 Elena Ramos-Ruperez1
Elena Ramos-Ruperez1 Vicente Escudero-Vilaplana2,3*Paula Ruiz-Briones2,3
Vicente Escudero-Vilaplana2,3*Paula Ruiz-Briones2,3 Roberto Collado-Borrell2,3
Roberto Collado-Borrell2,3 Cristina Villanueva-Bueno2,3
Cristina Villanueva-Bueno2,3 José Luis Revuelta-Herrero2,3Eva González-Haba2,3Xandra Garcia-Gonzalez2,3Sara Ibañez-Garcia2,3Sara Perez-Ramirez3,4
José Luis Revuelta-Herrero2,3Eva González-Haba2,3Xandra Garcia-Gonzalez2,3Sara Ibañez-Garcia2,3Sara Perez-Ramirez3,4 Eduardo Zatarain-Nicolás3,5,6,7Ana Herranz2,3María Sanjurjo2,3
Eduardo Zatarain-Nicolás3,5,6,7Ana Herranz2,3María Sanjurjo2,3- 1San Pablo Centro de Estudios Universitarios (CEU), University, Madrid, Spain
- 2Pharmacy Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 3Instituto de Investigación Sanitaria Gregorio Marañón, Madrid, Spain
- 4Medical Oncology Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 5Cardiology Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 6Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBER-CV), Madrid, Spain
- 7Complutense University, Madrid, Spain
Objective: The management of cardiotoxicity concerning the use of oral antineoplastic agents (OAAs) is a challenge for healthcare professionals. Our objective was to create a comprehensive medication management guide with dose adjustment recommendations on OAAs concerning cardiotoxic and lipid metabolic adverse events (AEs) to assist healthcare professionals when prescribing OAAs.
Materials and methods: A review of the available information on all dose adjustments necessary to safely prescribe and dispense OAAs concerning cardiotoxicity was conducted. In January 2023, we identified all OAAs authorized by the European Medicines Agency (EMA). For each drug, the latest summary of product characteristics (SPC) approved by the EMA and the tertiary data source Lexicomp® were reviewed. Cardiotoxic AEs were recorded, namely, QT interval prolongation, decrease in left ventricular ejection fraction (LVEF), imbalances in blood pressure (hypertension and hypotension), alterations in heart rate (tachycardia and bradycardia), and thrombosis. Any available dose adjustment recommendations in case of an occurrence of these adverse events were collected.
Results: In all, 93 different OAAs had been approved by the EMA and were reviewed. Among them, 51.6% have recognized cardiotoxic AEs and 10.8% can cause alterations in lipid metabolism. A total of 27 (29.0%) OAAs had specific recommendations regarding QT prolongation; 88.9% were listed in the SPC and 59.3% in Lexicomp®. Eight OAAs (9.68%) have reported a decrease in LVEF, and four of these drugs, namely, encorafenib, lorlatinib, ripretinib, and sunitinib, have specific management recommendations. Almost half (49.5%) of currently approved OAAs can potentially alter blood pressure; 34 (36.6%) of them have been reported to cause hypertension and 12 (12.9%) are related to hypotension. Tachycardia and/or bradycardia are associated with 22.6% and 8.6% of the evaluated drugs, respectively. Regarding thrombosis, 30 (32.3%) of the drugs analyzed included the appearance of a thrombus as a possible AE.
Conclusions: More than half of the OAAs can produce cardiotoxic effects, with the most frequent being blood pressure alteration and QT interval prolongation with a non-depreciable incidence of LV dysfunction or thrombosis. Before starting the treatment, it is necessary to stratify baseline cardiovascular risk, plan a surveillance schedule, and consider referral to cardio-oncology units.
1 Introduction
Oncohematology is the medical area with the largest pipeline of molecules in research. Oral antineoplastic agents (OAAs) currently represent a large percentage of these new treatments. Most OAAs act specifically against specific molecular targets, increasing their effectiveness. However, OAAs have a narrow therapeutic range, making them high-risk drugs that, without proper dosing and follow-up, have severe consequences (1).
OAAs present class adverse effects (AEs) that can lead to treatment interruption or, in the most severe cases, to the patient’s death. The most frequent AEs related to OAAs are gastrointestinal, hematological, and skin effects (2). The patients’ age, polypharmacy, and the presence of other comorbidities make patients especially vulnerable to drug AEs (3). A common comorbidity is cardiovascular (CV) disease, with approximately 11.3% of cancer patients having a previous cardiac history (4), including left ventricular dysfunction, atrial fibrillation, hypertension, and QT prolongation/arrhythmias.
Despite increased recognition and consensus of cardiotoxicity from cancer therapy (5) and recent international guidelines of cardio-oncology, such as the European Society of Cardiology (ESC) Guidelines (6), clinical care for patients remains a challenge due to the variability of these undesirable effects among the different OAAs, the high number of new molecules, and the low frequency of some of the toxicities. Besides, it should be noted that clinical trials exclude patients in risk situations, such as those with previous CV pathologies, making recommendations on these drugs challenging to make in many cases (6). Thus, due to the rapid development and availability of new OAA drugs, it is crucial to propose an updated practical approach to monitor and manage CV toxicities to improve the clinical response, medication safety, and quality of life of cancer patients treated with OAAs.
Our objective was to create a comprehensive medication management guide with dose adjustment recommendations on OAAs concerning cardiotoxic and lipid metabolic AEs to assist healthcare professionals in oncology and hematology when prescribing these drugs.
2 Materials and methods
A review of the available information on all dose adjustments necessary to safely prescribe and dispense OAAs concerning cardiotoxicity was conducted.
In January 2023, we identified all OAAs authorized by the European Medicines Agency (EMA). We considered as OAAs those drugs for oral administration divided into the following groups of drugs according to their Anatomical Therapeutic Chemical (ATC) (7): plant alkaloids (etoposide, topotecan, and vinorelbine), alkylating agents (busulfan, cyclophosphamide, chlorambucil, lomustine, and melphalan), anaplastic lymphoma kinase (ALK) inhibitors (alectinib, brigatinib crizotinib, ceritinib, and lorlatinib), antimetabolites (azacitidine, capecitabine, methotrexate, mercaptopurine, and trifluridine/tipiracil), BCR-ABL tyrosine kinase inhibitors (asciminib, bosutinib, dasatinib, imatinib, nilotinib, and ponatinib), Bruton’s tyrosine kinase (BTK) inhibitors (acalabrutinib, ibrutinib, and zanubrutinib), cyclin-dependent kinase (CDK) inhibitors (abemaciclib, palbociclib, and ribociclib), epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (afatinib, erlotinib, gefitinib, osimertinib, and poziotinib), hormone antagonists and related agents (abiraterone, anastrozole, apalutamide, bicalutamide, daralutamide, enzalutamide, exemestane, letrozole, relugolix, and tamoxifen), human epidermal growth factor receptor 2 tyrosine kinase receptor 2 (HER2) inhibitors (lapatinib, neratinib, and tucatinib), immunosuppresants (lenalidomide, pomalidomide, and thalidomide), Janus kinase (JAK) inhibitors (ferdatinib and ruxolitinib), mammalian target of rapamycin (mTOR) inhibitors (everolimus), mitogen-activated protein kinase (MEK) inhibitors (binimetinib, cobimetinib, and trametinib), polyadenosine diphosphate [ADP]–ribose polymerase (PARP) inhibitors (niraparib, olaparib, and rucaparib), serine/threonine kinase BRAF inhibitors (encorafenib, dabrafenib, and vemurafenib), vascular endothelial growth factor tyrosine kinase receptor (VEGF) inhibitors (axitinib and tivozanib), other protein kinase inhibitors (avapritinib, cabozantinib, capmatinib, gliteritinib, lenvatinib, midostaurine, nintedanib, pazopanib, pralsetinib, regorafenib, ripretinib, selpercatinib, sorafenib, sunitinib, tepotinib, and vandetanib), FGFR2 inhibitors (pemigatinib), phosphatidylinositol-3-kinase (Pi3K) inhibitors (alpelisib, idelalisib, and duvelisib), and other antineoplastic agents (hydroxycarbamide, ixazomib, selinexor, sonidegib, sotorasib, temozolomide, tretinoin, vismodegib, and venetoclax).
For each drug, the latest summary of product characteristics (SPC) approved by the EMA was reviewed. In cases where different prescription drugs with the same active ingredient were available (i.e., generic drugs), the SPC for the originally registered product was consulted. Besides, we reviewed the information available in the toxicity section for each different OAA at the tertiary data source Lexicomp®. Adverse events considered as cardiotoxicity and gathered for each OAA from both data sources were included, namely, QT interval prolongation, decrease in left ventricular ejection fraction (LVEF), imbalances in blood pressure (hypertension and hypotension), alterations in heart rate (tachycardia and bradycardia), and thrombosis. Due to their relationship with cardiovascular risk, alterations in lipid metabolism (hypertriglyceridemia and hypercholesterolemia) were also evaluated. Any available dose adjustment recommendations in case of an occurrence of these adverse events were collected.
The severity of each AE was graded according to the Common Terminology Criteria for Adverse Events (CTCAE v5.0 classification) (8). The CTCAE system is a product of the US National Cancer Institute (NCI) that uses a range of grades from 1 (mild) to 5 (death), specifying the specific conditions and symptoms that the patient must have to be classified in one or another category (Supplementary Material).
3 Results
At the time of the study (January 2023), 93 different OAAs had been approved by the EMA and were reviewed. Among them, 51.6% have recognized cardiotoxic AEs and 10.8% can cause alterations in lipid metabolism (Table 1).

Table 1 Cardiotoxic effect of oral antineoplastic agents.
A total of 27 (29.0%) OAAs had specific recommendations regarding QT prolongation; 88.9% were listed in the SPC and 59.3% in Lexicomp® (Supplementary Material). Recommendations on the management of QT prolongation described by the EMA and Lexicomp® concurred in 80.0% of OAAs. In cases with different recommendations, no clinically relevant discrepancies were found between the two data sources. The main discrepancies were due to the lack of information from the EMA on acalabrutinib, dabrafenib, gilteritinib, regorafenib, relugolix, and vinorelbine, and from Lexicomp® on alectinib, avapritinib, dabrafenib, cabozantinib, capecitabine, enzalutamide, encorafenib, lorlatinib lenalidomide, melphalan, methotrexate, imatinib, ponatinib, pomalidomide, pralsetinib, regorafenib, sunitinib, tepotinib, tivozanib, vandetanib, and vemurafenib in the analysis of some of the AEs studied. In general, EMA’s recommendations included more specific information for most of the drugs.
Regarding the decrease in LVEF, eight OAAs (9.7%) have reported this cardiotoxic effect, and four of these drugs, namely, encorafenib, lorlatinib, ripretinib, and sunitinib, have specific management recommendations (Table 2). It is worth noting that LVEF should be measured following international recommendations, preferably by echocardiogram and using 3D technology. In cases of an unclear echocardiography window, intravenous contrast can be administered or cardiac magnetic resonance as a gold standard can be performed (6).
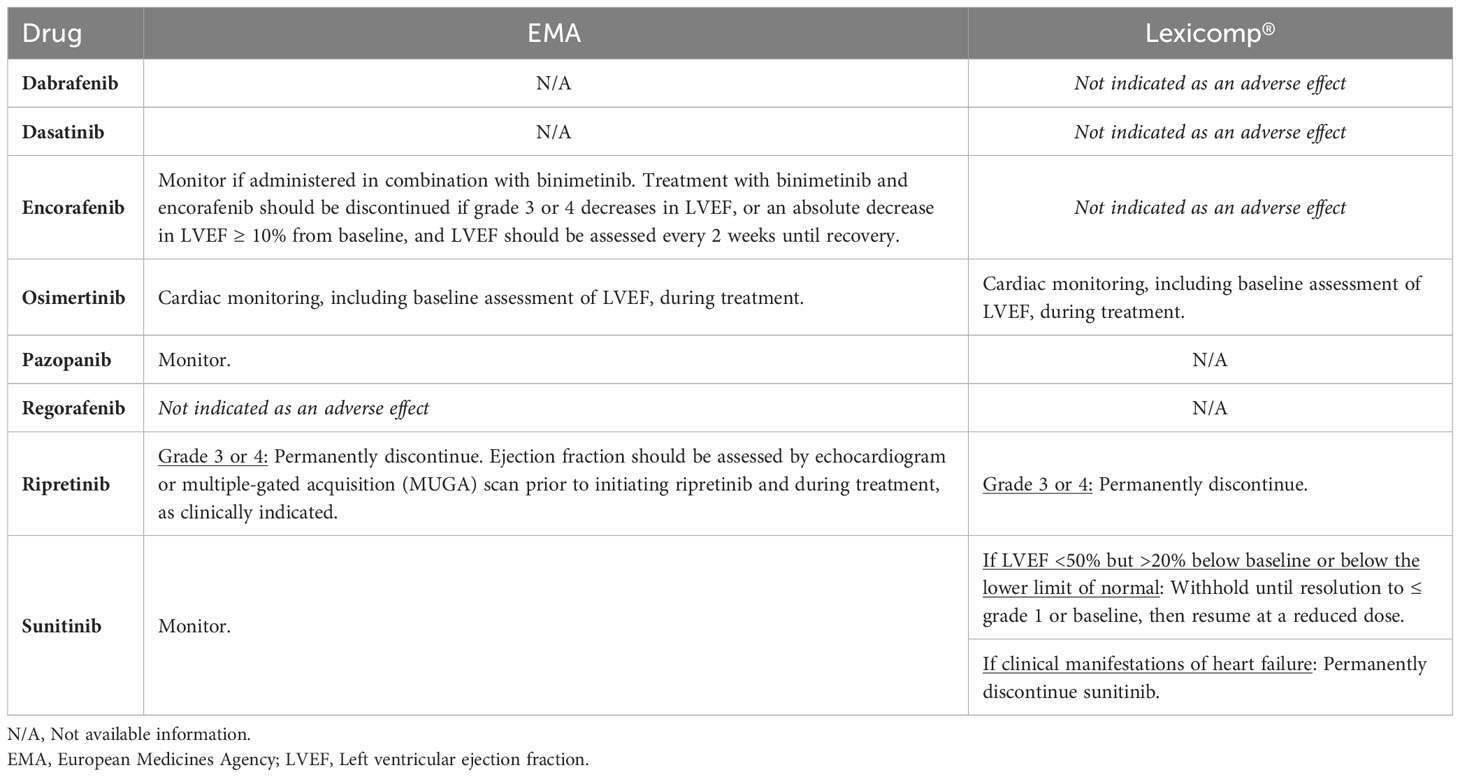
Table 2 Specific recommendations concerning oral antineoplastic agents in case of a decrease in LVEF.
Almost half (49.5%) of currently approved OAAs can potentially alter blood pressure control; 34 (36.6%) of them have been reported to cause hypertension and 12 (12.9%) are related to hypotension. Table 3 describes specific EMA and Lexicomp® recommendations for each OAA in case of imbalances in blood pressure. First-line antihypertensive treatment should be ACE-I or ARB, as they also prevent LVEF decrease and are the first line of treatment for general hypertension. For cases with high levels (systolic HTN over 160 mmHg), the addition of a dihydropyrimidine calcium channel blocker can help to achieve faster control of HTN levels due to the combined effect of RASS inhibition and arterial vasodilation, counteracting endothelial toxicity of most of the TKIs (6). In most cases of persistent hypertension despite adequate medical treatment, the OAA should be temporarily interrupted and/or its dose reduced. Regarding the management of hypotension, we have only found recommendations for 2 of the 10 drugs involved: dabrafenib and dasatinib. The special case of abiraterone should be mentioned, while spironolactone is not recommended as it may interact with the androgen-synthesis pathway where abiraterone actuates (9). In addition, it is important for patients to actively monitor their blood pressure at home. Home blood pressure monitoring provides valuable insights about a patient’s blood pressure patterns throughout the day, which can help healthcare providers make informed treatment decisions. Regular monitoring empowers patients to actively participate in their hypertension management, leading to better control of blood pressure and improved health outcomes.
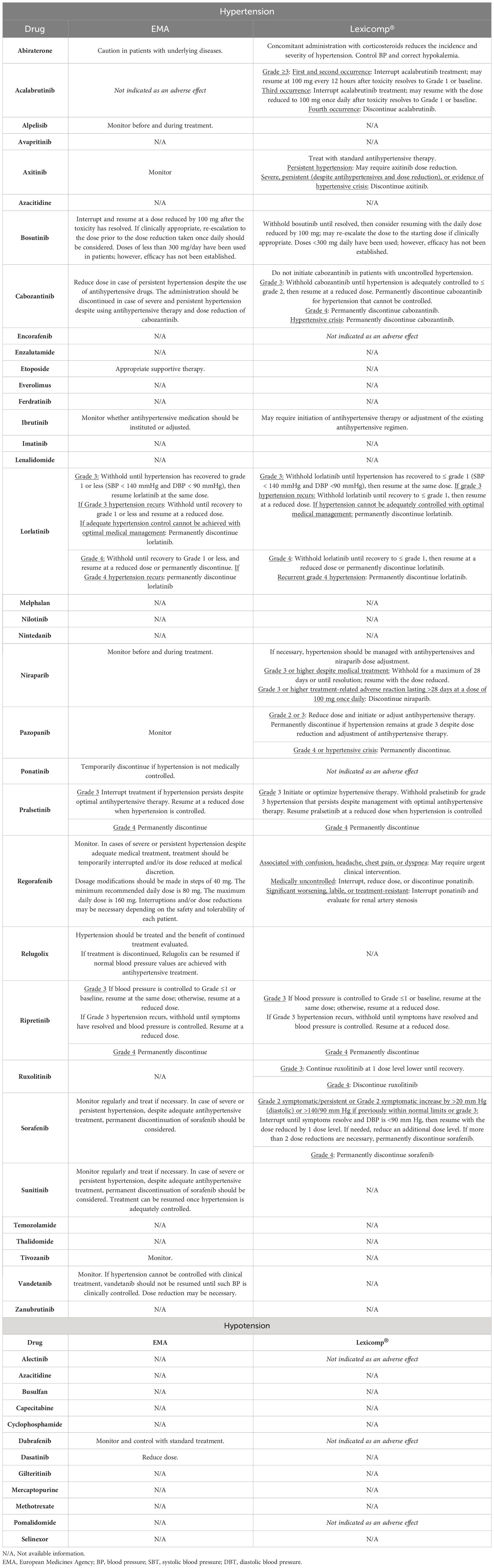
Table 3 Specific recommendations concerning oral antineoplastic agents in case of imbalances in blood pressure.
Tachycardia and/or bradycardia are associated with 22.58% and 8.6% of the evaluated drugs, respectively. Nilotinib and regorafenib are the only active substances that are known to cause both adverse effects (Table 4).
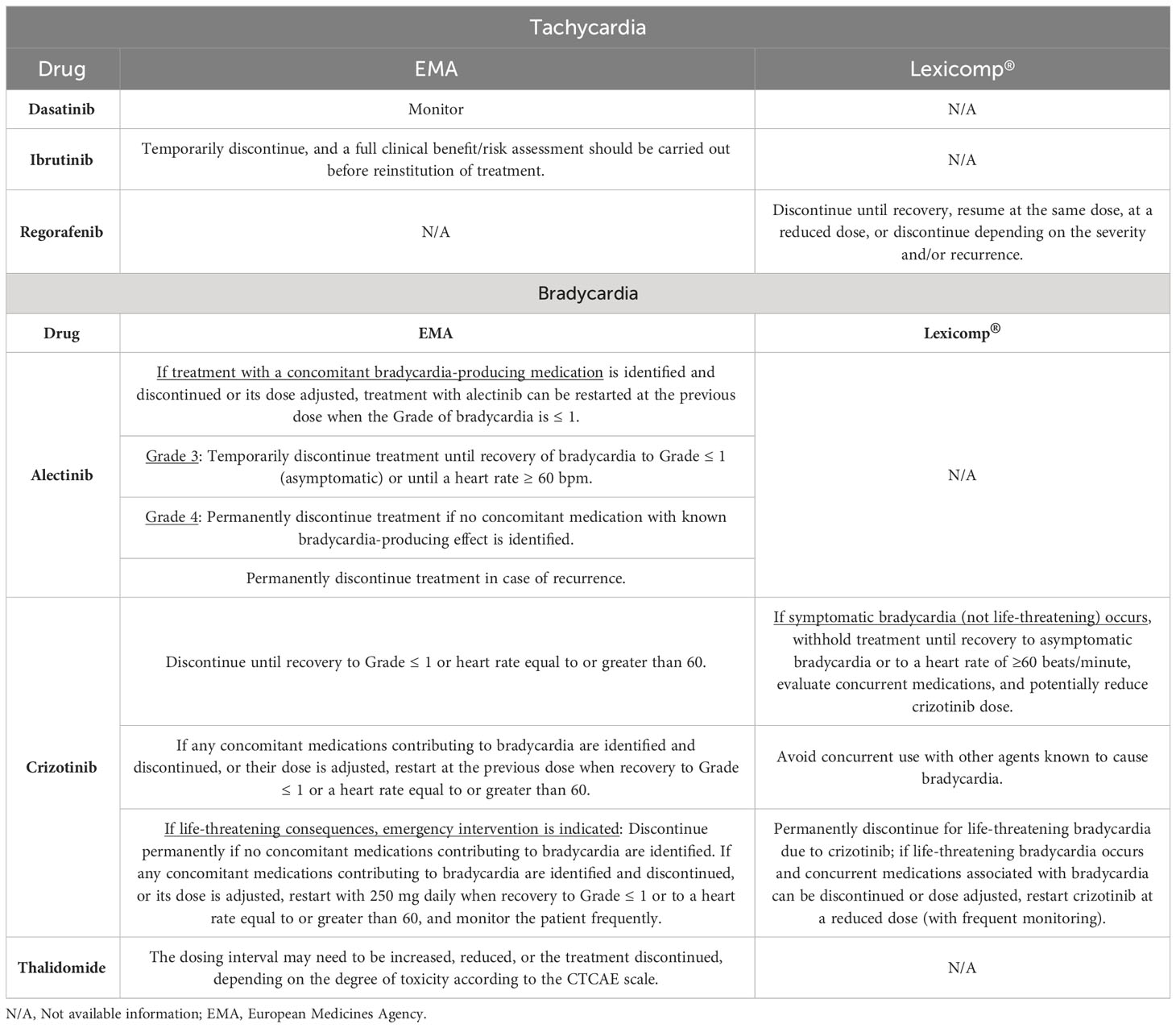
Table 4 Specific recommendations concerning oral antineoplastic agents in case of tachycardia and bradycardia.
Regarding thrombosis, 30 (32.3%) of the drugs analyzed included the appearance of a thrombus as a possible AE (Table 5). Specific management recommendations are issued in seven cases and often indicate OAA discontinuation in case of occurrence. For treatments with melphalan, lenalidomide, pomalidomide, or thalidomide, prophylactic antithrombotic treatment is recommended.
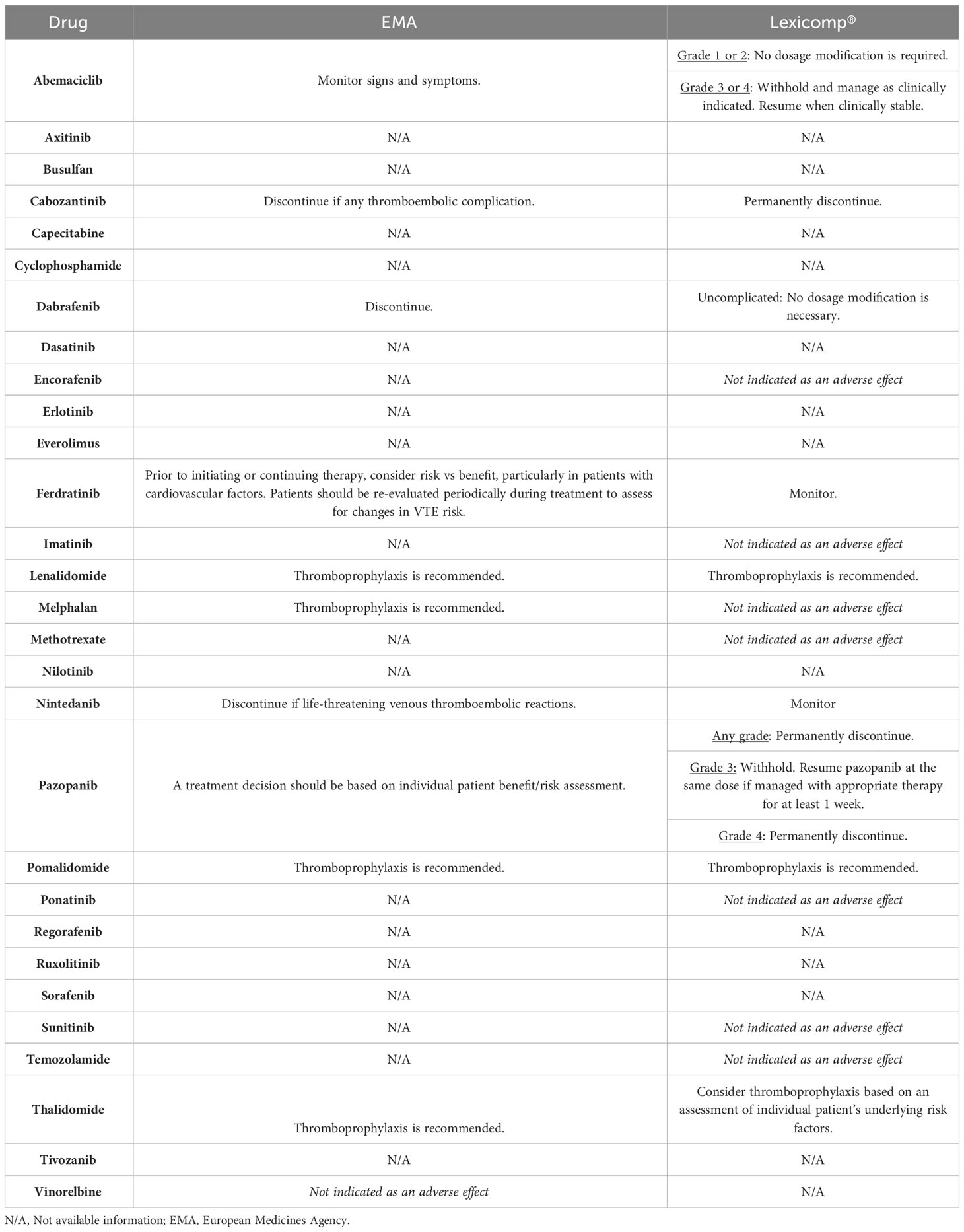
Table 5 Specific recommendations concerning oral antineoplastic agents in case of thrombosis.
A total of 10 OAAs have been associated with hypertriglyceridemia and hypercholesterolemia; we found that 3 (everolimus, lorlatinib, and nilotinib) out of 10 have a specific dose adjustment management (Table 6).

Table 6 Specific recommendations concerning oral antineoplastic agents of changes in the lipidic metabolism.
4 Discussion
To the best of our knowledge, this is the first guide to summarize the updated recommendations concerning the use of OAAs with their cardiotoxic effects and posology adjustments according to the EMA and Lexicomp®.
The fast inclusion in the clinical practice of OAAs, their significant adverse events, and the scarce experience with some groups of patients that were not included in clinical trials make it extremely important that careful management of OAAs is implemented. The mechanism and frequency of cardiotoxicity brought on by targeted molecular therapy are mainly unclear and probably underestimated. Healthcare professionals play a crucial role in patient education, assisting in identifying and managing AEs and drug interactions. Recently, the European Society of Cardiology (ESC) issued its first guideline, providing guidance on the definitions, diagnosis, treatment, and prevention of cancer therapy-related CV toxicity, and the management of CV disease caused directly or indirectly by cancer (6). However, this guideline does not detail specific recommendations for each of the drugs or dose adjustments. Therefore, we suggest that our review complements the recommendations provided by the ESC.
Our review presents a comprehensive guide of available recommendations concerning the dose and posology of OAAs when cardiotoxic events appear. We aimed to compile these recommendations to help clinicians to decide when to change the dose, end treatment, or take another action when a cardiac AE is detected. Considering the limitations of the information used to establish the safety profile of drugs during the premarketing period, there is a need for continuous safety surveillance after approval. As many of these therapeutic agents are approved through expedited procedures, the number of SPC changes in the postmarketing phase due to safety issues has increased. Likewise, it should be noted that specific information on dose adjustment recommendations in cases of adverse effects is reduced so that, in many cases, the recommendations are general for each side effect and not specific for each drug.
4.1 QT prolongation
Tyrosine kinase inhibitors are the therapeutic class most frequently associated with cardiac toxicities such as QT prolongation, left ventricular dysfunction, or arterial hypertension. QT prolongation is a severe cardiotoxic effect, which can lead to ventricular tachycardia (Torsades de Pointes) (10). Although this AE is rare, it is potentially life-threatening, and there is currently not much data on the prevalence of Torsade de Pointes in patients with cancer. We have identified that 29.0% of the OAAs analyzed can prolong the QT interval. A recent review that focused on QT prolongation graded 205 anticancer drugs as low, moderate, and high risk of QT prolongation. The authors identified eight drugs with a high risk of QT prolongation: arsenic trioxide, imatinib, ivosidenib, nilotinib, ribociclib, thiopental, toremifene, and vandetanib (11).
Several risk factors may increase the risk of QT prolongation. Among the non-cardiac risk factors are being from the female sex and hypothyroidism. Among the cardiac risk factors are congenital long QT syndrome, left ventricular dysfunction, and myocardial ischemia. In addition to QT prolongation, risk factors also increase the risk of concomitant treatments (antidepressants, antiemetics, antibiotics, antipsychotics, anti-fungal, antihistamines, and methadone) and AEs associated with cancer therapy (nausea and vomiting, dehydration followed by electrolyte imbalances such as hypokalemia, hypomagnesemia, and hypocalcemia, and of other adverse effects such as kidney failure, liver dysfunction, and poorly controlled diabetes) (12). Before starting a new OAA, these risk factors should be evaluated and corrected as possible, specifically potassium, calcium, and magnesium levels. Besides, patients with cancer often are polymedicated; thus, it is essential to check the possible drug-drug interactions between OAAs and cytochrome P450 3A4 inhibitors (amiodarone, digoxin, antihistamines, atorvastatin, carbamazepine, corticosteroids, etc.) since they can increase the plasma concentrations of many of the antiangiogenic protein kinase inhibitors. A dose reduction of the OAA may be necessary in these cases. That is the reason why ESC guidelines recommend avoiding heterogeneity in the method of corrected-QT measurement, defining a clear threshold of 500 msec as risky, and ruling out other causes of QT prolongation as ionic imbalances or other QT-prolonging drugs frequently prescribed in cancer patients (6). Otherwise, a QT prolongation can be interpreted as a concern and lead to an early withdrawal of a potentially beneficial antitumoral drug. The multidisciplinary management of cardiotoxicity in cardio-oncology units is mandatory to avoid such an error and should be generalized.
4.2 LVEF decrease
Left ventricular dysfunction and heart failure may occur due to mitochondrial damage, alterations in cardiac energy balance, and contractile protein dysfunction (13). The inhibition of platelet-derived growth factor receptor (PDGFR) and other tyrosine kinase receptors in cardiomyocytes, which determines their functioning and survival, disrupts the typical response of the myocyte to hypertensive stress (14). We have identified that 9.7% of the analyzed OAAs can decrease LVEF.
Various studies demonstrated heart failure with reduced ejection fraction or other cardiomyopathies induced by OAAs, such as encorafenib, lorlatinib, osimertinib, or sunitinib (15–17). Patel SR et al. observed, in a series of cases, that cardiotoxicity from osimertinib was reversible. They hypothesized that dose reduction may be a potential solution to prevent initial or recurrent cardiotoxicity (18). The initiation of heart failure drugs is recommended, and these patients should be referred to cardio-oncology for further studies and follow-up (19). Rechallenge of the drug may be considered under strict surveillance after a multidisciplinary discussion on the risk/benefit ratio (6).
4.3 Hypertension and hypotension
Hypertension is one of the most common comorbidities in cancer survivors and patients with active cancer. Its incidence varies according to age, history of hypertension, cancer type, and treatment. A retrospective large cohort study was conducted to estimate the incidence rates of new-onset hypertension in adult cancer patients. New-onset hypertension was observed in approximately one-third of the 25,090 patients with various types of cancer. The incidence rates of severe and crisis-level hypertension were highest in patients with gastric and ovarian cancer (20). Across all cancers, chemotherapy exposure was associated with a 2- to 3.5-fold increase in the risk of any grade of hypertension compared with periods without chemotherapy; higher hypertension levels showed more significant variability in relative risks by type and line of treatment but indicated an overall increase associated with chemotherapy exposure (21).
The mechanism by which OAAs induce hypertension is not entirely understood but can be directly related to the inhibition of vascular endothelial growth factor (VEGF) signaling via tyrosine kinase (22). The VEGF signaling pathway is also present in normal vascular endothelium, playing a physiological role in its function and in nitric oxide synthesis, thus its block compromises vasodilation. The pro-hypertensive mechanism of action is a class effect and is directly related to its antitumor action, so the increase in blood pressure, paradoxically, may be a marker of the effectiveness of oncologic treatment (23). Fortunately, blood pressure control with antihypertensive drugs does not seem to affect the effectiveness of anticancer treatment. The hypertensive effect of these agents is reversible, so a decrease in dose or temporary discontinuation of treatment can be used to control hypertension. This applies especially to protein kinase inhibitors, as they are administered daily orally for prolonged periods and can be restarted, or the dose adjusted once hypertension has been controlled with appropriate medication. Strict blood pressure control reduces the risk of heart failure and atrial fibrillation and avoids the need to interrupt effective anticancer treatment (24). According to our study, 36.6% of OAAs have hypertensive potential. Specifically, angiogenesis inhibitor drugs (VEGF pathway inhibitors) have a class effect on blood pressure and show the most significant problems. Introducing these drugs highlighted the importance of hypertension during cancer treatment since, as a group, they can induce it with a frequency that has been variably estimated to be between 17% and 80% of cases in different studies (25).
4.4 Lipid imbalance
The pathogenesis of hypertriglyceridemia associated with mTOR agent use, such as everolimus, is poorly understood but may be related to the reduced degradation of apolipoprotein B100 (26). Apolipoprotein B100 is formed in the liver and is essential to the assembly of very low-density lipoproteins. Additionally, everolimus may lower levels of lipoprotein lipase activity and increase free fatty acid levels, which can contribute to dyslipidemia (27). Specific recommendations for controlling cardiovascular risk factors in patients with cancer have been agreed upon by Spanish societies of cardiology, oncology, hematology, radiation oncology, and general practitioners and can serve as a guide for the management of this frequent adverse effect (3).
Screening for lipid levels is recommended for individuals without cardiovascular disease (CVD), especially for those with risk factors such as hypertension, family history of premature CVD, diabetes, and smoking. Lifestyle interventions, including smoking cessation, a Mediterranean diet, and exercise, should be discussed with all patients. For secondary prevention patients, high-intensity statin therapy is strongly encouraged, while for primary prevention patients, the decision to initiate moderate- or high-intensity statins should be based on individual CVD risk. Statin therapy is generally not recommended for primary prevention patients over 75 years, but exceptions can be made based on individual patient factors. Patients who cannot tolerate specific statin regimens may be offered lower-intensity options or alternate dosing schedules. Non-statin lipid-lowering drugs are not recommended as first-line monotherapy in primary prevention. Adherence to statin therapy should be reinforced, and monitoring of CK and ALT levels should be reserved for symptomatic or higher-risk patients as determined by the attending clinician (28).
4.5 Thrombosis
Regarding the thrombotic effect, some studies emphasized the importance of the ribosomal S6 kinase family, as it determines cardiomyocyte survival by inhibiting the phosphorylation of apoptosis-activating factors (2). By interfering with this molecular pathway, KIs may promote cardiac damage. The inhibition of the KIT and RAF1 pathways leads to vascular stem cell damage and endothelial dysfunction. Endothelial cell apoptosis and exposure to subendothelial collagen initiate the coagulation process, leading to thromboembolic episodes. Approximately 20% of patients with venous thromboembolism (VTE) have current cancer, according to extensive population-based studies and disease registry surveys. In these patients, VTE is linked to decreased survival and negatively affects the quality of life (29). In our review, we identified that 32.3% of OAAs may increase the risk of thrombosis. We also observed that patients with cancer are especially at risk of developing thrombosis.
In terms of study limitations, we have not found in the sources consulted any recommendations for the management of some OAAs, despite their cardiotoxicity. Therefore, the application of this guide would help to identify them as cardiotoxic drugs, but not help in their management. Second, we have focused this review on OAAs, but it should be taken into account that other cancer treatments, such as parenteral chemotherapy, immunotherapy, or monoclonal antibodies, can also produce cardiotoxic effects. In addition, it should be noted that continued research and approval of new OAAs are being developed. Finally, data were obtained from EMA and Lexicomp; thus, in cases with limited information, other sources, such as data from clinical trials, can be consulted to supplement the available information. Having the EMA and Lexicomp recommendations in the same Table could confuse some healthcare professionals as to which recommendation to follow. However, the objective is to have more information available, which can be useful in different situations. For example, a European professional could follow the EMA recommendations, or if another professional has doubts, it may be useful to consult both sources.
In conclusion, more than half of the OAAs can produce cardiotoxic effects, with the most frequent being blood pressure alteration and QT interval prolongation with a non-depreciable incidence of LV dysfunction or thrombosis. Before starting the treatment, it is necessary to stratify baseline cardiovascular risk, plan a surveillance schedule, and consider referral to cardio-oncology units, especially in high-risk patients such as those with pre-existing bradycardia, those taking anti-arrhythmic medicines or other drugs known to prolong QT intervals, and patients with previous heart disease or developed cardiotoxicity.
We suggest that this review can serve as a reference guide for the professionals involved in managing patients with cancer since it provides an easy way to identify the cardiotoxic effects of OAAs and the need for dosage adjustments.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
VE-V, RC-B, and CV-B defined the research question and objectives. VE-V, RC-B, CV-B, JR-H, SP-R, and EZ-N defined the methodology of the study. ER-R, PR-B, VE-V, XG-G, and SI-G conducted a search for information for the preparation of the guide. VE-V, AH, and MS were responsible for the research activity plan and its execution. ER-R and VE-V wrote the first draft. All authors contributed to the article and approved the submitted version.
Conflict of interest
VE-V received support for continuing education/advisory fees from Amgen, Astellas, Bristol-Myers Squibb, GlaxoSmithKline, Janssen, Merck Sharp & Dohme, Novartis, Roche, Sanofi, and Sobi outside the submitted work; RC-B received support for continuing education/advisory fees from Amgen, Astellas, Bristol-Myers Squibb, GlaxoSmithKline, Janssen, Merck Sharp & Dohme, Novartis, and Roche outside the submitted work. XG-G received support for continuing education/advisory fees from Amgen, Astellas, and Galápagos outside the submitted work. EZ-N received support for continuing education/advisory fees from AstraZeneca and Bayer outside the submitted work. AH received support for continuing education/advisory fees from Kern and Janssen outside the submitted work. MS received support for continuing education/advisory fees from Janssen, Roche, and Amgen outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1220305/full#supplementary-material
References
1. Escudero-Vilaplana V, Ribed A, Romero-Jimenez RM, Herranz-Alonso A, Sanjurjo-Saez M. Pharmacotherapy follow-up of key points in the safety of oral antineoplastic agents. Eur J Cancer Care (Engl) (2017) 26(3). doi: 10.1111/ecc.12463
2. Grela-Wojewoda A, Pacholczak-Madej R, Adamczyk A, Korman M, Püsküllüoğlu M. Cardiotoxicity induced by protein kinase inhibitors in patients with cancer. Int J Mol Sci (2022) 23(5):2815. doi: 10.3390/ijms23052815
3. Martín García A, Mitroi C, Mazón Ramos P, García Sanz R, Virizuela JA, Arenas M, et al. Stratification and management of cardiovascular risk in cancer patients. A consensus document of the SEC, FEC, SEOM, SEOR, SEHH, SEMG, AEEMT, AEEC, and AECC. Rev Esp Cardiol (Engl Ed) (2021) 74(5):438–48. doi: 10.1016/j.rec.2020.11.020
4. Varricchi G, Ameri P, Cadeddu C, Ghigo A, Madonna R, Marone G, et al. Antineoplastic drug-induced cardiotoxicity: a redox perspective. Front Physiol (2018) 9:167. doi: 10.3389/fphys.2018.00167
5. Herrmann J, Lenihan D, Armenian S, Barac A, Blaes A, Cardinale D, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement. Eur Heart J (2022) 43(4):280–99. doi: 10.1093/eurheartj/ehab674
6. Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, et al. ESC Scientific Document Group. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J (2022) 43(41):4229–361. doi: 10.1093/eurheartj/ehac244
7. Organization WH. ATC/DDD Index 2022 (2022). Available at: https://www.whocc.no/atc_ddd_index/ (Accessed 2 June 2022).
8. National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0 (2017) (Bethesda, Maryland).
9. Gill D, Gaston D, Bailey E, Hahn A, Gupta S, Batten J, et al. Efficacy of eplerenone in the management of mineralocorticoid excess in men with metastatic castration-resistant prostate cancer treated with abiraterone without prednisone. Clin Genitourin Cancer (2017) 15(4):e599–602. doi: 10.1016/j.clgc.2016.12.008
10. Rao VU, Reeves DJ, Chugh AR, O'Quinn R, Fradley MG, Raghavendra M, et al. Clinical approach to cardiovascular toxicity of oral antineoplastic agents: JACC state-of-the-art review. J Am Coll Cardiol (2021) 77(21):2693–716. doi: 10.1016/j.jacc.2021.04.009
11. Porta-Sánchez A, Gilbert C, Spears D, Amir E, Chan J, Nanthakumar K, et al. Incidence, diagnosis, and management of QT prolongation induced by cancer therapies: a systematic review. J Am Heart Assoc (2017) 6(12):e007724. doi: 10.1161/JAHA.117.007724
12. Baracaldo-Santamaría D, Llinás-Caballero K, Corso-Ramirez JM, Restrepo CM, Dominguez-Dominguez CA, Fonseca-Mendoza DJ, et al. Genetic and molecular aspects of drug-induced QT interval prolongation. Int J Mol Sci (2021) 22(15):8090. doi: 10.3390/ijms22158090
13. Berger M, Amini-Adlé M, Maucort-Boulch D, Robinson P, Thomas L, Dalle S, et al. Left ventricular ejection fraction decrease related to BRAF and/or MEK inhibitors in metastatic melanoma patients: A retrospective analysis. Cancer Med (2020) 9(8):2611–20. doi: 10.1002/cam4.2922
14. Chen MH, Kerkelä R, Force T. Mechanisms of cardiac dysfunction associated with tyrosine kinase inhibitor cancer therapeutics. Circulation (2008) 118(1):84–95. doi: 10.1161/CIRCULATIONAHA.108.776831
15. Okuzumi S, Matsuda M, Nagao G, Kakimoto T, Minematsu N. Heart failure with reduced ejection fraction caused by osimertinib in a patient with lung cancer: a case report and literature review. Cureus (2022) 14(8):e27694. doi: 10.7759/cureus.27694
16. Jin Y, Xu Z, Yan H, He Q, Yang X, Luo P. A comprehensive review of clinical cardiotoxicity incidence of FDA-approved small-molecule kinase inhibitors. Front Pharmacol (2020) 11:891. doi: 10.3389/fphar.2020.00891
17. Haas NB, Manola J, Ky B, Flaherty KT, Uzzo RG, Kane CJ, et al. Effects of adjuvant sorafenib and sunitinib on cardiac function in renal cell carcinoma patients without overt metastases: results from ASSURE, ECOG 2805. Clin Cancer Res (2015) 21(18):4048–54. doi: 10.1158/1078-0432.CCR-15-0215
18. Patel SR, Brown SN, Kubusek JE, Mansfield AS, Duma N. Osimertinib-induced cardiomyopathy. JACC Case Rep (2020) 2(4):641–5. doi: 10.1016/j.jaccas.2019.12.038
19. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Rev Esp Cardiol (Engl Ed) (2022) 75(6):523. doi: 10.1016/j.rec.2022.05.005
20. Fraeman KH, Nordstrom BL, Luo W, Landis SH, Shantakumar S. Incidence of new-onset hypertension in cancer patients: a retrospective cohort study. Int J Hypertens (2013) 2013:379252. doi: 10.1155/2013/379252
21. Robinson ES, Khankin EV, Karumanchi SA, Humphreys BD. Hypertension induced by vascular endothelial growth factor signaling pathway inhibition: mechanisms and potential use as a biomarker. Semin Nephrol (2010) 30(6):591–601. doi: 10.1016/j.semnephrol.2010.09.007
22. Camarda N, Travers R, Yang VK, London C, Jaffe IZ. VEGF receptor inhibitor-induced hypertension: emerging mechanisms and clinical implications. Curr Oncol Rep (2022) 24(4):463–74. doi: 10.1007/s11912-022-01224-0
23. Yasaka M, Yamaguchi T. Secondary prevention of stroke in patients with nonvalvular atrial fibrillation. CNS Drugs (2001) 15:623–31. doi: 10.2165/00023210-200115080-00005
25. Escalante CP, Zalpour A. Vascular endothelial growth factor inhibitor-induced hypertension: basics for primary care providers. Cardiol Res Pract (2011) 2011:816897. doi: 10.4061/2011/816897
26. Busaidy NL, Farooki A, Dowlati A, Perentesis JP, Dancey JE, Doyle LA, et al. Management of metabolic effects associated with anticancer agents targeting the PI3K-Akt-mTOR pathway. J Clin Oncol (2012) 30(23):2919–28. doi: 10.1200/JCO.2011.39.7356
27. Subramaniam S, Zell JA, Kunz PL. Everolimus causing severe hypertriglyceridemia and acute pancreatitis. J Natl Compr Canc Netw (2013) 11(1):5–9. doi: 10.6004/jnccn.2013.0003
28. Allan GM, Lindblad AJ, Comeau A, Coppola J, Hudson B, Mannarino M, et al. Simplified lipid guidelines: Prevention and management of cardiovascular disease in primary care. Can Fam Physician (2015) 61(10):857–67, e439-50.
Keywords: adverse event, cancer, cardiology, cardiotoxicity, oral antineoplastic therapy, safety
Citation: Ramos-Ruperez E, Escudero-Vilaplana V, Ruiz-Briones P, Collado-Borrell R, Villanueva-Bueno C, Revuelta-Herrero JL, González-Haba E, Garcia-Gonzalez X, Ibañez-Garcia S, Perez-Ramirez S, Zatarain-Nicolás E, Herranz A and Sanjurjo M (2023) Medication guide for dose adjustment and management of cardiotoxicity and lipid metabolic adverse events of oral antineoplastic therapy. Front. Oncol. 13:1220305. doi: 10.3389/fonc.2023.1220305
Received: 10 May 2023; Accepted: 02 August 2023;
Published: 25 August 2023.
Edited by:
Luigi Tarantini, IRCCS Local Health Authority of Reggio Emilia, ItalyReviewed by:
Agnes S. Kim, UCONN Health, United StatesAlessandro Inno, Ospedale Sacro Cuore Don Calabria, Italy
Vijay Udyavar Rao, Franciscan Health, United States
Copyright © 2023 Ramos-Ruperez, Escudero-Vilaplana, Ruiz-Briones, Collado-Borrell, Villanueva-Bueno, Revuelta-Herrero, González-Haba, Garcia-Gonzalez, Ibañez-Garcia, Perez-Ramirez, Zatarain-Nicolás, Herranz and Sanjurjo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente Escudero-Vilaplana, dmljZW50ZS5lc2N1ZGVyb0BzYWx1ZC5tYWRyaWQub3Jn