 Máté Szilcz1*
Máté Szilcz1* Jonas W. Wastesson1,2
Jonas W. Wastesson1,2 Amaia Calderón-Larrañaga2,3
Amaia Calderón-Larrañaga2,3 Lucas Morin1,4,5Henrik Lindman6Kristina Johnell1
Lucas Morin1,4,5Henrik Lindman6Kristina Johnell1- 1Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden
- 2Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet & Stockholm University, Stockholm, Sweden
- 3Stockholm Gerontology Research Center, Stockholm, Sweden
- 4Inserm CIC 1431, University Hospital of Besançon, Besançon, France
- 5Inserm U1018, High-Dimensional Biostatistics for Drug Safety and Genomics, CESP, Villejuif, France
- 6Department of Immunology, Genetics and Pathology, Experimental and Clinical Oncology; Clinical Oncology, Faculty of Medicine, Uppsala University Hospital, Uppsala, Sweden
Background: The appropriate time to discontinue chemotherapy at the end of life has been widely discussed. In contrast, few studies have investigated the patterns of endocrine treatment near death. In this study, we aimed to investigate the end-of-life endocrine treatment patterns of older women with metastatic breast cancer and explore characteristics associated with treatment.
Methods: A retrospective cohort study of all older women (age ≥65 years) with hormone receptor-positive breast cancer who died in Sweden, 2016 − 2020. We used routinely collected administrative and health data with national coverage. Treatment initiation was defined as dispensing during the last three months of life with a nine-month washout period, while continuation and discontinuation were assessed by previous use during the same period. We used log-binomial models to explore factors associated with the continuation and initiation of endocrine treatments.
Results: We included 3098 deceased older women with hormone receptor-positive breast cancer (median age 78). Overall, endocrine treatment was continued by 39% and initiated by 5% and of women during their last three months of life, while 31% discontinued and 24% did not use endocrine treatment during their last year of life. Endocrine treatment continuation was more likely among older and less educated women, and among women who had multi-dose drug dispensing, chemotherapy, and CDK4/6 use. Only treatment-related factors were associated with treatment initiation.
Conclusion: More than a third of women with metastatic breast cancer continue endocrine treatments potentially past the point of benefit, whereas late initiation is less frequent. Further research is warranted to determine whether our results reflect overtreatment at the end of life once patients’ preferences and survival prognosis are considered.
Introduction
Breast cancer is the most common cancer among women worldwide (1). One-third of patients with metastatic breast cancer are 70 years or older at diagnosis (2). Many older patients (80%) have oestrogen- or progesterone receptor-positive tumours and are thereby candidates for endocrine treatment that blocks the hormone production or intervenes at the cell level of breast cancer (3). Patients may benefit from multiple lines of endocrine treatment (4), but there are no guidelines about how close to death endocrine treatment should be either continued, initiated or discontinued. At the end of life, many treatments’ potential adverse effects might outweigh their beneficial effects (e.g., chemotherapy), especially for older patients vulnerable to toxicities (5). Yet, little is known about endocrine treatment patterns in older women at the end of life.
A substantial body of research discusses the end-of-life trade-offs with anticancer therapies, especially chemotherapy (6–8). As the patients’ prognosis worsens, anticancer treatments often fail to comply with the general guiding principle that the “treatment should not be worse than the disease” due to the potential toxicities and negative impact on quality of life near death (9). Thus, chemotherapy is widely recognized as an overtreatment close to death (10, 11). Endocrine treatment is a less aggressive treatment option with easier parenteral administration and lower toxicity than chemotherapy for older individuals (12). However, endocrine treatment may increase the risk of cardiovascular events, osteoporosis, fatigue, pain, pneumonitis, neutropenia, hyperglycaemia, anxiety, depression, musculoskeletal complications, and other minor adverse events (13–16). These adverse effects are especially unwarranted in older frail people with multiple comorbidities near the end of life, when the goals of care should ideally shift toward comfort and quality-of-life-oriented care in line with patient preferences (17). Initiation of endocrine treatment in the last three months of life has been deemed inadequate, while continuing endocrine treatment until the end of life has been considered questionable in patients older than 75 years of age (18).
There are no comprehensive evaluations of endocrine therapy near death, mainly because only a few studies on end-of-life care include endocrine therapies in their definition of anticancer therapy (19–21). To fill these knowledge gaps, we first aimed to investigate the pattern of endocrine therapy in the last three months of life among older women with hormone receptor-positive metastatic breast cancer using routinely collected Swedish register data with national coverage. Secondly, we explored which patient characteristics were associated with endocrine therapy initiation versus no use, and continuation versus discontinuation at the end of life.
Materials and methods
Study design and population
This was a retrospective cohort study of decedents, that included all older women (age ≥65 years) with hormone receptor-positive metastatic breast cancer who died in Sweden between 1 January 2016 and 31 December 2020 (n = 5,045). We used routinely collected administrative and health data with national coverage in Sweden. Data from the National Cause of Death Register were linked using pseudonymised identifiers to the National Patient Register, the National Prescribed Drug Register, the Total Population Register, the Swedish Social Service Register and the Swedish Register of Education (Supplementary eTable 1).
Women were included in the cohort if they had both a diagnosis of breast cancer (International Statistical Classification of Diseases, 10th Revision [ICD-10] code C50) registered on the death certificate and if they had metastases (ICD-10: C78-79) registered in the National Patient Register or National Cause of Death Register (n=5,045) (Supplementary eFigure 1). Decedents were assumed to be hormone receptor positive, thus potentially eligible for endocrine treatment, if they had at least one endocrine treatment recorded in the National Prescribed Drug Register, similarly to previous research (22). Otherwise, they were excluded from the study. Decedents dying from a potentially acute and unpredictable fatal event according to their underlying cause of death (e.g., falls, suicide, stroke without history of ischemic heart disease) were excluded (n=40) from the analysis (Supplementary eTable 2). The rationale was to ensure that only women whose death may have potentially been anticipated by clinicians were included in the study. Furthermore, we excluded patients without breast cancer diagnosis registered in the National Patient Register during the last five years of life (n=352) and patients first diagnosed with breast cancer close to (≤3 months) death (n=229), because these patients might not have been regarded as end-of-life patients at the time of prescription. (Figure 1).
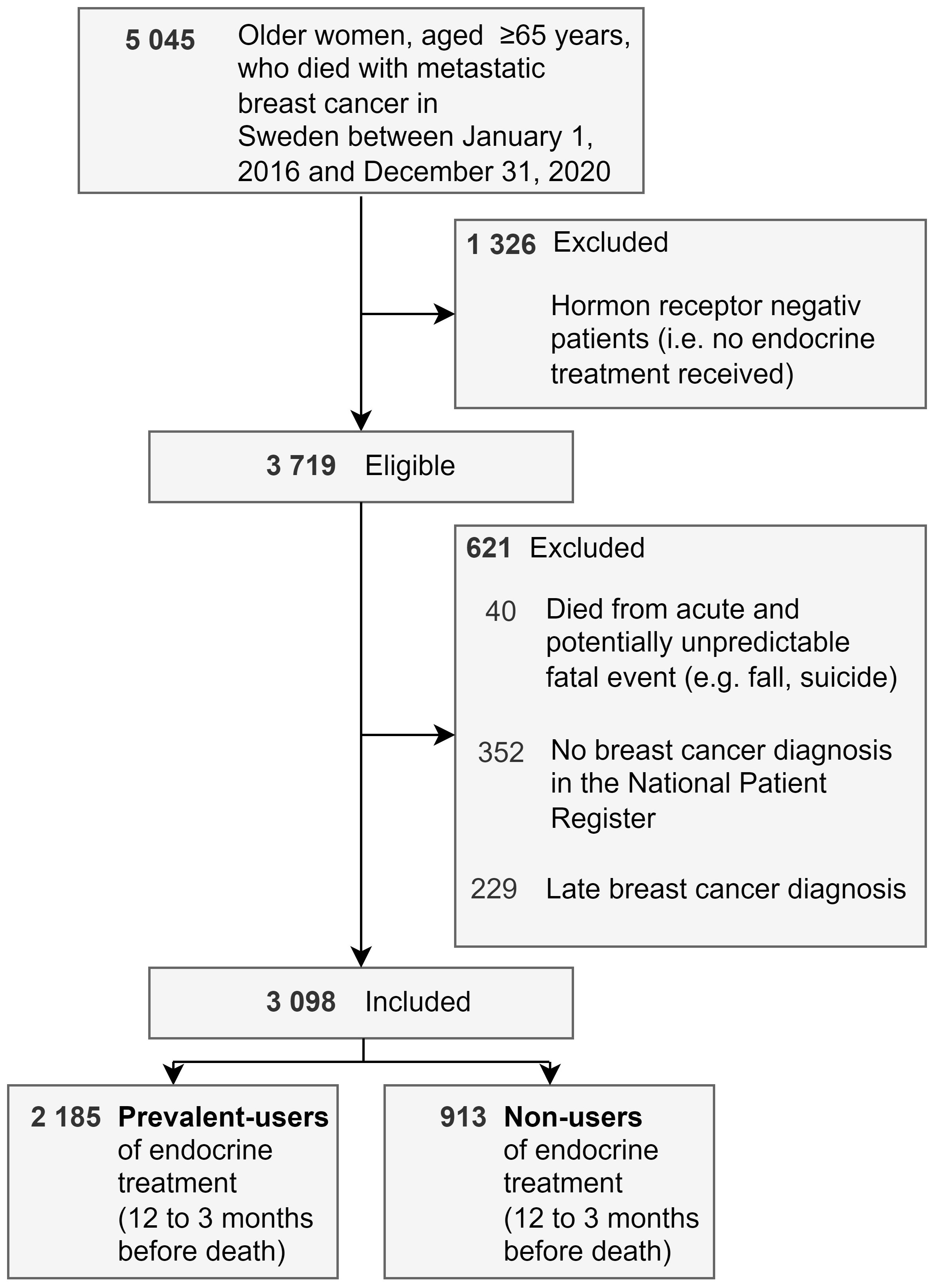
Figure 1 Flowchart.
The study population was divided into prevalent users of endocrine treatment and non-users during the period ranging from twelve to three months before death. Those with at least one endocrine treatment prescription between twelve to three months before death were classified as prevalent users, while the remaining patients were classified as non-users. This division was needed to confirm which patients were “at risk” for continuing or initiating endocrine treatment.
Outcome
Use of endocrine treatment was identified based on the Anatomical Therapeutic Chemical (ATC) codes (subgroup level ‘L02’ or everolimus [ATC: L01EG02]) from the National Prescribed Drug Register. Treatment exposure windows were constructed using a text parsing algorithm that calculates the prescribed daily dose based on the free text input of the prescriber. This method was described in detail elsewhere (23). We used four previously defined end-of-life treatment patterns (24): 1) Treatment continuation was defined as endocrine treatment dispensing during the last three months of life given previous use during twelve to three months before death; 2) Treatment discontinuation was defined as treatment dispensing during twelve to three months before death but no treatment dispensation during the last three months of life; 3) Treatment initiation was defined as the dispensing of endocrine treatment during the last three months of life, given a washout period of twelve to three months before death; and 4) No use was defined as no treatment dispensing during the last twelve months of life (Supplementary eFigure 2).
Patient-level characteristics
We extracted sociodemographic characteristics of decedents (e.g., sex, age at death, year of death, marital status) from national registries. Education was defined as the lifetime highest attained educational level and was categorised into ‘primary/elementary’, ‘secondary’, and ‘tertiary’ education based on the ISCED-97 classification system (25). Income quintiles correspond to the latest individual disposable income obtained from Statistics Sweden’s longitudinal integrated database for health insurance and labour market studies. Chronic multimorbidity was operationalised as the number of chronic diseases out of a list of 60 pre-defined conditions (26), which were captured in the National Patient Register and National Prescribed Drug Register during the period ranging from five years to three months before death (Supplementary eTable 3).We calculated the time since metastasis diagnosis (‘<1 year’, ‘1-3 years’, ‘>3 years’) and the Hospital Frailty Risk Score (27) (‘low’, ‘moderate’, ‘high’) based on the same data (Supplementary eTable 4). The cumulative time on endocrine treatment was evaluated using the same timeframe (five years to three months before death) and categorised as ‘<1 year’, ‘1-2 years’, ‘>2 years’. Nursing home residency was considered permanent if registered at least once in the Swedish Social Service Register (28) between one year and three months before death. Multi-dose drug dispensing scheme [i.e., patients receive machine-dispensed drugs packed in disposable bags (29)] was identified between one year and three months before death using the Swedish Prescribed Drug Register. Inpatient days were the sum of hospitalised days during the three months before death and categorised as ‘1-14 days’, ‘15-30 days’, and ‘>30 days’. We also identified treatments during the last three months of life potentially administered alongside or instead of endocrine treatments: cortisone (ATC: H02AB), CDK4/6 (palbociclib [ATC: L01EF01], ribociclib [ATC: L01EF02], abemaciclib [ATC: L01EF03]) or hospital chemotherapy (procedure codes [in Swedish KVÅ]: DT107, DT108, DT112, DT116, DT135) (30).
Statistical analysis
For the primary analysis, we measured the proportion of decedents who continued, discontinued, initiated and did not use endocrine treatment during the last year of life to investigate the pattern of endocrine therapy use. For the secondary analysis, we used log-binomial generalised linear models. We explored mutually adjusted patient characteristics associated with a higher probability of endocrine therapy continuation compared to those who discontinued (reference category) in the prevalent-user cohort, and the associated factors with higher probability of initiation compared to constant no use (reference category) in the cohort of non-users. We chose log-binomial modelling strategy over logistic regression because the former outputs risk ratios (RR) that favour the interpretability of the results compared to the odds ratios generated by logistic regression. Additionally, odds ratios might overestimate the underlying risks in cohort studies when the outcome is common (31).
We performed three prespecified sensitivity analyses of our study’s primary aim where different cohort inclusion criteria were used. First, we included only patients aged 75 years or more because the Morin indicators (18), which categorised endocrine treatments as inadequate to initiate at the end of life were validated for this age group. Second, we included all the patients who died with breast cancer, regardless of metastatic status, because the ICD10 codes of C78 and C79 used to identify women with metastasis have not been validated in Sweden. However, these codes have previously been used to capture populations of metastatic breast cancer in Sweden (22, 32). Third, we included only those with breast cancer (ICD10-code: C50) as the underlying cause of death.
All analyses were performed with SAS software version 9.4 and R statistical software version 4.0.5.
Guidelines and ethical approval
The present study was reported in keeping with the REporting of studies Conducted using Observational Routinely collected health Data (RECORD) guidelines (33) (Supplementary eTable 5) and was approved by the Regional Ethical Review Board of Stockholm (dnr: 2016/1001-31/4, 2020-03525; 2021-02004).
Results
Characteristics of the study population
We identified 5045 women aged 65 or more who died with metastatic breast cancer in Sweden between 1 January 2016 and 31 December 2020. Overall, 74% (n=3719) of individuals were assumed to be hormone receptor positive based on ever-receiving endocrine treatment prescription. We further excluded 33 patients who died from acute and potentially unpredictable fatal event, 352 patients who did not have any breast cancer diagnosis code registered in the National Patient Register, and 229 patients first diagnosed with breast cancer close (≤3 months) to death. The final study population consisted of 3098 decedents with a median age of 78 years (IQR 72–85) at death (Table 1). Large share (39%) of women had six or more comorbidities with a median of five (IQR 3–7) (Supplementary eTable 7). The prevalence of frailty was twelve per cent, and around eleven per cent lived in a nursing home. Patients spent a median of eleven days (IQR 1–23) in the hospital during the last three months of life. Almost half (48%) had accumulated more than two years of endocrine treatment prior to the last three months of life, and 28% of women were identified as a recipient of multi-dose drug dispensing. A small number of women (n=19, 0.6% of study population) died from COVID-19. The prevalent users who had endocrine treatment prescription between twelve to three months before death (n=2185; 71% of study population) were generally older, more frequently resided in a nursing home and used multi-dose drug dispensing scheme compared to the non-user group (n=913; 29% of study population).
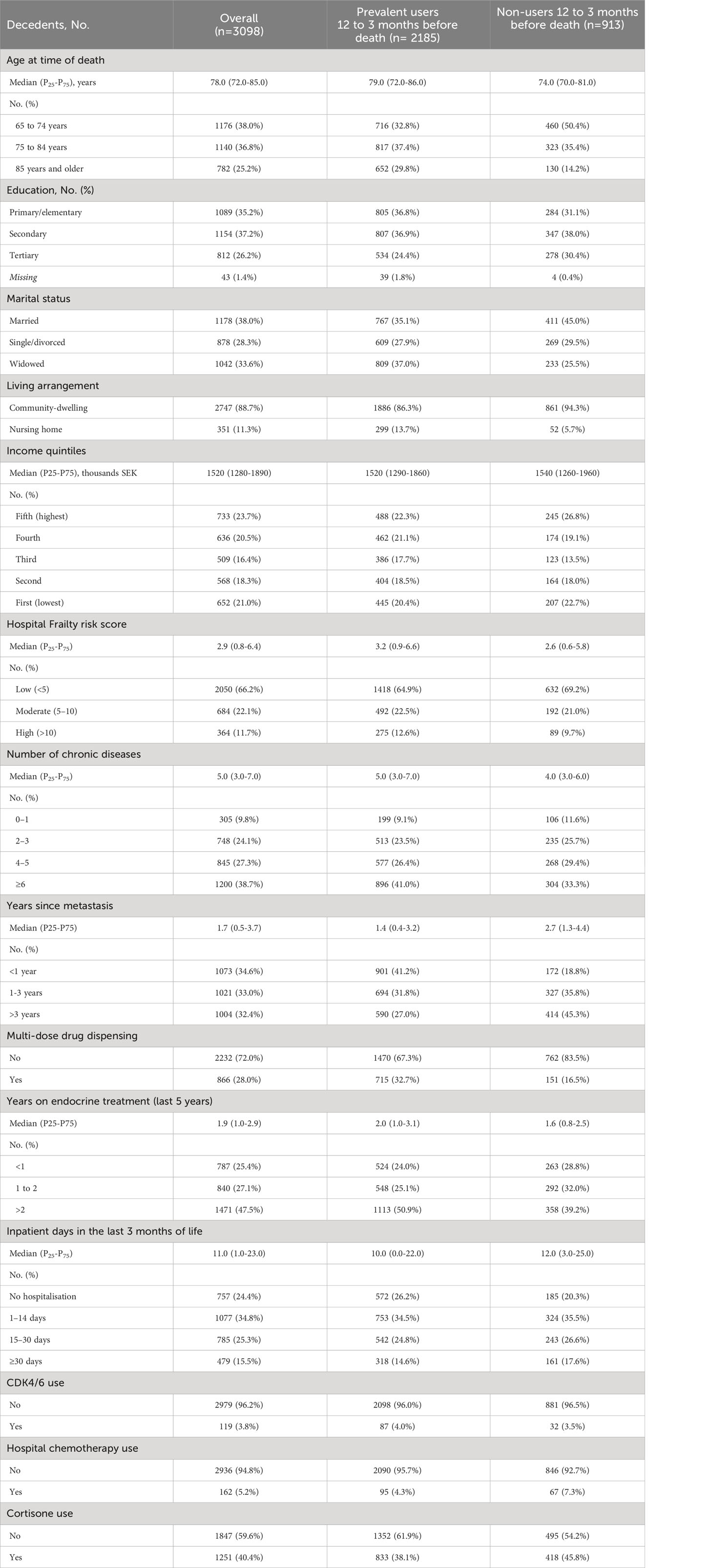
Table 1 Characteristics of women who died with hormone receptor-positive metastatic breast cancer, aged ≥65 years in Sweden, 2016-2020.
End-of-life treatment patterns and associated factors
During the last three months of life, endocrine treatment was continued by 1,217 women with hormone receptor-positive metastatic breast cancer. This corresponds to 39% of the entire cohort and 56% of the prevalent users. In contrast, 968 patients discontinued treatment (31% of the entire cohort, 44% of prevalent users) during the last year of life. Endocrine treatment was initiated during the last three months of life by 157 women, which accounts for 5% of the cohort and 17% of the previously non-user groups. Overall, 756 women (24% of the entire cohort) did not receive endocrine treatment during the last year of life (Table 2).

Table 2 Endocrine treatment patterns at the end of life of women who died with hormone receptor-positive metastatic breast cancer, aged ≥65 years in Sweden, 2016-2020.
Increased probability of endocrine treatment continuation (compared to discontinuation) was associated with higher age (RR85+ years: 1.26 [1.12-1.41]), multi-dose drug dispensing (RR: 1.22 [1.13-1.32]) and CDK4/6 use (RR 1.40 [1.25-1.58]) (Table 3). We found a lower probability of treatment continuation with higher education (RRtertirary education: 0.89 [0.81-0.98]) and chemotherapy use (RR: 0.66 [0.49-0.90]). Regarding treatment initiation (compared to no use), we found increased probability with the number of hospitalised days (RR1-14 inpatient days: 1.81 [1.12-2.91]), CDK4/6 use (3.16 [2.25-4.44]) and cortisone use (RR: 1.54 (1.17-2.04]). Those with earlier diagnosis of metastasis (RR>3 years: 0.49 [0.35-0.69]) or died in the year of 2020 (RR2020: 0.62 [0.38-1.00]) had lower propensity of treatment initiation.
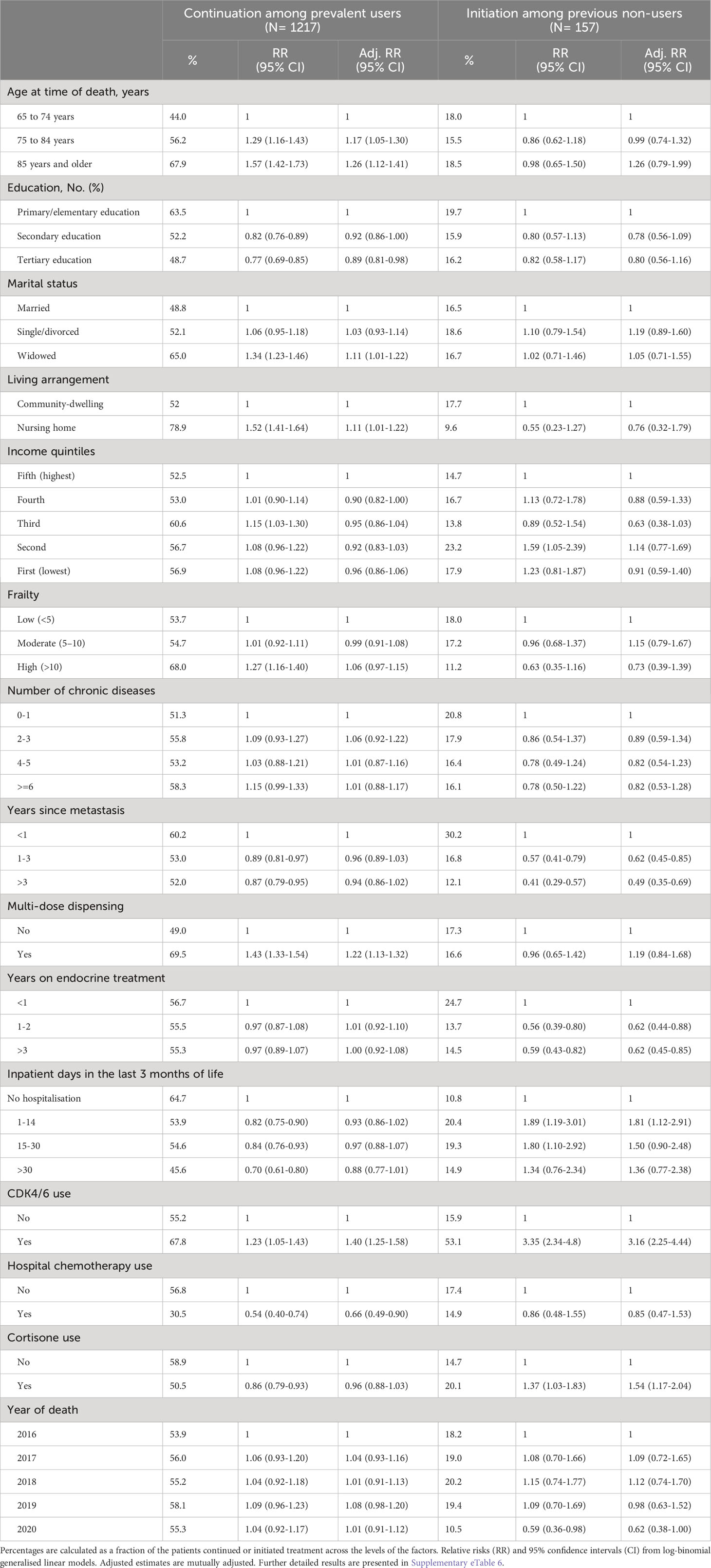
Table 3 Relative risks estimates of factors associated with endocrine treatment continuation and initiation at the end of life of women who died with hormone receptor-positive metastatic breast cancer, aged ≥65 years in Sweden, 2016-2020.
Sensitivity analyses
The prespecified sensitivity analyses showed that endocrine treatment continuation was equally the highest (47%) when we included in the cohort only patients aged 75 years and older, or included all breast cancer patients regardless of metastatic status. The endocrine treatment continuation was the lowest (37%) across the cohorts when only patients with breast cancer (ICD10-code: C50) as the underlying cause of death were included. The proportions of endocrine treatment initiation was the lowest (4%) in the cohort aged 75 years and older. In all the sensitivity analyses, the proportions of patients discontinuing treatment were lower than in the primary cohort. (Supplementary eTable 8).
Discussion
Main findings
In this nationwide register-based-cohort study of women aged 65 years and older with hormone receptor-positive metastatic breast cancer, we found that endocrine treatment was initiated by 5% in the last three months of life and continued by more than one-third of the study population, potentially past the point of benefit. Initiation has been deemed often inadequate and continuation questionable at the end of life of older people (18). The large difference in initiating and continuing treatment suggests different clinical decision-making mechanisms at the end of life. In our explorative analysis, endocrine treatment continuation was associated with higher age, multi-dose drug dispensing scheme and CDK4/6 use, while we found a negative association for higher education and chemotherapy use. Treatment initiation had a positive association with more hospitalised days, CDK4/6 and cortisone use. Little attention has been given to endocrine treatment in breast cancer patients near death. The high prevalence of treatment continuation in the last three months of life should alert clinicians to re-evaluate patients’ treatments close to death and avoid treatment with limited or no benefits. Whether the extent of end-of-life treatment with systematic endocrine therapies is justified should be studied further, also weighing in patient’s preferences, performance status and survival prognosis.
Interpretation and implications
The American Association of Clinical Oncologists suggests chemotherapy cessation near death (34), but no such recommendation is developed for systematic endocrine treatment at the end of life. The research on the appropriateness of end-of-life chemotherapy has possibly overshadowed discussions of other, less aggressive, systematic therapies such as endocrine treatments. Nevertheless, the potential adverse events of endocrine treatments (e.g., cardiovascular and musculoskeletal complications, depression) are non-negligible for older patients (13–16). Only a few studies include endocrine therapies in their definition of anticancer treatment (19–21). However, our estimates of older women who receive endocrine therapy near death surpass most estimates of the chemotherapy use (10, 11), indicating it should be considered when studying anticancer treatments. Overall, our findings are aligned with a study that reported a significant portion of women with breast cancer receive endocrine therapy alone or combined with chemo or immunotherapy at the end of life (21). Another study on patients with advanced cancer found that patients with breast cancer near death are at higher risk of receiving systematic anticancer therapy than other type of cancers due to the prevalent use of endocrine treatment (35).
We found that higher age is associated with the continuation (compared to discontinuation) of treatment. This contradicts earlier findings that older patients are less likely to receive anticancer treatment (36, 37), and that older age is associated with less likelihood of treatment continuation and initiation of prescribed drugs near death (24). Our results might partially reflect that patient involvement and shared decision–making decrease with age, resulting in continuation of routine prescriptions (38). We showed that higher educational attainment decreases the probability of end-of-life endocrine treatment continuation, which is supported by the notion that higher-educated individuals in general have higher health literacy and more control over their end-of-life care (39, 40). We found that chemotherapy use during the last three months was associated with lower a probability of endocrine treatment continuation, which might suggest a shift in disease management (i.e., attempt to relieve symptoms via palliative chemotherapy) (41). We further displayed that those who were not hospitalised are less likely to initiate treatment. This confirms the expectation that hospitalised patients receive more anticancer therapy at the end of life (20), which might be concerning given the increasing hospitalisation rates close to death (42). We showed a higher probability of endocrine treatment initiation and continuation if patients were also prescribed CDK4/6 treatment, which implies that they were in their earlier stages of the treatment course because CDK4/6 is recommended in first or second line (43). Furthermore, cortisone use was also associated with the initiation of endocrine treatment, indicating active adverse-effect control (e.g., headache, radicular pain) (41). Overall, our explorative findings should be considered hypothesis-generating, although they might also offer valuable insights to prescribers.
The considerable difference between the proportions of women initiating and continuing treatment at the end of life suggests a strong endowment effect (44): the aptitude not to initiate treatment but difficulty discontinuing. Furthermore, the continuation of endocrine treatment at a high rate at the end of life might be partially explained by the lower expected toxicity of endocrine treatments compared to other systematic anticancer therapies (e.g., chemotherapy, immunotherapy). Clinicians may view endocrine therapies as harmless and continue prescribing them, given their long-term indications. On the other hand, it might also reflect routine-based prescribing without carefully considering and re-evaluating the benefits and harms. Older people have fewer drug prescription changes, which is partly attributable to multi-dose drug dispensing (45). This is supported by our finding of increased probability of continuing treatment under the multi-dose drug dispensing scheme. Alternatively, our results might reflect that the women or their families want to continue these treatments regardless of potential adverse effects (46, 47). Patients and caregivers might equate continued treatment with not giving up, while clinicians might not want to deprescribe these medications to maintain hope (48, 49). Also, estimating the futility breaking point (i.e., the point in time after which the risks of the treatment outweigh its benefits) is both challenging and highly uncertain. However, simple tools like the ‘surprise question’ (50) or the Supportive and Palliative Care Indicators Tool (SPICT) (51) may help clinicians ascertain when treatment discontinuation should be discussed with the patient.
Our findings regarding women initiating endocrine treatment at the end of life might reflect several non-mutually exclusive mechanisms. Most importantly, estimating the remaining life expectancy of patients at the end of life is complicated (52). Clinicians may overestimate the benefit and underestimate the harms of the treatments because of cognitive bias (e.g., framing effects, impact and affect bias) (44, 53, 54). Also, patients might be considered well-functioning; thus, the active anticancer treatment seems appropriate. This might be reflected in our results, where we showed that those who had active treatment with CDK4/6 were also more likely to initiate endocrine treatment. While a study based on a panel of forty European experts classified endocrine treatments as inadequate to initiate at the end of life of older people (18), our study does not provide answers to whether the extent of treatment initiation we observed is indeed inadequate. However, our results highlight a further need to delineate potential pathways of treatment initiation of anticancer treatments at the end of life.
From a research perspective, our study highlights the need to further study to what extent systematic endocrine treatments can be considered as potential overtreatment. From a clinical practice perspective, we underline the importance of continuously re-evaluating patients’ ongoing prescriptions near death, especially among the older, less educated, and those with the multi-dose drug dispensing scheme. From a policy perspective, our study demonstrates a need to focus on quaternary prevention and advance care planning initiatives to prevent the overuse of medications at the end of life (55–57).
Strengths and limitations
To our knowledge, this is the first Swedish study to evaluate endocrine treatment patterns at the end of life in a population with metastatic breast cancer. However, several limitations should be acknowledged. First, the mortality follow-back design potentially underestimates the prognostic uncertainty that the prescribers experienced (some women might have died unexpectedly, which could explain why endocrine treatments were initiated or continued near death). However, we attempted to mitigate this bias by excluding those who died from sudden and unexpected causes of death. Second, the clinical appropriateness of prescribing could not be determined based on administrative data alone, since, among other factors, patient preferences, functional status, disease severity and prognosis were unavailable (58); thus, the presented estimates should be interpreted with caution. Third, patients might have been misclassified as metastatic due to other primary cancers. However, all individuals in our study sample had a diagnosis of breast cancer in their death certificate as well as in their inpatient or outpatient records at least three months before death. We also performed several sensitivity analyses demonstrating that altering the study population does not meaningfully change the results. Fourth, the National Prescribed Drug Register only contains data about prescription drugs dispensed through pharmacies. Nursing home drug storerooms or hospital-dispensed drugs are not included, which might have led to an underestimation of endocrine treatment use. Also, it is impossible to ascertain from the register data whether the patient consumed the dispensed drug or not. Some patients may have stopped using the treatments earlier than our study results reflect. Fifth, patients were assumed to be hormone receptor-positive if they received an endocrine treatment prescription in the previous five years because immunohistochemistry test results are not recorded in the register. This is also why we did not further classify patients according to HER2-status. Sixth, the covariate of chemotherapy use might suffer from non-differential misclassification due to the potential underreporting of the procedure codes that were used to capture this variable (30). Seventh, we presented multiple estimates from the same model, which might introduce bias known as the “Table 2 fallacy” (59). Nonetheless, we regard this analysis as exploratory and hypothesis generating. Finally, our results may only be generalisable to settings similar to Sweden.
Conclusion
In our nationwide cohort study, more than one third of older women with hormone receptor-positive metastatic breast cancer used endocrine treatments at the very last part of life, potentially past the point where treatment has a benefit. In addition, we found that endocrine treatment patterns differ across age, education, drug-dispensing scheme or among those with intensive treatments. Clinicians should be provided with training and resources to guide the deprescribing process near death of older individuals to reduce the burden of drug treatments and their potential harmful effects. Further research is warranted to determine whether our results reflect overtreatment at the end of life once patients’ preferences and survival prognosis are considered.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Data may be obtained from a third party and are not publicly available. Clinical data cannot be made publicly available because of privacy issues. However, additional results are available in the Supplementary Files. Requests to access these datasets should be directed to c29jaWFsc3R5cmVsc2VuQHNvY2lhbHN0eXJlbHNlbi5zZQ==.
Ethics statement
The study was approved by the Regional Ethical Review Board in Stockholm (dnr: 2016/1001-31/4, 2020-03525, 2021-02004).
Author contributions
MS, JW conceived and designed the study. MS performed the statistical analysis, interpreted the data, drafted, and critically revised the manuscript. JW, ACL, LM, HL and KJ interpreted the data and critically revised the manuscript. KJ obtained funding and acquired the data. KJ and JW provided supervision. KJ and MS are the guarantors of the study and data integrity. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by funding from the Swedish Research Council for Health, Working Life and Welfare (FORTE) and KID-funding. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest
MS received consulting fees from Parexel, Pfizer and Macanda. HL received honoraria from Lilly, AstraZeneca, Novartis, Daiichi Sankyo, and participated on a Data Safety Monitoring Board or Advisory Board for Lilly, Oasmia Pharmaceutical AB, MSD Oncology, Daiichi Sankyo, Novartis, Pierre Fabre, Seattle Genetics, BioNTech.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1223563/full#supplementary-material
References
1. Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Pineros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Int J Cancer (2021). doi: 10.1002/ijc.33588
2. Mariotto AB, Etzioni R, Hurlbert M, Penberthy L, Mayer M. Estimation of the number of women living with metastatic breast cancer in the United States. Cancer Epidemiol Biomarkers Prev (2017) 26:809–15. doi: 10.1158/1055-9965.EPI-16-0889
3. Crivellari D, Aapro M, Leonard R, von Minckwitz G, Brain E, Goldhirsch A, et al. Breast cancer in the elderly. J Clin Oncol (2007) 25:1882–90. doi: 10.1200/JCO.2006.10.2079
4. Biganzoli L, Battisti NML, Wildiers H, McCartney A, Colloca G, Kunkler IH, et al. Updated recommendations regarding the management of older patients with breast cancer: a joint paper from the European Society of Breast Cancer Specialists (EUSOMA) and the International Society of Geriatric Oncology (SIOG). Lancet Oncol (2021) 22:e327–40. doi: 10.1016/S1470-2045(20)30741-5
5. Menjak IB, Jerzak KJ, Desautels DN, Pritchard KI. An update on treatment for post-menopausal metastatic breast cancer in elderly patients. Expert Opin Pharmacother (2018) 19:597–609. doi: 10.1080/14656566.2018.1454431
6. Prigerson HG, Bao Y, Shah MA, Paulk ME, LeBlanc TW, Schneider BJ, et al. Chemotherapy use, performance status, and quality of life at the end of life. JAMA Oncol (2015) 1:778–84. doi: 10.1001/jamaoncol.2015.2378
7. Fang P, Jagsi R, He W, Lei X, Campbell EG, Giordano SH, et al. Rising and falling trends in the use of chemotherapy and targeted therapy near the end of life in older patients with cancer. J Clin Oncol (2019) 37:1721–31. doi: 10.1200/JCO.18.02067
8. Rochigneux P, Raoul JL, Beaussant Y, Aubry R, Goldwasser F, Tournigand C, et al. Use of chemotherapy near the end of life: what factors matter? Ann Oncol (2017) 28:809–17. doi: 10.1093/annonc/mdw654
9. Senkus E, Łacko A. Over-treatment in metastatic breast cancer. Breast (2017) 31:309–17. doi: 10.1016/j.breast.2016.06.024
10. Edman Kessler L, Sigfridsson J, Hatzidaki D, Bergh J, Foukakis T, Georgoulias V, et al. Chemotherapy use near the end-of-life in patients with metastatic breast cancer. Breast Cancer Res Treat (2020) 181:645–51. doi: 10.1007/s10549-020-05663-w
11. Wallington M, Saxon EB, Bomb M, Smittenaar R, Wickenden M, McPhail S, et al. 30-day mortality after systemic anticancer treatment for breast and lung cancer in England: a population-based, observational study. Lancet Oncol (2016) 17:1203–16. doi: 10.1016/S1470-2045(16)30383-7
12. Jerusalem G, Neven P, Marinsek N, Zhang J, Degun R, Benelli G, et al. Patterns of resource utilization and cost for postmenopausal women with hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer in Europe. BMC Cancer (2015) 15:787. doi: 10.1186/s12885-015-1762-3
13. Rugo HS, Rumble RB, Macrae E, Barton DL, Connolly HK, Dickler MN, et al. Endocrine therapy for hormone receptor-positive metastatic breast cancer: American society of clinical oncology guideline. J Clin Oncol (2016) 34:3069–103. doi: 10.1200/JCO.2016.67.1487
14. Bonneterre J, Buzdar A, Nabholtz JM, Robertson JF, Thürlimann B, von Euler M, et al. Anastrozole is superior to tamoxifen as first-line therapy in hormone receptor positive advanced breast carcinoma. Cancer (2001) 92:2247–58. doi: 10.1002/1097-0142(20011101)92:9<2247::AID-CNCR1570>3.0.CO;2-Y
15. Paridaens RJ, Dirix LY, Beex LV, Nooij M, Cameron DA, Cufer T, et al. Phase III study comparing exemestane with tamoxifen as first-line hormonal treatment of metastatic breast cancer in postmenopausal women: the European Organisation for Research and Treatment of Cancer Breast Cancer Cooperative Group. J Clin Oncol (2008) 26:4883–90. doi: 10.1200/JCO.2007.14.4659
16. Howell A, Cuzick J, Baum M, Buzdar A, Dowsett M, Forbes JF, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years' adjuvant treatment for breast cancer. Lancet (2005) 365:60–2. doi: 10.1016/S0140-6736(04)17666-6
17. Shrestha A, Martin C, Burton M, Walters S, Collins K, Wyld L. Quality of life versus length of life considerations in cancer patients: A systematic literature review. Psycho-oncology (2019) 28:1367–80. doi: 10.1002/pon.5054
18. Morin L, Laroche ML, Vetrano DL, Fastbom J, Johnell K. Adequate, questionable, and inadequate drug prescribing for older adults at the end of life: a European expert consensus. Eur J Clin Pharmacol (2018) 74:1333–42. doi: 10.1007/s00228-018-2507-4
19. Wein L, Rowe C, Brady B, Handolias D, Lipton L, Pook D, et al. Prevalence of systemic anticancer therapy for patients within the last 30 days of life: experience in a private hospital oncology group. Intern Med J (2017) 47:280–3. doi: 10.1111/imj.13260
20. Sivendran S, Lynch S, McNaughton C, Wong R, Svetec S, Moore JH, et al. Anticancer therapy at the end of life: lessons from a community cancer institute. J Palliative Care (2021) 36:87–92. doi: 10.1177/0825859719851484
21. Mattsson TO, Pottegård A, Jørgensen TL, Green A, Bliddal M. End-of-life anticancer treatment - a nationwide registry-based study of trends in the use of chemo-, endocrine, immune-, and targeted therapies. Acta Oncol (2021) 60:961–7. doi: 10.1080/0284186X.2021.1890332
22. Valachis A, Carlqvist P, Ma Y, Szilcz M, Freilich J, Vertuani S, et al. Overall survival of patients with metastatic breast cancer in Sweden: a nationwide study. Br J Cancer (2022) 127(4):720–5. doi: 10.1038/s41416-022-01845-z
23. Morin L, Johnell K, Laroche ML, Fastbom J, Wastesson JW. The epidemiology of polypharmacy in older adults: register-based prospective cohort study. Clin Epidemiol (2018) 10:289–98. doi: 10.2147/CLEP.S153458
24. Morin L, Wastesson JW, Laroche ML, Fastbom J, Johnell K. How many older adults receive drugs of questionable clinical benefit near the end of life? A cohort study. Palliat Med (2019) 33:1080–90. doi: 10.1177/0269216319854013
25. Halldén K. The Swedish educational system and classifying education using the ISCED-97, The international standard classification of education (ISCED97). An evaluation of content and criterion validity for 15 European countries. Mannheim: University of Mannheim (2008).
26. Calderon-Larranaga A, Vetrano DL, Onder G, Gimeno-Feliu LA, Coscollar-Santaliestra C, Carfi A, et al. Assessing and measuring chronic multimorbidity in the older population: A proposal for its operationalization. J Gerontol A Biol Sci Med Sci (2017) 72:1417–23. doi: 10.1093/gerona/glw233
27. Gilbert T, Neuburger J, Kraindler J, Keeble E, Smith P, Ariti C, et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet (2018) 391:1775–82. doi: 10.1016/S0140-6736(18)30668-8
28. Meyer AC, Sandström G, Modig K. Nationwide data on home care and care home residence: presentation of the Swedish Social Service Register, its content and coverage. Scand J Public Health (2021) 50(7):946–58 14034948211061016. doi: 10.1177/14034948211061016
29. Johnell K, Fastbom J. Multi-dose drug dispensing and inappropriate drug use: A nationwide register-based study of over 700,000 elderly. Scand J Prim Health Care (2008) 26:86–91. doi: 10.1080/02813430802022196
30. Szilcz M, Wastesson JW, Morin L, Calderon-Larranaga A, Lambe M, Johnell K. Potential overtreatment in end-of-life care in adults 65 years or older dying from cancer: applying quality indicators on nationwide registries. Acta Oncol (2022) 61:1437–45. doi: 10.1080/0284186X.2022.2153621
31. Knol MJ, Le Cessie S, Algra A, Vandenbroucke JP, Groenwold RH. Overestimation of risk ratios by odds ratios in trials and cohort studies: alternatives to logistic regression. Cmaj (2012) 184:895–9. doi: 10.1503/cmaj.101715
32. Valachis A, Carlqvist P, Szilcz M, Freilich J, Vertuani S, Holm B, et al. Use of classifiers to optimise the identification and characterisation of metastatic breast cancer in a nationwide administrative registry. Acta Oncol (2021) 60(12):1604–10. doi: 10.1080/0284186X.2021.1979645
33. Benchimol EI, Smeeth L, Guttmann A, Harron K, Moher D, Petersen I, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PloS Med (2015) 12:e1001885. doi: 10.1371/journal.pmed.1001885
34. Schnipper LE, Smith TJ, Raghavan D, Blayney DW, Ganz PA, Mulvey TM, et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: the top five list for oncology. J Clin Oncol (2012) 30:1715–24. doi: 10.1200/JCO.2012.42.8375
35. Wadhwa D, Hausner D, Popovic G, Pope A, Swami N, Maganti M, et al. Systemic anti-cancer therapy use in palliative care outpatients with advanced cancer. J Palliative Care (2021) 36:78–86. doi: 10.1177/0825859720975949
36. Craigs CL, Bennett MI, Hurlow A, West RM, Ziegler LE. Older age is associated with less cancer treatment: a longitudinal study of English cancer patients. Age Ageing (2018) 47:833–40. doi: 10.1093/ageing/afy094
37. Hamel MB, Lynn J, Teno JM, Covinsky KE, Wu AW, Galanos A, et al. Age-related differences in care preferences, treatment decisions, and clinical outcomes of seriously ill hospitalized adults: lessons from SUPPORT. J Am Geriatrics Soc (2000) 48:S176–82. doi: 10.1111/j.1532-5415.2000.tb03129.x
38. Chambaere K, Rietjens JA, Smets T, Bilsen J, Deschepper R, Pasman HR, et al. Age-based disparities in end-of-life decisions in Belgium: a population-based death certificate survey. BMC Public Health (2012) 12:447. doi: 10.1186/1471-2458-12-447
39. Chambaere K, Rietjens JA, Cohen J, Pardon K, Deschepper R, Pasman HR, et al. Is educational attainment related to end-of-life decision-making? A large post-mortem survey in Belgium. BMC Public Health (2013) 13:1055. doi: 10.1186/1471-2458-13-1055
40. Shim JK. Cultural health capital: A theoretical approach to understanding health care interactions and the dynamics of unequal treatment. J Health Soc Behav (2010) 51:1–15. doi: 10.1177/0022146509361185
41. Cherny NI, Paluch-Shimon S, Berner-Wygoda Y. Palliative care: needs of advanced breast cancer patients. Breast Cancer (Dove Med Press) (2018) 10:231–43. doi: 10.2147/BCTT.S160462
42. Szilcz M, Wastesson JW, Johnell K, Morin L. Unplanned hospitalisations in older people: illness trajectories in the last year of life. BMJ Support Palliat Care (2021), bmjspcare–2020-002778. doi: 10.1136/bmjspcare-2020-002778
43. Shah M, Nunes MR, Stearns V. CDK4/6 inhibitors: game changers in the management of hormone receptor–positive advanced breast cancer? Oncol (Williston Park) (2018) 32:216–22. doi: 10.1007/s11864-017-0443-7
44. Scott IA, Soon J, Elshaug AG, Lindner R. Countering cognitive biases in minimising low value care. Med J Aust (2017) 206:407–11. doi: 10.5694/mja16.00999
45. Wallerstedt SM, Fastbom J, Johnell K, Sjöberg C, Landahl S, Sundström A. Drug treatment in older people before and after the transition to a multi-dose drug dispensing system–a longitudinal analysis. PloS One (2013) 8:e67088. doi: 10.1371/journal.pone.0067088
46. Balmer CE, Thomas P, Osborne RJ. Who wants second-line, palliative chemotherapy? Psychooncology (2001) 10:410–8. doi: 10.1002/pon.538
47. Laryionava K, Hauke D, Heußner P, Hiddemann W, Winkler EC. "Often relatives are the key […]" -family involvement in treatment decision making in patients with advanced cancer near the end of life. Oncologist (2021) 26:e831–7. doi: 10.1002/onco.13557
48. Matsuyama R, Reddy S, Smith TJ. Why do patients choose chemotherapy near the end of life? A review of the perspective of those facing death from cancer. J Clin Oncol (2006) 24:3490–6. doi: 10.1200/JCO.2005.03.6236
49. Bluhm M, Connell CM, De Vries RG, Janz NK, Bickel KE, Silveira MJ. Paradox of prescribing late chemotherapy: oncologists explain. J Oncol Pract (2016) 12:e1006–15. doi: 10.1200/JOP.2016.013995
50. van Lummel EV, Ietswaard L, Zuithoff NP, Tjan DH, van Delden JJ. The utility of the surprise question: A useful tool for identifying patients nearing the last phase of life? A systematic review and meta-analysis. Palliat Med (2022) 36:1023–46. doi: 10.1177/02692163221099116
51. Piers R, Brauwer ID, Baeyens H, Velghe A, Hens L, Deschepper E, et al. Supportive and Palliative Care Indicators Tool prognostic value in older hospitalised patients: a prospective multicentre study. BMJ Support Palliative Care (2021), bmjspcare–2021-003042. doi: 10.1136/bmjspcare-2021-003042
52. Viganò A, Dorgan M, Buckingham J, Bruera E, Suarez-Almazor ME. Survival prediction in terminal cancer patients: a systematic review of the medical literature. Palliat Med (2000) 14:363–74. doi: 10.1191/026921600701536192
53. White N, Reid F, Harris A, Harries P, Stone P. A systematic review of predictions of survival in palliative care: how accurate are clinicians and who are the experts? PloS One (2016) 11:e0161407. doi: 10.1371/journal.pone.0161407
54. Hole B, Salem J. How long do patients with chronic disease expect to live? A systematic review of the literature. BMJ Open (2016) 6(12):e012248. doi: 10.1136/bmjopen-2016-012248
55. Martins C, Godycki-Cwirko M, Heleno B, Brodersen J. Quaternary prevention: reviewing the concept. Eur J Gen Pract (2018) 24:106–11. doi: 10.1080/13814788.2017.1422177
56. Rietjens JAC, Sudore RL, Connolly M, van Delden JJ, Drickamer MA, Droger M, et al. Definition and recommendations for advance care planning: an international consensus supported by the European Association for Palliative Care. Lancet Oncol (2017) 18:e543–51. doi: 10.1016/S1470-2045(17)30582-X
57. Jimenez G, Tan WS, Virk AK, Low CK, Car J, Ho AHY. Overview of systematic reviews of advance care planning: summary of evidence and global lessons. J Pain Symptom Manag (2018) 56:436–459.e25. doi: 10.1016/j.jpainsymman.2018.05.016
58. DuMontier C, Loh KP, Bain PA, Silliman RA, Hshieh T, Abel GA, et al. Defining undertreatment and overtreatment in older adults with cancer: A scoping literature review. J Clin Oncol (2020) 38:2558–69. doi: 10.1200/JCO.19.02809
Keywords: metastatic breast cancer, end of life, endocrine treatment, palliative care, overtreatment, Sweden
Citation: Szilcz M, Wastesson JW, Calderón-Larrañaga A, Morin L, Lindman H and Johnell K (2023) Endocrine treatment near the end of life among older women with metastatic breast cancer: a nationwide cohort study. Front. Oncol. 13:1223563. doi: 10.3389/fonc.2023.1223563
Received: 16 May 2023; Accepted: 21 September 2023;
Published: 09 October 2023.
Edited by:
Dharmendra Kumar Yadav, Gachon University, Republic of KoreaReviewed by:
Feng Liu-Smith, University of Tennessee Health Science Center (UTHSC), United StatesVijayasteltar B Liju, Ben-Gurion University of the Negev, Israel
Copyright © 2023 Szilcz, Wastesson, Calderón-Larrañaga, Morin, Lindman and Johnell. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Máté Szilcz, bWF0ZS5zemlsY3pAa2kuc2U=