 Daniel C. Moreira1
Daniel C. Moreira1 Oscar González-Ramella2
Oscar González-Ramella2 Maite Echavarría Valenzuela3
Maite Echavarría Valenzuela3 Angela K. Carrillo1
Angela K. Carrillo1 Lane Faughnan1
Lane Faughnan1 Godwin Job1Yichen Chen1
Godwin Job1Yichen Chen1 Cesar Villegas1
Cesar Villegas1 Andrea Ellis Irigoyen4Rosario Barra Urbays5Maribel Ramírez Martinez6Eduardo Altamirano Alvarez7
Andrea Ellis Irigoyen4Rosario Barra Urbays5Maribel Ramírez Martinez6Eduardo Altamirano Alvarez7 José Antonio León Espitia8
José Antonio León Espitia8 Norma Araceli López Facundo9
Norma Araceli López Facundo9 Julia Esther Colunga Pedraza10Flor de María Reyes Gutierrez11Ana Berenice Aguilar Román12
Julia Esther Colunga Pedraza10Flor de María Reyes Gutierrez11Ana Berenice Aguilar Román12 Edna Liliana Tamez Gómez13Claudia Selene Portillo Zavala14Natalia del Carmen Negroe Ocampo15Sandra Guadalupe Pulido Sanchez16Deyanira Cortés Alva17Paola Casillas Toral2Karime Salas Villa3Patricia Judith Mendoza Sánchez4
Edna Liliana Tamez Gómez13Claudia Selene Portillo Zavala14Natalia del Carmen Negroe Ocampo15Sandra Guadalupe Pulido Sanchez16Deyanira Cortés Alva17Paola Casillas Toral2Karime Salas Villa3Patricia Judith Mendoza Sánchez4 Carlos Pérez Alvarado5Gabriela Tamayo Pedraza6Margarita González Zamorano7José Manuel Ricardo Ávila Alba8Jocelyn Becerril Becerril9Hernán Ramírez Durán10
Carlos Pérez Alvarado5Gabriela Tamayo Pedraza6Margarita González Zamorano7José Manuel Ricardo Ávila Alba8Jocelyn Becerril Becerril9Hernán Ramírez Durán10 Antonio Sandoval Cabrera11Adolfo Pineda Gordillo12Dora Iveth de la Rosa Alonso13
Antonio Sandoval Cabrera11Adolfo Pineda Gordillo12Dora Iveth de la Rosa Alonso13 Leonardo Javier Mejía Marín14Leslie de los Ángeles Benítez Can15
Leonardo Javier Mejía Marín14Leslie de los Ángeles Benítez Can15 Itzel Gutiérrez Martinez16Mariana Isabel Jiménez Osorio17Naomi Echeandia1Erika Casillas18Karla Guerrero-Gomez18
Itzel Gutiérrez Martinez16Mariana Isabel Jiménez Osorio17Naomi Echeandia1Erika Casillas18Karla Guerrero-Gomez18 Meenakshi Devidas1
Meenakshi Devidas1 Paola Friedrich1*
Paola Friedrich1*- 1Department of Global Pediatric Medicine, St. Jude Children’s Research Hospital, Memphis, TN, United States
- 2Department of Pediatric Hematology/Oncology, Hospital Civil de Guadalajara Juan I. Menchaca, Guadalajara, Mexico
- 3Department of Pediatric Oncology, Hospital Pediátrico de Sinaloa, Culiacán, Mexico
- 4Department of Pediatric Oncology, Hospital Infantil Teletón de Oncología, Querétaro, Mexico
- 5Department of Pediatric Oncology, Centro Estatal de Cancerologia Dr. Miguel Dorantes Mesa, Xalapa, Mexico
- 6Department of Pediatric Oncology, Hospital General de Tijuana, Tijuana, Mexico
- 7Department of Pediatric Hematology/Oncology, Hospital General con Especialidades “Juan María Salvatierra”, La Paz, Mexico
- 8Department of Pediatric Oncology, Hospital General Leoón, León, Mexico
- 9Department of Pediatric Oncology, Hospital Materno Infantil ISSEMYM Toluca, Toluca, Mexico
- 10Department of Pediatric Hematology, Hospital Universitario “José Eleuterio González”, Monterrey, Mexico
- 11Department of Pediatric Hematology/Oncology, Hospital para el Niño del IMIEM, Toluca, Mexico
- 12Department of Pediatric Oncology, ONCOCREAN Tapachula, IMSS, Tapachula, Mexico
- 13Department of Pediatric Hematology/Oncology, Hospital Infantil de Tamaulipas, Ciudad Victoria, Mexico
- 14Department of Pediatric Oncology, Hospital Infantil de Especialidades de Chihuahua, Chihuahua, Mexico
- 15Department of Pediatric Oncology, Hospital General Agustín O´Horán, Mérida, Mexico
- 16Department of Pediatric Hematology, Hospital Infantil de Morelia “Eva Sámano de López Mateos”, Morelia, Mexico
- 17Department of Pediatric Oncology, Hospital del Niño DIF Hidalgo, Pachuca, Mexico
- 18Casa de la Amistad, Mexico City, Mexico
Background and aims: Pediatric acute lymphoblastic leukemia (ALL) survival rates in low- and middle-income countries are lower due to deficiencies in multilevel factors, including access to timely diagnosis, risk-stratified therapy, and comprehensive supportive care. This retrospective study aimed to analyze outcomes for pediatric ALL at 16 centers in Mexico.
Methods: Patients <18 years of age with newly diagnosed B- and T-cell ALL treated between January 2011 and December 2019 were included. Clinical and biological characteristics and their association with outcomes were examined.
Results: Overall, 2,116 patients with a median age of 6.3 years were included. B-cell immunophenotype was identified in 1,889 (89.3%) patients. The median white blood cells at diagnosis were 11.2.5 × 103/mm3. CNS-1 status was reported in 1,810 (85.5%), CNS-2 in 67 (3.2%), and CNS-3 in 61 (2.9%). A total of 1,488 patients (70.4%) were classified as high-risk at diagnosis. However, in 52.5% (991/1,889) of patients with B-cell ALL, the reported risk group did not match the calculated risk group allocation based on National Cancer Institute (NCI) criteria. Fluorescence in situ hybridization (FISH) and PCR tests were performed for 407 (19.2%) and 736 (34.8%) patients, respectively. Minimal residual disease (MRD) during induction was performed in 1,158 patients (54.7%). The median follow-up was 3.7 years. During induction, 191 patients died (9.1%), and 45 patients (2.1%) experienced induction failure. A total of 365 deaths (17.3%) occurred, including 174 deaths after remission. Six percent (176) of patients abandoned treatment. The 5-year event-free survival (EFS) was 58.9% ± 1.7% for B-cell ALL and 47.4% ± 5.9% for T-cell ALL, while the 5-year overall survival (OS) was 67.5% ± 1.6% for B-cell ALL and 54.3% ± 0.6% for T-cell ALL. The 5-year cumulative incidence of central nervous system (CNS) relapse was 5.5% ± 0.6%. For the whole cohort, significantly higher outcomes were seen for patients aged 1–10 years, with DNA index >0.9, with hyperdiploid ALL, and without substantial treatment modifications. In multivariable analyses, age and Day 15 MRD continued to have a significant effect on EFS.
Conclusion: Outcomes in this multi-institutional cohort describe poor outcomes, influenced by incomplete and inconsistent risk stratification, early toxic death, high on-treatment mortality, and high CNS relapse rate. Adopting comprehensive risk-stratification strategies, evidence-informed de-intensification for favorable-risk patients and optimized supportive care could improve outcomes.
1 Introduction
Pediatric acute lymphoblastic leukemia (ALL) is highly curable. Advances in the treatment of ALL embody one of the most successful examples of the progress of the field of pediatric oncology (1). An increased understanding of the biological underpinnings of ALL, the development of risk-stratified treatment, including response-based intensity, and the optimization of supportive care have led to a remarkable increase in cure rates (2, 3). In high-income countries (HICs), survival rates for pediatric ALL have surpassed 90%, and much of the current research focuses on decreasing short- and long-term treatment-related morbidity (4). Nonetheless, the majority of the children diagnosed with ALL live in low- and middle-income countries (LMICs) and do not have access to the optimal care that permits these high cure rates (5). Thus, the success of curing pediatric ALL depends on improving access to quality care for children in LMICs.
Recent studies show that the survival of pediatric patients with ALL varies considerably, with appreciably worse outcomes in LMICs (6). Data from CONCORD-3, an analysis of cancer-related survival from population-based cancer registries, showed survival rates between 50% and 70% for many countries in Latin America, Africa, and Asia (7). A recent simulation-based study estimated the survival of ALL at 61% in Latin America and the Caribbean (6). Mexico is an upper-middle-income country with approximately 2,300 new cases of pediatric ALL each year (8). The estimated 5-year overall survival for ALL in Mexico is approximately 60% (9–11). Adverse outcomes have been associated with late presentation, delayed diagnosis, malnutrition (12), infection-related deaths (13), and abandonment (14). In Mexico, between 2004 and 2019, Seguro Popular provided health coverage to the population without social security or private insurance, including financing care for children and adolescents with ALL. Since 2020, the Mexican health system has been in constant redesign. New health governance and financing strategies are being proposed, but their adoption, implementation, spread, and permanence remain to be determined.
In 2016, eight centers from eight different states in Mexico and St. Jude Children’s Research Hospital (St. Jude) in Memphis, United States, joined to create, and in 2017 launch, “Mexico in Alliance with St. Jude (MAS)”, a collaborative group dedicated to increasing the survival and quality of care of children and adolescents with cancer in Mexico. Within the workstream to identify gaps in access and quality care for children with care, a retrospective study was developed to ascertain deficiencies and strengths of care for pediatric ALL. This multi-institutional study sought to characterize the outcomes of children with ALL diagnosed at institutions in Mexico, correlating the findings with clinical and biological factors and elements related to access to quality care. Preliminary results have been used to co-design and co-produce prospective interdisciplinary projects over the years, including an evidence-based, consensus-derived, adapted treatment guideline, which now serves as the standard of care at many MAS member institutions.
2 Methods
2.1 Study context and oversight
This multicenter retrospective analysis was conducted across 16 pediatric cancer units in Mexico. St. Jude served as a coordinating center for the study, facilitating the electronic database, training for data abstraction, and data analysis. All centers are part of the cooperative group MAS. Institutional review board approval or exemption was obtained at St. Jude and each participating site.
2.2 Patient selection and data abstraction
All consecutive patients <18 years of age with newly diagnosed B- and T-cell ALL diagnosed between January 2011 and December 2019 at 16 resource and geographically diverse participating healthcare institutions were included. Clinical information on demographics, treatment, laboratory tests, molecular characteristics, and follow-up was extracted from institutional medical records. For treatment, given that institutions treated ALL with different protocols, and there was variability even within institutions at different timepoints, general descriptors of treatment approach were collected, including chemotherapy doses during induction, use of radiotherapy, and modification to planned treatment. Records were both paper-based and electronic and entered into a single electronic database. The data were first collected in 2018–2019, including inputs through 2015, and then expanded in 2021–2022 to include inputs through 2019 (Supplement 1). Data collection was completed in December of 2022.
2.3 Statistical analyses
Descriptive statistics were used to summarize patient characteristics. Categorical data are presented as percentages, and continuous data as means (standard deviations) or medians (interquartile range (IQR)). Event-free survival (EFS) and overall survival (OS) were calculated by the Kaplan–Meier method with standard errors by Peto et al. (15, 16) EFS was defined as the time from diagnosis to first event (induction failure, induction death, relapse, and remission death) or date of last contact for those who were event-free. OS was defined as the time from diagnosis to death or last contact for those still alive. For abandonment-sensitive EFS (A-EFS) and OS (A-OS), treatment abandonment was also considered an event. Log-rank test was used to compare survival curves between groups. Cumulative incidence rates were computed using the cumulative incidence function for competing risks, and comparisons were made using the K-sample test (17). Univariate and multivariable Cox regression analyses were used to assess the effect of factors on EFS. For all analyses, a p-value <0.05 was considered statistically significant. Analyses were conducted using SAS software, version 9.4, and R version 4.0.0.
3 Results
A total of 2,116 eligible patients were identified with a median age of 6.3 years (IQR, 7.5). Patient characteristics are presented in Table 1. Most patients had B-cell ALL (1,889, 89.3%) and no central nervous system (CNS) involvement (1,810, 85.5%). Only 160 (7.6%) of patients presented with T-cell phenotype, and only 61 (2.9%) of the patients were reported to have trisomy 21 (Down syndrome). The diagnostic lumbar puncture was traumatic in 127 patients (6.0%). Data on CNS status, immunophenotype, and karyotype were not available in 130 (6.1%), 39 (1.8%), and 745 (35.2%) patients, respectively.
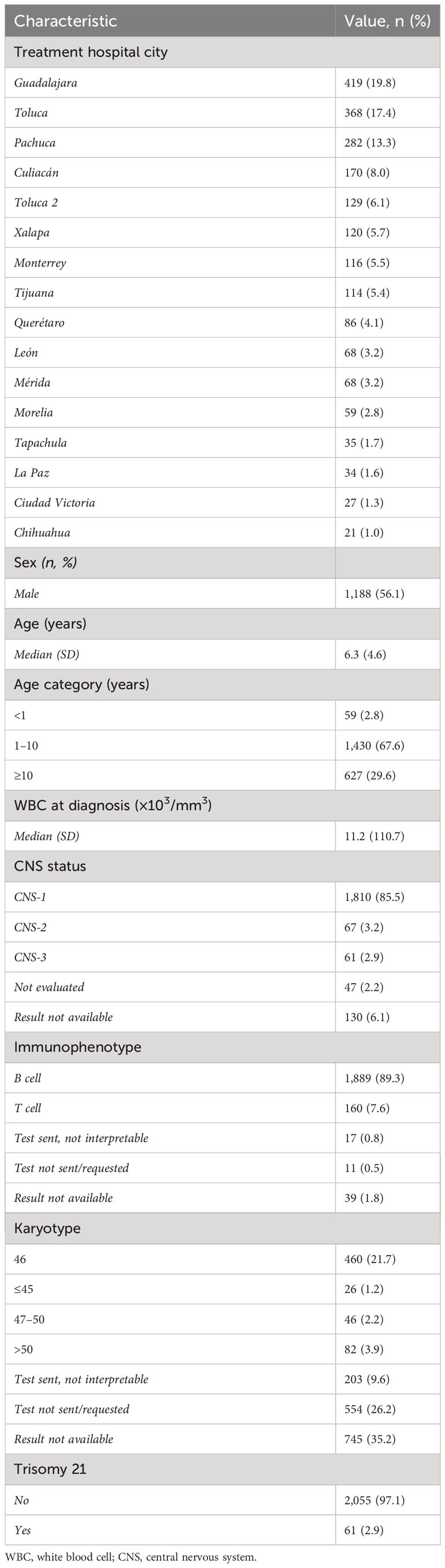
Table 1 Patient characteristics.
3.1 Risk stratification and treatment
Of the 1,889 patients with B-cell ALL, 1,488 (70.4%) patients were assigned high-risk therapy at the beginning of treatment, while 593 (28.0%) were assigned standard-risk therapy. Based on National Cancer Institute (NCI) standard-risk criteria for pediatric B-cell ALL (age 1–10 years and initial white blood cell (WBC) <50,000/mm3), 52.5% (991/1,889) of patients were assigned a risk group at the start of treatment that differs from what would be obtained utilizing this standard. Distribution of age and initial WBC shows that only 28.5% (538/1,889) and 23.2% (439/1,889) of patients, respectively, would fall within high-risk criteria for these two parameters. After induction therapy, patients were assigned final risk groups: 447 patients (23.3%) were classified as standard-risk, 1,262 patients (65.9%) as high-risk, and 126 patients (6.6%) as very high-risk. Risk-stratification data were unavailable for 200 patients.
Regarding treatment, 148 patients (7.0%) had received treatment for ALL prior to transfer to one of the 16 institutions, with the majority being the initiation of systemic corticosteroids. The 16 institutions used treatment protocols adapted from BFM, St. Jude’s Total XIIIB, or the Dana-Farber Cancer Institute (DFCI) 05-001 protocols. Prednisone, vincristine, asparaginase, and daunorubicin were the most used systemic chemotherapy agents during induction. The median doxorubicin equivalents during induction were 60 mg/m2 (IQR, 25.0). The median number of intrathecal chemotherapy doses was 4.0 (IQR, 3.0), with triple therapy (methotrexate, cytarabine, and hydrocortisone) being the most used intrathecal chemotherapy (71.1%). Among the 74 patients with BCR-ABL translocation, 24 (32.4%) started imatinib during induction. Sixty patients (3.1%) received radiation as part of treatment: 34 (56.7%) with CNS-1 status, 6 (10%) with CNS-2, 17 (28.3%) with CNS-3, and 3 (5%) with unknown CNS status.
During therapy, 323 patients (15.3%) had a substantial change to treatment, defined as the elimination or substitution of a chemotherapy agent in more than half of the doses of a treatment phase. Modifications due to toxicity or infection were the most frequently cited reason (38.1%, 123/323). Furthermore, the mean number of times chemotherapy was held for more than 2 weeks was 1.5 times per patient. Infection (68.7%) and chemotherapy-related side effects (56.8%) were the most cited reasons for the interruption of chemotherapy.
3.2 Access to molecular diagnostics
Fluorescence in situ hybridization (FISH) and PCR tests were performed for 407 (19.2%) and 736 (34.8%) patients, respectively. The median times to obtain results for the characterization of ALL samples were as follows: 1.0 days for immunophenotype (standard deviation (SD), 6.8 days), 10.0 days for FISH (SD, 13.7 days), 10.0 days for cytogenetics (SD, 23.0 days), and 8.0 days for PCR (SD, 14.8 days). To evaluate the availability of molecular tests and the frequency of recurrent alterations, five common translocations were assessed in patients with B-cell ALL (Table 2). Considering the cases where these tests were performed and available, samples were positive in 10.8% (106/981) for ETV6-RUNX1, 6.5% (74/1,133) for BCR-ABL, 7.8% (74/953) for E2A/PBX, 4.3% (40/940) for MLL translocations, and 6.4% (14/220) for iAMP21.
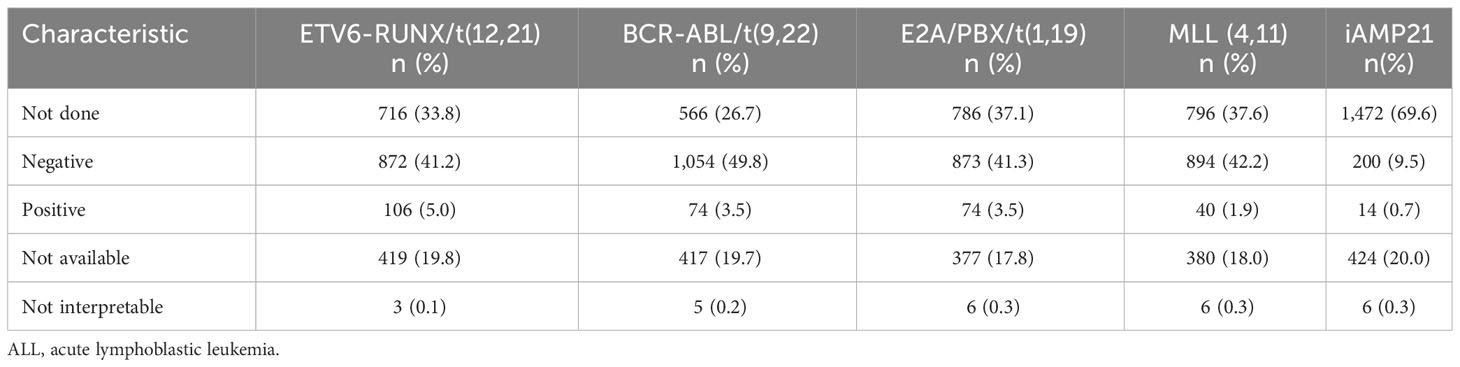
Table 2 Testing of recurrent translocations for B-cell ALL.
Minimal residual disease (MRD) was performed in 1,158 patients (54.7%) during induction (Table 3). All MRD tests were performed from bone marrow aspirate samples. Days 15 (35.5%) and 29 (29.1%) were the most common timepoints for MRD evaluation. Considering negative MRD thresholds of <1% on Days 8 and 15 and <0.01% on Day 29, 87.1% (27/31), 84.8% (341/402), and 73.9% (235/318) of tested patients had negative MRD during these timepoints, respectively.
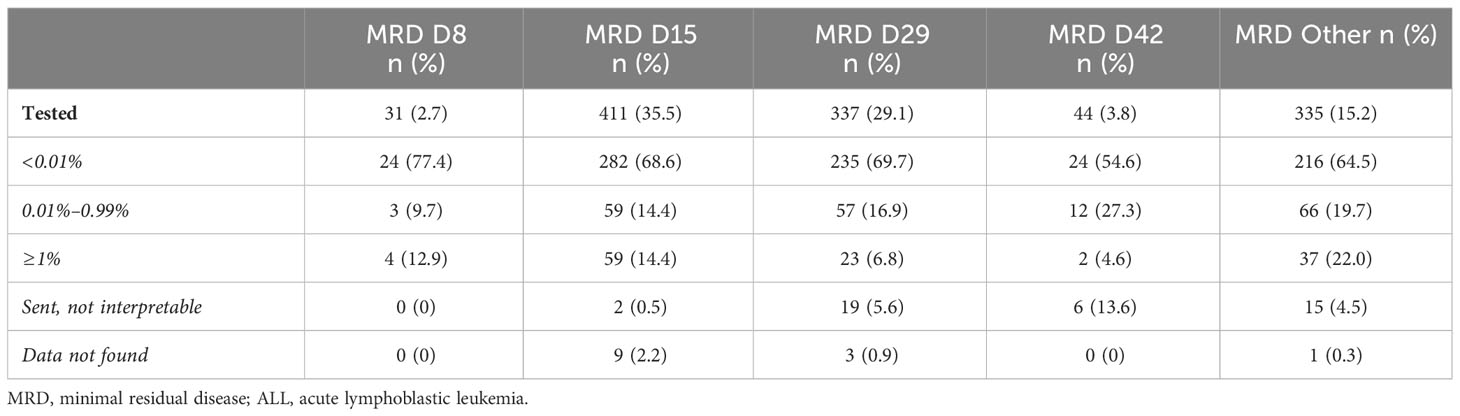
Table 3 MRD monitoring for B-cell ALL.
3.3 Early toxicity and death
During induction, there were 191 deaths (9.1%) reported: 142 in patients with B-cell ALL (7.5% of B-cell ALL patients) and 49 in patients with T-cell ALL (30.1% of T-cell ALL). Antibiotics were indicated for therapeutic purposes during induction in 1,536 patients (72.6%). Finally, clinical sepsis (542 patients), bacteremia (487 patients), pneumonia (276 patients), and meningitis (9 patients) were the most reported infections during induction.
3.4 Outcomes
Median follow-up was 3.7 years and was available for 2,106 patients (99.5%). Forty-five patients (2.1%) had induction failure. A total of 365 deaths (17.3%) were reported, including 191 deaths during induction and 174 additional deaths after achieving remission. Of the patients, 176 (6%) abandoned treatment, and 416 (19.6%) relapsed. Among the relapses, 225 (54.1%) were isolated bone marrow, 111 (26.7%) isolated CNS, 63 (15.1%) mixed, and 17 (4.1%) extramedullary (non-CNS) relapses.
Five-year EFS and OS rates based on clinical and biological characteristics are given in Table 4 and Figure 1. For the whole cohort, the 5-year EFS and OS were 57.6% ± 1.6% and 66.0%± 1.5%, respectively. The 5-year A-EFS and A-OS for the whole cohort were 54.5% ± 1.6% and 62.1% ± 1.5, respectively. The 5-year EFS was 58.9% ± 1.7% for B-cell ALL and 47.4% ± 5.9% for T-cell ALL, while the 5-year OS was 67.5% ± 1.6% for B-cell ALL and 54.3% ± 5.9% for T-cell ALL (Figure 1A). For the whole cohort, significantly higher outcomes were observed for patients aged 1–10 years and patients without substantial treatment modifications. Outcomes from the geographic territories with the highest number of patients are included in Supplement 2.
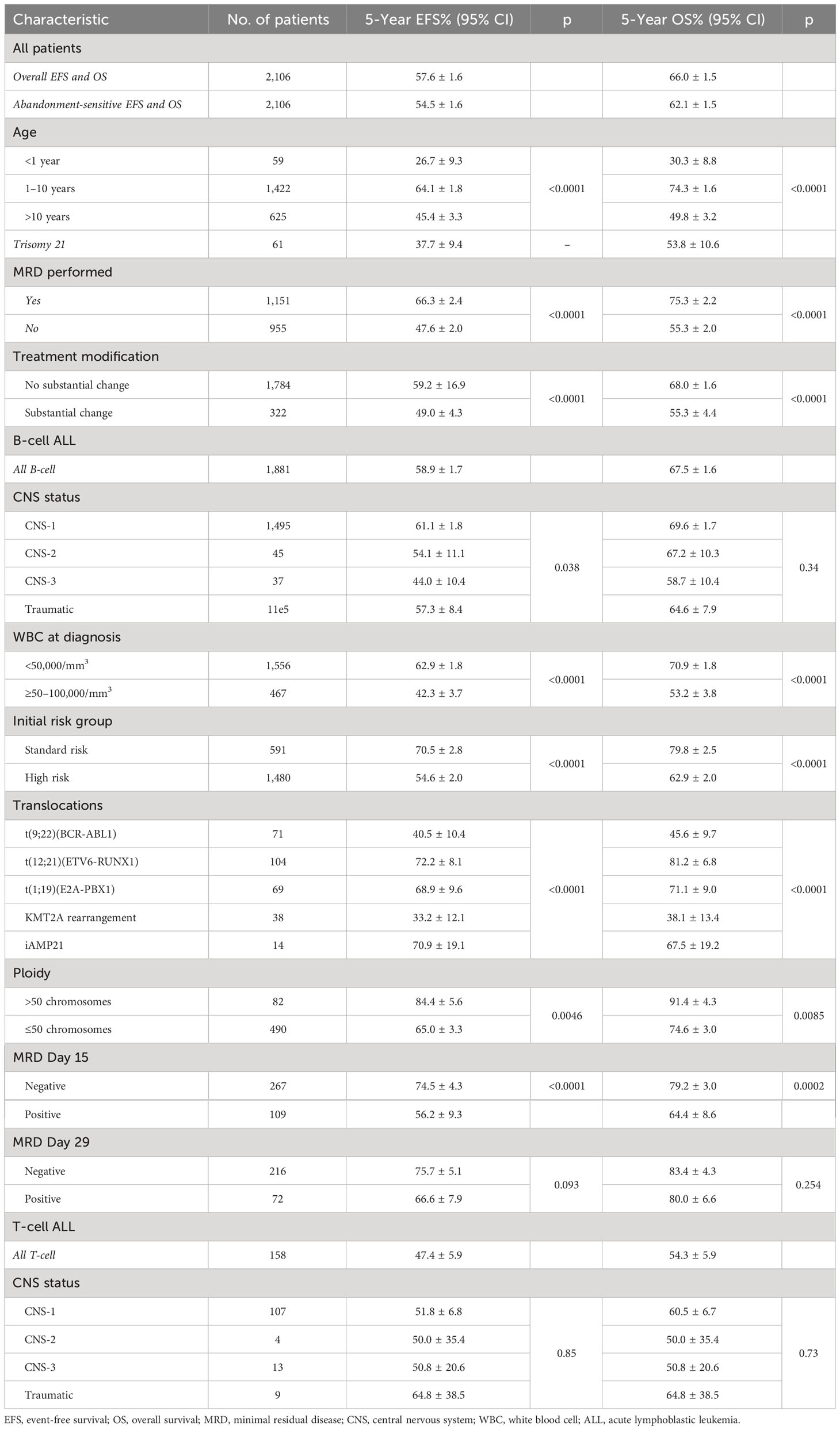
Table 4 EFS and OS by clinical and biological characteristics.
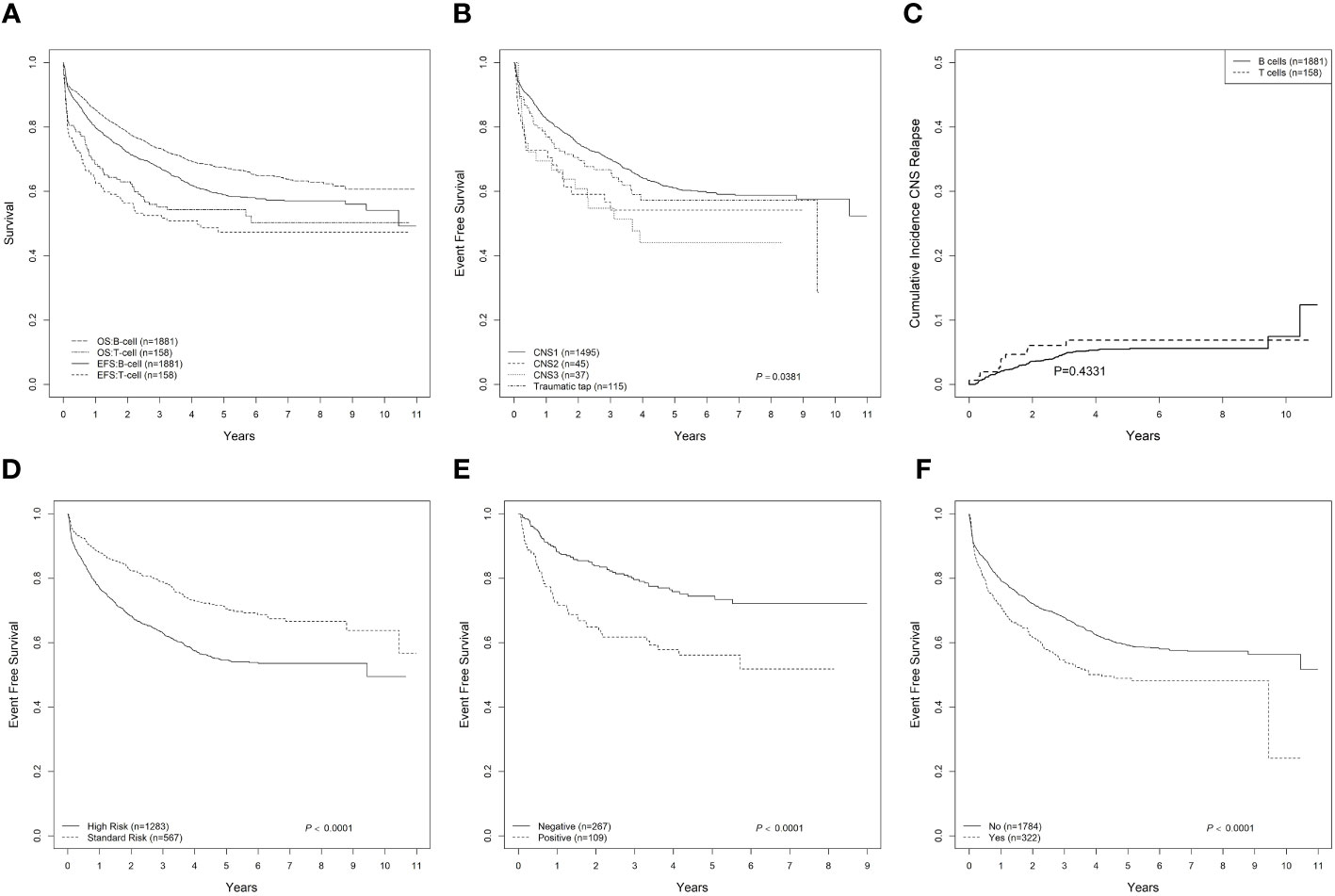
Figure 1 Outcome of pediatric ALL in Mexico. (A) EFS and OS for B-cell and T-cell ALL. (B) EFS for CNS status for B-cell ALL. (C) Cumulative incidence of CNS relapse for B-cell and T-cell ALL. (D) EFS for standard-risk and high-risk B-cell ALL. (E) EFS for B-cell ALL based on MRD status tested on Day 15. (F) EFS for B-cell and T-cell ALL based on substantial change to treatment. ALL, acute lymphoblastic leukemia; EFS, event-free survival; OS, overall survival; CNS, central nervous system; MRD, minimal residual disease.
Translocations also showed varying outcomes for B-cell ALL, with patients with t(9;22) (BCR-ABL1) having a 5-year EFS of 40.5% ± 10.4%. The 5-year EFS for B-cell ALL with CNS-1, CNS-2, and CNS-3 was 61.1% ± 1.8%, 54.1% ± 11.1%, and 44.0% ± 10.4%, respectively (p = 0.038) (Figure 1B). The 5-year cumulative incidence of CNS relapse was 5.5% ± 0.6% (Figure 1C). The 5-year EFS for B-cell ALL was 70.5% ± 2.8% for the standard-risk group and 54.6% ± 2.0% for the high-risk group (p < 0.0001) (Figure 1D). In patients with B-cell ALL and MRD performed on Day 15, the 5-year EFS was 74.5% ± 4.3% for patients with negative MRD and 56.2% ± 9.3% for patients with positive MRD (Figure 1E, p<0.001). For patients with substantial modifications to treatment (Figure 1F), 5-year EFS was also lower (p < 0.0001).
Univariate and multivariable Cox regression analyses of EFS were performed for B-ALL (Table 5). In univariate analyses, age (1–10 years), initial risk group (standard risk), and Day 15 MRD (negative) were significantly associated with lower EFS. In multivariable analyses, age and Day 15 MRD continued to have a significant effect on EFS.
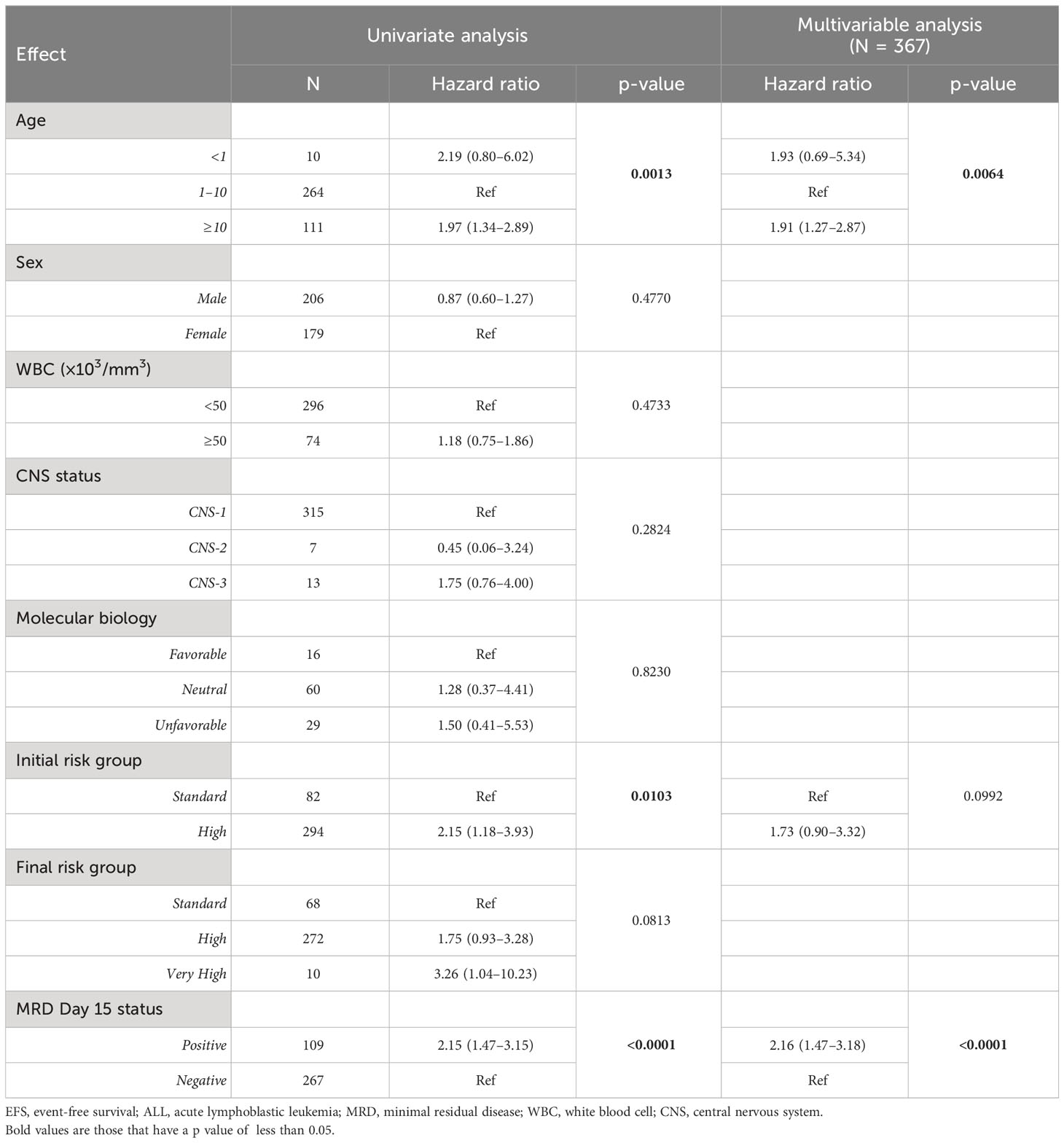
Table 5 Univariate and multivariable Cox regression analyses of EFS for B-cell ALL limited to patients with Day 15 MRD data.
4 Discussion
This detailed review of a large cohort of patients diagnosed and treated in Mexico has allowed for the evaluation of multiple elements of pediatric ALL care and outcomes. Our study analyzed data from 2,116 patients across 16 centers and suggests outcomes are lower than desirable, with a high frequency of treatment-related toxicity and relapse, and inconsistent access to diagnostic tests, both at diagnosis to characterize ALL samples and for disease monitoring through MRD.
Consistent with prior institutional and population-based cancer registry reports from Mexico (7, 9–11), our study describes lower OS and EFS for pediatric ALL than reported in HICs. Furthermore, regional variability can also be seen in our study, similar to published reports (9). Compared to reports from collaborative studies from North America and Europe, the outcomes from our report are close to 20% to 30% lower. High rates of death in induction, abandonment, death in remission, and relapse are the main contributing factors to these poor outcomes. Nonetheless, factors associated with outcomes from high-resource settings such as age, WBC count at diagnosis, ploidy, presence of translocation, and response to therapy (MRD) continue to portend prognostic significance.
We report an abandonment rate of 6%, like prior reports from Mexico (10, 18, 19) During the time that this cohort was treated, government-funded healthcare existed for children and adolescents with ALL. Despite coverage, treatment abandonment is a complex phenomenon, and it has been associated with social, economic, and treatment-related factors (20, 21). Social inequalities and social determinants of health continue to impact cancer outcomes even when direct costs for cancer care are covered (22). This study did not collect data on social determinants of health for the cohort; hence, additional analyses would be necessary to further describe factors that increase the risk of treatment abandonment in Mexico.
Induction has the highest risk of infectious complications due to prolonged immunosuppression from disease and the intensity of induction chemotherapy (23, 24). In our study, close to 10% mortality was seen during induction, with most deaths from infectious processes. This rate is markedly above reports not only of the clinical trials of cooperative groups in high-resource settings where <2% is usually reported (2, 25, 26) but also in pediatric oncology units in Central America (27, 28). The risk of death in induction was not associated with treatment intensity (anthracycline dose), suggesting that earlier diagnosis of ALL and improved management of infectious complications may be the most valuable intervention. Importantly, the MAS centers are participating in a project to implement a pediatric early warning system (PEWS) (29) and timely antibiotic administration in febrile patients (30) as mechanisms to improve treatment-related mortality. Additional interventions such as prophylactic antibiotics during induction (31) could be considered as strategies to decrease infectious mortality early in treatment. Interventions that mitigate unplanned toxicities could also impact the financial aspects of pediatric cancer care (32).
Contrary to most pediatric ALL studies, our study reports that most patients were classified as high-risk, including 70% at the beginning of induction. The NCI standard-risk criteria are effective risk stratification criteria (33), especially when access to molecular tests is inconsistent. Based on these two variables, we describe how close to 50% of patients were inappropriately assigned risk groups. Although other variables are used for risk assignment, such as steroid response and DNA index, this is unlikely to explain the large disparity. Ultimately, these data suggest that a large proportion of patients were over-treated, increasing the risk of treatment-related mortality and long-term morbidity. This is especially worrisome, as it is known that close to 40% of patients can be cured with minimally intensive therapy (34, 35). Standardized approach to risk stratification would optimize the intensity of therapy based on the risk of relapse.
In our report, the frequency of CNS-2 status was 3.2%. This is lower than recently published studies from North America, where St. Jude’s Total XVI had 33% (24) and COG’s standard-risk trial, AALL0331, had 8% (25). On further investigation, some centers included in the study did not have the capacity to perform cytospin to evaluate for leukemic blasts, hence likely under-reporting CNS-2 status. Given these elements and the previously mentioned discordance in risk stratification, the association of CNS status and outcomes in this cohort was likely confounded due to these factors.
Over the past decades, the molecular characterization of ALL has transformed the field of pediatric leukemia care (36). Access to advanced diagnostic tests to characterize ALL samples are essential to provide risk-adapted therapy, seeking to maximize cure rates and minimize therapy-associated toxicities. Our data suggested limited access to advanced diagnostics like FISH and PCR. Furthermore, uninterpretable tests were also reported, highlighting the need to improve the quality of testing also. Strategies to achieve increased access to quality diagnostics could be the identification of centralized, regional testing centers with adequate validation processes.
Response to treatment and MRD has been the most important prognostic factor for pediatric ALL (37–40). The role of MRD in risk stratification has already been used in LMICs for close to two decades, confirming its relevance in resource-limited settings even when simplified flow cytometry-based assays are utilized (41, 42). In our study, 55% of patients had MRD performed during different points of therapy. Importantly, in univariate and multivariable analyses, negative MRD was associated with EFS. Furthermore, patients whose MRD was performed, regardless of results, had better survival, suggesting that access to comprehensive testing can influence outcomes. Based on these data, consistent access to timely and high-quality MRD would optimize therapy for patients with ALL. Increasing access to MRD could be achieved by identifying regional centers to process samples for treatment response.
Pediatric ALL is a heterogeneous disease, with recurrent genetic alterations conferring treatment prognosis. Some studies have described a lower frequency of favorable translocations, like ETV6-RUNX1, in Hispanic populations within the United States (43). The frequency of ETV6-RUNX1 in our cohort is consistent with Hispanic patients in the United States, which is lower than other populations. Of the patients with ALL and BCR-ABL fusions, the 5-year OS was 45.6%, consistent with the outcomes seen before the use of ABL-class tyrosine kinase inhibitors (44). In our study, of the 74 patients identified with BCR-ABL1 fusions, only 24 received targeted therapy, likely hindering the possibility of early remission. It is important to note that an important fraction of the cohort does not have alterations frequently seen in pediatric ALL. It is unclear if this is related to a true variation or inherently a marker of inadequate access to comprehensive, validated molecular testing. Ultimately, the size of the cohort with complete molecular characterizations is insufficient to comprehensively describe variations of genetic alterations in ALL for the Mexican population.
Our study has limitations. As a retrospective study, the availability of all details of care was absent for some patients, especially as we sought to extract granular features of diagnostic evaluations and therapy. Nonetheless, given the size of the cohort and explicit mention of when data elements were absent, relevant conclusions can still be reached. Furthermore, as patients were treated with different protocols, the impact of specific treatment phases and chemotherapy strategies cannot be concluded from this study.
In Mexico, cancer is the leading cause of death in children aged 5–14 (45, 46); hence, investment in the care of children with ALL and pediatric cancer is imperative. The results from this study highlight areas that are relevant for interventions to improve quality care for children with ALL not only in Mexico but also in other LMICs. Based on these data, the MAS group has developed an evidence-based consensus-derived treatment guideline for ALL currently being used in more than 10 pediatric cancer units in Mexico. Furthermore, these data informed a peer-reviewed grant-funded prospective project to improve access to a consensus-derived diagnostic panel and support comprehensive risk stratification. Some of the outputs of these interventions are included in other manuscripts of this Frontiers in Oncology Research Topic. With these data-driven approaches, improved outcomes are anticipated.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by St. Jude Children’s Research Hospital and each participating site. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin. Exemption is due to retrospective nature of study.
Author contributions
DM: Formal Analysis, Supervision, Visualization, Writing – original draft, Writing – review & editing. OG-R: Investigation, Supervision, Writing – review & editing. ME: Investigation, Supervision, Writing – review & editing. AC: Data curation, Project administration, Writing – review & editing. LF: Project administration, Writing – review & editing. GJ: Formal Analysis, Writing – review & editing. YC: Formal Analysis, Writing – review & editing. CV: Supervision, Writing – review & editing. AI: Investigation, Writing – review & editing. RB: Investigation, Writing – review & editing. MR: Data curation, Investigation, Writing – review & editing. EA: Investigation, Writing – review & editing. JE: Investigation, Writing – review & editing. NL: Investigation, Writing – review & editing. JC: Investigation, Writing – review & editing. FR: Investigation, Writing – review & editing. AA: Investigation, Writing – review & editing. ET: Investigation, Writing – review & editing. CPZ: Investigation, Writing – review & editing. NN: Investigation, Writing – review & editing. SP: Investigation, Writing – review & editing. DC: Investigation, Writing – review & editing. PC: Data curation, Writing – review & editing. KS: Data curation, Writing – review & editing. PM: Data curation, Writing – review & editing. CPA: Data curation, Writing – review & editing. GT: Data curation, Writing – review & editing. MG: Data curation, Writing – review & editing. JÁ: Data curation, Writing – review & editing. JB: Data curation, Writing – review & editing. HR: Data curation, Writing – review & editing. AS: Data curation, Writing – review & editing. AP: Data curation, Writing – review & editing. DA: Data curation, Writing – review & editing. LM: Data curation, Writing – review & editing. LB: Data curation, Writing – review & editing. IG: Data curation, Writing – review & editing. MJ: Data curation, Writing – review & editing. NE: Data curation, Writing – review & editing. EC: Data curation, Supervision, Writing – review & editing. KG: Supervision, Writing – review & editing. MD: Formal Analysis, Writing – review & editing. PF: Conceptualization, Investigation, Methodology, Project administration, Resources, Writing – review & editing.
Funding
Funding was provided by ALSAC.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1255555/full#supplementary-material
References
1. Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med (2006) 354(2):166–78. doi: 10.1056/NEJMra052603
2. Hunger SP, Lu X, Devidas M, Camitta BM, Gaynon PS, Winick NJ, et al. Improved survival for children and adolescents with acute lymphoblastic leukemia between 1990 and 2005: a report from the Children's Oncology Group. J Clin Oncol (2012) 30(14):1663–9. doi: 10.1200/JCO.2011.37.8018
3. Vora A, Goulden N, Mitchell C, Hancock J, Hough R, Rowntree C, et al. Augmented post-remission therapy for a minimal residual disease-defined high-risk subgroup of children and young people with clinical standard-risk and intermediate-risk acute lymphoblastic leukaemia (UKALL 2003): a randomised controlled trial. Lancet Oncol (2014) 15(8):809–18. doi: 10.1016/S1470-2045(14)70243-8
4. Pui CH, Yang JJ, Hunger SP, Pieters R, Schrappe M, Biondi A, et al. Childhood acute lymphoblastic leukemia: progress through collaboration. J Clin Oncol (2015) 33(27):2938–48. doi: 10.1200/JCO.2014.59.1636
5. Ward ZJ, Yeh JM, Bhakta N, Frazier AL, Atun R. Estimating the total incidence of global childhood cancer: a simulation-based analysis. Lancet Oncol (2019) 20(4):483–93. doi: 10.1016/S1470-2045(18)30909-4
6. Ward ZJ, Yeh JM, Bhakta N, Frazier AL, Girardi F, Atun R. Global childhood cancer survival estimates and priority-setting: a simulation-based analysis. Lancet Oncol (2019) 20(7):972–83. doi: 10.1016/S1470-2045(19)30273-6
7. Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet (2018) 391(10125):1023–75. doi: 10.1016/S0140-6736(17)33326-3
8. Global Cancer Observatory . International Agency for Research on Cancer. Available at: https://gco.iarc.fr/today/home (Accessed May 1, 2023).
9. Munoz-Aguirre P, Huerta-Gutierrez R, Zamora S, Mohar A, Vega-Vega L, Hernández-Ávila JE, et al. Acute lymphoblastic leukaemia survival in children covered by seguro popular in Mexico: A national comprehensive analysis 2005-2017. Health Syst Reform (2021) 7(1):e1914897. doi: 10.1080/23288604.2021.1914897
10. Rivera-Luna R, Zapata-Tarres M, Shalkow-Klincovstein J, Velasco-Hidalgo L, Olaya-Vargas A, Finkelstein-Mizrahi N, et al. The burden of childhood cancer in Mexico: Implications for low- and middle-income countries. Pediatr Blood Cancer (2017) 64(6):e26366. doi: 10.1002/pbc.26366
11. Jaime-Perez JC, Lopez-Razo ON, Garcia-Arellano G, Pinzón-Uresti MA, Jiménez-Castillo RA, González-Llano O, et al. Results of treating childhood acute lymphoblastic leukemia in a low-middle income country: 10 year experience in Northeast Mexico. Arch Med Res (2016) 47(8):668–76. doi: 10.1016/j.arcmed.2017.01.004
12. Barr RD, Gomez-Almaguer D, Jaime-Perez JC, Ruiz-Argüelles GJ. Importance of nutrition in the treatment of leukemia in children and adolescents. Arch Med Res (2016) 47(8):585–92. doi: 10.1016/j.arcmed.2016.11.013
13. Ornelas-Sanchez M, Nuno-Vazquez L, Loera-Reyna A, Torres-Reyes D, Rivera-Gómez R, Sánchez A, et al. The "Golden Hour": a capacity-building initiative to decrease life-threating complications related to neutropenic fever in patients with hematologic Malignancies in low- and middle-income countries. Blood Adv (2018) 2(Suppl 1):63–6. doi: 10.1182/bloodadvances.2018GS112240
14. Nuño-Vázquez L, Rivera-Gomez R, Ornelas-Sánchez M, Ribeiro R, Roberts W, Aristizabal P, et al. Capacity-building initiative to improve clinical outcomes in pediatric acute lymphoblastic leukemia in the US-Mexico border region. Blood Adv (2017) 1(Suppl 1):70–3. doi: 10.1182/bloodadvances.2017GS101484
15. Kaplan E MP. Nonparametric estimation from incomplete observations. J Am Stat Assoc (1958) 53:457–81, 1958. doi: 10.1080/01621459.1958.10501452
16. Peto R, Pike MC, Armitage P, Breslow NE, Cox DR, Howard SV, et al. Design and analysis of randomized clinical trials requiring prolonged observation of each patient. Br J Cancer (1977) 35:1–39. doi: 10.1038/bjc.1977.1
17. Gray RJ. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat (1988) 16(3):1141–54. doi: 10.1214/aos/1176350951
18. Rivera-Luna R, Shalkow-Klincovstein J, Velasco-Hidalgo L, Cárdenas-Cardós R, Zapata-Tarrés M, Olaya-Vargas A, et al. Descriptive Epidemiology in Mexican children with cancer under an open national public health insurance program. BMC Cancer (2014) 14:790. doi: 10.1186/1471-2407-14-790
19. Jaime-Perez JC, Pinzon-Uresti MA, Jimenez-Castillo RA, Colunga-Pedraza JE, González-Llano Ó, Gómez-Almaguer D, et al. Relapse of childhood acute lymphoblastic leukemia and outcomes at a reference center in Latin America: organomegaly at diagnosis is a significant clinical predictor. Hematology (2018) 23(1):1–9. doi: 10.1080/10245332.2017.1333294
20. Friedrich P, Lam CG, Kaur G, Itriago E, Ribeiro RC, Arora RS. Determinants of treatment abandonment in childhood cancer: results from a global survey. PloS One (2016) 11(10):e0163090. doi: 10.1371/journal.pone.0163090
21. Bonilla M, Rossell N, Salaverria C, Gupta S, Barr R, Sala A, et al. Prevalence and predictors of abandonment of therapy among children with cancer in El Salvador. Int J Cancer (2009) 125(9):2144–6. doi: 10.1002/ijc.24534
22. Castro-Rios A, Reyes-Morales H, Pelcastre-Villafuerte BE, Rendón-Macías ME, Fajardo-Gutiérrez A. Socioeconomic inequalities in survival of children with acute lymphoblastic leukemia insured by social security in Mexico: a study of the 2007-2009 cohorts. Int J Equity Health (2019) 18(1):40.
23. Inaba H, Pei D, Wolf J, Howard SC, Hayden RT, Go M, et al. Infection-related complications during treatment for childhood acute lymphoblastic leukemia. Ann Oncol (2017) 28(2):386–92. doi: 10.1093/annonc/mdw557
24. O'Connor D, Bate J, Wade R, Clark R, Dhir S, Hough R, et al. Infection-related mortality in children with acute lymphoblastic leukemia: an analysis of infectious deaths on UKALL2003. Blood (2014) 124(7):1056–61. doi: 10.1182/blood-2014-03-560847
25. Jeha S, Pei D, Choi J, Cheng C, Sandlund JT, Coustan-Smith E, et al. Improved CNS control of childhood acute lymphoblastic leukemia without cranial irradiation: St Jude total therapy study 16. J Clin Oncol (2019) 37(35):3377–91. doi: 10.1200/JCO.19.01692
26. Maloney KW, Devidas M, Wang C, Mattano LA, Friedmann AM, Buckley P, et al. Outcome in children with standard-risk B-cell acute lymphoblastic leukemia: results of children's oncology group trial AALL0331. J Clin Oncol (2020) 38(6):602–12. doi: 10.1200/JCO.19.01086
27. Antillon FG, Blanco JG, Valverde PD, Castellanos M, Garrido CP, Girón V, et al. The treatment of childhood acute lymphoblastic leukemia in Guatemala: Biologic features, treatment hurdles, and results. Cancer (2017) 123(3):436–48. doi: 10.1002/cncr.30257
28. Navarrete M, Rossi E, Brivio E, Carrillo JM, Bonilla M, Vasquez R, et al. Treatment of childhood acute lymphoblastic leukemia in central America: a lower-middle income countries experience. Pediatr Blood Cancer (2014) 61(5):803–9. doi: 10.1002/pbc.24911
29. Agulnik A, Cardenas A, Carrillo AK, Bulsara P, Garza M, Alfonso Carreras Y, et al. Clinical and organizational risk factors for mortality during deterioration events among pediatric oncology patients in Latin America: A multicenter prospective cohort. Cancer (2021) 127(10):1668–78. doi: 10.1002/cncr.33411
30. Gonzalez ML, Aristizabal P, Loera-Reyna A, Torres D, Ornelas-Sánchez M, Nuño-Vázquez L, et al. The golden hour: sustainability and clinical outcomes of adequate time to antibiotic administration in children with cancer and febrile neutropenia in Northwestern Mexico. JCO Glob Oncol (2021) 7:659–70. doi: 10.1200/GO.20.00578
31. Sulis ML, Blonquist TM, Stevenson KE, Hunt SK, Kay-Green S, Athale UH, et al. Effectiveness of antibacterial prophylaxis during induction chemotherapy in children with acute lymphoblastic leukemia. Pediatr Blood Cancer (2018) 65(5):e26952. doi: 10.1002/pbc.26952
32. Jaime-Perez JC, Fernandez LT, Jimenez-Castillo RA, Colunga-Pedraza JE, Padilla-Medina JR, Mancías-Guerra C, et al. Hospitalization rate and costs in acute lymphoblastic leukemia of childhood in a low-income group: Financial impact in Northeast Mexico. Pediatr Blood Cancer (2017) 64(12):e26673. doi: 10.1002/pbc.26673
33. Smith M, Arthur D, Camitta B, Carroll AJ, Crist W, Gaynon P, et al. Uniform approach to risk classification and treatment assignment for children with acute lymphoblastic leukemia. J Clin Oncol (1996) 14(1):18–24. doi: 10.1200/JCO.1996.14.1.18
34. Gaynon PS, Trigg ME, Heerema NA, Sensel MG, Sather HN, Hammond GD, et al. Children's Cancer Group trials in childhood acute lymphoblastic leukemia: 1983-1995. Leukemia (2000) 14(12):2223–33. doi: 10.1038/sj.leu.2401939
35. Schrappe M, Reiter A, Ludwig WD, Harbott J, Zimmermann M, Hiddemann W, et al. Improved outcome in childhood acute lymphoblastic leukemia despite reduced use of anthracyclines and cranial radiotherapy: results of trial ALL-BFM 90. German-Austrian-Swiss ALL-BFM Study Group. Blood (2000) 95(11):3310–22.
36. Hunger SP, Mullighan CG. Acute lymphoblastic leukemia in children. N Engl J Med (2015) 373(16):1541–52. doi: 10.1056/NEJMra1400972
37. Pieters R, de Groot-Kruseman H, van der Velden V, Fiocco M, van den Berg H, de Bont E, et al. Successful therapy reduction and intensification for childhood acute lymphoblastic leukemia based on minimal residual disease monitoring: study ALL10 from the dutch childhood oncology group. J Clin Oncol (2016) 34(22):2591–601. doi: 10.1200/JCO.2015.64.6364
38. Vora A, Goulden N, Wade R, Mitchell C, Hancock J, Hough R, et al. Treatment reduction for children and young adults with low-risk acute lymphoblastic leukaemia defined by minimal residual disease (UKALL 2003): a randomised controlled trial. Lancet Oncol (2013) 14(3):199–209. doi: 10.1016/S1470-2045(12)70600-9
39. Place AE, Stevenson KE, VroOman LM, Harris MH, Hunt SK, O'Brien JE, et al. Intravenous pegylated asparaginase versus intramuscular native Escherichia coli L-asparaginase in newly diagnosed childhood acute lymphoblastic leukaemia (DFCI 05-001): a randomised, open-label phase 3 trial. Lancet Oncol (2015) 16(16):1677–90. doi: 10.1016/S1470-2045(15)00363-0
40. Borowitz MJ, Devidas M, Hunger SP, Bowman WP, Carroll AJ, Carroll WL, et al. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia and its relationship to other prognostic factors: a Children's Oncology Group study. Blood (2008) 111(12):5477–85. doi: 10.1182/blood-2008-01-132837
41. Yeoh AE, Ariffin H, Chai EL, Kwok CS, Chan YH, Ponnudurai K, et al. Minimal residual disease-guided treatment deintensification for children with acute lymphoblastic leukemia: results from the Malaysia-Singapore acute lymphoblastic leukemia 2003 study. J Clin Oncol (2012) 30(19):2384–92. doi: 10.1200/JCO.2011.40.5936
42. Pedrosa F, Coustan-Smith E, Zhou Y, Cheng C, Pedrosa A, Lins MM, et al. Reduced-dose intensity therapy for pediatric lymphoblastic leukemia: long-term results of the Recife RELLA05 pilot study. Blood (2020) 135(17):1458–66. doi: 10.1182/blood.2019004215
43. Kahn JM, Cole PD, Blonquist TM, Stevenson K, Jin Z, Barrera S, et al. An investigation of toxicities and survival in Hispanic children and adolescents with ALL: Results from the Dana-Farber Cancer Institute ALL Consortium protocol 05-001. Pediatr Blood Cancer (2018) 65(3):e26871. doi: 10.1002/pbc.26871
44. Arico M, Valsecchi MG, Camitta B, Schrappe M, Chessells J, Baruchel A, et al. Outcome of treatment in children with Philadelphia chromosome-positive acute lymphoblastic leukemia. N Engl J Med (2000) 342(14):998–1006. doi: 10.1056/NEJM200004063421402
45. Perez-Cuevas R, Doubova SV, Zapata-Tarres M, Flores-Hernández S, Frazier L, Rodríguez-Galindo C, et al. Scaling up cancer care for children without medical insurance in developing countries: The case of Mexico. Pediatr Blood Cancer (2013) 60(2):196–203. doi: 10.1002/pbc.24265
Keywords: acute lymphoblastic leukemia, Mexico, diagnostic capacity, low-and middle income countries, pediatric oncology
Citation: Moreira DC, González-Ramella O, Echavarría Valenzuela M, Carrillo AK, Faughnan L, Job G, Chen Y, Villegas C, Ellis Irigoyen A, Barra Urbays R, Ramírez Martinez M, Altamirano Alvarez E, León Espitia JA, López Facundo NA, Colunga Pedraza JE, Reyes Gutierrez FdM, Aguilar Román AB, Tamez Gómez EL, Portillo Zavala CS, Negroe Ocampo NdC, Pulido Sanchez SG, Cortés Alva D, Casillas Toral P, Salas Villa K, Mendoza Sánchez PJ, Pérez Alvarado C, Tamayo Pedraza G, González Zamorano M, Ávila Alba JMR, Becerril Becerril J, Ramírez Durán H, Sandoval Cabrera A, Pineda Gordillo A, de la Rosa Alonso DI, Mejía Marín LJ, Benítez Can LdlÁ, Gutiérrez Martinez I, Jiménez Osorio MI, Echeandia N, Casillas E, Guerrero-Gomez K, Devidas M and Friedrich P (2023) Evaluation of factors leading to poor outcomes for pediatric acute lymphoblastic leukemia in Mexico: a multi-institutional report of 2,116 patients. Front. Oncol. 13:1255555. doi: 10.3389/fonc.2023.1255555
Received: 09 July 2023; Accepted: 21 August 2023;
Published: 18 September 2023.
Edited by:
Juan Carlos Núñez-Enríquez, Instituto Mexicano del Seguro Social, MexicoReviewed by:
Elisa Dorantes, Federico Gómez Children’s Hospital, MexicoRosana Pelayo, Mexican Social Security Institute (IMSS), Mexico
Copyright © 2023 Moreira, González-Ramella, Echavarría Valenzuela, Carrillo, Faughnan, Job, Chen, Villegas, Ellis Irigoyen, Barra Urbays, Ramírez Martinez, Altamirano Alvarez, León Espitia, López Facundo, Colunga Pedraza, Reyes Gutierrez, Aguilar Román, Tamez Gómez, Portillo Zavala, Negroe Ocampo, Pulido Sanchez, Cortés Alva, Casillas Toral, Salas Villa, Mendoza Sánchez, Pérez Alvarado, Tamayo Pedraza, González Zamorano, Ávila Alba, Becerril Becerril, Ramírez Durán, Sandoval Cabrera, Pineda Gordillo, de la Rosa Alonso, Mejía Marín, Benítez Can, Gutiérrez Martinez, Jiménez Osorio, Echeandia, Casillas, Guerrero-Gomez, Devidas and Friedrich. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paola Friedrich, cGFvbGEuZnJpZWRyaWNoQHN0anVkZS5vcmc=