
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Oncol., 12 December 2023
Sec. Cancer Epidemiology and Prevention
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1257767
This article is part of the Research TopicInflammation and Chronic DiseaseView all 13 articles
 Justin C. Brown1,2,3,4*
Justin C. Brown1,2,3,4* Stephanie L.E. Compton1Jeffrey A. Meyerhardt5
Stephanie L.E. Compton1Jeffrey A. Meyerhardt5 Guillaume Spielmann6Shengping Yang1
Guillaume Spielmann6Shengping Yang1Background: Physical activity after surgical resection for colon cancer is associated with significantly longer disease-free survival. Inflammation is hypothesized to mediate the association between physical activity and disease-free survival in colon cancer.
Methods: In this exploratory analysis of a randomized dose-response trial, 39 colon cancer survivors who completed standard therapy were stratified by cancer stage and randomized in a 1:1:1 ratio to one of three treatment groups for 24 weeks of usual-care control, 150 min/wk of moderate-intensity aerobic exercise (low-dose), or 300 min/wk of moderate-intensity aerobic exercise (high-dose). Inflammation outcomes included high-sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL6), and soluble tumor necrosis factor-alpha receptor 2 (sTNFαR2). Mixed models for repeated measures were used to test the hypothesis that exercise was associated with dose-response reductions in inflammation; exploratory analyses examined treatment effects by cancer stage.
Results: In the overall population, aerobic exercise was not associated with dose-response reductions in hs-CRP, IL6, or sTNFαR2. Cancer stage modified the association between randomized group and hs-CRP (P=0.022) and IL6 (P<0.001) but not sTNFαR2 (P=0.39). In stage I-II disease, compared to control, exercise was not associated with inflammation outcomes. In stage III disease, compared to control, low-dose exercise reduced hs-CRP: −35.4% (95% CI: −70.1, −0.7) and IL6: −29.6% (95% CI: −58.4, −0.8) but not sTNFαR2: 2.7% (95% CI: sTNFαR2: −15.7, 21.1); high-dose exercise was not associated with inflammation outcomes in stage III disease.
Conclusion: This exploratory analysis offers preliminary data to support the hypothesis that inflammation may mediate the association between physical activity and disease-free survival in colon cancer.
Clinical trial registration: clinicaltrials.gov, identifier NCT02250053.
Physical activity after surgical resection for colon cancer is associated with a significantly longer disease-free survival (1, 2), by reducing the risk of disease recurrence in a subset of patients (3). The association between physical activity and disease-free survival is independent of known prognostic factors and occurs in a dose-response fashion, such that larger volumes of physical activity are associated with a higher probability of remaining alive and cancer-free (4). The biological mechanisms by which physical activity is associated with improved disease-free survival remain incompletely understood, but inflammation is postulated as a key mediator (5).
Inflammation activates the JAK-STAT and NF-κB signaling pathways to promote cancer cell proliferation, migration, and invasion (6). Inflammation that persists after recovery from colonic tumor resection is independently associated with shorter disease-free survival (7–9). In animal models, experimental manipulation of inflammatory pathways regulates the growth and progression of colonic tumors (10). However, data from clinical trials in colon cancer survivors are limited (11), and the effects of different exercise doses on inflammation outcomes are unknown.
We conducted an exploratory analysis to examine the effects of distinct doses of aerobic exercise using data from a trial that randomized colon cancer survivors to one of three groups for 24 weeks: usual-care control, 150 min/wk of moderate-intensity aerobic exercise (low-dose), or 300 min/wk of moderate-intensity aerobic exercise (high-dose) (12). We hypothesized that exercise would reduce inflammation in a dose-response fashion. Inflammation may correlate with colon cancer disease stage (13). Therefore, we examined if subjects with higher-stage colon cancer derive a larger anti-inflammatory benefit from exercise.
This study was a 24-week, phase II, single-center, randomized, dose-response trial. The study followed Good Clinical Practice and the ethical principles in the Declaration of Helsinki. The Institutional Review Board approved the trial protocol and informed consent document. All subjects provided informed consent and approval from their physician before completing any study activities. The study was registered on clinicaltrials.gov as NCT02250053, and detailed study methods are published (12). The prespecified primary and secondary outcomes are published (14–18). The inflammation outcomes reported here were not prespecified and were conducted for exploratory purposes to inform the design of future studies.
Subjects were eligible if they were diagnosed with histologically-proven stage I-III colon cancer, underwent surgical tumor resection, completed postoperative chemotherapy within 36 months of entering the study (if applicable), self-reported <150 min/wk of moderate- to vigorous-intensity physical activity (19), were age ≥18 years, provided written physician approval, had no additional surgery planned within the 24 week intervention period, and could walk unassisted for six minutes.
Subjects were stratified by cancer stage (I vs. II vs. III) and randomized to one of three groups: usual-care control, 150 min/wk of moderate-intensity aerobic exercise (low-dose), or 300 min/wk of moderate-intensity aerobic exercise (high-dose). Subjects were not blinded to treatment assignment. Outcome measures were obtained by assessors blinded to treatment assignment.
Subjects randomized to the low-dose or high-dose exercise groups utilized a study-provided in-home treadmill and heart rate monitor. The exercise intensity was prescribed at 50−70% of the age-predicted maximum heart rate. The low-dose and high-dose target exercise volume was 150 and 300 min/wk, respectively. Subjects were encouraged to individualize their frequency (days per week), fractionation (sessions per day), and duration (minutes per session) of exercise according to a schedule that promoted a high level of adherence to the prescribed exercise volume (17). Subjects randomized to the usual-care control group maintained their pre-study physical activity levels.
Demographic characteristics, including age, sex, and race, were self-reported. Cancer stage was obtained from the cancer registry, pathology reports, and physician records. At baseline and week 24, subjects underwent a fasting blood draw. Blood draws were performed after a minimum eight-hour fast and abstinence from alcohol consumption for 24 hours. A total of 30 mL of plasma was centrifuged, aliquoted, and stored at −80°C following standardized procedures. Circulating tumor cells were measured as previously described (15).
Inflammation measures included high-sensitivity C-reactive protein (hs-CRP), interleukin 6 (IL6), and soluble tumor necrosis factor-alpha receptor 2 (sTNFαR2). These inflammatory measures are associated with disease-free survival in colon cancer survivors (20–22). hs-CRP was measured as a marker of overall systemic inflammation (23). IL6 was measured as an activator of the JAK-STAT pathway (24). sTNFαR2 was measured as an activator of the NF-kB pathway (25). sTNFαR2 is a surrogate marker for TNFα that is more stable in plasma and less sensitive to diurnal variation (26). hs-CRP was quantified using an immunoturbidimetric assay (Roche Diagnostics). IL6 and sTNFαR2 were quantified using ultrasensitive sandwich enzyme immunoassays (R&D Systems). Baseline and week 24 samples were assayed simultaneously and in duplicate at the end of the study. Blinded quality-control samples were interspersed among cases. The median [interquartile range] time from biospecimen collection to laboratory analysis was 3.7 years [3.4, 3.8], and all samples were never previously thawed (27). The coefficients of variation for all samples were ≤8% (11).
Descriptive statistics for baseline variables include counts and proportions for categorical variables and means and standard deviations for continuous variables. Dependent variables were log-transformed in the inferential analysis to improve the distributional normality (28). The change was evaluated from baseline to follow-up in the three groups using mixed models for repeated measures. This modeling technique includes all data and accounts for the correlation between measures. Treatment effects were calculated as the treatment effect ratio, which quantifies the percent change in geometric means from baseline to week 24 (e.g., a treatment effect ratio of 0.75 indicates a 25% reduction), with 95% confidence intervals (CI). The regression models included the baseline value of the dependent variable and cancer stage (randomization stratification factor) as covariates to improve the precision of effect size estimation (29). Group-by-time interaction terms were included as fixed effects in the regression model. A test of trends with linear and nonlinear (quadratic) contrasts evaluated the presence of a dose-response relationship across randomized groups. Effect modification by cancer stage was evaluated by including a three-way interaction among cancer stage, randomized group, and time in the mixed models for repeated measures.
At randomization, cancer stage was a three-level variable (I vs. II vs.. III). However, for this analysis, subjects with stage I and II disease were combined (n=19) to provide a numeric balance to the number of subjects with stage III disease (n=20). The threshold for statistical significance for interactions was prespecified at P<0.10, because of known limitations in statistical power (30). Model fit was assessed using graphical and numeric techniques. Stata 17.0 (College Station, TX, USA) was used for all statistical analyses, and GraphPad Prism 9.4 (Boston, MA, USA) for data visualization.
Subjects were recruited and randomized between January 2015 and August 2015, with data collection ending in February 2016. The study completion rate was 97% (one subject was lost to follow-up; Supplementary Figure 1). At baseline, the age ranged from 35 to 81 years, and subjects were most often female (62%), of white race (79%), with stage III disease (51%), and treated with chemotherapy (72%; Table 1).
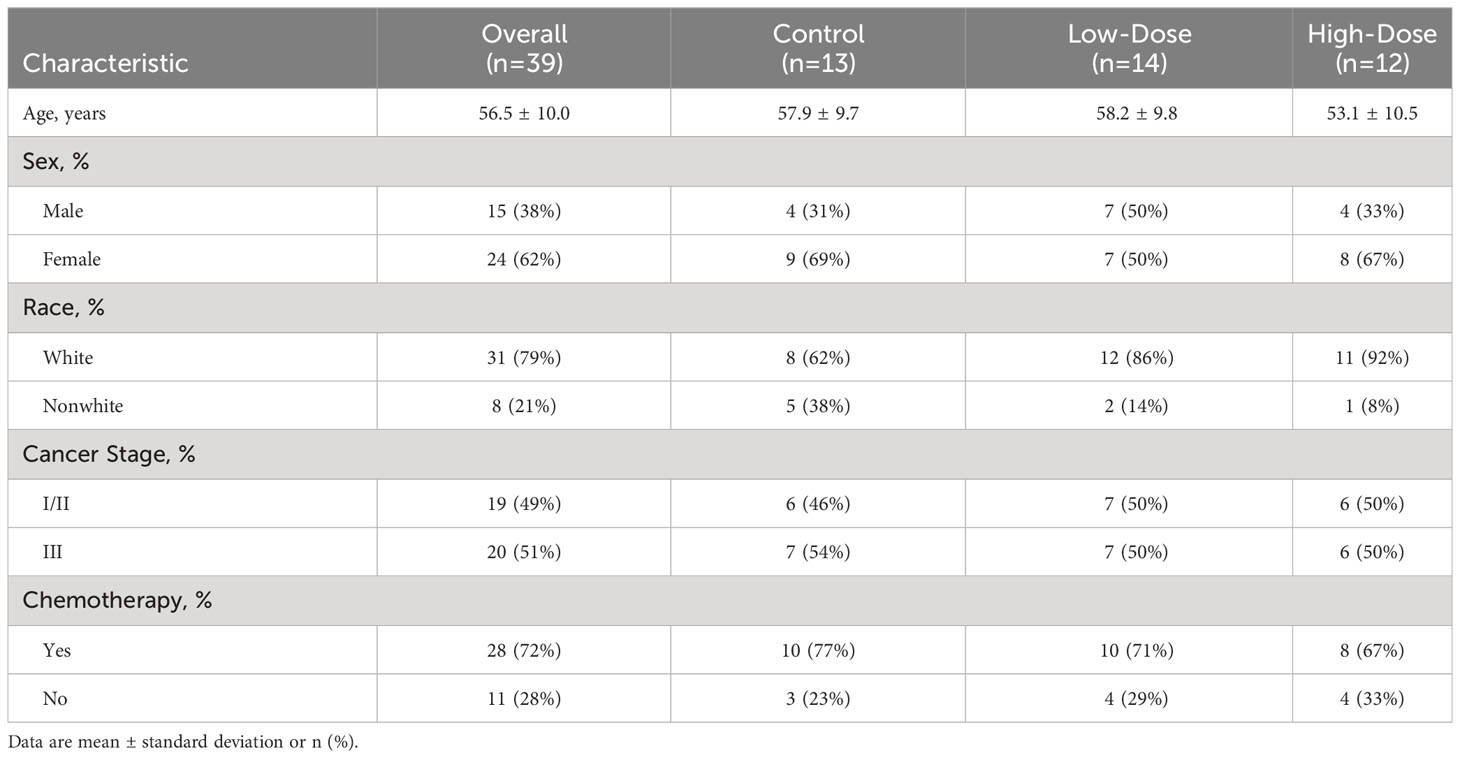
Table 1 Baseline subject characteristics overall and by randomized group.
At baseline, the mean (SD) hs-CRP was 2.53 (2.11) mg/L, IL6 was 2.07 (1.63) pg/mL, and sTNFαR2 was 2524 (840) pg/mL, indicating low to moderate inflammation. From baseline to week 24, the low-dose and high-dose groups completed an average of 141 min/wk (93% adherence) and 247 min/wk (89% adherence) of exercise, respectively. Exercise adherence ranged from 17−100% and 21−100% in the low-dose and high-dose groups, respectively. The low-dose and high-dose exercise groups averaged 3.5 and 4.3 days of exercise each week and 41.6 and 59.1 minutes per session, respectively. Detailed adherence trajectories have been reported (17).
In the overall intention-to-treat population, randomization to higher doses of aerobic exercise was not associated with dose-response reductions in hs-CRP (linear P=0.74; nonlinear P=0.41), IL6 (linear P=0.11; nonlinear P=0.77), or sTNFαR2 [(linear P=0.66; nonlinear P=0.75); Table 2].

Table 2 Change in inflammation outcomes by randomized group.
At study enrollment, subjects with stage I or II colon cancer had completed cancer-directed treatments a mean of 12.0 (5.6) months previously, and subjects with stage III colon cancer completed cancer-directed treatments a mean of 9.0 (6.1) months previously [Δ: −2.9 months (95% CI: −5.6, −0.3)]. Subjects with stage I and II colon cancer did not have different concentrations of hs-CRP (P=0.26), IL6 (P=0.74), or sTNFαR2 (P=0.44). Cancer stage modified the association between randomized group and hs-CRP (Pinteraction=0.022) and IL6 (Pinteraction<0.001) but not sTNFαR2 (Pinteraction=0.39). Exercise adherence did not differ between subjects with stage I or II versus stage III colon cancer (P=0.17).
Compared to control, randomization to low-dose or high-dose aerobic exercise was not associated with inflammation outcomes in subjects with stage I or II colon cancer (Table 3). Conversely, compared to control, randomization to low-dose aerobic exercise statistically significantly reduced hs-CRP: −35.4% (95% CI: −70.1, −0.7) and IL6: −29.6% (95% CI: −58.4, −0.8), but not sTNFαR2: 2.7% (95% CI: −15.7, 21.1) in subjects with stage III cancer, whereas randomization to high-dose aerobic exercise was not associated with a reduction in any inflammation outcome in subjects with stage III colon cancer.
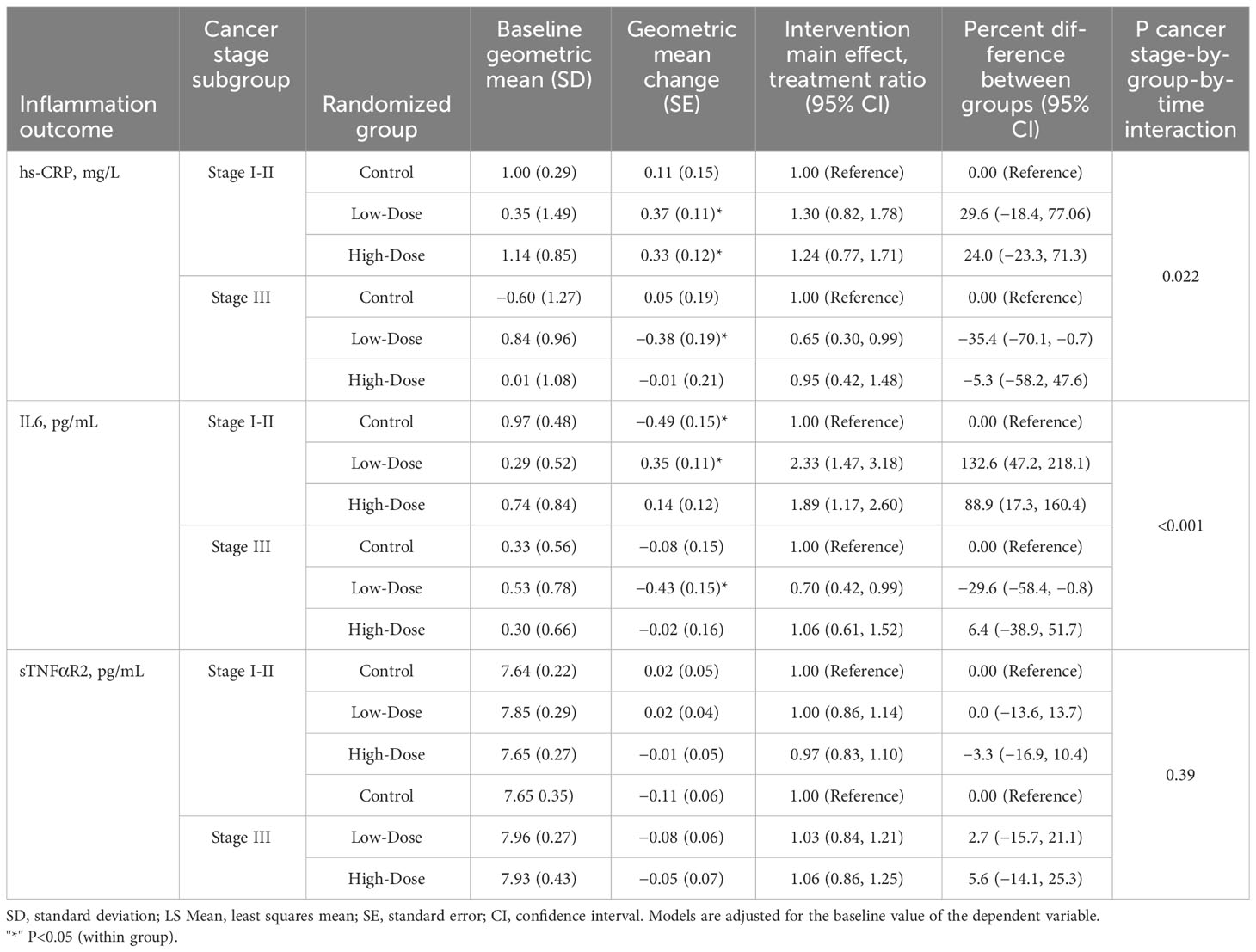
Table 3 Change in inflammation outcomes by cancer stage subgroup and randomized group.
Correlational analyses of inflammation outcomes at baseline and change from baseline to week 24 with previously reported variables are presented for hypothesis generation (Figure 1). Notably, baseline hs-CRP correlated with circulating tumor cells (r=0.43; 95% CI: 0.07, 0.68), and the change from baseline to week 24 in sTNFαR2 correlated with the change in circulating tumor cells (r=−0.44; 95% CI: −0.72, −0.04).

Figure 1 Correlational analyses of inflammation outcomes at baseline (A) and change from baseline to week 24 (B) with previously reported variables are presented for hypothesis generation hs-CRP, high sensitivity C-reactive protein; IL6, interleukin 6; sTNFαR2, soluble tumor necrosis factor alpha receptor 2; IGF-1, insulin-like growth factor 1; IGFBP-3, insulin-like growth factor binding protein 3; HOMA-IR, homeostatic model of insulin resistance; sICAM-1, soluble intercellular adhesion molecule 1; sVCAM-1, soluble vascular adhesion molecule 1; CTCs, circulating tumor cells. *P<0.05; **P<0.01; ***P<0.001.
In this exploratory analysis of insufficiently physically active colon cancer survivors with low to moderate inflammation at baseline, randomization to 150 min/wk of moderate-intensity aerobic exercise for 24 weeks reduced concentrations of hs-CRP and IL6 in those with stage III disease. Randomization to 300 min/wk of moderate-intensity aerobic exercise was not associated with any inflammation-lowering effect, nor was either dose of aerobic exercise assigned to those with stage I or II colon cancer. In correlational analyses, inflammation was associated with circulating tumor cell burden at baseline and during follow-up.
One mechanism by which physical activity is hypothesized to exert anticancer effects is by reducing inflammation within the host microenvironment (5). Our results demonstrate that 24 weeks of 150 min/wk of moderate-intensity aerobic exercise reduce hs-CRP and IL6 by 35.4% and 29.6% among stage III colon cancer survivors. In a prospective cohort study of 1,494 stage III colon cancer survivors, elevated hs-CRP and IL6 were associated with a 65% and 52% higher relative risk of disease recurrence or death, respectively (9). Our findings are consistent with the hypothesis that inflammation is a key mediator of the association between physical activity and disease-free survival in colon cancer survivors. Moreover, our results enhance the clinical relevance of experiments in tumor-bearing preclinical models that conclude inflammatory pathway blockade slows cancer cell growth and delays tumor progression (31, 32).
The results of the current analysis complement a prior trial that was conducted as part of the National Cancer Institutes (NCI) Transdisciplinary Research on Energetics and Cancer (TREC) Consortium (33). This prior trial used a 2×2 factorial design to evaluate the effect of 12 weeks of exercise or metformin on inflammation in 139 breast and colorectal cancer patients (11). Compared with control, randomization to 220 min/wk of moderate-intensity aerobic exercise statistically significantly reduced hs-CRP: −30.2% (95% CI, −50.3, −1.0) and IL6: −30.9% (95% CI, −47.3, −9.5); but did not significantly change sTNFαR2: 1.0% (95% CI, −10.4, 13.9) (11). Our results are compatible regarding the specificity of inflammatory biomarker response (e.g., hs-CRP and IL6 were lowered with exercise but not sTNFαR2) and the magnitude of biomarker response (e.g., −35.4% vs.. 30.2% for hs-CRP and −29.6% vs.. −30.9 for IL6). The absence of a statistically significant dose-response effect in the current analysis may indicate that the optimal dose of moderate-intensity aerobic exercise to reduce the studied inflammatory biomarkers in colon cancer survivors is between 150 and 220 min/wk.
The current analysis results complement what is known in healthy subjects without a history of cancer. In the Alberta Physical Activity and Breast Cancer Prevention (ALPHA) Trial, 320 postmenopausal women were randomized to 52 weeks of aerobic exercise or a usual care control group. Compared to control, randomization to 225 min/wk of moderate- to vigorous-intensity aerobic exercise statistically significantly reduced hs-CRP: −13% (95% CI: −21, −4), but did not significantly change IL6: −1% (95% CI: −8, 7) or TNFα: 0% (95% CI: −3, 4) (34). The Breast Cancer and Exercise Trial in Alberta (BETA) randomized 400 postmenopausal women to 52 weeks of 150 min/wk or 300 min/wk of aerobic exercise. Compared to 150 min/wk, randomization to 300 min/wk of moderate- to vigorous-intensity aerobic exercise, did not significantly change hs-CRP, IL6, or TNFα (35). The effects of exercise on inflammation in subjects without cancer has been summarized in a meta-analysis (36). These data in subjects without cancer are comparable to those in cancer survivors, such that the dose-response curve between exercise volume and change in inflammatory outcomes is not linear.
Our hypothesis that patients with higher-stage colon cancer derive a larger anti-inflammatory benefit from exercise was supported. Although our hypothesis was supported, subjects with stage III disease did not have more inflammation than subjects with stage I-II disease. This contrasts with prior reports that inflammation correlates with colon cancer disease stage (13). Aside from the extent of invasion through the bowel wall (T-stage) and lymph node metastases (N-stage), which are used to determine the American Joint Committee on Cancer (AJCC) overall cancer stage (37), the only baseline factor that differed between stage I-II versus stage III colon cancer survivors was the receipt of chemotherapy. However, chemotherapy per se did not modify the association between randomized groups and inflammatory outcomes. Other factors measured after randomization, such as exercise adherence, did not differ between subjects with stage I-II versus stage III disease. The biological explanation of why cancer stage modifies the association between randomized groups and inflammatory outcomes, therefore, remains uncertain. This observation will be prospectively interrogated in an ongoing randomized trial of exercise in colorectal cancer survivors (e.g., NCT03975491).
We previously reported that exercise lowers circulating tumor cells using this dataset. Over 24 weeks, statistically significant decreases in circulating tumor cells were observed in the low- and high-dose exercise groups, whereas no significant change was observed in the control group (15). Anthropometric measures, such as visceral fat, and metabolic measures, such as fasting insulin, were biological mediators of the association between exercise and reductions in circulating tumor cells (15). The current analysis suggests inflammation is a potential biological mediator of the association between exercise and reductions in circulating tumor cells. In a cross-sectional study of women with metastatic breast cancer, circulating tumor cells positively correlated with CRP (r=0.22; P=0.02) and IL6 (r=0.25; P=0.01) (38). Changes in circulating tumor cells after surgery and chemotherapy are prognostic of disease-free survival in colorectal cancer survivors (39, 40). Results from an ongoing randomized clinical trial (e.g., NCT03975491) will clarify the interplay of inflammation with circulating tumor cells and circulating tumor DNA to offer unique insight into mechanisms of treatment benefit in colorectal cancer survivors.
There are several limitations to this analysis. The primary limitation is that inflammatory outcomes were not prespecified in the study protocol; consequently, the results of this analysis are hypothesis-generating. The small sample size may have limited our ability to detect small but potentially clinically meaningful effects of exercise on inflammatory outcomes. The sample sizes were very small in the analysis stratified by cancer stage, resulting in uncertainty in the point estimates. The study duration was 24 weeks, which limits our ability to understand the benefits of exercise on inflammatory outcomes acutely and over longer time horizons. Study subjects were not enrolled based on having high inflammation at baseline, which limits our understanding of the effects of exercise in those with acute or chronic inflammation. We examined two distinct volumes of moderate-intensity aerobic exercise but not the effects of exercise intensity (e.g., light vs. moderate vs. vigorous) or exercise modality (e.g., weightlifting vs. high-intensity interval training) on inflammation outcomes. We examined three inflammation biomarkers associated with disease-free survival in colon cancer survivors (20–22). However, we acknowledge that inflammation can be quantified using many other biomarkers.
There are several strengths to this analysis. The two intervention groups, each prescribed a distinct dose of moderate-intensity aerobic exercise, allowed us to examine how inflammation outcomes change along the exercise dose curve. The aerobic exercise program was flexible, emphasizing home-based exercise, complemented with behavioral coaching from an exercise physiologist. Providing home-based treadmills incentivized study enrollment, as recruitment was completed ahead of schedule, and promoted excellent adherence to the exercise prescription over 24 weeks. Exercise adherence was objectively quantified using heart-rate monitors eliminating bias from self-report. Endpoint data collection, including inflammation assays, was conducted by staff blinded to the study group who adhered to standardized protocols to enhance rigor and reproducibility. Endpoint data collection was excellent (97% follow-up).
In one of the first randomized clinical trials evaluating two doses of moderate-intensity aerobic exercise in colon cancer survivors, this study suggests that 150 min/wk of moderate-intensity aerobic exercise may lower inflammation in select colon cancer survivors. The findings from this exploratory analysis are useful to inform the design of future studies that aim to identify the biological mediators of the relationship between physical activity and disease-free survival in colon cancer survivors.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of Pennsylvania School of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JB: Writing – original draft, Writing – review & editing. SC: Writing – review & editing. JM: Writing – review & editing. GS: Writing – review & editing. SY: Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers F-31CA192560; R21-CA182767; U54-CA155850; R00-CA218603; R25-CA203650; and U54-CA155626 and the National Institute of General Medicine Sciences of the National Institutes of Health under Award Number U54-GM104940.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that author JB was a member of the Frontiers editorial board, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1257767/full#supplementary-material
1. Meyerhardt JA, Heseltine D, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, et al. Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Clin Oncol (2006) 24(22):3535–41. doi: 10.1200/JCO.2006.06.0863
2. Brown JC, Ma C, Shi Q, Fuchs CS, Meyer J, Niedzwiecki D, et al. Physical activity in stage III colon cancer: CALGB/SWOG 80702 (Alliance). J Clin Oncol (2023) 41(2):243–54. doi: 10.1200/JCO.22.00171
3. Brown JC, Ma C, Shi Q, Niedzwiecki D, Zemla T, Couture F, et al. Association between physical activity and the time course of cancer recurrence in stage III colon cancer. Br J Sports Med (2023) 57(15):965–971. doi: 10.1136/bjsports-2022-106445
4. McTiernan A, Friedenreich CM, Katzmarzyk PT, Powell KE, Macko R, Buchner D, et al. Physical activity in cancer prevention and survival: A systematic review. Med Sci Sports Exerc. (2019) 51(6):1252–61. doi: 10.1249/MSS.0000000000001937
5. Brown JC, Gilmore LA. Physical activity reduces the risk of recurrence and mortality in cancer patients. Exerc Sport Sci Rev (2020) 48(2):67–73. doi: 10.1249/JES.0000000000000214
6. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature (2008) 454(7203):436–44. doi: 10.1038/nature07205
7. Yasui K, Shida D, Nakamura Y, Ahiko Y, Tsukamoto S, Kanemitsu Y. Postoperative, but not preoperative, inflammation-based prognostic markers are prognostic factors in stage III colorectal cancer patients. Brit J Cancer. (2021) 124(5):933–41. doi: 10.1038/s41416-020-01189-6
8. Chan JCY, Diakos CI, Chan DLH, Engel A, Pavlakis N, Gill A, et al. A longitudinal investigation of inflammatory markers in colorectal cancer patients perioperatively demonstrates benefit in serial remeasurement. Ann Surg (2018) 267(6):1119–25. doi: 10.1097/SLA.0000000000002251
9. Cheng E, Shi Q, Shields AF, Nixon AB, Shergill AP, Ma C, et al. Association of inflammatory biomarkers with survival among patients with stage III colon cancer. JAMA Oncol (2023) 9(3):404–13. doi: 10.1001/jamaoncol.2022.6911
10. Chung YC, Ku YL, Chiang HC, Liu WC, Kao TY, Yang CH, et al. Antibody to interleukin-6 receptor inhibits in vivo growth of human colorectal carcinoma cell xenografts. Anticancer Res (2021) 41(10):4907–16. doi: 10.21873/anticanres.15304
11. Brown JC, Zhang S, Ligibel JA, Irwin ML, Jones LW, Campbell N, et al. Effect of exercise or metformin on biomarkers of inflammation in breast and colorectal cancer: A randomized trial. Cancer Prev Res (Phila). (2020) 13(12):1055–62. doi: 10.1158/1940-6207.CAPR-20-0188
12. Brown JC, Troxel AB, Ky B, Damjanov N, Zemel BS, Rickels MR, et al. A randomized phase II dose-response exercise trial among colon cancer survivors: Purpose, study design, methods, and recruitment results. Contemp Clin Trials. (2016) 47:366–75. doi: 10.1016/j.cct.2016.03.001
13. Kantola T, Klintrup K, Vayrynen JP, Vornanen J, Bloigu R, Karhu T, et al. Stage-dependent alterations of the serum cytokine pattern in colorectal carcinoma. Brit J Cancer. (2012) 107(10):1729–36. doi: 10.1038/bjc.2012.456
14. Brown JC, Damjanov N, Courneya KS, Troxel AB, Zemel BS, Rickels MR, et al. A randomized dose-response trial of aerobic exercise and health-related quality of life in colon cancer survivors. Psychooncology (2018) 27(4):1221–8. doi: 10.1002/pon.4655
15. Brown JC, Rhim AD, Manning SL, Brennan L, Mansour AI, Rustgi AK, et al. Effects of exercise on circulating tumor cells among patients with resected stage I-III colon cancer. PloS One (2018) 13(10):e0204875. doi: 10.1371/journal.pone.0204875
16. Brown JC, Rickels MR, Troxel AB, Zemel BS, Damjanov N, Ky B, et al. Dose-response effects of exercise on insulin among colon cancer survivors. Endocr Relat Cancer. (2018) 25(1):11–9. doi: 10.1530/ERC-17-0377
17. Brown JC, Troxel AB, Ky B, Damjanov N, Zemel BS, Rickels MR, et al. Dose-response effects of aerobic exercise among colon cancer survivors: A randomized phase II trial. Clin Colorectal Cancer. (2018) 17(1):32–40. doi: 10.1016/j.clcc.2017.06.001
18. Brown JC, Zemel BS, Troxel AB, Rickels MR, Damjanov N, Ky B, et al. Dose-response effects of aerobic exercise on body composition among colon cancer survivors: a randomised controlled trial. Brit J Cancer. (2017) 117(11):1614–20. doi: 10.1038/bjc.2017.339
19. Paffenbarger R, Wing A, Hyde R. Paffenbarger physical activity questionnaire. Am J Epidemiol. (1978) 108:161–75. doi: 10.1093/oxfordjournals.aje.a112608
20. Shrotriya S, Walsh D, Bennani-Baiti N, Thomas S, Lorton C. C-reactive protein is an important biomarker for prognosis tumor recurrence and treatment response in adult solid tumors: A systematic review. PloS One (2015) 10(12):e0143080. doi: 10.1371/journal.pone.0143080
21. Knupfer H, Preiss R. Serum interleukin-6 levels in colorectal cancer patients–a summary of published results. Int J Colorectal Dis (2010) 25(2):135–40. doi: 10.1007/s00384-009-0818-8
22. Babic A, Shah SM, Song M, Wu K, Meyerhardt JA, Ogino S, et al. Soluble tumour necrosis factor receptor type II and survival in colorectal cancer. Brit J Cancer. (2016) 114(9):995–1002. doi: 10.1038/bjc.2016.85
23. Black S, Kushner I, Samols D. C-reactive protein. J Biol Chem (2004) 279(47):48487–90. doi: 10.1074/jbc.R400025200
24. Sansone P, Bromberg J. Targeting the interleukin-6/Jak/stat pathway in human Malignancies. J Clin Oncol (2012) 30(9):1005–14. doi: 10.1200/JCO.2010.31.8907
25. Rodriguez M, Cabal-Hierro L, Carcedo MT, Iglesias JM, Artime N, Darnay BG, et al. NF-kappaB signal triggering and termination by tumor necrosis factor receptor 2. J Biol Chem (2011) 286(26):22814–24. doi: 10.1074/jbc.M111.225631
26. Chan AT, Ogino S, Giovannucci EL, Fuchs CS. Inflammatory markers are associated with risk of colorectal cancer and chemopreventive response to anti-inflammatory drugs. Gastroenterology (2011) 140(3):799–808. doi: 10.1053/j.gastro.2010.11.041
27. Zuijdgeest-van Leeuwen SD, van den Berg JW, Wattimena JL, van der Gaast A, Swart GR, Wilson JH, et al. Lipolysis and lipid oxidation in weight-losing cancer patients and healthy subjects. Metabolism (2000) 49(7):931–6. doi: 10.1053/meta.2000.6740
28. Looney SW, Hagan JL. Analysis of biomarker data: a practical guide. Hoboken, New Jersey, USA: John Wiley & Sons (2015).
29. Fitzmaurice GM, Laird NM, Ware JH. Applied longitudinal analysis. Hoboken, New Jersey, USA: John Wiley & Sons (2012).
30. Greenland S. Tests for interaction in epidemiologic studies: a review and a study of power. Stat Med (1983) 2(2):243–51. doi: 10.1002/sim.4780020219
31. Crusz SM, Balkwill FR. Inflammation and cancer: advances and new agents. Nat Rev Clin Oncol (2015) 12(10):584–96. doi: 10.1038/nrclinonc.2015.105
32. Johnson DE, O'Keefe RA, Grandis JR. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat Rev Clin Oncol (2018) 15(4):234–48. doi: 10.1038/nrclinonc.2018.8
33. Schmitz KH, Gehlert S, Patterson RE, Colditz GA, Chavarro JE, Hu FB, et al. TREC to WHERE? Transdisciplinary research on energetics and cancer. Clin Cancer Res (2016) 22(7):1565–71. doi: 10.1158/1078-0432.CCR-14-1214
34. Friedenreich CM, Neilson HK, Woolcott CG, Wang Q, Stanczyk FZ, McTiernan A, et al. Inflammatory marker changes in a yearlong randomized exercise intervention trial among postmenopausal women. Cancer Prev Res (Phila). (2012) 5(1):98–108. doi: 10.1158/1940-6207.CAPR-11-0369
35. Friedenreich CM, O'Reilly R, Shaw E, Stanczyk FZ, Yasui Y, Brenner DR, et al. Inflammatory marker changes in postmenopausal women after a year-long exercise intervention comparing high versus moderate volumes. Cancer Prev Res (Phila). (2016) 9(2):196–203. doi: 10.1158/1940-6207.CAPR-15-0284
36. Del Rosso S, Baraquet ML, Barale A, Defago MD, Tortosa F, Perovic NR, et al. Long-term effects of different exercise training modes on cytokines and adipokines in individuals with overweight/obesity and cardiometabolic diseases: A systematic review, meta-analysis, and meta-regression of randomized controlled trials. Obes Rev (2023) 24(6):e13564. doi: 10.1111/obr.13564
37. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol (2010) 17(6):1471–4. doi: 10.1245/s10434-010-0985-4
38. Lohmann AE, Dowling RJO, Ennis M, Amir E, Elser C, Brezden-Masley C, et al. Association of metabolic, inflammatory, and tumor markers with circulating tumor cells in metastatic breast cancer. JNCI Cancer Spectr (2018) 2(2):pky028. doi: 10.1093/jncics/pky028
39. Uen YH, Lu CY, Tsai HL, Yu FJ, Huang MY, Cheng TL, et al. Persistent presence of postoperative circulating tumor cells is a poor prognostic factor for patients with stage I-III colorectal cancer after curative resection. Ann Surg Oncol (2008) 15(8):2120–8. doi: 10.1245/s10434-008-9961-7
Keywords: biomarkers, C-reactive protein, dose-response, interleukins, tumor necrosis factors
Citation: Brown JC, Compton SLE, Meyerhardt JA, Spielmann G and Yang S (2023) The dose-response effect of aerobic exercise on inflammation in colon cancer survivors. Front. Oncol. 13:1257767. doi: 10.3389/fonc.2023.1257767
Received: 07 August 2023; Accepted: 09 November 2023;
Published: 12 December 2023.
Edited by:
Frank A. Orlando, University of Florida, United StatesReviewed by:
Igor Lucas Gomes-Santos, Harvard Medical School, United StatesCopyright © 2023 Brown, Compton, Meyerhardt, Spielmann and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Justin C. Brown, anVzdGluLmJyb3duQHBicmMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.