 Natalia Cichowska-Cwalińska1,2
Natalia Cichowska-Cwalińska1,2 Michał Bieńkowski3Marta Popęda3Magdalena Dróżka1Jacek Rutkowski1
Michał Bieńkowski3Marta Popęda3Magdalena Dróżka1Jacek Rutkowski1 Jacek Jassem1
Jacek Jassem1 Renata Zaucha1*†
Renata Zaucha1*†- 1Department of Oncology and Radiotherapy, Medical University of Gdańsk, Gdańsk, Poland
- 2Early Phase Clinical Trials Centre, Medical University of Gdańsk, Gdańsk, Poland
- 3Department of Pathomorphology, Medical University of Gdańsk, Gdańsk, Poland
Aim: We hypothesized that markers of inflammation correlate with response to radiotherapy in patients with non-metastatic laryngeal cancer (LC). Our aim was to assess peripheral and local markers of inflammation including lymphocyte to monocyte ratio (LMR), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), infiltrating CD8+ lymphocytes (TILsCD8), and programmed death 1 ligand (PD-L1) expression.
Methods: We performed a retrospective single-center analysis of LC patients administered definitive (R-RT) or postoperative radiotherapy (PORT). The primary endpoint was overall survival (OS) in relation to peripheral and local inflammatory markers and their dynamic changes during RT.
Results: Study group included 215 patients (R-RT, n=116; PORT, n=99). The baseline (t0) NLR and LMR were significantly correlated with OS in the R-RT group. In patients with high and low NLR at t0, the five-year OS was 33% and 56% (p=0.010) and in high and low LMR at t0, the five-year OS was 56% and 27% (p=0.003), respectively. The LMR increase during R-RT predicted better prognosis: the five-year OS in high and low LMR was 57% and 31% at t2 (after 2 weeks of RT) (p=0.015), 49% and 26% at t4 (p< 0.001), and 50% and 25% at t6 (p=0.013), respectively. Multivariable analysis shows that the worse performance status (p=0.003), the presence of nodal metastases (p=0.0001), and low baseline LMR (p=0.049) in the R-RT group, and the presence of nodal metastases (p=0.035) and completion treatment on time (p=0.042) in PORT group were associated with poor prognosis. The PD-L1 expression had no significant prognostic value in any of the examined patients.
Conclusion: The baseline LMR and its dynamic changes during R-RT and baseline NLR are independent prognostic factors in patients with nonmetastatic LC. PD-L1 expression and number of TILsCD8 have no prognostic value in R-RT and PORT group.
Introduction
Laryngeal cancer (LC) is the second most common cancer of the head and neck (HNC) region globally, after oral cavity and lip cancers with 184,500 new cases and around 100,000 deaths per year (1). In this group surgery, followed by postoperative radiotherapy (PORT) or definitive radio-chemotherapy (R-RT) and recently approved immunotherapy remain the gold standard treatments for patients with nonmetastatic advanced LC.
Unfortunately, despite the presence of early symptoms, the majority of LC cases present with locally advanced disease (2–4). The tumor stage and location, as well as the patient’s age, and performance status significantly impact the treatment outcomes. The five-year local failure rates (five-year LFR), regional failure rates (RFR), and distant failure rates (DFR) are 11%, 6%, and 19%, respectively (5, 6).
Cancer patients show local and systemic immune alterations (7, 8); consequently, peripheral blood cells, including neutrophils, lymphocytes, monocytes, and platelets, represent easy-to-evaluate immune system markers to impact prognosis (9–14). Variations in their numbers were shown in several cancer types, including mesothelioma, pancreatic cancer, renal cell carcinoma, and non–small cell lung cancer (9–15). Whether these variations represent a surrogate for the increased tumor burden or a tumor-associated immunological process is unclear (9). Chemokines and other inflammatory cytokines can be produced by both cancer and host immune cells, and can promote carcinogenesis as well as tumor progression. Lymphocytes and monocytes are involved in cancer proliferation, tumor cell invasion, and metastasis (16, 17), and increased numbers of monocytes correlate with the immune tolerance of cancer (10).
The clearest relationship between pretreatment lymphocyte to monocyte ratio (LMR), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and survival has been shown in patients with metastatic disease (10, 14, 15, 18, 19). The dynamic changes in these parameters during or after radiotherapy may also have prognostic value (20, 21). These phenomena have been investigated in nasopharyngeal cancers and breast cancers treated with either definitive or adjuvant radiotherapy (19, 21), whereas their impact in LC is unclear. In this study, we evaluated prognostic baseline LMR, NLR, and PLR value, and radiation-induced LMR value changes in patients with non-metastatic LC. We also assessed the correlation of immune markers in primary tumors on OS.
Materials and methods
Patients and data collection
The study group comprised 215 consecutive patients with nonmetastatic LC confirmed by the multidisciplinary head and neck cancer tumor board who underwent R-RT or PORT at the Department of Clinical Oncology and Radiotherapy of the Medical University of Gdansk between 2012 and 2018. We retrospectively analyzed medical records for clinical characteristics, demographic data, treatment parameters, laboratory values, and survival. We calculated the baseline LMR, NLR, and PLR from blood counts (CBC) obtained within 15 days before treatment initiation. We also assessed the changes in LMR after 2 (t2), 4 (t4), and 6 (t6) weeks from RT initiation. We also performed a retrospective analysis of infiltrating CD8+ lymphocytes (TILsCD8) and programmed death 1 ligand (PD-L1) expression status in the archival biospecimens of the untreated primary tumor.
Pathological assessment
Formalin-fixed paraffin-embedded tissue blocks were collected from tumor resections or diagnostic biopsies of primary tumor. Tissue microarrays (TMA), comprising three representative tissue cores (1.5 mm in diameter) for each patient, were prepared using the Manual Tissue Arrayer MTA-1 (Beecher Instruments, Inc., USA). Non-neoplastic tissues (tonsil and placenta) served as positive and negative staining controls, respectively. The TMA sections were first stained with hematoxylin and eosin to verify the invasive neoplastic content within each core. Next, consecutive sections were stained with IVD-grade antibodies, anti-PD-L1 (SP263) and anti-CD8 (SP57), using the automated BenchMark ULTRA IHC/ISH system (Roche Diagnostics, Switzerland). Pathological evaluation was performed by a board-certified pathologist (MB). The immunohistochemical analysis of the tissue arrays were unblinded. PD-L1 expression was assessed in tumor cells (TCs). Cells with complete membrane staining were considered positive, and the proportions of positive cells in each core (rounded to 10%) were determined. For statistical analysis, the patients were divided into three groups: consistently negative (all cores with no positive cells), heterogeneous, and consistently PD-L1 high (const-high, all cores with >30% positive cells). The numbers of infiltrating CD8+ lymphocytes within the tumor parenchyma (stromal lymphocytes were excluded) were determined for each core. Next, for each patient, the mean number of TILsCD8 per 1.76 mm2 (i.e., the area of a single core) of invasive tumor was calculated and recorded semi-quantitatively. Scores of <5, 6–50, 51–199, and ≥200 lymphocytes per core were rated as immunoscores (IMs) of 0, 1, 2, and 3, respectively. For statistical analyses, patients were divided into two groups: TILsCD8-negative (IM = 0) and TILsCD8-positive (IM ≥ 1).
Treatment
All patients were treated in accordance with the departmental guidelines based on international recommendations and multidisciplinary decisions (22–25). Board-certified specialists in head and neck radiation oncology contoured the required target volumes and then prepared radiotherapy plans in accordance with International Commission on Radiation Units & Measurements (ICRU) report 83. All patients received photon radiotherapy using intensity modulated radiation therapy (IMRT) or volumetric modulated arc therapy (VMAT). The total dose was 66 Gy for R-RT and 54 Gy for PORT, with fractional doses in the range of 1.8 - 2.2 Gy. Medical physicists designed the treatment plans using the Eclipse system. Concomitant chemotherapy consisted of cisplatin (DDP) given at a dose of 100 mg/m2 i.v. at three-week intervals or 40 mg/m2 i.v. once a week. The overall survival time was defined as the time from the start of treatment to the date of death or to the date of last follow-up contact for patients still living.
Statistical analysis
Data were analyzed and visualized using the R computing environment (4.1.2) (26). Receiver operating characteristic (ROC) curves were plotted for LMR, NLR, and PLR vs. death using the “pROC” package to select the optimal cut-off values for further dichotomization (27). The associations between LMR, NLR, PLR, TILsCD8, PD-L1 status and clinicopathological characteristics were assessed using the Mann-Whitney-Wilcoxon for continuous variables and the chi-square test for categorical variables. The associations with OS, the primary end point, were evaluated using univariable and multivariable Cox regression models, and Hazard Ratios (HRs) and corresponding 95% confidence intervals (CIs) were reported. All variables with a statistically significant univariate association were included in the multivariate model. Differences in OS between groups were assessed using the log-rank test and visualized with Kaplan-Meier curves using the “ggplot2” (28) and “survminer” packages (29). A p value < 0.05 without multiple testing adjustments was considered statistically significant.
Results
The baseline characteristics of the 215 patients are presented in Table 1. The study group included more men than women (79% vs. 21%) and the median age was 62 years (range 36 to 93). A total of 215 patients received R-RT and PORT. All patients completed the intended radiotherapy. In ten patients, the total RT time was prolonged due to serious treatment-related complications (seven in R-RT and three in PORT). After a median follow-up of approximately 5 years (57.3 months), the median OS for the whole group was 6.6 years (79.7 months). The five-year OS for all patients was 70%.
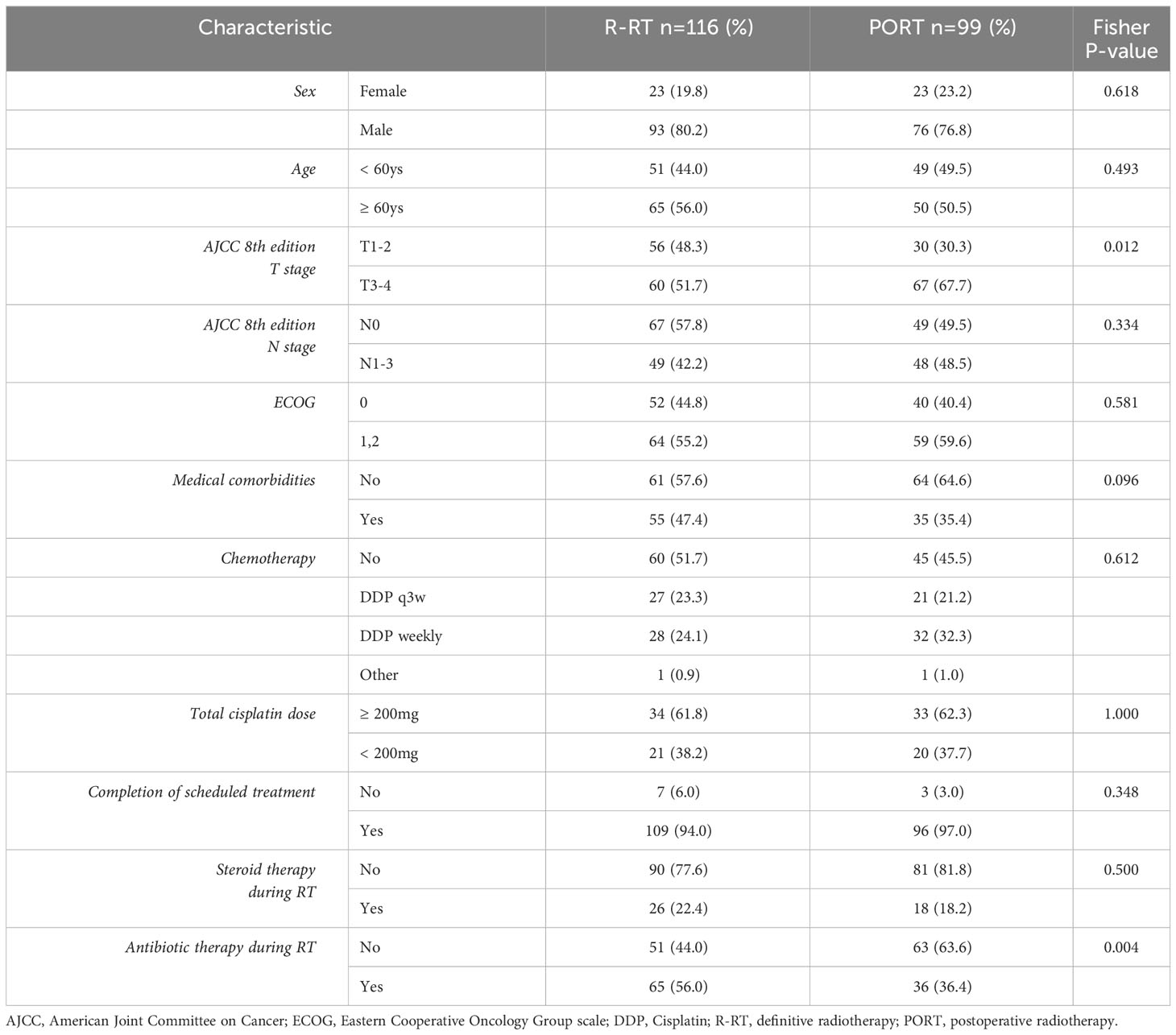
Table 1 Baseline characteristics of patients with laryngeal cancer treated with R-RT and PORT.
In univariate analysis the baseline performance status (ECOG ≥ 1; p = 0.0038), anemia (Hg<12.5g%; p = 0.02), and presence of nodal metastases (N ≥ 1; p = 0.00048) were significantly negatively correlated with treatment outcomes in the R-RT group. The only poor prognostic factor with statistical significance in the PORT group was any lymph node involvement (N ≥ 1 vs. N0, p = 0.043) (univariate analysis).
The DDP regimen (100 mg/m2 q3w or 40 mg/m2 q1) had no impact on OS in both groups. Patients in the R-RT group who received DDP at a total dose equal to or greater than 200 mg/m2 (n=34) showed markedly longer median five-year OS than patients who received less than 200 mg/m2 (n=21) (p<0.001). In the PORT group, the median OS was not achieved.
Significant univariable risk factors for the primary endpoint (OS) were entered as covariates in multivariable Cox regression models (Tables 2, 3). Clinical variables independently associated with OS in multivariable analysis in the R-RT group included the baseline performance status (ECOG ≥ 1; 0.003), the presence of nodal metastases (p=0.0001), and baseline LMR (p=0.049). The only variables that were independently associated with five-year OS in multivariable analysis in PORT group were the presence of nodal metastases (p=0.035) and completion of planned treatment on time (p=0.042).
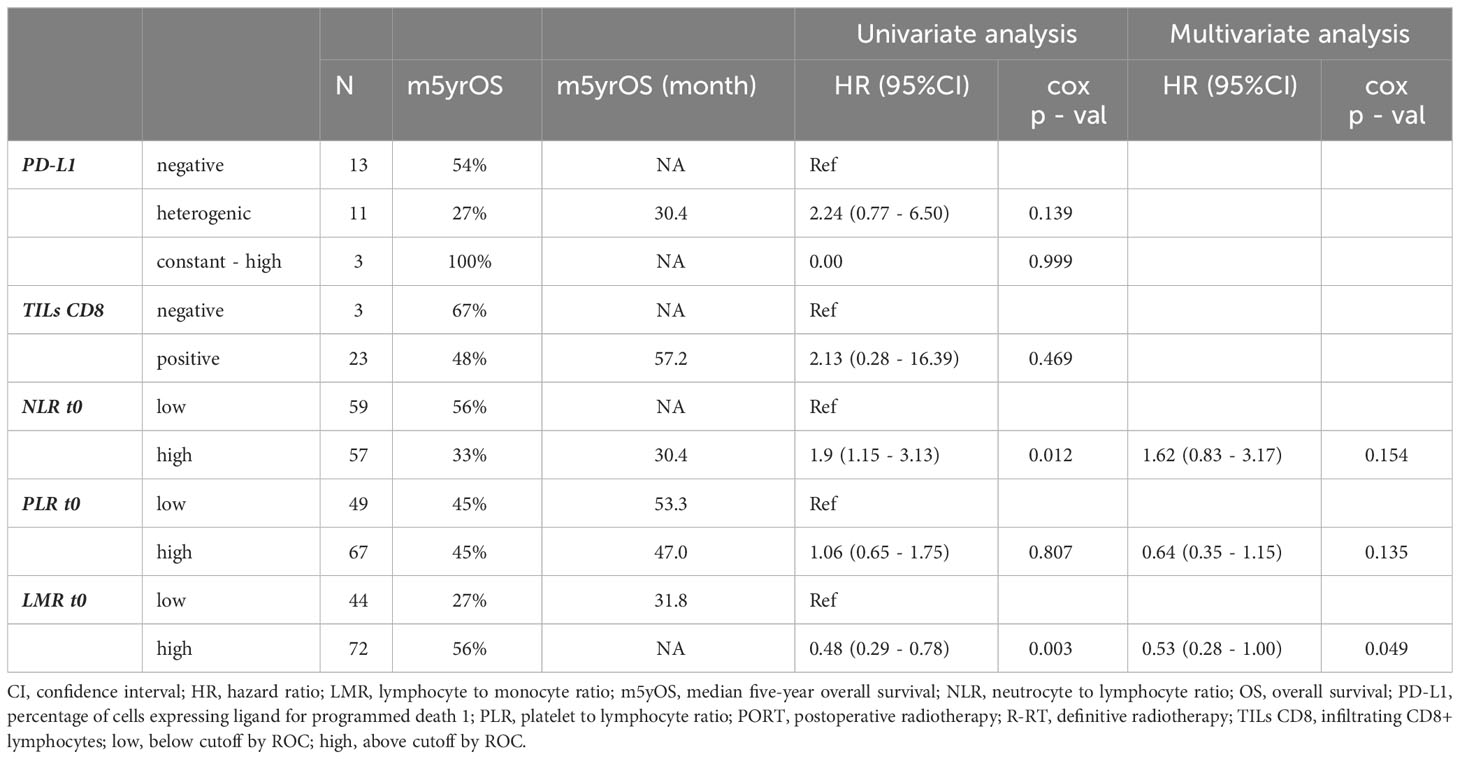
Table 2 Baseline inflammation biomarkers in laryngeal cancer - clinical and pathological in the R-RT group (n= 116).
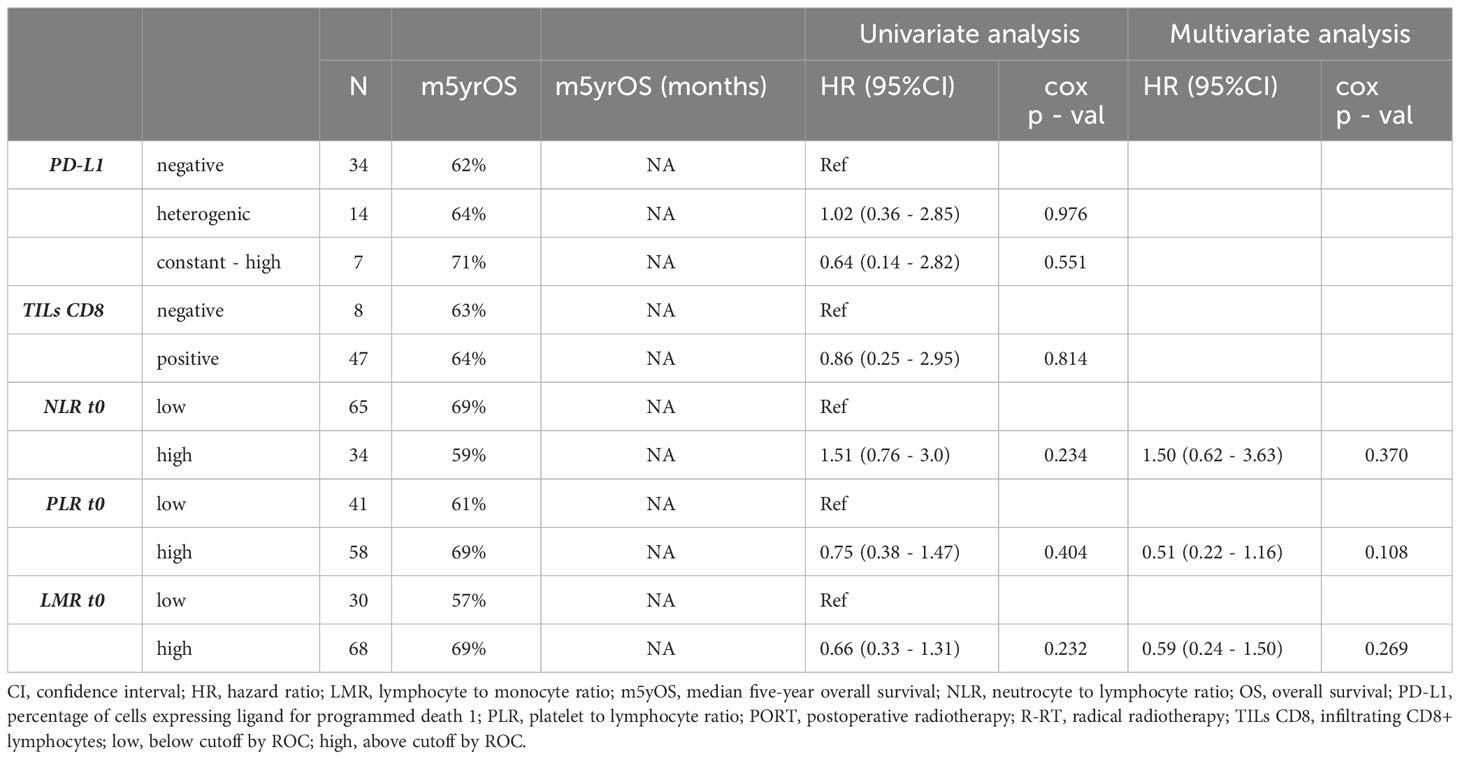
Table 3 Baseline inflammation biomarkers in laryngeal cancer - clinical and pathological in the PORT group (n= 99).
Baseline inflammation biomarkers
Prognostic impact of baseline peripheral and local inflammatory markers are shown in Tables 2, 3. Time-dependent receiver performance characteristics (ROC) curves revealed pretreatment cut-off values for NLR, PLR, and LMR in the whole group of 2.8, 129.7, and 2.2, respectively. Most of assessed patients had high (above cutoff by ROC) LMR and PLR pretreatment values.
The baseline high-NLR (t0) (n=57) value was correlated with worse long-term results in the R-RT group. The five-year OS in the high-NLR (n=57) and low-NLR (n=59) groups was 33% and 56%, respectively (HR 1.90; 95% CI 1.15–3.13 Cox p = 0.012) (Figure 1).
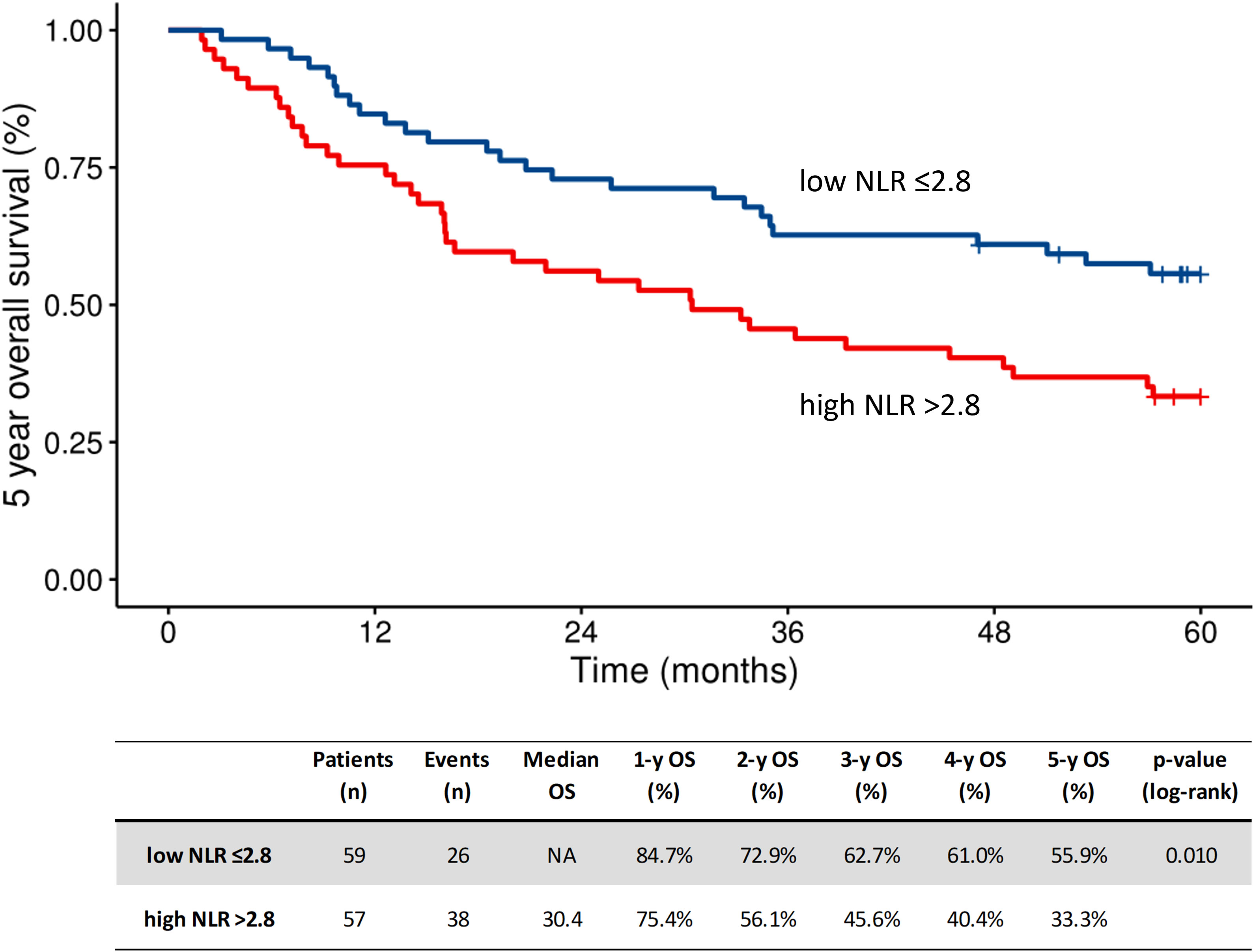
Figure 1 Kaplan-Meier plot of overall survival according to baseline NLR (t0) in the R-RT group. High, above cutoff by ROC; low, below cutoff by ROC; mOS, median overall survival; NLR, neutrocyte to lymphocyte ratio; R-RT, definitive radiotherapy.
In the R-RT group, patients with high LMR (n=72) received higher cumulative doses of cisplatin than those with low LMR (n=44). The number of complications was 20% higher during RT, with more common antibiotic use in the low-LMR group than in the high-LMR group (p = 0.024). The PORT group did not show these differences. The PLR had no prognostic value in either group.
In the R-RT and PORT groups, 51.6% (n=13) and 38.2% (n=21) of the patients, respectively, showed positive expression of PD-L1. The five-year OS was 80% for patients with const-high PD-L1 expression (HR=0.41, 95%CI: 0.09–1.75, p=0.218) vs. 60% for patients whose tumors were PD-L1 negative (Figure 2). The status of TILsCD8 positivity vs. negativity did not correlate with OS.
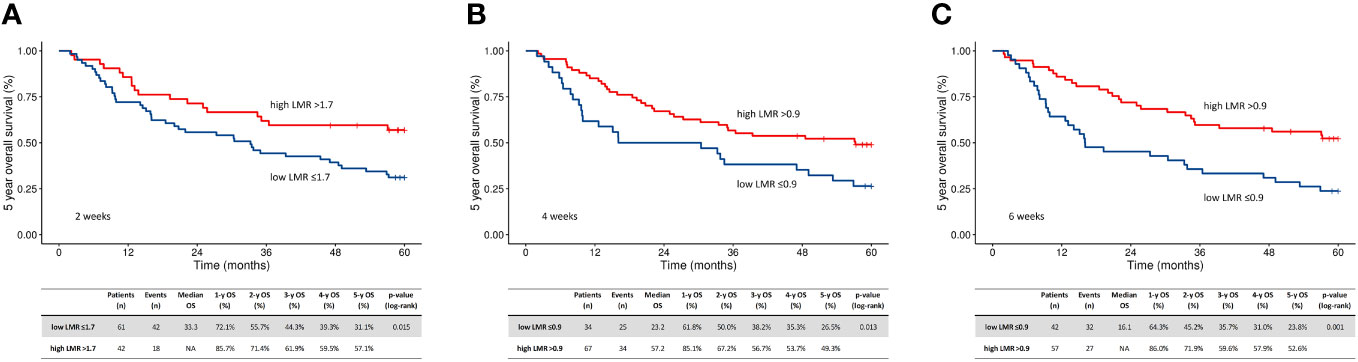
Figure 2 Kaplan-Meier plots of oncological outcome in relation to baseline LMR at two weeks (A), four weeks (B), and six weeks (C) after the start of radiotherapy - in the R-RT group. High, above cutoff by ROC; low, below cutoff by ROC; LMR, lymphocyte to monocyte ratio; mOS, median overall survival; R-RT, definitive radiotherapy.
RT-induced changes in LMR
The ROC LMR cut-off points for all patients were 2.2, 1.7, 0.9, and 0.9 at the predefined time points (t0, t2, t4, and t6, respectively). At each time point, the patients were divided into four groups based on their t0 values (low vs. high LMR) and their RT-related changes (i.e., increasing or decreasing values). Decreases in LMR values were most common in the second week of treatment (Table 4). Low LMR during RT predicted worse OS, regardless of the baseline LMR value. The five-year OS rates for patients with low (n=61) vs. high LMR (n=42) were 31% vs. 57% at t2 (HR 0.51; 95% CI 0.29-0.89, p = 0.017), 26% (n=34) vs. 49% (n=67) at t4 (p < 0.001), and 25% (n=42) vs. 50% at (n=57) t6 (HR 0.53; 95% CI 0.31-0.88, p = 0.015), respectively. (Figure 2) Patients with a decrease in LMR at t2 had a median OS of 23.2 months compared to 57.2 months for those without an LMR decrease (p = 0.010). A further decrease in the low baseline LMR group was the worst prognostic factor (in the R-RT group). In PORT patients, the LMR and its changes had no prognostic value (Figure 3).
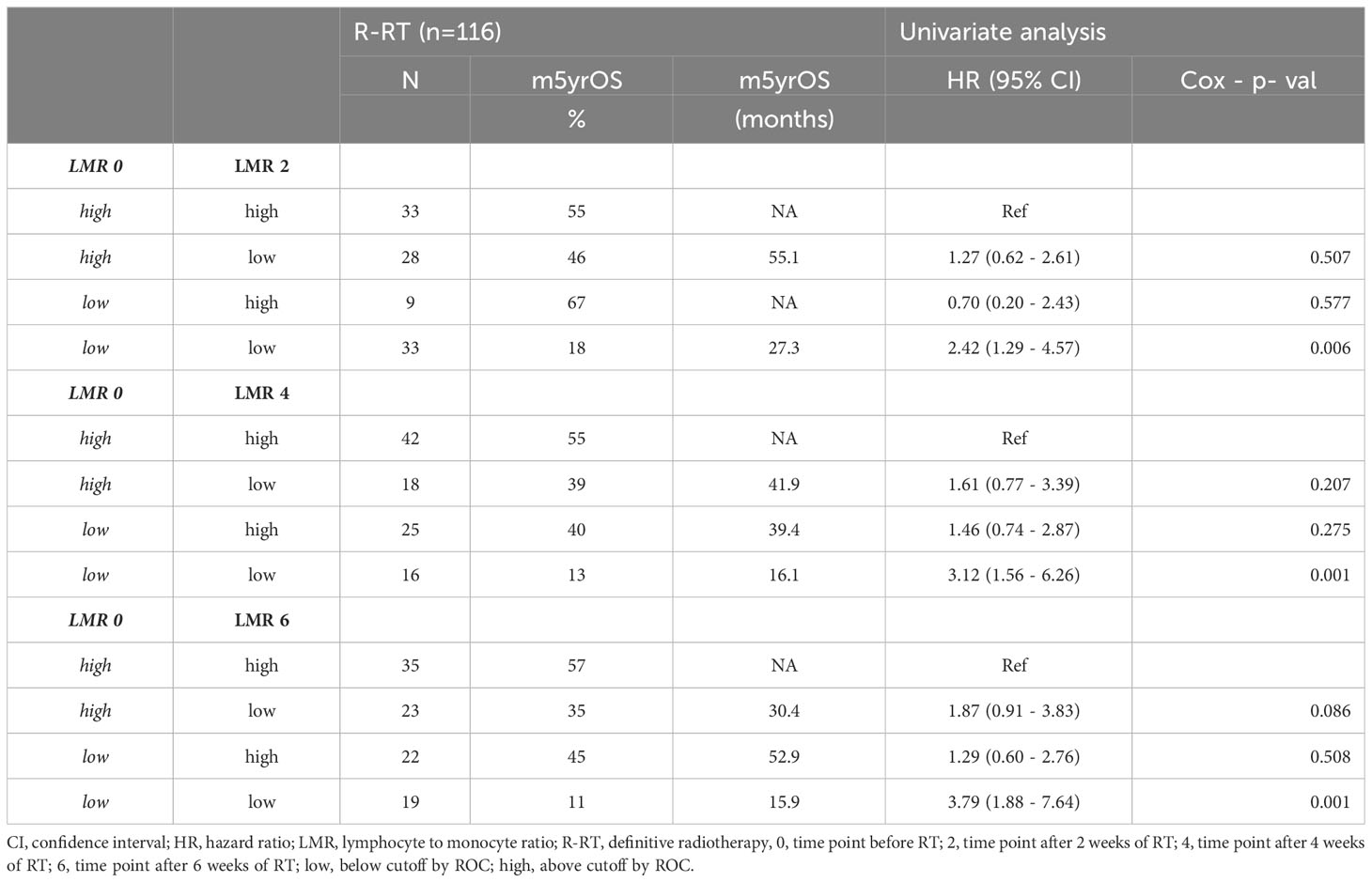
Table 4 RT induced LMR changes at time points, depending on the baseline LMR in the R-RT group.
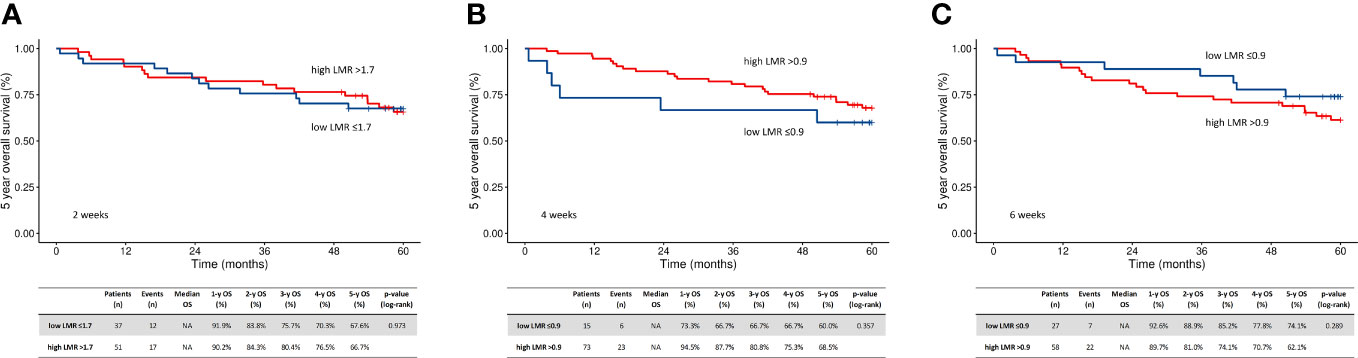
Figure 3 Kaplan-Meier plots of oncological outcome in relation to baseline LMR at two weeks (A), four weeks (B), and six weeks (C) after the start of radiotherapy - in the PORT group. High, above cutoff by ROC; low, below cutoff by ROC; LMR, lymphocyte to monocyte ratio; mOS, median overall survival; PORT, postoperative radiotherapy.
Discussion
Since 1863, when Virchow first suggested a relationship between inflammation and cancer progression, malignant neoplasms have been seen as a mixture of interplaying cells, including cancer cells, stromal cells, infiltrating lymphocytes, dendritic cells, and even microbes (30). Any type of anticancer therapy will therefore have an impact on these cell types. RT is detrimental to cells capable of proliferation, making tumor cells and intra-tumoral immune cells vulnerable. We hypothesized that tumor cell apoptosis induces a local immune reaction, which further impacts the peripheral blood parameters responsible for the general immune reaction. Our assessment of NLR, PLR, and LMR in patients with LC confirmed that in non-metastatic LC managed with R-RT, the baseline and subsequent changes in LMR correlate with patient outcomes.
Immune peripheral markers have earlier been studied in different types of nonmetastatic and metastatic malignancies (31–35). Despite the use of different cutoff values (1.8 and 5.8) (31, 32), these studies have also shown a prognostic role for LMR. In our study, cutoffs for LMR were established at each of the predefined time points during treatment. Previous research on this topic in HNC focused on measuring this biomarker once before treatment. Further, patients with low baseline LMR were excluded (19, 35). We found that the decrease in LMR during RT had a significant prognostic value, regardless of the baseline LMR value. The RT-induced LMR changes were investigated in 2021 by Chia-Hsin Lin et al. in Asiatic patients with HNC, including a large number of patients with nasopharyngeal tumors (19). In that study, LC accounted for less than 8%. The dynamic LMR changes were calculated as the difference between LMR measured at baseline and during RT (called a delta-LMR). A low delta-LMR at the second week of RT was correlated with less favorable five-year OS (73% vs. 59%, p <0.001).
Studies on non-small cell lung cancer (NSCLC), colorectal cancer, and breast cancer have shown that higher LMR values after treatment initiation (compared to baseline values) correlated with better PFS and, sometimes with better OS (21, 36–38).
Few studies have investigated LMR changes in the PORT setting. Kim et al. showed a negative impact of low RT-related LMR on the PFS and OS at the second week of conventional RT (50.4Gy in 28 fractions) in breast cancer patients irradiated with a breast-conserving approach (21). Our study has not demonstrated similar results in the PORT group.
Our results confirm that several pretreatment factors, including performance status (ECOG ≥1), anemia, the presence of nodal metastases, and high NLR, significantly predict unfavorable outcomes in the R-RT group. The prognostic value of NLR has not been fully clarified. A large study including 5,700 patients with LC showed that high baseline value of NLR and PLR significantly correlated with OS. The NLR cut-off point was close to the value in our study (3.0) (39).
In our study patients with low or high baseline LMR values showed both an increase and a decrease in this parameter after RT. The worst prognostic results were obtained in the low-low LMR group and the best in the high-high group. Conversely, the OS in the low-high group was not worse than in the high-low group, placing both groups in the intermediate risk zone. Our results indicate that patients with a baseline low-LMR value, especially those with a decrease in LMR in the second week of radiotherapy had more complications and more frequently required antibacterial and antifungal treatment than the low-high group. These are possibly patients who require special attention (40).
We set the cut-off for PD-L1 expression at 50% of the tumor infiltration cells. The consistently positive expression in cancer cells (greater than 30% in all three cores for one case) clearly separated the survival curves compared to patients with higher point expression, but without statistical significance (p=0.073). We realize that our group is too small to draw far-reaching conclusions.
The prognostic value of PD-L1 expression has conflicting evidence in several cancers, including NSCLC, breast cancer, bladder cancer, and HNC (41–45). Previous studies of HNC have shown a correlation between PD-L1 overexpression with either poor prognosis (46, 47) or good prognosis (48, 49). Some clinicopathological features, e.g. tumor stage, or tumor site, and non-diabetic patients were correlated with positive PD-L1, but not with OS (50). There can be many reasons for this. First, the value of PD-L1 expression is dynamic in each patient, depending on the place of sampling, the time of its collection, patients comorbidities and possibly taken medications. Secondly, PD-L1 positive cells may negatively regulate the antitumor response of T lymphocytes, which has led to poor prognosis (51). On the contrary, TILsCD8+ infiltration may induce PD-L1 expression, which may be the reason for the association between high PD-L1 expression and good prognosis (52).
Clinical trials with the addition of immunotherapy, in various configurations, to definitive radiochemotherapy failed to demonstrate a statistically significant improvement (53–55). Nevertheless, anti-PD-1 immunotherapy plus chemoradiation is associated with a favorable trend toward improved PFS versus standard therapy in patients with locally advanced HNC. The benefit is noticeable in patients with PD-L1 combined positive score (CPS) >=1, especially with CPS >=20 (54). Additionally, there is a theory that radiotherapy and cisplatin has been shown to increase PD-L1 expression, and the concurrent inhibition of the PD-1/PD-L1 pathway may boost the antitumor activity of radiotherapy (56).
The pathomorphological guidelines of TILsCD8 assessment for HNC are partially derived from data on breast cancer (57). Assessing the infiltration of TILs, should take into account that the tumors arise from the squamous epithelium associated with lymphoid tissue. The preexisting background of lymphoid stroma makes TIL assessment in HNC challenging. Therefore, we focused on the evaluation of the intratumoral rather than stromal TILs. We used scoring of the IHC values to describe TILsCD8. We discarded cases diagnosed by biopsy from pathological lymph nodes to standardize our analysis. Unfortunately, we had archival pathological material from tumor tissues from only 84 patients. The status of TILsCD8 patients in our study did not have prognostic impact. A relatively small number of patients does not allow for firm conclusions. However, other studies showed that high levels of TILsCD8 correlated with improved outcomes in patients administered definitive chemoradiotherapy, whereas stomal TILs did not (58). In patients managed with PORT, a favorable correlation was also confirmed for both intratumoral and stromal TILsCD8 (59, 60). Nowadays, there are no uniform cutoff guidelines for the evaluation of PD-L1 expression and the technical aspects of TILsCD8 evaluation in LC patients.
The role of TILs in predicting the efficacy of chemoradiotherapy in LC may be clarified in large clinical trials. Establishing unambiguous predictive features of responses to immune therapies affecting the PD-L1/PD-1 pathway is also particularly important. These drugs are increasingly available for the treatment of patients initially inoperable, with relapsed or disseminated disease. In the future, this treatment is likely to be implemented in the adjuvant treatment.
This study possesses several inherent limitations. Firstly, its retrospective nature led to the omission of certain data points. The pool of suitable archival biospecimens was limited once we refined our selection to encompass only the highest quality materials. A subset of these biospecimens originated from patients who underwent treatment over 5 years ago. However, it is important to note, that all assessed samples have adhered to European Union standards for fixation and storage since 2010. We have duly considered and accommodated this aspect, making adjustments to our analysis and interpretations to mitigate the potential for erroneous negative outcomes. Lastly, it’s worth mentioning that we lacked access to data pertaining to disease-free survival or patterns of relapse.
Conclusion
This study demonstrates that RT-inducted changes in LMR are associated with survival outcomes in LC patients administered definitive chemoradiotherapy.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Bioethical Committee of the Medical University of Gdańsk. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because this study has only the retrospective character.
Author contributions
Guarantor of integrity of the entire study: NC-C. Study concepts and design: NC-C, MP, MB, and RZ. Literature research: NC-C. (Clinical studies) gathering the clinical data: NC-C and MD. (Experimental studies) data analysis: NC-C and JR. Statistical analysis: MP. Manuscript preparation: NC-C. Manuscript editing: NC-C, MB, MP, MD, JR, JJ, and RZ. First authorship: NC-C. Senior and last authorship: RZ. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by the Medical University of Gdańsk statutory grant ST-23, 02-0023/7.
Acknowledgments
We would like to thank the staff who took care of our patients’ needs, and who were involved in gathering, documenting, verifying, forwarding and processing the clinical data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AJCC, American Joint Committee on Cancer; CBC, circulated blood cells; CIs, confidence intervals; CPS, PD-L1 combined positive score; DDP, Cisplatin; DFR, distant failure rate; ECOG, Eastern Cooperative Oncology Group scale; HRs, hazard ratios; HNC, head and neck cancer; ICRU, International Commission on Radiation Units & Measurements; IM, immunoscore; IMRT, Intensity Modulated Radiation Therapy; LC, laryngeal cancer; LFR, local failure rate; LMR, lymphocyte to monocyte ratio; NSCLC, non-small cell lung cancer; NLR, neutrophil to lymphocyte ratio; OS, overall survival; PD – L1, percentage of cells expressing ligand for programmed death 1; PLR, platelet to lymphocyte ratio; PORT, postoperative radiotherapy; RFR, regional failure rate; ROC, receiver operating characteristic; R -RT, definitive radiotherapy; t0, time point before RT; t2, time point after 2 weeks of RT; t4, time point after 4 weeks of RT; t6, time point after 6 weeks of RT; TCs, tumor cells; TILsCD8, infiltrating CD8+ lymphocytes; TMA, Tissue microarrays; VMAT, Volumetric Modulated Arc Therapy.
References
1. World Health Organization. Global cancer observatory. International Agency for Research on Cancer. International J Cancer (2021). Available at: https://gco.iarc.fr/.
2. Studer G, Peponi E, Kloeck S, Dossenbach T, Huber G, Glanzmann C. Surviving hypopharynx–larynx carcinoma in the era of IMRT. Int J Radiat OncologyBiologyPhysics (2010) 77(5):1391–6. doi: 10.1016/j.ijrobp.2009.07.005
3. Chao KSC, Ozyigit G, Blanco AI, Thorstad WL, Deasy JO, Haughey BH, et al. Intensity-modulated radiation therapy for oropharyngeal carcinoma: impact of tumor volume. Int J Radiat OncologyBiologyPhysics (2004) 59(1):43–50. doi: 10.1016/j.ijrobp.2003.08.004
4. González-Moles MÁ, Aguilar-Ruiz M, Ramos-García P. Challenges in the early diagnosis of oral cancer, evidence gaps and strategies for improvement: A scoping review of systematic reviews. Cancers (Basel) (2022) 14(19):4967. doi: 10.3390/cancers14194967
5. Leeman JE, Li JG, Pei X, Venigalla P, Zumsteg ZS, Katsoulakis E, et al. Patterns of treatment failure and postrecurrence outcomes among patients with locally advanced head and neck squamous cell carcinoma after chemoradiotherapy using modern radiation techniques. JAMA Oncol (2017) 3(11):1487. doi: 10.1001/jamaoncol.2017.0973
6. Setton J, Caria N, Romanyshyn J, Koutcher L, Wolden SL, Zelefsky MJ, et al. Intensity-modulated radiotherapy in the treatment of oropharyngeal cancer: An update of the memorial sloan-kettering cancer center experience. Int J Radiat OncologyBiologyPhysics (2012) 82(1):291–8. doi: 10.1016/j.ijrobp.2010.10.041
7. Ladbury CJ, Rusthoven CG, Camidge DR, Kavanagh BD, Nath SK. Impact of radiation dose to the host immune system on tumor control and survival for stage III non-small cell lung cancer treated with definitive radiation therapy. Int J Radiat OncologyBiologyPhysics (2019) 105(2):346–55. doi: 10.1016/j.ijrobp.2019.05.064
8. Gómez V, Mustapha R, Ng K, Ng T. Radiation therapy and the innate immune response: Clinical implications for immunotherapy approaches. Br J Clin Pharmacol (2020) 86(9):1726–35. doi: 10.1111/bcp.14351
9. Panje C, Riesterer O, Glanzmann C, Studer G. Neutrophil-lymphocyte ratio complements volumetric staging as prognostic factor in patients treated with definitive radiotherapy for oropharyngeal cancer. BMC Cancer (2017) 17(1):643. doi: 10.1186/s12885-017-3590-0
10. Templeton AJ, McNamara MG, Šeruga B, Vera-Badillo FE, Aneja P, Ocaña A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. JNCI: J Natl Cancer Institute (2014) 106(6). doi: 10.1093/jnci/dju124
11. Chowdhary M, Switchenko JM, Press RH, Jhaveri J, Buchwald ZS, Blumenfeld PA, et al. Post-treatment neutrophil-to-lymphocyte ratio predicts for overall survival in brain metastases treated with stereotactic radiosurgery. J Neurooncol (2018) 139(3):689–97. doi: 10.1007/s11060-018-2914-5
12. Proctor MJ, Morrison DS, Talwar D, Balmer SM, Fletcher CD, DStJ O’Reilly, et al. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur J Cancer (2011) 47(17):2633–41. doi: 10.1016/j.ejca.2011.03.028
13. Guthrie GJK, Charles KA, Roxburgh CSD, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil–lymphocyte ratio: Experience in patients with cancer. Crit Rev Oncol Hematol (2013) 88(1):218–30. doi: 10.1016/j.critrevonc.2013.03.010
14. Bojaxhiu B, Templeton AJ, Elicin O, Shelan M, Zaugg K, Walser M, et al. Relation of baseline neutrophil-to-lymphocyte ratio to survival and toxicity in head and neck cancer patients treated with (chemo-) radiation. Radiat Oncol (2018) 13(1):216. doi: 10.1186/s13014-018-1159-y
15. Aoyama J, Kuwahara T, Sano D, Fujisawa T, Tokuhisa M, Shimizu M, et al. Combination of performance status and lymphocyte-monocyte ratio as a novel prognostic marker for patients with recurrent/metastatic squamous cell carcinoma of the head and neck. Cancer Diagnosis Prognosis (2021) 1(4):353–61. doi: 10.21873/cdp.10047
16. Olingy CE, Dinh HQ, Hedrick CC. Monocyte heterogeneity and functions in cancer. J Leukoc Biol (2019) 106(2):309–22. doi: 10.1002/JLB.4RI0818-311R
17. Robinson A, Han CZ, Glass CK, Pollard JW. Monocyte regulation in homeostasis and Malignancy. Trends Immunol (2021) 42(2):104–19. doi: 10.1016/j.it.2020.12.001
18. Li KJ, Xia XF, Su M, Zhang H, Chen WH, Zou CL. Predictive value of lymphocyte-to-monocyte ratio (LMR) and neutrophil-to-lymphocyte ratio (NLR) in patients with oesophageal cancer undergoing concurrent chemoradiotherapy. BMC Cancer (2019) 19(1):1004. doi: 10.1186/s12885-019-6157-4
19. Lin CH, Chou WC, Wu YY, Lin CY, Chang KP, Liao CT, et al. Prognostic significance of dynamic changes in lymphocyte-to-monocyte ratio in patients with head and neck cancer treated with radiotherapy: results from a large cohort study. Radiotherapy Oncol (2021) 154:76–86. doi: 10.1016/j.radonc.2020.09.012
20. Pierce BL, Ballard-Barbash R, Bernstein L, Baumgartner RN, Neuhouser ML, Wener MH, et al. Elevated biomarkers of inflammation are associated with reduced survival among breast cancer patients. J Clin Oncol (2009) 27(21):3437–44. doi: 10.1200/JCO.2008.18.9068
21. Kim D, Bae SJ, Ahn SG, Jeong J, Park S, Park WC, et al. RT-induced dynamic changes in the lymphocyte-to-monocyte ratio in patients with breast cancer indicate poor prognosis. Breast Cancer Res Treat (2022) 193(3):637–47. doi: 10.1007/s10549-022-06601-8
22. Grégoire V, Eisbruch A, Hamoir M, Levendag P. Proposal for the delineation of the nodal CTV in the node-positive and the post-operative neck. Radiotherapy Oncol (2006) 79(1):15–20. doi: 10.1016/j.radonc.2006.03.009
23. Eisbruch A, Foote RL, O’Sullivan B, Beitler JJ, Vikram B. Intensity-modulated radiation therapy for head and neck cancer: Emphasis on the selection and delineation of the targets. Semin Radiat Oncol (2002) 12(3):238–49. doi: 10.1053/srao.2002.32435
24. Eisbruch A, Schwartz M, Rasch C, Vineberg K, Damen E, Van As CJ, et al. Dysphagia and aspiration after chemoradiotherapy for head-and-neck cancer: Which anatomic structures are affected and can they be spared by IMRT? Int J Radiat OncologyBiologyPhysics (2004) 60(5):1425–39. doi: 10.1016/j.ijrobp.2004.05.050
25. Grégoire V, Ang K, Budach W, Grau C, Hamoir M, Langendijk JA, et al. Delineation of the neck node levels for head and neck tumors: A 2013 update. DAHANCA, EORTC, HKNPCSG, NCIC CTG, NCRI, RTOG, TROG consensus guidelines. Radiotherapy Oncol (2014) 110(1):172–81. doi: 10.1200/JCO.2008.18.9068
26. R Core Team RF for SCVA. R: A language and environment for statistical computing (2018). Available at: https://www.R-project.org/.
27. Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC, et al. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinf (2011) 12(1):77. doi: 10.1186/1471-2105-12-77
29. Kassambara A, Kosinski M, Biecek P. Survminer: Drawing Survival Curves using ‘ggplot2’, in: R package version 0.4.6 (2019). Available at: https://CRAN.R-project.org/package=survminer (Accessed 1 Feb 2022).
30. Virchow R. Cellular pathology as based upon physiological and pathological histology. Philadelphia: J. B. Lippincott (1863).
31. Tan D, Fu Y, Tong W, Li F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. Int J Surgery (2018) 55:128–38. doi: 10.1016/j.ijsu.2018.05.030
32. Gong J, Jiang H, Shu C, Hu MQ, Huang Y, Liu Q, et al. Prognostic value of lymphocyte-to-monocyte ratio in ovarian cancer: a meta-analysis. J Ovarian Res (2019) 12(1):51. doi: 10.1186/s13048-019-0527-z
33. Nora I, Shridhar R, Huston J, Meredith K. The accuracy of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as a marker for gastrointestinal Malignancies. J Gastrointest Oncol (2018) 9(5):972–8. doi: 10.21037/jgo.2018.08.05
34. Phan TT, Ho TT, Nguyen HT, Nguyen HT, Tran TB, Nguyen ST. The prognostic impact of neutrophil to lymphocyte ratio in advanced non-small cell lung cancer patients treated with EGFR TKI. Int J Gen Med (2018) 11:423–30. doi: 10.2147/IJGM.S174605
35. Jiang R, Cai XY, Yang ZH, Yan Y, Zou X, Guo L, et al. Elevated peripheral blood lymphocyte-to-monocyte ratio predicts a favorable prognosis in the patients with metastatic nasopharyngeal carcinoma. Chin J Cancer (2015) 34(3):23. doi: 10.1186/s40880-015-0025-7
36. Li B, Wang S, Li C, Guo M, Xu Y, Sun X, et al. The kinetic changes of systemic inflammatory factors during bevacizumab treatment and its prognostic role in advanced non-small cell lung cancer patients. J Cancer (2019) 10(21):5082–9. doi: 10.7150/jca.30478
37. Shibutani M. Prognostic significance of the lymphocyte-to-monocyte ratio in patients with metastatic colorectal cancer. World J Gastroenterol (2015) 21(34):9966. doi: 10.3748/wjg.v21.i34.9966
38. Wan L, Wu C, Luo S, Xie X. Prognostic value of lymphocyte-to-monocyte ratio (LMR) in cancer patients undergoing immune checkpoint inhibitors. Dis Markers (2022) 2022:1–20. doi: 10.1155/2022/3610038
39. Hu X, Tian T, Sun Q, Jiang W. Prognostic value of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in laryngeal cancer: What should we expect from a meta-analysis? Front Oncol (2022) 12. doi: 10.3389/fonc.2022.945820
40. Lambin P, Lieverse RIY, Eckert F, Marcus D, Oberije C, van der Wiel AMA, et al. Lymphocyte-sparing radiotherapy: The rationale for protecting lymphocyte-rich organs when combining radiotherapy with immunotherapy. Semin Radiat Oncol (2020) 30(2):187–93. doi: 10.1016/j.semradonc.2019.12.003
41. Tuminello S, Sikavi D, Veluswamy R, Gamarra C, Lieberman-Cribbin W, Flores R, et al. PD-L1 as a prognostic biomarker in surgically resectable non- small cell lung cancer: A meta-analysis. Transl Lung Cancer Res (2020) 9(4):1343–60. doi: 10.21037/tlcr-19-638
42. Davey MG, Ryan ÉJ, Davey MS, Lowery AJ, Miller N, Kerin MJ. Clinicopathological and prognostic significance of programmed cell death ligand 1 expression in patients diagnosed with breast cancer: meta-analysis. Br J Surgery (2021) 108(6):622–31. doi: 10.1093/bjs/znab103
43. Zhu L, Sun J, Wang L, Li Z, Wang L, Li Z. Prognostic and clinicopathological significance of PD-L1 in patients with bladder cancer: A meta-analysis. Front Pharmacol (2019) 10. doi: 10.3389/fphar.2019.00962
44. Nocini R, Vianini M, Girolami I, Calabrese L, Scarpa A, Martini M, et al. PD-L1 in oral squamous cell carcinoma: A key biomarker from the laboratory to the bedside. Clin Exp Dent Res (2022) 8(3):690–8. doi: 10.1002/cre2.590
45. Lenouvel D, González-Moles MÁ, Ruiz-Ávila I, Gonzalez-Ruiz L, Gonzalez-Ruiz I, Ramos-García P. Prognostic and clinicopathological significance of PD-L1 overexpression in oral squamous cell carcinoma: A systematic review and comprehensive meta-analysis. Oral Oncol (2020) 106:104722. doi: 10.1016/j.oraloncology.2020.104722
46. Lenouvel D, González-Moles MÁ, Talbaoui A, Ramos-García P, González-Ruiz L, Ruiz-Ávila I, et al. An update of knowledge on PD-L1 in head and neck cancers: Physiologic, prognostic and therapeutic perspectives. Oral Dis (2020) 26(3):511–26. doi: 10.1111/odi.13088
47. Kim T, Jung SH, Kim SK, Kwon HJ. P16 expression and its association with PD-L1 expression and FOXP3-positive tumor infiltrating lymphocytes in head and neck squamous cell carcinoma. Mol Cell Toxicol (2019) 15(2):137–43. doi: 10.1007/s13273-019-0017-9
48. Chen SW, Li SH, Shi DB, Jiang WM, Song M, Yang AK, et al. Expression of PD-1/PD-L1 in head and neck squamous cell carcinoma and its clinical significance. Int J Biol Markers (2019) 34(4):398–405. doi: 10.1177/1724600819884722
49. Roper E, Lum T, Palme CE, Ashford B, Ch’ng S, Ranson M, et al. PD-L1 expression predicts longer disease free survival in high risk head and neck cutaneous squamous cell carcinoma. Pathology (2017) 49(5):499–505. doi: 10.1016/j.pathol.2017.04.004
50. Wusiman D, Guo L, Huang Z, Li Z, Liu S, Ying J, et al. The clinicopathological significance of PD-L1 expression assessed by the combined positive score (CPS) in head and neck squamous cell carcinoma. Pathol Res Pract (2022) 236:153934. doi: 10.1016/j.prp.2022.153934
51. Fang Q, Wu Y, Du W, Zhang X, Chen D. Incidence and prognostic significance of PD-L1 expression in high-grade salivary gland carcinoma. Front Oncol (2021) 11. doi: 10.1111/odi.13088
52. Sun X, Shu P, Fang Y, Yuan W, Zhang Q, Sun J, et al. Clinical and prognostic significance of tumor-infiltrating CD8+ T cells and PD-L1 expression in primary gastrointestinal stromal tumors. Front Oncol (2021) 11. doi: 10.3389/fonc.2021.789915
53. Bourhis J, Tao Y, Sun X, Sire C, Martin L, Liem X, et al. LBA35 Avelumab-cetuximab-radiotherapy versus standards of care in patients with locally advanced squamous cell carcinoma of head and neck (LA-SCCHN): Randomized phase III GORTEC-REACH trial. Ann Oncol (2021) 32:S1310. doi: 10.1016/j.annonc.2021.08.2112
54. Machiels JP, Tao Y, Burtness B, Tahara M, Rischin D, Alves GV, et al. LBA5 Primary results of the phase III KEYNOTE-412 study: Pembrolizumab (pembro) with chemoradiation therapy (CRT) vs placebo plus CRT for locally advanced (LA) head and neck squamous cell carcinoma (HNSCC). Ann Oncol (2022), 33:S1399. doi: 10.1016/j.annonc.2022.08.029
55. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro G, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet (2019) 394(10212):1915–28. doi: 10.1016/S0140-6736(19)32591-7
56. Girolami I, Marletta S, Fiorentino V, Battocchio S, Cerbelli B, Fiamengo B, et al. Effect of radio-chemotherapy on PD-L1 immunohistochemical expression in head and neck squamous cell carcinoma. J Pers Med (2023) 13(2):363. doi: 10.3390/jpm13020363
57. Hendry S, Salgado R, Gevaert T, Russell PA, John T, Thapa B, et al. Assessing tumor-infiltrating lymphocytes in solid tumors: A practical review for pathologists and proposal for a standardized method from the international immuno-oncology biomarkers working group: Part 2: TILs in melanoma, gastrointestinal tract carcinomas, non–small cell lung carcinoma and mesothelioma, endometrial and ovarian carcinomas, squamous cell carcinoma of the head and neck, genitourinary carcinomas, and primary brain tumors. Adv Anat Pathol (2017) 24(6):311–35. doi: 10.1097/PAP.0000000000000161
58. Balermpas P, Michel Y, Wagenblast J, Seitz O, Weiss C, Rödel F, et al. Tumour-infiltrating lymphocytes predict response to definitive chemoradiotherapy in head and neck cancer. Br J Cancer (2014) 110(2):501–9. doi: 10.1038/bjc.2013.640
59. Balermpas P, Rödel F, Rödel C, Krause M, Linge A, Lohaus F, et al. CD8+ tumour-infiltrating lymphocytes in relation to HPV status and clinical outcome in patients with head and neck cancer after postoperative chemoradiotherapy: A multicentre study of the German cancer consortium radiation oncology group (DKTK-ROG). Int J Cancer (2016) 138(1):171–81. doi: 10.1002/ijc.29683
Keywords: lymphocyte-to-monocyte ratio (LMR), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), programmed death 1 ligand 1 (PD-L1), laryngeal cancer (LC)
Citation: Cichowska-Cwalińska N, Bieńkowski M, Popęda M, Dróżka M, Rutkowski J, Jassem J and Zaucha R (2023) Radiotherapy-induced dynamic changes in the lymphocyte-to-monocyte ratio in patients with laryngeal cancer indicate poor prognosis. Front. Oncol. 13:1234953. doi: 10.3389/fonc.2023.1234953
Received: 05 June 2023; Accepted: 20 September 2023;
Published: 10 October 2023.
Edited by:
Jean-Francois Daisne, University Hospitals Leuven, BelgiumReviewed by:
Carine Michiels, University of Namur, BelgiumMichel Bila, University Hospitals Leuven, Belgium
Copyright © 2023 Cichowska-Cwalińska, Bieńkowski, Popęda, Dróżka, Rutkowski, Jassem and Zaucha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renata Zaucha, cnphdWNoYUBndW1lZC5lZHUucGw=
†Senior and last authorship