 Andrea Pace1
Andrea Pace1 Giuseppe Lombardi2Veronica Villani1Dario Benincasa1Claudia Abbruzzese1
Giuseppe Lombardi2Veronica Villani1Dario Benincasa1Claudia Abbruzzese1 Ilaria Cestonaro2Martina Corrà2
Ilaria Cestonaro2Martina Corrà2 Marta Padovan2Giulia Cerretti2
Marta Padovan2Giulia Cerretti2 Mario Caccese2
Mario Caccese2 Antonio Silvani3Paola Gaviani3Diana Giannarelli4Gennaro Ciliberto1
Antonio Silvani3Paola Gaviani3Diana Giannarelli4Gennaro Ciliberto1 Marco G. Paggi1*
Marco G. Paggi1*- 1IRCCS - Regina Elena National Cancer Institute, Rome, Italy
- 2Veneto Institute of Oncology IOV-IRCCS, Padua, Italy
- 3IRCCS Besta Neurological Institute, Milan, Italy
- 4Fondazione Policlinico Universitario A. Gemelli, IRCCS, Rome, Italy
Introduction: Drug repurposing is a promising strategy to develop new treatments for glioblastoma. In this phase II clinical trial, we evaluated the addition of chlorpromazine to temozolomide in the adjuvant phase of the standard first-line therapeutic protocol in patients with unmethylated MGMT gene promoter.
Methods: This was a multicenter phase II single-arm clinical trial. The experimental procedure involved the combination of CPZ with standard treatment with TMZ in the adjuvant phase of the Stupp protocol in newly-diagnosed GBM patients carrying an unmethylated MGMT gene promoter. Progression-free survival was the primary endpoint. Secondary endpoints were overall survival and toxicity.
Results: Forty-one patients were evaluated. Twenty patients (48.7%) completed 6 cycles of treatment with TMZ+CPZ. At 6 months, 27 patients (65.8%) were without progression, achieving the primary endpoint. Median PFS was 8.0 months (95% CI: 7.0-9.0). Median OS was 15.0 months (95% CI: 13.1-16.9). Adverse events led to reduction or interruption of CPZ dosage in 4 patients (9.7%).
Discussion: The addition of CPZ to standard TMZ in the first-line treatment of GBM patients with unmethylated MGMT gene promoter was safe and led to a longer PFS than expected in this population of patients. These findings provide proof-of-concept for the potential of adding CPZ to standard TMZ treatment in GBM patients with unmethylated MGMT gene promoter.
Clinical trial registration: https://clinicaltrials.gov/study/NCT04224441, identifier NCT04224441.
1 Introduction
Glioblastoma (GBM) is a frequent and severe brain tumor, characterized by poor response to treatment and an almost certainty of relapse. First-line GBM treatment, regardless of the molecular classification of the disease (1), consists in maximal surgical resection followed by radiotherapy with concomitant temozolomide (TMZ) treatment, followed by adjuvant TMZ. This scheme is however associated with a median overall survival (OS) of 14.6 months and a 5-year survival <5% (2), therefore leaving an unmet clinical need.
GBM presents high invasive and infiltrative properties (3), also coupled with a distinctive cellular heterogeneity, a prerequisite for a swift adaptation to treatment (4–7). Indeed, GBM has the ability to recover from genetic damages induced by radiotherapy and TMZ by means of an effective DNA repair system, especially in tumors characterized by unmethylated O6-methylguanine methyltransferase (MGMT) gene promoter (8). Of note, GBM is among the few tumors in which a single-drug treatment is currently in use: it may be possible to speculate that the addition of another therapy may help overcome resistance to TMZ (9).
An interesting characteristic of GBM is its responsiveness to neurotransmitters, as monoamines (10–12). The well-known interplay between neurons and tumors, especially GBM (11, 13), and the more recent identification of a synaptic neuron-GBM connectivity (14) confirms that neuron-secreted mediators are taken up by GBM cells, where they act as oncogenic stimuli (15). These findings paved the way for considering the addition of selected neuroleptic drugs as potential addition to GBM treatment (16). Indeed, many psychotropic drugs act on multiple postsynaptic receptors and display diverse pharmacological activity (16), including the ability to counteract GBM growth in vitro (17–19). Upon these assumptions, we evaluated the effects of one of the progenitors of neuroleptic medications, i.e., the antipsychotic drug chlorpromazine (CPZ), in use for about 70 years for psychiatric disorders in GBM patients. CPZ is a compound listed in the 2021 WHO Model List of Essential Medicines (20).
In an in vitro study, our group has already assayed CPZ effects on established and primary human GBM cells. The results defined the role of this drug in hindering GBM cell growth by acting at different levels through multimodal antitumor effects without any relevant action on non-cancer neuroepithelial cells (21, 22). In addition, CPZ acts synergistically with TMZ in hindering GBM vitality and stemness capabilities (21).
CPZ is a safe, low-cost and promptly available medication. All these conditions paved the way for repurposing CPZ as an add-on drug in GBM therapy. To this end, we planned the RACTAC (Repurposing the Antipsychotic drug Chlorpromazine as a Therapeutic Agent in the Combined treatment of newly diagnosed glioblastoma) phase II multicenter, single-arm study, in which CPZ is added to adjuvant TMZ in the first-line therapy of GBM patients whose tumor is characterized by an unmethylated MGMT gene promoter (8).
This study was designed with the purpose of investigating the clinical efficacy and safety of the addition of CPZ to the adjuvant TMZ administration in the first-line treatment of GBM patients carrying an unmethylated MGMT gene promoter.
2 Materials and methods
2.1 Study design
This was a multicenter, phase II single-arm clinical trial conducted in three Italian referral centers: the Regina Elena National Cancer Institute (Rome), the Veneto Institute of Oncology (Padua) and the Besta Neurological Institute (Milan).
The experimental procedure involved the combination of CPZ with standard treatment with TMZ in the adjuvant phase of the Stupp protocol (2) in newly diagnosed GBM patients carrying an unmethylated MGMT gene promoter. All patients received CPZ tablets [“Largactil”, Teofarma S.R.L., Valle Salimbene (PV), Italy], during TMZ adjuvant treatment at a starting dose of 25 mg/day orally from day 1 onwards. The dosage was increased to 50 mg/day at the second cycle of treatment, if well tolerated, and continued for 6 cycles or until disease progression, death, unacceptable toxicity, or consent withdrawal (Figure 1).
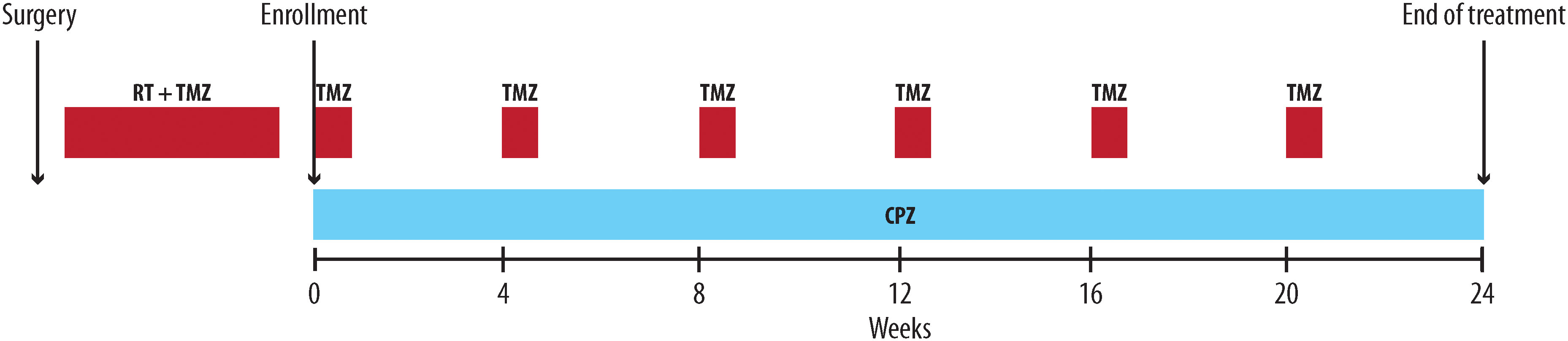
Figure 1 The RACTAC scheme: Scheme of the daily addition of CPZ during the adjuvant phase of the first line protocol for newly diagnosed GBM patients with unmethylated MGMT gene promoter. RT, radiotherapy; TMZ, temozolomide; CPZ, chlorpromazine.
This clinical trial has been approved by our Institutional Ethics Committee on September 6, 2019, and is registered as EudraCT #2019-001988-75 and ClinicalTrials.gov Identifier #NCT0422444.
2.2 Eligibility
Patients aged 18-75 years with newly diagnosed and histologically confirmed supratentorial GBM (World Health Organization 2016) and unmethylated MGMT gene promoter status were eligible. MGMT gene promoter methylation status was assessed in a local laboratory for each participating center by pyrosequencing or methylation-specific PCR. Additional inclusion criteria were: gadolinium (Gd)-enhanced MRI 48 h after surgery; stable or decreasing dose of steroids for 1 week before enrolment; Karnofski performance status (KPS) ≥70; satisfactory laboratory blood and biochemical results within 2 weeks prior to enrolment.
2.3 Endpoints
Progression-Free Survival (PFS) was the primary endpoint of this study. PFS was defined as the time from the start of the Stupp regimen (2) to the earliest documented date of disease progression, based on Response Assessment in Neuro-Oncology (RANO) criteria (23, 24), as determined by the investigator, death due to any cause, or censored at the date of the last assessment. Evaluating a meta-analysis of 91 GBM clinical trials, the choice of PFS as an endpoint can be considered appropriate as a surrogate endpoint for earlier evaluation. The 6-month PFS appears correlated with 1-year overall survival (OS) and median OS (25).
The secondary endpoints of this study were: (i) Overall survival (OS); defined as the time from diagnosis to the date of death from any cause or loss-to-follow-up); (ii) combination treatment toxicity. Adverse events (AEs) were evaluated according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events version 5.0. Safety assessments were performed from treatment initiation through 30 days after the last dose of chemotherapy with TMZ plus CPZ; (iii) Quality of Life (QoL), assessed by means of the EORTC QLQ C30+BN20 questionnaire at baseline and every 3 cycles (26, 27). Data on QoL are under evaluation at the time of drafting of this manuscript and will be presented in a separate paper.
2.4 Follow-up
Patients were followed-up monthly during adjuvant chemotherapy and every 3 months after completion of the standard treatment if the disease was stable. Radiological assessment was done by Gd brain MRI every 12 weeks from the first drug administration until progression.
Response assessment during study was based on investigators’ evaluation using the RANO criteria (23, 24), which included blinded interpretation of MRI scans, assessment of neurological status, KPS scores, and steroid use.
2.5 Statistical analysis
All analyses were performed for the patients who received at least one dose of the study treatment. The primary objective of the study was to evaluate the proportion of patients free from progression after 6 months (PFS-6). Considering as unacceptable a percentage of PFS-6 (P0) equal to 35% and a desirable PFS-6 of 55% (P1), a minimum of 41 patients would be needed to guarantee a power of 80% at a significance level of 5% (one-sided) (28). If at least 20 patients were progression-free after 6 months, the treatment would be considered sufficiently active. All survival curves were estimated using the Kaplan-Meier method.
Clinical and demographic characteristics are reported as absolute counts and percentage when related to categorical items and as median and range if referred to quantitative variables.
3 Results
3.1 Patient characteristics
Between April 2020 and August 2022, 45 patients were screened; 41 received at least one cycle of treatment and were included in the final analysis. Study follow-up was closed on December 31, 2022. Patients’ baseline characteristics and demographics are summarized in Table 1. The study was not adequately powered to determine whether there were any sex differences in clinical response to the treatment.
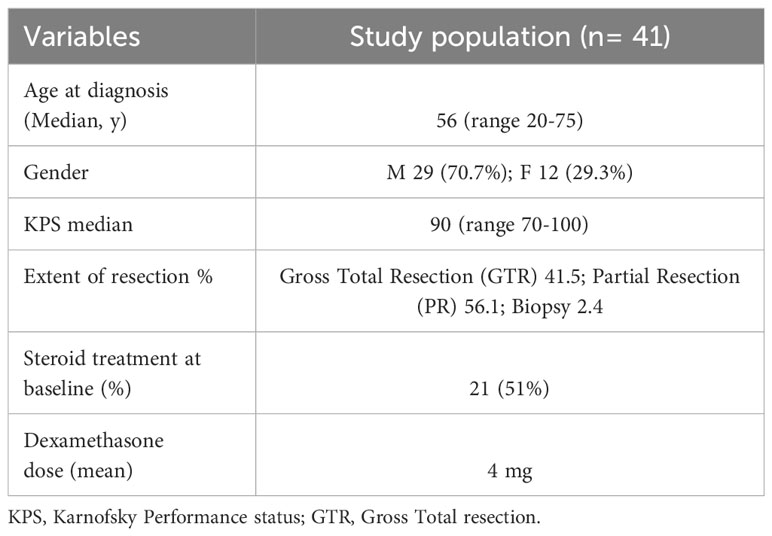
Table 1 Baseline characteristics of the enrolled GBM patients.
Twenty patients (48.7%) completed 6 cycles of treatment with TMZ at standard dose plus CPZ; twenty-one patients (51.2%) discontinued the treatment due to early progression (median cycles completed = 5.5, range 2-6). The median follow-up was 15 months (range 3-37).
3.2 Progression-free survival
At 6 months, 27 (65.8%) patients were alive and without progression: thus, the primary endpoint was achieved. Overall, 35 patients (85.4%) experienced disease progression, with a median PFS of 8.0 months (95% CI: 7.0-9.0) (Figure 2). PFS at different time points is reported in Table 2.
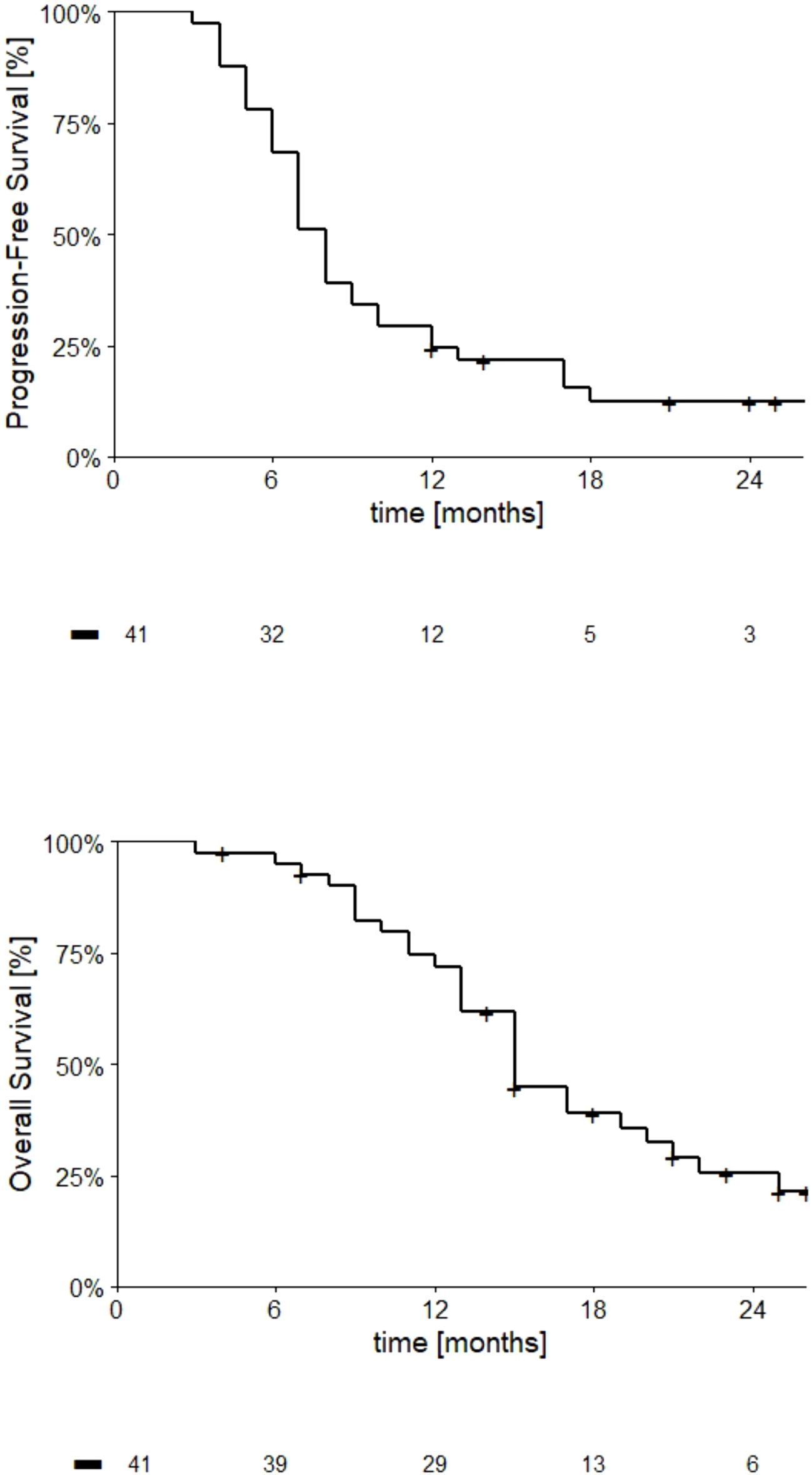
Figure 2 Kaplan-Meier curves describing PFS and OS trends (upper and lower charts, respectively) in GBM patients with unmethylated MGMT gene promoter treated according to the RACTAC protocol. The number of patients at risk at respective time points are indicated below the abscissa.

Table 2 Progression-free survival (PFS) and overall survival (OS) in GBM patients with unmethylated MGMT gene promoter treated according to the RACTAC protocol.
3.3 Overall survival
At study closure, 29 deaths (69.7%) have been observed, and median overall survival was 15.0 months (95% CI: 13.1-16.9). OS at different time-points is reported in Figure 2; Table 2.
3.4 Role of the extent of resection
Patients who underwent a gross total resection (GTR) had a longer PFS and OS than patients who underwent a partial resection (PR). As described (29), the extent of resection is an important prognostic factor for survival in glioblastoma (GBM) patients. This is also true in our case series, which was developed on a chronological basis and is representative of the general population of these patients, with a prevalence of PRs plus one case of biopsy.
3.5 Toxicity
The treatment scheme was associated with the onset of an expected dose-dependent sedation, especially at the beginning of the CPZ administration, and liver toxicity (1 serious case), however expected for both CPZ and TMZ. Treatment was well tolerated in all patients with mild somnolence (grade 1-2) in 8 (19.5%) and asthenia in 12 (29.2%) patients. In three patients, grade 3-4 hyper-transaminasaemia was observed (7%). Adverse events led to reduction or interruption of CPZ dosage in 4 patients (9.7%). Decreased platelets count grade 3 was observed in one patient and neutropenia grade 3 in one. All these data are summarized in Table 3.
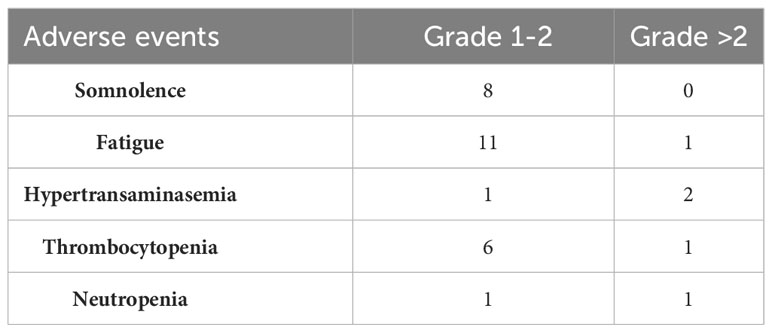
Table 3 Drug-related adverse events.
4 Discussion
GBM patients with unmethylated MGMT gene promoter comprise 55-60% of total GBM cases and have a poorer prognosis due to their intrinsic resistance to alkylating agents. At present, while it is well recognized that TMZ brings a benefit in patients with methylated MGMT gene promoter, its use in cases of unmethylated MGMT gene promoter is still controversial. Indeed, EANO evidence-based guidelines on diagnosis and treatment of diffuse gliomas of adulthood report that TMZ might only be effective in GBM patients with methylated MGMT gene promoter, whereas its effectiveness on patients with unmethylated MGMT gene promoter is modest (8, 30).
Various therapeutic strategies have been investigated in phase II clinical trials to overcome drug resistance or bypass DNA repair pathways in GBM patients with unmethylated MGMT gene promoter (8, 31). In the same setting, addition of drugs other than TMZ alone in the first-line treatment did not lead to encouraging results (32–34). Other studies evaluated the efficacy of new agents as replacements for TMZ in the first-line treatment of GBM patients with unmethylated MGMT gene promoter. For example, in the EORTC 26082 phase II trial, temsirolimus was administered either during radiotherapy or as adjuvant treatment, showing no clinical benefit (35). In a single arm phase II trial, enzastaurin, a protein kinase C inhibitor, administered before, concomitantly with, and after radiotherapy in GBM patients with unmethylated MGMT gene promoter, did not achieve the primary endpoint of PFS at 6 months (36). On the other hand, in the same population of GBM patients, bevacizumab plus irinotecan provided a better PFS at 6 months than TMZ, but with no improvement in OS (37).
Our results show that the addition of CPZ to standard TMZ in the first-line treatment of GBM patients with unmethylated MGMT gene promoter was safe and led to a longer PFS, i.e., 8.0, than expected in this patient population. This finding met the primary endpoint of the study. A recent meta-analysis of five phase III clinical trials found that the standard-of-care treatment for GBM patients with unmethylated MGMT gene promoter results in a PFS of 4.99 months and an OS of 14.11 months (38).
In our study, however, median OS was 15 months, thus not representing a clinically relevant improvement over the data reported in this meta-analysis. Such an outcome could also relate to the administration of CPZ only in the adjuvant phase of treatment. Further studies are needed to investigate the concomitant association of CPZ also during radiotherapy.
The safety profile of CPZ was consistent with its well-known pharmacological profile, even when administered concomitantly with TMZ. In our study, the most frequent adverse event were mild somnolence (grade 1-2) in 18% of patients, usually in the first month of treatment, and fatigue, observed in 30% of patients, a symptom commonly reported within a range of 40-70% in primary brain tumor patients (39).
Quality of life (QoL) is an important outcome to be evaluated in these GBM patients. In our study, it has been measured by means of the EORTC QLQ-C30 and QLQ-BN20 questionnaires. These evaluations are currently in progress, and the results will be published shortly.
Most relevant limitations of the RACTAC trial are the small number of patients included in the study and the lack of a control group. However, the clinical characteristics of the patients at baseline appear representative of the real-world population of unmethylated MGMT gene promoter GBM. The PFS observed in this trial was 8.0 months and resulted promisingly longer than that reported in previous published trials in this population.
CPZ is a well-known DRD2 antagonist (40) and therefore has been successfully used in the treatment of psychiatric disorders. We intended to take advantage of its ability to interfere with the function of DRD2, as well as a number of other neuromediator receptors (https://go.drugbank.com/drugs/DB00477), to hamper the pseudo-synaptic, oncogenic interplay between neurons and GBM. In addition, it should be considered that there is also a profound interplay between peripheral/central nervous systems and cancer, which acts through monoamine neuromediators and could represent a vulnerability targetable through the use of repurposed neuropsychiatric drugs in oncology and appliable to diverse cancer types (41, 42).
Evaluating the features of CPZ possibly useful in GBM treatment, we could also consider a number of studies showing the ability of this drug to hinder GBM malignant features in preclinical settings (43). In the same context, during the course of the RACTAC clinical trial, our group further refined the pharmacological effects of CPZ on GBM cells in vitro, demonstrating the ability of this medication to hinder GBM malignant features at multiple levels (21, 22) other than its known interference with the activity of neurotransmitters.
Since the plasticity of GBM and its ability to remodulate its cell population based on the selective pressure generated by therapies, we can state that this tumor cannot be defined as a “single-path disease”, being therefore quite unsatisfying to treat it by means of targeted therapies. On these premises, it appears reasonable to consider the opportunity to use “dirty drugs”, i.e., drugs that are not too targeted, but are able to hit some generalized vulnerabilities characterizing cancer cells.
Considering the escalation of the costs of novel anticancer medications, the long time it takes for them to reach the market and the consequent nonavailability for a great number of patients, the use of repurposed drugs can dramatically cut down time and drug expenses for effective medications to reach the bedside, with significant benefits for the patients and the Health Systems. In addition, the characteristics inherent in repositionable drugs represent a further therapeutic chance for GBM patients for which no second-line therapy is currently established as effective or for those that have already experienced all known therapeutic opportunities.
The RACTAC phase II clinical study was designed to investigate whether adding CPZ to the standard adjuvant TMZ in the Stupp protocol could improve therapeutic efficacy in patients with GBM with an unmethylated MGMT gene promoter. It also assessed the tolerability of adding a neuroleptic medication to GBM patients after neurosurgery and combined chemo-radiotherapy. This clinical trial is a proof-of-concept for the effectiveness of interfering with oncogenic monoamine signaling between neurons and GBM to inhibit tumor growth and malignancy, and, although not exhaustive, it can support the initiation of a subsequent phase III randomized clinical study.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: GARR repository at the following link: https://gbox.garr.it/garrbox/s/HZ2g4aBD26lJh1e.
Ethics statement
The studies involving humans were approved by Comitato Etico Centrale IRCCS – Sezione IFO-Fondazione Bietti, Roma (EudraCT # 2019-001988-75; ClinicalTrials.gov Identifier: NCT04224441). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AP: Conceptualization, Data curation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. GL: Data curation, Resources, Validation, Writing – review & editing. VV: Data curation, Writing – review & editing. DB: Data curation, Writing – review & editing. CA: Data curation, Writing – review & editing. IC: Data curation, Resources, Writing – review & editing. MCo: Data curation, Resources, Writing – review & editing. MP: Data curation, Resources, Writing – review & editing. GCe: Data curation, Resources, Writing – review & editing. MCa: Data curation, Resources, Writing – review & editing. AS: Data curation, Writing – review & editing. PG: Data curation, Resources, Writing – review & editing. DG: Data curation, Formal analysis, Writing – review & editing. GCi: Funding acquisition, Supervision, Writing – review & editing. MGP: Conceptualization, Data curation, Funding acquisition, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Work partially financed by Funds Ricerca Corrente 2018-2019, 2020-2021, 2022-2023 from Italian Ministry of Health (GC, MGP) and by the European Union - NextGenerationEU through the Italian Ministry of University and Research under PNRR - M4C2-I1.3 Project PE_00000019 “HEAL ITALIA” to Marco G. Paggi, CUP H83C22000550006. This work was financially supported through funding from the institutional “Ricerca Corrente” granted by the Italian Ministry of Health. The views and opinions expressed are those of the authors only and do not necessarily reflect those of the European Union or the European Commission. Neither the European Union nor the European Commission can be held responsible for them.
Acknowledgments
This paper is dedicated to the memory of our friend and colleague Armando Felsani, who recently passed away and who contributed so much to the advancement of knowledge in the field of cell differentiation and cell cycle regulation. We thank Luca Giacomelli, PhD, for useful discussion. Editorial and graphical assistance were provided by Aashni Shah, Valentina Attanasio and Massimiliano Pianta (Polistudium SRL, Milan, Italy), and was supported by internal funds. We thank the patients who participated in the RACTAC trial and their families.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol (2016) 131(6):803–20. doi: 10.1007/s00401-016-1545-1
2. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med (2005) 352(10):987–96. doi: 10.1056/NEJMoa043330
3. Rao JS. Molecular mechanisms of glioma invasiveness: the role of proteases. Nat Rev Cancer (2003) 3(7):489–501. doi: 10.1038/nrc1121
4. Lan X, Jorg DJ, Cavalli FMG, Richards LM, Nguyen LV, Vanner RJ, et al. Fate mapping of human glioblastoma reveals an invariant stem cell hierarchy. Nature (2017) 549(7671):227–32. doi: 10.1038/nature23666
5. Gimple RC, Bhargava S, Dixit D, Rich JN. Glioblastoma stem cells: lessons from the tumor hierarchy in a lethal cancer. Genes Dev (2019) 33(11-12):591–609. doi: 10.1101/gad.324301.119
6. Couturier CP, Ayyadhury S, Le PU, Nadaf J, Monlong J, Riva G, et al. Single-cell RNA-seq reveals that glioblastoma recapitulates a normal neurodevelopmental hierarchy. Nat Commun (2020) 11(1):3406. doi: 10.1038/s41467-020-17186-5
7. Hubert CG, Lathia JD. Seeing the GBM diversity spectrum. Nat Cancer (2021) 2(2):135–7. doi: 10.1038/s43018-021-00176-x
8. Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med (2005) 352(10):997–1003. doi: 10.1056/NEJMoa043331
9. Czarnywojtek A, Borowska M, Dyrka K, Van Gool S, Sawicka-Gutaj N, Moskal J, et al. Glioblastoma multiforme: the latest diagnostics and treatment techniques. Pharmacology (2023) 108(5):423–31. doi: 10.1159/000531319
10. Caragher SP, Hall RR, Ahsan R, Ahmed AU. Monoamines in glioblastoma: complex biology with therapeutic potential. Neuro Oncol (2018) 20(8):1014–25. doi: 10.1093/neuonc/nox210
11. Caragher SP, Shireman JM, Huang M, Miska J, Atashi F, Baisiwala S, et al. Activation of dopamine receptor 2 prompts transcriptomic and metabolic plasticity in glioblastoma. J Neurosci (2019) 39(11):1982–93. doi: 10.1523/JNEUROSCI.1589-18.2018
12. Venkataramani V, Tanev DI, Strahle C, Studier-Fischer A, Fankhauser L, Kessler T, et al. Glutamatergic synaptic input to glioma cells drives brain tumour progression. Nature (2019) 573(7775):532–8. doi: 10.1038/s41586-019-1564-x
13. Barygin OI, Nagaeva EI, Tikhonov DB, Belinskaya DA, Vanchakova NP, Shestakova NN. Inhibition of the NMDA and AMPA receptor channels by antidepressants and antipsychotics. Brain Res (2017) 1660:58–66. doi: 10.1016/j.brainres.2017.01.028
14. Hanahan D, Monje M. Cancer hallmarks intersect with neuroscience in the tumor microenvironment. Cancer Cell (2023) 41(3):573–80. doi: 10.1016/j.ccell.2023.02.012
15. Venkataramani V, Schneider M, Giordano FA, Kuner T, Wick W, Herrlinger U, et al. Disconnecting multicellular networks in brain tumours. Nat Rev Cancer (2022) 22(8):481–91. doi: 10.1038/s41568-022-00475-0
16. Persico M, Abbruzzese C, Matteoni S, Matarrese P, Campana AM, Villani V, et al. Tackling the behavior of cancer cells: molecular bases for repurposing antipsychotic drugs in the treatment of glioblastoma. Cells (2022) 11(2):263. doi: 10.3390/cells11020263
17. Oliva CR, Zhang W, Langford C, Suto MJ, Griguer CE. Repositioning chlorpromazine for treating chemoresistant glioma through the inhibition of cytochrome c oxidase bearing the COX4-1 regulatory subunit. Oncotarget (2017) 8(23):37568–83. doi: 10.18632/oncotarget.17247
18. Kang S, Lee JM, Jeon B, Elkamhawy A, Paik S, Hong J, et al. Repositioning of the antipsychotic trifluoperazine: Synthesis, biological evaluation and in silico study of trifluoperazine analogs as anti-glioblastoma agents. Eur J Med Chem (2018) 151:186–98. doi: 10.1016/j.ejmech.2018.03.055
19. Omoruyi SI, Ekpo OE, Semenya DM, Jardine A, Prince S. Exploitation of a novel phenothiazine derivative for its anti-cancer activities in Malignant glioblastoma. Apoptosis (2020) 25(3-4):261–74. doi: 10.1007/s10495-020-01594-5
20. World Health Organization. World Health Organization Model List of Essential Medicines, 22nd List. Geneva: World Health Organization (2021). Available at: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02.
21. Matteoni S, Matarrese P, Ascione B, Buccarelli M, Ricci-Vitiani L, Pallini R, et al. Anticancer properties of the antipsychotic drug chlorpromazine and its synergism with temozolomide in restraining human glioblastoma proliferation in vitro. Front Oncol (2021) 11:635472. doi: 10.3389/fonc.2021.635472
22. Matteoni S, Matarrese P, Ascione B, Ricci-Vitiani L, Pallini R, Villani V, et al. Chlorpromazine induces cytotoxic autophagy in glioblastoma cells via endoplasmic reticulum stress and unfolded protein response. J Exp Clin Cancer Res (2021) 40(1):347. doi: 10.1186/s13046-021-02144-w
23. Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol (2010) 28(11):1963–72. doi: 10.1200/JCO.2009.26.3541
24. Radbruch A, Fladt J, Kickingereder P, Wiestler B, Nowosielski M, Baumer P, et al. Pseudoprogression in patients with glioblastoma: clinical relevance despite low incidence. Neuro Oncol (2015) 17(1):151–9. doi: 10.1093/neuonc/nou129
25. Han K, Ren M, Wick W, Abrey L, Das A, Jin J, et al. Progression-free survival as a surrogate endpoint for overall survival in glioblastoma: a literature-based meta-analysis from 91 trials. Neuro Oncol (2014) 16(5):696–706. doi: 10.1093/neuonc/not236
26. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
27. Osoba D, Aaronson NK, Muller M, Sneeuw K, Hsu MA, Yung WK, et al. The development and psychometric validation of a brain cancer quality-of-life questionnaire for use in combination with general cancer-specific questionnaires. Qual Life Res (1996) 5(1):139–50. doi: 10.1007/BF00435979
28. A'Hern RP. Sample size tables for exact single-stage phase II designs. Stat Med (2001) 20(6):859–66. doi: 10.1002/sim.721
29. Katsigiannis S, Grau S, Krischek B, Er K, Pintea B, Goldbrunner R, et al. MGMT-positive vs MGMT-negative patients with glioblastoma: identification of prognostic factors and resection threshold. Neurosurgery (2021) 88(4):E323–9. doi: 10.1093/neuros/nyaa562
30. Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol (2021) 18(3):170–86. doi: 10.1038/s41571-020-00447-z
31. Weiler M, Hartmann C, Wiewrodt D, Herrlinger U, Gorlia T, Bahr O, et al. Chemoradiotherapy of newly diagnosed glioblastoma with intensified temozolomide. Int J Radiat Oncol Biol Phys (2010) 77(3):670–6. doi: 10.1016/j.ijrobp.2009.05.031
32. Nabors LB, Fink KL, Mikkelsen T, Grujicic D, Tarnawski R, Nam DH, et al. Two cilengitide regimens in combination with standard treatment for patients with newly diagnosed glioblastoma and unmethylated MGMT gene promoter: results of the open-label, controlled, randomized phase II CORE study. Neuro Oncol (2015) 17(5):708–17. doi: 10.1093/neuonc/nou356
33. Raizer JJ, Giglio P, Hu J, Groves M, Merrell R, Conrad C, et al. A phase II study of bevacizumab and erlotinib after radiation and temozolomide in MGMT unmethylated GBM patients. J Neurooncol (2016) 126(1):185–92. doi: 10.1007/s11060-015-1958-z
34. Asano K, Fumoto T, Matsuzaka M, Hasegawa S, Suzuki N, Akasaka K, et al. Combination chemoradiotherapy with temozolomide, vincristine, and interferon-beta might improve outcomes regardless of O6-methyl-guanine-DNA-methyltransferase (MGMT) promoter methylation status in newly glioblastoma. BMC Cancer (2021) 21(1):867. doi: 10.1186/s12885-021-08592-z
35. Wick W, Gorlia T, Bady P, Platten M, van den Bent MJ, Taphoorn MJ, et al. Phase II Study of Radiotherapy and Temsirolimus versus Radiochemotherapy with Temozolomide in Patients with Newly Diagnosed Glioblastoma without MGMT Promoter Hypermethylation (EORTC 26082). Clin Cancer Res (2016) 22(19):4797–806. doi: 10.1158/1078-0432.CCR-15-3153
36. Wick W, Steinbach JP, Platten M, Hartmann C, Wenz F, von Deimling A, et al. Enzastaurin before and concomitant with radiation therapy, followed by enzastaurin maintenance therapy, in patients with newly diagnosed glioblastoma without MGMT promoter hypermethylation. Neuro Oncol (2013) 15(10):1405–12. doi: 10.1093/neuonc/not100
37. Herrlinger U, Schafer N, Steinbach JP, Weyerbrock A, Hau P, Goldbrunner R, et al. Bevacizumab plus irinotecan versus temozolomide in newly diagnosed O6-methylguanine-DNA methyltransferase nonmethylated glioblastoma: the randomized GLARIUS trial. J Clin Oncol (2016) 34(14):1611–9. doi: 10.1200/JCO.2015.63.4691
38. Alnahhas I, Alsawas M, Rayi A, Palmer JD, Raval R, Ong S, et al. Characterizing benefit from temozolomide in MGMT promoter unmethylated and methylated glioblastoma: a systematic review and meta-analysis. Neurooncol Adv (2020) 2(1):vdaa082. doi: 10.1093/noajnl/vdaa082
39. Valko PO, Siddique A, Linsenmeier C, Zaugg K, Held U, Hofer S. Prevalence and predictors of fatigue in glioblastoma: a prospective study. Neuro Oncol (2015) 17(2):274–81. doi: 10.1093/neuonc/nou127
40. Beaulieu JM, Gainetdinov RR. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacol Rev (2011) 63(1):182–217. doi: 10.1124/pr.110.002642
41. Magnon C, Hondermarck H. The neural addiction of cancer. Nat Rev Cancer (2023) 23:317–34. doi: 10.1038/s41568-023-00556-8
42. Chang A, Botteri E, Gillis RD, Lofling L, Le CP, Ziegler AI, et al. Beta-blockade enhances anthracycline control of metastasis in triple-negative breast cancer. Sci Transl Med (2023) 15(693):eadf1147. doi: 10.1126/scitranslmed.adf1147
Keywords: glioblastoma, drug repurposing, chlorpromazine, adjuvant treatment, MGMT
Citation: Pace A, Lombardi G, Villani V, Benincasa D, Abbruzzese C, Cestonaro I, Corrà M, Padovan M, Cerretti G, Caccese M, Silvani A, Gaviani P, Giannarelli D, Ciliberto G and Paggi MG (2023) Efficacy and safety of chlorpromazine as an adjuvant therapy for glioblastoma in patients with unmethylated MGMT gene promoter: RACTAC, a phase II multicenter trial. Front. Oncol. 13:1320710. doi: 10.3389/fonc.2023.1320710
Received: 12 October 2023; Accepted: 20 November 2023;
Published: 14 December 2023.
Edited by:
Cesare Zoia, San Matteo Hospital Foundation (IRCCS), ItalyReviewed by:
Alessia Pellerino, University Hospital of the City of Health and Science of Turin, ItalySoma Sengupta, University of North Carolina at Chapel Hill, United States
Alberto Campione, University of Insubria, Italy
Copyright © 2023 Pace, Lombardi, Villani, Benincasa, Abbruzzese, Cestonaro, Corrà, Padovan, Cerretti, Caccese, Silvani, Gaviani, Giannarelli, Ciliberto and Paggi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco G. Paggi, bWFyY28ucGFnZ2lAaWZvLml0