 Yuan Zhao
Yuan Zhao Leiwen Tang
Leiwen Tang Jing Shao
Jing Shao Dandan Chen1
Dandan Chen1 Yueying Jiang
Yueying Jiang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 20 September 2023
Sec. Breast Cancer
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1222947
This article is part of the Research Topic Physical Exercise and other Health Behaviors in the Management of Breast Cancer Patients View all 5 articles
Background: Exercise has the potential to reduce symptoms for breast cancer patients during adjuvant treatment, and high-quality systematic reviews are essential for guiding clinical practice. The objective of this umbrella review is to examine current research evidence concerning the effectiveness of exercise on symptom management in breast cancer patients undergoing adjuvant treatment.
Methods: An umbrella review was conducted. We searched for eligible systematic reviews through 11 databases until August 13rd, 2023. Two authors independently screened titles and abstracts, assessing the full-text studies based on inclusion criteria. We used AMSTAR-2 to appraise the quality of the meta-analyses. The results would be presented with narrative summaries if the replication rate of the original study for a symptom was higher than 5% (calculated via the Corrected Covered Area, CCA). The protocol was documented in the PROSPERO registry (CRD42023403990).
Results: Of the 807 systematic reviews identified, 15 met the inclusion criteria, and 7 symptoms were the main focus. The main form of exercise mentioned was aerobic combined resistance exercise. The results of the quality assessment were mostly critically low (10/15). The repetition rate calculated by CCA showed moderate to very high repetition rates (10% to 18.6%). The findings of the included reviews indicated that the effects of exercise on relieving symptoms during breast cancer adjuvant treatment were mixed.
Conclusions: Research is still needed to confirm the majority of studies’ recommendations for exercise during adjuvant treatment for breast cancer patients, as it is crucial for managing symptoms in the rehabilitation process. To increase the efficiency of exercise in symptom management, future studies may focus more on the application of bridge symptoms, symptom networks, and ecological instantaneous assessment.
According to the 2020 Global Cancer Statistics (1), female breast cancer has surpassed lung cancer as the most commonly diagnosed cancer, with an estimated 2.3 million new cases (11.7%) and 685000 deaths, making it already the fifth leading cause of cancer mortality worldwide. Breast cancer is the most common cancer among women, accounting for one in four new cases and one in six cancer-related deaths worldwide (1). In China, breast cancer makes up 15% of all new cancer cases in women, and it is the primary reason for cancer deaths in those under 45 (2).
With the improvements in early screening and treatment technologies, the survival period of breast cancer patients is prolonged. The need to improve the quality of life during cancer rehabilitation is becoming an increasingly important research topic with the rising number of survivors, particularly in breast cancer, the most common malignancy among women (3). According to the most recent statistics from the US, there are more than 4 million breast cancer survivors, including those who are still receiving treatment and those who have finished (4). This suggested that many breast cancer survivors must deal with persistently unpleasant side effects brought on by cyclical or long-term therapies such as chemotherapy, hormonal therapy, and radiation therapy (5). The majority of cancer therapies are assessed for safety based on acute side effects rather than chronic conditions that, while less serious, can have a considerable impact on the survivors’ quality of life for years to come (6). Oncology patients frequently only receive follow-up care that assesses tumor recurrence rather than treating other problems that are occasionally even overlooked. One of these easily overlooked problems is symptoms, which are also the main clinical manifestation of the adverse outcomes of the neoplasm or its therapy (7). Fatigue, sleeplessness, nausea, and vomiting are typical side effects of chemotherapy which often appear in the early stages of the chemotherapy cycle and may change afterward (8). Common and known side effects derived from post-chemotherapy hormone therapies, such as those based on aromatase inhibitors (AIs) and tamoxifen, may result in musculoskeletal, vasomotor, and urinary symptoms (9). Radiation therapy may bring symptoms like lymphedema, and cardiotoxicity (10, 11). Whether concurrent or not, most breast cancer patients experience these adjuvant treatments, as well as the distressing side effects associated with the treatment process, which can significantly impact patient outcomes.
Patients with breast cancer undergo not only medication-assisted treatment, or radiation therapy but also lifestyle and mental modifications as part of their rehabilitation process (12). Exercise oncology during this rehabilitation is receiving more and more attention (13, 14). Quality of life and physical activity levels during breast cancer rehabilitation are highly associated. Exercise may help to improve the quality of life, treatment-related symptoms, adjuvant therapy completion rates, and even health outcomes of breast cancer patients (15–18), making it a crucial component of rehabilitation care. Exercise benefits breast cancer patients with fatigue (19), depression and anxiety (20), musculoskeletal symptoms linked to aromatase inhibitors (21), lymphedema (22, 23), and inflammation (5), according to several studies. Some studies have also proven that exercise reduces the risk of developing other chronic diseases in breast cancer patients (24, 25).
Different exercise programs have different types, intensities, durations, and frequencies. When considering the type and dose of exercise, a multicenter study suggested that a higher volume of aerobic exercise or combined exercise may prevent the deterioration of symptoms related to adjuvant therapy (26). Another trial showed that supervised, moderate- to high-intensity resistance and aerobic exercise programs were most effective in reducing fatigue, musculoskeletal, and gastrointestinal symptoms for breast cancer patients receiving chemotherapy (17). And the combination of exercise with whole-body vibration might be considered a secure and well-tolerated intervention to reduce musculoskeletal symptoms, which was revealed in a pilot study (27). Recently, a randomized controlled study (28) examined the effects of various exercise doses on patient-reported outcomes in breast cancer patients during chemotherapy. But the trend plots in this study for various symptoms over time revealed no absolute association between exercise dose and symptoms. With regard to the phase of the exercise, some trials explored exercise programs during or after adjuvant therapy for breast cancer (29, 30), other researchers indicated that exercise should begin early in the diagnosis of breast cancer (31, 32), which might help to achieve the exercise goal at the end of adjuvant therapy and also made it easier to maintain exercise during rehabilitation after discharge. In terms of the duration of exercise, most studies followed up for a short term, which was within 6 months (33, 34).
There is still work to be done in successfully transferring exercise oncology into clinical practice (35) since various breast cancer patients have distinct exercise demands and require different exercise programs. Given the side effects of breast cancer adjuvant treatments and the benefits of exercise in reducing treatment-related symptoms, current evidence concerning the effectiveness of exercise on symptoms among breast cancer patients receiving adjuvant treatment requires being thoroughly summarized through Umbrella Review. The characteristics of exercise interventions, the adjuvant treatments that breast cancer survivors received, and the symptoms they underwent are the major items we concentrate on and extract.
This umbrella review protocol was documented in the PROSPERO registry (CRD42023403990).
We used JBI’s three-step process to conduct a more thorough search of the relevant articles. First, we conducted a limited search in two databases (PubMed and CINAHL), and then we examined the text words in the titles and abstracts of the papers we found. Up until December 8th, 2022, we conducted additional searches in databases, namely PubMed, Web of Science (WOS), the Cochrane Library, the Cumulative Index of Nursing and Allied Health (CINAHL) Plus with full text, Excerpta Medica dataBASE (EMBASE), PsycINFO, Wanfang Data Knowledge Service Platform, China National Knowledge Infrastructure (CNKI), China Biomedical Literature Database (CBMdisc), China Science and Technology Journal Database (VIP). With regard to the five main themes of “breast cancer,” “adjuvant treatment,” “exercise,” “symptoms,” and “systematic review,” we employed Medical Subject Headings (MeSH) terms and free texts based on PICOS (please see Table 1 for the precise search strategies). We manually searched the references of the articles we chose to find additional sources. All acquired articles are saved in NoteExpress. We conducted a search update on August 13rd, 2023, and added searches in Scopus and the Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library.
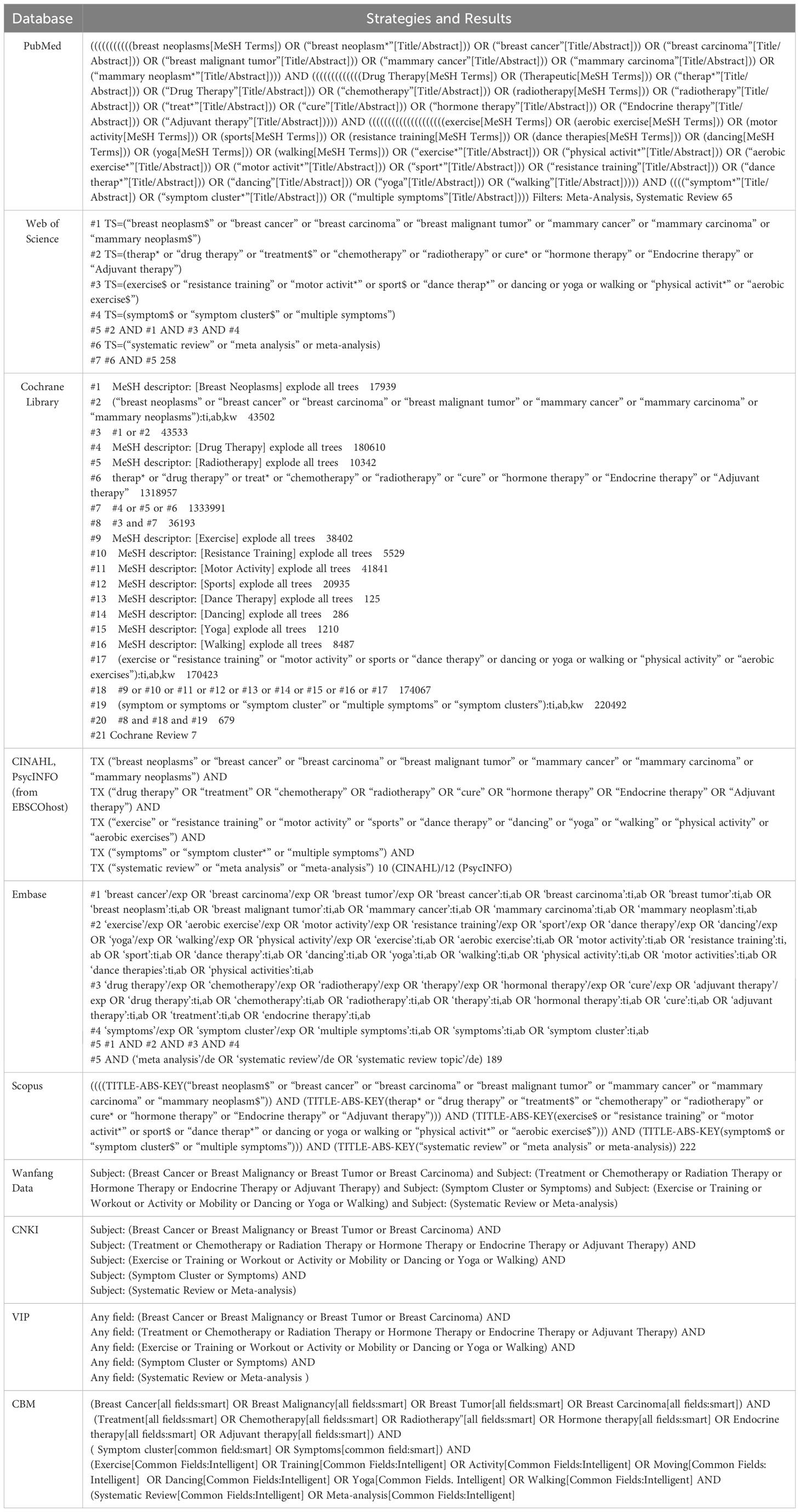
Table 1 Search strategies.
The PICOS framework (Population, Intervention, Comparison, Outcome, Study design) was used for the inclusion and exclusion criteria for this literature: (1) the study population is breast cancer patients; (2) studies assess the effects of exercise on symptom management, with the exercise intervention spanning the period from initiation to the cessation of cancer adjuvant treatment; (3) the control group can be in any intervention; (4) studies measuring the symptoms as primary or secondary outcome indicators (these symptoms are measurable using symptom screening tools and may have a clinical impact on breast cancer patients, they may not always meet established diagnostic criteria.); (5) studies are meta-analyses conducted with systematic methods (both observational and interventional studies were available). Included studies required to outline at least one adjuvant treatment used on breast cancer patients. Due to the dearth of resources for translation into other languages, we only considered studies published in English or Chinese. Less than three studies or 100 individuals were not included. We chose the one that provided the most in-depth details in the repeated literature. The updated reviews were only included in their most recent iteration. Excluded items included books, editorials, comments, trial procedures, and conference papers.
Two researchers independently evaluated the retrieved eligible articles by scanning the titles and abstracts of each study in accordance with the inclusion criteria after duplicates had been moved by NoteExpress. The remaining articles were then read in their entirety. Any disputes were settled through conversation or by requesting a third party.
The first author, publication year, country, guidelines, main databases, number of primary studies and participants, risk of bias, data synthesis, and main conclusion were among the data that two researchers independently extracted from the final eligible studies. We specifically extracted the characteristics of participants and data on how well exercise programs affected some symptoms. A file was used to hold all of the extracted data. Any discrepancies in the extracted data were discussed and resolved.
We used the AMSTAR-2 (A Measurement Tool to Assess Systematic Reviews version 2) (36) to assess the methodological quality of included meta-analyses. The 16 items in this measurement tool can each be responded to “yes”, “partial yes”, or “no”, among which seven items (items 2,4,7,9,11,13,15) are critical domains. AMSTAR-2 has shown good consistency, construct validity, and feasibility. Its overall reliability could be rated as “high” (no weakness or one noncritical item), “moderate” (more than one noncritical item), “low” (one critical item with or without noncritical items), or “critically low” (more than one critical item with or without noncritical items). Independent couples of two authors performed data extraction and the methodological assessment. In the same way, whenever there were any differences during this procedure, we talked about them or asked a third person for assistance.
The possibility of duplicate primary studies often exists in meta-analyses of similar topics. Current guidelines to address overlap suggest that assessing and documenting the degree of overlap in primary studies, calculated via the Corrected Covered Area (CCA) is a promising method (37). The calculation formula is “CCA=(N-r)/(r*c-r)”. (c=Number of included reviews, r=Number of publications of primary studies, N=Number of total primary studies including double counting). The calculation results could be slight (CCA<5%), moderate (CCA from 6% to 10%), high (CCA from 11% to 15%), and very high overlap (CCA>15%). We quantitatively pooled the final effect sizes when a certain symptom was estimated with a low repetition rate (less than 5%); otherwise, we would narratively summarize our findings. We provide a specific calculation of the repetition rate in Supplementary Material 5.
The literature search revealed 807 records, of which 317 were duplicates. After screening titles and abstracts, we excluded 387 reports on the first round: 294 studies were irrelevant to the theme; 36 had other interventions or included multiple interventions; 32 studies had ineligible literature types (narrative review, integrated review, umbrella review, or overview, scoping review); 16 studies without symptom outcomes; 7 protocols; 1 study was unavailable; 1 conference abstract; 103 reports remained. We conducted a second round of selection by reading the full text. In the end, we included 15 articles, of which 3 were Cochrane reviews. A PRISMA diagram is shown in Figure 1.
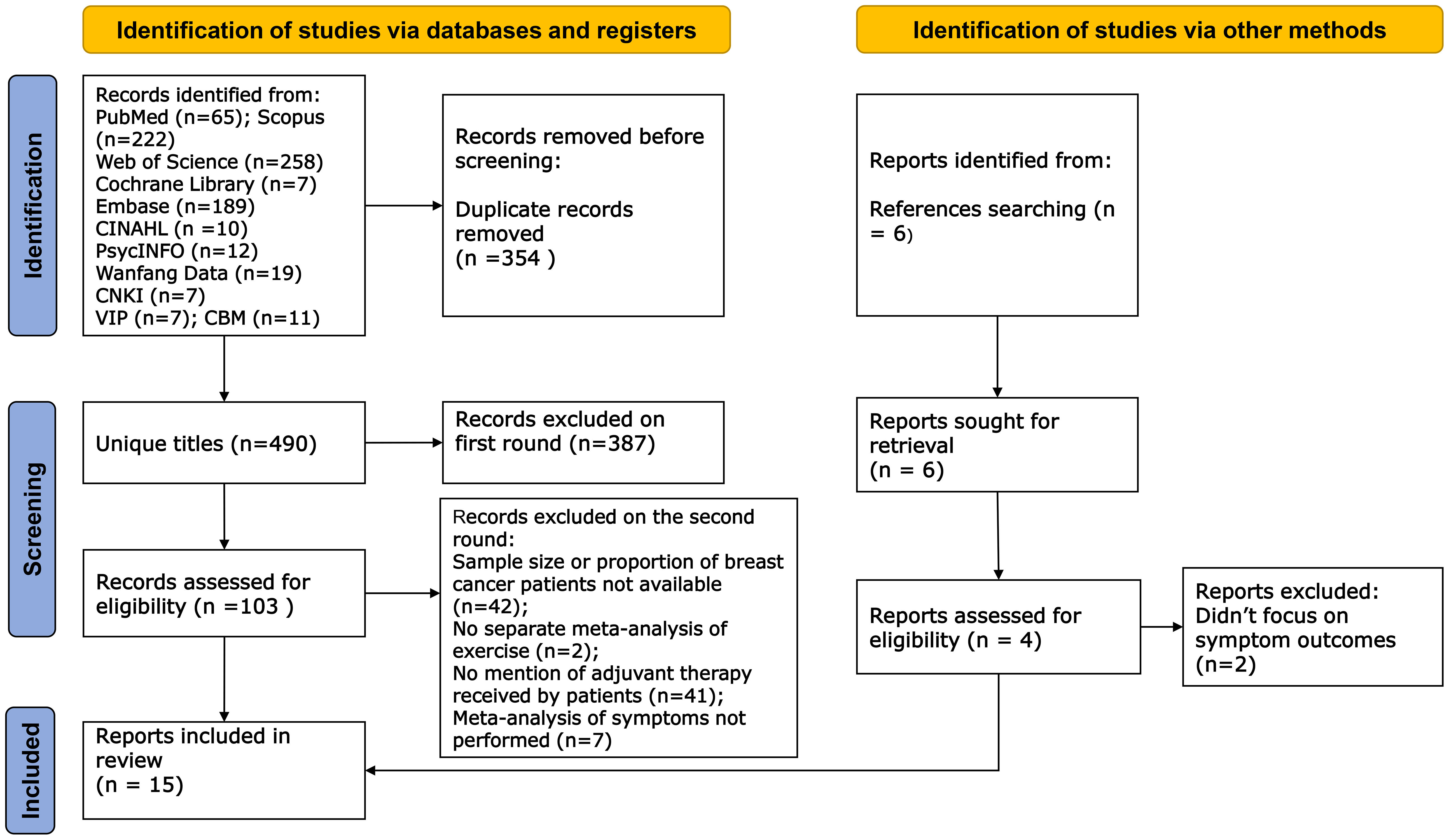
Figure 1 PRISMA diagram.
We summarized the main characteristics of the 15 included reviews in Tables 2, 3. The 15 included reviews were conducted by Chinese (21, 41, 46, 48, 49) (n=5), German (40, 42)(n=2), Dutch (38) (n=1), American (45) (n=1), Brazil (51) (n=1), Australian (47) (n=1), Spanish (50) (n=1), Colombia (39) (n=1), Ireland (44) (n=1), and Greek (43) (n=1). The sample size included in meta-analyses varied with a wide range of 400 to 2964. The number of primary studies included in each systematic review ranged from 5 to 32. The included reviews were published in 2015 or later. All primary studies in eligible meta-analyses conducted randomized controlled trials, and the majority of them assessed the outcomes of the symptoms using self-reporting questionnaires. While publishing bias and reporting bias were rarely presented in studies.
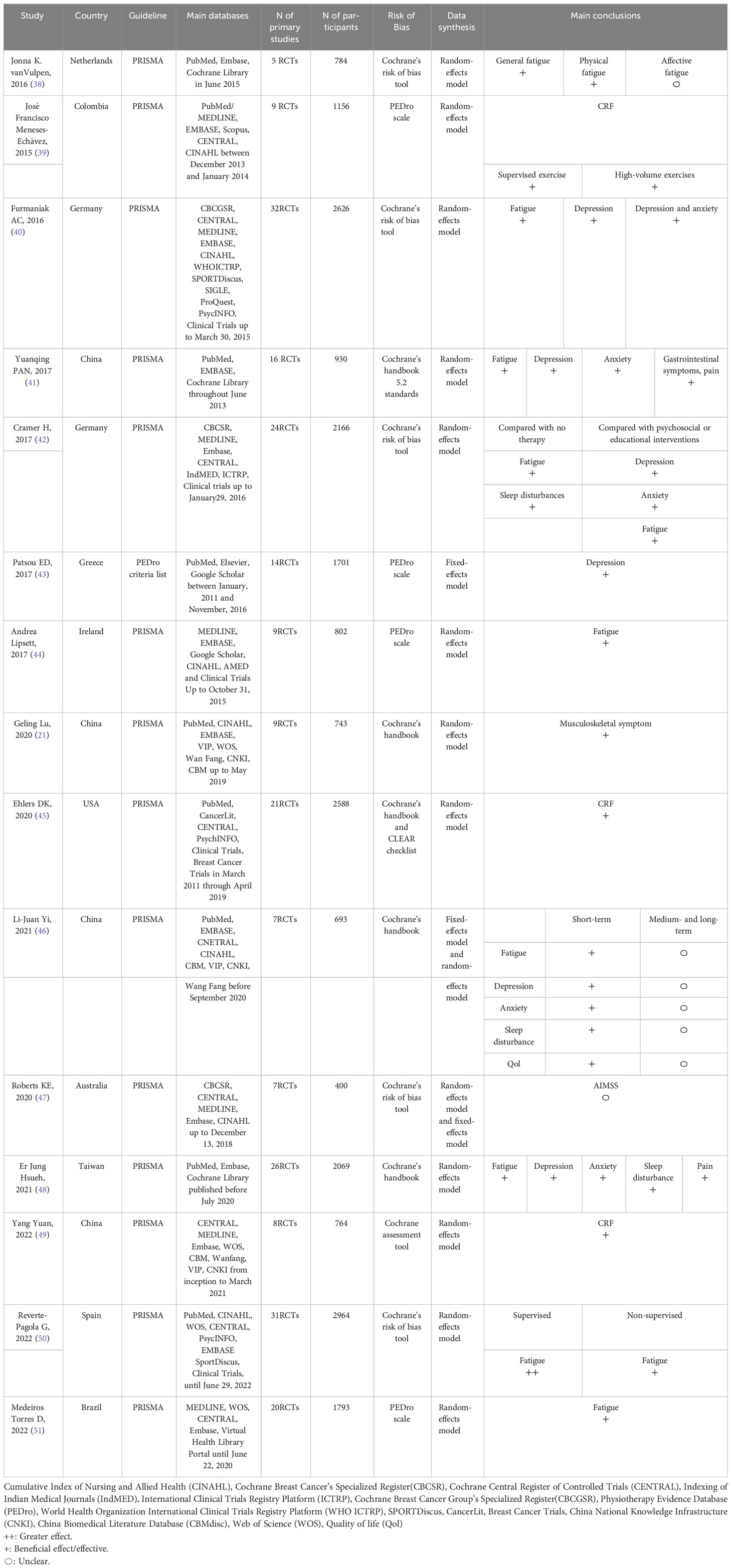
Table 2 Characteristics of the reviews.
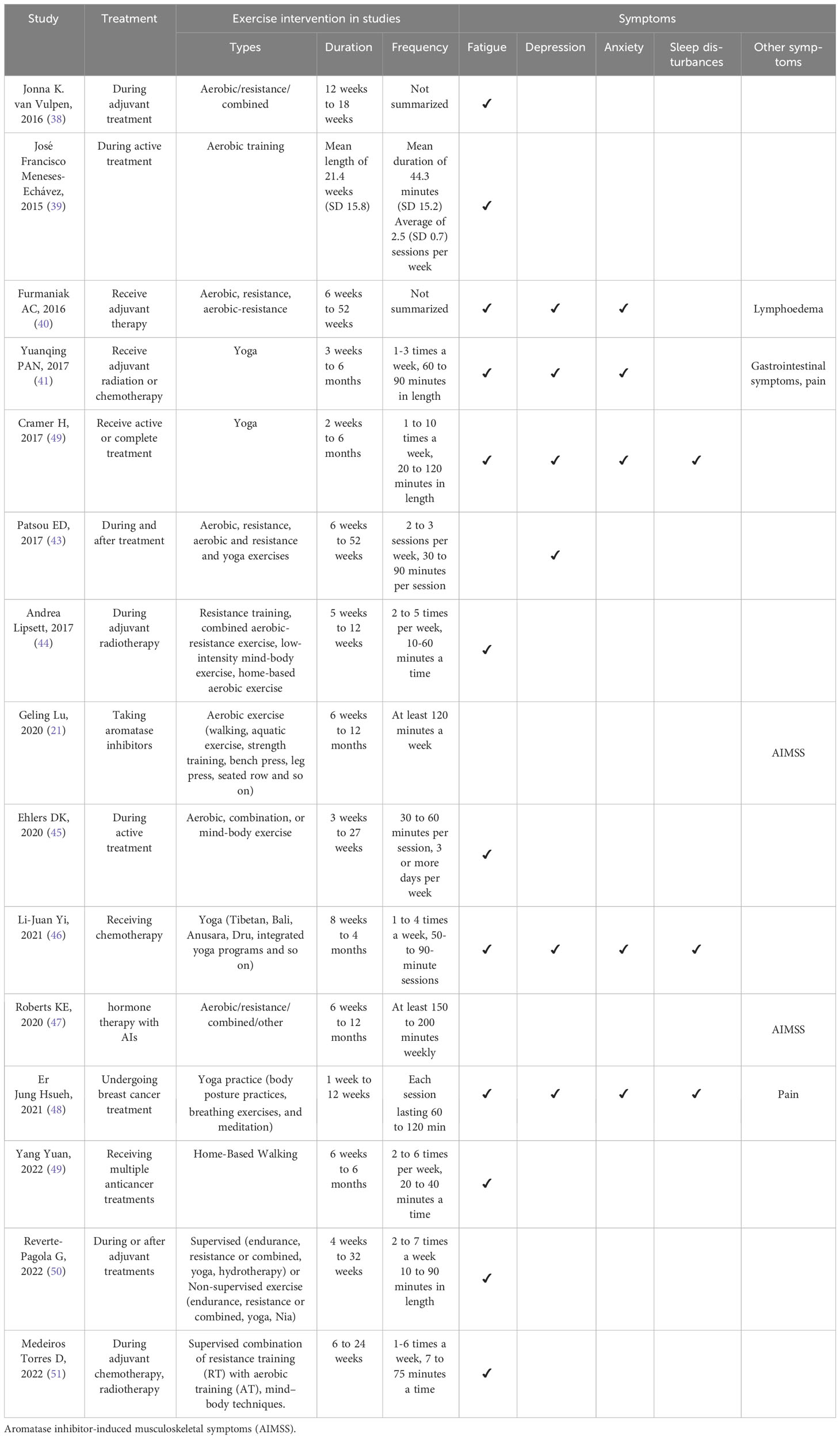
Table 3 Characteristics of the exercise.
Among 15 systematic reviews, 9 involved multimodal exercise (21, 38, 40, 43–45, 47, 50, 51), which could be a combination of aerobic and resistance exercise (21, 38, 40, 43–45, 47, 51), or a combination of supervised and unsupervised exercise (50). Yoga was mentioned in 4 systematic reviews (41, 42, 46, 48). 1 systematic review concentrated on aerobic exercise (39), and 1 focused on home-based walking (49). The total duration of the exercise interventions was between 1 week to 52 weeks, with most of them lasting 3 weeks to 6 months. Short-term exercise is considered an exercise intervention within 6 months, 6~12 months belongs to the medium-term, and exercise beyond 12 months is long-term (46). Most original studies contained in the included reviews (38, 39, 41, 42, 44, 46, 48, 49, 51) had a follow-up time of 6 months, with insufficient evidence of medium- and long-term exercise. Most systematic reviews (11/15) described the exercise frequency by providing the number of times per week and the duration of each exercise (39, 41–46, 48–51), and some described the total duration of one week’s exercise (21, 47). 2 reviews didn’t generally summarize the exercise frequency (38, 40). In all included systematic reviews, the effects of exercise on a total of seven symptoms—fatigue, anxiety, depression, sleep disturbance, musculoskeletal symptoms, lymphedema, and gastrointestinal symptoms—were examined.
Please see Table 3 for details on the effect of exercise on various symptoms and exercise-related characteristics. The effectiveness of exercises on fatigue symptoms in breast cancer patients was estimated by 18 meta-analyses from 12 systematic reviews (38–42, 44–46, 48–51) that were included. The final CCA result of 12.1% shows a significant number of primary reports that overlap. During adjuvant treatment for breast cancer patients, one review (38) found that exercise helped reduce general fatigue, notably physical fatigue, but had no effect on affective fatigue. Another review (50) found that supervised exercise had a greater anti-fatigue effect than unsupervised exercise. In breast cancer patients receiving adjuvant therapy, several systematic reviews concluded that short-term exercise (within 6 months) was effective in reducing fatigue (38, 39, 41, 42, 44, 48, 49, 51), although the effects of medium- and long-term exercise on reducing fatigue were erratic (40, 45, 46, 50).
Seven meta-analyses in total, chosen from six systematic reviews (40–43, 46, 48), were used to determine the effect of exercise on depression. A high repetition rate is indicated by the CCA, which is 14.4%. After eliminating duplicates from five systematic reviews (40–42, 46, 48) with 43 primary studies, anxiety was analyzed and the CCA was extremely high (18.6%). The findings of the systematic reviews showed that short-term exercise had a positive effect on relieving depression and anxiety in breast cancer patients during adjuvant treatment. One systematic review (46) compared the effectiveness of short-term exercise with medium- to long-term exercise in reducing depression and anxiety, and found that there was relatively insufficient evidence for medium- to long-term exercise on both symptoms.
The effect of exercise on sleep disturbance symptoms in breast cancer patients was examined in six meta-analyses that were selected from three systematic reviews (40, 42, 46). 10% is the final CCA, which indicates a moderate duplicate rate. There are few research on the effects of exercise in reducing sleep disturbance in breast cancer patients receiving adjuvant therapy, and the medium- and long-term effects of exercise on sleep disturbance are unclear. Short-term exercise was recommended for reducing sleep disturbance during breast cancer adjuvant treatment according to the findings of all meta-analyses (42, 46, 48).
Two included reviews (21, 47) analyzed the effect of exercise in reducing musculoskeletal symptoms among women with breast cancer during the hormone therapy period (taking aromatase inhibitors). Three original studies were repeated in these two systematic reviews, leaving nine original studies. An inconsistent conclusion was reached by two systematic reviews. While one research found that exercise could successfully effectively relieve musculoskeletal symptoms and advised encouraging patients to exercise actively under medical supervision (21), another found no clear evidence of the effect of exercise (47). The HOPE study by Irwin et al (52). was the one contained in both of these two reviews. With the largest sample size among the primary studies (of 121 participants with breast cancer), the HOPE study reported a 29% improvement in pain symptoms assigned to exercise, compared to a 3% increase in those receiving usual care at 12 months.
Just one included meta-analysis (41) mentioned gastrointestinal symptoms such as nausea, vomiting, or loss of appetite, and the final aggregated estimation revealed a small effect with moderate heterogeneity (SMD= -0.39, 95%CI -0.54, -0.25, P= .00, I2 = 37.8%).
Between the primary studies included in each meta-analysis, there were differences in a number of factors, including sophisticated exercise programs, various types of adjuvant therapies and symptoms, and how symptom outcomes were quantified, etc. Therefore, there is significant heterogeneity among the included systematic reviews and meta-analyses.
All of the studies with an overall confidence rating of “high” come from the Cochrane Library (40, 42, 47), whereas 10 studies have “critically low” ratings (21, 38, 39, 41, 43–46, 48, 49), and 2 studies have “low” ratings (50, 51). The essential items 2, 4, and 7 don’t match the standards, which is the leading cause of the low score. We find that 12 out of 15 studies have either a list of omitted studies or an explanation for exclusions (21, 38, 39, 41, 43–46, 48–51). In comparison, 8 studies didn’t register with procedures (21, 38, 41, 43–46, 49), 5 didn’t supply a complete retrieval strategy (21, 43, 45, 46, 48), and 3 have only provided a partial one (38, 39, 41). When evaluating the included 15 pieces of literature, the answers to items 1, 3, 8, 9, 11, 13, and 14 are all “yes” at 100%. Table 4 contains the specifics of each evaluation item.
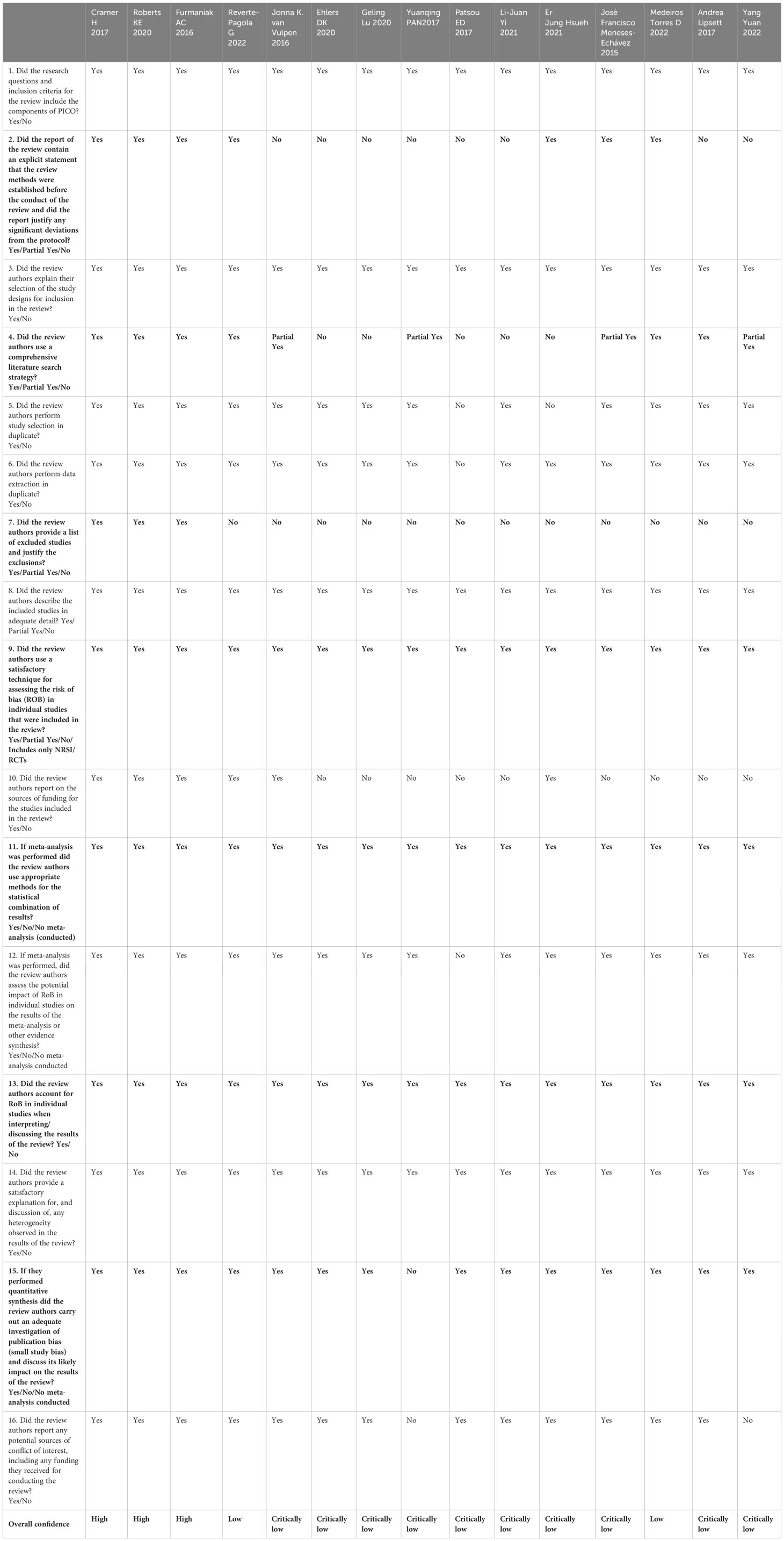
Table 4 The methodological quality of the included reviews according to the AMSTAR 2 tool.
To our knowledge, this is the first overview that thoroughly describes the role that exercise plays in symptom relief for breast cancer patients undergoing adjuvant treatment. Compared to previous umbrella reviews (53–55), which focused mainly on the benefits of exercise in reducing fatigue in cancer patients, we focused on breast cancer patients receiving adjuvant treatment and covered a wider range of symptoms. It is well known that during adjuvant treatment, the discomfort symptoms experienced by breast cancer patients typically appear in clusters, or “symptom clusters”, which refer to the simultaneous occurrence of at least two linked symptoms defined by Professor M. J. Dodd and other academics in 2001 (56). Symptoms are also interrelated and can be analyzed through symptom networks. Researchers presented the idea of “symptomics” by using symptom network analysis to study the particular link between symptoms (57), which further assisted in explaining the patterns of patient symptoms in the real world at the mechanistic level. It may contribute to increasing the efficiency of symptom management and performing targeted intervention with the novel perspective of assessing and analyzing the symptom cluster and symptom network of breast cancer patients during adjuvant treatment.
There were mixed effects of the exercise on fatigue according to the findings of our included systematic reviews. Short-term (within 6 months) exercise is effective in reducing general fatigue during adjuvant treatment in breast cancer patients, but the benefit of medium-term (6~12 months) or longer-term (more than 12 months) exercise is still unsure. Also, the effect of exercise on affective fatigue needs to be explored in more studies. Future studies should not only extend the duration of exercise interventions and follow-ups but also consider fatigue from a multidimensional perspective to precisely implement exercise interventions.
Our study’s comprehensive research revealed the alleviating effect of short-term exercise on anxiety and depression during adjuvant breast cancer treatment. Therefore, the medium- to long-term effects of exercise remain to be demonstrated. Furthermore, the relationship between mind and body may be taken into account, which may help to improve the effectiveness of exercise interventions. According to the relevant research, mindfulness yoga was an established mind-body exercise focused on mindfulness stress reduction (43). With good compliance in both groups (82.3% in the experimental group, 80.9% in the control group), a randomized controlled trial (58) found that mindfulness yoga was effective in reducing anxiety and depressive symptoms in breast cancer patients who had received adjuvant chemotherapy (anxiety inter-group effect 1.18, 95% CI: 0.2, 2.17; depression inter-group effect 1.49, 95% CI: 0.48, 2.5). Other mind-body exercises include Tai Chi and Qigong, both of which also have a lack of evidence in current studies for their effects in relieving anxiety or depression during adjuvant treatment of breast cancer. Based on this, future research could also explore whether mindfulness yoga, Tai Chi, or Qigong is more effective in improving symptoms during adjuvant breast cancer treatment compared to other exercises
Our final findings showed a positive effect of short-term exercise on sleep disturbance symptoms in three systematic reviews (40, 42, 46). The mechanism of correlation between symptoms uncovered by symptom clusters indicates that other unpleasant symptoms may contribute to or exacerbate sleep disturbances. One study in 2022 (59) put the symptoms (fatigue, sleep disturbance, and depression) as symptom clusters, which contained F-S-D (fatigue-sleep disturbance-depression), F-S (fatigue-sleep disturbance), F-D (fatigue-depression), and S-D (sleep disturbance-depression) symptom clusters. This study proposed a wide range of interventions that could alleviate all these four symptom clusters (F-S-D, F-S, F-D, S-D), further suggesting that symptom clusters may provide valuable clues for developing symptom management strategies, such as targeting an identified bridge symptom within or between core symptom clusters to improve the efficiency of the intervention.
In particular, aromatase inhibitors (AIs), which are linked to joint and muscular symptoms and are referred to as aromatase inhibitor-associated musculoskeletal symptoms (AIMSS) (60), are frequently used to treat hormone-positive (HR+) breast cancer in women. AIMSS are often an underdiagnosed and underestimated complication of such treatments. Data have shown that AIMSS can occur in up to 40% of HR+ breast cancer survivors receiving AI treatment (61), and that dropout rates for AIs due to the side effects can reach 20% during the first year of treatment (62–64). Bone health is always a challenge (12). The processes underlying AIMSS are still poorly understood, but they may be linked to extreme estrogen depletion (65). Previous studies have demonstrated the advantages of exercise in improving AIMSS in breast cancer patients by presenting pathological and physiological explanations: Exercise raises bone density (66), improves bodily fluid circulation to tissues (67), and may increase the pain threshold (68). However, our findings indicate that the empirical study of the effect of exercise on AIMSS is still limited and that the inconsistent results of the included studies call for larger sample sizes and longer follow-up periods.
Other symptoms, such as lymphedema and gastrointestinal symptoms, are also symptoms that may occur or be present during adjuvant therapy in breast cancer patients. However, there is a limited number of studies on exercise during adjuvant therapy to improve these symptoms. In the case of lymphedema, the role of exercise on lymphedema has not reached a consistent conclusion in research. In addition to this, most studies (69, 70) have focused only on whether exercise increases the risk of developing lymphedema in breast cancer patients but not on the effect of exercise on relieving lymphedema during breast cancer adjuvant therapy. Our study focused on the latter and there may be some bias. The risk of lymphedema varies among breast cancer patients receiving different treatments, and in order to develop a more precise Exercise Plan, future studies should analyze the main causes of lymphedema based on the clinical context of breast cancer patients receiving treatment and follow up the effect of exercise during adjuvant therapy on lymphedema for a longer time. In patients with breast cancer receiving adjuvant therapy, particularly during chemotherapy, gastrointestinal symptoms (GIs) are frequent. The included systematic review’s findings (41) revealed that exercise had small effects on GIs, but the evidence is still insufficient and needs to be supplemented by more studies. GI symptoms like nausea, vomiting, and bloating are prevalent in symptom clusters, but those clusters often are inconsistent (71). A lack of appetite and malnutrition may result from these symptoms. In addition to necessary nutritional intervention which was the only focus in existing studies (72, 73), future studies might look into the potential effectiveness of combining exercise and dietary interventions in mitigating gastrointestinal symptoms.
In conclusion, during adjuvant treatment for breast cancer patients, as multiple symptoms always occur simultaneously, we should concentrate on the idea of symptom clusters and explore precise exercise interventions for bridging symptoms within or between symptom clusters. Besides, symptom networks are an extension and deepening of symptom clusters and can identify mechanisms of complex symptom interactions as well as potential targets for intervention in the real world. These two topics might be the subject of future research to boost symptom management efficiency.
Overall, the quality of the included studies needs to be improved. The systematic review should strictly follow the PRISMA process and reporting standards, which can be found in EQUATOR online. According to the results of our quality assessment, the following three areas need the most improvement: The systematic review should be preceded by a study protocol and registration, followed by a thorough database search and the provision of search strategies for each database. Lastly, provide a list of excluded studies and justify the exclusions.
This article has the following limitations. Firstly, although the retrieval approach is not restricted to English or Chinese, we did include meta-analyses that were only published in these two languages, which might have a language bias. Secondly, non-peer-reviewed literature, systematic reviews without meta-analyses were excluded, as were reviews with less than 3 primary studies or 100 participants, all of which could have resulted in reporting bias. Thirdly, we did not perform subgroup analyses of different types of exercise or symptoms, only presented the results descriptively. The final concern is that the inclusion criteria for our literature were severely restricted, which may also result in some bias.
Several symptoms brought on by adjuvant treatment for breast cancer can be alleviated with exercise, but this benefit needs to be further demonstrated. First, future studies must increase the sample size. Second, although a growing number of recent studies have explored changes in symptom clusters or symptom networks over time during breast cancer adjuvant treatment, their clinical practice is inadequate. The complexity of the symptoms is one potential cause. To solve this problem, future research may use ecological transient assessment to dynamically assess symptoms. Thirdly, we found that there is still a lack of research on the effects of exercise on relieving symptom clusters or symptom networks during adjuvant therapy in breast cancer patients. We expect that further research will be conducted to examine the effects of exercise on improving bridge symptoms identified within or between symptom clusters and, in addition, advance the development of symptomics using symptom network analysis. This will improve the efficiency of symptom management and better meet the specific needs of more patients with breast cancer.
The findings of this study offer some suggestions for further research by shedding light on the contribution of exercises to several symptoms in breast cancer patients receiving adjuvant treatment. Future studies might examine the effect of exercise on relieving bridge symptoms found within or between core symptom clusters during breast cancer adjuvant treatment. Alternatively, we may promote the application of symptom network analysis and make use of ecological instantaneous assessment to track changes in symptom networks dynamically.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
The research presented in this article is part of the following research projects: 1. Project source: Zhejiang medical and Health Science and Technology program, Project Name: A social network study of Health information speaking and communication behavior in patients with coronary heart disease, Project number: 2022KY838, Project registration number: ChiCTR230069238, Ethical Approval No.: Sir Run Shaw Ethics Review 2022, No. 0062; 2. Project source: Zhejiang medical and Health Science and Technology program, Project Name: The behavior regulation and influencing factors of internet health information seeking in patients with chronic diseases, Project number: 2021RC011, Project registration number: ChiCTR220066038, Ethical approval number: Sir Run Shaw Ethics Review 20210504, No. 0035.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1222947/full#supplementary-material
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin (2016) 66(2):115–32. doi: 10.3322/caac.21338
3. Firkins J, Hansen L, Driessnack M, Dieckmann N. Quality of life in “chronic” cancer survivors: a meta-analysis. J Cancer Surviv Res Pract (2020) 14(4):504–17. doi: 10.1007/s11764-020-00869-9
4. The American Cancer Society. (Breast Cancer Facts & Figures 2022-2024 and ancer Facts & Figures 2023) . Available at: https://www.bcrf.org/breast-cancer-statistics-and-resources/.
5. Andrijauskaite K, Wargovich MJ. Role of natural products in breast cancer related symptomology: Targeting chronic inflammation. Semin Cancer Biol (2022) 80:370–8. doi: 10.1016/j.semcancer.2020.08.011
6. Di Nardo P, Lisanti C, Garutti M, Buriolla S, Alberti M, Mazzeo R, et al. Chemotherapy in patients with early breast cancer: clinical overview and management of long-term side effects. Expert Opin Drug Saf (2022) 21(11):1341–55. doi: 10.1080/14740338.2022.2151584
7. Silva da Costa N, Alves da Silva AS, de Melo-Neto JS. Effects of dance therapy in women with breast cancer: A systematic review protocol. Neto MG Ed PloS One (2022) 17(6):e0257948. doi: 10.1371/journal.pone.0257948
8. Hsu HT, Lin KC, Wu LM, Juan CH, Hou MF, Hwang SL, et al. Symptom cluster trajectories during chemotherapy in breast cancer outpatients. J Pain Symptom Manage (2017) 53(6):1017–25. doi: 10.1016/j.jpainsymman.2016.12.354
9. Peddie N, Agnew S, Crawford M, Dixon D, MacPherson I, Fleming L. The impact of medication side effects on adherence and persistence to hormone therapy in breast cancer survivors: A qualitative systematic review and thematic synthesis. Breast Edinb Scotl (2021) 58:147–59. doi: 10.1016/j.breast.2021.05.005
10. Taylor CW, Kirby AM. Cardiac side-effects from breast cancer radiotherapy. Clin Oncol R Coll Radiol G B (2015) 27(11):621–9. doi: 10.1016/j.clon.2015.06.007
11. Ezzo J, Manheimer E, McNeely ML, Howell DM, Weiss R, Johansson KI, et al. Manual lymphatic drainage for lymphedema following breast cancer treatment. Cochrane Database Syst Rev (2015) 5):CD003475. doi: 10.1002/14651858.CD003475.pub2
12. De La Torre-Montero JC, Casla-Barrio S, Herrero-López B, García-Saénz JÁ. Editorial: Exercise, physical therapy, and wellbeing in breast cancer patients. Front Oncol (2023) 13:1118718. doi: 10.3389/fonc.2023.1118718
13. Watson G, Coyne Z, Houlihan E, Leonard G. Exercise oncology: an emerging discipline in the cancer care continuum. Postgrad Med (2022) 134(1):26–36. doi: 10.1080/00325481.2021.2009683
14. Stout NL, Brown JC, Schwartz AL, Marshall TF, Campbell AM, Nekhlyudov L, et al. An exercise oncology clinical pathway: Screening and referral for personalized interventions. Cancer (2020) 126(12):2750–8. doi: 10.1002/cncr.32860
15. Reis AD, Pereira PTVT, Diniz RR, de Castro Filha JGL, Dos Santos AM, Ramallo BT, et al. Randomized exercise trial of aromatase inhibitor-induced arthralgia in breast cancer survivors. Health Qual Life Outcomes (2018) 16(1):58. doi: 10.1186/s12955-018-0882-2
16. Dieli-Conwright CM, Courneya KS, Demark-Wahnefried W, Sami N, Lee K, Sweeney FC, et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: a randomized controlled trial. Breast Cancer Res BCR. (2018) 20(1):124. doi: 10.1186/s13058-018-1051-6
17. van Waart H, Stuiver MM, van Harten WH, Geleijn E, Kieffer JM, Buffart LM, et al. Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: results of the PACES randomized clinical trial. J Clin Oncol Off J Am Soc Clin Oncol (2015) 33(17):1918–27. doi: 10.1200/JCO.2014.59.1081
18. Courneya KS, Segal RJ, Mckenzie DC, Dong H, Gelmon K, Friedenreich CM, et al. Effects of exercise during adjuvant chemotherapy on breast cancer outcomes. Med Sci SPORTS Exerc (2014) 46(9):1744–51. doi: 10.1249/MSS.0000000000000297
19. Franzoi MA, Agostinetto E, Perachino M, Del Mastro L, de Azambuja E, Vaz-Luis I, et al. Evidence-based approaches for the management of side-effects of adjuvant endocrine therapy in patients with breast cancer. Lancet Oncol (2021) 22(7):e303–13. doi: 10.1016/S1470-2045(20)30666-5
20. Mehnert A, Veers S, Howaldt D, Braumann KM, Koch U, Schulz KH. Effects of a physical exercise rehabilitation group program on anxiety, depression, body image, and health-related quality of life among breast cancer patients. Onkologie (2011) 34(5):248–53. doi: 10.1159/000327813
21. Lu G, Zheng J, Zhang L. The effect of exercise on aromatase inhibitor-induced musculoskeletal symptoms in breast cancer survivors :a systematic review and meta-analysis. Support Care Cancer (2020) 28(4):1587–96. doi: 10.1007/s00520-019-05186-1
22. Wang L, Shi YX, Wang TT, Chen KX, Shang SM. Breast cancer-related lymphoedema and resistance exercise: An evidence-based review of guidelines, consensus statements and systematic reviews. J Clin Nurs (2023) 32(9-10):2208–27. doi: 10.1111/jocn.16437
23. Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, et al. American college of sports medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc (2010) 42(7):1409–26. doi: 10.1249/MSS.0b013e3181e0c112
24. Dieli-Conwright CM, Courneya KS, Demark-Wahnefried W, Sami N, Lee K, Buchanan TA, et al. Effects of aerobic and resistance exercise on metabolic syndrome, sarcopenic obesity, and circulating biomarkers in overweight or obese survivors of breast cancer: A randomized controlled trial. J Clin Oncol (2018) 36(9):875–83. doi: 10.1200/JCO.2017.75.7526
25. Lee K, Tripathy D, Demark-Wahnefried W, Courneya KS, Sami N, Bernstein L, et al. Effect of aerobic and resistance exercise intervention on cardiovascular disease risk in women with early-stage breast cancer: A randomized clinical trial. JAMA Oncol (2019) 5(5):710. doi: 10.1001/jamaoncol.2019.0038
26. Courneya KS, McKenzie DC, Mackey JR, Gelmon K, Friedenreich CM, Yasui Y, et al. Effects of exercise dose and type during breast cancer chemotherapy: multicenter randomized trial. J Natl Cancer Inst (2013) 105(23):1821–32. doi: 10.1093/jnci/djt297
27. De Sire A, Lippi L, Ammendolia A, Cisari C, Venetis K, Sajjadi E, et al. Physical exercise with or without whole-body vibration in breast cancer patients suffering from aromatase inhibitor—Induced musculoskeletal symptoms: A pilot randomized clinical study. J Pers Med (2021) 11(12):1369. doi: 10.3390/jpm11121369
28. An K, Morielli AR, Kang D, Friedenreich CM, McKenzie DC, Gelmon K, et al. Effects of exercise dose and type during breast cancer chemotherapy on longer-term patient-reported outcomes and health-related fitness: A randomized controlled trial. Int J Cancer (2020) 146(1):150–60. doi: 10.1002/ijc.32493
29. Juvet LK, Thune I, Elvsaas IKØ, Fors EA, Lundgren S, Bertheussen G, et al. The effect of exercise on fatigue and physical functioning in breast cancer patients during and after treatment and at 6 months follow-up: A meta-analysis. Breast Edinb Scotl (2017) 33:166–77. doi: 10.1016/j.breast.2017.04.003
30. Browall M, Mijwel S, Rundqvist H, Wengström Y. Physical activity during and after adjuvant treatment for breast cancer: an integrative review of women’s experiences. Integr Cancer Ther (2018) 17(1):16–30. doi: 10.1177/1534735416683807
31. Foucaut AM, Berthouze SE, Touillaud M, Morelle M, Bourne-Branchu V, Kempf-Lépine AS, et al. Deterioration of physical activity level and metabolic risk factors after early-stage breast cancer diagnosis. Cancer Nurs (2015) 38(4):E1–9. doi: 10.1097/NCC.0000000000000187
32. Ginzac A, Bernadach M, Molnar I, Duclos M, Thivat E, Durando X. Adapted physical activity for breast cancer patients treated with neoadjuvant chemotherapy and trastuzumab against HER2 (APACAN2): A protocol for a feasibility study. Front Oncol (2021) 11:744609. doi: 10.3389/fonc.2021.744609
33. Nyrop K, Callahan L, Cleveland R, Arbeeva L, Hackney B, Muss H. Randomized controlled trial of a home-based walking program to reduce moderate to severe aromatase inhibitor-associated arthralgia in breast cancer survivors. Oncologist (2017) 22(10):1238–49. doi: 10.1634/theoncologist.2017-0174
34. Huang H, Wen F, Yang T, Lin Y, Tsai J, Shun S, et al. The effect of a 12-week home-based walking program on reducing fatigue in women with breast cancer undergoing chemotherapy: a randomized controlled study. Int J Nurs Stud (2019) 99:103376. doi: 10.1016/j.ijnurstu.2019.06.007
35. Gu J, Hu M, Chen Y, Yu J, Ji Y, Wei G, et al. Bibliometric analysis of global research on physical activity and sedentary behavior in the context of cancer. Front Oncol (2023) 13:1095852. doi: 10.3389/fonc.2023.1095852
36. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (2017) 358:j4008. doi: 10.1136/bmj.j4008
37. Hennessy EA, Johnson BT. Examining overlap of included studies in meta-reviews: Guidance for using the corrected covered area index. Res Synth Methods (2020) 11(1):134–45. doi: 10.1002/jrsm.1390
38. van Vulpen JK, Peeters PHM, Velthuis MJ, van der Wall E, May AM. Effects of physical exercise during adjuvant breast cancer treatment on physical and psychosocial dimensions of cancer-related fatigue: A meta-analysis. Maturitas (2016) 85:104–11. doi: 10.1016/j.maturitas.2015.12.007
39. Meneses-Echávez JF, González-Jiménez E, Ramírez-Vélez R. Effects of supervised exercise on cancer-related fatigue in breast cancer survivors: a systematic review and meta-analysis. BMC Cancer (2015) 15(1):77. doi: 10.1186/s12885-015-1069-4
40. Furmaniak AC, Menig M, Markes MH. Exercise for women receiving adjuvant therapy for breast cancer. Cochrane Breast Cancer Group, ed. Cochrane Database Syst Rev (2016) 2016(9). doi: 10.1002/14651858.CD005001.pub3
41. Pan Y, Yang K, Wang Y, Zhang L, Liang H. Could yoga practice improve treatment-related side effects and quality of life for women with breast cancer? A systematic review and meta-analysis: Benefits of yoga for breast cancer. Asia Pac J Clin Oncol (2017) 13(2):e79–95. doi: 10.1111/ajco.12329
42. Cramer H, Lauche R, Klose P, Lange S, Langhorst J, Dobos GJ. Yoga for improving health-related quality of life, mental health and cancer-related symptoms in women diagnosed with breast cancer. Cochrane Breast Cancer Group, ed. Cochrane Database Syst Rev (2017) 2017(1). doi: 10.1002/14651858.CD010802.pub2
43. Patsou ED, Alexias GD, Anagnostopoulos FG, Karamouzis MV. Effects of physical activity on depressive symptoms during breast cancer survivorship: a meta-analysis of randomised control trials. ESMO Open (2017) 2(5):e000271. doi: 10.1136/esmoopen-2017-000271
44. Lipsett A, Barrett S, Haruna F, Mustian K, O’Donovan A. The impact of exercise during adjuvant radiotherapy for breast cancer on fatigue and quality of life: A systematic review and meta-analysis. Breast Edinb Scotl (2017) 32:144–55. doi: 10.1016/j.breast.2017.02.002
45. Ehlers DK, DuBois K, Salerno EA. The effects of exercise on cancer-related fatigue in breast cancer patients during primary treatment: a meta-analysis and systematic review. Expert Rev Anticancer Ther (2020) 20(10):865–77. doi: 10.1080/14737140.2020.1813028
46. Yi LJ, Tian X, Jin YF, Luo MJ, Jiménez-Herrera MF. Effects of yoga on health-related quality, physical health and psychological health in women with breast cancer receiving chemotherapy: a systematic review and meta-analysis. Ann Palliat Med (2021) 10(2):1961–75. doi: 10.21037/apm-20-1484
47. Roberts KE, Rickett K, Feng S, Vagenas D, Woodward NE. Exercise therapies for preventing or treating aromatase inhibitor-induced musculoskeletal symptoms in early breast cancer. In: Cochrane Database Syst Rev. Cochrane Breast Cancer Group (2020). doi: 10.1002/14651858.CD012988.pub2
48. Hsueh EJ, Loh EW, Lin JJA, Tam KW. Effects of yoga on improving quality of life in patients with breast cancer: a meta-analysis of randomized controlled trials. Breast Cancer (2021) 28(2):264–76. doi: 10.1007/s12282-020-01209-6
49. Yuan Y, Lin L, Zhang N, Xie C, Liang J, Qi Y, et al. Effects of home-based walking on cancer-related fatigue in patients with breast cancer: A meta-analysis of randomized controlled trials. Arch Phys Med Rehabil (2022) 103(2):342–52. doi: 10.1016/j.apmr.2021.06.020
50. Reverte-Pagola G, Sánchez-Trigo H, Saxton J, Sañudo B. Supervised and non-supervised exercise programs for the management of cancer-related fatigue in women with breast cancer: A systematic review and meta-analysis. Cancers (2022) 14(14):3428. doi: 10.3390/cancers14143428
51. Medeiros Torres D, Jorge Koifman R, da Silva Santos S. Impact on fatigue of different types of physical exercise during adjuvant chemotherapy and radiotherapy in breast cancer: systematic review and meta-analysis. Support Care Cancer (2022) 30(6):4651–62. doi: 10.1007/s00520-022-06809-w
52. Irwin ML, Cartmel B, Gross CP, Ercolano E, Li F, Yao X, et al. Randomized exercise trial of aromatase inhibitor-induced arthralgia in breast cancer survivors. J Clin Oncol Off J Am Soc Clin Oncol (2015) 33(10):1104–11. doi: 10.1200/JCO.2014.57.1547
53. Jiang M, Ma Y, Yun B, Wang Q, Huang C, Han L. Exercise for fatigue in breast cancer patients: An umbrella review of systematic reviews. Int J Nurs Sci (2020) 7(2):248–54. doi: 10.1016/j.ijnss.2020.03.001
54. Zhou HJ, Wang T, Xu YZ, Chen YN, Deng LJ, Wang C, et al. Effects of exercise interventions on cancer-related fatigue in breast cancer patients: an overview of systematic reviews. Support Care Cancer Off J Multinatl Assoc Support Care Cancer (2022) 30(12):10421–40. doi: 10.1007/s00520-022-07389-5
55. Zhang YB, Zhong XM, Han N, Tang H, Wang SY, Lin WX. Effectiveness of exercise interventions in the management of cancer-related fatigue: a systematic review of systematic reviews. Support Care Cancer Off J Multinatl Assoc Support Care Cancer (2023) 31(3):153. doi: 10.1007/s00520-023-07619-4
56. Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status of patients with cancer. Oncol Nurs Forum (2001) 28(3):465–70.
57. Fried EI, Boschloo L, van Borkulo CD, Schoevers RA, Romeijn JW, Wichers M, et al. Commentary: “Consistent superiority of selective serotonin reuptake inhibitors over placebo in reducing depressed mood in patients with major depression”. Front Psychiatry (2015) 6:117. doi: 10.3389/fpsyt.2015.00117
58. Liu W, Liu J, Ma L, Chen J. Effect of mindfulness yoga on anxiety and depression in early breast cancer patients received adjuvant chemotherapy: a randomized clinical trial. J Cancer Res Clin Oncol (2022) 148(9):2549–60. doi: 10.1007/s00432-022-04167-y
59. Wong WM, Chan DNS, He X, So WKW. Effectiveness of pharmacological and nonpharmacological interventions for managing the fatigue–sleep disturbance–depression symptom cluster in breast cancer patients undergoing chemotherapy: A systematic review. Cancer Nurs (2022). doi: 10.1097/NCC.0000000000001048
60. Lintermans A, Laenen A, Van Calster B, Van Hoydonck M, Pans S, Verhaeghe J, et al. Prospective study to assess fluid accumulation and tenosynovial changes in the aromatase inhibitor-induced musculoskeletal syndrome: 2-year follow-up data. Ann Oncol Off J Eur Soc Med Oncol (2013) 24(2):350–5. doi: 10.1093/annonc/mds290
61. Crew KD, Greenlee H, Capodice J, Raptis G, Brafman L, Fuentes D, et al. Prevalence of joint symptoms in postmenopausal women taking aromatase inhibitors for early-stage breast cancer. J Clin Oncol Off J Am Soc Clin Oncol (2007) 25(25):3877–83. doi: 10.1200/JCO.2007.10.7573
62. Sestak I, Cuzick J, Sapunar F, Eastell R, Forbes JF, Bianco AR, et al. Risk factors for joint symptoms in patients enrolled in the ATAC trial: a retrospective, exploratory analysis. Lancet Oncol (2008) 9(9):866–72. doi: 10.1016/S1470-2045(08)70182-7
63. Murphy CC, Bartholomew LK, Carpentier MY, Bluethmann SM, Vernon SW. Adherence to adjuvant hormonal therapy among breast cancer survivors in clinical practice: a systematic review. Breast Cancer Res Treat (2012) 134(2):459–78. doi: 10.1007/s10549-012-2114-5
64. Migliaccio S, de Sire A, Marocco C, Fornari R, Paoletta M, Greco EA, et al. Approach in aromatase inhibitors - induced osteoporosis: results from an Italian multicenter observational study. Clin cases Miner Bone Metab (2018) 15(3):334–9.
65. Scaturro D, de Sire A, Terrana P, Curci C, Vitagliani F, Falco V, et al. Early Denosumab for the prevention of osteoporotic fractures in breast cancer women undergoing aromatase inhibitors: A case-control retrospective study. J Back Musculoskelet Rehabil (2022) 35(1):207–12. doi: 10.3233/BMR-210012
66. Troy KL, Mancuso ME, Butler TA, Johnson JE. Exercise early and often: effects of physical activity and exercise on women’s bone health. Int J Environ Res Public Health (2018) 15(5). doi: 10.3390/ijerph15050878
67. Church TS, Earnest CP, Skinner JS, Blair SN. Effects of different doses of physical activity on cardiorespiratory fitness among sedentary, overweight or obese postmenopausal women with elevated blood pressure: a randomized controlled trial. JAMA (2007) 297(19):2081–91. doi: 10.1001/jama.297.19.2081
68. Hyder T, Marino CC, Ahmad S, Nasrazadani A, Brufsky AM. Aromatase inhibitor-associated musculoskeletal syndrome: understanding mechanisms and management. Front Endocrinol (2021) 12:713700. doi: 10.3389/fendo.2021.713700
69. Kwan ML, Cohn JC, Armer JM, Stewart BR, Cormier JN. Exercise in patients with lymphedema: a systematic review of the contemporary literature. J Cancer Surviv (2011) 5(4):320–36. doi: 10.1007/s11764-011-0203-9
70. Hasenoehrl T, Keilani M, Palma S, Crevenna R. Resistance exercise and breast cancer related lymphedema – a systematic review update. Disabil Rehabil (2020) 42(1):26–35. doi: 10.1080/09638288.2018.1514663
71. So WKW, Law BMH, Ng MSN, He X, Chan DNS, Chan CWH, et al. Symptom clusters experienced by breast cancer patients at various treatment stages: A systematic review. Cancer Med (2021) 10(8):2531–65. doi: 10.1002/cam4.3794
72. de, Souza APS, da Silva LC, Fayh APT. Nutritional intervention contributes to the improvement of symptoms related to quality of life in breast cancer patients undergoing neoadjuvant chemotherapy: A randomized clinical trial. Nutrients (2021) 13(2). doi: 10.3390/nu13020589
73. Grupińska J, Budzyń M, Maćkowiak K, Brzeziński JJ, Kycler W, Leporowska E, et al. Beneficial effects of oral nutritional supplements on body composition and biochemical parameters in women with breast cancer undergoing postoperative chemotherapy: A propensity score matching analysis. Nutrients (2021) 13(10). doi: 10.3390/nu13103549
Keywords: exercise, breast cancer, adjuvant treatment, symptom, umbrella review
Citation: Zhao Y, Tang L, Shao J, Chen D, Jiang Y, Tang P and Wang X (2023) The effectiveness of exercise on the symptoms in breast cancer patients undergoing adjuvant treatment: an umbrella review of systematic reviews and meta-analyses. Front. Oncol. 13:1222947. doi: 10.3389/fonc.2023.1222947
Received: 15 May 2023; Accepted: 28 August 2023;
Published: 20 September 2023.
Edited by:
Cassiano Merussi Neiva, São Paulo State University, BrazilReviewed by:
Marco Invernizzi, University of Eastern Piedmont, ItalyCopyright © 2023 Zhao, Tang, Shao, Chen, Jiang, Tang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leiwen Tang, dGFuZ2x3QHpqdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.