
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol. , 23 January 2024
Sec. Genitourinary Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1266369
This article is part of the Research Topic Expert Opinions in Genitourinary Oncology View all 6 articles
 Alina Rosinha1
Alina Rosinha1 Carlos Rabaça2Fernando Calais3
Carlos Rabaça2Fernando Calais3 João Moreira Pinto4
João Moreira Pinto4 João Vasco Barreira5,6Ricardo Fernandes7Rodrigo Ramos8Ana Cristina Fialho9José Palma dos Reis10*
João Vasco Barreira5,6Ricardo Fernandes7Rodrigo Ramos8Ana Cristina Fialho9José Palma dos Reis10*Non-metastatic castration-resistant prostate cancer (nmCRPC) represents a challenging disease state in prostate cancer care. nmCRPC patients with a high risk of progression to metastatic disease who are identified by a prostate-specific antigen doubling time (PSADT) ≤10 months are eligible for treatment with the novel androgen receptor inhibitors (ARIs), shown to delay disease progression and extend survival. However, nmCRPC is often unexploited in clinical practice due to a lack of standardization in the methodology and in the tools used for its identification. In this article, a group of Urology and Oncology specialists with acknowledged expertise in prostate cancer reviews the state of the art in the management of high-risk nmCRPC patients, identifies gaps and unmet needs, and proposes strategies to optimize the identification of this patient subgroup in the clinical practice and improve their health outcomes.
According to recent data, prostate cancer ranked second as the most common cancer in men in 2020, accounting for an estimated 1.4 million diagnoses and 375,000 deaths globally that year (1). In Portugal, the latest data from the National Cancer Registry (RON) relates to 2019 and shows that prostate cancer was the most frequently diagnosed cancer in men that year, with 6912 new cases, and resulted in 1901 deaths (2), and GLOBOCAN 2020 reported 6759 new cases (20% of all cancers in men) and 1917 deaths from the disease (1).
Prostate cancer is a biologically heterogeneous entity, with histomorphologic and molecular characteristics that show substantial diversity between different patients (inter-patient heterogeneity) and within a given tumor (intra-tumoral heterogeneity), both in primary tumors (3–8) and in metastatic disease (9–12), with implications in diagnosis, clinical management, and prognosis (4, 13–15).
The clinical presentation can range from localized indolent to rapidly progressing metastatic disease (16–18). For patients presenting with early-stage disease at diagnosis, local therapy is often curative. However, more than 20% of patients experience biochemical recurrence, indicated by a rise in prostate-specific antigen (PSA) levels (19–21), and become eligible for first-line androgen deprivation therapy (ADT) (22). Progression during ADT, observed in 10−20% of patients (23), marks the onset of the castration-resistant state (24, 25), an advanced disease state with increased likelihood of metastases (26, 27). Around 15−30% of these patients become castration-resistant without imaging evidence of metastases, defining the non-metastatic (nm or M0) castration-resistant prostate cancer (CRPC) disease state (28–30).
The organ-specific serum marker PSA and its doubling time (PSADT), which measures the exponential increase in serum PSA over time (31), are used as measures of increasing cancer volume and prognostic biomarkers to guide treatment decisions. Guidelines recommend PSA testing every 3–4 months and imaging assessment every 3–6 months for patients with PSADT ≤ 10 months and every 6–12 months for those with PSADT >10 months (32). Despite these recommendations, PSA and imaging assessment are underused in the real-world practice after initiation of continuous ADT, as shown in a large, population-based cohort study where more than half of patients with CRPC who progressed to high-risk nmCRPC received ≤2 PSA tests in the previous year and 31% received no imaging studies in the following 12 months (33). Infrequent patient monitoring hinders proper disease staging, risk stratification, and detection of treatment failure and/or metastases, with suboptimal patient outcomes. Both the joint EAU-EANM-ESTRO-ESUR-SIOG and ESMO guidelines strongly recommend the use of PSADT to define the risk of recurrence in prostate cancer after radical prostatectomy and radiation therapy (22, 34).
PSADT represents the number of months it takes for PSA to increase two-fold and is calculated assuming an exponential rise in serum PSA. The formula takes into account the natural logarithm of 2 divided by the slope obtained from fitting a linear regression of the natural log of PSA over time, i.e., PSADT = [ln(2)*/IT]/[ln(PSA final) – ln(PSA initial)] (35). However, several different PSADT definitions have been used according to the mathematical formula employed and the PSA values included (number, time period, intervals) (36), with the values retrieved also shown to vary widely among calculations (37). For example, the Memorial Sloan Kettering Cancer Center method calculates a regression slope integrating all PSA values, while other methods do not include all PSA values and transform PSA before estimating the slope (37). Regardless of these disparities, according to the EAU - EANM - ESTRO - ESUR - ISUP - SIOG guidelines, some rules can be assumed for PSADT calculation (34):
● At least 3 PSA measurements are required (35);
● A minimum time period between measurements (4 weeks) is preferable due to potential statistical ‘noise’ when PSA values are obtained too close together (this can be reconsidered in case of very active disease);
● All PSA values should be >0.20 ng/mL and follow a global rising trend;
● All included PSA values should be obtained within the past 12 months at most, to reflect the current disease activity;
● PSADT is often mentioned in months, or in weeks in highly active disease.
nmCRPC is a disease stage defined by a very specific diagnosis established within a sensitive time period. It is formally defined by a 25% rise in PSA levels from nadir (starting at ≥1.0 ng/mL and with a minimum rise of 2.0 ng/mL) in the presence of castrate testosterone levels (<50 ng/dL) and absence of detectable disease on conventional imaging (computed tomography [CT] and bone scan or magnetic resonance imaging [MRI]) (24, 25). This PSA rise must be confirmed by a second value obtained ≥3 weeks later in the same context of castrate testosterone levels (<50 ng/dL) (24).
Data about the prevalence of nmCRPC is scarce, with one study from 2013 estimating it to range from 2−8% in different countries, with a trend toward an increase over the next years due to widespread PSA screening (38).
Patients are mostly asymptomatic, with data retrieved from the placebo arms of clinical trials indicating that up to 60% develop overt metastatic disease within 3−5 years (29, 39–41). However, these patients were assessed with conventional imaging methods (CT/MRI), and more recent evidence suggests that some may already have metastatic disease if prostate-specific membrane antigen ligand positron emission tomography (PSMA-PET) imaging had been employed instead. Indeed, emerging studies suggest that PSMA-PET detects prostate cancer with superior sensitivity to conventional imaging, as the study by Fendler et al., in which PSMA-PET was positive in 196 of 200 patients with high-risk nmCRPC and detected 55% of M1 disease and 44% of pelvic disease despite negative conventional imaging (42); and the study by Fourquet and colleagues, which used PSMA-PET to restage 30 nmCRPC patients and found at least one malignant focus in 90% of those (43). Notwithstanding, the performance of PSMA-PET in nmCRPC is still poorly studied and there are no phase III trials showing a survival benefit with its use versus CT/MRI to guide treatment decisions. This is also reflected in the recent EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines, which do not consider PSMA-PET in the management of nmCRPC (34). Overall, the use of PSMA-PET in nmCRPC at this point is still being investigated.
Several prognostic markers of metastasis-free survival (MFS) and overall survival (OS) have been identified in nmCRPC, including baseline PSA (29, 40), PSA velocity (29), PSA at CRPC diagnosis (44, 45), and PSADT (39, 46). Since the presence of metastatic disease is associated with increased morbidity and mortality and decreased quality of life (47), preventing or delaying progression to metastatic state is the primary therapeutic goal in the nmCRPC patient population (47).
Until 2018, there was no standard of care for patients with nmCRPC progressing on ADT, neither PSA or PSADT cut-offs to guide treatment decisions. Patients were usually managed with a watchful waiting approach until the detection of metastases or with loco-regional treatments (48). Maximal androgen blockade, through the addition of a first-generation antiandrogen (e.g., bicalutamide) to ADT, and switching or withdrawal of antiandrogens were sometimes offered to these patients without evidence of a survival benefit demonstrated in clinical trials, with short-term PSA responses and limited benefit (49–52).
The introduction of next-generation androgen receptor inhibitors (ARIs) apalutamide, darolutamide, and enzalutamide changed the therapeutic landscape of prostate cancer, providing therapy options with improved outcomes, including for nmCRPC patients. These agents have been shown to extend MFS in nmCRPC patients with no detectable metastases on conventional imaging and a PSADT <10 months on continuous ADT (i.e., at high risk of developing metastatic disease) when added to ADT in the respective landmark phase 3 SPARTAN, ARAMIS, and PROSPER trials (53–55). In subsequent analyses with longer follow-up, they also demonstrated a survival benefit for these patients, reducing the risk of death compared to placebo by 22–31% (56–58). These results led to the recommendation in international guidelines for the use of apalutamide, darolutamide, or enzalutamide in addition to ADT in patients with nmCRPC and a PSADT <10 months (34, 59), with factors like treatment toxicity, patient comorbidities, drug interactions, and access determining the choice of the best agent for each individual patient.
PSA and PSADT are prognostic biomarkers used to guide therapy intensification with life-prolonging therapies in nmCRPC. Both have been linked to patient outcomes in this setting, with patients who present a rise in PSA level and a short PSADT (PSADT ≤10 months) bearing a higher risk of metastatic progression and death (29, 39, 40, 60).
Regular PSA monitoring and imaging assessment are crucial for identifying nmCRPC prior to the development of metastases, particularly given that these patients are often asymptomatic (61, 62). In addition, regular PSA monitoring allows the accurate calculation of PSADT, crucial for prognostic risk assessment in nmCRPC and for making evidence-based decisions toward therapy intensification through the addition of ARIs to the treatment backbone, delaying the development of metastases and improving survival (53, 54, 58). In a recent retrospective study, among 944 nmCRPC patients, 97.6% progressed to high-risk disease with PSADT ≤10 months (33), highlighting the relevance of this biomarker in the identification of the high-risk nmCRPC state.
Although the treatment landscape for nmCRPC has substantially evolved, the timely identification of high-risk nmCRPC patients in the clinical practice remains an unmet need. This is mainly due to inconsistency in the frequency of PSA monitoring in the routine practice and therefore in the calculation of PSADT, and to a lack of standardization in the methodology and tools used to do this calculation. These patients are mainly followed in Urology and Oncology setting, where the clinical practice of identification of the high-risk state has been variable and non-systematic, both regarding the frequency of PSADT assessment and the tools used to do it. And this represents a significant barrier for successfully incorporating the currently available treatments into the real-world practice and offering these patients a more favorable prognosis.
It is therefore crucial that urologists and oncologists managing nmCRPC patients adopt and routinely apply proper tools to calculate PSADT and make treatment decisions for their patients accordingly. Some tools are already available to allow healthcare providers to accurately estimate PSADT at the point of care and assist them in their decision-making process. These include the online PSADT calculator and two materials that resulted from the conversion into physical format of the results retrieved by the online calculator and have the potential to be more easily accessed in the daily clinical practice and more convenient for the clinician: the PSA Do-IT ruler and the PSA Do-IT table.
The PSADT calculator (https://www.mdapp.co/psa-doubling-time-calculator-535/) is an online tool for determining the number of months it takes for PSA levels to double. The scientific rationale and calculations for the development of the calculator are based on publications in the literature (36, 63) and are detailed on the calculator’s website. The accuracy of the estimate improves as more PSA values are entered into the calculator. Therefore, for prostate cancer patients with biochemical recurrence, an optimal PSADT calculation should include as many of the patient’s PSA values as possible within two years of the first documented PSA recurrence. A shorter PSADT (≤6 months) is a negative predictor, reflecting a faster increase in PSA levels, while a longer PSADT (>6 months) is a positive predictor, reflecting a slower increase in PSA levels over time (63–66).
The PSA Do-IT ruler is a material resource developed by Janssen Portugal directly derived from the online PSADT calculator to quickly and easily identify patients with a PSADT ≤10 months in clinical practice (Figure 1). It can be carried in the pocket or kept on the office desk and used to quickly screen and identify these patients based on the months between PSA measurements and the percentage PSA variation, allowing a quick assessment of the patient’s risk status.

Figure 1 PSA Do-IT ruler for identifying patients with PSADT ≤10 months in the clinical practice.
The PSA Do-IT table is another material resource developed by Janssen Portugal to quickly identify patients with a PSADT ≤10 months, based on the results obtained by the online PSADT calculator (Figure 2). By combining two different PSA levels and the time between measurements, the table provides a reference PSA value. Increases in PSA above those shown in the table identify patients with a PSA-DT ≤ 10 months.
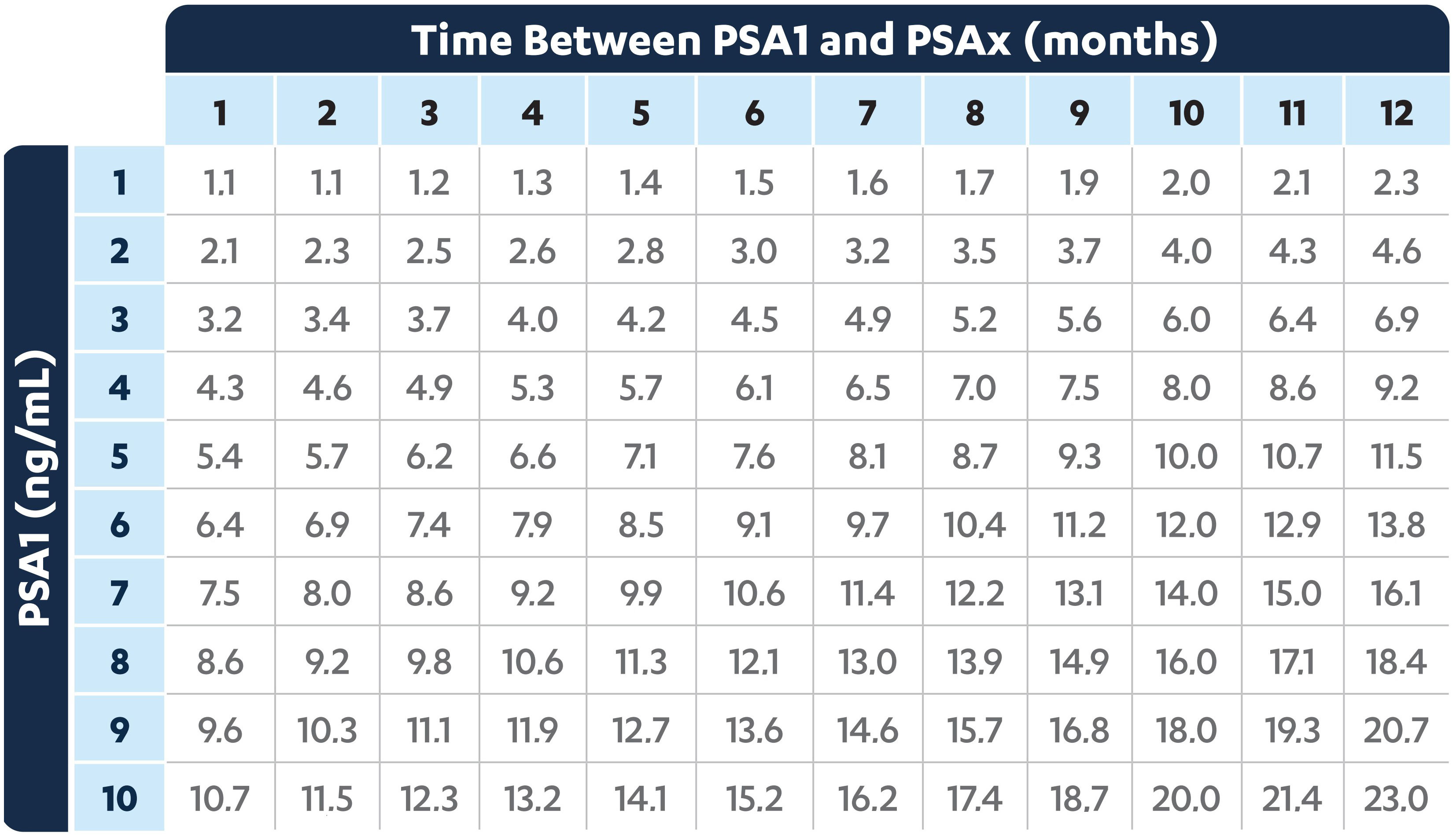
Figure 2 PSA Do-IT table for identifying patients with PSADT ≤10 months in the clinical practice.
The identification of high-risk nmCRPC patients is an evidence-based process that relies on an objective assessment: a PSADT value ≤10 months. For it to be effective, this assessment should be done regularly and using a standardized approach, but it is currently hindered by several difficulties in the daily practice and by a lack of standardization in the methodology used to do it.
Total PSA assessment and PSADT calculation are the methods preferred by specialists treating prostate cancer for identifying high-risk nmCRPC patients. PSADT is a widely acknowledged and validated method for risk stratification and definition of eligibility for treatment with new-generation ARIs, as it was the method used in clinical trials of these agents and is foreseen in the guidelines. It is not the only risk stratification tool used, with Gleason Score also having a prominent role.
However, urologists and oncologists identify several obstacles in the clinical practice that hamper the management of nmCRPC patients and consequently the identification of the high-risk disease state. Among these are lengthy diagnostic procedures, difficulties in scheduling imaging exams in due time, difficulties in scheduling appointments and in following patients for PSA assessment in time, and short consultation time, among others. Due to these obstacles, PSA assessment and consequently PSADT calculation are done inconsistently and heterogeneously among specialists, clinical practices, and patients. Some physicians estimate PSADT in every patient visit, with the periodicity of visits depending on the previous PSADT value and/or PSA kinetics; others recalculate PSADT at each patient visit in the case of patients who are in castration resistance with evidence of biochemical progression; others calculate PSADT every 3 months, possibly extending the interval to every 6 months if PSADT is very low; some only calculate PSADT at the time of the multidisciplinary Urology consultation, after the patient has been diagnosed with nmCRPC in the Urology consultation and referred to multidisciplinary follow-up; others calculate PSADT on a patient-by-patient basis according to the patient’s PSA kinetics at least twice a year. This overall lack of consistency and standardization in the procedure for identifying high-risk patients, together with the narrow time window to do it and lack of awareness of some healthcare providers about its importance challenge the optimal management of this patient subgroup, as there is the risk of missing patients who could otherwise benefit from treatment with ARIs.
Among the tools currently available to identify high-risk nmCRPC patients, the PSA Do-IT Ruler and PSA Do-IT Table are considered good and useful materials to raise awareness for PSADT calculation, but the online PSADT calculator remains the preferred and most frequently used tool among physicians.
Given this scenario, the identification of high-risk nmCRPC patients can and should be optimized, allowing patients to achieve the best health outcomes. Incorporating the PSADT calculation into laboratory request forms with the remaining analyses has the potential to be a reminder of this assessment and facilitate and expedite PSADT calculation. Implementing a physician alert when the patient has a PSADT ≤10 months, with subsequent referral to multidisciplinary group meeting, and optimizing analytical procedures and hospital appointment scheduling are additional strategies that can be used to improve the identification of high-risk nmCRPC patients in the clinical practice.
Regardless of these measures, the importance of routine PSADT calculation should be reinforced among the medical community, and awareness should be raised to its relevance as a key step to offer patients the best treatment approach. This can be achieved through the development of training and awareness initiatives directed at medical specialists who follow these patients, as well as multidisciplinary meetings with specialties involved in their management.
According to the guidelines, once identified, nmCRPC patients with PSADT ≤10 months indicative of a high risk of metastases should be treated with ARIs in combination with ADT. However, this is not the only criterion, as individual patient characteristics also impact the treatment decision. Some patients with uncontrolled comorbidities, poor performance status, and/or reduced life expectancy may not be eligible for treatment with the novel ARIs and a watchful waiting approach may be more indicated. On the other hand, biological age is not an absolute exclusion criterion for treatment eligibility. Patient and family expectations should also be assessed and considered in the treatment decision, validating their understanding of the treatment clinical benefit. Overall, the experts consider that the focus should be on the patient and not on the disease.
Overall, the patterns of care for patients with nmCRPC are under-optimized, in particular for those with high-risk disease. The current practice in the management of these patients is of under- and non-standardized monitoring, precluding timely institution of treatment with a direct impact on patients’ outcomes. The treatment landscape for high-risk nmCRPC has substantially evolved, but the routine and standardized calculation of PSADT in these patients’ clinical practice remains an unmet need, as only the confirmation of PSADT ≤10 months provides formal indication to treat patients with novel and effective therapies. There are several ways to optimize this process in the clinical practice, such as incorporating the PSADT calculation into the laboratory request form, creating physician alerts for patients with PSADT ≤10 months, with subsequent referral to multidisciplinary assessment, and optimizing analytical procedures and scheduling of appointments at the hospital. The successful implementation of these measures will predictably improve the real-world patterns of care for nmCRPC patients.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
AR: Formal Analysis, Validation, Writing – review & editing. CR: Formal Analysis, Validation, Writing – review & editing. FC: Formal Analysis, Validation, Writing – review & editing. JMP: Formal Analysis, Validation, Writing – review & editing. JVB: Formal Analysis, Validation, Writing – review & editing. RF: Formal Analysis, Validation, Writing – review & editing. RR: Formal Analysis, Validation, Writing – review & editing. ACF: Conceptualization, Formal Analysis, Validation, Writing – review & editing. JPR: Formal Analysis, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This project received financial support from Janssen-Cilag Farmacêutica, Lda.
The authors acknowledge the medical writing and editorial support in the preparation of this manuscript provided by Joana Cavaco-Silva (jo.cvsilva@gmail.com), Ph.D.
ACF is employed by the company Janssen-Cilag Farmacêutica, Lda. JMP received honoraria as a consultant/speaker from Astellas, AstraZeneca, Bayer, Bristol Myers-Squibb, Janssen, Merck, MSD, Novartis, Pierre Fabre, Pfizer, Roche, Sanofi, and Servier. JPR has participated in lectures subjected to honoraria and advisory boards for Janssen, Bayer and Astellas.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received financial support from Janssen-Cilag Farmacêutica, Lda. for the logistics of expert meetings and editorial support.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. RON. Registo Oncológico Nacional de Todos os Tumores na População Residente em Portugal, em 2019. Porto: Instituto Português de Oncologia do Porto Francisco Gentil - EPE (2022). Available at: https://ron.min-saude.pt/pt/biblioteca/publicacoes-ron/ron-2019/.
3. Spratt DE, Zumsteg ZS, Feng FY, Tomlins SA. Translational and clinical implications of the genetic landscape of prostate cancer. Nat Rev Clin Oncol (2016) 13(10):597–610. doi: 10.1038/nrclinonc.2016.76
4. Mitchell T, Neal DE. The genomic evolution of human prostate cancer. Br J Cancer (2015) 113(2):193–8. doi: 10.1038/bjc.2015.234
5. Boutros PC, Fraser M, Harding NJ, de Borja R, Trudel D, Lalonde E, et al. Spatial genomic heterogeneity within localized, multifocal prostate cancer. Nat Genet (2015) 47(7):736–45. doi: 10.1038/ng.3315
6. Løvf M, Zhao S, Axcrona U, Johannessen B, Bakken AC, Carm KT, et al. Multifocal primary prostate cancer exhibits high degree of genomic heterogeneity. Eur Urol (2019) 75(3):498–505. doi: 10.1016/j.eururo.2018.08.009
7. Marusyk A, Janiszewska M, Polyak K. Intratumor heterogeneity: the Rosetta stone of therapy resistance. Cancer Cell (2020) 37(4):471–84. doi: 10.1016/j.ccell.2020.03.007
8. Fraser M, Berlin A, Bristow RG, van der Kwast T. Genomic, pathological, and clinical heterogeneity as drivers of personalized medicine in prostate cancer. Urol Oncol Semin Orig Investig (2015) 33(2):85–94. doi: 10.1016/j.urolonc.2013.10.020
9. Beltran H, Prandi D, Mosquera JM, Benelli M, Puca L, Cyrta J, et al. Divergent clonal evolution of castration-resistant neuroendocrine prostate cancer. Nat Med (2016) 22(3):298–305. doi: 10.1038/nm.4045
10. Hong MKH, Macintyre G, Wedge DC, Van Loo P, Patel K, Lunke S, et al. Tracking the origins and drivers of subclonal metastatic expansion in prostate cancer. Nat Commun (2015) 6(1):6605. doi: 10.1038/ncomms7605
11. Haffner MC, Mosbruger T, Esopi DM, Fedor H, Heaphy CM, Walker DA, et al. Tracking the clonal origin of lethal prostate cancer. J Clin Invest (2013) 123(11):4918–22. doi: 10.1172/JCI70354
12. Gundem G, Van Loo P, Kremeyer B, Alexandrov LB, Tubio JMC, Papaemmanuil E, et al. The evolutionary history of lethal metastatic prostate cancer. Nature (2015) 520(7547):353–7. doi: 10.1038/nature14347
13. Lipinski KA, Barber LJ, Davies MN, Ashenden M, Sottoriva A, Gerlinger M. Cancer evolution and the limits of predictability in precision cancer medicine. Trends Cancer (2016) 2(1):49–63. doi: 10.1016/j.trecan.2015.11.003
14. Aihara M, Wheeler TM, Ohori M, Scardino PT. Heterogeneity of prostate cancer in radical prostatectomy specimens. Urology (1994) 43(1):60–6. doi: 10.1016/S0090-4295(94)80264-5
15. Cyll K, Ersvær E, Vlatkovic L, Pradhan M, Kildal W, Avranden Kjær M, et al. Tumour heterogeneity poses a significant challenge to cancer biomarker research. Br J Cancer (2017) 117(3):367–75. doi: 10.1038/bjc.2017.171
16. Attard G, Parker C, Eeles RA, Schröder F, Tomlins SA, Tannock I, et al. Prostate cancer. Lancet (2016) 387(10013):70–82. doi: 10.1016/S0140-6736(14)61947-4
17. Nelson WG, De Marzo AM, Isaacs WB. Prostate cancer. N Engl J Med (2003) 349(4):366–81. doi: 10.1056/NEJMra021562
18. Sartor O, de Bono JS. Metastatic prostate cancer. Longo DL editor. N Engl J Med (2018) 378(7):645–57. doi: 10.1056/NEJMra1701695
19. Zumsteg ZS, Spratt DE, Romesser PB, Pei X, Zhang Z, Polkinghorn W, et al. The natural history and predictors of outcome following biochemical relapse in the dose escalation era for prostate cancer patients undergoing definitive external beam radiotherapy. Eur Urol (2015) 67(6):1009–16. doi: 10.1016/j.eururo.2014.09.028
20. Boorjian SA, Thompson RH, Tollefson MK, Rangel LJ, Bergstralh EJ, Blute ML, et al. Long-term risk of clinical progression after biochemical recurrence following radical prostatectomy: the impact of time from surgery to recurrence. Eur Urol (2011) 59(6):893–9. doi: 10.1016/j.eururo.2011.02.026
21. Artibani W, Porcaro AB, De Marco V, Cerruto MA, Siracusano S. Management of biochemical recurrence after primary curative treatment for prostate cancer: A review. Urol Int (2018) 100(3):251–62. doi: 10.1159/000481438
22. Parker C, Castro E, Fizazi K, Heidenreich A, Ost P, Procopio G, et al. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2020) 31(9):1119–34. doi: 10.1016/j.annonc.2020.06.011
23. Kirby M, Hirst C, Crawford ED. Characterizing the castration-resistant prostate cancer population: a systematic review. Int J Clin Pract (2011) 65(11):1180–92. doi: 10.1111/j.1742-1241.2011.02799.x
24. Scher HI, Morris MJ, Stadler WM, Higano C, Basch E, Fizazi K, et al. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the prostate cancer clinical trials working group 3. J Clin Oncol (2016) 34(12):1402–18. doi: 10.1200/JCO.2015.64.2702
25. Mateo J, Fizazi K, Gillessen S, Heidenreich A, Perez-Lopez R, Oyen WJG, et al. Managing nonmetastatic castration-resistant prostate cancer. Eur Urol (2019) 75(2):285–93. doi: 10.1016/j.eururo.2018.07.035
26. Saad F, Bögemann M, Suzuki K, Shore N. Treatment of nonmetastatic castration-resistant prostate cancer: focus on second-generation androgen receptor inhibitors. Prostate Cancer Prostatic Dis (2021) 24(2):323–34. doi: 10.1038/s41391-020-00310-3
27. El-Amm J, Aragon-Ching JB. The current landscape of treatment in non-metastatic castration-resistant prostate cancer. Clin Med Insights Oncol (2019) 13:117955491983392. doi: 10.1177/1179554919833927
28. Inoue T, Segawa T, Kamba T, Yoshimura K, Nakamura E, Nishiyama H, et al. Prevalence of skeletal complications and their impact on survival of hormone refractory prostate cancer patients in Japan. Urology (2009) 73(5):1104–9. doi: 10.1016/j.urology.2008.07.062
29. Smith MR, Kabbinavar F, Saad F, Hussain A, Gittelman MC, Bilhartz DL, et al. Natural history of rising serum prostate-specific antigen in men with castrate nonmetastatic prostate cancer. J Clin Oncol (2005) 23(13):2918–25. doi: 10.1200/JCO.2005.01.529
30. Nakabayashi M, Hayes J, Taplin M-E, Lefebvre P, Lafeuille M-H, Pomerantz M, et al. Clinical predictors of survival in men with castration-resistant prostate cancer. Cancer (2013) 119(16):2990–8. doi: 10.1002/cncr.28102
31. Schmid H-P, McNeal JE, Stamey TA. Observations on the doubling time of prostate cancer.The use of serial prostate-specific antigen in patients with untreated disease as a measure of increasing cancer volume. Cancer (1993) 71(6):2031–40. doi: 10.1159/000474708
32. Saad F. UPDATE – 2021 Canadian Urological Association (CUA)-Canadian Uro Oncology Group (CUOG) castration-resistant prostate cancer (CRPC) guideline: What has changed since 2019? Can Urol Assoc J (2021) 15(2):11–2. doi: 10.5489/cuaj.7160
33. Malone S, Wallis CJD, Lee-Ying R, Basappa NS, Cagiannos I, Hamilton RJ, et al. Patterns of care for non-metastatic castration-resistant prostate cancer: A population-based study. BJUI Compass (2022) 3(5):383–91. doi: 10.1002/bco2.158
34. Mottet N, Cornford P, van den Bergh R, Briers E, Eberli D, De Meerleer G, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer. Edn. presented at the EAU Annual Congress Milan. Arnhem, The Netherlands: EAU Guidelines Office. (2023). Available at: http://uroweb.org/guidelines/compil.
35. Arlen PM, Bianco F, Dahut WL, D’Amico A, Figg WD, Freedland SJ, et al. Prostate Specific Antigen Working Group guidelines on prostate specific antigen doubling time. J Urol (2008) 179(6):2181–5; discussion 2185-6. doi: 10.1016/j.juro.2008.01.099
36. Vickers AJ, Brewster SF, Velocity PSA. and doubling time in diagnosis and prognosis of prostate cancer. Br J Med Surg Urol (2012) 5(4):162–8. doi: 10.1016/j.bjmsu.2011.08.006
37. O’Brien MF, Cronin AM, Fearn PA, Smith B, Stasi J, Guillonneau B, et al. Pretreatment prostate-specific antigen (PSA) velocity and doubling time are associated with outcome but neither improves prediction of outcome beyond pretreatment PSA alone in patients treated with radical prostatectomy. J Clin Oncol (2009) 27(22):3591–7. doi: 10.1200/JCO.2008.19.9794
38. Liede A, Arellano J, Hechmati G, Bennett B, Wong S. International prevalence of nonmetastatic (M0) castration-resistant prostate cancer (CRPC). J Clin Oncol (2013) 31(15_suppl):e16052–2. doi: 10.1200/jco.2013.31.15_suppl.e16052
39. Smith MR, Saad F, Oudard S, Shore N, Fizazi K, Sieber P, et al. Denosumab and bone metastasis–free survival in men with nonmetastatic castration-resistant prostate cancer: exploratory analyses by baseline prostate-specific antigen doubling time. J Clin Oncol (2013) 31(30):3800–6. doi: 10.1200/JCO.2012.44.6716
40. Smith MR, Cook R, Lee K-A, Nelson JB. Disease and host characteristics as predictors of time to first bone metastasis and death in men with progressive castration-resistant nonmetastatic prostate cancer. Cancer (2011) 117(10):2077–85. doi: 10.1002/cncr.25762
41. Karantanos T, Corn PG, Thompson TC. Prostate cancer progression after androgen deprivation therapy: mechanisms of castrate resistance and novel therapeutic approaches. Oncogene (2013) 32(49):5501–11. doi: 10.1038/onc.2013.206
42. Fendler WP, Weber M, Iravani A, Hofman MS, Calais J, Czernin J, et al. Prostate-specific membrane antigen ligand positron emission tomography in men with nonmetastatic castration-resistant prostate cancer. Clin Cancer Res (2019) 25(24):7448–54. doi: 10.1158/1078-0432.CCR-19-1050
43. Fourquet A, Aveline C, Cussenot O, Créhange G, Montravers F, Talbot J-N, et al. 68Ga-PSMA-11 PET/CT in restaging castration-resistant nonmetastatic prostate cancer: detection rate, impact on patients’ disease management and adequacy of impact. Sci Rep (2020) 10(1):2104. doi: 10.1038/s41598-020-58975-8
44. Miyake H, Watanabe K, Matsushita Y, Watanabe H, Tamura K, Motoyama D, et al. Assessment of factors predicting disease progression in Japanese patients with non-metastatic castration-resistant prostate cancer. Anticancer Res (2020) 40(2):1101–6. doi: 10.21873/anticanres.14049
45. Moreira DM, Howard LE, Sourbeer KN, Amarasekara HS, Chow LC, Cockrell DC, et al. Predictors of time to metastasis in castration-resistant prostate cancer. Urology (2016) 96:171–6. doi: 10.1016/j.urology.2016.06.011
46. Howard LE, Moreira DM, De Hoedt A, Aronson WJ, Kane CJ, Amling CL, et al. Thresholds for PSA doubling time in men with non-metastatic castration-resistant prostate cancer. BJU Int (2017) 120(5B):E80–6. doi: 10.1111/bju.13856
47. Scher HI, Solo K, Valant J, Todd MB, Mehra M. Prevalence of prostate cancer clinical states and mortality in the United States: estimates using a dynamic progression model. Filleur S editor. PloS One (2015) 10(10):e0139440. doi: 10.1371/journal.pone.0139440
48. Ingrosso G, Bottero M, Becherini C, Caini S, Alì E, Lancia A, et al. A systematic review and meta-analysis on non-metastatic castration resistant prostate cancer: The radiation oncologist’s perspective. Semin Oncol (2022) 49(5):409–18. doi: 10.1053/j.seminoncol.2022.09.005
49. Suzuki H, Okihara K, Miyake H, Fujisawa M, Miyoshi S, Matsumoto T, et al. Alternative nonsteroidal antiandrogen therapy for advanced prostate cancer that relapsed after initial maximum androgen blockade. J Urol (2008) 180(3):921–7. doi: 10.1016/j.juro.2008.05.045
50. Lodde M, Lacombe L, Fradet Y. Salvage therapy with bicalutamide 150 mg in nonmetastatic castration-resistant prostate cancer. Urology (2010) 76(5):1189–93. doi: 10.1016/j.urology.2009.12.057
51. Sartor AO, Tangen CM, Hussain MHA, Eisenberger MA, Parab M, Fontana JA, et al. Antiandrogen withdrawal in castrate-refractory prostate cancer. Cancer (2008) 112(11):2393–400. doi: 10.1002/cncr.23473
52. Cattrini C, Caffo O, De Giorgi U, Mennitto A, Gennari A, Olmos D, et al. Apalutamide, darolutamide and enzalutamide for nonmetastatic castration-resistant prostate cancer (nmCRPC): A critical review. Cancers (Basel) (2022) 14(7):1792. doi: 10.3390/cancers14071792
53. Smith MR, Saad F, Chowdhury S, Oudard S, Hadaschik BA, Graff JN, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med (2018) 378(15):1408–18. doi: 10.1056/NEJMoa1715546
54. Fizazi K, Shore N, Tammela TL, Ulys A, Vjaters E, Polyakov S, et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med (2019) 380(13):1235–46. doi: 10.1056/NEJMoa1815671
55. Hussain M, Fizazi K, Saad F, Rathenborg P, Shore N, Ferreira U, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med (2018) 378(26):2465–74. doi: 10.1056/NEJMoa1800536
56. Smith MR, Saad F, Chowdhury S, Oudard S, Hadaschik BA, Graff JN, et al. Apalutamide and overall survival in prostate cancer. Eur Urol (2021) 79(1):150–8. doi: 10.1016/j.eururo.2020.08.011
57. Sternberg CN, Fizazi K, Saad F, Shore ND, De Giorgi U, Penson DF, et al. Enzalutamide and survival in nonmetastatic, castration-resistant prostate cancer. N Engl J Med (2020) 382(23):2197–206. doi: 10.1056/NEJMoa2003892
58. Fizazi K, Shore N, Tammela TL, Ulys A, Vjaters E, Polyakov S, et al. Nonmetastatic, castration-resistant prostate cancer and survival with darolutamide. N Engl J Med (2020) 383(11):1040–9. doi: 10.1056/NEJMoa2001342
59. Schaeffer E, Srinivas S, Antonarakis ES, Armstrong AJ, Bekelman JE, Cheng H, et al. NCCN guidelines insights: prostate cancer, version 1.2021. J Natl Compr Cancer Netw (2021) 19(2):134–43. doi: 10.6004/jnccn.2021.0008
60. Smith MR, Saad F, Shore ND, Oudard S, Miller K, Tombal B, et al. Effect of denosumab on prolonging bone-metastasis-free survival (BMFS) in men with nonmetastatic castrate-resistant prostate cancer (CRPC) presenting with aggressive PSA kinetics. J Clin Oncol (2012) 30(5_suppl):6–6. doi: 10.1200/jco.2012.30.5_suppl.6
61. Mori A, Hashimoto K, Koroki Y, Wu DB-C, Masumori N. The correlation between metastasis-free survival and overall survival in non-metastatic castration resistant prostate cancer patients from the Medical Data Vision claims database in Japan. Curr Med Res Opin (2019) 35(10):1745–50. doi: 10.1080/03007995.2019.1619543
62. Tombal B. Non-metastatic CRPC and asymptomatic metastatic CRPC: which treatment for which patient? Ann Oncol (2012) 23:x251–8. doi: 10.1093/annonc/mds325
63. Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA (1999) 281(17):1591. doi: 10.1001/jama.281.17.1591
64. Rodriguez-Vida A, Rodríguez-Alonso A, Useros-Rodríguez E, Lopez-Campos F, Amor-Carro O, Arribas-Ruiz A, et al. Impact of new systemic therapies in overall survival in non-metastatic castration resistant prostate cancer: systematic review and meta-analysis. Clin Genitourin Cancer (2022) 20(2):197.e1–197.e10. doi: 10.1016/j.clgc.2021.11.008
65. Van den Broeck T, van den Bergh RCN, Briers E, Cornford P, Cumberbatch M, Tilki D, et al. Biochemical recurrence in prostate cancer: the European association of urology prostate cancer guidelines panel recommendations. Eur Urol Focus (2020) 6(2):231–4. doi: 10.1016/j.euf.2019.06.004
Keywords: high-risk, identification, non-metastatic castration-resistant prostate cancer, prostate-specific antigen, prostate-specific antigen doubling time, standardization
Citation: Rosinha A, Rabaça C, Calais F, Pinto JM, Barreira JV, Fernandes R, Ramos R, Fialho AC and Palma dos Reis J (2024) Improving the identification of high-risk non-metastatic castration-resistant prostate cancer patients in clinical practice. Front. Oncol. 13:1266369. doi: 10.3389/fonc.2023.1266369
Received: 24 July 2023; Accepted: 25 September 2023;
Published: 23 January 2024.
Edited by:
Liang Cheng, Brown University, United StatesReviewed by:
Kazuhiro Yoshimura, Independent Researcher, Osaka, JapanCopyright © 2024 Rosinha, Rabaça, Calais, Pinto, Barreira, Fernandes, Ramos, Fialho and Palma dos Reis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Palma dos Reis, anBhbG1hcmVpc0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.