 Tomoya Yokota1*
Tomoya Yokota1* Takashi Mukaigawa2Yoshichika Yasunaga3Hirofumi Ogawa4Tsuyoshi Onoe4Takashi Yurikusa5Aiko Yamashita6
Takashi Mukaigawa2Yoshichika Yasunaga3Hirofumi Ogawa4Tsuyoshi Onoe4Takashi Yurikusa5Aiko Yamashita6- 1Division of Gastrointestinal Oncology, Shizuoka Cancer Center, Shizuoka, Japan
- 2Division of Head and Neck Surgery, Shizuoka Cancer Center, Shizuoka, Japan
- 3Division of Plastic and Reconstructive Surgery, Shizuoka Cancer Center, Shizuoka, Japan
- 4Division of Radiation Oncology, Shizuoka Cancer Center, Shizuoka, Japan
- 5Division of Dentistry and Oral Surgery, Shizuoka Cancer Center, Shizuoka, Japan
- 6Division of Nutrition, Shizuoka Cancer Center, Shizuoka, Japan
Head and neck cancer (HNC) treatment is becoming increasingly multidisciplinary, and patient characteristics vary. Therefore, a multidisciplinary tumor board (MTB) is essential in clinical practice. This review provides insights into the benefits and tips for improving head and neck MTB from the perspective of medical oncologists. The MTB is a platform to discuss the optimal application of the standard of care to each case, reach a consensus, and establish a recommendation to support patients’ decision-making. A productive and educational MTB also provides an opportunity to share information on ongoing clinical trials with physicians. Case presentations should be systematic to discuss all new and challenging cases before, during, and after the treatment. Human resource development, particularly of head and neck medical oncologists, is crucial. The type of multidisciplinary network between medical staff and the extent of patient intervention differs among MTB teams. Subsequently, a virtual MTB can establish a medical network between institutions that will contribute to the equalization and centralization of head and neck oncologic care.
1 Introduction
Treatment targets and strategies for head and neck cancer (HNC) are becoming more diversified and complicated. Indeed, clinicians need to consider the general condition, tumor staging, comorbidities, current and previous therapies, and patient preferences to ensure optimal cancer care for each patient. Therefore, a multidisciplinary approach is crucial in HNC care.
The National Cancer Institute (NCI) defines a multidisciplinary tumor board (MTB) as a treatment planning approach in which a group of health-care professionals, who are experts in different specialties, review and discuss the medical condition and treatment options of patients (1). MTB are now conducted worldwide for the management of patients with various cancers. A review by Fleissig et al. reported the effectiveness of MTB in terms of better team dynamics, communication, and educational opportunities for health care professionals, improved patient satisfaction, and improved clinical outcomes for patients considered by MTB versus individual care (2). Furthermore, a study revealed that a review by MTB at an NCI-designated cancer center has a diagnostic impact for many patients with breast cancer (3).
Clinical practice in HNC may differ by country owing to the reimbursement system, socioeconomic situation, and culture. For instance, HNC practice in Japan has long been led by otorhinolaryngologists, head and neck surgeons, and oral and maxillofacial surgeons. Japanese physicians hesitated to extrapolate evidence from Western countries to their practice, particularly in HNC pharmacotherapy. Since the 2000s, pharmacotherapy has been recognized as an independent subspecialty of cancer treatment in Japan, owing to its complexity and evolution. With the increasing need for knowledgeable and experienced HNC medical oncologists, multidisciplinary approach through MTB has been considered best practice in the care of HNC.
Here, we reviewed the benefits of MTB in the clinical practice of HNC from the perspective of medical oncologists. We then discussed suggestions for implementing a productive MTB. Finally, we addressed MTB concerns that require improvement and future directions.
2 The importance of MTB in the clinical practice of HNC
A recent meta-analysis demonstrated that the MTB improved cancer evaluation processes and survival across multiple subtypes (4). Notably, one study demonstrated that treating squamous cell carcinoma of the head and neck (SCCHN) via a multidisciplinary team improved survival (5). Furthermore, the Spanish Society for Head and Neck Cancer elaborated expert consensus on the multidisciplinary approach for SCCHN, and concluded that MTB is essential for achieving the best results, not only in terms of outcome, but also in terms of organ-function preservation and quality of life (6, 7).
HNC treatment is more multidisciplinary than other malignancies, because managing patients with locally advanced, recurrent, or metastatic HNC is complex. For successful HNC treatment, close cooperation among medical staff is necessary for supportive care of mucositis, skin toxicity, and nutritional support in CRT management. Various specialties provide supportive care for individual patients; thus, MTB offers an opportunity to share patient information among medical staff. Furthermore, expertise is required for its management. For instance, the development of minimally invasive surgical techniques, including transoral laser microsurgery and transoral robotic surgery (TORS), has resulted in surgery being the primary treatment for oropharyngeal cancer (8). Currently, intensity-modulated radiotherapy is more frequently used than three-dimensional conformal radiation for definitive and postoperative CRT. Proton beam and boron neutron capture therapies have also been introduced into clinical practice for HNC (9). Near-infrared photoimmunotherapy targets the EGFR and is a novel cancer phototherapy molecule (10). Furthermore, molecular targeting agents such as anti-EGFR antibodies, immune checkpoint inhibitors, tyrosine kinase inhibitors (TKIs), and classical cytotoxic agents are available for HNC treatment. In practice, it is challenging for recent clinicians to make therapeutic decisions and manage patients within an organ-specific team. Thus, MTB discussion is crucial in assessing the indications for each treatment modality and making a consensus decision.
HNC prevalence in geriatric patients is increasing (11–13), and most cases are associated with heavy smoking and drinking habits. Therefore, patients with HNC are often diagnosed with cardiovascular or cerebrovascular diseases, chronic obstructive pulmonary disease, diabetes, and renal impairment, which reduces their performance status. In MTB discussions, patient comorbidities and disease characteristics should guide the preferred treatment option.
Taken together, MTB is the best setting for such medical staff interactions.
3 Composition of HNC-MTB member
HNC-MTB membership varies depending on the institution. Specialists in treatment modalities, such as head and neck surgeons, otorhinolaryngologists, radiation oncologists, plastic surgeons, and medical oncologists, primarily comprise MTBs. Advice from diagnostic radiologists and pathologists helped us with the initial staging, histopathological diagnosis, and histological examination of the surgical specimens. In cases of skull base surgery, eye tumors, and malignant melanoma of the head and neck, neurosurgeons, ophthalmologists, and dermatologists may be included in the MTB. In addition to medical doctors, MTB membership is frequently expanded to include dentists, dental hygienists, physical therapists, dieticians, nurses, pharmacists, and social workers who provide supportive care. Furthermore, medical students’ participation should be encouraged because participating in the MTB is an oncology practice useful for their education. Head and neck surgeons of organ-specific divisions are often selected as the chairperson in the MTB. However, rotation may be considered.
4 MTB benefits from the perspective of medical oncologists
4.1 Establishing collaboration among medical staff in multidisciplinary cancer treatment
MTB helps to identify high-risk patients after surgery and to discuss on indications for postoperative CRT, induction or neoadjuvant chemotherapy, and optimal supportive care approaches to reduce treatment-related morbidity (14). Advanced tongue cancer treatment is an example of a multidisciplinary approach with the collaboration of medical oncologists, radiation oncologists, radiologists, head and neck surgeons, and reconstructive surgeons in HNC. This synergy enables the prompt development of an effective treatment plan for each patient in a series of glossectomies, tongue reconstruction, percutaneous endoscopic gastrostomy, and postoperative CRT (15). Furthermore, dieticians, physical therapists, dentists, and dental hygienists provide nutritional support (16, 17), rehabilitation of chewing ability and oral intake, oral care, and follow-up of radiotherapy-related toxicities, such as osteoradionecrosis, to maintain patients’ quality of life (QOL).
Medical oncologists are general physicians in cancer care who communicate closely with patients and their families. Medical oncologists are pivotal, particularly in HNC pharmacotherapy; however, they should also consider local and systemic therapies in multimodal combination and sequencing (18). Consequently, they need to be able to negotiate with other specialists as coordinators appropriately. For instance, surgical resection or palliative radiation may be required to manage locoregional diseases, even during palliative chemotherapy for recurrent or metastatic (RM)-SCCHN. In head and neck emergencies, such as tumor bleeding, infection, and airway obstruction, early referral to a head and neck surgeon is recommended. Thus, head and neck medical oncologists should always consider diverse treatment strategies.
Esophageal cancer and head and neck cancers are frequently observed simultaneously (19–21); however, their treatment strategies are often complex and challenging. The MTB, in which gastrointestinal oncologists participate, is ideal for discussing how to approach each cancer—simultaneously or sequentially. The treatment strategies include synchronous resection of both cancers, synchronous CRT for both cancers, staged resection and CRT (22, 23), or induction chemotherapy for each cancer (24). These options were selected per case based on tumor staging, invasiveness, complications, curability, and QOL, such as swallowing function. Treating multiple synchronous cancers allows medical oncologists to demonstrate their tumor-agnostic treatment skills.
4.2 Improvement of pharmacotherapy quality―checking the complex and diverse pharmacotherapy system
Pharmacotherapy is an important treatment modality for patients with HNC. CDDP is essential in HNC treatment, and CDDP-based concurrent CRT confers a survival benefit and laryngeal preservation in locally advanced (LA) SCCHN over radiotherapy alone (25). Treatment with cetuximab and immune checkpoint inhibitors improves the prognosis of patients with RM-SCCHN. Multitarget and selective TKIs are used for treating unresectable thyroid cancer (26–28). Thus, medical oncologists play roles in determining pharmacotherapy indications and fully and safely utilizing these agents.
Since HNC patients are often geriatrics and typically have several comorbidities, standard therapy is applied for a limited number of patients in real-world clinical practices. For instance, CDDP administration is associated with toxicities and serious adverse events in elderly patients or those with cardiac, renal, or neurogenic dysfunction. Therefore, surgeons and radiation oncologists often select radiotherapy alone for patients with LA-SCCHN. With effective communication among medical oncologists, surgeons, and radiation oncologists, MTB members may propose alternative treatment options to reduce or prevent the toxicity of high-dose CDDP-based CRT, including CDDP dose modification, modified administration scheduling, or use of alternative drugs based on individual organ function (29).
Notably, personalized treatment strategies should be proposed based on the risk-benefit ratio of each treatment option for patients ineligible for standard care. The following challenges may be discussed by the MTB for patients for whom the optimal standard care is unsuitable (Table 1):
1) Definitive or postoperative CRT for patients for whom CDDP is unsuitable.
2) Induction chemotherapy for patients with LA-SCCHN with high-risk disease or those for whom organ preservation is the goal but are ineligible for the docetaxel plus CDDP and 5-fluorouracil regimen.
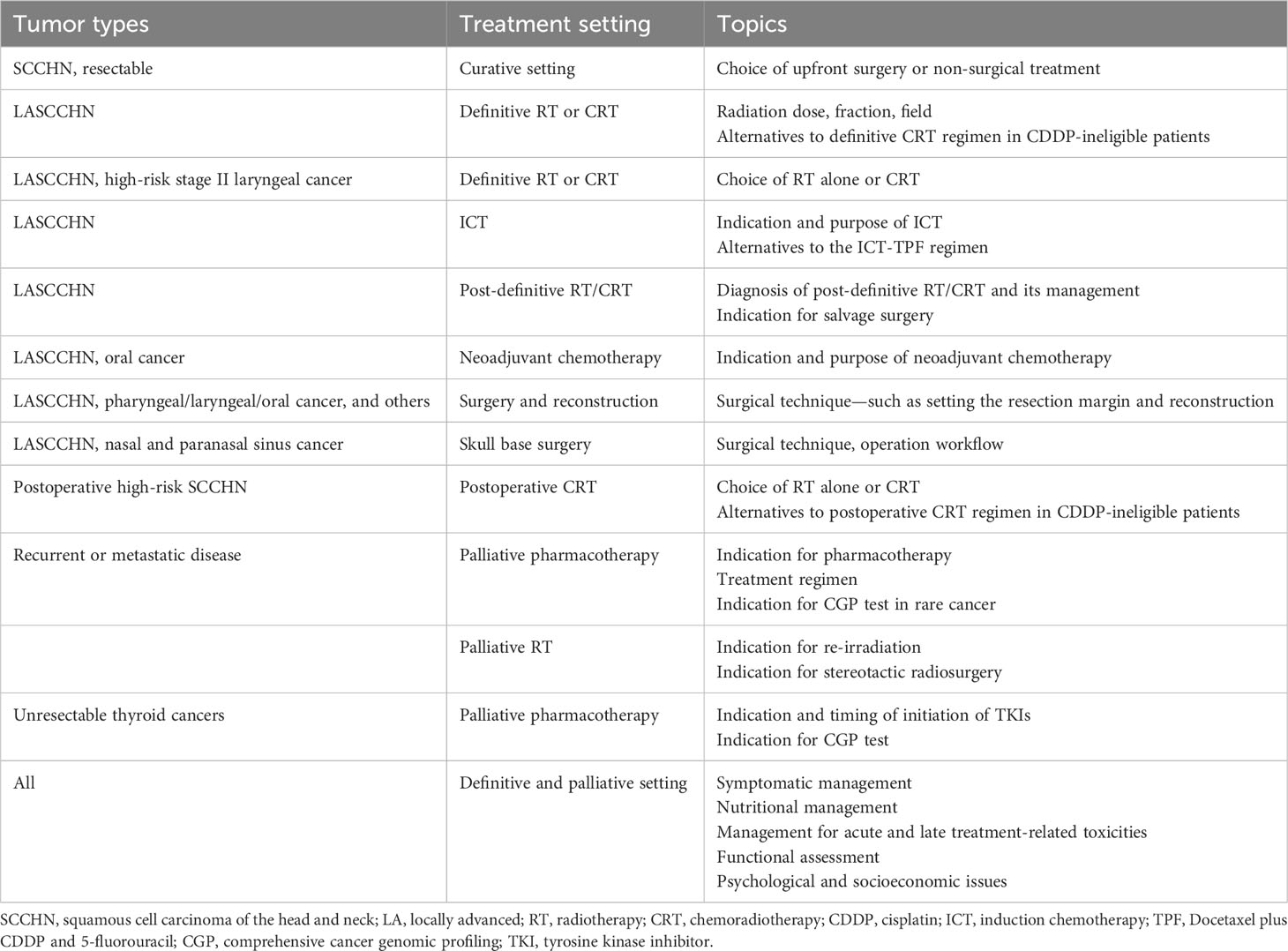
Table 1 Issues to be discussed in head and neck MTB.
4.3 Establishing a consensus to support patients’ decision-making
Some patients with HNC need support in decision-making regarding treatment modalities and nutritional support. For instance, CRT is preferred for young patients with LA-SCCHN who wish to preserve their organs; however, total laryngectomy is often performed in elderly patients at high risk of aspiration pneumonia induced by definitive CRT. The patient can decide whether to undergo laryngectomy or CRT; however, medical support is essential for decision-making directly related to survival outcomes and QOL, such as eating, swallowing, and voice functions. Rather than always leaving the choice of treatment to the patient and family, establishing a consensus on the recommended treatment by the MTB and guiding the patient in decision-making are fundamental.
4.4 Sharing information on ongoing clinical trials
High-volume centers are often invited to company- and physician-initiated clinical trials in head and neck oncology. These institutions are responsible for participating in clinical trials. Head and neck surgeons and otorhinolaryngologists often make primary contact with new patients with HNC. The MTB shares information with these divisions on ongoing clinical trials and announces the recruitment of candidates regularly.
5 Tips for implementing a productive MTB
5.1 To optimally present all new cases
All new patients should be presented and examined by multidisciplinary specialists on the MTB, regardless of planning their initial treatment strategies, such as upfront surgery, radiotherapy, or endoscopic resection, for early-stage cancer because alternative treatment options may be proposed. The approval in the MTB should be documented.
Cases should be sequentially presented based on the categorization from the perspective of each medical department. Thus, all cases can be systematically included in the agenda. The categorization may include the following examples (Table 1):
1) For cases mainly treated with surgery with or without reconstruction, surgical techniques, such as setting the resection margin and reconstruction, are discussed among surgeons. Neurosurgeons and ophthalmologists also participate in discussions on skull base surgery for nasal and paranasal sinus cancers.
2) The dose, fraction, field, and palliative or definitive settings are determined for cases primarily treated with radiation. Indications for stereotactic radiosurgery of metastatic lung lesions and re-irradiation are also discussed.
3) New cases that require multimodal treatment.
4) Challenging cases during or after treatment (Section 4.2)
Head and neck medical oncologists should have the following discussions (Table 1).
1) Upfront surgery or non-surgical treatment in resectable laryngeal and pharyngeal cancers
2) Indications for induction chemotherapy before CRT and its purpose, such as survival improvement with a distant control and laryngeal preservation
3) Indication for neoadjuvant chemotherapy before surgery for oral cancer (30)
4) Definitive radiotherapy alone or CRT for high-risk stage II laryngeal cancer (31)
5) Adjuvant CRT or radiotherapy alone for postoperative high-risk SCCHN
6) Pharmacotherapy indication for recurrent and metastatic disease
7) Risks and benefits of re-irradiation for recurrent diseases
8) TKI initiation time for thyroid cancer
9) Indication for a comprehensive genomic profiling test for rare cancer
5.2 To discuss challenging cases during or after treatment
In addition to all new HNC cases, prompt information sharing on challenging cases within the MTB is necessary during or after treatment with surgery, radiation, or chemotherapy (Table 1). The patients tolerate the standard of care; however, the subsequent treatment course for each individual varies. Therefore, irregular adverse events may occur during the treatment.
For instance, the MTB can reach a consensus on posttreatment diagnosis and management after definitive CRT, enabling us to perform additional diagnostic modalities, such as free needle biopsy, positron emission tomography, or observation. Medical oncologists find it challenging to resolve anatomical and radiological diagnostic issues; therefore, asking head and neck surgeons and diagnostic radiologists for their opinions on MTB helps. Furthermore, determining the indications for salvage surgery for residual disease after CRT is possible. MTB can also confirm whether patients with RM-SCCHN have indications for palliative RT aimed at locoregional control (Table 1).
5.3 Discussion on an individual case basis using evidence
Standards of care and clinical practice guidelines are established based on evidence from clinical trial data. Therefore, determining a treatment plan for patients without these factors is impossible. First, all physicians involved in treating HNC should understand the updated guidelines.
However, MTB is responsible for discussing the preferred treatment strategy on an individual case basis, using evidence and guidelines. The National Comprehensive Cancer Network guidelines provide recommendations for the appropriate care of approximately 95% of patients (32). However, administering only standard treatment to each case is not feasible. Physicians should recognize that the patient characteristics in clinical trials do not completely reflect those in clinical practice. Most patients with HNC cannot be completely treated according to guidelines alone owing to various factors such as organ dysfunction, comorbidities, multiple cancers, and socioeconomic issues such as alcohol dependence, living without relatives, and being on welfare. Unfortunately, these patients are often declared untreatable and treated out of pocket because of the unavailability of standard care or a lack of evidence. Ironically, this may be the disadvantage of guideline supremacy. Evidence derived from clinical trials and standard treatments is essential; however, sufficient evidence to manage all patients with HNC with varying pathophysiology is not available. Therefore, individual patient conditions should be considered in MTB when applying these recommendations. Furthermore, patients’ requests to their healthcare providers should be provided according to their diverse values.
Thus, the MTB is a forum for discussing the appropriate assessment and response to each patient’s condition based on their physical and social needs rather than solely relying on evidence (33).
5.4 To create a relaxed atmosphere in MTB
MTB educates medical students, residents, and fellowship-trained young doctors; thus, they should regularly present cases and actively exchange opinions from the standpoint of their respective specialties. However, because medical staff with different positions and occupations gather at the MTB, young doctors hesitate to express their opinions. Therefore, creating a relaxed atmosphere where participants can freely speak on various issues may create a high-quality democratic MTB.
6 Issues to be solved in HNC multidisciplinary team
Human resource development is critical. Recently, medical oncologists with backgrounds in head and neck surgery and otorhinolaryngology have been trained. However, the number of head and neck medical oncologists remains small, and a large regional disparity exists. HNC is a highly specialized field; however, many aspects are to be learned from other fields, such as gastrointestinal and respiratory oncology. Therefore, organ-agnostic training programs for head and neck medical oncologists should be promoted in university hospitals and cancer centers.
Attending physicians are central to patient management as leading physicians (Figure 1). The attending physician for patients undergoing non-surgical treatment in the MTB team may vary depending on the institution and region. Medical oncologists are involved in non-surgical treatment as attending physicians in the EU, the USA, and high-volume centers in Japan. Head and neck surgeons, otorhinolaryngologists, and radiation oncologists are in general hospitals in Asia-Pacific countries/regions because of the limited number of head and neck medical oncologists.
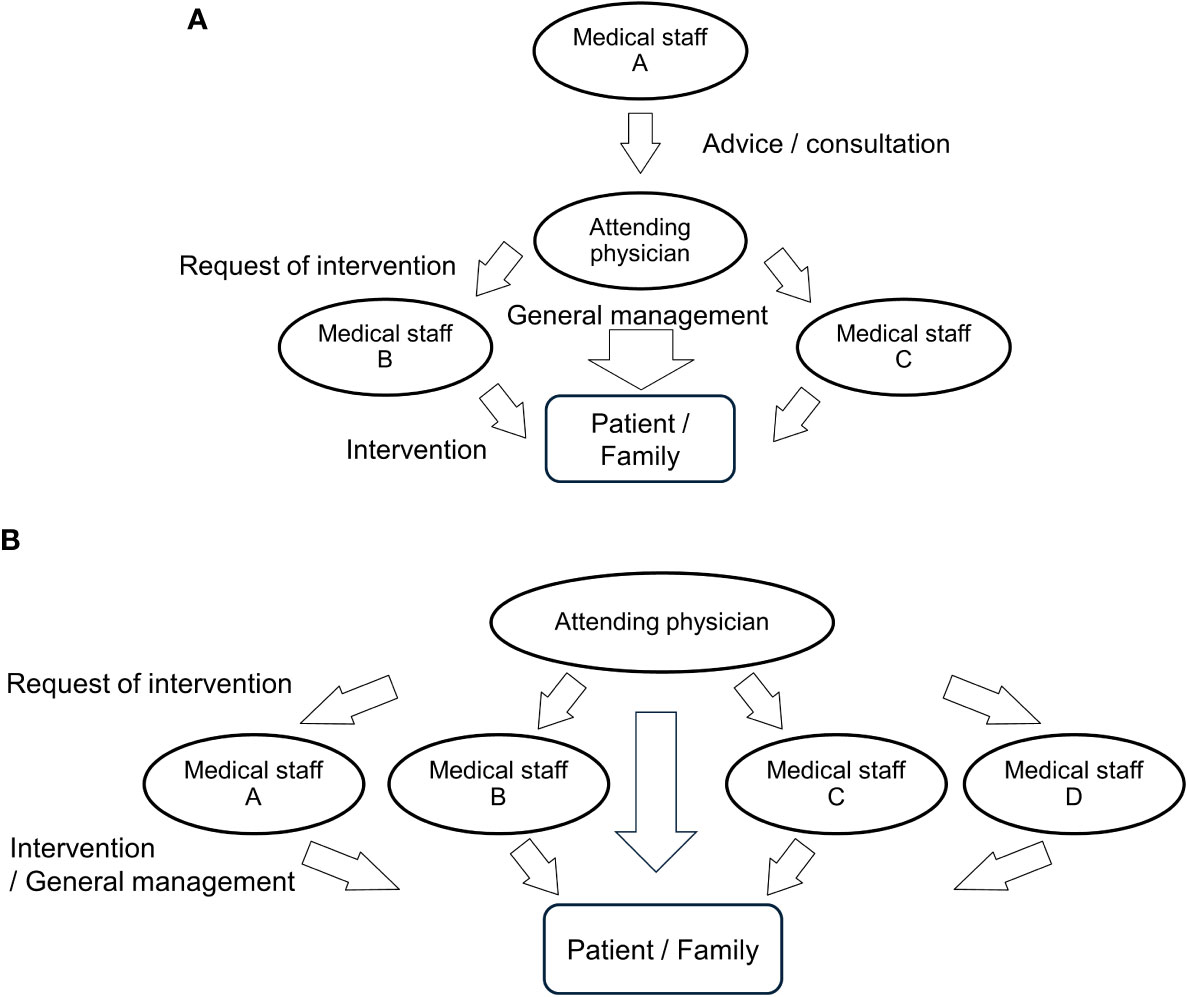
Figure 1 Type of multidisciplinary network among medical staff. The type of multidisciplinary network among medical staff and the extent of patient intervention differ among MTB teams. (A) Attending physicians are in charge of general management and communicate closely with patients. Staff A provides the attending physician with advice but lacks direct contact with patients. Medical staff B and C work on their treatment modalities at the request of the attending physician; however, they are not as involved in general management as attending physicians. (B) All staff members are involved in patient management, including treatment modalities and general management.
Non-attending physicians in MTBs tend to focus only on the treatment modalities of their specialties, such as radiation therapy, pharmacotherapy, reconstruction, and rehabilitation. Thus, they are undertaking only one part of the multimodal treatments. However, the attending physician oversees various patients’ management for general medical care and supportive and socioeconomical care (Figure 1). For instance, in treating CRT, the attending physician is involved in obtaining informed consent, managing systemic care, administering all medications, observing acute and late radiotherapy-related adverse events, emergency hospitalization, medical insurance documentation, and communication with a home doctor. However, all these responsibilities are burdensome for one physician. Approximately 56% of oncologists report an episode of emotional stress in caring for cancer patients, known as burnout, at some stage of their careers (34).
Therefore, all physicians in the MTB should view patients holistically and be proactively involved in systemic management in treating their patients. One of the solutions in the limited human resources may be to rotate attending physician among the medical departments. By doing so, it would be possible to avoid concentrating the burden of patient management on a particular department. If physicians follow each other in a multidisciplinary team and promote specialization, division, and efficiency of labor, a specific department or staff members will not be exhausted, and the resultant mental relaxation of the staff will positively affect patients and their families.
7 Conclusions and future direction of the head and neck MTB
The treatment strategy for HNC is becoming more complex and multidisciplinary, and patient characteristics vary; therefore, MTB is indispensable in clinically treating HNC. The MTB discusses the optimal application of standard care on an individual case basis, through which a consensus MTB recommendation is established to support patients’ decision-making. Additionally, MTB is educational, and case presentations should be systematic.
Having faced difficulties with limited clinical resources and healthcare office availability during the COVID-19 pandemic, head and neck care coordination has changed substantially. MTB has transitioned into a remote and virtual format (35–37). Virtual communication platforms will enable the implementation of MTB within large academic medical centers and multiple satellite hospitals in the future. Virtual MTB also contributes to establishing a medical network in regions of low resource availability, enhancing decentralization of head and neck oncologic care.
Author contributions
ToY: Conceptualization, Writing – original draft, Writing – review & editing. TM: Conceptualization, Writing – review & editing. YY: Conceptualization, Writing – review & editing. HO: Conceptualization, Writing – review & editing. TO: Conceptualization, Writing – review & editing. TaY: Conceptualization, Writing – review & editing. AY: Conceptualization, Writing – review & editing.
Funding
This study was supported by the Japan Agency for Medical Research and Development (23ck0106767h0002).
Acknowledgments
We would like to thank Editage (www.editage.com) for the English language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
SCCHN, squamous cell carcinoma of the head and neck; LA, locally advanced; RT, radiotherapy; CRT, chemoradiotherapy; CDDP, cisplatin; ICT, induction chemotherapy; TPF, Docetaxel plus CDDP and 5-fluorouracil; CGP, comprehensive cancer genomic profiling; TKIs, tyrosine kinase inhibitor.
References
1. National Cancer Institute. Definition of tumor board review. Available at: http://www.cancer.gov/dictionary?cdrid_322893 (Accessed January 15, 2014).
2. Fleissig A, Jenkins V, Catt S, Fallowfield L. Multidisciplinary teams in cancer care: are they effective in the UK? Lancet Oncol (2006) 7(11):935–43. doi: 10.1016/S1470-2045(06)70940-8
3. Garcia D, Spruill LS, Irshad A, Wood J, Kepecs D, Klauber-DeMore N. The value of a second opinion for breast cancer patients referred to a national cancer institute (NCI)-designated cancer center with a multidisciplinary breast tumor board. Ann Surg Oncol (2018) 25(10):2953–7. doi: 10.1245/s10434-018-6599-y
4. Prades J, Remue E, van Hoof E, Borras JM. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy (2015) 119:464–74. doi: 10.1016/j.healthpol.2014.09.006
5. Liu JC, Kaplon A, Blackman E, Miyamoto C, Savior D, Ragin C. The impact of the multidisciplinary tumor board on head and neck cancer outcomes. Laryngoscope (2020) 130:946–50. doi: 10.1002/lary.28066
6. Mañós M, Giralt J, Rueda A, Cabrera J, Martinez-Trufero J, Marruecos J, et al. Multidisciplinary management of head and neck cancer: First expert consensus using Delphi methodology from the Spanish Society for Head and Neck Cancer (part 1). Oral Oncol (2017) 70:58–64. doi: 10.1016/j.oraloncology.2017.04.004
7. Rueda A, Giralt J, Mañós M, Lozano A, Sistiaga A, García-Miragall E, et al. Multidisciplinary management of head and neck cancer: First expert consensus using Delphi methodology from the Spanish Society for Head and Neck Cancer (part 2). Oral Oncol (2017) 70:65–72. doi: 10.1016/j.oraloncology.2017.04.005
8. Cracchiolo JR, Baxi SS, Morris LG, Ganly I, Patel SG, Cohen MA, et al. Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base. Cancer (2016) 122:1523–32. doi: 10.1002/cncr.29938
9. Jin WH, Seldon C, Butkus M, Sauerwein W, Giap HB. A review of boron neutron capture therapy: Its history and current challenges. Int J Part Ther (2022) 9:71–82. doi: 10.14338/IJPT-22-00002.1
10. Meulemans J, Delaere P, Vander Poorten V. Photodynamic therapy in head and neck cancer: Indications, outcomes, and future prospects. Curr Opin Otolaryngol Head Neck Surg (2019) 27:136–41. doi: 10.1097/MOO.0000000000000521
11. Italiano A, Ortholan C, Dassonville O, Poissonnet G, Thariat J, Benezery K, et al. Head and neck squamous cell carcinoma in patients aged > or = 80 years: Patterns of care and survival. Cancer (2008) 113:3160–8. doi: 10.1002/cncr.23931
12. Mountzios G. Optimal management of the elderly patient with head and neck cancer: Issues regarding surgery, irradiation and chemotherapy. World J Clin Oncol (2015) 6:7–15. doi: 10.5306/wjco.v6.i1.7
13. Sikora AG, Toniolo P, DeLacure MD. The changing demographics of head and neck squamous cell carcinoma in the United States. Laryngoscope (2004) 114:1915–23. doi: 10.1097/01.mlg.0000147920.66486.bc
14. Liao CT, Kang CJ, Lee LY, Hsueh C, Lin CY, Fan KH, et al. Association between multidisciplinary team care approach and survival rates in patients with oral cavity squamous cell carcinoma. Head Neck (2016) 38 Suppl 1:E1544–53. doi: 10.1002/hed.24276
15. Yokota T, Iida Y, Ogawa H, Kamijo T, Onozawa Y, Todaka A, et al. Prognostic factors and multidisciplinary postoperative chemoradiotherapy for clinical T4a tongue cancer. Oncology (2016) 91:78–84. doi: 10.1159/000446439
16. Garg S, Yoo J, Winquist E. Nutritional support for head and neck cancer patients receiving radiotherapy: a systematic review. Support Care Cancer (2010) 18:667–77. doi: 10.1007/s00520-009-0686-3
17. Paccagnella A, Morello M, Da Mosto MC, Baruffi C, Marcon ML, Gava A, et al. Early nutritional intervention improves treatment tolerance and outcomes in head and neck cancer patients undergoing concurrent chemoradiotherapy. Support Care Cancer (2010) 18:837–45. doi: 10.1007/s00520-009-0717-0
18. Nishimura A, Yokota T, Hamauchi S, Onozawa Y, Shirasu H, Kawabata T, et al. Incurable locoregional disease is a strong poor prognostic factor in recurrent or metastatic squamous cell carcinoma of the head and neck. Int J Clin Oncol (2021) 26:1822–30. doi: 10.1007/s10147-021-01965-1
19. Abemayor E, Moore DM, Hanson DG. Identification of synchronous esophageal tumors in patients with head and neck cancer. J Surg Oncol (1988) 38:94–6. doi: 10.1002/jso.2930380207
20. Kuwano H, Morita M, Tsutsui S, Kido Y, Mori M, Sugimachi K. Comparison of characteristics of esophageal squamous cell carcinoma associated with head and neck cancer and those with gastric cancer. J Surg Oncol (1991) 46:107–9. doi: 10.1002/jso.2930460208
21. Morita M, Kuwano H, Ohno S, Sugimachi K, Seo Y, Tomoda H, et al. Multiple occurrence of carcinoma in the upper aerodigestive tract associated with esophageal cancer: Reference to smoking, drinking and family history. Int J Cancer (1994) 58:207–10. doi: 10.1002/ijc.2910580211
22. Matsumoto A, Watanabe M, Mine S, Nishida K, Shigaki H, Kawabata K, et al. Comparison of synchronous versus staged surgeries for patients with synchronous double cancers of the esophagus and head-and-neck. Dis Esophagus (2016) 30:1–6. doi: 10.1111/dote.12509
23. Matsumoto A, Watanabe M, Shigaki H, Nishida K, Mine S, Sano T, et al. Efficacy of staged treatment strategy for patients with synchronous double cancers of the esophagus and head and neck: A retrospective study. World J Surg (2016) 40:388–94. doi: 10.1007/s00268-015-3276-1
24. Okamoto T, Katada C, Komori S, Yamashita K, Miyamoto S, Kano K, et al. A retrospective study of treatment for curative synchronous double primary cancers of the head and neck and the esophagus. Auris Nasus Larynx (2018) 45:1053–60. doi: 10.1016/j.anl.2017.12.005
25. Adelstein DJ, Li Y, Adams GL, Wagner H, Kish JA, Ensley JF, et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol (2003) 21:92–8. doi: 10.1200/JCO.2003.01.008
26. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro G, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet (2019) 394:1915–28. doi: 10.1016/S0140-6736(19)32591-7
27. Ferris RL, Blumenschein G Jr., Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med (2016) 375:1856–67. doi: 10.1056/NEJMoa1602252
28. Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med (2008) 359:1116–27. doi: 10.1056/NEJMoa0802656
29. Yokota T, Hamauchi S, Shirasu H, Onozawa Y, Ogawa H, Onoe T, et al. How should we approach locally advanced squamous cell carcinoma of head and neck cancer patients ineligible for standard non-surgical treatment? Curr Oncol Rep (2020) 22:118. doi: 10.1007/s11912-020-00984-x
30. Chaukar D, Prabash K, Rane P, Patil VM, Thiagarajan S, Ghosh-Laskar S, et al. Prospective phase II open-label randomized controlled trial to compare mandibular preservation in upfront surgery with neoadjuvant chemotherapy followed by surgery in operable oral cavity cancer. J Clin Oncol (2022) 40:272–81. doi: 10.1200/JCO.21.00179
31. Hamauchi S, Yokota T, Onozawa Y, Ogawa H, Onoe T, Kamijo T, et al. Chemoradiotherapy for high-risk stage II laryngeal cancer. Int J Clin Oncol (2020) 25(9):1596–603. doi: 10.1007/s10147-020-01705-x
32. Available at: https://education.nccn.org/tumorboards#group-tabs-node-course-default5.
33. Oliveira TB, Mesía R, Falco A, Hsieh JC, Yokota T, Saada-Bouzid E, et al. Defining the needs of patients with recurrent and/or metastatic head and neck cancer: An expert opinion. Crit Rev Oncol Hematol (2021) 157:103200. doi: 10.1016/j.critrevonc.2020.103200
34. Whippen DA, Canellos GP. Burnout syndrome in the practice of oncology: Results of a random survey of 1,000 oncologists. J Clin Oncol (1991) 9:1916–20. doi: 10.1200/JCO.1991.9.10.1916
35. Amin NB, Bridgham KM, Brown JP, Moyer KF, Taylor RJ, Wolf JS, et al. Regionalization of head and neck oncology tumor boards: Perspectives of collaborating physicians. OTO Open (2023) 7:e18. doi: 10.1002/oto2.18
36. Dharmarajan H, Anderson JL, Kim S, Sridharan S, Duvvuri U, Ferris RL, et al. Transition to a virtual multidisciplinary tumor board during the COVID-19 pandemic: University of Pittsburgh experience. Head Neck (2020) 42:1310–6. doi: 10.1002/hed.26195
Keywords: head and neck oncology, medical oncologists, multidisciplinary intervention, multidisciplinary tumor board, evidence-based medicine, personalized medicine
Citation: Yokota T, Mukaigawa T, Yasunaga Y, Ogawa H, Onoe T, Yurikusa T and Yamashita A (2023) Multidisciplinary tumor board for head and neck cancer from the perspective of medical oncologists—optimizing its effectiveness. Front. Oncol. 13:1257853. doi: 10.3389/fonc.2023.1257853
Received: 13 July 2023; Accepted: 14 August 2023;
Published: 30 August 2023.
Edited by:
Nerina Denaro, IRCCS Ca ‘Granda Foundation Maggiore Policlinico Hospital, ItalyReviewed by:
Yuri Ueda, Tokyo Medical University Hospital, JapanKai Wang, Chinese Academy of Medical Sciences and Peking Union Medical College, China
Copyright © 2023 Yokota, Mukaigawa, Yasunaga, Ogawa, Onoe, Yurikusa and Yamashita. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomoya Yokota, dC55b2tvdGFAc2NjaHIuanA=