 Liliana Aguiar De Azevedo1Charles Orione2Cécile Tromeur1Francis Couturaud1Renaud Descourt3
Liliana Aguiar De Azevedo1Charles Orione2Cécile Tromeur1Francis Couturaud1Renaud Descourt3 Margaux Geier3*
Margaux Geier3*- 1Service de Pneumologie, Centre Hospitalier Regional Universitaire de Brest, Brest, Brittany, France
- 2Service de Pneumologie, Centre Hospitalier de Cornouaille, Quimper, France
- 3Service d’oncologie médicale, Centre Hospitalier Regional Universitaire de Brest, Brest, Brittany, France
Background: Venous thromboembolism (VTE) is a serious complication in non-small cell lung cancer (NSCLC) patients. The use of thromboprophylactic therapy is subject to an accurate assessment of the VTE risk depending on patients, tumor characteristics and type of systemic antineoplastic treatments. However, little is known concerning the risk of VTE in patients suffering from an advanced NSCLC treated with first-line chemo-immunotherapy and the impact of tumor biomarkers such as PD-L1 expression.
Methods: We performed a retrospective, observational, single-centre study in a cohort of advanced NSCLC patients treated with first-line chemo-immunotherapy. The primary endpoint was the incidence of VTE. Secondary endpoints were the cumulative incidence of VTE, the impact of PD-L1 on VTE occurrence, overall survival, the rate of VTE recurrence under anticoagulant treatment and the rate of bleeding complications.
Results: 109 patients were included, of whom 21 (19.3%) presented a VTE event during a median follow-up of 13 months. VTE incidence at 3, 6 and 12 months was 12.1%, 15.1% and 17.5% respectively. 61% were pulmonary embolisms, 9.5% were isolated deep vein thrombosis and 14.3% were central venous catheter-related thrombosis. Our study did not show a significant impact of PD-L1 on VTE occurrence. Overall survival at 6, 12 and 24 months was 81.9%, 74.4% and 70.3% respectively. Four patients developed a recurrent VTE under anticoagulation therapy 3 to 5 months after the first VTE event. One patient suffered from a major bleeding complication while under anticoagulation therapy, leading to death.
Conclusion: VTE is a common complication in advanced NSCLC patients treated with concomitant chemo-immunotherapy. In our study, 19.3% of patients developed a VTE during a median follow-up of 13 months. PD-L1 did not appear to be associated with VTE occurrence. We recorded high VTE recurrence rates despite anticoagulant treatment. Further investigations are needed to determine if high PD-L1 expression is associated with VTE.
1 Introduction
Cancer is one of the major known risk factors of venous thromboembolism (VTE) (1, 2) and one of the main causes of mortality in patients developing VTE (3). On the other hand, VTE is correlated with a lower survival and represents the second leading cause of death in cancer patients (4). Moreover, VTE recurrences are more frequent in cancer patients than in general population (5–7) and have higher mortality rates, especially in lung cancer patients (8).
Cancer-associated VTE risk varies according to cancer type, the presence of metastases or disease progression, but also the use of systemic treatments such as chemotherapy (9). VTE risk scores have been developed, such as the Khorana score (4), to help identify patients at high risk that might benefit from a thromboprophylactic treatment. According to current guidelines, direct oral anticoagulants (DOACs) can be used as an alternative to low-molecular weight heparin (LMWH) and must be preferred to vitamin K antagonists (VKAs) in treatment or prophylaxis of cancer-associated VTE (10, 11). Indeed, four randomized controlled trials have shown that DOACs are as efficient and as safe as LMWH in cancer-associated VTE (12–15). However, the high rates of bleeding complications in cancer patients under anticoagulation make it necessary to carefully assess the VTE risk factors and the indication for anticoagulant treatment in this population (7, 16).
Lung cancer is one of the most common cancers and is the leading cause of cancer-related mortality in France and worldwide. Lung cancer has one of the highest incidence rates of VTE − ranging from 3% to more than 20% according to several studies (17–19) − as well as one of the highest rates of VTE recurrence and bleeding complications among solid cancers (7, 16). Among non-small cell lung cancer (NSCLC), the subtype adenocarcinoma is associated with a higher risk of VTE (20, 21) and this risk might be increased by chemotherapy and other systemic treatments such as molecules interfering with the vascular endothelial growth factor (VEGF) pathway (9).
In recent years, the advent of immunotherapy has revolutionized the treatment and prognosis of NSCLC. The first-line current standard of care of advanced NSCLC without actionable driver mutations is based on the association of a platinum-based chemotherapy and immunotherapy (22, 23). If chemotherapy or anti-VEGF are widely recognized risk factors of VTE, the risk associated with immune checkpoint inhibitors remains unclear (9, 24, 25). Tumor molecular and genetic characteristics also appear to play a role in VTE formation (26). Several studies have shown an association between the existence of ALK or ROS1 translocations and the occurrence of VTE in NSCLC (26–29). This association is less clear concerning the impact of other tumoral markers: some studies suggest a higher VTE risk in patients with KRAS mutations and no association or a protective effect of EGFR mutations (26, 29–32). Moreover, little is known about the impact of the programmed death-ligand 1 (PD-L1) expression regarding the risk of VTE. PD-L1 is a protein expressed at the surface of tumor cells that inhibits the anti-tumor immune response. Immunotherapy drugs target PD-L1 or its receptor on T cells (PD-1) and hence interrupt the inhibition signal. PD-L1 score is a predictive marker of the efficacy of immunotherapy (22, 23). Therefore, immunotherapy and the level of PD-L1 expression could play an important role in the coagulation cascade and in the thrombosis mechanisms by activating the immune response, by generating an inflammatory tumor microenvironment and by enhancing the tissue factor expression in activated immune cells (33–36). Several studies suggest an association between the expression of PD-L1 and the incidence of VTE in NSCLC (25–27, 37). Therefore, in our study, we aimed at determining VTE incidence in NSCLC patients treated with the association of chemotherapy and immunotherapy (CT-IO) in first-line and to assess if PD-L1 is an independent risk factor of VTE.
2 Methods
2.1 Study population and design
We performed an observational retrospective single-centre cohort study at the Brest University Hospital. Patients were first identified by using the CHIMIO® software database. Patients were included if they were 18 years of age or older; if they had a confirmed diagnosis of an advanced stage NSCLC (metastatic, locally advanced non eligible for surgery or radiotherapy; or metastatic relapse of an initially localized tumor); if they had received at least one dose of a first-line treatment with an association of CT-IO according to current standards of care (a platinum-based chemotherapy associated either to pemetrexed for the non-squamous subtypes or to paclitaxel for the squamous subtype (SCC) with an inhibitor of PD-1: pembrolizumab); and if they had given their non-opposition agreement to participate in the study.
Exclusion criteria were: a small-cell histology; a previous systemic therapy for metastatic disease; patients presenting a synchronous diagnosis of cancer; patients followed in an outside institution; patients under legal protection measures and patients refusing to participate.
All patient’s relevant clinical and biological data were collected from the electronic medical record as well as tumor profile and successive lines of cancer treatment. VTE events included pulmonary embolism (PE) associated or not to deep vein thrombosis (DVT), DVT alone, central venous catheter-related thrombosis (CRT) and extensive superficial vein thrombosis (SVT) requiring an anticoagulant treatment, other vein thrombosis (superior vena cava, jugular and upper limbs veins or visceral vein thrombosis) occurring in the three months before the cancer diagnosis (inaugural VTE), during CT-IO treatment or after the first-line treatment. All VTE events were confirmed by an imaging exam: computed tomography pulmonary angiography (CTPA) or ventilation/perfusion scan for PE, doppler ultrasound for DVT, or angiography for CRT or others. Incidental VTE events were also considered. VTE recurrence was defined as a venous thrombosis in a new site or an extension of the thrombosis at the initial site. Use of anticoagulant treatment and bleeding complications were reviewed. Bleeding complications were classified according to the International Society on Thrombosis and Haemostasis (ISTH) definitions in major and minor bleeding.
2.2 Study outcomes
The primary endpoint was to determine the incidence of VTE in our cohort (i.e. VTE occurring in the three months before the cancer diagnosis (inaugural VTE), during CT-IO treatment or after the first-line treatment).
Secondary endpoints included:
1. The cumulative incidence of VTE from date of cancer diagnosis at specific time of interest (3, 6 and 12 months)
2. VTE occurrence according to PD-L1 expression (divided in three subgroups: PD-L1 < 1%; PD-L1: 1-49% and PD-L1 ≥ 50%).
3. Overall survival (OS) measured from start of first-line CT-IO treatment to death or censured at date of data collection for alive patients
4. VTE recurrence rate and characteristics
5. Bleeding complications under anticoagulation treatment
2.3 Statistical analysis
Descriptive analyses were done using median (± interquartile range [IQR]) for quantitative variables, and percentages for categorical variables. Comparison between the VTE group and the no-VTE group were performed using Student’s t-test or Wilcoxon nonparametric test. Chi-square or Fisher’s tests were used for categorical variables. A p-value < 0.05 was considered as statistical significance. VTE-free survival and overall survival were estimated by the Kaplan-Meier method. Estimations of cumulative incidence and 95% confidence intervals (95% CI) were calculated. All statistical analysis were performed using the RStudio® software (RStudio Desktop 2022.02.3 + 492 version).
2.4 Ethical considerations
This non-interventional study was approved by the Institutional Review Board of the French learned society for respiratory medicine – “ Société de Pneumologie de Langue Française” – (reference CEPRO 2022-041), by a regional ethics committee and France’s national data protection authority (CNIL), according to French law. All patients alive received written information before enrolment. Opposition should be expressed within 15 days in case of refusal.
3 Results
3.1 Patient’s baseline characteristics
From December, 2019 to February, 2022, a total of 112 patients received a first line treatment with CT-IO for an advanced NSCLC at the Department of Oncology of the Brest University Hospital. Three of them were excluded because of a synchronous neoplasm. A total of 109 patients were included in the analyses.
Population characteristics were well balanced between patients who developed VTE (VTE group n=21) and those who did not (no-VTE group n=88) (Table 1). Median age of patients was 62.7 years (37 to 79 years); 37.9% were females; 98.1% were current or former smokers; the main comorbidities were chronic respiratory and cardiovascular diseases. Only one patient (in the no-VTE group) had a prior VTE history. In the VTE group, 19.0% of patients had a prior cancer history compared to 11.4% in the no-VTE group but this difference was not statistically significant. The rate of immobility was significantly higher in the VTE group. Khorana score, previous use of anticoagulation or anti-platelet drugs did not differ between both groups, neither did the use of erythropoietin or steroids. Approximatively 90% of patients had a metastatic disease or a metastatic recurrence. No patient was treated with prior thoracic radiation. There were no significant differences between groups in terms of ECOG performance-status, stage, number of metastatic sites or presence of brain metastases. The tumor histology was an adenocarcinoma in 61.4% of the no-VTE group compared to 81.0% in the VTE group, but this difference was not statistically significant. In the no-VTE group, 44.3% of patients had a PD-L1 score <1%; 28.4% had a PD-L1 = 1-49% and 27.3% had a PD-L1≥50% compared to 38.1%; 23.8% and 38.1% respectively in the VTE-group but these differences were not statistically significant, nor was the difference observed in KRAS mutations (47.7% in the VTE group versus 31.8% in the no-VTE group). The mean duration of the first line CT-IO treatment was 6.4 months (maximum = 31.1 months).
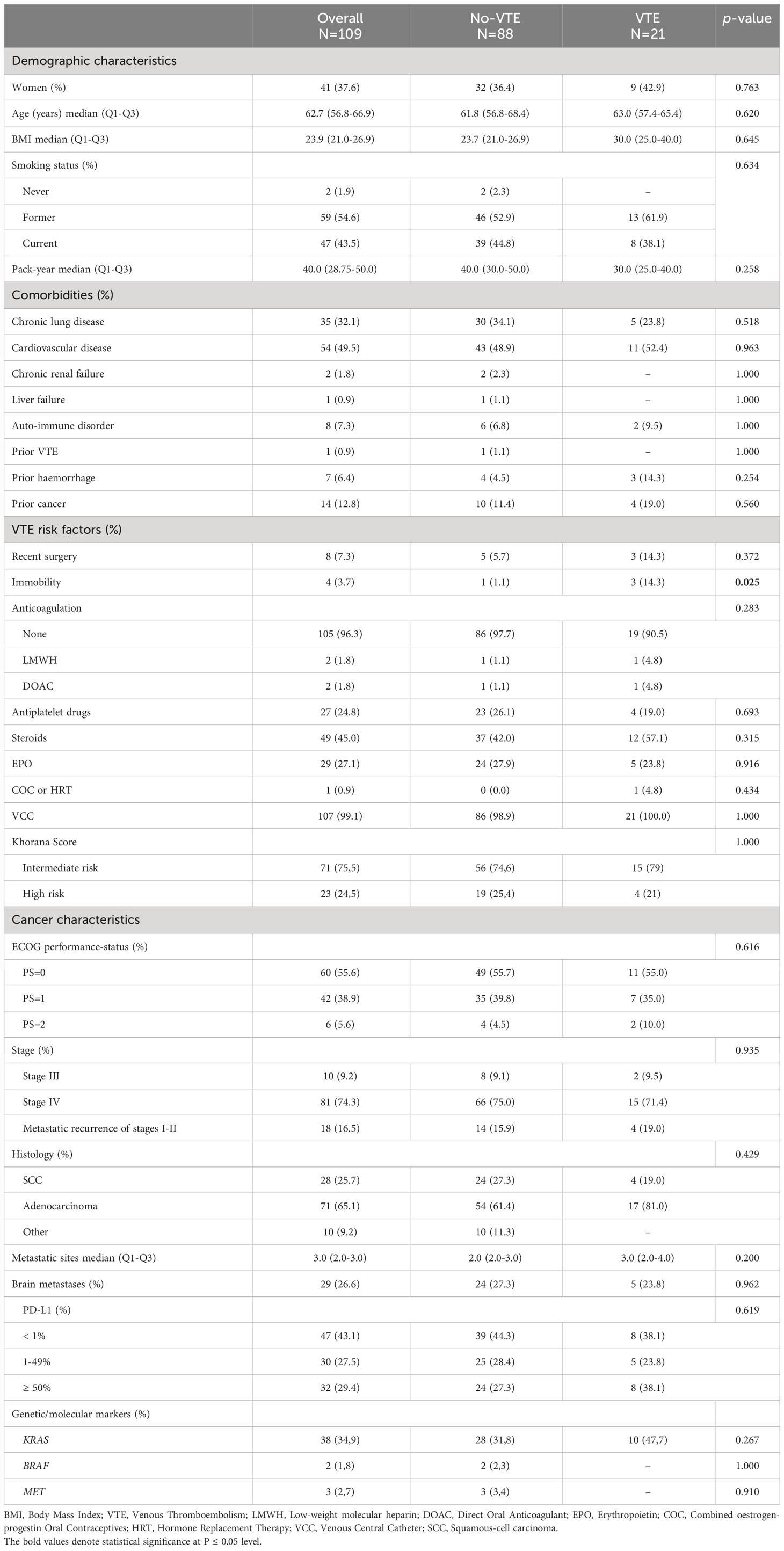
Table 1 Characteristics of the population.
Concerning the use of anticoagulants in our cohort, a total of 29 patients (26.6%) were treated with anticoagulants: 3 patients (2.7%) were already under anticoagulant treatment for an atrial fibrillation before the cancer diagnosis (all three with DOACs), 21 (19.3%) received anticoagulation during the follow-up because of VTE (66.7% with LMWH and 28.6% with DOACs), and 6 (5.5%) received anticoagulation for a no-VTE indication. Besides, 27 patients (24.8%) had an antiplatelet treatment.
3.2 First VTE event
VTE occurred in 21 of 109 patients (19.3%) during a median follow-up of 13 months (IQR: 7.1 – 22.3 months). Among these, 13 (61.9%) were PE (associated or not to DVT); 2 (9.5%) were DVT alone; 3 (14.3%) were CRT, one (4.7%) was an extensive SVT and 2 (9.5%) were other site thrombosis. Four patients had PE associated with DVT at the same time (2 were inaugural and 2 during CT-IO treatment). Among them, only one patient had in situ PE with DVT.
VTE was inaugural in 38.1% of cases, occurred during the first line CT-IO treatment in 38.1% of cases and after the first line treatment in 19% of cases. VTE incidence was especially high during the first 12 months after cancer diagnosis with a cumulative incidence at 3 months, 6 months and 12 months of 12.1% (95% CI: 5.7 - 18.1), 15.1% (95% CI: 8.0 - 21.6) and 17.5% (95% CI: 9.7 – 24.6) respectively (Figure 1). The median delay between the cancer diagnosis and the VTE occurrence was 62 days (IQR: 9-97 days).
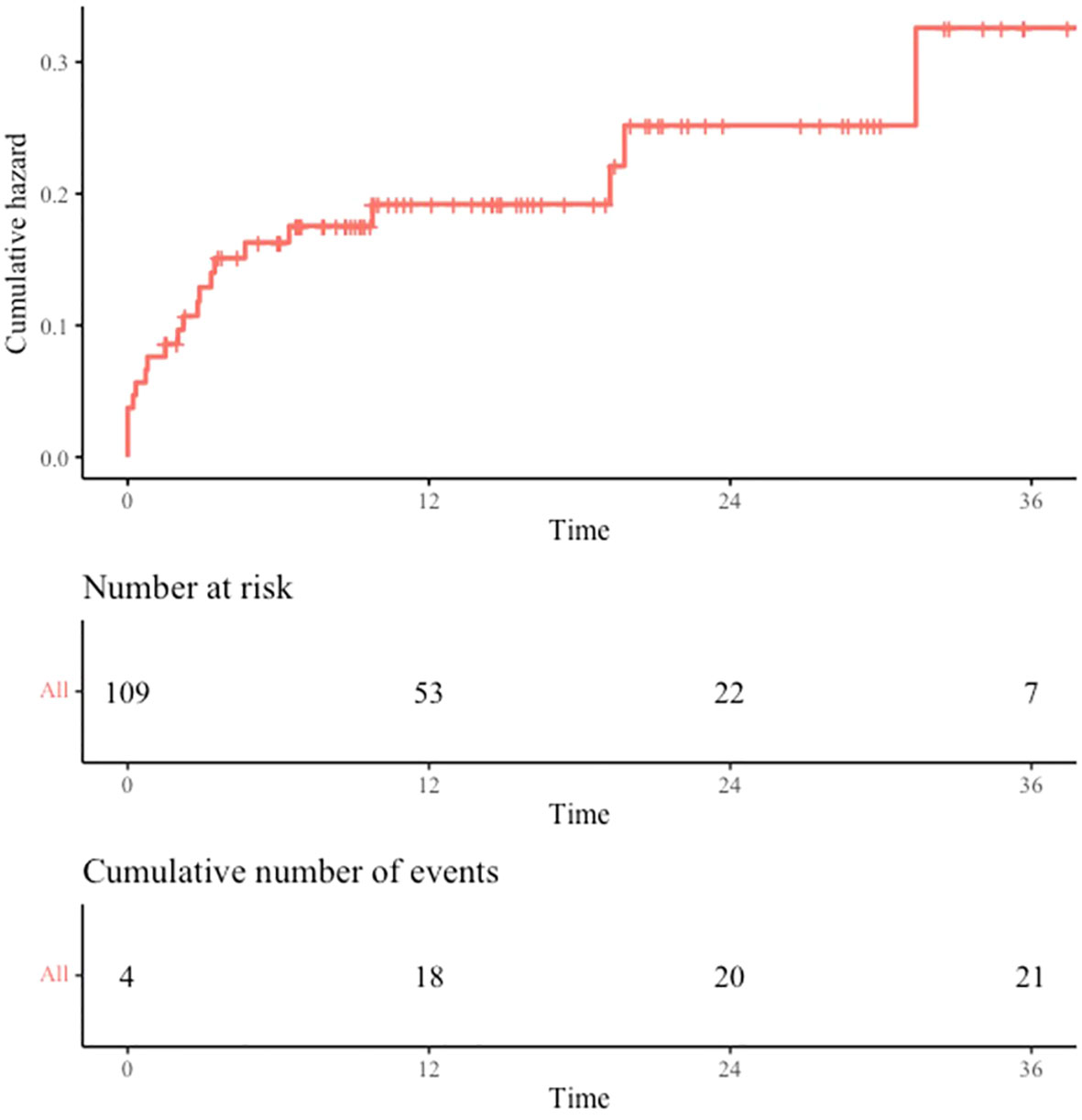
Figure 1 VTE incidence. Cumulative incidence of VTE from cancer diagnosis date. VTE occurring before cancer diagnosis are recorded at time 0. Time is expressed in months.
Among the total VTE events, 14 (66.7%) were symptomatic while 7 (33.3%) were incidental.
The anticoagulant treatment for the first VTE event was LMWH in 66.7%, DOACs in 28.6% and one patient had an inferior vena cava filter. No patient was treated with VKAs in our cohort. One PE as first-VTE event (4.8%) occurred while the patient was under prior anticoagulant treatment (DOAC). No patient developed VTE while receiving bevacizumab or after.
3.3 VTE occurrence and PD-L1 expression
In our study, VTE was not associated to PD-L1 tumor proportion score (Figure 2). No significant difference was observed when comparing VTE occurrence according to different PD-L1 scores (neither comparing PD-L1 <1% vs 1-49% vs ≥ 50%, nor comparing PD-L1 <1% vs ≥ 1% or PD-L1 <50% vs ≥ 50%). However, a trend emerged to higher PD-L1 scores in the VTE group, but this difference was not statistically significant.
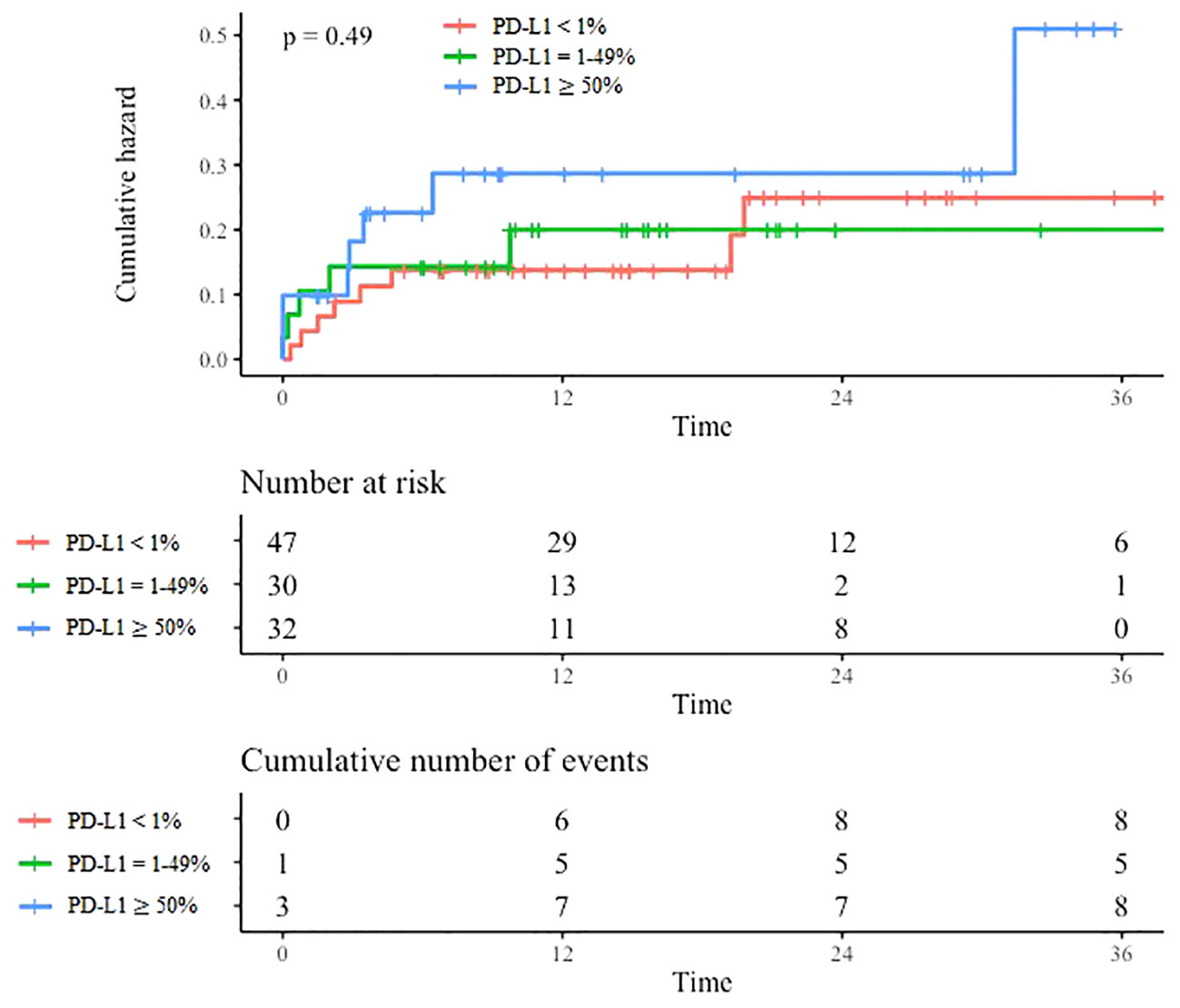
Figure 2 VTE incidence according to PD-L1 expression. Cumulative incidence of VTE according to PD-L1 expression. Time is expressed in months from cancer diagnosis.
3.4 Survival outcomes
With a median follow-up of 13 months (IQR: 7.1 – 22.3 months), the estimated rates of OS at 6 months, 12 months and 24 months were respectively 81.9% (95% CI: 74.8-89.6), 74.4% (95% CI: 66.1-83.8) and 70.3% (95% CI: 61.0-81.1). Median OS was not reached (Figure 3). At the time of data cut-off, a total of 66 patients were still alive (60.6%) and 43 had died (39.4%).
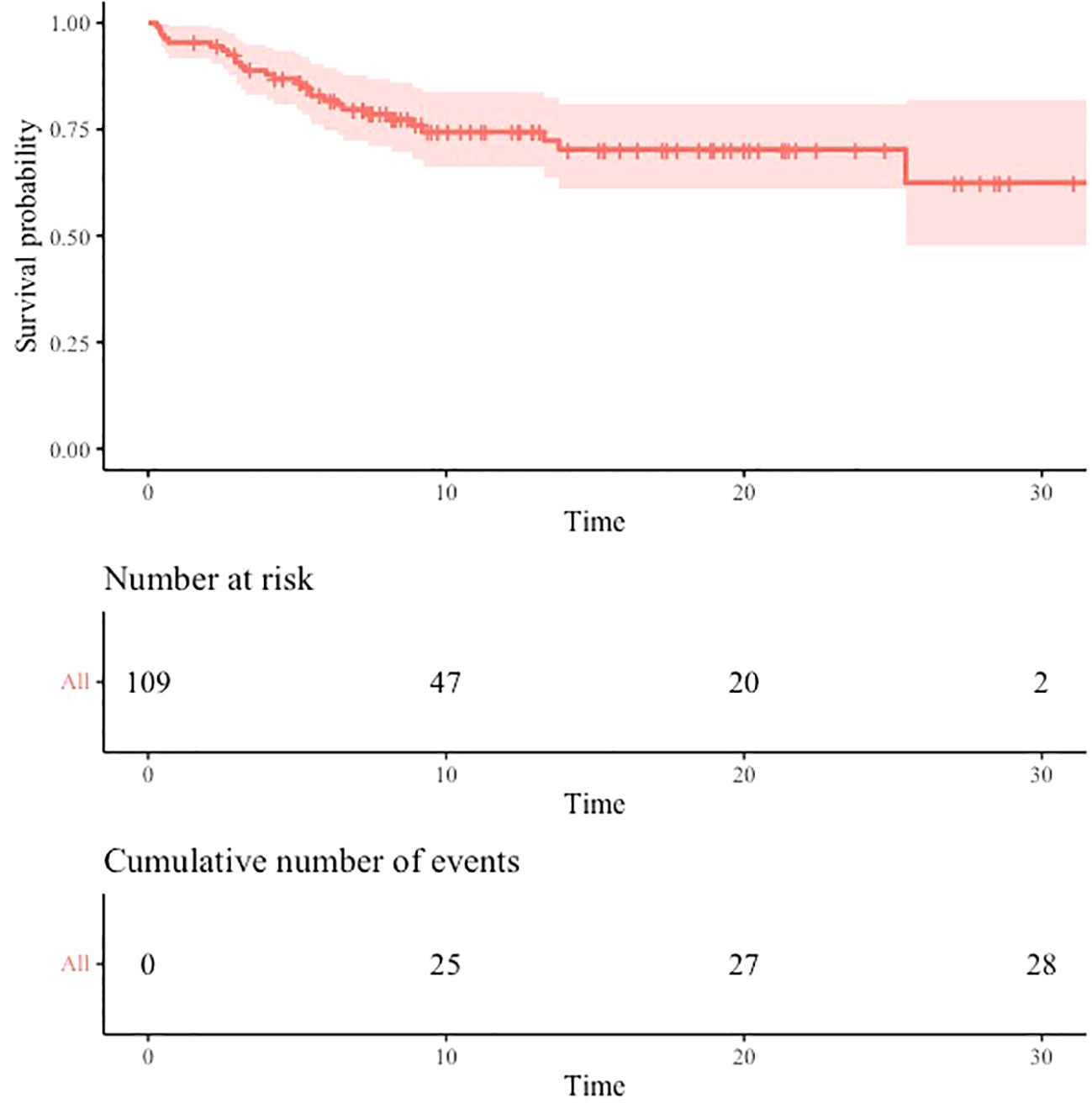
Figure 3 Overall survival. Estimated overall survival from start of first-line treatment. Time is expressed in months.
3.5 Recurrent VTE
Four patients (19.0%) presented a recurrent VTE. They all occurred under anticoagulation therapy: three with standard doses of LMWH and one with DOAC. Three of the patients were women. None had a prior VTE history before the cancer diagnosis. Three patients had an intermediate Khorana score risk at diagnosis and one had a high risk. The latter was one of the two patients to present a second VTE recurrence. In all four cases, the first VTE event was inaugural. The VTE recurrence occurred 3 to 5 months after the first VTE event. No context of immobility or recent surgery was noted. All four patients had a metastatic adenocarcinoma and only one had brain metastases. Two had a PD-L1 score ≥ 50%, one had a PD-L1 score between 1-49% and one had a PD-L1<1%. Two harbored a KRAS mutation. Two of them presented a second VTE recurrence. Only one patient had atypical VTE associated with CRT at first and second recurrence. Management consisted in catheter removal and +25% increased dose of LMWH at first recurrence and no change at second recurrence because of clinical deterioration. All four patients died 1 to 4 months after the VTE recurrence and, on average, 6.3 months after the index VTE date. Three died due to cancer progression and one died due to a major bleeding complication. Recurrent VTE characteristics are summarized in Table 2.
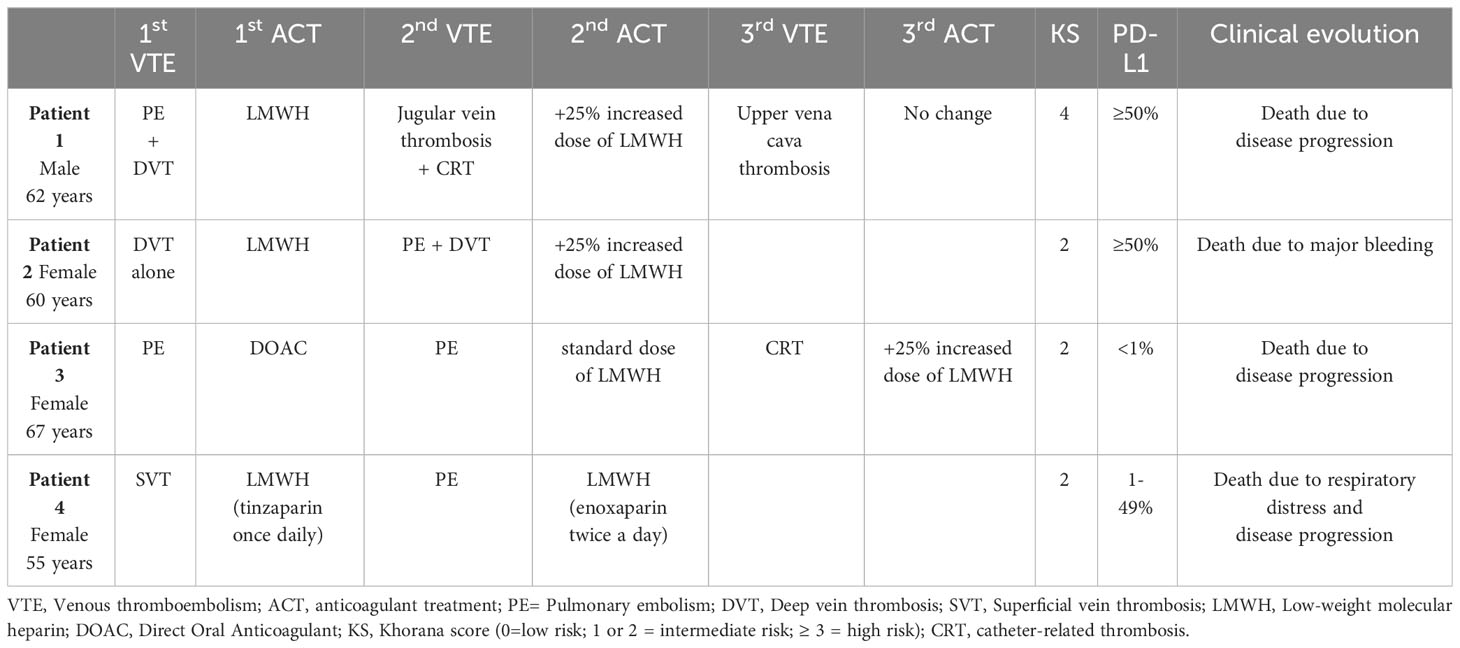
Table 2 Recurrent VTE events.
3.6 Bleeding complications under anticoagulant treatment
One patient (0.9%) presented a major bleeding complication in the form of a major hemoptysis leading to respiratory distress and patient’s death despite bronchial arterial embolization. The patient was a woman aged sixty who presented a metastatic adenocarcinoma with brain metastases and a PD-L1 score ≥ 50%. She did not suffer from hemostasis disorders nor from hepato-renal disorders (neither at the diagnosis nor at the time of the bleeding event) and had no prior bleeding history. She did not receive any anti-VEGF treatment. She was under supratherapeutic +25% LMWH dose for a recurrent VTE (according to French guidelines) when the bleeding complication occurred. Surprisingly, no minor bleeding events were reported in our study.
4 Discussion
Depending on the study, VTE incidence in lung cancer varies hugely ranging from 3% to more than 20% (17). In our cohort, the incidence of VTE (19.3%) was particularly high compared to previous studies in patients with NSCLC treated with chemotherapy but was consistent with more recent studies in patients treated with concomitant checkpoint inhibitors (18, 38). Indeed, Hill et al. recently reported a VTE incidence − considering only PE and DVT − of 9.9% at 6 months and 12.8% at 12 months in NSCLC patients treated with CT-IO. Former studies often recorded VTE events only in hospitalized patients or at the initial cancer diagnosis and did not consider VTE occurring in ambulatory patients or during the consecutive lines of systemic treatment. Besides, patients with prior VTE history or undergoing anticoagulation were often excluded. Most studies only recorded PE and DVT whereas we chose to include all VTE events, including CRT and other vein thrombosis (the rate of PE +/- DVT in our study was 13.8%) as well as incidental VTE events, as they all required a prolonged anticoagulation treatment and reflected a prothrombotic state.
Our analysis did not show a significant association between PD-L1 score and VTE occurrence. However, a trend emerged to higher PD-L1 scores in the VTE group and notably a higher VTE rate in patients with PD-L1 score ≥ 50% even if these results were not statistically significant. Other studies have previously shown an association between high PD-L1 scores and VTE (25, 27, 37). Absence of statistical significance in our study may be due to a lack of power because of its reduced size. On the other hand, the PD-L1≥ 50% patients that were included in our study may not be representative of all the PD-L1≥ 50% population as they probably had a more extended and aggressive disease than patients treated with single immunotherapy.
In our cohort, median follow-up achieved 13 months and surprisingly median OS was not reached. OS at 6 months was similar to the ones reported in clinical trials or other real-world studies of NSCLC treated with first-line CT-IO (39–41). However, OS at 12 and 24 months were higher than previously described despite our population was similar in terms of median age, sex, ECOG performance status, disease stage and PD-L1 distribution, and although we had a higher rate of brain metastases. Indeed, the latest results of phase III trials KEYNOTE-189 (pembrolizumab plus chemotherapy in metastatic nonsquamous NSCLC) and KEYNOTE-407 (pembrolizumab plus chemotherapy in metastatic SCC) reported median OS of 22.0 and 17.1 months respectively (22, 23). OS rates at 12 and 24 months were 69.8% and 45.7% in KEYNOTE-189 and 64.7% and 37.5% in KEYNOTE-407. A real-world study performed by Waterhouse et al. showed a median OS of 10.6 months in SCC and 12.0 months in nonsquamous NSCLC. OS at 12 and 24 months were 45.1% and 24.5% respectively in SCC and 49.9% and 32.5% in nonsquamous NSCLC. Highest OS in our study might be the consequence of the limited size of our cohort and the short follow-up resulting in less precise estimations at 12 and 24 months with wider 95% CI. Survival analyses according to PD-L1 expression were not performed as it was not the aim of this study and as prior studies already showed that high PD-L1 scores were associated with higher OS (39–41). Survival analyses according to VTE occurrence were not performed as this would have required more sophisticated statistical analysis considering the competing risk of death and as it is well recognized that cancer patients experiencing VTE have a shorter survival.
We found a higher VTE recurrence rate (19%) than reported in previous trials comparing DOACs versus LMWH for the treatment of cancer-associated VTE (12–15, 42) but similar to other real-world studies (7, 16). Only one of the four patients presenting a VTE recurrence had a high Khorana score risk highlighting the poor prognostic value of this indicator. We observed a higher proportion of PD-L1 ≥ 1% among patients presenting a VTE recurrence but, because of the limited size of our study population, no conclusion with a statistical significance can be driven by this observation. VTE recurrences occurred in the first months after the first VTE event. Patients experiencing a VTE recurrence died shortly after, highlighting the impact of VTE recurrences on survival and suggesting an aggressive underlying disease.
Only one patient (0.9%) presented a major bleeding complication while under anticoagulant treatment. No clinically relevant non-major (CRNM) bleeding event was noted, probably because these events were unreported in the medical records. Besides, we did not consider minor hemoptysis as CRNM bleedings since it is a sign of the disease itself rather than a clinically relevant complication. We did not find any study reporting bleeding events among lung cancer patients; we only found studies evaluating the efficacy and safety of anticoagulants for VTE in lung cancer patients (42). The main limitations of our study were its retrospective design and the reduced size of the cohort as well as a limited follow-up duration. However, ours is one of the first studies assessing VTE incidence in a real-world cohort of NSCLC patients treated with CT-IO as first-line therapy and evaluating the role of PD-L1 as a possible predictor marker of VTE. Our study brings new data on this frequent and serious complication in NSCLC in the era of chemo-immunotherapy associations. Further studies with a prospective design and more patients are needed to assess more accurately the risk of VTE associated to different anticancer therapies and tumor markers, especially if high PD-L1 expression might be associated with VTE.
5 Conclusion
VTE is a common and serious complication in advanced NSCLC patients treated with first-line concomitant chemo-immunotherapy, often inaugural or occurring in the first months after cancer diagnosis. The incidence of VTE achieved 19.3% in our study. PD-L1 did not appear to be statistically associated with VTE occurrence. We recorded high VTE recurrence rates despite anticoagulant treatment. Further investigations are needed to determine if high PD-L1 expression is associated with VTE.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Institutional Review Board of the French learned society for respiratory medicine – “Société de Pneumologie de Langue Française” – (reference CEPRO 2022-041). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
Category 1: Conception and design of study: LA, MG, CO, RD. Acquisition of data: LA.Analysis and/or interpretation of data: LA, MG, CO. Category 2: Drafting the manuscript: LA, MG, CO. Revising the manuscript critically for important intellectual content: All authors. Category 3: Approval of the version of the manuscript to be published (the names of all authors must be listed): LA, MG, CO, RD, CT, FC.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CT-IO, chemo-immunotherapy; CRT, Central venous catheter-related thrombosis; CTPA, Computed tomography pulmonary angiography; DOACs, Direct oral anticoagulants; DVT, Deep vein thrombosis; IQR, Interquartile range; LMWH, Low-molecular weight heparin; NSCLC, Non-small cell lung cancer; PD-L1, Programmed death-ligand 1; PE, Pulmonary embolism; SCC, Squamous cell carcinoma; SD, Standard deviation; SVT, Superficial vein thrombosis; VEGF, Vascular endothelial growth factor; VKAs, Vitamin K antagonists; VTE, Venous thromboembolism.
References
1. Fernandes CJ, Morinaga LTK, Alves JL, Castro MA, Calderaro D, Jardim CVP, et al. Cancer-associated thrombosis: the when, how and why. Eur Respir Rev (2019) 28:180119. doi: 10.1183/16000617.0119-2018
2. Heit JA, Spencer FA, White RH. The epidemiology of venous thromboembolism. J Thromb Thrombolysis (2016) 41:3–14. doi: 10.1007/s11239-015-1311-6
3. Laporte S, Mismetti P, Décousus H, Uresandi F, Otero R, Lobo JL, et al. the RIETE Investigators, 2008. Clinical Predictors for Fatal Pulmonary Embolism in 15 520 Patients With Venous Thromboembolism: Findings From the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) Registry. Circulation (2008)117:1711–6. doi: 10.1161/CIRCULATIONAHA.107.726232
4. Khorana AA, Kuderer NM, McCrae K, Milentijevic D, Germain G, Laliberté F, et al. Cancer associated thrombosis and mortality in patients with cancer stratified by khorana score risk levels. Cancer Med (2020) 9:8062–73. doi: 10.1002/cam4.3437
5. Heit JA, Mohr DN, Silverstein MD, Petterson TM, O’Fallon WM, Melton LJ. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: A population-based cohort study. Arch Intern Med (2000) 160:761. doi: 10.1001/archinte.160.6.761
6. Hutten BA, Prins MH, Gent M, Ginsberg J, Tijssen JGP, Büller HR. Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both Malignancy and achieved international normalized ratio: A retrospective analysis. JCO (2000) 18:3078–83. doi: 10.1200/JCO.2000.18.17.3078
7. Prandoni P, Lensing AWA, Piccioli A, Bernardi E, Simioni P, Girolami B, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood (2002) 100:3484–8. doi: 10.1182/blood-2002-01-0108
8. Weber C, Pharm D, Adal NG, Riedel E, Soff GA. Identification and characterization of recurrent venous thrombosis in cancer patients. Blood (2010) 116(21):3328. doi: 10.1182/blood.V116.21.3328.3328
9. Madison CJ, Melson RA, Conlin MJ, Gundle KR, Thompson RF, Calverley DC. Thromboembolic risk in patients with lung cancer receiving systemic therapy. Br J Haematol (2021) 194:179–90. doi: 10.1111/bjh.17476
10. Key NS, Khorana AA, Kuderer NM, Bohlke K, Lee AYY, Arcelus JI, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. JCO (2020) 38:496–520. doi: 10.1200/JCO.19.01461
11. Mahé I, Meyer G, Girard P, Bertoletti L, Laporte S, Couturaud F, et al. Traitement de la maladie veineuse thromboembolique au cours du cancer. Mise à jour mars 2021. [Treatment of cancer-associated venous thromboembolism. Update March 2021]. Rev Des Maladies Respiratoires (2021) 38:427–37. doi: 10.1016/j.rmr.2021.03.001
12. Raskob GE, van Es N, Verhamme P, Carrier M, Di Nisio M, Garcia D, et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N Engl J Med (2018) 378:615–24. doi: 10.1056/NEJMoa1711948
13. Young AM, Marshall A, Thirlwall J, Chapman O, Lokare A, Hill C, et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). JCO (2018) 36:2017–23. doi: 10.1200/JCO.2018.78.8034
14. McBane RD, Wysokinski WE, Le Rademacher JG, Zemla T, Ashrani A, Tafur A, et al. Apixaban and dalteparin in active Malignancy associated venous thromboembolism: The ADAM VTE trial. J Thromb Haemost (2020) 18:411–21. doi: 10.1111/jth.14662
15. Agnelli G, Becattini C, Meyer G, Muñoz A, Huisman MV, Connors JM, et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N Engl J Med (2020) 382:1599–607. doi: 10.1056/NEJMoa1915103
16. Chee CE, Ashrani AA, Marks RS, Petterson TM, Bailey KR, Melton LJ, et al. Predictors of venous thromboembolism recurrence and bleeding among active cancer patients: a population-based cohort study. Blood (2014) 123:3972–8. doi: 10.1182/blood-2014-01-549733
17. Li Y, Shang Y, Wang W, Ning S, Chen H. Lung cancer and pulmonary embolism: what is the relationship? A review. J Cancer (2018) 9:3046–57. doi: 10.7150/jca.26008
18. Connolly GC, Dalal M, Lin J, Khorana AA. Incidence and predictors of venous thromboembolism (VTE) among ambulatory patients with lung cancer. Lung Cancer (2012) 78:253–8. doi: 10.1016/j.lungcan.2012.09.007
19. Chew HK, Davies AM, Wun T, Harvey D, Zhou H, White RH. The incidence of venous thromboembolism among patients with primary lung cancer. J Thromb Haemost (2008) 6:601–8. doi: 10.1111/j.1538-7836.2008.02908.x
20. Blom JW, Osanto S, Rosendaal FR. The risk of a venous thrombotic event in lung cancer patients: higher risk for adenocarcinoma than squamous cell carcinoma. J Thromb Haemost (2004) 2:1760–5. doi: 10.1111/j.1538-7836.2004.00928.x
21. Lee Y-G, Kim I, Lee E, Bang S-M, Kang CH, Kim YT, et al. Risk factors and prognostic impact of venous thromboembolism in Asian patients with non-small cell lung cancer. Thromb Haemost (2014) 111:1112–20. doi: 10.1160/TH13-11-0956
22. Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N Engl J Med (2018) 378:2078–92. doi: 10.1056/NEJMoa1801005
23. Paz-Ares L, Luft A, Vicente D, Tafreshi A, Gümüş M, Mazières J, et al. Pembrolizumab plus chemotherapy for squamous non–small-cell lung cancer. N Engl J Med (2018) 379:2040–51. doi: 10.1056/NEJMoa1810865
24. Icht O, Darzi N, Shimony S, Jacobi O, Reinhorn D, Landman Y, et al. Venous thromboembolism incidence and risk assessment in lung cancer patients treated with immune checkpoint inhibitors. J Thromb Haemost (2021) 19:1250–8. doi: 10.1111/jth.15272
25. Deschênes-Simard X, Richard C, Galland L, Blais F, Desilets A, Malo J, et al. Venous thrombotic events in patients treated with immune checkpoint inhibitors for non-small cell lung cancer: A retrospective multicentric cohort study. Thromb Res (2021) 205:29–39. doi: 10.1016/j.thromres.2021.06.018
26. Liu Y, Wang W, Wu F, Gao G, Xu J, Li X, et al. High discrepancy in thrombotic events in non-small cell lung cancer patients with different genomic alterations. Transl Lung Cancer Res (2021) 10:1512–24. doi: 10.21037/tlcr-20-1290
27. Xiong W, Du H, Ding W, Sun J, Xu M, Guo X. The association between pulmonary embolism and the cancer-related genomic alterations in patients with NSCLC. Respir Res (2020) 21:185. doi: 10.1186/s12931-020-01437-6
28. Dou F, Zhang Y, Yi J, Zhu M, Zhang S, Zhang D, et al. Association of ALK rearrangement and risk of venous thromboembolism in patients with non-small cell lung cancer: A prospective cohort study. Thromb Res (2020) 186:36–41. doi: 10.1016/j.thromres.2019.12.009
29. Qian X, Fu M, Zheng J, Zhou J, Zhou J. Driver genes associated with the incidence of venous thromboembolism in patients with non-small-cell lung cancer: A systematic review and meta-analysis. Front Oncol (2021) 11:680191. doi: 10.3389/fonc.2021.680191
30. Roopkumar J, Poudel SK, Gervaso L, Reddy CA, Velcheti V, Pennell NA, et al. Risk of thromboembolism in patients with ALK- and EGFR-mutant lung cancer: A cohort study. J Thromb Haemost (2021) 19:822–9. doi: 10.1111/jth.15215
31. Dou F, Li H, Zhu M, Liang L, Zhang Y, Yi J, et al. Association between oncogenic status and risk of venous thromboembolism in patients with non-small cell lung cancer. Respir Res (2018) 19:88. doi: 10.1186/s12931-018-0791-2
32. Corrales-Rodriguez L, Soulières D, Weng X, Tehfe M, Florescu M, Blais N. Mutations in NSCLC and their link with lung cancer-associated thrombosis: A case-control study. Thromb Res (2014) 133:48–51. doi: 10.1016/j.thromres.2013.10.042
33. Date K, Ettelaie C, Maraveyas A. Tissue factor-bearing microparticles and inflammation: a potential mechanism for the development of venous thromboembolism in cancer. J Thromb Haemost (2017) 15(12):2289–99. doi: 10.1111/jth.13871
34. De Palma R, Cirillo P, Ciccarelli G, Barra G, Conte S, Pellegrino G, et al. Expression of functional tissue factor in activated T-lymphocytes in vitro and in vivo: A possible contribution of immunity to thrombosis? Int J Cardiol (2016) 218:188–95. doi: 10.1016/j.ijcard.2016.04.177
35. Goel A, Khorana A, Kartika T, Gowda S, Tao DL, Thawani R, et al. Assessing the risk of thromboembolism in cancer patients receiving immunotherapy. Eur J Haematol (2022) 108:271–7. doi: 10.1111/ejh.13734
36. Roopkumar J, Swaidani S, Kim AS, Thapa B, Gervaso L, Hobbs BP, et al. Increased incidence of venous thromboembolism with cancer immunotherapy. Med (N Y) (2021) 2:423–34. doi: 10.1016/j.medj.2021.02.002
37. Nichetti F, Ligorio F, Zattarin E, Signorelli D, Prelaj A, Proto C, et al. Is there an interplay between immune checkpoint inhibitors, thromboprophylactic treatments and thromboembolic events? Mechanisms and impact in non-small cell lung cancer patients. Cancers (2019) 12:67. doi: 10.3390/cancers12010067
38. Hill H, Robinson M, Lu L, Slaughter D, Amin A, Mileham K, et al. Venous thromboembolism incidence and risk factors in non-small cell lung cancer patients receiving first-line systemic therapy. Thromb Res (2021) 208:71–8. doi: 10.1016/j.thromres.2021.10.014
39. Rodríguez-Abreu D, Powell SF, Hochmair MJ, Gadgeel S, Esteban E, Felip E, et al. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: protocol-specified final analysis from KEYNOTE-189. Ann Oncol (2021) 32:881–95. doi: 10.1016/j.annonc.2021.04.008
40. Paz-Ares L, Vicente D, Tafreshi A, Robinson A, Soto Parra H, Mazières J, et al. A randomized, placebo-controlled trial of pembrolizumab plus chemotherapy in patients with metastatic squamous NSCLC: protocol-specified final analysis of KEYNOTE-407. J Thorac Oncol (2020) 15:1657–69. doi: 10.1016/j.jtho.2020.06.015
41. Waterhouse D, Lam J, Betts KA, Yin L, Gao S, Yuan Y, et al. Real-world outcomes of immunotherapy–based regimens in first-line advanced non-small cell lung cancer. Lung Cancer (2021) 156:41–9. doi: 10.1016/j.lungcan.2021.04.007
Keywords: venous thromboembolism, non-small cell lung cancer, PD-L1 expression, chemo-immunotherapy, VTE recurrence, bleeding complications
Citation: Aguiar De Azevedo L, Orione C, Tromeur C, Couturaud F, Descourt R and Geier M (2024) Incidence of venous thromboembolism and association with PD-L1 expression in advanced non-small cell lung cancer patients treated with first-line chemo-immunotherapy. Front. Oncol. 13:1221106. doi: 10.3389/fonc.2023.1221106
Received: 11 May 2023; Accepted: 11 December 2023;
Published: 08 January 2024.
Edited by:
Nobukazu Fujimoto, Okayama Rosai Hospital, JapanReviewed by:
Julien Ancel, Reims University, FranceArianna Pannunzio, Sapienza University of Rome, Italy
Copyright © 2024 Aguiar De Azevedo, Orione, Tromeur, Couturaud, Descourt and Geier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Margaux Geier, bWFyZ2F1eC5nZWllckBjaHUtYnJlc3QuZnI=