 Lucía Notario1
Lucía Notario1 Marc Cucurull1Gabriela Cerdà1Carolina Sanz2
Marc Cucurull1Gabriela Cerdà1Carolina Sanz2 Enric Carcereny1Ana Muñoz-Mármol2
Enric Carcereny1Ana Muñoz-Mármol2 Ainhoa Hernández1
Ainhoa Hernández1 Marta Domènech1
Marta Domènech1 Teresa Morán1
Teresa Morán1 Montse Sánchez-Céspedes3Marta Costa4Jose-Luis Mate2
Montse Sánchez-Céspedes3Marta Costa4Jose-Luis Mate2 Anna Esteve5
Anna Esteve5 Maria Saigí1*
Maria Saigí1*- 1Medical Oncology Department, Catalan Institute of Oncology (ICO)-Badalona, Germans Trias i Pujol University Hospital (HUGTiP), Badalona-Applied Research Group in Oncology (B-ARGO), Germans Trias i Pujol Research Institute (IGTP), Badalona, Barcelona, Spain
- 2Pathology Department, Germans Trias i Pujol University Hospital (HUGTiP), Germans Trias i Pujol Research Institute (IGTP), Badalona, Barcelona, Spain
- 3Cancer Genetics Group, Josep Carreras Leukaemia Research Institute (IJC), Badalona, Barcelona, Spain
- 4Badalona-Applied Research Group in Oncology (B-ARGO), Germans Trias i Pujol Research Institute (IGTP), Badalona, Barcelona, Spain
- 5Statistics Department, Catalan Institute of Oncology (ICO)-Badalona, Applied Research Group in Oncology (B-ARGO), Germans Trias i Pujol Research Institute (IGTP), Badalona, Barcelona, Spain
Approximately 20% of lung adenocarcinomas harbor activating mutations at KRAS, an oncogene with the ability to alter the tumor immune microenvironment. In this retrospective study, we examined 103 patients with KRAS-mutant lung adenocarcinoma who were treated with immunotherapy-based regimens and we evaluated the clinical outcomes according to PD-L1 expression and the type of KRAS mutation. Among all patients included, 47% carried KRAS G12C mutation whereas 53% harbored KRAS non-G12C mutations. PD-L1 status was available for 77% of cases, with higher expression among KRAS G12C tumors (p = 0.01). Better overall survival and progression-free survival were observed in high PD-L1 expression tumors, regardless of KRAS mutation type. The heterogeneous nature of KRAS-mutant tumors and the presence of other co-mutations may contribute to different outcomes to immunotherapy-based strategies.
Highlights
● KRAS G12C mut LuADs are significantly associated with high PD-L1 expression.
● Better clinical outcomes are associated with high PD-L1 expression, regardless of KRAS mut type.
● A subset of long-term responders (LTR) to IT-based regimens were enriched with KRAS G12C mut and high PD-L1 expression.
Introduction
Lung adenocarcinoma (LuAD) harbors a significant number of targetable oncogenic mutations among lung cancer. The most common oncogenic mutations are found in KRAS, occurring in 20%–25% of the cases. These mutations primarily affect codons 12 (85%) and 13 (10%), found in exon 2, and codon 61 (5%), found in exon 3. The KRAS G12C mutation, resulting in a change from glycine to cysteine, prevails in 43% of the cases and is associated with tobacco exposure. In contrast, non-smokers, commonly exhibit G12D mutations, a change from glycine to aspartic acid, and G12V mutations, a change from glycine to valine (1).
Currently, the standard first-line treatment for patients with KRAS G12C LuADs involves IT-based regimens, either combined or not with platinum-based chemotherapy (ChT) according to PD-L1 expression levels. Mazieres et al., in a retrospective cohort, demonstrated that KRAS-driven tumors express higher rates of PD-L1 and present higher tumor mutational burden compared with other oncogenic alterations, suggesting that it might predict better responses to IT (2). However, the study did not evaluate the existing differences based on the type of KRAS mutation. On the other hand, most phase III pivotal trials with IT did not stratify by KRAS status, and the efficacy of IT according to KRAS mutation subtype remains to be determined (3).
Recently, the emergence of novel allosteric inhibitors of KRAS G12C is expected to change the paradigm of treatment approach for these tumors. Phase I/II trials with sotorasib and adagrasib presented an overall response rate (ORR) of 32% and 45%, respectively, along with an acceptable toxicity. As a result, these inhibitors have received the approval of the Food and Drug Administration (FDA) for the treatment of patients with KRAS G12C mutations after progression to initial therapy (4, 5). To further enhance the outcomes, novel drugs such as BI-3406 which disrupts the interaction of SOS1-KRAS, as well as TNO155, which inhibits SHP2, a protein that integrates growth and differentiation signals from receptor tyrosine kinases into the RAS/MAPK cascade, are being evaluated. These drugs in combination with sotorasib or adagrasib are being studied to improve treatment outcomes (5). Additionally, there have been promising findings from preclinical models combining PD-1 inhibitors with KRAS G12C-specific inhibitors. These combinations are being addressed in clinical trials (NCT04613596).
As a result, targeting KRAS beyond KRAS G12C inhibitors has emerged as a significant and rapidly evolving area of research. This refers not only to the development of novel therapeutic strategies targeting KRAS but also to the immunoregulatory role of KRAS and the effectiveness of current immunotherapies in KRAS-driven tumors, which has not been directly addressed in the literature. Of note, KRAS G12C-mutant tumors are commonly associated with tobacco exposure and exhibit higher tumor mutational burden, which might predict better responses to IT (6). We hypothesized that those patients might present better clinical outcomes to IT-based therapies.
In this work, we aim to study the clinical outcomes of existing immunotherapies based on the type of KRAS mutation and PD-L1 expression levels. We will examine a cohort of patients with metastatic KRAS-mutant tumors treated with IT-based regimens in our daily practice.
Methods
Study population
A medical record search was used to identify patients treated at the Catalan Institute of Oncology (ICO)-Badalona with a primary tumor diagnosis of NSCLC harboring KRAS mut and treated with IT-based regimens for metastatic disease, from June 2013 to June 2020. Clinical data were retrospectively collected, and patient consent forms were obtained with the approval of the local Institutional Review Board (PI-19-275).
Molecular analysis and PD-L1 expression
The KRAS mutation status was determined by analyzing the primary tumor. The tumor tissue samples were tested by KRAS Idylla Mutation Test (Biocartis), a real-time PCR test designed for the identification of mutations in codons 12, 13, and 61; in the most recent cases (2020–2021), they were tested by the NGS panels: Oncomine Solid Tumour, Oncomine Focus Assay, or Oncomine Comprehensive Assay (Thermo Fisher) which includes 22, 52, and 164 genes, respectively, involved in lung cancer pathogenesis. The PD-L1 status in tumor cells was determined by immunohistochemistry (IHC) assay (Ventana clone SP263), and it was categorized as follows: negative <1%, low 1%–49%, and high 50%–100% expression.
Statistical analysis
Clinical characteristics, KRAS mutation type, and line of IT treatment were collected for all patients. We classified patients into two groups based on the KRAS mutation type: G12C or non-G12C. Baseline characteristics were compared using the chi-square and Fisher’s exact test for categorical data. Survival Kaplan–Meier model was used to estimate survival, and medians were compared between groups using the log-rank test. Progression-free survival (PFS) to IT was calculated from the time of IT initiation to date of disease’s progression or death, whichever occurred first. Overall survival (OS) was calculated from the time from starting IT treatment to date of death or last follow-up. The assessment of best overall response (ORR) to IT was performed according to RECIST 1.1 criteria, and response rates were compared between groups using the chi-square test. We defined a subset of long-term responders (LTR) to IT, defined as those patients who did not progress within 24 months after IT treatment initiation.
Results
Clinical and molecular characteristics according to KRAS mut type
We identified 103 patients with metastatic non-small cell lung cancer harboring KRAS mutations from June 2013 to June 2020, n = 47 KRAS G12C, n = 52 KRAS non-G12C, n = 4 unknown. PD-L1 was available in 78 cases (77%). Clinical and molecular characteristics according to KRAS mut type are shown in Table 1. The distribution of KRAS mutations in our non-G12C sub-cohort (n = 52) was as follows: G12V (n = 16), G12A (n = 12), G12D (n = 8), G13C (n = 5), and the frequency of the rest of mutations (G12S, G12F, G13D, Q61H) were below 5.
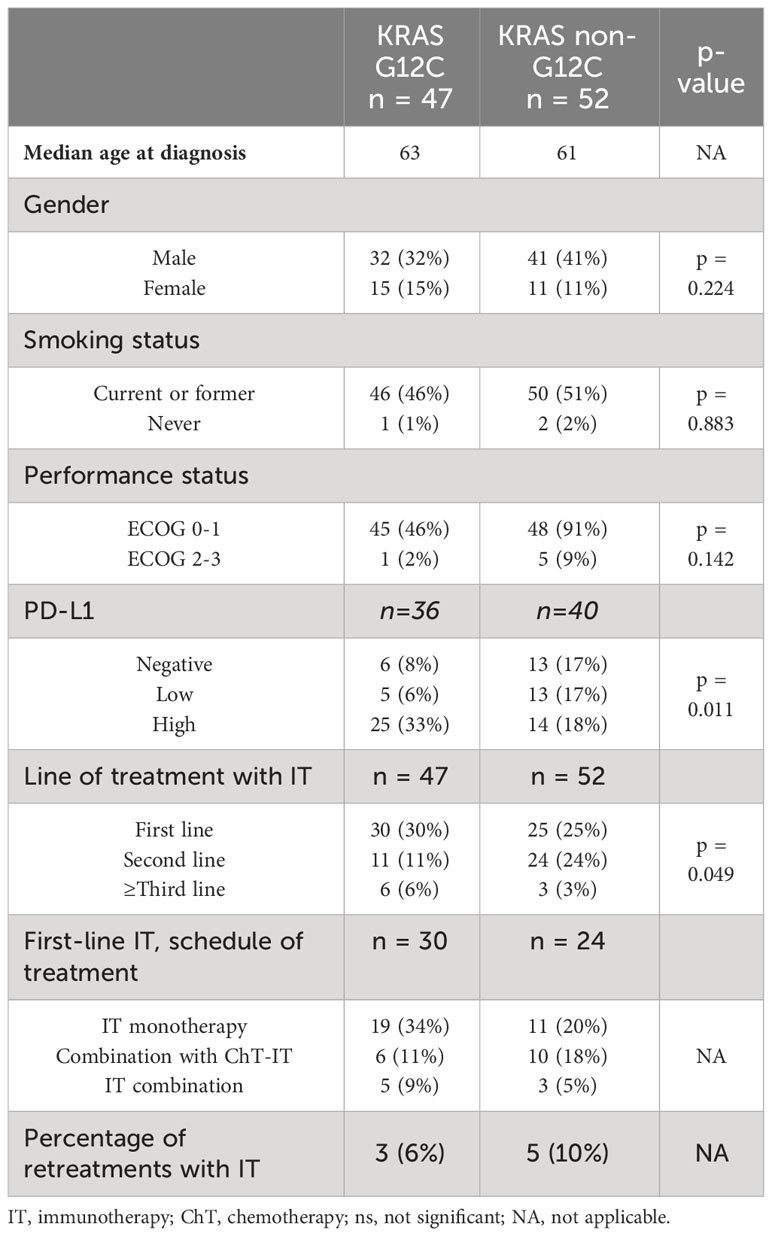
Table 1 Patient characteristics by KRAS mutation (KRAS G12C vs. non-G12C).
Clinical outcomes in KRAS mutant patients treated with IT
All patients included in the study were treated with IT for advanced disease: 54% in the first line, 36% in the second line, and 10% in the third or further lines. Overall, 19 patients (20%) were treated within clinical trials. Treatment schedules included different IT-based regimens at that period for the first line: ChT-IT (30%) with platinum-based doublet; IT–IT (15%); and/or IT alone (55%), the anti-PD(L)-1-based regimen being the most prevalent one (Table 1).
PD-L1 status was available in 77% of cases: 39% high, 19% low, and 19% negative. High PD-L1 (≥50%) was predominantly found in KRAS G12C vs. non-G12C (64% vs. 36%, p = 0.01). However, no statistically significant differences were observed in the overall response rate (ORR) to IT according to KRAS mut type: 49% of patients with KRAS G12C obtained partial or complete response compared with 42% in the non-G12C group, p value = 0.2 (Figure 1).
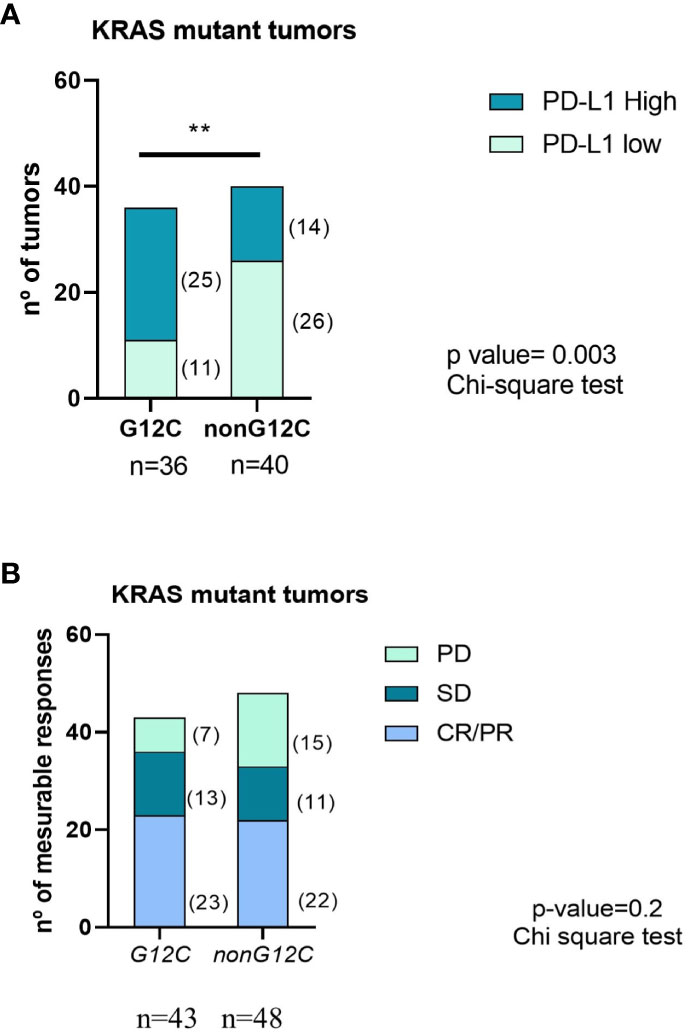
Figure 1 PD-L1 status (A) and ORR to IT (B) according to KRAS mutation type. PD, Progressive disease; SD, Stable disease; CR/PR, Complete/Partial response. ** means statistically significant with p-value <0.005 using chi-square test.
After a median follow-up of 26.5 months (m), the mPFS of the entire cohort was 13.3 m (95% CI 5.6-20.9) and the mOS was 17.9m (95% CI 15.5–20.3). Significant differences were observed in mPFS to IT according to PD-L1 expression, regardless of the line of treatment they received the IT: 23.1 m (95% CI 18.1–28.1) in PDL1 ≥50% vs. 10.1 m (2.5–17.6) in PDL1 <50% (p-value 0.045). However, we could not demonstrate significant differences in mPFS to IT according to KRAS G12C vs. no-G12C: 10.1 m (2.2–18) vs. 13.3 m (2.4–24.3), p = 0.612, respectively (Figure 2). No significant differences in median overall survival (mOS) were neither observed in G12C vs. non-G12C: 17.9 m (16.6–19.2) vs. 20.6 m (12.6–28.5), p = 0.39.
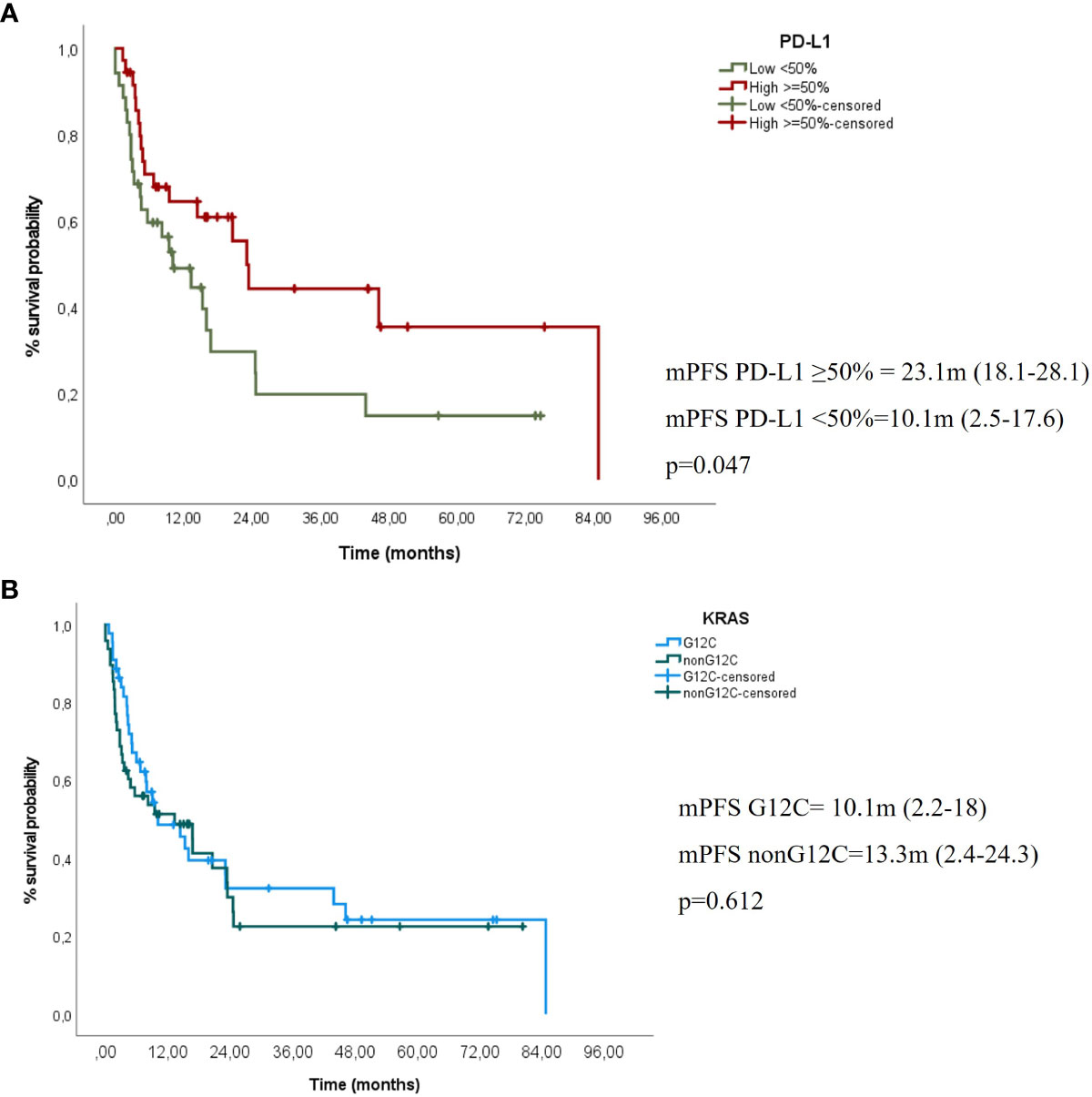
Figure 2 (A) mPFS to IT according to PD-L1 expression (high ≥50% vs. negative/low <50% (B) mPFS to IT according to KRAS mutation type (KRAS G12C vs. non-G12C).
In addition, in the most recent cases available for NGS (n = 30), we could determine KRAS mutant allele frequency, which in our cohort varies from 7.1% to 84.9%, with a mean value of 40.15%. Notably, no statistically significant differences were observed in terms of PFS or OS when employing the mean as a threshold (data details are not presented).
Finally, we identified a subset of LTR to IT (n = 17, 16%). Although not significant, they were enriched with KRAS G12C mutations (64%, p-value = 0.09) and high PDL1 expression (57%, p-value = 0.1) compared with the non-LTR, with no significant clinical differences.
Discussion
In our cohort, we observed that tumors harboring KRAS G12C mutations were significantly associated with higher expression of PD-L1, as compared with KRAS non-G12C. No significant differences were observed according to the smoking habit or clinical characteristics. We also observed that patients with high PDL1 expression presented better mPFS to IT-based regimens compared with low PD-L1, regardless of the line they received the IT. However, we did not observe significant differences in mPFS to IT according to KRAS mutation type, despite the tendency of KRAS G12C to present better ORR to IT as compared with KRAS non-G12C.
Several phase III trials evaluating the efficacy of IT in NSCLC did not stratify by KRAS status, and only post-hoc analyses have been performed on that subset. Results remain controversial. While IT alone given as a first-line therapy seems to favor KRAS-mutant tumors compared with KRAS-wild type, no differences were observed when IT is given in further lines of treatment (3, 7) Another study from real-world data published by Frost et al. from a multicenter and retrospective study evaluated the efficacy of first-line pembrolizumab in 119 patients with KRAS-mutant LuADs with high PD-L1 expression (≥50%). Co-mutations in TP53 were also evaluated. Patients with KRAS G12C/TP53 had significantly higher ORR (100% vs. 27.3%; p = 0.003) and longer mPFS (33.3 vs. 2.8 months; HR, 0.18; 95% CI: 0.06–0.53; p = 0.002) than tumors with KRAS non-G12C/TP53 mutations suggesting that KRAS G12C present better outcomes to immune-based therapies depending also on the co-mutation partners (8).
We also observed that the benefit of using IT was maintained for a subset of patients for at least ≥24 months after initiating IT. These patients, known as long-term responders (LTR), constitute 16% of our cohort population and were predominantly KRAS G12C and enriched with high PDL1 expression, although no significant differences were observed. The available literature lacks substantial information regarding tumor and patient’s characteristics of the LTR, although a few authors have suggested a potential association with adenocarcinoma histopathology and high PD-L1 expression (9).
One of the limitations of our study is the heterogeneity of the IT-based regimens that patients have received, which impairs to reach definitive conclusions. Only 16 patients received ChT-IT for the first-line setting (30%), which nowadays is the standard of care for tumors with PD-L1 <50%, regardless of the KRAS mutation status. Another caveat is the lack of the NGS profile for most of the patients included in the study, which was only performed in the most recent cases (2020–2021) due to diagnostic protocols in our daily clinical practice. Currently, next-generation sequencing (NGS) is the gold standard for molecular diagnosis in lung cancer since it provides a broad genetic information that helps to determine the therapeutic options. Optimizing novel panels including a wide range of genes related with carcinogenesis are becoming the standard of care. However, despite the advantages of the NGS technology, access to NGS panels varies broadly among the different areas and health systems worldwide. Co-mutations such as STK11, KEAP1, or TP53 are emerging as predictive markers of response to IT, particularly in those patients with KRAS G12C mutations (10). In addition, in contrast to KRAS Idylla real-time PCR, NGS panels allow us to identify the KRAS mutant allele fraction, although in our cohort, additional subanalysis stratifying by KRAS mutant allele fraction did not allow to elucidate relevant differences in clinical outcomes. It is becoming essential to assess the genetic profile to predict different outcomes when testing different therapeutic strategies.
Another relevant topic to be addressed is the predictive value to PD-(L)1 blockade among KRAS non-G12C mutations. In this current work comprising more than 2,000 KRAS mutant LC patients, Ricciuti et al. show that KRAS G12D mutant patients harbor distinct clinical, genomic, and immunologic features and present worse clinical outcomes to PD-(L)1 blockade. Owing to the limited size of our subcohort, definitive conclusions referring to this aspect could not be reached. These inquiries continue to be of considerable interest and merit in-depth exploration within more extensive patients cohorts (11). Finally, in four cases, the KRAS mutation subtype was unknown because we could not access this piece of information. Those patients were remitted from other hospitals, and this constitutes another caveat of the retrospective nature of our study.
On the other hand, the strength of this study is the sample size from a multidisciplinary oncologic institution, and the long-term follow-up for all the patients included, which will help to elucidate the role of current IT in KRAS-mutant LuAD patients and the impact on OS, including a subset of LTR, in the era of the incorporation of KRAS G12C-specific inhibitors.
Future directions in the therapeutic landscape will focus on how to integrate IT with KRAS G12C inhibitors or panKRAS inhibitors. Recently the first data of the Codebreak 100/101 study, evaluating the combination of anti-PD(L)1 pembrolizumab or atezolizumab with sotorasib in KRAS G12C-mutant patients, showed promising results and represents a novel potential strategy. However, the balance between efficacy and toxicity with the combination, particularly grade 3–4 hepatotoxicity, remains crucial in this setting (NCT03600883, NCT04185883) (12).
In conclusion, despite that no significant differences were observed in IT-based regimens in lung cancer patients according to the type of KRAS mutation (G12C vs. non-G12C), efforts to find novel predictive biomarkers in addition to PD-L1 for KRAS mutant patients will help to tailor treatment in this specific population and offer them rationally designed therapeutic strategies combining both IT-based regimens with targeted therapy.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Germans Trias i Pujol Institutional Review Board (PI-19-275). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a by- product of routine care or industry. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
LN: Conceptualization; Data curation; Formal analysis; Writing: original draft; review & editing. MCu: Formal analysis; Writing: original draft; review & editing. GC: review & editing. CS: Data curation; Formal analysis, review & editing. EC: Conceptualization; review & editing. AM-M: Data curation; Formal analysis, review & editing. AH: review & editing. MD: review & editing. TM: review & editing. MS-C: review & editing. MCo: review & editing. J-LM: review & editing. AE: Data curation; Formal analysis; review & editing. MS: Conceptualization; Data curation; Formal analysis; Writing: original draft; review & editing. All authors contributed to the article and approved the submitted version.
Acknowledgments
LN received an SCBO grant. MD is supported by a Rio Hortega contract from the Instituto de Salud Carlos III (ISC-III) (CM19/0068). MS is currently supported by a Joan Rodés contract from the ISC-III (JR20/00015). We thank Ulises Ferrandiz for his support in clinical data management. We also thank the Mentoring program at ICO Badalona, which logistically supports the realization of the current work.
Conflict of interest
TM reports Consulting/Advisory Role fees by Roche, Bristol Myers, Boehringer, and Astra Zeneca; Research Funding Grant by Kyowa Kirin and Janssen, all of them unrelated with the current work. MS reports a sponsored research agreement with Merck Serono and Roche Farma outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Herbst, Roy S, Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature (2018) 553:446–54. doi: 10.1038/nature25183
2. Mazieres J, Drilon A, Lusque A, Mhanna L, Cortot AB, Mezquita L, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol (2019) 30(8):1321–8. doi: 10.1093/annonc/mdz167
3. Noordhof AL, Damhuis RAM, Hendriks LEL, de Langen AJ, Timens W, Venmans BJW, et al. Prognostic impact of KRAS mutation status for patients with stage IV adenocarcinoma of the lung treated with first-line pembrolizumab monotherapy. Lung Cancer (2021) 155:163–9. doi: 10.1016/j.lungcan.2021.04.001
4. Skoulidis F, Li BT, Dy GK, Price TJ, Falchook GS, Wolf J, et al. Sotorasib for lung cancers with KRAS P.G12C mutation. New Engl J Med (2021) 384:2371–2381. doi: 10.1056/nejmoa2103695
5. Cucurull M, Notario L, Sanchez-Cespedes M, Hierro C, Estival A, Carcereny E, et al. Targeting KRAS in lung cancer beyond KRAS G12C inhibitors: the immune regulatory role of KRAS and novel therapeutic strategies. Front Oncol (2022) 11:793121. doi: 10.3389/fonc.2021.793121
6. Goodman AM, Kato S, Bazhenova L, Patel SP, Frampton GM, Miller V, et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers Mol Cancer Ther (2017) 16:2598–608. doi: 10.1158/1535-7163.mct-17-0386
7. Passiglia F, Cappuzzo F, Alabiso O, Bettini AC, Bidoli P, Chiari R, et al. Efficacy of nivolumab in pre-treated non-small-cell lung cancer patients harbouring KRAS mutations. Br J Cancer (2019) 120:57–62. doi: 10.1038/s41416-018-0234-3
8. Frost N, Kollmeier J, Vollbrecht C, Grah C, Matthes B, Pultermann D, et al. KRASG12C/TP53 co-mutations identify long-term responders to first line palliative treatment with pembrolizumab monotherapy in PD-L1 high (≥50%) lung adenocarcinoma. Trans Lung Cancer Res (2021) 10:737–52. doi: 10.21037/tlcr-20-958
9. Frigola J, Navarro A, Carbonell C, Callejo A, Iranzo P, Cedrés S, et al. Molecular profiling of long-term responders to immune checkpoint inhibitors in advanced non-small cell lung cancer. Mol Oncol (2021) 15(4):887–900. doi: 10.1002/1878-0261.12891
10. Skoulidis F, Byers LA, Diao L, Papadimitrakopoulou VA, Tong P, Izzo J, et al. Co-occurring genomic alterations define major subsets of KRAS-mutant lung adenocarcinoma with distinct biology, immune profiles, and therapeutic vulnerabilities. Cancer Discovery (2015) 5:860–77. doi: 10.1158/2159-8290.cd-14-1236
11. Ricciuti B, Alessi JV, Elkrief A, Wang X, Cortellini A, Li YY, et al. Dissecting the clinicopathologic, genomic, and immunophenotypic correlates of KRASG12D-mutated non-small-cell lung cancer. Ann Oncol (2022) 33(10):1029–40. doi: 10.1016/j.annonc.2022.07.005
Keywords: non-small cell lung cancer, lung adenocarcinoma, KRAS, PD-L1, immunotherapy
Citation: Notario L, Cucurull M, Cerdà G, Sanz C, Carcereny E, Muñoz-Mármol A, Hernández A, Domènech M, Morán T, Sánchez-Céspedes M, Costa M, Mate J-L, Esteve A and Saigí M (2023) Characterization of a cohort of metastatic lung cancer patients harboring KRAS mutations treated with immunotherapy: differences according to KRAS G12C vs. non-G12C. Front. Oncol. 13:1239000. doi: 10.3389/fonc.2023.1239000
Received: 12 June 2023; Accepted: 02 October 2023;
Published: 17 October 2023.
Edited by:
Wouter H. Van Geffen, Medical Center Leeuwarden, NetherlandsReviewed by:
Francesco Pepe, University of Naples Federico II, ItalyIgnacija Vlašić, Rudjer Boskovic Institute, Croatia
Copyright © 2023 Notario, Cucurull, Cerdà, Sanz, Carcereny, Muñoz-Mármol, Hernández, Domènech, Morán, Sánchez-Céspedes, Costa, Mate, Esteve and Saigí. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Saigí, bXNhaWdpQGljb25jb2xvZ2lhLm5ldA==