially valuable (Table 3 – consensus statement 4) as it may prevent brain metastases, especially in case of ex-CNS recurrence.
For CNS-only recurrences, the consensus is that continuation of osimertinib as a part of a broad treatment strategy could be an effective treatment option (Table 3 – consensus statement 3). For indolent CNS recurrences, continuation of osimertinib monotherapy could also be a valuable treatment option, given the CNS recurrence could stem from underexposure to osimertinib. However, further evidence is needed on the appropriate osimertinib dosing regimen and/or combination with other therapies before these treatment approaches are considered outside clinical trials. The use of osimertinib for both ex-CNS and CNS-only recurrence was identified to be more suitable for patients with asymptomatic progression which indicates that the tumor growth is gradual and the risk of resistance to osimertinib is relatively lower than within symptomatic progression (Table 3 – consensus statements 3 & 4).
In cases where osimertinib was considered as a treatment option within the recurrence scenarios, the consensus was that treatment would continue until disease progression or toxicities were observed, or patient quality of life deteriorated. For a low progression risk patient (e.g., indolent oligometastatic progression), the duration of osimertinib treatment should be limited and a decision to stop treatment should be taken after monitoring the efficacy and patient’s health profile and considering the safety and tolerance profile of osimertinib and patient wishes (Table 3 – consensus statement 6). For a high progression risk patient, the treatment duration would be longer compared to a low progression risk patient with an aim to avoid any residual disease flare after osimertinib treatment cessation.
Outcomes from the phase 3 ADAURA trial show significant improvements in DFS and OS for EGFR-mutated NSCLC patients with stage IB to IIIA disease. Nonetheless, patterns of recurrence were reported within the osimertinib group, although lower compared with placebo (9, 10). In the absence of clinical guidance on how to treat recurrences during or after the completion of the adjuvant-osimertinib regimen, our consensus study offers a qualitative framework for clinicians in such scenarios, drawing from international expert consensus. While recognizing the importance of additional clinical data from trials and real-world settings, the study provides broader treatment considerations. It also considers osimertinib’s efficacy, as supported by FLAURA, AURA3, and ADAURA trials (7, 9, 23), with panelists acknowledging its potential benefits across various recurrence scenarios, including oligometastatic CNS recurrences and CNS metastases. In addition, panelists acknowledged the potential treatment value of combination therapies using osimertinib with local consolidative therapy, chemotherapy, and other systemic therapies; however, further efficacy and safety data is needed. The suitability of each combination approach under different recurrence scenarios was not tested in this study indicating the need for more discussion on clinical experience in the absence of concrete data.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
MM: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. AS: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. CM: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. NL: Writing – review & editing. CN: Writing – review & editing. DP: Writing – review & editing. SP: Writing – review & editing. JR: Writing – review & editing. ES: Writing – review & editing. RS: Writing – review & editing. MT: Writing – review & editing. FY: Writing – review & editing. BS: Supervision, Writing – review & editing. CG: Supervision, Writing – review & editing. Y-LW: Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by AstraZeneca, Cambridge, UK. An independent third party, Charles River Associates (CRA), designed the study, moderated the consensus meeting, and supported manuscript development.
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
NL reports research funding from Amgen, AstraZeneca Canada, Bayer, EMD Serono, Guardant Health, Lilly, MSD, MSD Oncology, Roche Canada, and Takeda; travel and accommodation support from Merck Sharp & Dohme. CN reports advisor to Medtronic, Johnson & Johnson; speaker fees from AstraZeneca, Merck Sharp & Dohme, Roche, Medtronic, Johnson & Johnson. DP reports being an advisor to AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Merck, Novartis, Pfizer, Roche, Janssen, and Abbvie; honoraria from AstraZeneca, Bristol-Myers Squibb, Celgene, Eli Lilly, Merck, Novartis, Pfizer, Roche, Janssen, and Abbvie; travel and accommodation grants from AstraZeneca, Roche, Novartis, and Pfizer; and conducting clinical trials research as principal or co-investigator institutional financial interests for AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Pfizer, Roche, Medimmun, Sanofi-Aventis, Taiho Pharma, Novocure, Daiichi Sankyo, Abbvie, and Janssen. SP reports consultancy to Amgen, AstraZeneca, Bayer, BeiGene, Blueprint, BMS, Boehringer Ingelheim, Daiichi Sankyo, EQRx, GlaxoSmithKline, Guardant Health, Janssen, Lilly, Merck KGaA, MSD, Novartis, Pfizer, Roche, Sanofi, Seattle Genetics, Takeda, and Turning Point Therapeutics. JR reports being an advisor to AbbVie, Amgen, AstraZeneca, BioAtla, BMS, Daichi-Sankyo, G1 Therapeutics, Genentech, Gritstone Bio, Guardant, Janssen, Lilly, Jazz, Summit Therapeutics Takeda; speaker fees from AstraZeneca; institutional research funding from BioAtla, AbbVie, AstraZeneca, Blueprint, RedCloud, Loxo Oncology, Daiichi Sankyo, Enliven, ORIC, and Summit. ES reports being an advisor to AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Lilly, Merck KGaA, MSD Oncology, Novartis, Roche/Genentech, Seagen, and Takeda; honoraria from AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo/Astra Zeneca, and Merck KGaA; research funding from AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, and Roche/Genentech. RS reports being an advisor to Amgen, AstraZeneca, Bayer, BMS, Boehringer Ingelheim, Janssen, Lily, Merck, Merck Serono, Novartis, Pfizer, Puma, Roche, Taiho, Takeda, Thermo Fisher, Yuhan and has received research grants from AstraZeneca and Boehringer Ingelheim. MT reports being an advisor to AstraZeneca Japan, Chugai Pharma, Lilly Japan, MSD, Novartis and MiREXS; honoraria from AstraZeneca Japan, Bristol-Myers Squibb Japan, Chugai Pharma, Johnson & Johnson, Lilly Japan, Medtronic, MSD K.K, Novartis, Ono Pharmaceutical, Taiho Pharmaceutical, and Teijin Pharma; research funding from AstraZeneca Japan, Boehringer Ingelheim KK, Bristol-Myers Squibb KK, Merck, Ono Pharmaceutical, BMG Incorporated, and MiREXS. FY reports speaker fees from MSD, Pfizer, Roche, AstraZeneca, and Bristol-Myers Squibb. BS reports wife’s employment with PPD and Xalud Therapeutics; leadership at Verrica Pharmaceuticals; stock and other ownership interests in Pfizer, PPD, and Xalud Therapeutics; personal honoraria from AstraZeneca, Bristol Myers Squibb, Genentech, and Pfizer; consulting or advisor role at AstraZeneca, Gala Therapeutics, Medtronic, Arcus Biosciences, and Pfizer; research funding from Bristol Myers Squibb Foundation; patents, royalties, and other intellectual property related with a therapeutic antibody targeting ART1, an extracellular mono-ADP ribosyltransferase, for the treatment of cancer patent application filed; other relationship with Lung Cancer Research Foundation and Lungevity. CG reports being an advisor to AstraZeneca, Boehringer Ingelheim, and MSD Oncology; honoraria from AstraZeneca, Boehringer Ingelheim, Lilly, MSD Oncology, Novartis, Roche, and Takeda; research funding from AstraZeneca; travel and accommodation support from Boehringer Ingelheim, Bristol-Myers Squibb, and Roche. Y-LW reports being an advisor to AstraZeneca, Boehringer Ingelheim, Roche, and Takeda; honoraria from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb/China, Hengrui Pharmaceutical, Lilly, MSD Oncology, Pfizer, and Roche; research funding from Boehringer Ingelheim, Pfizer, and Roche.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1330468/full#supplementary-material
CNS, central nervous system; CT, computerized tomography; DFS, disease-free survival; EGFRm, Epidermal growth factor receptor mutation; HR, hazard ratio; HRQoL, Health-related quality of life; MDT, multi-disciplinary team; MRD, minimal residual disease; MRI, magnetic resonance imaging; NGS, next-generation sequencing); OS, overall survival; PET, positron emission tomography; SBRT, stereotactic body radiation therapy; SRS, stereotactic radiosurgery; TKI, tyrosine kinase inhibitor; NSCLC,non-small-cell lung cancer; WBRT, whole-brain radiotherapy.
1. American Lung Association. EGFR and lung Cancer (2022). Available at: https://www.lung.org/lung-health-diseases/lung-disease-lookup/lung-cancer/symptoms-diagnosis/biomarker-testing/egfr (Accessed 13 February 2023).
2. O’Leary C, Gasper H, Sahin KB, Tang M, Kulasinghe A, Adams MN, et al. Epidermal growth factor receptor (EGFR)-mutated non-small-cell lung cancer (NSCLC). Pharmaceuticals (2020) 13(10):273. doi: 10.3390/ph13100273
3. Ellison G, Zhu G, Moulis A, Dearden S, Speake G, McCormack R. EGFR mutation testing in lung cancer: a review of available methods and their use for analysis of tumor tissue and cytology samples. J Clin pathol (2013) 66(2):79–89. doi: 10.1136/jclinpath-2012-201194
4. Melosky B, Kambartel K, Häntschel M, Bennetts M, Nickens DJ, Brinkmann J, et al. Worldwide prevalence of epidermal growth factor receptor mutations in non-small cell lung cancer: a meta-analysis. Mol Diagn Ther (2022) 26(1):7–18. doi: 10.1007/s40291-021-00563-1
5. Roviello G, Imperatori M, Aieta M, Sollitto F, Landriscina M. Adjuvant treatment for EGFR-mutated non-small cell lung cancer: do we have a major breakthrough? J Thorac Disease (2018) 10(Suppl 18):S2114. doi: 10.21037/jtd.2018.06.114
6. Zhao P, Zhen H, Zhao H, Zhao L, Cao B. Efficacy and safety of adjuvant EGFR-TKIs for resected non-small cell lung cancer: a systematic review and meta-analysis based on randomized control trials. BMC cancer (2022) 22(1):1–5. doi: 10.1186/s12885-022-09444-0
7. Mok TS, Wu YL, Ahn MJ, Garassino MC, Kim HR, Ramalingam SS, et al. Osimertinib or platinum–pemetrexed in EGFR T790M–positive lung cancer. New Engl J Med (2017) 376(7):629–40. doi: 10.1056/nejmoa1612674
8. Wu YL, Tsuboi M, He J, John T, Grohe C, Majem M, et al. Osimertinib in resected EGFR-mutated non–small-cell lung cancer. New Engl J Med (2020) 383(18):1711–23. doi: 10.1056/NEJMoa2027071
9. Herbst RS, Wu YL, John T, Grohe C, Majem M, Wang J, et al. Adjuvant osimertinib for resected EGFR-mutated stage IB-IIIA non–small-cell lung cancer: updated results from the phase III randomized adaura trial. J Clin Oncol (2023) 41(10):1830. doi: 10.1200/jco.22.02186
10. Tsuboi M, Herbst RS, John T, Kato T, Majem M, Grohé C, et al. Overall survival with osimertinib in resected EGFR-mutated NSCLC. New Engl J Med (2023) 389:137–47. doi: 10.1056/NEJMoa2304594
11. Isla D, Felip E, Garrido P, Insa A, Majem M, Remon J, et al. A Delphi consensus panel about clinical management of early-stage EGFR-mutated non-small cell lung cancer (NSCLC) in Spain: A Delphi consensus panel study. Clin Trans Oncol (2023) 25(1):283–91. doi: 10.1007/s12094-022-02941-5
12. Passaro A, Leighl N, Blackhall F, Popat S, Kerr K, Ahn MJ, et al. ESMO expert consensus statements on the management of EGFR mutant non-small-cell lung cancer. Ann Oncol (2022) 33(5):466–87. doi: 10.1016/j.annonc.2022.02.003
13. College of American Pathologists. The Liquid Biopsy . Available at: https://www.cap.org/member-resources/articles/the-liquid-biopsy (Accessed 03 August 2023).
14. Kunimasa K, Mimura C, Kotani Y. Erlotinib is effective for leptomeningeal carcinomatosis due to disease flare after osimertinib treatment failure. J Thorac Oncol (2017) 12(7):e93–4. doi: 10.1016/j.jtho.2017.02.025
15. Takahashi T, Umeguchi H, Tateishi A, Yoshida T, Motoi N, Ohe Y. Disease flare of leptomeningeal metastases without radiological and cytological findings after the discontinuation of osimertinib. Lung Cancer (2021) 151:1–4. doi: 10.1016/j.lungcan.2020.11.010
16. Popat S, Navani N, Kerr KM, Smit EF, Batchelor TJ, Van Schil P, et al. Navigating diagnostic and treatment decisions in non-small cell lung cancer: expert commentary on the multidisciplinary team approach. Oncol (2021) 26(2):e306–15. doi: 10.1002/onco.13586
17. NCCN. Non-Small Cell Lung Cancer Version 4.2019, NCCN Guidelines (2019). Available at: https://www.nccn.org/guidelines/guidelines-process/transparency-process-and-recommendations/GetFileFromFileManagerGuid?FileManagerGuidId=8fc17b3b-ec6c-4758-b0c7-15c51649fc64.
18. Planchard D, Popat ST, Kerr K, Novello S, Smit EF, Faivre-Finn C, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29:iv192–237. doi: 10.1093/annonc/mdy275
19. Park K, Vansteenkiste J, Lee KH, Pentheroudakis G, Zhou C, Prabhash K, et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with locally-advanced unresectable non-small-cell lung cancer: a KSMO-ESMO initiative endorsed by CSCO, ISMPO, JSMO, MOS, SSO and TOS. Ann Oncol (2020) 31(2):191–201. doi: 10.1016/j.annonc.2019.10.026
20. Wu YL, Planchard D, Lu S, Sun H, Yamamoto N, Kim DW, et al. Pan-Asian adapted Clinical Practice Guidelines for the management of patients with metastatic non-small-cell lung cancer: a CSCO–ESMO initiative endorsed by JSMO, KSMO, MOS, SSO and TOS. Ann Oncol (2019) 30(2):171–210. doi: 10.1093/annonc/mdy554
21. Postmus PE, Kerr KM, Oudkerk M, Senan S, Waller DA, Vansteenkiste J, et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2017) 28:iv1–21. doi: 10.1093/annonc/mdx222
22. Kroeze SG, Pavic M, Stellamans K, Lievens Y, Becherini C, Scorsetti M, et al. Metastases-directed stereotactic body radiotherapy in combination with targeted therapy or immunotherapy: systematic review and consensus recommendations by the EORTC–ESTRO OligoCare consortium. Lancet Oncol (2023) 24(3):e121–32. doi: 10.1016/S1470-2045(22)00752-5
Keywords: osimertinib, non-small cell lung cancer, adjuvant treatment, EGFR mutation, recurrence, treatment sequencing
Citation: Mirza M, Shrivastava A, Matthews C, Leighl N, Ng CSH, Planchard D, Popat S, Rotow J, Smit EF, Soo R, Tsuboi M, Yang F, Stiles B, Grohe C and Wu Y-L (2024) Treatment decision for recurrences in non-small cell lung cancer during or after adjuvant osimertinib: an international Delphi consensus report. Front. Oncol. 13:1330468. doi: 10.3389/fonc.2023.1330468
Received: 30 October 2023; Accepted: 31 December 2023;
Published: 23 January 2024.
Edited by:
Yusuke Okuma, National Cancer Center Hospital, JapanReviewed by:
Alberto Pavan, Azienda ULSS 3 Serenissima, ItalyCopyright © 2024 Mirza, Shrivastava, Matthews, Leighl, Ng, Planchard, Popat, Rotow, Smit, Soo, Tsuboi, Yang, Stiles, Grohe and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Myriam Mirza, bW1pcnphQGNyYWkuY29t
†These authors have contributed equally to this work
‡Steering committee members (study supervisors)
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.