 Nicolas Roussot1,2,3,4*
Nicolas Roussot1,2,3,4* Julie Vincent1Remi Palmier1Guillaume Constantin5Leila Bengrine1
Julie Vincent1Remi Palmier1Guillaume Constantin5Leila Bengrine1 Jean-David Fumet1,2,3,4
Jean-David Fumet1,2,3,4 François Ghiringhelli1,2,3,4,6
François Ghiringhelli1,2,3,4,6- 1Department of Medical Oncology, Centre Georges-François Leclerc, Dijon, France
- 2Health Sciences Department, University of Burgundy, Dijon, France
- 3Cancer Biology Transfer Platform, Centre Georges-François Leclerc, Dijon, France
- 4Equipe TIRECs, Labellisée Ligue Contre le Cancer, Centre de Recherche INSERM LNC-UMR1231, Dijon, France
- 5Department of Biostatistics, Centre Georges-François Leclerc, Dijon, France
- 6Genetic and Immunology Medical Institute, Dijon, France
Background: Advanced biliary tract cancer (BTC) has a poor prognosis. Gemcitabine with platinum chemotherapy was the standard first-line chemotherapeutic regimen until the recent addition of anti-PD-1/PD-L1 antibodies. After disease progression, the only second-line chemotherapy that has demonstrated a survival benefit versus supportive care is FOLFOX (folinic acid, fluorouracil, and oxaliplatin), with a modest benefit. This study aimed to assess the efficacy and safety of second-line FOLFIRI (folinic acid, fluorouracil, and irinotecan) combined with bevacizumab for advanced BTC.
Methods: This single-center retrospective study enrolled patients with metastatic BTC (intrahepatic cholangiocarcinoma [ICC], extrahepatic cholangiocarcinoma [ECC], or gallbladder carcinoma) that progressed after first-line gemcitabine-based chemotherapy. FOLFIRI-bevacizumab was administered intravenously every 2 weeks [folinic acid 200 mg/m², fluorouracil 400 mg/m² (bolus), fluorouracil 2400 mg/m² (46-h continuous intravenous infusion), irinotecan 180 mg/m², and bevacizumab 5 mg/kg] until unacceptable toxicity, patient refusal, or disease progression.
Results: Overall, 28 patients received the FOLFIRI-bevacizumab regimen after gemcitabine-based chemotherapy. The median overall survival (OS) was 9.0 months (95% CI 6.4–16.5). The OS rate was 39.3% (95% CI 24.8–62.3) and 10.7% (95% CI 3.7–32.1) at 12- and 24-months respectively. The median progression-free survival (PFS) was 5.2 months (95% CI 3.1–10.2) with FOLFIRI-bevacizumab. The PFS rates at 12 months and 24 months were 17.9% (95% CI 8.19–39.5] and 10.7% (95% CI 3.7–31.2), respectively. The overall response rate (ORR) to FOLFIRI-bevacizumab was 23.1%, with a disease control rate (DCR) of 69.3%. Grade 3-4 adverse events (sAE) were reported in 20 patients (71.4%) treated with FOLFIRI-bevacizumab.
Conclusion: FOLFIRI-bevacizumab as a second-line treatment for advanced BTC after gemcitabine-based chemotherapy showed efficacy and safety with a promising tumor response rate in this retrospective single-center study.
1 Introduction
Biliary tract cancer (BTC), which encompasses intrahepatic cholangiocarcinoma (ICC), extrahepatic cholangiocarcinoma (ECC), and gallbladder cancer, has been known to have a poor prognosis (1), with an increase in incidence in high-income countries. To date, surgery is the only curative therapy available for patients with resectable tumors. Liver resection for intrahepatic BTC provides a 5-year overall survival (OS) rate of 25–40% with a median OS of 40 months (2). Notably, most patients are diagnosed with unresectable locally advanced or metastatic BTC and are therefore no longer candidates for this therapeutic option (3). Thus, most patients receive systemic palliative care. Until recently, the first-line standard therapy for metastatic disease was based on a combination of platinum and gemcitabine (4), with cisplatin (5) or oxaliplatin (6–8). In randomized phase III studies, the combination of gemcitabine with cisplatin provided a median OS of 11.7 months (9), numerically better results than oxaliplatin with only 9.5 months of median OS (10). Immunotherapy adjunction with chemotherapy using anti-PD-L1 durvalumab prolongs the survival, with a median OS exceeding 1 year, irrespective of PD-L1 expression (11). Similar results were obtained with pembrolizumab (12). These chemoimmunotherapy protocols are now considered the standard first-line treatment for advanced BTC (13). After disease progression, the ABC-06 trial is the only randomized phase III study that has demonstrated an improvement in OS with FOLFOX versus supportive care (14). Nonetheless, the efficacy of FOLFOX in the second-line setting of metastatic BTC remains modest, with a median progression-free survival (PFS) and median OS of 4.0 and 6.2 months, respectively, and a poor objective response rate of 5%. Because the evidence for irinotecan-based therapies is currently limited, we report the efficacy and safety of the FOLFIRI-bevacizumab combination as a second-line treatment for advanced BTC after gemcitabine-based chemotherapy.
2 Materials and methods
2.1 Patients
This single-center retrospective study was conducted at the Georges-François Leclerc Center in Dijon, France and included patients with advanced BTC treated between 2009 and 2022. The patients were required to have a histologically confirmed diagnosis of BTC with metastatic or unresectable disease that progressed after first-line gemcitabine-based chemotherapy. Progression was confirmed using thoracic, abdominal, and pelvic computed-tomography (CT) scans. Only patients who received FOLFIRI-bevacizumab as a second-line treatment in a metastatic setting were included in the analyses. The off-label use of this treatment regimen was validated by a local multidisciplinary staff member.
2.2 Treatment regimen
Physical examination, complete blood cell count, and serum chemistry were performed before the initiation of chemotherapy. The FOLFIRI-bevacizumab regimen consisted of bevacizumab injection (5 mg/kg over 90 min) followed by irinotecan (180 mg/m² i.v. over 90 min) concurrently with folinic acid (200 mg/m² i.v. over 120 min), followed by fluorouracil (400 mg/m² i.v. bolus) and fluorouracil (2400 mg/m² IV infusion over 46 h). This treatment was administered every two weeks. Adverse events were graded according to the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE 5.0). Dose reduction or treatment suspension was based on the grade of adverse events. The treatment was continued until unacceptable toxicity, patient refusal, or disease progression was observed.
2.3 Follow-up
Before every FOLFIRI-bevacizumab cycle, a complete physical examination, complete blood cell counts, and serum chemistry were performed. The tumor response was assessed every four cycles or when clinical progression was suspected according to symptoms and clinical examination with thoracic, abdominal, and pelvic CT-scans and determined using RECIST version 1.1. If a CT-scan does not provide a proper assessment of the tumor response, magnetic resonance imaging (MRI) can be performed.
2.4 Statistical analyses
Progression-free survival (PFS) at the second-line was calculated from the date of FOLFIRI-bevacizumab initiation to the date of progression or death. The overall survival (OS) at second-line treatment was calculated from the date of FOLFIRI-bevacizumab initiation to the date of death from any cause or censored at the date of the last follow-up. PFS at first-line treatment was calculated from the date of diagnosis of advanced biliary tract cancer to the date of progression or death, and OS at first-line treatment was calculated from the date of diagnosis to the date of death from any cause or censored at the date of last follow-up. The curves were plotted using a Kaplan–Meier analysis.
3 Results
3.1 Patient characteristics
Overall, 28 patients received FOLFIRI-bevacizumab as a second-line treatment for advanced BTC. A combination of gemcitabine and oxaliplatin (n=20, 71.4%) was the most frequently used first-line regimen (Table 1). The median age was 69.0 years and the majority of patients were male (n=16; 57.1%). Most patients had intrahepatic disease (n=19; 67.9%), with a similar proportion of extrahepatic disease (n=4; 14.3%) and gallbladder disease (n=5; 17.9%). Among the enrolled patients, 16 (57.1%) patients were diagnosed with metastatic disease, 8 (28.6%) patients with unresectable locally advanced disease, and 4 (14.3%) patients with resectable BTC. One patient underwent gallbladder removal for cholecystitis, which turned out to be an adenocarcinoma with peritoneal carcinomatosis. The mean baseline CA19-9 level was 1387.3 kU/L. Notably, 16 (57.1%) patients underwent molecular testing for advanced BTC. The genomic characteristics of these patients are shown in Figure 1.
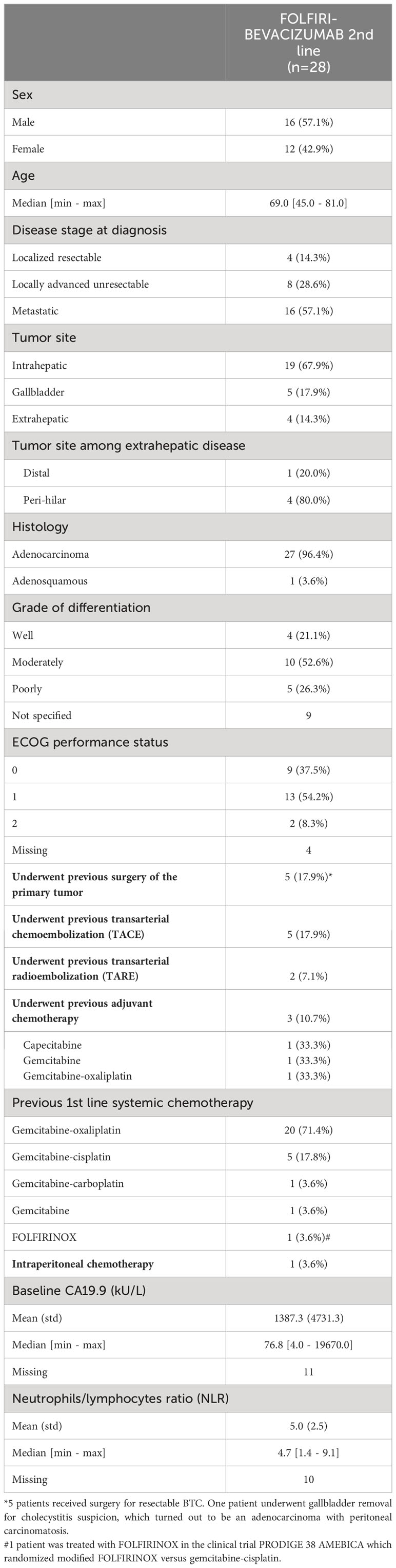
Table 1 Baseline characteristics.
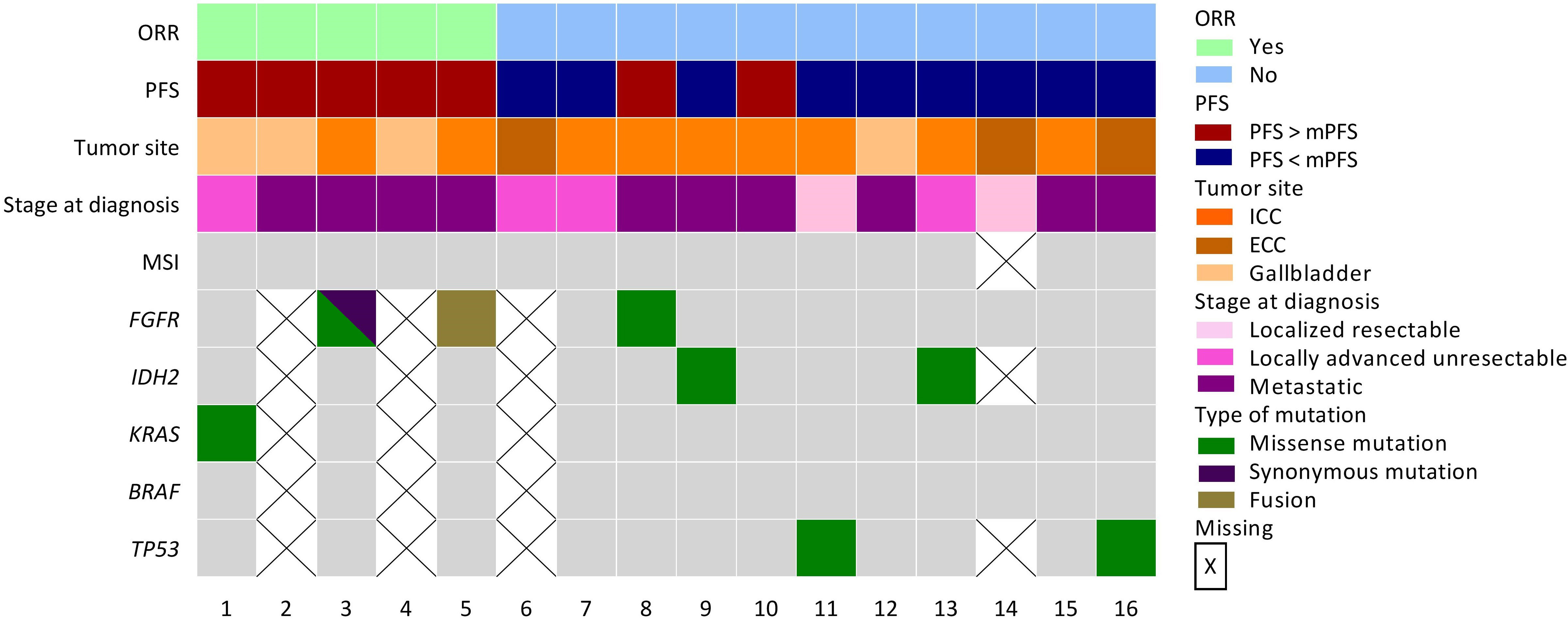
Figure 1 Genomic characterization of patients. Oncoplot representing genomic landscape among patients that have received molecular testing (n=16; 57.1%). * Patient 3 was diagnosed with a FGFR1 missense mutation (c.2223C>A; p.Phe741Leu) and with a FGFR3 synonymous mutation (c.933G>A; p.Thr311Thr).
3.2 Efficacy of the first-line treatment
In the first-line setting of metastatic disease, 26 (92.8%) patients were treated with a combination of gemcitabine and a platinum derivative (oxaliplatin for 20 (71.4%) patients, cisplatin for five (17.8%) patients, and carboplatin (3.6%) for one patient) (Table 1). The median OS from the first line of systemic chemotherapy was 16.5 months (95% CI 12.3–25.7). The OS rate was 67.9% (95% CI 52.6–87.6) at 12-months and 32.1% (95% CI 18.8–55.1) at 24-months (Supplemental Figure 1A). The median PFS was 7.6 months (95% CI 3.4–9.5). The PFS rates at 12 months and 24 months were 25.0% (95% CI 13.2–47.5) and 10.7% (95% CI 3.7–31.2), respectively (Supplemental Figure 1B). Among the 27 (96.4%) patients assessable for tumor response, the ORR was 42.9%, and the disease control rate (DCR) was 67.9% (Supplemental Table 1). The median OS tended to be longer for gallbladder cancer with 28.6 months (95% CI 21.7-not evaluable [NE]) than for ICC with 16.4 months (95% CI 10.3–36.9) and ECC with 12.9 months (95% CI 12.3–NE) (log-rank p-value = 0.1944, Supplemental Figure 2A). The median PFS for ICC, ECC, and gallbladder cancer were 5.6 (95% CI 2.5–14.3), 8.6 (95% CI 5.0–NE), and 10.1 months (95% CI 2.6–NE) (log-rank p-value = 0.7766, Supplemental Figure 2B), respectively. Patients who received local treatment for BTC, that is, previous surgery of the primary tumor, transarterial chemoembolization (TACE), or transarterial radioembolization (TARE), tended to have a longer OS than those who did not, although the PFS was similar (Supplemental Figures 3A, B).
3.3 Efficacy of FOLFIRI-bevacizumab in the second line setting
The median OS from the initiation of FOLFIRI-bevacizumab as a second-line treatment for metastatic disease was 9.0 months (95% CI 6.4–16.5). The OS rate was 39.3% (95% CI 24.8–62.3) at 12-months and 10.7% (95% CI 3.7–32.1) at 24-months (Figure 2A). The median PFS was 5.2 months (95% CI 3.1–10.2) with FOLFIRI-bevacizumab. The PFS rates at 12 months and 24 months were 17.9% (95% CI 8.1–39.5) and 10.7% (95% CI 3.7–31.2), respectively (Figure 2B). Of the 28 patients treated with FOLFIRI–bevacizumab, 26 (92.3%) patients were assessed for tumor response (Table 2). The ORR with FOLFIRI-bevacizumab was 21.4%, with six patients achieving a partial response. However, complete responses were not observed. A total of 42.9% (n=12) of the patients had stable disease with FOLFIRI-bevacizumab, which led to a DCR of 64.3%. The median OS was significantly different within distinct tumor sites (log-rank p = 0.0373, Figure 3A). Patients with metastatic gallbladder cancer had the longest median OS of 15.9 months (95% CI 10.5–NE). Patients with metastatic ICC had 10.2 months (95% CI 6.8–19.7) of median OS. Finally, metastatic ECC was the tumor site with the worst prognosis, with a median OS of 6.1 months (5.7–NE). The median PFS tended to be longer for gallbladder cancer than for ICC and ECC, at 11.8 (95% CI 3.0–NE), 4.9 (95% CI 2.9–10.6) and 4.6 months (95% CI 3.1–NE) (log-rank p-value = 0.0956, Figure 3B). Patients that have received local treatment for BTC tended to have a longer OS than those who did not, with 11.7 (6.1–NE) and 7.8 months (6.4–7.15), respectively (logrank p-value = 0.1402, Figure 4A). A similar trend was observed for PFS (log-rank test, p-value = 0.1061; Figure 4B). Two patients diagnosed with TP53 missense mutations had a particularly short PFS of 1.68 and 4.93 months.
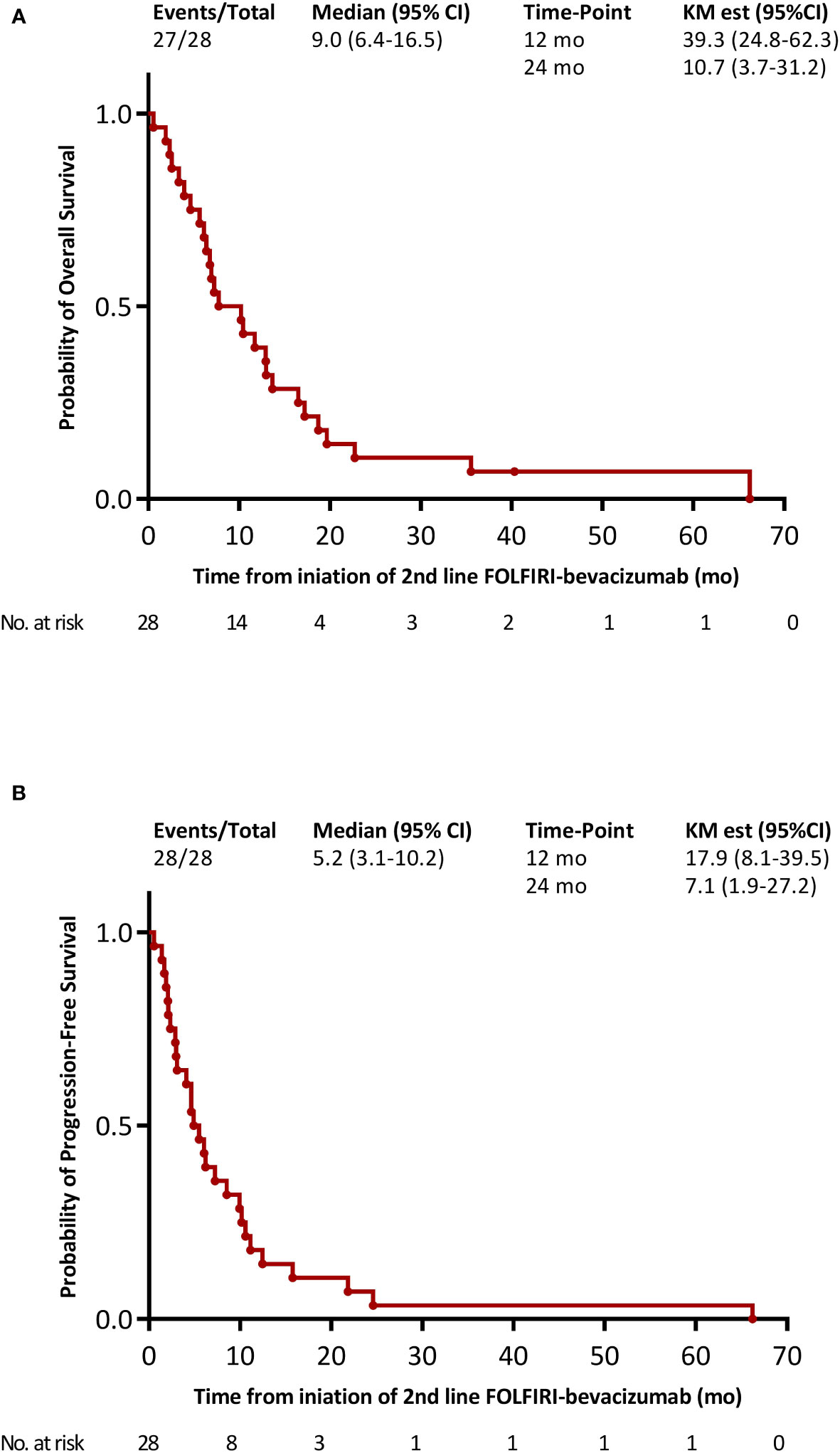
Figure 2 Kaplan-Meier survival curves with FOLFIRI-bevacizumab as the 2nd line treatment for metastatic disease. (A) overall survival; (B) progression-free survival.
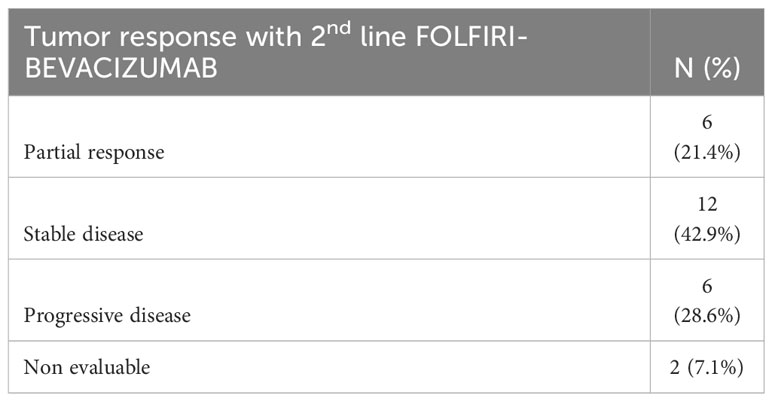
Table 2 Overall response rate with FOLFIRI-bevacizumab as the 2nd line treatment for metastatic disease.
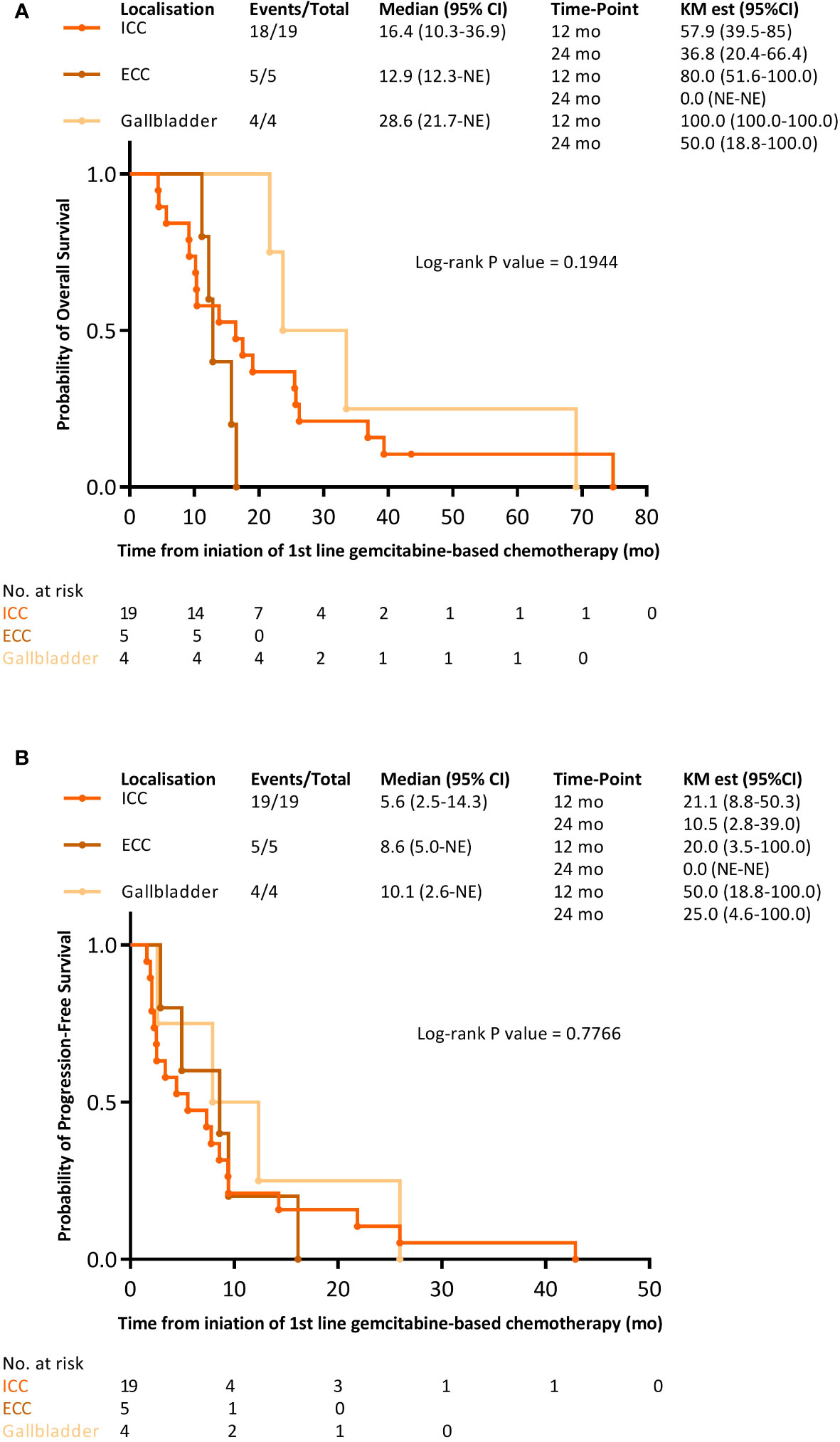
Figure 3 Kaplan-Meier survival curves with FOLFIRI-bevacizumab as the 2nd line treatment for metastatic disease within distinct tumor sites. (A) overall survival; (B) progression-free survival.
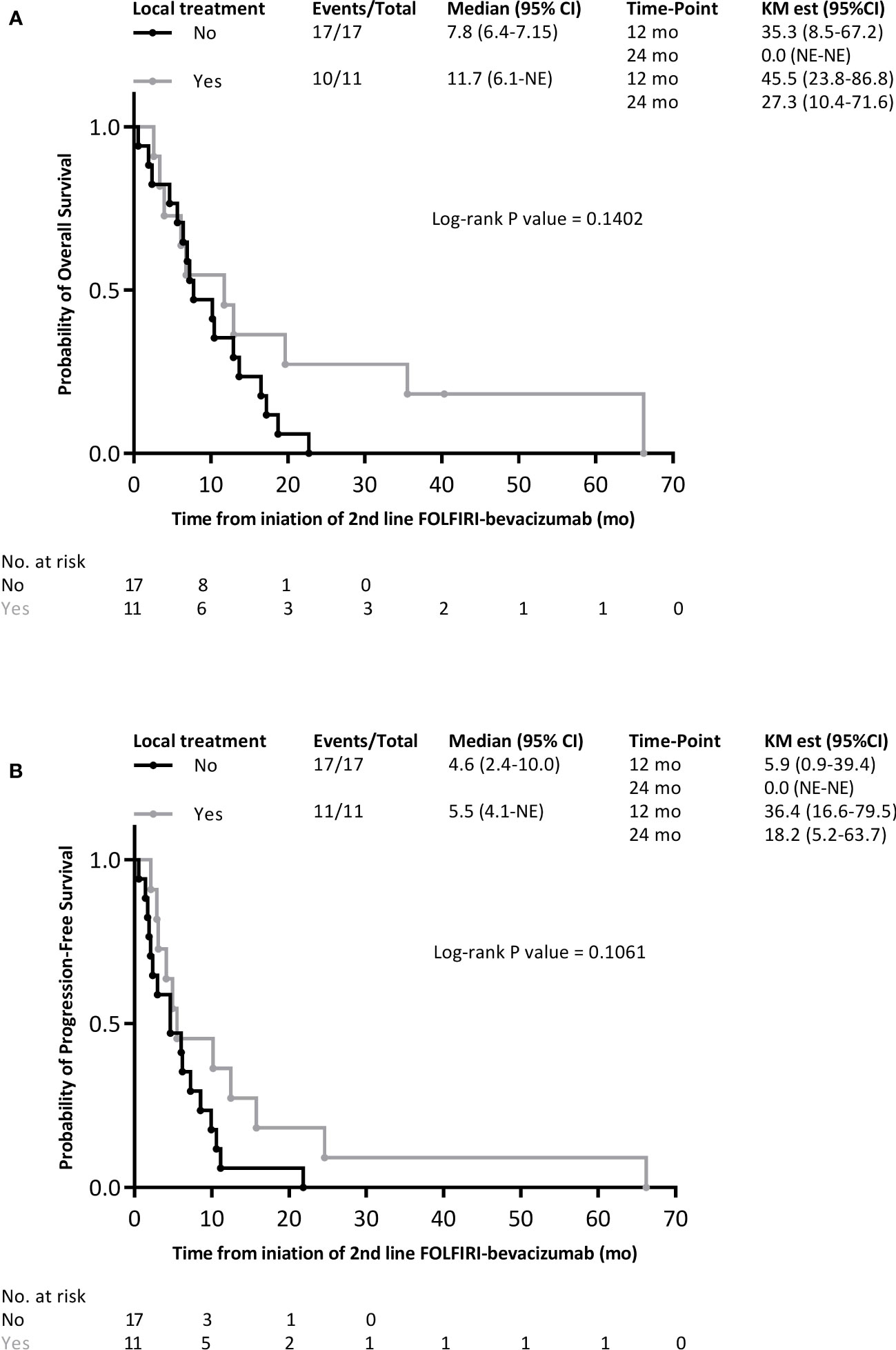
Figure 4 Kaplan-Meier survival curves with FOLFIRI-bevacizumab as the 2nd line treatment for metastatic disease within local treatment subgroups/. (A) overall survival; (B) progression-free survival.
3.4 Safety
Anemia (n=19, 67.9%), nausea (n=14, 50%), bleeding (n=14, 50%), and diarrhea (n=14, 50%) were the most frequent mild AEs. Grade 3 or higher adverse events (sAEs) occurred in 20 (71.4%) patients who received FOLFIRI-bevacizumab as the second-line treatment for metastatic disease. The most frequent hematological and non-hematological severe AEs were neutropenia (n=8, 28.6%) and infection (n=13, 46.4%), respectively. Only 2 (7.1%) grade ≥ 3 bleedings occurred. One patient had a gastric/duodenal hemorrhage related to gastric and duodenal ulcers that required transfusion. The other case involved grade 4 digestive bleeding related to esophageal varices that required transfusion and endoscopic ligature. Notably, 4 (14.3%) grade ≥ 3 hypertension occurred with FOLFIRI-bevacizumab but no grade ≥ 3 proteinuria. No grade 5 adverse events were reported. Table 3 summarizes the frequencies of AEs.
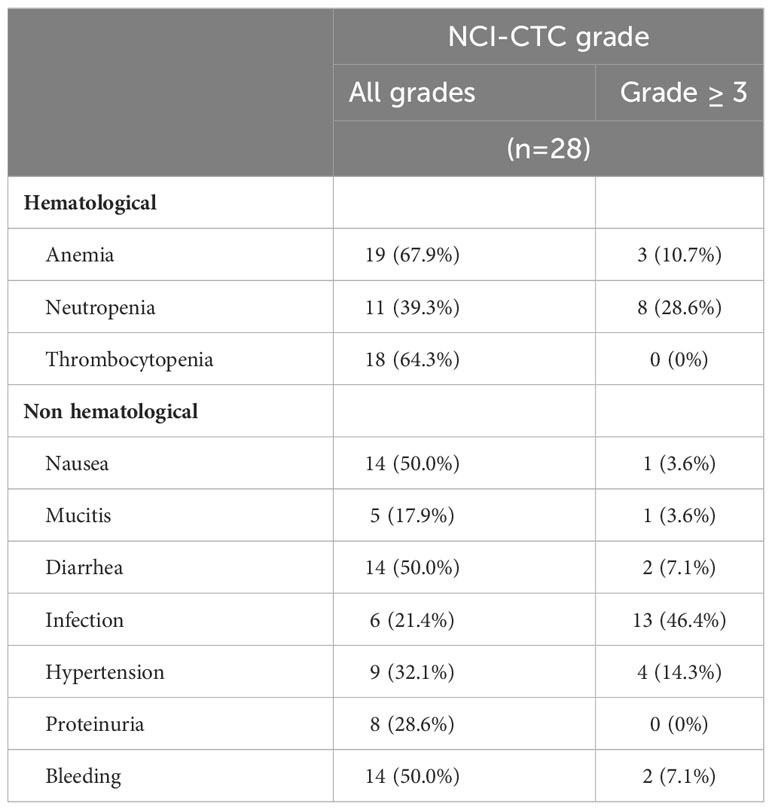
Table 3 Safety with FOLFIRI-bevacizumab.
4 Discussion
The results of this single-center retrospective study suggest that the combination of FOLFIRI with bevacizumab is an active and safe second-line regimen in patients with advanced BTC who show disease progression with gemcitabine-based chemotherapy.
In this study, the majority of patients received a combination of gemcitabine and oxaliplatin as the first-line systemic treatment for metastatic disease. The first-line standard of care for advanced BTC consists of a gemcitabine-based combination therapy (15), with cisplatin being the preferred option (5). Oxaliplatin remains an alternative to cisplatin when renal function is a concern (13). Nevertheless, the median PFS in the first-line setting observed in this cohort was slightly longer than that previously published in studies reporting the efficacy of the gemcitabine-oxaliplatin combination (10, 16, 17) and close to the 8.0 months reached with gemcitabine and cisplatin (9). Before immunotherapy adjunction demonstrated improvement in survival in the first-line setting in the TOPAZ- (11) and Keynote-966 (12) phase III studies, neither targeted therapy addition (10, 18) nor chemotherapy intensification with modified FOLFIRINOX (19) or the addition of albumin-bound paclitaxel succeeded in improving survival. In Asia, the addition of S-1 to gemcitabine and cisplatin in the first-line setting prolongs survival compared to the chemotherapy doublet (20). The IMBrave-151 (21) phase II trial assessed the combination of atezolizumab, bevacizumab, gemcitabine, and cisplatin and showed promising preliminary results; however, it lacked an appropriate control group with gemcitabine and cisplatin.
From a molecular perspective, BTC is a heterogeneous disease with distinct genomic and epigenomic landscapes (22, 23). Based on this molecular dismemberment, targeted therapies have been used to improve outcomes beyond first-line therapy. In the present study, more than half of the patients underwent molecular testing. Two of these patients were diagnosed with FGFR pathway alterations. As expected in patients with such features, the type of BTC was ICC (24). One patient was observed to have a FGFR1 missense mutation (c.2223C>A; p.Phe741Leu) along with a synonymous FGFR3 mutation (c.933G>A; p.Thr311Thr), while the second patient was diagnosed with a FGFR2 fusion (FGFR2-C5orf15) that would have rendered him a candidate for targeted therapies since pemigatinib (25), infigratinib (26), or futibatinib (27, 28) are validated options for patients with FGFR2 fusions (13). One patient harbored a IDH2 mutation; however, ivosidenib (29, 30) has only been proposed for patients with IDH1 mutations. Patients harboring BRAF mutations are candidates for dabrafenib with trametinib (31). The amplification of HER2/neu is targeted by trastuzumab, which is either associated with pertuzumab (32) or FOLFOX (33). Pembrolizumab is the preferred option for patients with mismatch repair deficiency (dMMR) or microsatellite instability (MSI-H) (34). Recently, adagrasib showed a promising efficacy in advanced BTC harboring a KRASG12C mutation, with an ORR of 41.7% (35). Globally, molecular screening techniques enable treatment with molecular targeted agents, which prolong survival in patients with advanced BTC (36).
The choice of second-line chemotherapy for patients without targetable genomic alterations was based on retrospective and non-randomized studies (37–39) until the ABC-06 trial established FOLFOX as the standard of care (13). After progression to first-line gemcitabine-based chemotherapy, nearly half of the patients are offered second-line chemotherapy. In a retrospective German study, nearly one-third of patients received FOLFOX/CAPOX (capecitabine-oxaliplatin) and less than a tenth was offered FOLFIRI or FOLFIRINOX (40). Studies that assessed the FOLFIRI regimen in this setting are summarized in Table 4. FOLFIRI-bevacizumab in this study allows reaching a median PFS and OS of 5.2 and 9.0 months, respectively, with a promising ORR of 21.4% and a DCR of 64.3%. Our study seems to be numerically comparable favorably with previous reports on therapy consisting of FOLFIRI alone. In the second-line setting, the ABC-06 (14) study was the only randomized phase III trial that demonstrated the survival benefit of FOLFOX over supportive care. Despite its modest efficacy, with a median PFS of 4.0 months, median OS of 6.2 months, and poor ORR of 5%, this regimen is the standard of care after gemcitabine-based chemotherapy for patients without actionable mutations (13). Irinotecan-based therapies using nanoliposomal irinotecan (Nal-iri) were assessed. NIFTY (50), a Korean phase IIb study, and NALIRICC (51), a German phase II study, are two clinical trials that compared Nal-iri with 5-FU to 5-FU alone after gemcitabine-based therapies. While the first met its primary endpoint with an improvement of the median PFS with the Nal-iri – 5-FU combination over 5-FU alone (7.1 months vs. 1.4 months; hazard ratio 0.56, 95% CI 0.39–0.81; p=0.0019), the second did not since the two regimens reached a median PFS of 2.76 and 2.3 months, respectively. These contradictory results highlight that biliary tract cancer presents with different biological features in Western and Asian countries, which may affect the response to therapy (52, 53). However, the ORR were similar for NIFTY and NALIRICC (14.8% and 14.3%, respectively). Table 5 summarizes prospective randomized studies on second-line therapies for advanced BTC.
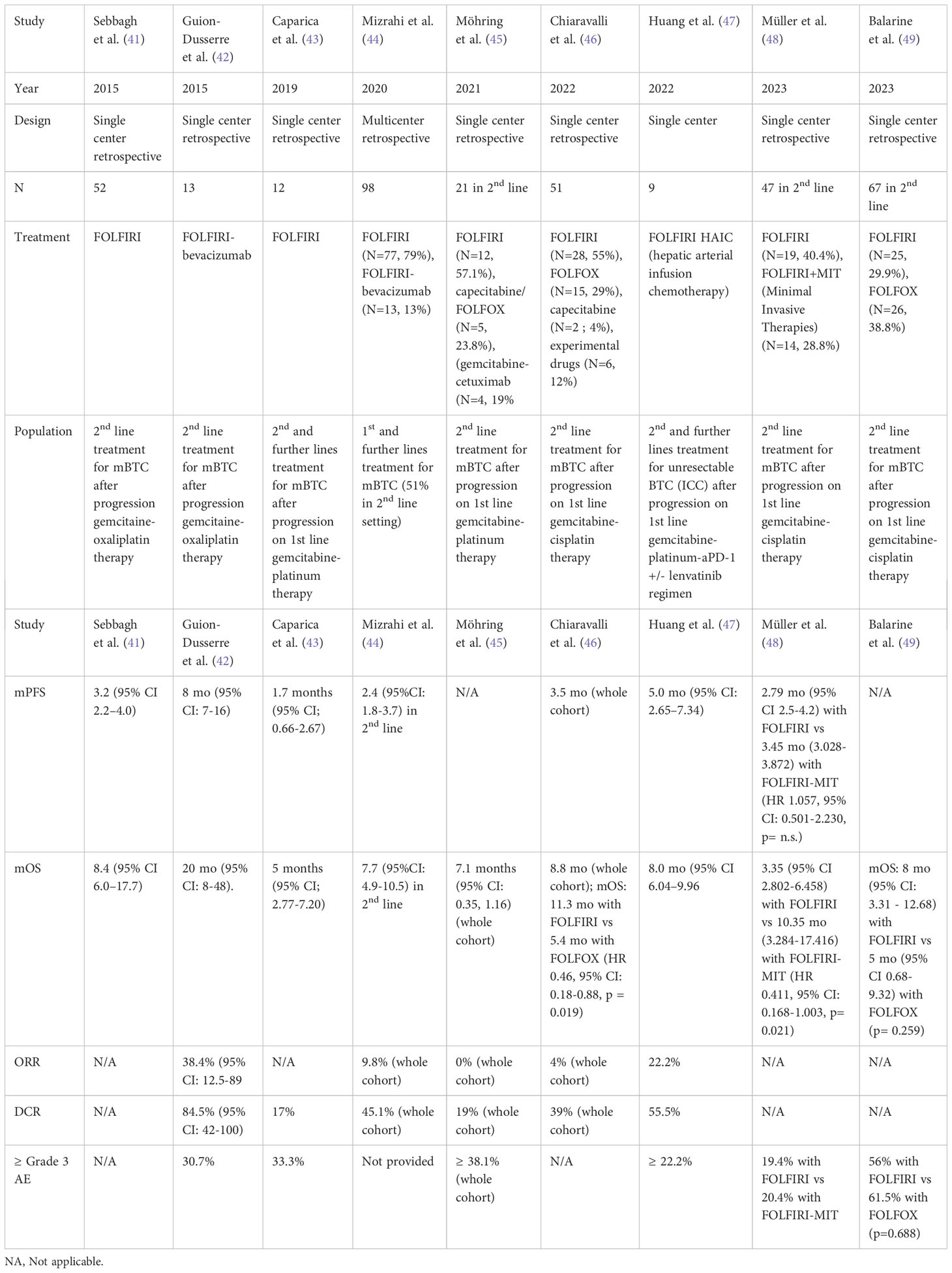
Table 4 non randomized studies that have assessed FOLFIRI in the second-line setting of advanced BTC.
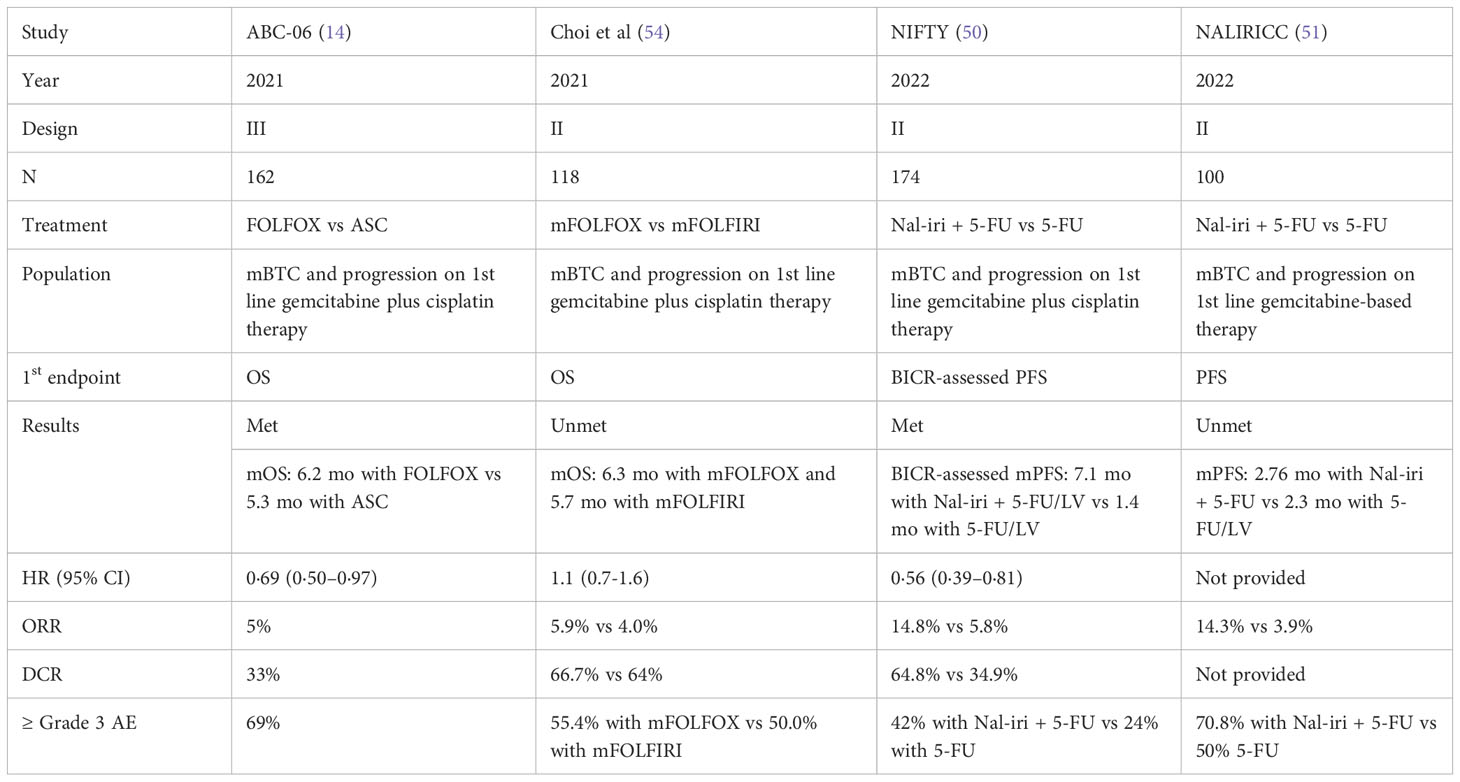
Table 5 Prospective randomized studies for second-line treatment of advanced BTC.
In conclusion, our study on the FOLFIRI-bevacizumab regimen after progression to first-line gemcitabine-based therapy showed promising activity with a safety profile. The survival outcomes with this combination were similar to those achieved with FOLFOX, FOLFIRI, and Nal-IRI + 5FU. However, the adjunction of an anti-angiogenic agent with bevacizumab may provide a higher response rate. Hence, this regimen could benefit symptomatic patients with a massive tumor burden for whom obtaining a rapid response is crucial.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by loi Informatique et libertés de 1978 modifiée et le Règlement (UE) n°2016/679 relatif à la protection des données personnelles (RGPD). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NR: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. JV: Investigation, Writing – review & editing. RP: Investigation, Writing – review & editing. GC: Writing – review & editing, Formal Analysis, Software. LB: Investigation, Writing – review & editing. JF: Investigation, Writing – review & editing. FG: Conceptualization, Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1293670/full#supplementary-material
References
1. Valle JW, Kelley RK, Nervi B, Oh D-Y, Zhu AX. Biliary tract cancer. Lancet (2021) 397:428–44. doi: 10.1016/S0140-6736(21)00153-7
2. Mazzaferro V, Gorgen A, Roayaie S, Droz Dit Busset M, Sapisochin G. Liver resection and transplantation for intrahepatic cholangiocarcinoma. J Hepatol (2020) 72:364–77. doi: 10.1016/j.jhep.2019.11.020
3. Hezel AF, Deshpande V, Zhu AX. Genetics of biliary tract cancers and emerging targeted therapies. JCO (2010) 28:3531–40. doi: 10.1200/JCO.2009.27.4787
4. Eckel F, Schmid RM. Chemotherapy in advanced biliary tract carcinoma: a pooled analysis of clinical trials. Br J Cancer (2007) 96:896–902. doi: 10.1038/sj.bjc.6603648
5. Okusaka T, Nakachi K, Fukutomi A, Mizuno N, Ohkawa S, Funakoshi A, et al. Gemcitabine alone or in combination with cisplatin in patients with biliary tract cancer: a comparative multicentre study in Japan. Br J Cancer (2010) 103:469–74. doi: 10.1038/sj.bjc.6605779
6. André T, Tournigand C, Rosmorduc O, Provent S, Maindrault-Goebel F, Avenin D, et al. Gemcitabine combined with oxaliplatin (GEMOX) in advanced biliary tract adenocarcinoma: a GERCOR study. Ann Oncol (2004) 15:1339–43. doi: 10.1093/annonc/mdh351
7. Harder J, Riecken B, Kummer O, Lohrmann C, Otto F, Usadel H, et al. Outpatient chemotherapy with gemcitabine and oxaliplatin in patients with biliary tract cancer. Br J Cancer (2006) 95:848–52. doi: 10.1038/sj.bjc.6603334
8. Jang J-S, Lim HY, Hwang IG, Song HS, Yoo N, Yoon S, et al. Gemcitabine and oxaliplatin in patients with unresectable biliary cancer including gall bladder cancer: a Korean Cancer Study Group phase II trial. Cancer Chemother Pharmacol (2010) 65:641–7. doi: 10.1007/s00280-009-1069-7
9. Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A, et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N Engl J Med (2010) 362:1273–81. doi: 10.1056/NEJMoa0908721
10. Lee J, Park SH, Chang H-M, Kim JS, Choi HJ, Lee MA, et al. Gemcitabine and oxaliplatin with or without erlotinib in advanced biliary-tract cancer: a multicentre, open-label, randomised, phase 3 study. Lancet Oncol (2012) 13:181–8. doi: 10.1016/S1470-2045(11)70301-1
11. Oh D-Y, Ruth He A, Qin S, Chen L-T, Okusaka T, Vogel A, et al. Durvalumab plus gemcitabine and cisplatin in advanced biliary tract cancer. NEJM Evidence (2022) 1. doi: 10.1056/EVIDoa2200015
12. Kelley RK, Ueno M, Yoo C, Finn RS, Furuse J, Ren Z, et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet (2023) 401:1853–65. doi: 10.1016/S0140-6736(23)00727-4
13. Vogel A, Bridgewater J, Edeline J, Kelley RK, Klümpen HJ, Malka D, et al. Biliary tract cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol (2023) 34:127–40. doi: 10.1016/j.annonc.2022.10.506
14. Lamarca A, Palmer DH, Wasan HS, Ross PJ, Ma YT, Arora A, et al. Second-line FOLFOX chemotherapy versus active symptom control for advanced biliary tract cancer (ABC-06): a phase 3, open-label, randomised, controlled trial. Lancet Oncol (2021) 22:690–701. doi: 10.1016/S1470-2045(21)00027-9
15. Valle JW, Borbath I, Khan SA, Huguet F, Gruenberger T, Arnold D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2016) 27:v28–37. doi: 10.1093/annonc/mdw324
16. André T, Reyes-Vidal JM, Fartoux L, Ross P, Leslie M, Rosmorduc O, et al. Gemcitabine and oxaliplatin in advanced biliary tract carcinoma: a phase II study. Br J Cancer (2008) 99:862–7. doi: 10.1038/sj.bjc.6604628
17. Sharma A, Kalyan Mohanti B, Pal Chaudhary S, Sreenivas V, Kumar Sahoo R, Kumar Shukla N, et al. Modified gemcitabine and oxaliplatin or gemcitabine + cisplatin in unresectable gallbladder cancer: Results of a phase III randomised controlled trial. Eur J Cancer (2019) 123:162–70. doi: 10.1016/j.ejca.2019.10.004
18. Valle JW, Vogel A, Denlinger CS, He AR, Bai L-Y, Orlova R, et al. Addition of ramucirumab or merestinib to standard first-line chemotherapy for locally advanced or metastatic biliary tract cancer: a randomised, double-blind, multicentre, phase 2 study. Lancet Oncol (2021) 22:1468–82. doi: 10.1016/S1470-2045(21)00409-5
19. Phelip JM, Desrame J, Edeline J, Barbier E, Terrebonne E, Michel P, et al. Modified FOLFIRINOX versus CISGEM chemotherapy for patients with advanced biliary tract cancer (PRODIGE 38 AMEBICA): A randomized phase II study. JCO (2022) 40:262–71. doi: 10.1200/JCO.21.00679
20. Ioka T, Kanai M, Kobayashi S, Sakai D, Eguchi H, Baba H, et al. Randomized phase III study of gemcitabine, cisplatin plus S-1 versus gemcitabine, cisplatin for advanced biliary tract cancer (KHBO1401 - MITSUBA). J Hepato Biliary Pancreat (2023) 30:102–10. doi: 10.1002/jhbp.1219
21. El-Khoueiry AB, Ren Z, Chon H, Park JO, Kim JW, Pressiani T, et al. IMbrave151: A phase 2, randomized, double-blind, placebo-controlled study of atezolizumab with or without bevacizumab in combination with cisplatin plus gemcitabine in patients with untreated, advanced biliary tract cancer. JCO (2023) 41:491–1. doi: 10.1200/JCO.2023.41.4_suppl.491
22. Nakamura H, Arai Y, Totoki Y, Shirota T, Elzawahry A, Kato M, et al. Genomic spectra of biliary tract cancer. Nat Genet (2015) 47:1003–10. doi: 10.1038/ng.3375
23. Jusakul A, Cutcutache I, Yong CH, Lim JQ, Huang MN, Padmanabhan N, et al. Whole-genome and epigenomic landscapes of etiologically distinct subtypes of cholangiocarcinoma. Cancer Discovery (2017) 7:1116–35. doi: 10.1158/2159-8290.CD-17-0368
24. Goyal L, Shi L, Liu LY, Fece de la Cruz F, Lennerz JK, Raghavan S, et al. TAS-120 overcomes resistance to ATP-competitive FGFR inhibitors in patients with FGFR2 fusion–positive intrahepatic cholangiocarcinoma. Cancer Discovery (2019) 9:1064–79. doi: 10.1158/2159-8290.CD-19-0182
25. Abou-Alfa GK, Sahai V, Hollebecque A, Vaccaro G, Melisi D, Al-Rajabi R, et al. Pemigatinib for previously treated, locally advanced or metastatic cholangiocarcinoma: a multicentre, open-label, phase 2 study. Lancet Oncol (2020) 21:671–84. doi: 10.1016/S1470-2045(20)30109-1
26. Javle M, Lowery M, Shroff RT, Weiss KH, Springfeld C, Borad MJ, et al. Phase II study of BGJ398 in patients with FGFR-altered advanced cholangiocarcinoma. JCO (2018) 36:276–82. doi: 10.1200/JCO.2017.75.5009
27. Meric-Bernstam F, Bahleda R, Hierro C, Sanson M, Bridgewater J, Arkenau H-T, et al. Futibatinib, an irreversible FGFR1–4 inhibitor, in patients with advanced solid tumors harboring FGF/FGFR aberrations: A phase I dose-expansion study. Cancer Discovery (2022) 12:402–15. doi: 10.1158/2159-8290.CD-21-0697
28. Goyal L, Meric-Bernstam F, Hollebecque A, Valle JW, Morizane C, Karasic TB, et al. Futibatinib for FGFR2 -rearranged intrahepatic cholangiocarcinoma. N Engl J Med (2023) 388:228–39. doi: 10.1056/NEJMoa2206834
29. Abou-Alfa GK, Macarulla T, Javle MM, Kelley RK, Lubner SJ, Adeva J, et al. Ivosidenib in IDH1-mutant, chemotherapy-refractory cholangiocarcinoma (ClarIDHy): a multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol (2020) 21:796–807. doi: 10.1016/S1470-2045(20)30157-1
30. Zhu AX, Macarulla T, Javle MM, Kelley RK, Lubner SJ, Adeva J, et al. Final overall survival efficacy results of ivosidenib for patients with advanced cholangiocarcinoma with IDH1 mutation: the phase 3 randomized clinical clarIDHy trial. JAMA Oncol (2021) 7:1669. doi: 10.1001/jamaoncol.2021.3836
31. Subbiah V, Lassen U, Élez E, Italiano A, Curigliano G, Javle M, et al. Dabrafenib plus trametinib in patients with BRAFV600E-mutated biliary tract cancer (ROAR): a phase 2, open-label, single-arm, multicentre basket trial. Lancet Oncol (2020) 21:1234–43. doi: 10.1016/S1470-2045(20)30321-1
32. Javle M, Borad MJ, Azad NS, Kurzrock R, Abou-Alfa GK, George B, et al. Pertuzumab and trastuzumab for HER2-positive, metastatic biliary tract cancer (MyPathway): a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol (2021) 22:1290–300. doi: 10.1016/S1470-2045(21)00336-3
33. Lee C, Chon HJ, Cheon J, Lee MA, Im H-S, Jang J-S, et al. Trastuzumab plus FOLFOX for HER2-positive biliary tract cancer refractory to gemcitabine and cisplatin: a multi-institutional phase 2 trial of the Korean Cancer Study Group (KCSG-HB19–14). Lancet Gastroenterol Hepatol (2023) 8:56–65. doi: 10.1016/S2468-1253(22)00335-1
34. Marabelle A, Le DT, Ascierto PA, Di Giacomo AM, De Jesus-Acosta A, Delord J-P, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair–deficient cancer: results from the phase II KEYNOTE-158 study. JCO (2020) 38:1–10. doi: 10.1200/JCO.19.02105
35. Bekaii-Saab TS, Yaeger R, Spira AI, Pelster MS, Sabari JK, Hafez N, et al. Adagrasib in advanced solid tumors harboring a KRAS G12C mutation. JCO (2023) 41:4097–106. doi: 10.1200/JCO.23.00434
36. Verlingue L, Malka D, Allorant A, Massard C, Ferté C, Lacroix L, et al. Precision medicine for patients with advanced biliary tract cancers: An effective strategy within the prospective MOSCATO-01 trial. Eur J Cancer (2017) 87:122–30. doi: 10.1016/j.ejca.2017.10.013
37. Fiteni F, Jary M, Monnien F, Nguyen T, Beohou E, Demarchi M, et al. Advanced biliary tract carcinomas: a retrospective multicenter analysis of first and second-line chemotherapy. BMC Gastroenterol (2014) 14:143. doi: 10.1186/1471-230X-14-143
38. on behalf of the GICO group (Gruppo Italiano COlangiocarcinoma), Fornaro L, Vivaldi C, Cereda S, Leone F, Aprile G, et al. Second-line chemotherapy in advanced biliary cancer progressed to first-line platinum-gemcitabine combination: a multicenter survey and pooled analysis with published data. J Exp Clin Cancer Res (2015) 34:156. doi: 10.1186/s13046-015-0267-x
39. Belkouz A, De Vos-Geelen J, Mathôt RAA, Eskens FALM, Van Gulik TM, Van Oijen MGH, et al. Efficacy and safety of FOLFIRINOX as salvage treatment in advanced biliary tract cancer: an open-label, single arm, phase 2 trial. Br J Cancer (2020) 122:634–9. doi: 10.1038/s41416-019-0698-9
40. Thol F, Gairing SJ, Czauderna C, Thomaidis T, Gamstätter T, Huber Y, et al. Outcomes in patients receiving palliative chemotherapy for advanced biliary tract cancer. JHEP Rep (2022) 4:100417. doi: 10.1016/j.jhepr.2021.100417
41. Sebbagh S, Roux J, Dreyer C, Neuzillet C, De Gramont A, Orbegoso C, et al. Efficacy of a sequential treatment strategy with GEMOX-based followed by FOLFIRI-based chemotherapy in advanced biliary tract cancers. Acta Oncol (2016) 55:1168–74. doi: 10.1080/0284186X.2016.1191670
42. Guion-Dusserre J-F, Lorgis V, Vincent J, Bengrine L, Ghiringhelli F. FOLFIRI plus bevacizumab as a second-line therapy for metastatic intrahepatic cholangiocarcinoma. WJG (2015) 21:2096–101. doi: 10.3748/wjg.v21.i7.2096
43. Caparica R, Lengelé A, Bekolo W, Hendlisz A. FOLFIRI as second-line treatment of metastatic biliary tract cancer patients. Autops Case Rep (2019) 9:e2019087. doi: 10.4322/acr.2019.087
44. Mizrahi JD, Gunchick V, Mody K, Xiao L, Surapaneni P, Shroff RT, et al. Multi-institutional retrospective analysis of FOLFIRI in patients with advanced biliary tract cancers. WJGO (2020) 12:83–91. doi: 10.4251/wjgo.v12.i1.83
45. Möhring C, Feder J, Mohr RU, Sadeghlar F, Bartels A, Mahn R, et al. First line and second line chemotherapy in advanced cholangiocarcinoma and impact of dose reduction of chemotherapy: A retrospective analysis. Front Oncol (2021) 11:717397. doi: 10.3389/fonc.2021.717397
46. Chiaravalli M, Bensi M, Bagalà C, Di Stefano B, Beccia V, Spring A, et al. The impact of second-line treatment after fist-line cisplatin plus gemcitabine in advanced biliary tract cancers: A mono-institutional retrospective study. JCO (2022) 40:e16180–0. doi: 10.1200/JCO.2022.40.16_suppl.e16180
47. Huang P, Huang X, Zhou Y, Yang G, Sun Q, Shi G, et al. The efficacy and safety of hepatic arterial infusion chemotherapy based on FOLFIRI for advanced intrahepatic cholangiocarcinoma as second-line and successive treatment: A real-world study. Can J Gastroenterol Hepatol (2022) 2022:1–7. doi: 10.1155/2022/9680933
48. Müller C, Omari J, Mohnike K, Bär C, Pech M, Keitel V, et al. Multidisciplinary treatment of patients with progressive biliary tract cancer after first-line gemcitabine and cisplatin: A single-center experience. Cancers (2023) 15:2598. doi: 10.3390/cancers15092598
49. Balarine M, Felismino T, Camandaroba M. P-52 FOLFIRI or FOLFOX in second line of advanced biliary tract cancer: A retrospective analysis. Ann Oncol (2022) 33:S265. doi: 10.1016/j.annonc.2022.04.142
50. Yoo C, Kim K, Jeong JH, Kim I, Kang MJ, Cheon J, et al. Liposomal irinotecan plus fluorouracil and leucovorin versus fluorouracil and leucovorin for metastatic biliary tract cancer after progression on gemcitabine plus cisplatin (NIFTY): a multicentre, open-label, randomised, phase 2b study. Lancet Oncol (2021) 22:1560–72. doi: 10.1016/S1470-2045(21)00486-1
51. Vogel A, Wenzel P, Folprecht G, Schütt P, Wege H, Kretzschmar A, et al. 53MO Nal-IRI and 5-FU/LV compared to 5-FU/LV in patients with cholangio- and gallbladder carcinoma previously treated with gemcitabine-based therapies (NALIRICC – AIO-HEP-0116). Ann Oncol (2022) 33:S563–4. doi: 10.1016/j.annonc.2022.07.081
52. Clements O, Eliahoo J, Kim JU, Taylor-Robinson SD, Khan SA. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: A systematic review and meta-analysis. J Hepatol (2020) 72:95–103. doi: 10.1016/j.jhep.2019.09.007
53. Sithithaworn P, Yongvanit P, Duenngai K, Kiatsopit N, Pairojkul C. Roles of liver fluke infection as risk factor for cholangiocarcinoma. J Hepatobiliary Pancreat Sci (2014) 21:301–8. doi: 10.1002/jhbp.62
54. Choi IS, Kim KH, Lee JH, Suh KJ, Kim J-W, Park JH, et al. A randomised phase II study of oxaliplatin/5-FU (mFOLFOX) versus irinotecan/5-FU (mFOLFIRI) chemotherapy in locally advanced or metastatic biliary tract cancer refractory to first-line gemcitabine/cisplatin chemotherapy. Eur J Cancer (2021) 154:288–95. doi: 10.1016/j.ejca.2021.06.019
Keywords: FOLFIRI, FOLFIRI plus bevacizumab, bevacizumab, chemotherapy, second-line, advanced biliary tract cancer, metastatic biliary tract cancer, biliary tract cancer
Citation: Roussot N, Vincent J, Palmier R, Constantin G, Bengrine L, Fumet J-D and Ghiringhelli F (2023) FOLFIRI-bevacizumab as a second-line treatment for advanced biliary tract cancer after gemcitabine-based chemotherapy. Front. Oncol. 13:1293670. doi: 10.3389/fonc.2023.1293670
Received: 13 September 2023; Accepted: 13 November 2023;
Published: 30 November 2023.
Edited by:
Yan-Shen Shan, National Cheng Kung University Hospital, TaiwanReviewed by:
Sakshi M., Emory University, United StatesLimei Zhu, University of Michigan, United States
Copyright © 2023 Roussot, Vincent, Palmier, Constantin, Bengrine, Fumet and Ghiringhelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolas Roussot, bnJvdXNzb3RAY2dmbC5mcg==