
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol. , 20 September 2023
Sec. Genitourinary Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1268309
This article is part of the Research Topic Expert Opinions in Genitourinary Oncology View all 6 articles
 Ambroise Champion1
Ambroise Champion1 Daniel Rudolf Zwhalen2
Daniel Rudolf Zwhalen2 Christoph Oehler2
Christoph Oehler2 Daniel Taussky1,3*
Daniel Taussky1,3* Stephanie G. C. Kroeze4Irene A. Burger5,6David Benzaquen1
Stephanie G. C. Kroeze4Irene A. Burger5,6David Benzaquen1There are few randomized trials to evaluate the use of PSMA-PET in the planning of post-prostatectomy radiotherapy. There are two unresolved questions 1) should we increase the dose to lesions visible on PSMA-PET 2) can we reduce dose in the case of a negative PSMA-PET. In this review, we summarize and discuss the available evidence in the literature. We found that in general, there seems to be an advantage for dose-increase, but ta large recent study from the pre-PSMA era didn’t show an advantage for dose escalation. Retrospective studies have shown that conventional doses to PSMA-PET-positive lesions seem sufficient. On the other hand, in the case of a negative PSMA-PET, there is no evidence that dose-reduction is possible. In the future, the combination of PSMA-PET with genomic classifiers could help in better identify patients who might benefit from either dose- de-or -increase. We further need to identify intraindividual references to help identify lesions with higher aggressiveness.
Prostate-specific membrane antigen (PSMA) positron emission tomography (PET) has led to a shift in the management of many different clinical situations in prostate cancer (1). It is foreseeable that as we gain more experience with PSMA-PET, with its better accuracy to detect recurrence, we will be able to improve the management of biochemical recurrence after prostatectomy (2, 3). The dilemma in the era of evidence-based medicine is that there are very few randomized trials to evaluate the use of PSMA in the planning of radiotherapy treatment (4). There are essentially two unresolved questions that we try to address in this review: 1) can lesions visible on PSMA-PET benefit from dose-escalation (5, 6). 2) can we reduce dose in the case of a negative PSMA-PET (7). In this review, we summarize and discuss the available evidence in the literature on whether PSMA-PET can help in postoperative radiotherapy by dose-tailoring, either by focal de-escalation or escalation of the applied radiation dose.
In primary, untreated prostate cancer, the randomized proPSMA trial has shown prospectively, that [68Ga]-PSMA-11 PET-CT is more accurate in staging prostate cancer than conventional imaging (Computed tomography (CT) and bone scan) (8). There is so far no randomized trial to show such an advantage in the postoperative setting, except for a large number of retrospective studies conducted on large numbers of patients. Thus, in a scoping review for patients with biochemical recurrence, Valle et al. (9), summarized 45 articles with over 240 patients imaged with [18F]-Fluciclovine and over 3000 patients imaged with [68Ga]-PSMA-11 and showed that PSMA-PET imaging resulted in a higher detection rate of local recurrences or metastases than conventional imaging or other PET tracers at low PSA values. Depending on the tracer used in PSMA-PET, changes in treatment management occurred in 40–77% of patients (9). Whether or not one finds such lesions on PSMA-PET depends heavily on the PSA at the time of imaging. In a large multicenter study of more than 2000 patients published in 2022 (10), the detection rate was 44% (44/105) when PSA levels were < 0.25 ng/mL. In conclusion, PSMA-PET has been shown to improve the detection rate of recurrence after prostatectomy compared to conventional imageing but how to implement the findings into daily practice has not been established yet.
Retrospective studies found an advantage for dose-escalation. Two early retrospective studies as well as later studies, including a more recent one, found that higher doses of salvage RT might reduce progression rates (11, 12). They showed that an EQD2 of 68 Gy or 70.2 Gy in 1.8 Gy fractions resulted in the most favorable results, but only in the subgroup with positive surgical margins (n=98). King, in his extensive review (13), found that in patients treated with radiotherapy only without androgen deprivation therapy (ADT), that the radiotherapy dose and PSA level prior to RT were the only significant factors for recurrence (PSA ≥0.2 ng/mL after salvage radiotherapy). He reported a very well fit sigmoidal relationship between dose and recurrence with an improvement in recurrence-free survival by 2.0% per additional Gy given [95%CI: 1.1–3.2]. He calculated that a dose of 70 Gy would achieve a 58.4% rate of RFS vs. 38.5% for 60 Gy. However, he could not identify a subgroup of patients who might benefit from dose-escalation. Similar findings were described even ten years earlier by Ohri et al. (14) in their systematic review and regression meta-analysis with radiobiological modelling. They stated that the maximum achievable 5-year recurrence-free survival following salvage RT appears to be between 70% and 80%. This suggests that a portion of patients who receive salvage RT already have occult extra-pelvic disease. Indeed, as reported by King (13), Ohri et al. (14) found that the 5-year recurrence-free survival increased by 2.5% per Gy (95% CI: 1.0–4.0%) and that recurrence-free survival decreased with increasing pre-radiotherapy PSA, (–18.1% per 1 ng/mL increase, 95% CI: [–29.2% to –7.0%]). A smaller (n=144) prospective study had shown an advantage for a dose increase from 66 to 72 Gy in the salvage setting only in in patients with a higher Gleason score (8–10). However, a longer follow-up period of 4-years revealed no advantage of dose escalation for biochemical PFS (15). In this line a recently published, much larger, prospective randomized study [SAKK 09/10 (n=350)] (16) showed no advantage for dose-escalation to 70 Gy compared to 64 Gy. But higher dose resulted in higher gastrointestinal toxicity. Surgical margin status was not analyzed as a prognostic factor in this study. In this trial, patients were treated to the prostate bed only, no routine PSMA-PET was performed and no androgen deprivation therapy (ADT) was given (16).
In conclusion, although a large randomized trial found no advantage for dose escalation to 70Gy, several retrospective studies showed an advantage.
The above-mentioned data seem in in contradiction to the results with PSMA-PET: conventional doses to PSMA-PET-positive lesions seem sufficient. Only Rowe et al. (17) found a high rate of persistent local disease on PSMA-PET within the radiotherapy field after salvage radiotherapy. They reported that 7/32 patients (22%) had such a recurrence and that six of these local recurrences were within 100% of the prescribed isodose of 66.6-72 Gy (17). The local recurrence rate in this study was much higher than the one reported by Byrne et al. (18) who found a PSMA-PET determined local failure rate within the radiation-field in only 2/50 (4%) of patients treated with prostate bed radiotherapy, despite even slightly lower doses of 64-68 Gy. Another study by Solomonidou et al. (19) using PSMA-PET before salvage radiotherapy also found a lower in-field recurrence rate and showed that recurrences appeared in only 1/16 patients inside of the RT-field treated with 66-70 Gy. This in patients who had a PSMA-PET before salvage radiotherapy and a second one at PSA relapse. The above findings show that in the PSMA-era in-field recurrences after salvage radiotherapy are rare. Interestingly, the study by Byrne et al. (18) found that salvage radiotherapy with the help of PSMA-CT to the prostate bed (n=310) or bed with lymph nodes (n=99) lead to an excellent in-field control (4% vs. 6%) and a similar control rate for PSA relapse of 71% and 70%, respectively, despite a higher rate of ADT in the group with nodal RT (13% vs 92%). Isolated nodal failure occurred in 1/3 of the patients with prostate bed therapy only but was rare in the group with prostate bed and pelvic node irradiation. Nevertheless, although local recurrence after radiotherapy is rare, there is some promising data on dose-escalation to >72 Gy on PSMA-positive lesions. Vogel et al. (20) used a simultaneous-integrated boost for PSMA-PET-positive lesions to 76.5 Gy in 2.25 Gy vs. 68 Gy in 2 Gy fractions. They found a better PSA-response rate for patients treated with dose-escalation. Only 1/7 patients who had a PSMA-PET for recurrence after radiotherapy had a local recurrence. It wasn’t clear if this recurrence was in the boost-volume or not. Another study investigated dose-escalation in patients with a positive MRI after prostatectomy. Benziane-Ouaritini (21) et al. found that dose of ≥72 Gy showed better progression free survival on multivariate analysis. Others are studying dose-escalation to the lymphnodes (Prospser 1) (22), in patients with insufficient PSA response after 50 Gy. It therefore seems that the benefit of dose-escalation to positive lesions on PSMA-PET is not clear.
There are two possible explanations in the case of an elevated PSA post-prostatectomy but absence of radiologic disease on PSMA-PET. Either the patient is metastatic and needs to ADT to radiotherapy. Or, there is non-visible local disease and dose-reduction would risk undertreating the patient. According to the recently published Advanced Prostate Cancer Consensus Conference (APCCC) 2022 (23), the decision on how to best treat these patients depends on several factors. But radiation- dose-reduction was not an option.
While the experts in APCC Conference didn’t discuss to not treat patients with a negative PSMA-PET, others, especially in Australia, argue that there is no clear opinion on how to treat patients with negative PSMA-PET (24).
Another possibility would be to spare the prostate bed and treat the lymphnodes only. This because post-radiotherapy recurrences in PSMA-PET negative patients occurred in 44% in the lymphnodes (25). There are a few studies with a smaller number of patients, which focused on the prognostic importance of a negative PSMA-PET, summarized in Table 1. For example, Scharl et al. (25) in their retrospective multicenter review compared 173 patients with a negative PSMA-PET with 168 patients with only local disease in the prostatic bed. Univariate analysis for biochemical progression-free survival (PFS) post radiotherapy showed that PSMA-PET negative patients had better PFS than PET/CT positive patients (80.8% vs. 71.6% p = 0.019). However, risk factors were not even distributed in both groups, PSA doubling time was significantly shorter in the PSMA-PET positive group. The authors concluded, that salvage RT should not be withhold from patients with negative PSMA PET/CT. Similarly, Emmet et al. (27) found that patients with a negative PSMA-PET had the best 3-yr freedom from progression (FFP; 82.5%) compared to patients with localized disease. even though the patients with a negative PSMA-PET received smaller radiotherapy fields and were less likely to receive ADT. This is in line with an earlier publication of Emmet et al. (26) reporting that in PSMA-PET negative patients treatment response was not different compared to patients with a positive PSMA-PET in the prostate-bed. This in patients with a PSA 0.05-1.0 ng/mL, treatment response defined as both PSA ≤ 0.1 ng/mL and >50% reduction in PSA. Another study (29) showed a nearly identical outcome in PSMA-PET positive and negative patients. In a retrospective study from 2 German centers, Schmidt-Hegemann et al. (29) showed that PSMA-negative and -positive patients had the same outcome when treated with salvage radiotherapy alone without ADT. In this study, 53% (48/90) of the patients had a negative PSMA. The median follow-up in this study was short (23 months) and therefore results on outcome should be considered cautiously. Biochemical recurrence in patients treated without ADT was not different whether the PSMA was negative or positive (29). Interestingly, in contradiction to the other studies, in a recent study, Solomonidou et al. (19) found that patients with a PSA of <0.2 ng/mL and with localized disease on PSMA-PET had worse biochemical recurrence-free survival than patients with a negative PSMA-PET. Some argue that a negative PSMA-PET doesn’t require immediate treatment and that progression to treatment in initially un-treated patients with a negative PSMA-PET is only 15-60% (27, 30). In conclusion, it seems that a negative PSMA-PET isn’t necessarily a sign for better outcome after salvage radiotherapy. It seems that results are similar in patients treated with a negative and positive PSMA-PET. Therefore, so far there is no scientific evidence for dose-de-escalation or omission of treating the prostate-bed in this context.
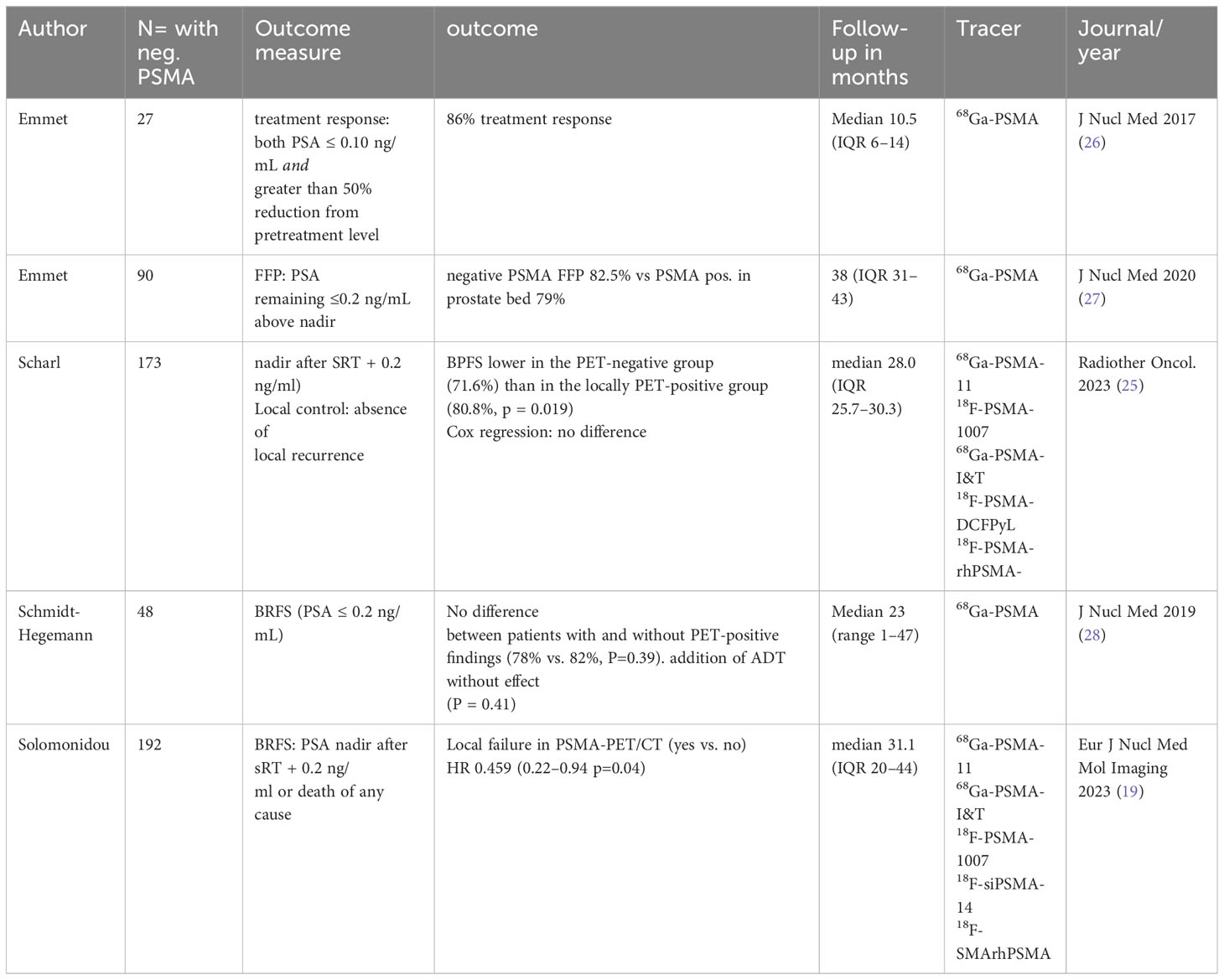
Table 1 Publications with a negative PSMA-PET.
In a smaller open-label randomised controlled trial, the use of 18F-fluciclovine-PET/CT for the decision-making process in radiotherapy resulted in a 12% improvement in event-free survival at 3 years. An event was defined as a PSA of 0.2 ng/mL higher than the nadir after radiotherapy, followed by another rise or persistent PSA, or failure on imaging or digital rectal examination (31).
If one may not rely only on PSMA-PET for dose tailoring, maybe one could use PSMA-PET in conjunction with clinical factors. Patients with a low PSA and positive surgical margins are probably the ones who benefit most from salvage-radiotherapy. In these patients with low PSA and positive surgical margins, the benefit from dose – escalation might be biggest because of the higher chance of local recurrence.
The importance of treating patients in the postoperative setting at a low PSA level has been recently shown in a multicenter retrospective study of >2500 patients (32). It was found that all-cause mortality was higher for patients with a prior radiotherapy PSA of >0.25 ng/mL compared to ≤0.25 ng/mL. Other studies in the era of PSMA-PET have shown similar results (33–35).
A multi-institutional database for patients treated with salvage RT as well as in the adjuvant setting has shown that positive margins have the best positive predictive factor for biochemical control after postoperative radiotherapy (36). Similar results were reported in a much earlier EORTC 22911 study by Van der Kwast et al. (37), who showed that positive surgical margins were the only factor predicting for the benefit of adjuvant radiotherapy. Patients who had positive surgical margins and were treated with adjuvant radiotherapy had a 5-year recurrence free survival of 78% vs. 49% for patients in the control arm receiving radiotherapy in a non-adjuvant setting No benefit was found for the other two inclusion criteria; extracapsular extension and seminal vesicle invasion. Adjuvant radiotherapy had no effect on outcome in patients with a high Gleason score or seminal vesicle involvement if the surgical margins were negative. These patients seemed to have already metastasized. It must be noted that a large (>11,500 patients) retrospective series showed the effect of salvage radiotherapy in more aggressive margin-negative patients (38). But this effect might have been influenced by the use of ADT or other risk factors.
If we have no clear data on tailoring radiation-therapy dose according to PSMA-PET findings, maybe PSMA can help as a biomarker. Spohn et al. (39), in a multicenter study consisting of 235 patients with recurrence on PSMA-PET after prostatectomy, found that PSMA positive recurrence with an SUVmax (standardized uptake value) in the 4th quartile was a marker for biochemical recurrence after salvage radiotherapy (HR 2.3, p=0.022). They further found that biochemical recurrence-free survival at 2 years in patients with recurrence confined to the prostate bed was 80%. This led to their conclusion that patients with prostate bed -confined disease might benefit from intensification of local treatment instead of systemic treatment. Other studies have found a correlation between quantitative PSMA uptake and cancer aggressiveness (40, 41). But it is presently not possible to use PSMA as a reproducible biomarker. Values between different centers can’t be compared. Differences in SUV between centers are too big due to differences in tracers, scanners, protocols, and imaging time points. Although validation of genomic classifiers is still needed (42), a combination with PSMA-PET could further help identify more favorable subgroups. Patients in SAKK 09/10 with a Decipher score of low to intermediate, had a 5-year freedom from biochemical progression (FFBP) of 71% (43). This is similar or a bit inferior to the ~ 80%, in the most favorable prognostic factor groups in the PSMA-PET studies (39).
Another possibility may be the use of PSMA as a biomarker on circulating tumor cells (CTCs). So far, in small studies, a high fraction of PSMA-negative CTCs has been shown to be a negative prognostic factor in metastatic hormone-resistant cancers (44, 45).
In the future, intraindividual references (e.g., PSMA Score with respect to uptake in liver/blood pool for 68Ga-PSMA-11) could help to identify lesions with higher aggressiveness that could benefit from dose-escalation. In the mean-time, PSMA-PET findings have already been incorporated into nomograms (35).
In conclusion, while PSMA can serve as a road map for dose-tailoring in radiotherapy in the postoperative salvage setting, we couldn’t find a scientific rationale for dose reduction in PSMA-PET negative or dose increase in PSMA-PET positive patients. Because some studies show cancer persistence in the radiotherapy field after PSMA-PET guided radiotherapy, several ongoing studies are pursuing the avenue of dose-escalation with PSMA—imaging, especially with hypofractionation (46, 47). Patients with positive surgical margins and low-PSAs have the highest risk of local recurrence only and might benefit most from dose-escalation.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
AC: Writing – original draft, Writing – review & editing. DZ: Writing – original draft, Writing – review & editing. CO: Writing – original draft, Writing – review & editing. DT: Writing – original draft, Writing – review & editing, Conceptualization. SK: Writing – original draft, Writing – review & editing. IB: Writing – original draft, Writing – review & editing. DB: Writing – original draft, Writing – review & editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Farolfi A, Calderoni L, Mattana F, Mei R, Telo S, Fanti S, et al. Current and emerging clinical applications of PSMA PET diagnostic imaging for prostate cancer. J Nucl Med (2021) 62(5):596–604. doi: 10.2967/jnumed.120.257238
2. Shakespeare TP. Effect of prostate-specific membrane antigen positron emission tomography on the decision-making of radiation oncologists. Radiat Oncol (2015) 10:1–4. doi: 10.1186/s13014-015-0548-8
3. Zilli T. PET/CT-based salvage radiotherapy for recurrent prostate cancer after radical prostatectomy: impact on treatment management and future directions. Front Oncol (2021) 11:742093. doi: 10.3389/fonc.2021.742093
4. Petit C, Delouya G, Taussky D, Barkati M, Lambert C, Beauchemin M-C, et al. PSMA-PET/CT–guided intensification of radiation therapy for prostate cancer (PSMAgRT): findings of detection rate, effect on cancer management, and early toxicity from a phase 2 randomized controlled trial. Int J Radiat Oncol Biol Phys (2023) 116(4):779–87. doi: 10.1016/j.ijrobp.2022.12.055
5. Ng M, Guerrieri M, Wong LM, Taubman K, Sutherland T, Benson A, et al. Changes in management after 18F-DCFPyL PSMA PET in patients undergoing postprostatectomy radiotherapy, with early biochemical response outcomes. J Nucl Med (2022) 63(9):1343–8. doi: 10.2967/jnumed.121.263521
6. Zamboglou C, Strouthos I, Sahlmann J, Farolfi A, Serani F, Medici F, et al. Metastasis-free survival and patterns of distant metastatic disease after prostate-specific membrane antigen positron emission tomography (PSMA-PET)-guided salvage radiation therapy in recurrent or persistent prostate cancer after prostatectomy. Int J Radiat Oncol Biol Phys (2022) 113(5):1015–24. doi: 10.1016/j.ijrobp.2022.04.048
7. Berghen C, De Meeler G. Postoperative radiation therapy in prostate cancer: Timing, duration of hormonal treatment and the use of PSMA PET-CT. Int J Radiat Oncol Biol Phys (2022) 113(2):252–3. doi: 10.1016/j.ijrobp.2021.03.014
8. Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet (2020) 395(10231):1208–16. doi: 10.1016/S0140-6736(20)30314-7
9. Valle L, Shabsovich D, de Meerleer G, Maurer T, Murphy DG, Nickols NG, et al. Use and impact of positron emission tomography/computed tomography prior to salvage radiation therapy in men with biochemical recurrence after radical prostatectomy: a scoping review. Eur Urol Oncol (2021) 4(3):339–55. doi: 10.1016/j.euo.2021.01.007
10. Abghari-Gerst M, Armstrong WR, Nguyen K, Calais J, Czernin J, Lin D, et al. A comprehensive assessment of 68Ga-PSMA-11 PET in biochemically recurrent prostate cancer: results from a prospective multicenter study on 2,005 patients. J Nucl Med (2022) 63(4):567–72. doi: 10.2967/jnumed.121.262412
11. Macdonald OK, Schild SE, Vora SA, Andrews PE, Ferrigni RG, Novicki DE, et al. Radiotherapy for men with isolated increase in serum prostate specific antigen after radical prostatectomy. J Urol (2003) 170(5):1833–7. doi: 10.1097/01.ju.0000091835.80547.a4
12. Maier J, Forman J, Tekyi-Mensah S, Bolton S, Patel R, Pontes JE. Salvage radiation for a rising PSA following radical prostatectomy. Urol Oncol (2004) 22(1):50–6. doi: 10.1016/j.urolonc.2003.12.001
13. King CR. The timing of salvage radiotherapy after radical prostatectomy: a systematic review. Int J Radiat Oncol Biol Phys (2012) 84(1):104–11. doi: 10.1016/j.ijrobp.2011.10.069
14. Ohri N, Dicker AP, Showalter TN. Reply letter to: Salvage radiotherapy: A plea for dose-escalation with intensity modulated radiotherapy. Eur J Cancer (2012) 48(9):1414. doi: 10.1016/j.ejca.2012.01.023
15. Qi X, Li H-Z, Gao X-S, Qin S-B, Zhang M, Li X-M, et al. Toxicity and biochemical outcomes of dose-intensified postoperative radiation therapy for prostate cancer: results of a randomized phase III trial. Int J Radiat Oncol Biol Phys (2020) 106(2):282–90. doi: 10.1016/j.ijrobp.2019.09.047
16. Ghadjar P, Hayoz S, Bernhard J, Zwahlen DR, Hölscher T, Gut P, et al. Dose-intensified versus conventional-dose salvage radiotherapy for biochemically recurrent prostate cancer after prostatectomy: the SAKK 09/10 randomized phase 3 trial. Eur Urol (2021) 80(3):306–15. doi: 10.1016/j.eururo.2021.05.033
17. Rowe LS, Harmon S, Horn A, Shankavaram U, Roy S, Ning H, et al. Pattern of failure in prostate cancer previously treated with radical prostatectomy and post-operative radiotherapy: A secondary analysis of two prospective studies using novel molecular imaging techniques. Radiat Oncol (2021) 16:1–11. doi: 10.1186/s13014-020-01733-x
18. Byrne K, Eade T, Kneebone A, Guo L, Hsiao E, Schembri G, et al. Delineating sites of failure following post-prostatectomy radiation treatment using 68Ga-PSMA-PET. Radiotherapy Oncol (2018) 126(2):244–8. doi: 10.1016/j.radonc.2017.10.022
19. Solomonidou N, Germanou D, Strouthos I, Karagiannis E, Farolfi A, Koerber SA, et al. PSMA-PET/CT-guided salvage radiotherapy in recurrent or persistent prostate cancer and PSA< 0.2 ng/ml. Eur J Nucl Med Mol Imag (2023) 50:1–8. doi: 10.1007/s00259-023-06185-5
20. Vogel MM, Dewes S, Sage EK, Devecka M, Eitz KA, Gschwend JE, et al. Feasibility and outcome of PSMA-PET-based dose-escalated salvage radiotherapy versus conventional salvage radiotherapy for patients with recurrent prostate cancer. Front Oncol (2021) 11:715020. doi: 10.3389/fonc.2021.715020
21. Benziane-Ouaritini N, Zilli T, Giraud A, Ingrosso G, Di Staso M, Trippa F, et al. Prostatectomy bed image-guided dose-escalated salvage radiotherapy (SPIDER): an international multicenter retrospective study. Eur Urol Oncol (2023) 6(4):390–8. doi: 10.1016/j.euo.2023.02.013
22. Gunnlaugsson A, Johannesson V, Wieslander E, Brun E, Bitzen U, Ståhl O, et al. A prospective phase II study of prostate-specific antigen-guided salvage radiotherapy and 68Ga-PSMA-PET for biochemical relapse after radical prostatectomy–The PROPER 1 trial. Clin Trans Radiat Oncol (2022) 36:77–82. doi: 10.1016/j.ctro.2022.07.001
23. Gillessen S, Bossi A, Davis ID, de Bono J, Fizazi K, James ND, et al. Management of patients with advanced prostate cancer. Part I: intermediate-/high-risk and locally advanced disease, biochemical relapse, and side effects of hormonal treatment: report of the Advanced Prostate Cancer Consensus Conference 2022. Eur Urol (2023) 83(3):267–93. doi: 10.1016/j.eururo.2022.11.002
24. Khanna Y, Chinni V, Gnanasambantham K, O’Sullivan R, Ballok ZE, Ryan A, et al. Can 68Ga-PSMA positron emission tomography and multiparametric MRI guide treatment for biochemical recurrence after radical prostatectomy. BJU Int. (2023) 132:321–8. doi: 10.1111/bju.16037
25. Scharl S, Zamboglou C, Strouthos I, Farolfi A, Serani F, Lanzafame H, et al. Salvage radiotherapy is effective in patients with PSMA-PET-negative biochemical recurrence-results of a retrospective study. Radiotherapy Oncol (2023) 184:109678. doi: 10.1016/j.radonc.2023.109678
26. Emmett L, van Leeuwen PJ, Nandurkar R, Scheltema MJ, Cusick T, Hruby G, et al. Treatment outcomes from 68Ga-PSMA PET/CT–informed salvage radiation treatment in men with rising PSA after radical prostatectomy: prognostic value of a negative PSMA PET. J Nucl Med (2017) 58(12):1972–6. doi: 10.2967/jnumed.117.196683
27. Emmett L, Tang R, Nandurkar R, Hruby G, Roach P, Watts JA, et al. 3-Year freedom from progression after 68Ga-PSMA PET/CT–triaged management in men with biochemical recurrence after radical prostatectomy: results of a prospective multicenter trial. J Nucl Med (2020) 61(6):866–72. doi: 10.2967/jnumed.119.235028
28. Schmidt H, Suciu S, Punt CJ, Gore M, Kruit W, Patel P, et al. Pretreatment levels of peripheral neutrophils and leukocytes as independent predictors of overall survival in patients with American Joint Committee on Cancer Stage IV Melanoma: results of the EORTC 18951 Biochemotherapy Trial. J Clin Oncol (2007) 25(12):1562–9. doi: 10.1200/JCO.2006.09.0274
29. Schmidt-Hegemann N-S, Stief C, Kim T-H, Eze C, Kirste S, Strouthos I, et al. Outcome after PSMA PET/CT–based salvage radiotherapy in patients with biochemical recurrence after radical prostatectomy: a 2-institution retrospective analysis. J Nucl Med (2019) 60(2):227–33. doi: 10.2967/jnumed.118.212563
30. Ong S, Pascoe C, Kelly BD, Ballok Z, Webb D, Bolton D, et al. PSMA PET-CT imaging predicts treatment progression in men with biochemically recurrent prostate cancer—A prospective study of men with 3 year follow up. Cancers (2022) 14(11):2717. doi: 10.3390/cancers14112717
31. Jani AB, Schreibmann E, Goyal S, Halkar R, Hershatter B, Rossi PJ, et al. 18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): a single centre, open-label, phase 2/3 randomised controlled trial. Lancet (2021) 397(10288):1895–904. doi: 10.1016/S0140-6736(21)00581-X
32. Tilki D, Chen M-H, Wu J, Huland H, Graefen M, Mohamad O, et al. Prostate-specific antigen level at the time of salvage therapy after radical prostatectomy for prostate cancer and the risk of death. J Clin Oncol (2023) 41(13):2428. doi: 10.1200/JCO.22.02489
33. Abugharib A, Jackson WC, Tumati V, Dess RT, Lee JY, Zhao SG, et al. Very early salvage radiotherapy improves distant metastasis-free survival. J Urol (2017) 197(3 Part 1):662–8. doi: 10.1016/j.juro.2016.08.106
34. Moreira DM, Jayachandran J, Presti JC Jr., Aronson WJ, Terris MK, Kane CJ, et al. Validation of a nomogram to predict disease progression following salvage radiotherapy after radical prostatectomy: results from the SEARCH database. BJU Int (2009) 104(10):1452–6. doi: 10.1111/j.1464-410X.2009.08623.x
35. Zamboglou C, Peeken JC, Janbain A, Katsahian S, Strouthos I, Ferentinos K, et al. Development and validation of a multi-institutional nomogram of outcomes for PSMA-PET–based salvage radiotherapy for recurrent prostate cancer. JAMA Network Open (2023) 6(5):e2314748–e. doi: 10.1001/jamanetworkopen.2023.14748
36. Campbell SR, Tom MC, Agrawal S, Efstathiou JA, Michalski JM, Abramowitz MC, et al. Integrating prostate-specific antigen kinetics into contemporary predictive nomograms of salvage radiotherapy after radical prostatectomy. Eur Urol Oncol (2022) 5(3):304–13. doi: 10.1016/j.euo.2021.04.011
37. Van der Kwast TH, Bolla M, Van Poppel H, Van Cangh P, Vekemans K, Da Pozzo L, et al. Identification of patients with prostate cancer who benefit from immediate postoperative radiotherapy: EORTC 22911. J Clin Oncol (2007) 25(27):4178–86. doi: 10.1200/JCO.2006.10.4067
38. Stephenson AJ, Eggener SE, Hernandez AV, Klein EA, Kattan MW, Wood DP Jr., et al. Do margins matter? The influence of positive surgical margins on prostate cancer–specific mortality. Eur Urol (2014) 65(4):675–80. doi: 10.1016/j.eururo.2013.08.036
39. Spohn SK, Farolfi A, Schandeler S, Vogel MM, Ruf J, Mix M, et al. The maximum standardized uptake value in patients with recurrent or persistent prostate cancer after radical prostatectomy and PSMA-PET-guided salvage radiotherapy—a multicenter retrospective analysis. Eur J Nucl Med Mol Imag (2022) 50:1–10. doi: 10.1007/s00259-022-05931-5
40. Chen M, Qiu X, Zhang Q, Zhang C, Zhou Y, Zhao X, et al. PSMA uptake on [68Ga]-PSMA-11-PET/CT positively corrects with prostate cancer aggressiveness. Q J Nucl Med Mol Imaging: Off Publ Ital Assoc Nucl Med (AIMN)[and] Int Assoc Radiopharmacology (IAR),[and] Section Soc (2019) 66(1):67–73. doi: 10.1097/01.JU.0000557493.33637.42
41. Zschaeck S, Andela SB, Amthauer H, Furth C, Rogasch JM, Beck M, et al. Correlation between quantitative PSMA PET parameters and clinical risk factors in non-metastatic primary prostate cancer patients. Front Oncol (2022) 12:1714. doi: 10.3389/fonc.2022.879089
42. Spohn SK, Draulans C, Kishan AU, Spratt D, Ross A, Maurer T, et al. Genomic classifiers in personalized prostate cancer radiotherapy approaches–a systematic review and future perspectives based on international consensus. Int J Radiat Oncol Biol Phys (2022) 116(3):503–20. doi: 10.1016/S2666-1683(22)02485-5
43. Dal Pra A, Ghadjar P, Hayoz S, Liu V, Spratt D, Thompson D, et al. Validation of the Decipher genomic classifier in patients receiving salvage radiotherapy without hormone therapy after radical prostatectomy–an ancillary study of the SAKK 09/10 randomized clinical trial. Ann Oncol (2022) 33(9):950–8. doi: 10.1016/j.annonc.2022.05.007
44. Derlin T, Riethdorf S, Schumacher U, Lafos M, Peine S, Coith C, et al. PSMA-heterogeneity in metastatic castration-resistant prostate cancer: Circulating tumor cells, metastatic tumor burden, and response to targeted radioligand therapy. Prostate (2023) 83(11):1076–88. doi: 10.1002/pros.24549
45. Gupta S, Halabi S, Yang Q, Roy A, Tubbs A, Gore Y, et al. PSMA-positive circulating tumor cell detection and outcomes with abiraterone or enzalutamide treatment in men with metastatic castrate-resistant prostate cancer. Clin Cancer Res (2023) 29(10):1929–37. doi: 10.1158/1078-0432.CCR-22-3233
46. Francolini G, Jereczek-Fossa BA, Di Cataldo V, Simontacchi G, Marvaso G, Gandini S, et al. Stereotactic or conventional radiotherapy for macroscopic prostate bed recurrence: A propensity score analysis. La Radiologia Medica. (2022) 127(4):449–57. doi: 10.1007/s11547-022-01465-w
Keywords: prostate cancer, postoperative radiotherapy, PSMA-PET, PSA, dose ecalation
Citation: Champion A, Zwhalen DR, Oehler C, Taussky D, Kroeze SGC, Burger IA and Benzaquen D (2023) Can PSMA PET/CT help in dose-tailoring in post-prostatectomy radiotherapy? Front. Oncol. 13:1268309. doi: 10.3389/fonc.2023.1268309
Received: 27 July 2023; Accepted: 04 September 2023;
Published: 20 September 2023.
Edited by:
Liang Cheng, Brown University, United StatesReviewed by:
Francolini Giulio, University of Florence, ItalyCopyright © 2023 Champion, Zwhalen, Oehler, Taussky, Kroeze, Burger and Benzaquen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Taussky, ZGFuaWVsLnRhdXNza3kuY2h1bUBzc3NzLmdvdXYucWMuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.